Embed Size (px)
Citation preview

B
HA
HVa
b
c
ARRAA
KHMRS4V
pwApf
0d
Journal of Virological Methods 175 (2011) 129– 132
Contents lists available at ScienceDirect
Journal of Virological Methods
jou rn al h om epage: www.elsev ier .com/ locate / jv i romet
rief report
IV-1 nucleotide mixture detection in the virco®TYPE HIV-1 genotyping assay: comparison between Sanger sequencing and 454 pyrosequencing
ans De Wolfa,∗, Herwig Van Marckb, Wendy Mostmansb, Kim Thysa, Ina Vandenbrouckeb,eerle Van Eygenb, Theresa Patterya, Peter Verhasselt c, Jeroen Aerssensb
Virco BVBA, Turnhoutseweg 30, 2340 Beerse, BelgiumTibotec BVBA, Turnhoutseweg 30, 2340 Beerse, BelgiumJanssen, Turnhoutseweg 30, 2340 Beerse, Belgium
rticle history:eceived 12 January 2011eceived in revised form 19 April 2011ccepted 20 April 2011vailable online 27 April 2011
eywords:IV-1ixtures
esistance testinganger54iral load
a b s t r a c t
HIV-1 Protease (PR) and Reverse Transcriptase (RT) genotyping is well established for the managementof antiretroviral (ARV) drug therapy, as it is able to detect gene mutations encoding resistance to ARVcompounds or drug classes, that are associated with reduced drug susceptibility (i.e. phenotype). A cor-rect phenotypic interpretation from the derived PR–RT genotype (i.e. virtual phenotype), requires a wellcharacterized geno-phenotype correlative database and appropriate statistical predictive models. Theapplicability of the virtual phenotype for the patient, will, however, not only depend on the accuracy ofthe statistical models and the database they rely on, but also depend largely on the sequence informationthat is provided. Since HIV-1 evolves as a complex of closely related but non-identical viral genomes (i.e.quasispecies) it is crucial that the sequencing method used, is able to characterize most of the geneticmixtures that make up the different quasispecies within a single patient. US regulatory agencies requirethat developers of HIV-1 genotyping assays, determine and report the HIV-1 mixture detection level oftheir assay. Hence, the mixture scoring sensitivity of the population-based Sanger sequencing method,along with the defined mixture scoring rules, used to drive the virco®TYPE HIV-1 virtual phenotype,was investigated by comparing it to the 454 pyrosequencing technique, which is able to generate thecomplete viral population sequence. To this end the PR–RT coding sequence of 20 clinical isolates wasdetermined by both sequencing methodologies. The genotyping assay which feeds the virco®TYPE HIV-1virtual phenotype was able to call automatically 97.5% (i.e. 268 mixtures) and 95.3% (i.e. 326 mixtures) ofthe mixtures that were present between 25 and 75% and between 20 and 80% in the viral population, asdetected by 454. From the not called mixtures, all but one did present a mixture sequence in the SangerDNA chromatograms, however, with a peak surface area for the second peak that was below the thresholdsetting for automatic mixture calling in the basecaller software (i.e. 25%). Viral loads ranged from 470 to629,000 copies/mL and exerted no effect on the mixture calling relationship between both sequencing
2
methodologies (R = 0.92). In some occasions (i.e. 55 mixtures) the genotyping assay would detect auto-matically mixtures that were present below 20% in the viral population, when measured by 454. Hence,the mixture scoring sensitivity of the automated high throughput virco®TYPE HIV-1 genotyping assayis currently set at 97.5% and 95.3%, for mixtures present at 25 and 20% in the viral population and mayidentify occasionally mutations that are present at lower frequencies. These findings were not influencedby the viral load of the examined samples.In order to manage successfully therapy for HIV-1 affectedatients antiretroviral (ARV) drug resistance testing has becomeidespread in the developed world (Hirsch et al., 2008). Optimal
RV drug regimen, long term suppression of the virus and therevention of emerging resistant strains can, indeed, be derivedrom the ARV drug resistance test outcome, which is measured∗ Corresponding author. Tel.: +32 014 64 18 76.E-mail address: [email protected] (H. De Wolf).
