Embed Size (px)
Citation preview

Received: 18 February 2002Revised: 22 May 2002Accepted: 5 June 2002Published online: 24 August 2002© Springer-Verlag 2002
Abstract Purpose: To correlate thecross-sectional images of cornealdiseases obtained by optical coher-ence tomography (OCT) with lightmicroscopy (LM) to determine thecorneal components represented inOCT images. Methods: In a prospec-tive comparative tissue study clin-icopathological correlations of sixpatients with pseudophakic bullouskeratopathy (n=3), advanced kerato-conus (n=1), persistent epithelial de-fect with corneal thinning (n=1), andretrocorneal membrane (n=1) wereincluded. Immediately before aplanned penetrating keratoplasty(PKP) noncontact slitlamp-adaptedOCT of the cornea was performed.After PKP and following standardhistological processing the speci-mens were examined under LM tocompare qualitatively the morpholo-gy, and quantitatively the morphom-etry at selected corneal locations.Results: The cross-sectional optical-reflectivity profiles enabled the re-producible morphological evaluationof the corneal structures and changes.Layers of relative high reflectivitycorresponded to the anterior cornealsurface and internal stromal layers.
In contrast, the deeper corneal epi-thelial layer demonstrated relativelow reflectivity by OCT. An increasein light reflectivity corresponded tocorneal scarring, irregularities of thecorneal lamellae, and deposition ofbasal membrane material. Low sig-nal intensity was particularly due tofluid accumulations and shadowing.The most prominent changes werecaused by corneal scars or edema-tous tissue. The morphometric analy-sis with OCT revealed, in this study,thickness measurements rangingfrom 31 to 902 µm. Although themean OCT thickness values were upto 9% (P=0.014) higher than thosederived from LM, there was a signif-icant positive correlation (r=0.94;P<0.001) between corneal OCT andthe light-microscopic measurements.Conclusion: Noncontact slitlamp-adapted corneal OCT revealed agood correlation with histologicalsections. The differences noted werepartly related to shrinking processesduring preparation. Thus, with cer-tain limitations, OCT allows a non-invasive optical biopsy of pathologi-cal structures in corneal diseases.
Graefe’s Arch Clin Exp Ophthalmol(2002) 240:727–734
DOI 10.1007/s00417-002-0518-3
C L I N I C A L I N V E S T I G AT I O N
Christopher WirbelauerJörg WinklerGerd O. BastianHeike HäberleDuy Thoai Pham
Histopathological correlation of corneal diseaseswith optical coherence tomography
Introduction
Slitlamp biomicroscopy is the standard technique to ex-amine clinically the anatomical structures of the eye. Op-tical coherence tomography (OCT) allows precise cross-sectional imaging enabling noncontact representation of
the anterior eye segment and cornea [13, 14, 17, 28, 29].OCT differentiates between light backscattered from dif-ferent depths in the cornea, also permitting the character-ization of internal corneal structures, and allows to dis-tinguish the layered structure of the cornea for anteriorsegment morphometry. In recent clinical studies compar-
Presented in part at the 99th Annual Meet-ing of the Deutsche OphthalmologischeGesellschaft in Berlin
The authors have no commercial, propri-etary or financial interest in any research ordevices described in the presented study
C. Wirbelauer (✉ ) · H. Häberle · D.T. PhamKlinik für Augenheilkunde, Vivantes Klinikum Neukölln, Rudower Strasse 48, 12351 Berlin, Germanye-mail: [email protected].: +49-30-60043131Fax: +49-30-60043546
J. Winkler · G.O. BastianAugenklinik der Medizinischen Universitätzu Lübeck, Lübeck, Germany

ison of the OCT images with slitlamp biomicroscopy ob-servations [10, 29] confirmed that corneal OCT can re-solve the epithelium or provide measurements of the in-ternal corneal layers [30, 32]. The main advantage ofOCT is the objective documentation of corneal disorders,and OCT imaging could improve the diagnosis and clini-cal management of corneal diseases. Although compari-sons for posterior eye segment morphology with knownretinal anatomy and OCT images were performed clini-cally [9, 24], only in-vitro [13] or experimental animalstudies compared histological specimens [4, 15, 19, 27].This clinical study sought to investigate the histopatho-logical correlation of OCT in corneal diseases to allowimproved identification of anatomic features.
