Embed Size (px)
Citation preview

1
Tracheostomy, Oxygen and Ventilators for Children
Dorothy Page, FNP Department of Pedi Pulmonary
Umass Memorial
History of Tracheostomy
l 1546-1st tracheostomy done for upper airway obstruction on adult
l 1620-1st pediatric trach; child with coins lodged in thraot
l 1799- George Washington died of upper airway obstruction allegedly because no one wanted to operate on him
l 1808- first tracheostomy on child with Diphtheria

2
l 1880- first pediatric tracheostomy tube l 1950-used for acute airway compromise: ie
diphtheria, croup, epiglottitis/ trach removed when child well
l Vaccines and endotracheal intubation eliminated this need
l 1965- NICU- trachs as result of long term ventilation
National Incidence
l Relatively infrequent/ about 5000 in US
l 0.07% of all pedi discharges l 60% male l Rates highest in youngest and oldest
pedi age group

3
Reasons for tracheostomy
l Infant: congenital, pulmonary/prolonged intubation, prematurity
l 1-9 year old: pulmonary, injury, chronic upper respiratory, large foreign body
l 15-19 year old: injury 77%, pulmonary, neurological
Early Trach Complications
l Local infection l Accidental decannulation l Pneumothorax l Acute hemorrhage l Death

4
Late Trach Complications
l Decannulation l Obstruction l Subglottic stenosis l Tracheal fistula/Tracheitis l Granulation l Death
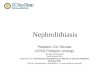
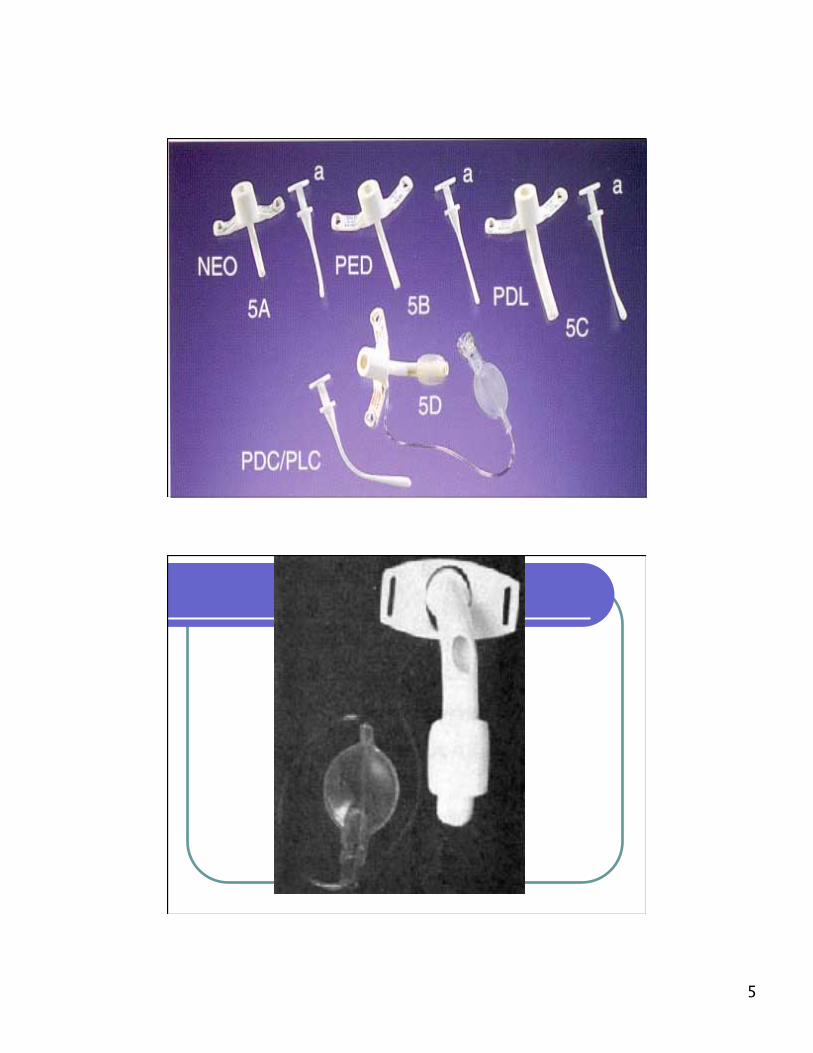
Types of trach tubes
l Uncuffed l Cuffed l Fenestrated l T-tube l Always check size, length and
manufacturer; “new” trach sizing; starts at 3.0 neo; custom trachs
5