166-0934/$ – see front matter © 2011 Elsevier B.V. All rights reserved.oi:10.1016/j.jviromet.2011.04.023
© 2011 Elsevier B.V. All rights reserved.
as a fold change (FC) in the half maximal inhibitory concentra-tion (IC50) of the ARV drug. A variety of high throughput genotypicand phenotypic assays are available on the market, providing ARVdrug resistant information (e.g. Hirsch et al., 2008; Van Houteet al., 2009; Broder, 2010). Among them, the virco®TYPE HIV-1 assay (Virco, Belgium) infers IC50 fold changes from the viral
genotype using the Virtual phenotypeTM Linear model (VPT-LM)(for review see Van Houte et al., 2009). The latter uses 2nd orderlinear regression (LRM) to model genotype–phenotype associa-tions from a large correlative database, adopting biological and/or
1 logica
c2
sbSldwKLpa(
vptaasottsMnCn
ecq2crs
emtfitMsdmasaapccinp(nsp
deua
30 H. De Wolf et al. / Journal of Viro
linical cut-offs to determine the drug susceptibility (Winters et al.,009).
More specifically, the HIV-1 PR–RT coding sequence is tran-cribed reversely and amplified in a one step RT-PCR, followedy a nested PCR. PR–RT amplicons are prepared subsequently foranger sequencing, using a high throughput ABI 3730xl capil-ary sequencer from Applied Biosystems. Resistant mutations areetected by comparing the viral PR–RT sequence from the patientith the Wild Type (WT) HXB2 reference strain (GenBank ID:03455). The amino acid mutation profile is fed into the VPT-M, after which an ARV resistance profile is calculated for thatarticular HIV-1 genotype, based on weight factors that are associ-ted with ARV drug resistant mutations or mutation combinationsVermeiren et al., 2007).
The Sanger sequencing method, which is used to obtain theiral PR–RT sequences, is driven by a dye-terminator sequencingrocess. During this process, DNA fragments are tagged differen-ially, based on their ending nucleotide and ordered into subsetsccording to their length. Separation of the different fragments isccomplished in the ABI 3730xl true capillary gel electrophore-is (for a review see Dolnik, 1999). The latter results in a seriesf Gaussian-like peaks that correspond to either one of the fourerminal DNA nucleotides (i.e. DNA chromatogram). The size ofhe peak is proportional to the number of DNA fragments in theub-population of fragments with the same length (Andrade andanolakos, 2004). Time ordering of the peaks results in the DNA
ucleotide sequence. To this end, Sequencher v 4.1.4 (Gene Codesorporation) is used, which calls automatically the most likelyucleotides, based on the raw DNA chromatogram.
Due to its high reverse transcriptase error rate, HIV-1 does, how-ver, not evolve as a single genome, but rather forms a complex oflosely related but non-identical genomes within the patient (i.e.uasispecies) (e.g. Garcia-Arriaza et al., 2007; Paredes and Clotets,010). Hence, without prior labor intensive and time consumingloning techniques the DNA chromatogram produced by Sangeremains a mixture of different HIV-1 genotypes (i.e. populationequence).
Recently, several “next generation” sequencing technologiesmerged that offer the possibility to sequence single DNA frag-ents from complex mixtures, at a relatively low cost and a high
hroughput mode (for a review see Metzker, 2010). Of these, therst commercially available technology, Roche’s 454, circumventshe cloning requirement by using an emulsion PCR (Morozova and
arra, 2008). During this process, a single bead containing one,ingle-strand DNA is isolated within a PCR mixture droplet. Eachroplet acts as an individual amplification reactor, yielding severalillion clonal copies of a unique DNA fragment per bead (Morozova
nd Marra, 2008). Each DNA-containing bead is deposited into aingle well of a picotiter plate and is sequenced subsequently using
sequencing-by-synthesis technique (i.e. pyrosequencing). When new nucleotide is added to the growing DNA chain by the DNAolymerase, a pyrophosphate molecule is released. ATP Sulfurylaseonverts the pyrophosphate into ATP which drives the enzymaticonversion of luciferin and associated emission of photons, releas-ng a chemiluminescent signal. The signal is recorded and theon-incorporated nucleotides are washed away. Signal intensity isroportional to the number of nucleotides that are incorporatedi.e. homopolymers). This cycle is repeated for each of the fourucleotides resulting in a sequential signaling pattern that corre-ponds to the nucleotide sequence of the DNA template (i.e. DNAyrogram) (Margulies et al., 2005).
