Embed Size (px)
Citation preview

Histology: Its Influence on
Therapeutic Decision Making
Mark A. Socinski, MD
Professor of Medicine and Thoracic Surgery
Director, Lung Cancer Section, Division of Hematology/Oncology
Co-Director, UPMC Lung Cancer Center of Excellence and Lung and Thoracic Malignancies Program
University of Pittsburgh

•
• • •
•
• •

•
•
•
• •

•
•
•

•
•
•
•

• •
•
• •
•

Histology: Its Influence on
Therapeutic Decision Making
Mark A. Socinski, MD
Professor of Medicine and Thoracic Surgery
Director, Lung Cancer Section, Division of Hematology/Oncology
Co-Director, UPMC Lung Cancer Center of Excellence and Lung and Thoracic Malignancies Program
University of Pittsburgh

Disclosures
Advisory Committee
Bristol-Myers Squibb Company, Daiichi Sankyo Inc, Lilly
Contracted Research
Bayer HealthCare Pharmaceuticals, Boehringer Ingelheim Pharmaceuticals Inc, Bristol-Myers Squibb Company, Celgene Corporation, Genentech BioOncology, GlaxoSmithKline, Lilly, Merck, Novartis Pharmaceuticals Corporation, Pfizer Inc, Roche Laboratories Inc, Synta Pharmaceuticals Corp
Speakers Bureau Celgene Corporation, Genentech BioOncology

Overview of NSCLC Histologies
NSCLC adenocarcinoma
Adenocarcinoma is a malignant epithelial tumor with glandular differentiation or mucin production, showing acinar, papillary, bronchoalveolar, or solid with mucin growth patterns or a mixture of these patterns.
NSCLC large cell carcinoma
Large cell carcinoma is an undifferentiated non-small cell carcinoma that lacks the cytologic and architectural features of small cell carcinoma and glandular or squamous differentiation.
NSCLC squamous cell carcinoma
Squamous cell carcinoma is a malignant epithelial tumor showing keratinization and/or intercellular bridges that arise from bronchial epithelium. These features vary with degree of differentiation, being prominent in well-differentiated tumors and focal in poorly differentiated tumors.
Images copyright © 2007 Asterand PLC Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart. IARCPress. 2004:26-30.
Diagnostic Accuracy – influenced by type of biopsy procedure, quantity of tumor in the specimen, degree of tumor differentiation, use of ancillary studies, experience of the pathologist

EASY CASES- MORPHOLOGY IS SUFFICIENT
SCLC ADC SQC
SQC- basaloid ADC-solid pattern LCNEC
NOT SO EASY CASES – IHC SHOULD HELP

IMMUNOHISTOCHEMISTRY AND NSCLC
MARKER ADENOCARCINOMA SQUAMOUS CELL CARCINOMA
CK 7 ~90 ~20-30 CK5/6 10-20 ~100 P63 10-20 ~100
TTF-1 70-90 Almost never P40 Almost never ~100
Cytokeratin 20, Napsin A, surfactant A, Ber-EP4, B72.3, synaptophysin, chromogranin, CD56, CEA

IMMUNOHISTOCHEMISTRY AND NSCLC- SMALL SPECIMENS
IHC 1 SQC/1 ADC and/or mucin
ADC IHC + or mucin+
SQC IHC -
NSCLC, favor ADC
SQC IHC + ADC
IHC - or mucin-
NSCLC, favor SQC
SQC IHC + ADC
IHC + or mucin+
NSCLC,NOS possible
adenosquamous
IHC- mucin -
NSCLC,NOS

Small Biopsies/Mixed Histology
• Confidence in the diagnosis aids therapeutic choices .talk to your pathologist
• Clearly sampling bias is an issue • When uncertain, clinical factors must be considered - smoking status, age, co-morbidities, PS, etc • Optimize cytotoxic choices based on.. - efficacy (ORR, PFS, OS benefits) - toxicity • Second pathologic opinions can be helpful

5 Reasons Why Medical Oncologists Care About Histology
• Reason #1 – Bevacizumab • Reason #2 – Pemetrexed • Reason #3 – Molecular testing • Reason #4 – nab-paclitaxel • Reason #5 - Necitumumab

