Embed Size (px)
Citation preview

HIV and Infant Feeding
CARK Region Conference on Prevention of HIV Infection in Infants,
Almaty March 1-3 2005
Dr. Arun Gupta MD FIAP
Regional Coordinator IBFAN Asia Pacific

Outline of the Presentation
• Overview
• UN Goals and Guidelines
• Risk of transmission and some issues
• Experience from India, training materials developed
• Way forward
• Some challenges

In 5 participating nations
Country EBF 0-6I.M.R
• Turkmenistan 13 71
• Kazakhstan 36 61
• Tajikistan 14 53
• Uzbekistan 16 52
• Kyrgyzstan 24 52
Source : SOWC 2004

Timing of Mother-to-Child Timing of Mother-to-Child TransmissionTransmission
Early Antenatal(<36 wks)
Late Antenatal(36 wks to labor)
Late Postpartum(6-24 months)
Early Postpartum(0-6 months)
Adapted from N Shaffer, CDC
5-10% 10-20% 10-20%
Labor and Delivery BreastfeedingPregnancy

MTCT in 100 HIV+ Mothers by Timing of Transmission
0
20
40
60
80
100
Uninfected: 63
Breastfeeding: 15
Delivery: 15
Pregnancy: 7

Global Strategy for Infant and Young Child Feeding
• Adopted by the WHA and UNICEF Executive board in 2002
• Recognises that 2/3 deaths of annual 10.9 million U-5 deaths, occur during 1st yr. and are related to inappropriate feeding practices
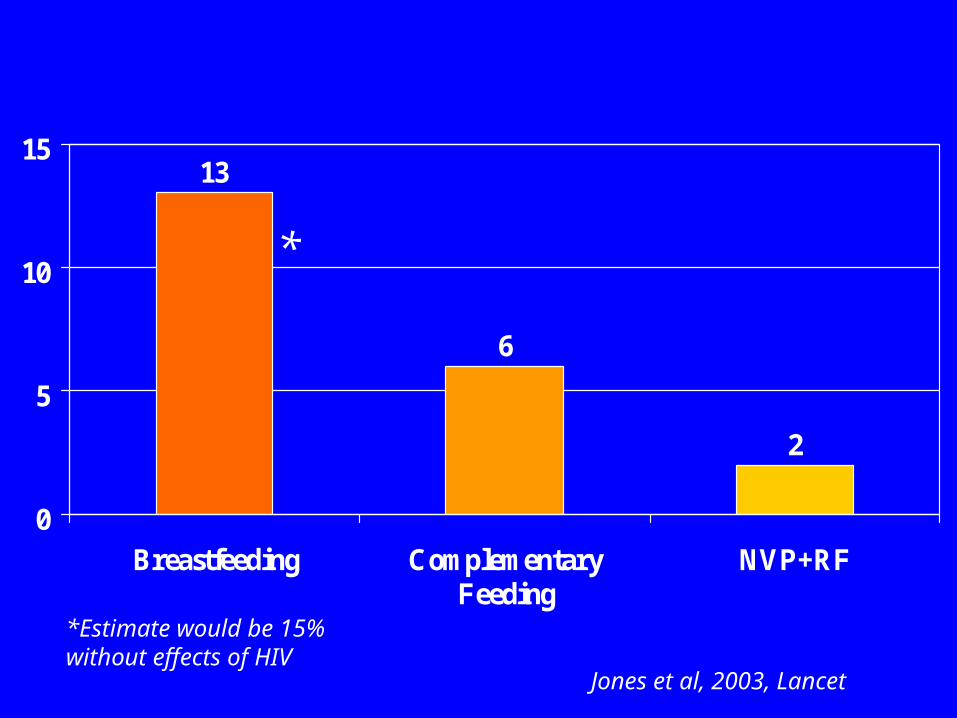
Proportion of all < 5 yrs deaths that could be prevented with infant feeding
interventions 13
6
2
0
5
10
15
Breastfeeding ComplementaryFeeding
NVP+RF
Jones et al, 2003, Lancet
*
*Estimate would be 15% without effects of HIV