Compared to Sanger sequencing, 454 generates “raw” sequence
ata at approximately 100 times higher throughput (Strausbergt al., 2008). As such, 454 technology is able to generate the individ-al HIV-1 genomes that are present as mixtures within the patientnd make up the entire viral population sequence. Calling thesel Methods 175 (2011) 129– 132
mixtures correctly in a population sequence is a pre-requisite forcorrect assignment and early monitoring of the ARV drug resis-tant associated mutations. US regulatory agencies require thatdevelopers of HIV-1 genotyping assays, determine and report theHIV-1 mixture detection level of their assay (U.S. Department ofHealth and Human Services, Food and Drug Administration, 2007).The latter is expected generally to range between 20 and 40%for Sanger sequencing based assays when viral loads are above1000 copies/mL.
Against this background the mixture calling sensitivity of theSanger based PR RT genotypic assay, which drives the virco®TYPEHIV-1 virtual phenotype was assessed and the Sanger populationsequence output and mixtures with the HIV-1 genome distributionobtained by 454 sequencing were compared.
Twenty clinical isolates were selected based on their viralload and presence of mixtures in previously determined Sangersequencing rounds (Fig. 1). Starting from 256 �L plasma, RNA wasextracted on silica membranes using an MDX extraction platformfrom Qiagen. All samples were reversely transcribed and amplifiedin a one step RT-PCR using primers 3′RT (CAT TGC TCT CCA ATT ACTGTG ATA TTT CTC ATG) and 5′OUT (GCC CCT AGG AAA AAG GGCTGT TGG), followed by a nested PCR, using 3′IN (CAT CTA CAT AGAAAG TTT CTG CTC C) and 5′IN (CTA GGA AAA AGG GCT GTT GGA AATG). This amplification procedure yielded 300 �L of GPRT ampliconfor each clinical isolate. A total of 100 �L amplicon was purified,using the Qiaquick 96 PCR purification kit from Qiagen, and pre-pared for Sanger sequencing, with four forward primers (GAG AGCTTC AGG TTT GGG G; AAT TGG GCC TGA AAA TCC; CCT CCA TTC CTTTGG ATG GG; CAG ACC AGA GCC AAC AGC CCC) and four reverseprimers (CTC CCA CTC AGG AAT CC; GTA CTG TCC ATT TAT CAG G;CTT CCC AGA AGT CTT GAG TTC; CTA ACT GGT ACC ATA ATT TCACTA AGG GAG G). All 20 sequencing PCR products were purifiedusing the DyeEx purification kit from Qiagen. The dye-labelled DNAfragments were ran on an ABI 3730XL capillary gel electrophore-sis system from Applied Biosystems. A mixture was called in theSanger sequence when it covered at least 25% of the surface area ofthe major peak in the DNA chromatogram. The remaining 200 �L ofthe 20 GPRT amplicons was nebulized, for shotgun 454 sequencing(i.e. standard platform), according to the manufacturer’s ShotgunDNA Library Preparation Method Manual (GS-FLX, Roche AppliedScience). During the nebulization process each GPRT amplicon issheared into fragments ranging from 400 to 800 base pairs, result-ing in twenty libraries of smaller-sized DNA fragments. Fragmentswith frayed ends were made blunt by T4 DNA polymerase and T4polynucleotide kinase. Primer sequences (Adaptors “A” and “B”, ofwhich “B” also contains a Biotin tag) were ligated subsequently tothe ends of each polished fragment, providing the priming regionsto support both amplification and nucleotide sequencing. Adap-tors also included sequence barcodes (MID’s) to allow for samplemultiplexing in sequencing lanes on the Roche GS FLX instrument.Ligation mixtures were immobilized onto magnetic streptavidin-coated beads via the biotin moiety of Adaptor B, generating a librarywith single stranded template DNA (sstDNA), flanked by one Adap-tor A at the 5′-end and one Adaptor B at the 3′-end only. Following afill-in reaction, using a strand-displacing DNA polymerase, the non-biotinylated strand of each double stranded fragment was meltedoff to isolate the sstDNA. Quality assessment was performed withan Agilent 2100 BioAnalyzer. The sstDNA libraries were quantifiedusing the RiboGreen method (Invitrogen) and two equimolar poolswere created, each containing 10 libraries. 454 Shotgun sequenc-ing was carried out with the 454 Life Sciences platform (GS-FLX,Roche Applied Science). The shotgun approach was chosen instead