Reason #1: Bevacizumab in NSCLC: Bleeding in Randomized Phase II Trial • 6 life-threatening pulmonary hemorrhages; 4 fatal
– Overall incidence: 9% (6/66) – 5 occurred at bevacizumab 7.5 mg/kg
• Apparent risk factors – Baseline hemoptysis – Histology
• Squamous histology: 31% (4/13) • Nonsquamous histology: 4% (2/53)
Johnson. J Clin Oncol. 2004;22:2184; Sandler. ASCO. 2005 (abstr 4).
Chemotherapy-naïve stage IIIB (wet)
or IV NSCLC N=99
Carboplatin + Paclitaxel Placebo Bevacizumab
15 mg/kg
Carboplatin + Paclitaxel Bevacizumab 7.5 mg/kg
Carboplatin + Paclitaxel Bevacizumab 15 mg/kg
PD
PD=progressive disease.

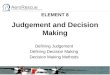
Reason #2: Cisplatin/Pemetrexed vs Cisplatin/ Gemcitabine in Advanced NSCLC: Results
1.23;1.00, 1.51
9.4;8.4, 10.2 10.8;9.5, 12.1
Survival Time (months) in Patients With SCC
Surv
ival
Pro
babi
lity
9.4 mos Median Survival
10.8 mos Adjusted HR CP vs CG
1.23
Squamous Nonsquamous
Median Survival
0.81;0.70, 0.94
Survival Time (months) in Patients With Nonsquamous Histology
Surv
ival
Pro
babi
lity
10.4 mos
0.81
11.8 mos
Adjusted HR CP vs CG
Scagliotti GV et al: J Clin Oncol. 26 (21), 2008: 3543-3551.

Reason #3 – Molecular Testing

Molecular Profiling and Therapeutic Decision Making for Advanced NSCLC
General Guidelines for 2013
• Who to test: patients with NSCLC and adenocarcinoma component
• What to test for: EGFR mutation and ALK fusion (+ others?)
• When to test: at the time of diagnosis (not just when treatment decision needed)
• What specimen: core needle biopsy (or multi-pass FNA), cytology cell block, surgical biopsy (bone biopsy problematic)
• How to test: concurrently (not sequentially test-by-test)
• How long a turnaround time is acceptable?: 2 weeks or less
• When to re-test: after a targeted therapy intervention (to assess for tumor evolution in the molecular profile)
Adapted from: CAP/IASLC/AMP Guidelines

Socinski MA et al, Annals of Oncology, 24:2390-6, 2013
Reason #4: ORR by Histology: CbP vs Cb-nab-P in Advanced NSCLC
a 95% CIs for response rate ratios are calculated according to the asymptotic 95% CI of the relative risk of nab-PC to sb-PC.

0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40
0
20
40
60
80
100
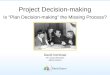
Reason #5: SQUIRE Primary Outcome: Overall Survival ITT1
GC+N N=545
GC N=548
Stratified HR (95% CI) 0.84 (0.74, 0.96) Stratified p-value (log-rank) 0.01 Median, months (95% CI) 11.5 (10.4, 12.6) 9.9 (8.9, 11.1)
Time Since Randomization (Months)
Ove
rall
Sur
viva
l (%
)
GC+N GC
1Thatcher N, et al. Lancet Oncol 2015;16(7):763-74
Necitumumab + Cis/Gem Vs Cis/Gem Alone in Stage IV Squamous Carcinoma

Why Do Medical Oncologists Care About Histology?
• Molecular testing – Current guidelines recommend routine testing for
EGFR and ALK in adenocarcinoma • Therapeutic considerations
– Bevacizumab contraindicated in squamous histology due to risk of pulmonary hemorrhage
– Pemetrexed indicated in non-squamous histologies – Nab-P + Cb has superior ORR in squamous histology – Necitumumab indicated in squamous histology
• Prognosis – In general, individuals with non–squamous cell lung
cancer do slightly better than those with squamous cell
Lindeman et al, 2013, Scagliotti et al, 2008. Johnson et al, 2004. Thatcher et al, 2015

Histology: Its Influence on
Therapeutic Decision Making
Mark A. Socinski, MD
Professor of Medicine and Thoracic Surgery
Director, Lung Cancer Section, Division of Hematology/Oncology
Co-Director, UPMC Lung Cancer Center of Excellence and Lung and Thoracic Malignancies Program
University of Pittsburgh

•
• •
•
•
•

•
• • •
•