Embed Size (px)
Citation preview

FROM THE ANAlyST’S COUCH
HIV combination productsLisette Oversteegen, Mansi Shah and Holger Rovini ‘Wing sofa sleeper’, image courtesy of eurway.com
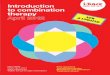
Three years after the discovery of the human immunodeficiency virus (HIV) in 1984, GlaxoSmithKline’s (GSK’s) Retrovir (zidovudine) became the first drug to be approved for the treatment of this disease (FIG. 1). It belongs to the class of nucleoside reverse transcriptase inhibitors (NRTIs), which have been at the forefront of antiretroviral therapy ever since.
However, even in combination with each other, NRTIs could only produce transient viral suppression and the necessity to administer high doses led to high levels of toxicity and resistance. With the introduction of HIV protease inhibitors (PIs) in 1995, it was found that major and prolonged reductions in viral burden could be achieved by the combination of a PI with two NRTIs — known as highly active antiretroviral therapy (HAART). Similar results were later obtained by adding a member of a third class of drugs known as non-nucleoside reverse transcriptase inhibitors (NNRTIs) to two NRTIs. NNRTI-based HAART regimens have quickly become the preferred choice for initial anti-retroviral therapy, whereas drugs from the newest classes, such as Roche and Pfizer’s entry inhibitors and Merck’s integrase inhibitor, form useful adjuncts.
The evolution of NRTI combinationsAdherence to antiretroviral regimens is a key factor in achieving durable viral suppression and limiting the development of drug resistance. However, initial anti-HIV regimens required taking as many as 18 pills daily, and so efforts to allow easier dosing schedules and reduce pill burden became focal points for many companies. GSK launched Combivir (lamivudine/zidovudine), the first fixed-dose combination of two NRTIs, in 1997. As a single tablet taken twice-daily, it rapidly became the backbone of HAART. GSK launched two more NRTI combinations, Trizivir and Epzicom, in 2000 and 2004, respectively.
Trizivir (lamivudine, abacavir and zidovudine) is the only triple NRTI combination that is currently available; however, it has been associated with greater toxicity and sub-optimal virological
activity. Meanwhile, acceptance for Epzicom (lamivudine/abacavir) has been higher owing to its once-daily administration, although both fixed-dose combinations have been linked to hypersensitivity reactions to its abacavir component.
A fourth NRTI combination, Gilead’s Truvada (tenofovir/emtricitabine), was launched in the United States in 2004 and in Europe in 2005. Its favourable tolerability, once-daily dosing and superior efficacy over Combivir made this drug the new gold-standard in the NRTI class. Truvada was also the overall highest-selling drug on the market for the treatment of HIV in 2006, with sales of approximately US$1.2 billion worldwide¹.
The first cross-class combinationNRTI combinations have greatly improved patient adherence to therapy, but as they must still be combined with drugs from other classes in order to maximize the efficacy of the HAART regimen, the pill burden is still significant. The first cross-class fixed-dose combination, Atripla, was developed by Gilead and Bristol–Myers Squibb (BMS), and launched in 2006 in the United States. This once-daily pill containing an NNRTI (efavirenz) and two NRTIs (tenofovir and emtricitabine) is more efficacious compared with the dual NRTI combinations and has greatly simplified early stage HIV therapy. Atripla has therefore become the most popular choice of therapy for the treatment-naive patients.
Although Atripla is the only branded cross-class combination available in Western countries (table 1), India-based generics companies, such as Aurobindo and Cipla, have developed and received FDA approval for several other NNRTI–NRTI/NRTI products under the US President’s Emergency Plan for AIDS Relief (PEPFAR) programme. These cross-class combinations comprise of older compounds that have been surpassed in efficacy and safety by newer products, but are still prescribed in developing countries. As soon as the patents of the individual ingredients of these combinations expire, generics companies will be allowed to promote their products
in the high-priced United States market as well. Although these will be no match for modern products like Atripla, the cheaper combinations of generic drugs are still likely to experience a rapid uptake, particularly in an increasingly cost containment-focused environment.
The future of combination productsThe current dual NRTI combinations are highly effective, simple and convenient with relatively mild side effects. The key unmet need in this class is still for agents to combat viral resistance. The lack of novel dual NRTI combinations that address this need can be attributed to the slow progress of pipeline NRTIs resulting from several mid-stage development setbacks. However, there are more opportunities to create cross-class combinations, for example, a product combining the components of a PI-based HAART regimen.
Gilead and BMS could be in a good position to build on their collaboration in the development of Atripla and develop a cross-class combination consisting of Gilead’s developmental integrase inhibitor, elvitegravir, and BMS’s once-daily PI Reyataz (atazanavir). Such a combination could potentially become a popular choice of therapy for the treatment-experienced population because of atazanavir’s good safety profile and once-daily dosing.