Risks of artificial feeding(in developing countries risks are elevated above these
levels)
Increased levels of accute illness:
• Respiratory infections
• Middle ear infection: 3-4x risk
• Gastroenteritis: 3-4x risk (developing countries 17-25x)
• Bacterial infection requiring hospitalization: 10x risk
• Meningitis: 4x risk
• Higher mortality from sudden infant death syndrom (SIDS)

Risks of Artificial feeding
Dose-related difference in mental development:
• Lower scores of mental development tests at 18 months
• Difference in mental development and school performance at 3-5 years
• Lower scores of prematures on intelligence tests at 7-8 years
• Deficits in neurological development (lack of essential fatty acids)
• Difference in visual acuity

Risks …….
Effects on the health of mothers:
• Higher risk of impaired bonding, abuse, neglect and abandonment
• Increased risk of anemia due to early return of menstruation
• Increased risk of breast and ovarian cancer
• Increased risk of new pregnancy
HIV/Infant feeding is about Assessing the risks
Breastfeeding Formula
HIV Mortality
Unique global consensus
• 9 UN agencies ratified in 2003
• 5 priority actions, first being development of policy and plans for IYCF including HIV, promotion of exclusive breastfeeding for ALL babies

UN Guidelines 2004
According to the UN Guidelines, replacement feeding choice be supported by HIV positive women when it is acceptable, feasible, affordable , sustainable and safe for them. Otherwise exclusive breastfeeding during first months is recommended.

Key elements on Infant Feeding in the European
strategy• Positioned firmly within the context of
human rights
• Reiterating the UN recommendations
• Emphasis on counselling and support for the chosen option
• Interventions within the context of overall protection, promotion and support of breastfeeding
• Emphasis on Code and BFHI implementation

Risk of transmission and some issues

Risk Factors For Postnatal Transmission
Mother• Immune/health
status
• Plasma viral load
• Breast milk virus
• Breast inflammation (mastitis, abscess, nipple lesions)
• New HIV infection
• Viral Characteristics
Infant• Breastfeeding
duration
• Non-exclusive BF
• Age (first months)
• Lesions in mouth, intestine
• Prematurity
• Infant immune response

Risk Factor: Early Mixed breastfeeding
7
1619
25
7
2426
36
0
5
10
15
20
25
30
35
40
Birth 3 mo 6 mo 15 mo
%EBF to 3 mo
Partial BF
Coutsoudis et al, 1999; 2001
Cumulative HIV transmission Durban, SA

Postnatal HIV Transmission
12.814.7
8.77
0
5
10
15
EBF PBF MBF Total
% H
IV
+ at
18 m
onth
s
Piwoz et al., MoPpB2008
(n=2055)(n=2055)ZVITAMBO, ZimbabweZVITAMBO, Zimbabwe
by Early Feeding Practicesby Early Feeding Practices
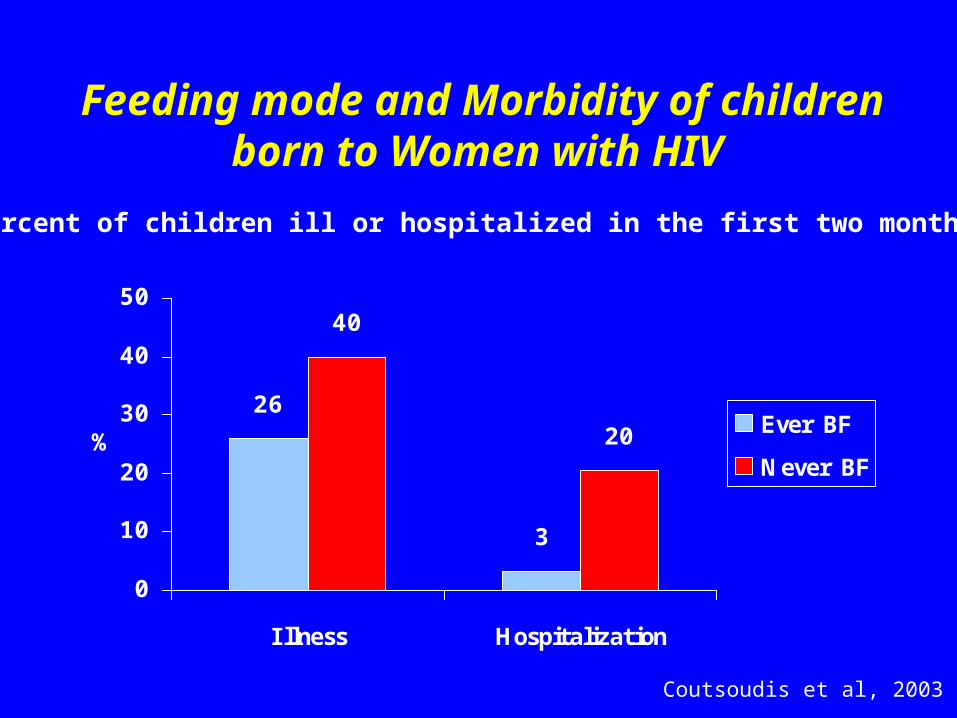
Feeding mode and Morbidity of children born to Women with HIV
26
40
20
3
0
10
20
30
40
50
I llness Hospitalization
%Ever BF
Never BF
Coutsoudis et al, 2003
Percent of children ill or hospitalized in the first two months