6

7

8
Sizing of tube
l Large enough to allow adequate ventilation and small enough to allow laryngeal airflow which will maintain speech
l Small enough to minimize pressure on trachea and stoma
l Neonatal: less than 7kg/ Pedi over 7 kg l Custom tubes only from company
Sizing
l Tube to extend 2cm below stoma l No closer than 1-2 cm to carina l Shorter better l Better to breathe through and around trach l All should have universal 15mm adapter for
ambu/ metal needs to be fitted l Poorly fitting tubes hurt….

9
Material of tube
l Most pedi are silicone or plastic l Single cannula/ the double narrows ID
and increases airway pressure l Metal tubes in special circumstances l Bivona: has some metal particles/ need
to change prior to MRI
Cuffed vs Uncuffed
l Uncuffed preferable in children l Cuffed if child on ventilator l Monitor cuff pressure every shift: balloon
inflated/deflated l Use air except Bivona TTS(tight to shaft) l Mark amount of air/amount in insert l Don’t overfill/ deflate once a shift for 15”
if tolerated

10
Fenestrated?
l No consensus l ?better translaryngeal airflow l ?aid in secretion removal l ?promote granulation tissue l Inner cannula needs to be removed for
speech but replaced to ventilate with ambu
Trach tube changes
l Best if planned for l Good to have second person l Lubricant should be used sparingly l Never force trach in or out…if you
cannot remove trach, child needs to get medical attention

11

12
Frequency of tube changes
No consensus -most common weekly -more changes may decrease granulation
and keep up skills -cuffed trach repeated change stretches
stoma
Duration of tube use
l Inspect before use/ do not use if cracks or tears
l Discard if silastic is stiff l Manufacturers state life maximum life
of tube is 29 days(at least change every 29 days)
l Tube cannot be reused or cleaned due to biofilm development

13
Cleaning Trach Tubes
l Don’t reuse l Problems with bacterial biofilm and
resistance to cleaning l Peroxide and detergents do not clean l Boiling bends tube l Need new tube with each change
Tracheostomy ties
l Metal beads l Cotton twill: cheap, easily soiled, need
scissors l Velcro: more expensive, child can pull
apart l Shoelaces: Cheap, check dyes l Tie snug: one finger

14

15
Stoma care
l Inspect l Keep clean and dry l Soap and water l Remove secretions with H2O2 l Avoid: pressure necrosis, routine
ointment or creams l Dressings trap moisture

16
Suctioning
l Frequency: based on clinical assessment including lung sounds, oxygen need, increase in vent pressure alarms
l Encourage patient to cough first l Clean technique, use of gloves

17
l Suction through clean water/ saline after use
l Wipe catheter with alcohol after use l Air dry and place in clean bag unless
child has secretions that prohibit reuse/ only reuse a couple of times/ if cloudy do not use
Technique
l Pressure in infants 60-80 mm Hg l Premeasure cath with trach tube l Only to end of trach tube l Twirl catheter with intermittent
suction on insertion and removal l Less than 5 seconds l Cath size is largest that fits

18
Preoxygenation/ Post oxygenation
Use of ambu bag prior to suctioning if… -child with decreased respiratory reserve -oxygen drops during suctioning -cardiac distress during suctioning -on supplemental oxygen Do Not bag if secretions are visible
Use of saline in trach
l Consensus is that routine use of normal saline is not recommended

