Embed Size (px)
Citation preview

HIV and TB Co-infection HIV and TB Co-infection
North Dakota HIV SymposiumNorth Dakota HIV SymposiumMay 19, 2010May 19, 2010
David McNamara, M.D. David McNamara, M.D.
Clinical Assistant Professor of Medicine Clinical Assistant Professor of Medicine
University of North DakotaUniversity of North Dakota
Infectious Disease Division Infectious Disease Division
MeritCare, Fargo ND MeritCare, Fargo ND

Disclosures Disclosures
• No commercial disclosures No commercial disclosures
• Dakota AIDS Education & Training Dakota AIDS Education & Training Center Center

Learning ObjectivesLearning Objectives
• Learners should be familiar with:Learners should be familiar with:
• Epidemiology of HIV-TB Co-infectionEpidemiology of HIV-TB Co-infection
• HIV screening in TB infectionHIV screening in TB infection
• Drug interactions between Drug interactions between medications for HIV and TBmedications for HIV and TB

OverviewOverview
• Scope of Problem Scope of Problem
• TB in HIV infection TB in HIV infection
• DiagnosisDiagnosis
• TreatmentTreatment
• Drug Interactions Drug Interactions
• SummarySummary

Convergence of Two EpidemicsConvergence of Two Epidemics
• Catastrophic collision of Catastrophic collision of TB and HIV infection TB and HIV infection
• Worldwide 2008:Worldwide 2008:
• 33.2 million persons HIV+33.2 million persons HIV+• ~~30% co-infected with TB 30% co-infected with TB
• 9.4 million new TB cases 9.4 million new TB cases • 40% increase from 199040% increase from 1990• Driven by HIV epidemic Driven by HIV epidemic
Chaisson R. JID 2010:201 (1 March)Chaisson R. JID 2010:201 (1 March)

• ~~1/3 HIV infected persons worldwide are 1/3 HIV infected persons worldwide are infected with TB (usually latent)infected with TB (usually latent)
• 8-10% develop active disease each year8-10% develop active disease each year
• 20072007• 9.27 million new TB cases 9.27 million new TB cases
• 15% occurred in HIV+ persons15% occurred in HIV+ persons• Africa 80%Africa 80%• India 11% India 11%
• 450,000 deaths from TB in HIV+ persons 450,000 deaths from TB in HIV+ persons
Swaminathan S. CID 2010:50 (15 May) Swaminathan S. CID 2010:50 (15 May)
Epidemiology Epidemiology

Mortality Mortality
• Worldwide Worldwide • 1.8 million deaths from TB in 20071.8 million deaths from TB in 2007
• 25% (450,000) also HIV+ 25% (450,000) also HIV+ • 2 million deaths from HIV 2 million deaths from HIV
• 22% from TB22% from TB
• TB the leading cause of death in HIV TB the leading cause of death in HIV
• HIV infection contributes to HIV infection contributes to ~~1/4 TB 1/4 TB deaths deaths

Geographic DistributionGeographic DistributionWHO Global Tuberculosis Control 2009 Report WHO Global Tuberculosis Control 2009 Report

Swaminathan S. CID 2010:50 (15 May) Swaminathan S. CID 2010:50 (15 May)

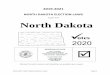
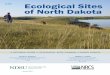
Estimated HIV Coinfection in Persons Reported Estimated HIV Coinfection in Persons Reported with TB, United States,with TB, United States,
1993–2008*1993–2008*
0
10
20
30
1993 1996 1999 2002 2005 2008
All Ages Aged 25–44
% C
oin
fect
ion
*Updated as of May 20, 2009.
Note: Minimum estimates based on reported HIV-positive status among all TB cases in the age group.
cdc.govcdc.gov

ImplicationsImplications
• Global TB incidence and mortality Global TB incidence and mortality would be decreasing if not for HIV would be decreasing if not for HIV epidemicepidemic
• Increasingly, need to manage Increasingly, need to manage patients with both HIV and TB patients with both HIV and TB
• Why this deadly synergy between Why this deadly synergy between these two infections? these two infections?
Swaminathan S. CID 2010:50 (15 May) Swaminathan S. CID 2010:50 (15 May)

