Embed Size (px)
DESCRIPTION
manual
Citation preview

1
Microscopic AnatomyLaboratory Manual

2
© 1992 Washington University School of Medicine
The Microscopic Anatomy Laboratory Manual is a result of the combined efforts of several former and
current members of the Department of Anatomy and Neurobiology. The principle contributors include
Drs. Allen Enders, Barry King, Milton Goldstein, Nancy Baenziger, Richard Bischoff, David Menton and
Adolph Cohen.
Credit is also due to the many students down through the years who have contributed useful suggestions
for improving the Manual. Indeed, it was at the suggestion of our students that the Manual was written
in the first place.
Finally, I wish to acknowledge our University, who has steadfastly underwritten the expense of producing
the Manual every year, permitting us to distribute it to our students at no further cost to them.
Paul C. Bridgman, Ph. D.
Coursemaster of Microscopic Anatomy
Department of Anatomy and Neurobiology
Washington University School of Medicine
Box 8108
660 South Euclid Avenue
St. Louis, Missouri 63110

3
Introduction 9The demise of the teaching labThe value of the teaching labSuggestions for success in the histology lab
Slide Collection 11Student Loan CollectionBox ABox B
Slide Inventory
Histological Methods 15Fixation
Functions of a fixative
Dehydration and EmbeddingSectioningStaining Sections and Tissues
The Microscope 19Theoretical Considerations
Study questions
Cleaning the MicroscopeCleaning the oil immersion lens
Illumination of the Light MicroscopeThe Dual-View Teaching Head
Install the dual body-tube as follows
Proper Use of the dual teaching head
The Cell 25Basophilic vs. AcidophilicMembranous Structures in the Cell
Contents

4
Filamentous and Tubular Organelles
Epithelial Tissues 31Simple EpitheliaPseudostratified EpitheliaStratified EpitheliaTransitional
Blood 35Wright’s Stained Smear of Peripheral Blood
Preparation of slide
Staining Method
Abnormalities of erythrocytes
Common artifacts in blood smears
Study questions on EMs.
Fibrous Connective Tissue 41Loose Connective TissueDense Connective TissueEmbryonic Connective TissueElectron Micrographs
Cartilage 45Hyaline CartilageElastic CartilageFibrocartilageElectron Micrographs
Bone 47Ground Bone PreparationsEndochondral Ossification
CONTENTS

5
Intramembranous Ossification
Muscle 51Skeletal MuscleSmooth MuscleCardiac Muscle
Peripheral Nerves 53Can you identify in slide 92A
Integrative questions in neuroanatomy
Cardiovascular System 57Arteries and VeinsLymphaticsHeart
Hemopoiesis 59Electron Micrographs
Lymphatic Tissue 61ThymusPeripheral Lymphoid TissueSpleen
Integumentary System 67Epidermis and DermisHairSweat Glands
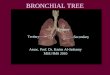
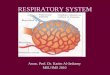
Respiratory System 71Nasal CavityTracheaLung
CONTENTS

6
Electron Micrographs
Oral Cavity 75LipsTeethTonguePalateSalivary Glands
Esophagus and Stomach 79EsophagusStomach
Intestine 81DuodenumJejunumIleumColonAppendixRectumElectron Micrographs
Pancreas 83Exocrine PancreasEndocrine PancreasElectron Micrographs
Liver and Gallbladder 85Liver
Contents of the portal tract
Gallbladder
CONTENTS

7
Electron Micrographs of Liver
Urinary System 89KidneyUreter & Bladder
Layers of ureter and bladder
Endocrine System 93HypophysisThyroidParathyroidAdrenal Gland
Male Reproductive System 97TestisAccessory Reproductive StructuresPenis
Female Reproductive System 103OvaryUterusVaginaOviductPlacentaThe Female Breast
Glossary 109