Patients and methods
Patients
Prospectively, six patients undergoing planned penetrating kerato-plasty (PKP) for corneal diseases were included. The mean agewas 70±10 (mean ± SD) years (range 53 to 82 years). A completeophthalmologic examination was performed on each patient. Thepatient’s primary corneal diagnosis on slitlamp examination werepseudophakic bullous keratopathy (three eyes), advanced kerato-conus (one eye), corneal thinning with epithelial hyperplasia fol-lowing persistent epithelial defect after extensive alkali injury(one eye), and retrocorneal membrane with endothelial decompen-sation (one eye). Informed consent was obtained from all patients,and the study had approval by the ethics committee of our institu-tion.
Corneal optical coherence tomography
The central cornea was examined with a clinical slitlamp-adaptedOCT system (Medical Laser Center and 4Optics AG, Lübeck,Germany). The principle of OCT is based on low-coherence interferometry having as light source a superluminescent diode(SLD-361, Superlum, Moscow, Russia) operating at a wavelengthof 830 nm with a bandwidth of 20 nm and an intensity of the inci-
dent light of less than 200 µW. The sample arm of the interferome-ter and the scanning module were integrated in the projected slit ofa standard clinical slitlamp (BQ 900, Haag-Streit, Bern, Switzer-land) as described previously [28, 29, 31]. In this study the OCTinfrared light was adjusted on the central cornea and pathologicalstructures. All measurements were performed perpendicularly tothe cornea to avoid image distortions. Calibration of the OCTsystem was repeated at regular intervals throughout the study [31].
Slitlamp-adapted OCT enabled us to visualize corneal changesin vivo using the axial interference profile of the corneal reflec-tions [28, 31]. All images presented are in logarithmic gray-scale.The stored data from the highest-quality corneal OCT image wasthen further processed for quantitative assessment of cornealstructures, i.e., total corneal thickness, epithelial and stromalthickness, and pathological changes (Wizard 8.8, 4Optics AG).The optical-signals profile was analyzed and the peak reflectionswere used for comparison with the histological layers. The reflect-ed optical-delay signals were then transformed into geometric val-ues with the instrument-specific calibration factor and the grouprefractive index of the cornea (n=1.3853) [11, 28, 31].
Light microscopy
Immediately after corneal transplantation the corneas were fixedovernight in Bouin’s solution containing 9% formaldehyde. Thespecimens were dehydrated in a series of graded ethanol(70%–100%) and embedded in paraffin wax under standard histo-logical procedures. Paraffin from the sections (4–5 µm) was dis-solved in xylene, and the sections were immersed in acetone thenwashed with PBS at pH 7.6. For routine histological examinationsthe sections were stained with hematoxylin-eosin and evaluatedwith a light microscope (Axioskop, Zeiss, Oberkochen, Germany).Photographs of representative areas at low magnification weretaken with Kodak TRI-X Pan films (Axiophot, Zeiss).
Alignment of the OCT and light-micrograph cross-sectionswas performed by an overlay technique corresponding to promi-nent anatomic features. The extent of morphological changes wasthen quantitatively assessed with a micrometer gauge for the cor-neal, epithelial, and stromal thicknesses, and further pathological-ly altered structures. The diameter of all alteration sites was mea-sured and average values were determined for each eye. For thequantitative analysis of data obtained by light microscopy (LM)the magnification value and a tissue shrinkage of 10% were con-sidered [16, 23]. At least two matched locations were evaluated ineach corneal section resulting in 60 morphometrical values forcomparison with OCT thickness signals.