OverviewOverview
• Scope of ProblemScope of Problem
• TB in HIV infectionTB in HIV infection
• DiagnosisDiagnosis
• Treatment Treatment
• Drug Interactions Drug Interactions
• Summary Summary

Biology of TBBiology of TB
• If airborne TB inhaled, person becomes infectedIf airborne TB inhaled, person becomes infected
• Most develop latent (inactive) TB Infection Most develop latent (inactive) TB Infection • immune system sequesters TB bacilli and immune system sequesters TB bacilli and
prevents active infectionprevents active infection• can reactivate to active TB in future can reactivate to active TB in future
• ~5-~5-10% lifetime risk for HIV negative 10% lifetime risk for HIV negative • ~~8-10% per year with untreated HIV 8-10% per year with untreated HIV
• Some develop active TB right awaySome develop active TB right away• Will feel sick, spread disease to others Will feel sick, spread disease to others • More likely if immunocompromised More likely if immunocompromised
• HIV, chemotherapy, elderly, malnourishedHIV, chemotherapy, elderly, malnourished

Biology of HIV Biology of HIV
• HIV infection depletes CD4+ T cellsHIV infection depletes CD4+ T cells
• T-cell arm of immune systemT-cell arm of immune system• Cellular control of infection withCellular control of infection with
• VirusesViruses• FungiFungi• Mycobacteria Mycobacteria
• HIV-infected patients vulnerable to infection HIV-infected patients vulnerable to infection with pathogens that immune system usually with pathogens that immune system usually controls controls

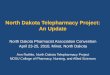
http://msl.cs.uiuc.edu/~yershova/bcb495/bcbProject-3.htm
HIV Infection: CD4 Cell DeclineHIV Infection: CD4 Cell Decline

Manifestations of TB in HIV+ personsManifestations of TB in HIV+ persons
• Depends on level of immunosuppressionDepends on level of immunosuppression
• Early HIV infection Early HIV infection • similar to non-HIV patientssimilar to non-HIV patients• pulmonary disease predominatespulmonary disease predominates
• AIDS: severe immunosuppression AIDS: severe immunosuppression • extrapulmonary sites common extrapulmonary sites common • miliary, lymphadenitis miliary, lymphadenitis • paucibacillary disease, lymphadenitis paucibacillary disease, lymphadenitis
• Similar to childhood TBSimilar to childhood TB• AFB-smear negative pulmonary disease AFB-smear negative pulmonary disease

HIV-TB ChallengesHIV-TB Challenges
• Prompt diagnosisPrompt diagnosis
• Effective treatmentEffective treatment
• Successful prevention strategies Successful prevention strategies
• TB Recurrence in HIV+ persons after TB Recurrence in HIV+ persons after therapy completion therapy completion

Recurrence of TB Recurrence of TB
• HIV-negative patients with 4-drug therapy and DOTHIV-negative patients with 4-drug therapy and DOT• 2-3% recurrence 2-3% recurrence
• HIV-positive patientsHIV-positive patients• 14+ % recurrence rate14+ % recurrence rate
• Some relapse with original strainSome relapse with original strain• Most re-infect with new strain Most re-infect with new strain • Often with MDR TBOften with MDR TB
• Why this discrepancy? Why this discrepancy? • TB treatment does not alter ongoingTB treatment does not alter ongoing
• immunosuppression immunosuppression • risk for TB exposurerisk for TB exposure

What can reduce recurrence rates? What can reduce recurrence rates?
• Complete DOT for all patients with TBComplete DOT for all patients with TB
• ART for patients with TB and HIV ART for patients with TB and HIV
• Infection control in HIV and TB care Infection control in HIV and TB care settings settings

OverviewOverview
• Scope of ProblemScope of Problem
• TB in HIV infection TB in HIV infection
• DiagnosisDiagnosis
• Treatment Treatment
• Drug Interactions Drug Interactions
• Summary Summary