19
Humidification
l Inspired air through trach may have humidity deficit
l Consequence of dryness may be deterioration of pulmonary function and increased risk of infection
l Air going into trach needs to be heated and humidified
Types of humidification
l Bubble jet: used in ICU setting/ costly and challenging to manage
l Jet nebulizer: small spray H2O droplets may be heated or at room temperature
l HME: artificial nose/ attaches to trach/ helps child to be more portable

20
Speech Development
l All children with trach need speech therapy l Baby sign language for early communication l Assess child’s hearing l Use of speaker valve ie Passey-Muir as early
as tolerated: thin secretions, person in attendance, deflate cuff

21

22
Decannulation
l Decannulate when need for trach is gone and child is able to maintain airway
l Process: smaller trach, cap tube or pull trach?
l Once trach out, child has sensation of air in mouth and can taste food…child may object
Feeding issues
l Oral stimulation l Oral feeding; different textures and
temperatures l Prepares for speech l May like very, very spicy foods

23
Safety/ Child Issues
l Need for play l Protect trach from small objects l Child who pulls out trach l Monitors
Post trach
l May need laryngeal reconstruction l Better results if done within 25
months of age l 32% fail first attempt to decannulate
24
At school…need to know…
l Why was trach placed…how critical? l Size? Cuffed? l Know how to change trach l Child should travel with all supplies and
trach one size smaller l Travel: HCP card, second person,
monitor, seltbelt equipment, cell phone l Emergency plan…who responds?
School
l Needs one to one nurse door to door l Needs specific orders on suctioning,
oxygen l Needs HCP and emergency plan l Tutoring plan each year; starts at day
one if child able l Must attend field trips; parent does
not have to go….a nurse must go

25
School nurse
l Needs to be comfortable with stepping in for 1:1 nurse in emergency
l Emergency plan includes: what to do if SN needs to step in/what to do in lock down or evacuation/ what is 911 emergency for child ie if trach emergently changed…
l Child travels with “go-bag” of supplies
School nurse
l Plan for 1:1 or SN to check “go-bag” each AM
l Plug in all equipment whenever possible l Have a plan to check on school
equipment regularly and document

26
Oxygen: Reasons for ….
l Chronic respiratory failure l Cardiac abnormalities l Hypoxia due to neurological issues l Aspiration
Oxygen in school
l Why is oxygen needed? How critical? l Need to know usual flow rate as well
as sick and emergency plan for HCP l Is flow based on pulse oximetry, vital
signs, observation, child request? l Given during periods of increased need
such as mild illness or exercise?

27
Oxygen devices
l Liquid: filled from mother tank at home: cold to touch: needs to stay upright
l Gas: green cylinders: size based on flow rate
l Concentrators: not advisable in children due to variable output of O2
Oxygen devices
l Pulse oximeter in nurse’s office l Always have backup tank in nurse
office: check daily that tank full l Notify fire department if O2 stored
in school

28
Oxygen
l Health care plan and emergency plan l Plan for lock down and stay in place l Check child’s supplies daily l Safe storage and transport l Secure tanks in bus
Ventilators
l Child who cannot breathe without artificial support: ie chronic hypoventilation, CCHS, chronic aspiration, cardiac failure, chronic respiratory failure

29
Types
l Pressure based: used in children: portable: more stable: includes CPAP machines
l Volume based hospital only l Children with vents. Usually have trach
and need O2
In school…
l HCP and Emergency plan spell out all possible scenarios including transportation, field trips, rapid evacuation
l SN needs to spend time on a regular basis with child in case SN needs to “step in”
l 1:1 nurse

30
In school…..
l Child carries go-bag of supplies which is checked daily
l Keep equipment plugged: know how long batteries last: they need to be with child daily
l If batteries do not last 8 hours, consider getting backup batteries from home care company
If you have child with trach, O2 or vent in school…..
l Make sure MD orders are clear and outline plans
l HCP and Emergency plan l Know the child l Check equipment and plug in batteries l Call us!

31
Resources
l Supporting Students With Sp. Health Care Needs at School: Porter, S: Respiratory section (great!)
l Pediatric Nursing Skills/ Prentice Hall l Aaron’s Tracheostomy Book l NASN journal: Oct. 2013: Emer.
Preparedness at School….