728
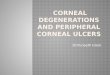
Fig. 1a, b Patient with pseudo-phakic bullous keratopathywith diffuse stromal edema. a Gray-scale slitlamp-adaptedOCT reveals a thickened cor-nea with increased stromal lightreflectivity and mild Descemet’sfolds. Note posterior increaseof central signal intensity (asterisk). b LM (hematoxylin-eosin, magnification × 85)shows diffuse stromal edemawith irregular swelling of thecorneal lamellae. E epithelium,S stroma

Statistical analysis
All results were presented as mean ± SD, and range. The statisti-cal comparison of the individual thickness parameters betweenLM with the optical values determined with the corneal OCTmethod was performed with the mean comparison for dependentvariables (Student’s paired t-test), linear regression analysis, thecomparison of the regression line with the line of equality, andPearson’s correlation coefficient (r). The regression equationy=a+b×x related the parameters, if the intercept, a, was not statis-tically different from 0, and the slope, b, was statistically differ-ent from 0. Then y corresponded to x, and the parameters werenot statistically different. A P value below 0.01 was consideredsignificant.
Results
Morphological changes
The cross-sectional optical-reflectivity profiles enableda descriptive morphological evaluation of the cornealstructures and the wide variation of changes present inthe patients studied. In Figs. 1, 2, 3, and 4, the anatomi-cal layers of the cornea can be delineated, and OCTscans revealed structural landmarks, allowing assign-ment of corneal structures with changes in relative re-flectivity, evident at each interface. Layers of relativehigh reflectivity corresponded to the anterior surface ofthe cornea and internal stromal layers (Fig. 1a). In con-trast, the deeper corneal epithelial layers demonstrated arelatively low signal intensity by OCT (Fig. 1a). Thestroma appeared as a large band of variable OCT signalwith a posterior increase in central signal intensity(Fig. 1a). These characteristic features and histologicallandmarks of the cornea revealed to be consistent in theserial sections (Figs. 2, 3, and 4). Additionally, patho-logical aspects were imaged. These included an irregu-lar epithelial layer (Figs. 2 and 3), marked corneal scar-ring with degenerative changes and thinning (Figs. 2and 3), irregular and edematous stroma with Descemet’sfolds (Figs. 1 and 4), and a thickened, reduplicatedretrocorneal membrane (Fig. 4). A variable increase inlight reflectivity in the OCT scans corresponded to cor-neal scarring (Figs. 2b and 3b), irregularities of the cor-neal lamellae due to corneal edema or fibrosis (Fig. 1a,2b, and 3b), and deposition of hyalinized or basal mem-brane material (Fig. 4a). A decrease in signal intensitywas particularly due to fluid accumulations, leading to adecrease in microscopic scatterers in the tissue, cysticlesions, and shadowing (Figs. 2, 3, and 4). The mostprominent changes with the largest backscattering signalwere caused by scarred or edematous tissue. Thus, cor-neal OCT enabled, in these selected cases, an optical biopsy, with a direct histopathological correlation of the laminated corneal structure, and optical differentia-tion of pathological changes with high scatter coeffi-cients.
Morphometrical analysis
The results of the quantitative corneal OCT thicknessvalues compared with LM thickness values are summa-rized in Table 1. The mean corneal OCT thickness was
729
Fig. 2a–c Patient with advanced keratoconus and healed hydropswith significant corneal thinning and structural changes with api-cal stromal scarring. a Clinical photograph (the line represents theregion of the OCT scan). b Gray-scale slitlamp-adapted OCT de-picts an irregular and markedly thinned epithelium and stromawith variable and focal increase in light reflectivity. c LM (hema-toxylin-eosin, magnification × 37.5) demonstrates progressed epi-thelial and stromal thinning with focal degenerative changes andhyalinization in the apical stromal region

371±260 µm (31–902 µm) and the corrected LM thick-ness 340±212 µm (12–766 µm). The mean of the differ-ences was 31 µm or approximately 9%, with high indi-vidual variations (P=0.014).