Challenges in Diagnosis Challenges in Diagnosis of HIV-associated TBof HIV-associated TB
• Fewer bacilli in sputum than HIV –Fewer bacilli in sputum than HIV –
• Sputum AFB smear standard Sputum AFB smear standard diagnostic method in most regionsdiagnostic method in most regions
• HIV+ patients more likely to HIV+ patients more likely to have smear-negative pulmonary have smear-negative pulmonary TBTB
• Sputum AFB culture slow, not Sputum AFB culture slow, not readily available readily available
• CXR: less sensitive in HIV+ CXR: less sensitive in HIV+ • ~~14-22% HIV + patients with 14-22% HIV + patients with
pulmonary TB have normal CXR pulmonary TB have normal CXR

• MicroscopyMicroscopy• AFB smearAFB smear• Cheap, rapidCheap, rapid• Depends on bacterial load Depends on bacterial load • Low sensitivity in HIVLow sensitivity in HIV
~~45% 45%
• Culture Culture • More sensitive than More sensitive than
microscopy microscopy • Can use probes on +culture Can use probes on +culture
to differentiate TB from NTM to differentiate TB from NTM (common in HIV+ patients)(common in HIV+ patients)
Diagnostic Methods Diagnostic Methods

Diagnostic Methods Diagnostic Methods
• Sputum direct Probe (MTD)Sputum direct Probe (MTD)• Sensitivity variable in smear negative disease Sensitivity variable in smear negative disease • Expensive, complex to performExpensive, complex to perform
• PPD skin testPPD skin test• Poor sensitivity in HIV due to anergyPoor sensitivity in HIV due to anergy• Can’t differentiate latent vs. active disease Can’t differentiate latent vs. active disease • Poor sensitivity in setting of active TBPoor sensitivity in setting of active TB
• In HIV negative patients, only In HIV negative patients, only ~~50% +PPD 50% +PPD
• QuantiFERON blood testQuantiFERON blood test• Interferon gamma release assay Interferon gamma release assay • Can’t differentiate latent vs. active TBCan’t differentiate latent vs. active TB• Does not differentiate between IRIS and Does not differentiate between IRIS and
failure of TB treatment failure of TB treatment

• All patients with active TB need an HIV blood testAll patients with active TB need an HIV blood test
• Order: HIV 1/2 Antibody Order: HIV 1/2 Antibody
• HIV/TB co-infection significantly impacts HIV/TB co-infection significantly impacts prognosis and drug treatmentprognosis and drug treatment
• Treat both HIV and TBTreat both HIV and TB• Protease Inhibitor Antiretrovirals Protease Inhibitor Antiretrovirals
• significant interaction with Rifampin significant interaction with Rifampin
Diagnosis of HIV Diagnosis of HIV

% w
ith
Tes
t R
es
ult
s
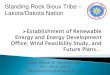
*Updated as of May 20, 2009.
Note: Includes TB patients with positive, negative, or indeterminate HIV test results. Persons from California reported with AIDS only through 2004. (HIV test results are not reported from California)
Reporting of HIV Test Results Reporting of HIV Test Results in Persons with TB by Age Groupin Persons with TB by Age Group
United States, 1993–2008*United States, 1993–2008*
0
20
40
60
80
1993 1996 1999 2002 2005 2008
All Ages Aged 25–44
cdc.govcdc.gov

WHO Global Tuberculosis Control 2009 Report WHO Global Tuberculosis Control 2009 Report

OverviewOverview
• Scope of ProblemScope of Problem
• TB in HIV infection TB in HIV infection
• DiagnosisDiagnosis
• TreatmentTreatment • Latent TB in setting of HIV Latent TB in setting of HIV • Active TB with HIV co-infectionActive TB with HIV co-infection• When to start ART (AntiRetroviral Therapy)When to start ART (AntiRetroviral Therapy)
• Drug Interactions Drug Interactions
• Summary Summary