of the amplicon 454 method, because of the fragment size (i.e.inability to generate a full bi-directional sequence) and the factthat the same amplicon had to be used in both sequence methodsto allow for a correct comparison. Possible differences between the
H. De Wolf et al. / Journal of Virological Methods 175 (2011) 129– 132 131
106
Viral load4244464850
454 at 25%
Sanger
A
104
105
of m
ixtu
res
24262830323436384042
Viral Load
102
103
Num
ber
68
1012141618202224
101
Clinical isolate
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
0246
10650B
105
10
Viral load
32343638404244464850
454 at 20%
Sanger
Viral Load
103
104
Num
ber
of m
ixtu
res
14161820222426283032
101
102
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
02468
101214
Clinical isolate
F late bv
sActc(vsecr
icles
igst
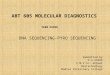
ig. 1. Viral load distribution and number of genetic mixtures scored per clinical isoersus the corresponding number of mixtures called by Sanger sequencing (�).
hotgun and amplicon 454 method are not known for this assay. custom plugin for CLC Genomics Workbench was used for cal-ulating variant frequencies at each nucleotide position relative tohe reference sequence. Inhouse developed algorithms for nonspe-ific primer binding and secondary structure removal were appliedVandenbroucke et al., submitted for publication). Finally, sequenceariants obtained by 454 at frequencies below 0.5% were not con-idered for this analysis, as they may result from 454 sequencingrror (Vandenbroucke et al., submitted for publication). The medianoverage in the twenty clinical isolates ranged in from 297.5 to 1474eads.
Possible correlation between the number of mixtures detectedn Sanger and 454 sequencing was investigated by the REG pro-edure in SAS/STAT® (SAS Institute Inc., SAS 9.1.3), using log viraload as a co-variate in the model. The latter procedure fits the lin-ar regression model by least squares (SAS Institute Inc., 2008). Aignificance level of 5% was used throughout.
The viral load and number of mixtures, detected by 454 sequenc-
ng to be present at 25% in the viral population, are representedraphically for each clinical isolate in Fig. 1a. At a 25% cut-off, 454equencing generated a total of 275 mixtures, ranging from 1 upo 33 mixtures per clinical isolate (Fig. 1a). Viral loads ranged fromy 454 pyrosequencing and present at 25% (A) or 20% (B) in the viral population (�)
470 to 629,000 copies/mL and showed no relation to the numberof mixtures that were scored (R2 = 0.01; p = 0.618). Analysis of theDNA chromatograms for the same PR–RT amplicons returned 268mixtures (Fig. 1a). Six from the seven mixtures that Sanger failedto detect were, nevertheless, present in the DNA chromatogrambut at surface areas below 25% of the major peak. As such theywere not considered automatically by the base calling software. Theonly mixture that could not be detected in the DNA chromatogram,belonged to clinical isolate 2 and had a viral load of 804 copies/mL.Hence, under the current high throughput conditions, the Sangermethod was able to automatically call 97.5% of the mixtures thatwere present at frequencies between 25 and 75% in the viral popu-lation, identified as such by the 454 method. The 2.5% of mixturesthat were not called automatically by Sanger sequencing at 25% ofthe major peak surface area, were distributed evenly among thedifferent viral load clinical isolates (Fig. 1a).