In Fig. 5 the combined corneal OCT thickness valuesare compared with the measurements with LM. Thegraph reveals that there was a positive linear relationwith a regression line of y=1.15x–21. In this study the
730
Fig. 3a–c Patient who suffered severe alkali injury and persistentepithelial defect, in whom extensive noninfectious stromal meltingand epithelial hyperplasia developed. a Clinical photograph (theline represents the region of the OCT scan). b Gray-scale slitlamp-adapted OCT displays a hyporeflective, irregularly thickened epi-thelial layer and marked stromal thinning, with variably increasedreflectivity in the central and anterior stroma. c LM (hematoxylin-eosin, magnification × 60) reveals a hyperplastic epithelium withsubepithelial hyalinization, irregularly scarred stromal lamellae,and marked corneal thinning
Fig. 4a, b Patient with retrocorneal membrane due to fibrousmetaplasia of the endothelial cells following chronic inflammationof the anterior eye segment and pseudophakic bullous keratopathy.a Gray-scale slitlamp-adapted OCT shows diffusely increasedstromal light reflectivity with a hyper-reflective retrocorneal mem-brane. b LM (hematoxylin-eosin, magnification × 62.5) depictsdiffuse stromal edema with a thickened and reduplicated Descem-et’s membrane containing basal membrane material
Fig. 5 Graphic representation of the quantitative morphometricvalues determined by LM and the corneal OCT method. The re-gression line, the line of equality, the linear regression equation(y), the correlation coefficient (r), the P value, and the number ofcases (n) are displayed

comparison of the regression line with the line of equali-ty revealed that the intercept was –21 µm (t=–0.96,P=0.34), and not statistically different from 0. The slopeof the regression equation was 1.15, which was signifi-cantly different from 0 (t=20.97, P<0.001), and suggest-ed a positive correlation between the histological and op-tical corneal structures. The correlation coefficient of0.94 (P<0.001) confirmed a statistically significant lin-ear relationship between both parameters. However, adrift of the regression line toward higher optical valuescompared to the line of equality could be noted. Exceptfor the OCT epithelial thickness values, which revealedonly a weak correlation with LM values (r=0.47,P=0.037), all measured substructures had highly signifi-cant (P<0.001) correlation coefficients (Table 1).
Discussion
OCT is a high-resolution and noncontact technique thatcan create precise cross-sectional images of the anteriorand posterior eye segment. Previous morphological studies have assumed a correlation between the color-coded bands and the cell layers of the cornea and retinaseen on histology, since the spatial separation of the cod-ed bands in OCT images is similar to that of a histologi-cal section [9, 10, 14, 17, 24, 29]. However, the clinicalcorrelation of OCT with slitlamp biomicroscopy, fundusphotography, or fluorescein angiography is only of limit-ed value for morphological studies, since imaging tissueswith different reflection patterns or scattering propertieswill not necessarily reflect different tissue morphologies.
In this descriptive study, conventional histopathologywas used to improve the understanding of qualitative andquantitative OCT findings in disease processes of thecornea. OCT revealed to be effective in delineating thecross-sectional location of visible markers and relativereflectivity of elements of the corneal anatomy andpathological conditions. Currently, only in-vitro [13] orexperimental studies of normal animal retina morpholo-gy have been performed to assess the issue of the mecha-nisms of image contrast between different tissues [4, 15,
19, 27]. These studies correlated the optical propertiesand light distributions of OCT with histology, to assessthe exact relationship between reflectivity and retinallayers. In our clinicopathological investigation cornealscans enabled the discrimination between tissue layers inareas, where anatomic features were well defined with apositive significant correlation between OCT and LM.However, there was no exact agreement in the derivedthickness values due to high individual variability andpossible artifactual changes in tissue morphology alsoassociated with histological sample preparation. It is im-portant to note that OCT and LM are fundamentally dif-ferent techniques that generate images of microscopictissue elements. OCT utilizes propagated infrared lightwaves incident onto a scattering medium, such as un-stained corneal tissue, which are absorbed, transmitted,or scattered. The part of light that is scattered can bebent, refracted or reflected. Only the reflected part canbe processed by the OCT detection system and used forsignal analysis. Thus, OCT images are generated as a re-sult of the interaction between a partially coherent beamof optical radiation and the corneal tissue componentsalong the axis of the beam. In the composite, multi-lay-ered cornea as scattering medium, the most importantoptical properties for the propagation of light and signalgeneration from the time delay of light reflected back arechanges of structure, refractive