Latent TB and Latent TB and HIV infection HIV infection
• Screen for latent TB in HIV+ patientsScreen for latent TB in HIV+ patients• PPD skin test (PPD skin test (>>5 mm positive)5 mm positive)• QuantiFERON blood test can be QuantiFERON blood test can be
used; limited dataused; limited data
• Isoniazid 300mg PO daily x 9 monthsIsoniazid 300mg PO daily x 9 months

Treatment of Active TB Treatment of Active TB with HIV Co-infection with HIV Co-infection
• Refer to Refer to • physician expert in both HIV and physician expert in both HIV and
TB treatmentTB treatment• Public Health RN for DOTPublic Health RN for DOT
• Why? Why?
• Risk for failure highRisk for failure high• negative consequences to patient, negative consequences to patient,
close contacts and community close contacts and community

Treatment of Active TB Treatment of Active TB with HIV Co-infection with HIV Co-infection
• Basic principles in HIV+ similar to non-HIVBasic principles in HIV+ similar to non-HIV
• HIV-TB specific challenges HIV-TB specific challenges • Frequency of anti-mycobacterial Frequency of anti-mycobacterial
administrationadministration• Drug interactions Drug interactions • Overlapping drug toxicitiesOverlapping drug toxicities• IRIS: Immune Reconstitution IRIS: Immune Reconstitution
Inflammatory Syndrome Inflammatory Syndrome

First-line TB therapy First-line TB therapy
• Induction phase: 8 weeks Induction phase: 8 weeks • INH, RIF, PZA, EMB daily or 3x/ weekINH, RIF, PZA, EMB daily or 3x/ week
• Continuation phase: 18 weeksContinuation phase: 18 weeks• INH, RIF daily or 3x/weekINH, RIF daily or 3x/week
• Every effort should be made to use Every effort should be made to use rifamycin-based therapy for entire course rifamycin-based therapy for entire course
• Continuation phase: avoidContinuation phase: avoid• once-weekly INH-rifapentine once-weekly INH-rifapentine • 2x/ week dosing 2x/ week dosing

Treatment: DOTTreatment: DOTDirectly Observed Directly Observed
Therapy Therapy
• Mandatory for all active tuberculosisMandatory for all active tuberculosis
• Critical for HIV-TB Co-infectionCritical for HIV-TB Co-infection• Risk of relapse is higher Risk of relapse is higher
• Public Health RN Public Health RN

Treatment:Treatment:When to start antiretroviral therapy? When to start antiretroviral therapy?
• Optimal timing of initiation of ART in active Optimal timing of initiation of ART in active TB has been uncertainTB has been uncertain
• Concerns Concerns • Drug interactions (rifampin and PIs)Drug interactions (rifampin and PIs)• Overlapping drug toxicitiesOverlapping drug toxicities• IRISIRIS• High pill burdenHigh pill burden• Programmatic challenges Programmatic challenges

Karim et al. NEJM 362;8. Feb. 25, 2010Karim et al. NEJM 362;8. Feb. 25, 2010
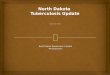
• SAPIT Trial, South Africa SAPIT Trial, South Africa
• 642 patients with TB, HIV and CD4 <500 cells/uL642 patients with TB, HIV and CD4 <500 cells/uL
• Randomized to 3 groups for ART initiation Randomized to 3 groups for ART initiation • Early Integrated: within 4 weeksEarly Integrated: within 4 weeks• Late Integrated: within 4 weeks of completion Late Integrated: within 4 weeks of completion
of Intensive phase TB treatmentof Intensive phase TB treatment• Sequential: After completion of TB therapySequential: After completion of TB therapy

• Study stopped early due to decreased mortality in Study stopped early due to decreased mortality in integrated therapy groupsintegrated therapy groups
• 56% relative reduction in risk of death 56% relative reduction in risk of death
• Adverse effects similar between groups Adverse effects similar between groups
Karim et al. NEJM 362;8. Feb. 25, 2010Karim et al. NEJM 362;8. Feb. 25, 2010