Higher Rates of Hospitalization for Non-Breastfed Infants of HIV+
Mothers in a PMTCT Program in Pune, India
Phadke et al, 2003
BF Non-BF
sample 62 86
hospitalizations 0 27*
deaths 0 4
*p<0.0001, no significant differences between BF and non-BF for any other infant or maternal characteristics

Global experience
A compilation and review of current global programme evidence – mostly “grey literature”

Mixed Feeding Before 6 Months
• Although results differed across programs, most HIV-positive mothers ended up mixed feeding, often very soon after delivery, regardless of whether they chose to replacement feed or exclusively breastfeed initially
• Across cultures, there is great pressure to introduce other liquids or foods (often ritual) by two months or even earlier
• This issue needs wider Behaviour change focus

Exclusive breastfeeding vs RF
• Both are a big challenge
• Aim at avoiding “mixed feeding”
• “World missing opportunity to reduce mother-to child HIV transmission through exclusive breastfeeding “….UNICEF Press Release

Exclusive breastfeeding Vs RF
• As effective as RF in reducing MTCT
• New hope for countries where RF is not AFASS as increasing exclusive breastfeeding rates would in fact reduce infant HIV in general populations
• Exclusive breastfeeding is achievable may be up to 70% if not 100% (Macedonia, Armenia, and many countries have shown)

Elements of PMTCT/PPTCT
• Voluntary and confidential HIV testing and counselling in routine antenatal care;
• Ensuring that ANC includes detection and treatment of sexually transmitted infections (STIs) and counselling on safer sex;
• Provision of prophylactic antiretroviral drugs to HIV-positive pregnant women and, in some regimens, to their babies;
• Safer obstetric practices;
• Counselling and support for informed decisions on feeding

Attn: Counseling for IF options
• HIV positive women get adequate info on all options on breastfeeding or replacement feeding.
• Info: unbiased, accurate and individualized, it should be compatible with local cultures and her beliefs.
• Info alone is not enough , more efforts are needed to modify her behaviour, here comes role of counseling by health staff.

India experience

Qualitative study
• Feasibility study reported that 70% women who chose RF return to ‘mixed feeding’ in 2 weeks period.
• Counseling bias existed towards RF
• Where good IF counselling was made available, more women chose exclusive breastfeeding

National action
• A colloquium on infant feeding and HIV
• Strong partnerships established with Government of India NACO, UNICEF and others.
• Led to several consultations and further to assessment of current status of counseling develop training for infant feeding options

Assessment of VCCTC / PPTCT counselors
• None Knew about AAFSS
• None Knew 10 Steps of Successful BF
• None knew about national recommendation on optimal infant feeding