8

9
The demise of the teaching labIn the last 25 years, most courses at this and other medical schools have either de-emphasized or discontinued the laboratory as a learning experience. It is, perhapsironic that this should occur at the same time that nearly everyone concerned with themedical school curriculum recognizes the pedagogical inadequacy and tedium ofcountless hours of lectures. While there has been broad agreement that "activelearning" should, wherever possible, replace "passive learning," active learning hasnot always included laboratory study. In many courses, labs have been replaced withdiscussion groups and problem-solving sessions. Laboratory study has alwaysincluded these immensely important components, but when discussions and problem-solving are divorced from the lab experience, they too can become more passive thanactive.
There are several reasons for the demise of the lab in medical education. First,labs are expensive. The microscopic anatomy lab at this medical school involves anexpenditure of approximately $250,000 in microscopes alone. In addition, severalthousand dollars is spent each year in the administration and maintenance of ourteaching laboratories, microscopes, slide sets and supplies. The cost of the grossanatomy lab (and its associated body donation program) greatly exceeds the cost ofthe microscopic anatomy lab. Secondly, labs are demanding and labor-intensive forthe faculty. It is relatively easy to give a dozen or so lectures and/or discussions eachyear on selected subjects closely related to one's field of expertise and research, butfar more demanding to serve effectively in a teaching laboratory where wide-rangingquestions emerge spontaneously from both the lab and the lecture. Finally, manystudents find the lab an "inefficient" way to learn, given the great demands on their timeand energy. It is much easier and quicker to either read or hear what you "need toknow" than to discover it for yourself in a lab.
The value of the teaching labPerhaps then, a defense of the teaching laboratory is in order. Your microscopicanatomy faculty believes that the expense, labor, and putative inefficiency of a lab areeasily compensated by a sense of discovery and depth of insight not easily obtainedby any other means. Even lectures become tolerable if they are followed by anopportunity to examine for oneself the very subject of the lecture. Lectures anddiscussions remain only mental exercises, until one has an opportunity to both use andreinforce that information with personal experience. More importantly, the informationthat can be gleaned from the study of actual biological tissues and organs is essentiallywithout limits. In contrast, the prepared information to be found in a lecture, book,photograph, etc., is finite and necessarily reflects the bias of its author. For biologicalknowledge to increase, there must be some point where the closed loop of codified
Introduction

10
information is open to the discovery of new information from nature itself. There aremany examples in the biomedical research literature of observations that could havebeen made by an astute observer of our class set of microscope slides and electronmicrographs. We are convinced that if you have made a good career choice inmedicine and/or biomedical research, you will appreciate the opportunity to discoverfor yourself the marvelously complex world of microscopic anatomy. Your facultyis enthusiastic about assisting you in this discovery, and, indeed, we will be learningwith you.
Suggestions for success in the histology labFirst, we urge you to regularly attend lab. Only by regular practice and experiencewill you learn to grasp the three-dimensional world of microscopic anatomy from thenearly (but not quite) two-dimensional specimens on your microscope slides. Beforeyou come to lab, you may find it helpful to read the relevant section of your lab guideand atlas. Also, the Menton collection in the library has proved useful to many as alab orientation or preview. This collection is available in three forms: color 35-mmtransparencies, Kodak Photo CDs and a computer tutorial on the network. All ofthese comprise the same specimens you will be studying in the lab.
When you come to lab, we suggest that you bring your textbook or atlas as youwill often find a photo or drawing that assists you in understanding the specimens onyour slides. Perhaps the most important suggestion we can give you is that you notleave the lab until you have seen several examples of each of the structures printedin boldface in this manual. This is best accomplished by keeping your eyes open forstructures you have already seen as you search for new ones. Typically, the samestructure will appear in several places on your slides, giving you a chance to see themin several planes of section.
The double-viewing attachment we provide gives you an opportunity to viewyour slides with another observer -- both seeing the same specimen right-side-up andwith a common pointer. This encourages analysis and discussion of histologicalstructures with your lab partner or the faculty, and teaches you to use the terminologyyou will encounter in your medical career.
Finally, we urge you to consider drawing many of your specimens in an unlinednotebook. Even a bad drawing teaches you to be a careful observer.
INTRODUCTION