IRIS:IRIS:Immune Reconstitution Inflammatory SyndromeImmune Reconstitution Inflammatory Syndrome
• Worsening of symptoms or X Ray with Worsening of symptoms or X Ray with immunologic recovery immunologic recovery
• Occurs with infections in settings of Occurs with infections in settings of immunosuppression when immune system immunosuppression when immune system recoversrecovers
• HIV, chemotherapy, immunosuppressantsHIV, chemotherapy, immunosuppressants• Mycobacterial and fungal diseases Mycobacterial and fungal diseases
• Common as CD4 cell count improves with ART Common as CD4 cell count improves with ART
• Hard to tell between treatment failure and IRISHard to tell between treatment failure and IRIS
• Treat with steroidsTreat with steroids
• Occasionally may have to hold ARTOccasionally may have to hold ART

OverviewOverview
• Scope of ProblemScope of Problem
• TB in HIV infection TB in HIV infection
• Diagnosis Diagnosis
• Treatment Treatment
• Drug InteractionsDrug Interactions
• Summary Summary

Drug InteractionsDrug Interactions
• Significant drug interactions between Significant drug interactions between cornerstone drugs cornerstone drugs
• antimycobacterials antimycobacterials • rifampin, rifabutin rifampin, rifabutin
• antiretroviralsantiretrovirals• Protease InhibitorsProtease Inhibitors• NNRTIs: efavirenz NNRTIs: efavirenz
• Despite this, imperative to treat TB with Despite this, imperative to treat TB with rifamycin-based therapy if at all possible rifamycin-based therapy if at all possible

Sterling TR CID 2010; 50(S3):S223-230Sterling TR CID 2010; 50(S3):S223-230

Drug InteractionsDrug Interactions
• Rifamycins and Protease Inhibitors Rifamycins and Protease Inhibitors • Rifampin will Rifampin will PI levels PI levels
• Avoid rifampin and PIs Avoid rifampin and PIs • Use efavirenz-based ART if possibleUse efavirenz-based ART if possible
• low dose Rifabutin ok with PIs low dose Rifabutin ok with PIs • Rifabutin 150 mg 3x/week Rifabutin 150 mg 3x/week
• Rifampin and NNRTIRifampin and NNRTI• use high dose efavirenz 800 mg daily use high dose efavirenz 800 mg daily
• Avoid rifampin and raltegravir Avoid rifampin and raltegravir

Drug Interactions Drug Interactions
• Treatment of TB-HIV co-infection by Treatment of TB-HIV co-infection by physician expert in treatment of both physician expert in treatment of both
• Verify regimens and dosing with Verify regimens and dosing with referencesreferences
• Incorrect dosing leads to: Incorrect dosing leads to:
• Resistance in both HIV and TBResistance in both HIV and TB
• Treatment failure Treatment failure
• Spread of drug-resistant TB Spread of drug-resistant TB

OverviewOverview
• Scope of ProblemScope of Problem
• TB in HIV infection TB in HIV infection
• Diagnosis Diagnosis
• Treatment Treatment
• Drug Interactions Drug Interactions
• Summary Summary

SummarySummary
• Screen for HIV Screen for HIV
• Maintain high index of suspicion for Maintain high index of suspicion for TB in HIV patients TB in HIV patients
• Patients with HIV-TB co-infection Patients with HIV-TB co-infection should be managed by physician should be managed by physician expert in both diseases expert in both diseases
• All patients with active TB need an All patients with active TB need an HIV testHIV test
• All patients with TB need DOT All patients with TB need DOT

Acknowledgments Acknowledgments
• Anne Grande, Education Coordinator, Anne Grande, Education Coordinator, Dakota AIDS Education & Training Dakota AIDS Education & Training CenterCenter
• North Dakota Department of Health North Dakota Department of Health

Resources Resources
• Centers for Disease Control and PreventionCenters for Disease Control and Prevention
•cdc.govcdc.gov
• National Jewish Medical CenterNational Jewish Medical Center•nationaljewish.orgnationaljewish.org
•Denver TB courseDenver TB course