Although the Sanger method is not quantitative, a distinctionmust still be made between the mixture surface area in the DNA
chromatogram and the number of quasispecies that could actuallybe present in the mutant spectrum. Indeed, a mixture that is scoredat “25% of the major peak surface area” is not present at 25% in theviral population, but rather at 20%, since the signal of the major
132 H. De Wolf et al. / Journal of Virological Methods 175 (2011) 129– 132
Table 1Results of the regression analysis between the number of mixtures scored by Sanger sequencing and the total number of mixtures scored by 454 sequencing, present at 20%in the viral population, using log viral load as a co-variate. .
Source DF SS MS F ratio p value Parameter Estimate p value
Model 2 2923.6 1461.8 103.1 <0.0001 Intercept −2.758 0.4868Error 17 240.9 14.2 454 mixtures 0.997 <0.0001
Total 19 3164.6
DF, degrees of freedom; SS, sum of squares; MS, mean square.
60
S 2 758 0 997 454 * 1 123 L VL
40
45
50
55Sange rmixtures = -2.758 + 0.997 454mixtures* + 1.123 Log VL
R2 = 0.92
Root MSE = 3.76
* p<0.05
20
25
30
35
Tota
l num
ber
of m
ixtu
res s
core
d in S
anger
5
10
15
20
Sange r mixtures = 454mixtures
Total number of mixtures scored in 454 at 20%
6055504540353025201510500
Fig. 2. Number of mixtures scored in Sanger sequencing versus the total number ofmixtures scored in 454 sequencing, present at 20% in the viral population. Regressione(
atmpmitsrcqs
npbtlipSdb
v92aTs
quation estimated via the REG procedure in SAS, using log viral load as a co-variatesee Table 1).
nd minor peaks add up to 100%. Hence, when the mixture detec-ion threshold of the base calling software is set at 25%, Sanger
ay start to detect quasispecies that are present at 20% in the viralopulation. At a mixture detection limit of 20%, 454 returned 342ixtures (Fig. 1b). From those 342 mixtures, all but 16 were scored
n the DNA chromatograms as well. Fifteen out of these 16 mix-ures were nevertheless present in the DNA chromatograms but aturface areas below 25% of the major peak. Hence, under the cur-ent high throughput conditions, the Sanger method was able toall automatically 95.3% of the mixtures that were present at fre-uencies between 20 and 80% in the viral population, identified asuch by the 454 method.
Finally, there is a highly significant correlation between the totalumber of mixtures scored by Sanger and the number of mixtures,resent between 20 and 80% in the viral population, as detectedy 454 (Fig. 2; R2 = 0.92; p < 0.0001). The parameter estimates forhe regression model are presented in Table 1 and indicate that theog viral load does not contribute significantly to the mixture call-ng relationship between both sequencing methodologies (Table 1;arameter estimate: 1.1; p = 0.2461). In addition, it is noted thatanger sequencing called 55 additional mixtures that were notetected by 454 sequencing at the 20% mixture scoring threshold,ut were all 55 detected at lower 454 mixture frequencies.
In conclusion, the Sanger based genotype assay which feeds theirco®TYPE HIV-1 virtual phenotype is able to detect automatically7.5% and 95.3% of the mixtures that are respectively present at
5% and 20% in the viral population, and might identify occasion-lly additional mutations that are present at a lower frequency.hese findings were not influenced by the viral load of the examinedamples.Log viral load 1.123 0.2461
In addition, it is also important to acknowledge that low abun-dance drug resistant HIV variants as low as 1% of the circulating viralquasispecies can be detected in both treatment naïve and experi-enced patients that can impact clinical response (Lataillade et al.,2010). However, to understand the impact and clinical relevanceof such low abundance variance detected by ultra-deep sequenc-ing methodologies on clinical outcome, additional studies would berequired to determine how viral factors of mutational load, muta-tion linkage and specific mutational patterns interact and impacttreatment responses in the clinic.
References
Andrade, L., Manolakos, E.S., 2004. Robust normalization of DNA chromatograms byregression for improved base-calling. J. Franklin Inst. 341, 3–22.