index at the interfaces,and the scattering properties. These can lead to specularreflections and sharp signal peaks. In this study, imagingof corneal structures depended not only on the amount ofspatial variation and optical contrast in relative densityand reflectivity of adjacent corneal structures, but alsoon the resolving power of the instrument. Therefore,some limits in the resolution of this clinical OCT systemwere observed, when compared with the microscopicstudy of fixed, stained tissue. The axial resolution in cor-neal tissue of 11 µm OCT depended on the coherencelength and bandwidth of the light source, image process-ing, noise, and the influence of overlying tissues. Theclinical axial precision of this system was found to be5.8 µm and is similar to the axial digital sampling incre-ment of 5.6 µm [31]. The lateral resolution depended on
731
Table 1 Corneal OCT thickness values compared with LM thickness values of the studied tissue structures
Tissue OCT (µm) LM (µm) Da rb P nc
Mean ± SD Range Mean ± SD Range
Total cornea 531±185 245–745 488±118 312–766 0.137 0.81 <0.001 17Epithelium 48±14 31–68 51±22 12–92 0.514 0.47 0.037 15Stroma 527±164 221–713 455±133 238–733 0.014 0.82 <0.001 14Pathological structures 365±240 68–902 354±170 83–638 0.688 0.92 <0.001 14Total values 371±260 31–902 340±212 12–766 0.014 0.94 <0.001 60
a Paired-samples test of the differences between OCT and LMthickness values with a P value of <0.01 considered significant
b Pearson’s correlation coefficient with a P value of <0.01 consid-ered significantc Number of matched locations measured

the spot size of 10 µm and the lateral sampling rate. Al-though increasing the lateral sampling density for mor-phological analysis would improve the lateral resolution[8], the total image acquisition time during scanningwould also increase proportionally with possible eye mo-tion artifacts [29]. The presented OCT system at 830 nmhad a composite cross-sectional resolution in tissue of11 µm axially and 28 µm laterally, and thus, images inthis study were under-sampled to maintain an acceptableacquisition time and to provide a wide field of view.
The observed reflections in normal corneas corre-sponded to the anterior surface of the cornea, the epithe-lial–stroma interface, and the posterior corneal bound-aries. Although corneal OCT was sufficiently sensitiveto detect relatively small changes, the resolution of thisclinical OCT system was not sufficient to visualize theBowman or Descemet membranes, both of which are ap-proximately 10–15 µm thick. This confirms that to detecttwo structures as distinct entities in the signal transitionsthey must be separated by a distance greater than the fi-nite length of the light wave produced. The anterior sur-face of the cornea was the site of the greatest change inrefractive index between adjacent layers, and this alsoproduced the highest reflections. However, these specu-lar reflections can lead to loss of important signal fea-tures at higher saturation levels, and thus, mask reflec-tions from deeper cellular and connective tissue layers ofthe cornea. Although overall changes in the cornealthickness and marked pathological changes were easilydetermined by OCT, the precise location of intracornealtissue boundaries and fine adjacent substructures in cor-neal OCT images is more difficult to define [30, 32].This is also dependent on the relatively small and hetero-geneous intracorneal fluctuations in the layer-to-layer re-fractive index and scatter coefficients with possible com-plete, partial, or multiple backscatter of light. As recentlyproposed, a wavelength of 1,310 nm might provide ahigher contrast for imaging of these internal cornealstructures [12, 25], and further research on optical tissuemodels with single and multiple scattering, with orderedand randomly distributed scatterers could be helpful tounderstand the mechanisms of OCT image contrast.
In this and previous clinical studies [10, 29] the nor-mal corneal stroma revealed highly variable scatteringpatterns in OCT with a frequent progressive posterior in-crease of central reflectivity. Although corneal diseaseswith structural changes in collagen fibril size and spatialarrangement might lead to increased stromal light scat-tering, the anterior and posterior stroma differ in specificways [3]. In general, the posterior stroma is ultrastructur-ally more ordered, with wider and thicker corneal lamel-lae [18], more hydrated, more easily swollen [21], andhas a lower refractive index [22] as well as differentscattering properties [6] than the anterior stroma. Theseultrastructural and optical differences between the anteri-or and posterior stroma could lead to a change in the
central OCT signals in the posterior stroma (Fig. 1a).Since the anterior human stroma was predicted to scatterapproximately twice as much light independently of thewavelength as the posterior stroma, based on the fibrillarultrastructure and differential density of the collagen fi-bers [6], the observed posterior increase in central reflec-tivity is probably influenced in great part by the stromalwater content and its effects on the infrared light of OCT.