11
Slide Collection
Student Loan Collection
Two students must share a set of slides comprising Box A and Box B. Slides in Box B aredistinguished by the presence of a line below the slide number; those in Box A have no underline.Each slide also bears the number of it's slide set - please do not mix them with other sets. Youwill be held responsible for the slides in the set you are issued.
Abbreviations usedAB Alcian blue
AF Aldehyde-fuchsin
BS Bodian silver
CCH Copper-chrome hematoxylin
CIV Carmine injection - vascular system perfused with gelatin and carmine
FG Fast green
H & E Hematoxylin and eosin
H & OGE Hematoxylin and orange G-erythrosin
IH Iron hematoxylin
MC Muci-carmine
MT Mallory trichrome
OG Orange green
OT Osmium tetroxide
PAS Periodic acid - Schiff
PTAH Phosphotungstic acid hematoxylin
RF Resorcin-fuchsin
SB Sudan black
VH Verhoeff’s hematoxylin
All specimens are human tissue unless otherwise indicated.

12
SLIDE COLLECTION
1A Skin, digital, monkey; H & E; AF; OG; FG; CIV2A Skin, digital monkey; Bodian silver (carmine)3A Scalp, human L.S.4A Scalp, bald; H & E5A Skin, scalp; H & E6A Skin, adult thigh; H & OGE; VH7A Skin, palmar, monkey; H & E; plastic section8A Skin, axillae; H & E9A Tendon; H & El0A Musculotendinous junction; H & EllA Musculotendinous junction; PTAHl2A Skeletal muscle, monkey; H & E; plastic sectionl3A Skeletal muscle, dog; H & OGEl4A Skeletal muscle, dog; IHl5A Heart, mammal; H & El6A Heart, monkey; H & E; plastic sectionl7A Heart, monkey; H & El8A Heart, monkey, base of ventricles; AF, OG, FGl9A Heart, ventricle, dog; PTAH20A Heart, beef, endocardium, Purkinje fibers; H & E2lA Heart, human, left ventricle; H & E22A Vena cava; H & E23A Aorta; H & OGE; VH24A Arteries, monkey; H & E25A Artery, vein, nerve; VH26A Mesentery; whole mount, CIV27A Artery and vein, monkey; H & E; plastic section28A Tibia, cross section, rabbit; H & E29A Bone marrow, hyperplastic; H & E30A Tonsil, dog; H & OGE31A Blood smear, normal; Wright's stain32A Bone marrow, human; Wright’s stain33A Aorta, monkey; H & E; plastic section34A Lymph node, monkey; H & E; plastic section35A36A Lymph node, dog; silver impregnation; H & OGE37A Thymus, human; H & E; plastic section38A Thymus, infant; H & E39A Areolar tissue spread; RF40A Thymus, newborn; H & E4lA Thymus, involuting; H & E42A Fatty thymus, adult, small mammal; H & E43A Spleen; silver impregnation; H & OGE44A Spleen, engorged; H & E45A Spleen, washed through artery, dog; H & OGE46A Spleen, phagocytosed carbon, rat; H & E47A Spleen, monkey; H & E; plastic section48A Spinal ganglion, cat; H & E49A Tendon, monkey; H & E; plastic section50A Elastic cartilage, ear, dog; H & OGE; VH
5lA Vertebral column, cat, longitudinal section; H & E52A Fibro-cartilage, intervertebral disc; H & E53A Vertebral column, cat; H & E54A Jaw bone, infant; H & E55A Thorax, human fetus (40 mm); tetrachrome56A Ribs, stillborn; M (with fast green rather than aniline blue)57A Foot, 5-month fetus; H & OGE58A Finger, stillborn; and 5-month fetus; H & OGE59A Compact bone, ground section60A Knee joint, cat; H & E6lA Developing “membrane” bone; H & E62A Fracture, l3 days, rabbit; H & E63A Lip; H & E64A Tooth and mandible, monkey; H & E65A Tongue, monkey; H & E66A Tongue with taste buds, monkey; H & E67A Parotid gland, dog; H & OGE68A Parotid gland, monkey; H & E; PAS69A Submandibular gland, monkey; H & E; aldehyde fuchsin70A Submandibular gland, monkey; PAS7lA Submandibular gland; H & E72A Submandibular gland, monkey; H & E; plastic section73A Larynx, frontal section; H & E74A Sublingual gland, monkey; H & E75A Esophagus; H & E76A Esophagus and trachea; H & E77A Gastro-esophageal junction, monkey; CCH; Muci78A Stomach, fundus; H & OGE79A Stomach, fundus, monkey; H & E; plastic section80A Stomach, fundus, dog; IH; PAS8lA Mesothelium, rabbit; silver stain82A Pyloro-duodenal junction, monkey; H & E83A Pyloro-duodenal junction, monkey; CCH; Muci84A Jejunum, 40 years; H & E85A Jejunum, monkey; H & E; PAS (carmine)86A Jejunum, monkey; H & E; plastic section87A Duodenum, human; H & E; plastic section88A Ileum, human; H & E; plastic section89A Ileum; H & E90A9lA Ileum, cat, Peyer’s patch; H & E92A Nerve, dorsal root ganglion in culture; OT and SB93A Enteric nerve plexus (Auerbach), cat; Richardson silver94A Colon, monkey; H & E95A Rectum, human; H & E96A Appendix, human; H & E; plastic section97A Appendix, carmine-injected vessels98A Appendix, infant; H & E99A Recto-anal junction; H & OGEl00A Adipose tissue, monkey; H & E; plastic section
Box A