How did we address this• Combined the training modules of WHO/UNICEF on
Breastfeeding(1998) and IF-HIV(2000) counseling, based on UN guidelines, updated including AFASS and exclusive breastfeeding. (Infant feeding and HIV Counselling course: 5-6 days)
• Tested and prepared trainers ( existing set of trainers of breastfeeding counseling were chosen)
• Trained all 54 counsellors of Delhi state having 11 centers of PPTCT ( 15 million population)
• Added complementary feeding (3rd WHO/UNICEF course 2002)
• 3 in 1 course has been now ready and trainers are available , 7 days instead of 11 days.
(6 days are needed additionally to prepare trainers)



Way forward

Key action for decision makers
• A national level colloquium to address this problem and build consensus among various partners, and share new information to plan ahead.
• And Assessment process can then begin

Key action….
Situation Assessment and analysis– Policy development addressing IF&HIV
– Implementing the CODE
– Prevention of HIV aims at women and children
– Current programmes on breastfeeding for ALL babies
– Does clarity exists on integration of counseling of HIV & IF in services
– Has the costs been calculated
– Training materials, job aid available for health workers
– Are woman provided counseling
– Is there sufficient capacity to undertake this task

Actions to strengthen existing approaches
• CODE implementation: – Takes out baby food manufacturers out of programme
implementation
– takes care of accurate unbiased information
– it is for ALL babies and mothers,
– Ensures independent research free from commercial interest
• BFHI : cans set standards of care and opportunity for action– VCCT
– Training facility for counsellors
– Counselling on all feeding options

Strengthen approaches for making breastfeeding safer for ALL women
• Provide adequate lactation counseling and support, involving families/communities
– increase adherence to exclusive breastfeeding
– promote good breastfeeding techniques
– prevent cracked nipples, maintain breast health
• Immediate treatment for mastitis, other systemic infections that could affect viral load in BM
– could prevent a sizeable fraction of BF transmission
– may be most important in early month(s)
• Safe sex/condom use for prevention

Make breastfeeding safer for HIV+ women
• Assist families with decisions about early breastfeeding cessation
– assess health status of mother and infant
– prepare for the process so that the transition is safe (cup-feeding, safe preparation/hygiene, stigma)
– heat treat breast milk if weaning is gradual
– could prevent ½ to ¾ of BF transmission
• Provide adequate infant nutrition after breastfeeding ends
– appropriate breast milk substitutes and/or multi-nutrient supplements should be provided to prevent malnutrition

Make replacement feeding safer for HIV+ women
• Provide safe water & environmental conditions
– rural and urban areas may vary
• Family support, community understanding
• Postnatal follow-up and enhanced care
– essential child health interventions
• Screen mothers, target use to those most at risk
• Take measures to prevent unnecessary use of RF
– need to strengthen efforts to support optimal infant feeding for all

Some challenges

Challenges
• HIV testing capacity -counseling on RF not possible without mother’s testing and knowing her status.
• Balancing risk of not breastfeeding vs risk of HIV from BF ->the role of BF in child survival in adverse conditions
• Prevention of ‘spillover’
• Increasing exclusive breastfeeding rates
• Replacing BM in infants’ diet. BF contributes 100% nutrient needs of up to 6mos, 50% to 1yr; and 35% up to 2yrs!

Challenges
Identifying RF that is available and can meet the nutritional needs of baby, meets all AFASS conditions and avoids spillover effects to the majority of children.
Formative research and direct observations of homes in both rural and urban settings helps answer this, incl. discussions with mothers
Quality counselling is very important especially for infant feeding as poor counselling may lead to mixed feeding resulting in greater risk of HIV transmission via BF

Challenges
• Capacity for follow up of HIV positive mothers, whether exclusively breastfeeding or exclusively artificially feeding/nutrition support/breast care/primary prevention!
• Monitoring and evaluation: Many programmes suffer from lack of M/E providing no or little evidence of health effects and benefits/impact of the different options, and extent of spillover.
• Ensuring Human Rights are not cast aside but rather embedded in legal frameworks

Thank you !



