Corneal OCT enabled the quantitative analysis of the height of the reflectivity and the optical distance between reflectivity peaks. This allowed the objec-tive, non-invasive in-vivo documentation of pathologicalchanges with a close correlation with the clinical chang-es and LM. Although the mean OCT thickness valueswere 9% (P=0.014) higher than the values derived fromLM, there was a significant positive correlation (r=0.94;P<0.001) between corneal OCT and the LM measure-ments. In experimental animal studies the relationshipbetween OCT and LM measurements of total retinalthickness in retina specimens also had a strong linearcorrelation (r=0.98), but with high individual variationsfor internal structures of up to 30%, depending on polar-ization settings [4]. This further confirms the currentlimitations of conventional OCT compared with histolo-gy [5]. Although the OCT epithelial thickness valuescorresponded well with the LM values, only a weak cor-relation was found (Table 1). This could be related to thedecrease in discrimination for internal corneal structures,but is also influenced by the measurement range avail-able for statistical analysis [2]. Furthermore, the outerOCT signal is not specific for the epithelium, partly con-sisting of a surface-related signal [30, 32]. In the patientswith swollen corneas and compensatory Descemet’sfolds at the posterior side due to pseudophakic bullouskeratopathy examined in this study, great variations inthickness values could be another source of variability.However, the two highest OCT signals were confirmedto be the surface of the cornea and the internal limits tothe anterior chamber, allowing precise and accurate mea-surement of total corneal thickness with noncontact slit-lamp-adapted OCT [29, 31].
Light micrographs of fixed tissue, although the goldstandard in this comparison, are also limited. The corne-al tissues had to be surgically removed, rapidly fixed,and then dehydrated with minimal distortion. Each pro-cessing step added potential artifacts to the final imagingof corneal morphology. Thus, the marked individual di-mensional variations could be related to different shrink-ing properties of the tissues in the course of processing,with the greatest impact from gradient-ethanol dehydra-tion and paraffin infiltration [16]. In fact, conventionaltissue-processing procedures can lead to variable shrink-age or swelling of the cornea, and can produce consider-able alterations of the tissue dimensions. We used a cor-rection value of 10% for histological thickness measure-ments [6, 16, 23], but tissues with higher water content
732

have shown more dramatic shrinkage [26], and in a sepa-rate experimental evaluation on porcine corneas we ob-served a mean shrinkage effect of about 25% (unpub-lished results). Although in experimental retinal studies agood correlation was found between OCT and histologi-cal retinal thickness, the differences were approximately45% [19]. In contrast, another study revealed that histo-logical sections of the retina averaged 4% to 12% largerthan the corresponding OCT images [27]. Thus, furtherquantitative comparison from stained cryosections of un-fixed corneas might enable a more accurate relationship,due to processing without fixation, dehydration or em-bedment, with better preservation of tissue dimensions asshown in other retinal studies [15].
Another important source of error could be related tothe unknown refractive index for pathologically alteredcorneal tissue. As previously recommended we used, forOCT thickness determinations at a wavelength of830 nm, the corneal group refractive index of 1.3853[11, 28, 31]. In the normal cornea the most importantchanges from the empirically derived refractive indicesoccur at the epithelium (n=1.401) and the posterior stro-ma (n=1.373) [22]. However, in pathological processeswith tissue scarring and edema the intra-individual andlocal variations of dispersion or refractive index could bemore dramatic, and thus greatly influence the propaga-tion of light through the different corneal components.For example, dry collagen has a refractive index of1.547, corneal fibrils of 1.47, and the ground substanceof 1.35 [20]. An increasing hydration of corneal tissue
with aqueous humor would lead to a decrease of the re-fractive index toward 1.336 [20].