Broder, S., 2010. The development of antiretroviral therapy and its impact on theHIV-1/AIDS pandemic. Antivir. Res. 85, 1–18.
Dolnik, V., 1999. DNA sequencing by capillary electrophoresis (review). J. Biochem.Biophys. Methods 41, 103–119.
Garcia-Arriaza, J., Domingo, E., Briones, C., 2007. Characterization of minority sub-populations in the mutant spectrum of HIV-1 quasispecies by successive specificamplifications. Virus Res. 129, 23–134.
Hirsch, M.S., Günthard, H.F., Schapiro, J.M., Brun-Vézinet, F., Clotet, B., Hammer, S.M.,Johnson, V.A., Kuritzkes, D.R., Mellors, J.W., Pillay, D., Yeni, P.G., Jacobsen, D.M.,Richman, D.D., 2008. Antiretroviral drug resistance testing in adult HIV-1 infec-tion: 2008 recommendations of an International AIDS Society-USA panel. Clin.Infect. Dis. 47, 266–285.
Lataillade, M., Chiarella, J., Yang, R., Schnittman, S., Wirtz, V., Uy, J., Seekins, D.,Krystal, M., Mancini, M., McGrath, D., Simen, B., Egholm, M., Kozal, M., 2010.Prevalence and clinical significance of HIV drug resistance mutations by ultradeep sequencing in antiretroviral-naïve subjects in the CASTLE study. PLoS ONE5, 1–7.
Margulies, M.M., Egholm, W.E., Altman, S., Attiya, J.S., Bader, L.A., Bemben, J., Berka,M.S., Braverman, M.S., 2005. Genome sequencing in microfabricated high-density picolitre reactors. Nature 437, 76–380.
Metzker, M.L., 2010. Sequencing technologies – the next generation. Nat. Rev. Genet.11, 31–46.
Morozova, O., Marra, M.A., 2008. Applications of next-generation sequencing tech-nologies in functional genomics. Genomics 92, 255–264.
Paredes, R., Clotets, B., 2010. Clinical management of HIV-1 resistance. Antivir. Res.85, 245–265.
Roche Diagnostics GmbH, December 2007. GS FLX Shotgun DNA Library PreparationMethod Manual. Roche Applied Science, 68298 Mannheim, Germany.
SAS/STAT® , SAS Institute Inc., 2000–2009. SAS 9.1.3 Help and Documentation. SASInstitute Inc., Cary, NC.
Strausberg, R.L., Levy, S., Rogers, Y.-H., 2008. Emerging DNA sequencing technologiesfor human genomic medicine. Drug Discov. Today 13, 569–577.
U.S. Department of Health and Human Services, Food and Drug Administration, Cen-ter for Biologics Evaluation and Research, 2007. Guidance for Industry. Class IISpecial Controls Guidance Document: In Vitro HIV Drug Resistance GenotypeAssay.
Vandenbroucke, I., Van Marck, H., Verhasselt, P., Thys, K., Mostmans, W., Dumont,S., Van Eygen, V., Coen, K., Tuefferd, M., Aerssens, J. Minor variant detection inamplicons using 454 massive parallel pyrosequencing: experiences and consid-erations for successful applications BioTechniques, submitted for publication.
Van Houte, M., Picchio, G., Van Der Borght, K., Pattery, T., Lecocq, P., Bacheler, L.,2009. A comparison of HIV-1 drug susceptibility as provided by conventionalphenotyping and by a phenotype prediction tool based on viral genotype. J.Med. Virol. 81, 1702–1709.
Vermeiren, H., Van Craenenbroeck, E., Alen, P., Bacheler, L., Picchio, G., Lecocq, P.,2007. Prediction of HIV-1 drug susceptibility phenotype from the viral genotype
using linear regression modeling. J. Virol. Methods 145, 47–55.Winters, B., Van Craenenbroeck, E., Van Der Borght, K., Lecocq, P., Villacian, J.,Bacheler, L., 2009. Clinical cut-offs for HIV-1 phenotypic resistance estimates:update based on recent pivotal clinical trial data and a revised approach to viralmixtures. J. Virol. Methods 162, 101–108.