Furthermore, members of newer classes of drugs such as chemokine (c-c motif) receptor 5 (CCR5) entry inhibitors and integrase inhibitors, which have recently been approved as part of combination regimens in treatment-experienced patients, could also be combined with existing products to create novel cross-class combinations.
However, such strategies require key players, who perceive each other as competitors, to share sensitive information in order to collaborate. An alternative strategy would be to acquire a developmental compound from a smaller company. An example for this is the takeover of Triangle Pharmaceuticals (who developed emtricitabine) by Gilead, enabling Gilead to formulate Truvada, which became the first blockbuster drug in HIV therapy. ▶
N e w s & a N a ly s i s
NATURE REVIEWS | drug discovery VolUME 6 | DECEMBER 2007 | 951
© 2007 Nature Publishing Group

Nature Reviews | Drug Discovery
1,500
1,000
500
2,000
0
HIV
-rel
ated
dea
ths
200620042002200019981996199419921990198819861984
HIVdiscovered
First NRTI(Retrovir)launched
First PI(Invirase)launched
First NNRTI(Viramune)launched
First EI(Fuzeon)launched
First NRTI+NRTIcombination(Combivir) launched
First NRTI+NRTI+NNRTI combination(Atripla) launched
Impactof HAART
Nature Reviews | Drug Discovery
Single- componentHIV drugs
Epzicom
Truvada
Trizivir
Combivir
Atripla
US$8 billion US$9.8 billion
a 2006 b 201063%
14%
10%
5%
2%6% 54%
15%
2%
6%
3%
20%
HIV COMbINATION pROdUCTS | maRkeT INdIcaToRs
▶
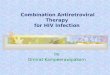
Figure 1 | Timeline of the development of the Hiv market (1984–2006) and uK Hiv-related deaths (1894–2005)3. EI, entry inhibitors; HAART, highly active antiretroviral therapy; NNRTI, non-nucleoside reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; PI, protease inhibitor.
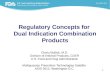
of all anti-HIV drug classes, the NRTIs had the highest sales in 2006, followed by the PIs. In 2010, Datamonitor expects the entry inhibitors (EIs) and other novel drug classes such as integrase inhibitors to have a large share of the HIV market. Revenues of the NRTI class will decrease owing to major patent expiries. Atripla is furthermore expected to take a significant share away from the NRTI combination Truvada.
Sales of combination products totalled almost $3 billion in 2006 (REF. 2), more than half of these revenues were attributed to GSK’s combination products. However, the launch of Atripla will make Gilead and BMS more prominent players in the HIV arena. In 2010, revenues of combination products are estimated to account for almost $4.5 billion, which is 45% of the overall HIV sales in the six major markets (France, Germany, Italy, Spain, UK and the US) (FIG. 2) with a compound annual growth rate (CAGR) of %10 (REF. 2) (2006–2010).
Lisette Oversteegen, Mansi Shah & Holger Rovini are at Datamonitor Healthcare,
108–110 Finchley Road, London NW3 5JJ, UK. e-mail: [email protected]
doi:10.1038/nrd2448
1. Gilead 2006 Annual Report. Gilead Sciences 2006 Annual Report [online], http://www.gilead.com/AR2006/index.php (2006).
2. MIDAS Sales Data, IMS Health, April 2007. 3. Health Protection Agency (2006). A complex picture —
HIV & other sexually transmitted infections in the United Kingdom: 2006. [online], http://www.hpa.org.uk/publications/2006/hiv_sti_2006/pdf/a_complex_Picture_2006_last.pdf (2007).
Figure 2 | Market shares (by sales) of fixed dose combination products of the total Hiv market in 2006 and 2010 (estimated)2.
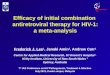
Table 1 | overview of currently launched fixed-dose combination products for the treatment of HIV*
drug class Pill volume
Total pills per day
dosing schedule
combination product Total pills per day
dosing schedule
2006 sales‡
Tenofovir NRTI 300 mg Once dailyTruvada
Atripla
Once daily 1,125
Emtricitabine NRTI 200 mg Once daily Once daily 174
Efavirenz NNRTI 600 mg Once daily – – –
Abacavir NRTI 300 mg Once dailyEpzicom
Combivir
Trizivir
Once daily 396
Lamivudine NRTI 300 mg Once daily Twice daily 478
Zidovudine NRTI 300 mg Twice daily Twice daily 789
*From REF. 2. ‡Sales in US$ millions are based on MIDAS sales data, IMS Health April 2007. NNRTI, non-nucleoside transcriptase inhibitor; NRTI, nucleoside transcriptase inhibitor.
N e w s & a N a ly s i s
952 | DECEMBER 2007 | VolUME 6 www.nature.com/reviews/drugdisc
© 2007 Nature Publishing Group