In summary, our descriptive histopathological investi-gation contributed to the understanding of the infraredlight–tissue interaction in OCT, and enabled the correla-tion of the cross-sectional variation of the light-reflectionprofile with morphological changes in LM. Although thelight-reflection profile provided rapid, non-invasive, andobjective results of corneal dimensions, only the two-dimensional scan enabled the morphological evaluationof the corneal anatomy and demonstration of size andshape of corneal abnormalities. Despite the high resolu-tion, we observed that this clinical OCT system was lim-ited to relatively large morphological changes, comparedwith LM. Refinements of the current imaging modalitieswith shorter coherence lengths or broader spectral band-widths, such as dual-beam OCT [1] or ultra-high-resolu-tion OCT, reaching a resolution of 2 µm in the cornea[5], combined with advanced scanning methods [25]could enable us to visualize the microstructural detailsand cellular layers more precisely, and eventually allowmore detailed diagnostic imaging of tissue morphologywithout the need for excision of specimens [7]. Thus,with certain limitations, the current slitlamp-adaptedOCT system can provide a noncontact optical biopsy ofthe corneal structures, and could be helpful to investi-gate, diagnose and monitor corneal diseases.
Acknowledgement In memory of Professor G. O. Bastian, whounexpectedly died in February 2002. This work was supported inpart by the “Herbert Funke-Stiftung”, Berlin.
733
References
1. Baumgartner A, Hitzenberger CK, Ergun E, Stur M, Sattmann H, DrexlerW, Fercher AF (2000) Resolution-improved dual-beam and standard opti-cal coherence tomography: a compari-son. Graefes Arch Clin Exp Ophthal-mol 238:385–392
2. Bland JM, Altmann DG (1986) Statis-tical methods for assessing agreementbetween two methods of clinical mea-surement. Lancet I:307–310
3. Bron AJ (2001) The architecture of thecorneal stroma (editorial). Br J Ophthal-mol 85:379–381
4. Chauhan DS, Marshall J (1999) The in-terpretation of optical coherence to-mography images of the retina. InvestOphthalmol Vis Sci 40:2332–2342
5. Drexler W, Morgner U, Ghanta RK,Kärtner FX, Schuman JS, Fujimoto JG(2001) Ultrahigh-resolution ophthal-mic optical coherence tomography. Nat Med 7:502–507
6. Freund DE, McCally RL, Farrell RA,Cristol SM, L’Hernault NL, Edel-hauser HF (1995) Ultrastructure in anterior and posterior stroma of per-fused human and rabbit corneas. Invest Ophthalmol Vis Sci 36:1508–1523
7. Fujimoto JG, Brezinski ME, TearneyGJ, Boppart SA, Bouma B, Hee MR,Southern JF, Swanson EA (1995) Opti-cal biopsy and imaging using opticalcoherence tomography. Nat Med1:970–972
8. Gurses-Ozden R, Ishikawa H, Hoh ST,Liebmann JM, Mistlberger A, Green-field DS, Dou HL, Ritch R (1999) In-creasing sampling density improves re-producibility of optical coherence to-mography measurements. J Glaucoma8:238–241
9. Hee MR, Izatt JA, Swanson EA,Huang D, Shuman JS, Lin CP, PuliafitoCA, Fujimoto JG (1995) Optical co-herence tomography of the human retina. Arch Ophthalmol 113:325–332
10. Hirano K, Ito Y, Suzuki T, Kojima T,Kachi S, Miyake Y (2001) Optical co-herence tomography for the noninva-sive evaluation of the cornea. Cornea20:281–289
11. Hitzenberger CK, Baumgartner A,Drexler W, Fercher AF (1994) Inter-ferometric measurement of cornealthickness with micrometer precision.Am J Ophthalmol 118:468–476
12. Hoerauf H, Gordes R, Scholz C, Wirbelauer C, Koch P, Engelhardt R,Winkler J, Laqua H, Birngruber R(2000) First experimental and clinicalresults with transscleral optical coher-ence tomography. Ophthalmic Surg Lasers 31:218–222
13. Huang D, Swanson EA, Lin CP, Schuman JS, Stinson WG, Chang W,Hee MR, Flotte T, Gregory K, PuliafitoCA, Fujimoto JG (1991) Optical coher-ence tomography. Science 254:1178–1181

14. Huang D, Wang I, Lin CP, PuliafitoCA, Fujimoto JG (1991) Micron-reso-lution ranging of cornea anterior cham-ber by optical reflectometry. LasersSurg Med 11:419–425
15. Huang Y, Cideciyan AV, PapastergiouGI, Banin E, Semple-Rowland SL, Milam AH, Jacobson SG (1998) Rela-tion of optical coherence tomographyto microanatomy in normal and rdchickens. Invest Ophthalmol Vis Sci39:2405–2416
16. Iwadare T, Mori H, Ishiguro K, TakeishiM (1984) Dimensional changes of tis-sues in the course of processing. J Microsc 136:323–327
17. Izatt JA, Hee MR, Swanson EA,Lin CP, Huang D, Schuman JS, Puliafito CA, Fujimoto JG (1994) Micrometer-scale resolution imagingof the anterior eye in vivo with opticalcoherence tomography. Arch Ophthal-mol 112:1584–1589
18. Komai Y, Ushiki T (1991) The three-dimensional organization of collagenfibrils in the human cornea and sclera.Invest Ophthalmol Vis Sci 32:2244–2258
19. Li Q, Timmers AM, Hunter K, Gonzalez-Pola C, Lewein AS, ReitzeDH, Hauswirth WW (2001) Noninva-sive imaging by optical coherence to-mography to monitor retinal degenera-tion in the mouse. Invest OphthalmolVis Sci 42:2981–2989
20. Maurice DM (1957) The structure andtransparency of the cornea. J Physiol136:263–268
21. Müller LJ, Pels E, Vrensen GFJM (2001)The specific architecture of the anteriorstroma accounts for maintenances ofcorneal curvature. Br J Ophthalmol85:437–443
22. Patel S, Marshall J, Fitzke III FW(1995) Refractive index of the humancorneal epithelium and stroma. J Refract Surg 11:100–105
23. Patel SV, McLaren JW, Camp JJ, Nelson LR, Bourne WM (1999) Auto-mated quantification of keratocyte density by using confocal microscopyin vivo. Invest Ophthalmol Vis Sci40:320–326
24. Puliafito CA, Hee MR, Lin CP, ReichelE, Schuman JS, Duker JS, Izatt JA,Swanson EA, Fujimoto JG (1995) Im-aging of macular diseases with opticalcoherence tomography. Ophthalmology102:217–219
25. Radhakrishnan S, Rollins AM, RothJE, Yazdanfar S, Westphal V, Barden-stein DS, Izatt JA (2001) Real-time optical coherence tomography of theanterior segment at 1310 nm. Arch Ophthalmol 119:1179–1185
26. Stiekland NC (1975) A detailed analy-sis of the effects of various fixatives onanimal tissue with particular referenceto muscle tissue. Stain Technol 50:255–264
27. Toth CA, Narayan DG, Boppart SA,Hee MR, Fujimoto JG, Birngruber R,Cain CP, DiCarlo CD, Roach WP(1997) A comparison of retinal mor-phology viewed by optical coherencetomography and by light microscopy.Arch Ophthalmol 115:1425–1428
28. Wirbelauer C, Scholz C, Hoerauf H,Engelhardt R, Birngruber R, Laqua H(2000) Corneal optical coherence to-mography before and immediately afterexcimer laser photorefractive keratec-tomy. Am J Ophthalmol 130:693–699
29. Wirbelauer C, Scholz C, Hoerauf H,Bastian GO, Engelhardt R, BirngruberR, Laqua H (2001) Untersuchungen derHornhaut mittels optischer Kohärenz-tomographie. Ophthalmologe 98:151–156
30. Wirbelauer C, Scholz C, Engelhardt R,Laqua H, Pham DT (2001) Biomorpho-metrie des Hornhautepithels mittelsspaltlampenadaptierter optischer Kohä-renztomographie. Ophthalmologe98:848–852
31. Wirbelauer C, Scholz C, Hoerauf H,Pham DT, Laqua H, Birngruber R(2002) Noncontact corneal pachymetrywith slitlamp-adapted optical coher-ence tomography. Am J Ophthalmol133:444–450
32. Wirbelauer C, Scholz C, Häberle H,Laqua H, Pham DT (2002) Corneal optical coherence tomography beforeand after excimer laser phototherapeu-tic keratectomy for recurrent epithelialerosions. J Cataract Refract Surg28:1631–1637
734