13
SLIDE COLLECTION
lB Liver, bile canaliculi; silver impregnation2B Liver, infant; H & E3B Liver, dog; intravenous carbon injection4B Liver, rat; intravenous trypan blue; H & E5B Liver, cat; carmine injected vessels6B Liver, rat; regenerating; H & E7B Liver, monkey; H & E; plastic section8B Gallbladder, monkey; H & E; plastic section9B Gallbladder; H & El0B Pancreas, human; H & EllB Pancreas, cat; H & E; guinea pig; aldehyde fuchsinl2B Pancreas, monkey; H & E; plastic sectionl3B Thyroid gland, monkey; H & E; plastic sectionl4B Thyroid and parathyroid, dog; H & OGEl5B Neck organs, monkey; H & El6B Thyroid, rabbit, hyperplastic; H & El7B Adrenal and kidney, fetal, human; tetrachromel8B Adrenal, dog; H & El9B Adrenal, monkey; H & E20B Adrenal, monkey; H & E; plastic section2lB Adrenal, infant; H & E22B Parathyroid, human; H & E23B Hypophysis; H & E24B Hypophysis, human; Masson25B Hypophysis, rabbit; PAS; orange G; alcian blue26B Pituitary and hypothalamus, cat; H & E27B28B Nasal cavity, cat; H & E29B30B Soft palate, cat; H & E3lB Lung, monkey; H & E; plastic section32B Lung, monkey; VH and picro-ponceau33B Epiglottis, elastic cartilage; VH34B Palate, cat; H & E35B Trachea; H & E36B Trachea, monkey; H & E; plastic section37B Lung, rabbit; H & E; aldehyde fuchsin38B Lung, cat collapsed, pneumothorax; H & E39B Lung, thick section40B Lung, dog; carmine injected vessels4lB42B Kidney, 40 years; H & E43B Kidney, rabbit; carmine injected; orange G, fast green44B Kidney, monkey; H & E; plastic section45B46B Kidney, rabbit; carmine injected; PAS; H & E47B Kidney, guinea pig; silver impregnation48B Ureter, monkey; H & E; plastic section49B Kidney, mouse; alkaline phosphatase50B
5lB Bladder, relaxed and stretched; H & E52B53B Testis, monkey, mature; H & E or tetrachrome54B Testis and epididymis, monkey; H & E55B Testis, monkey; H & E; plastic section56B Testis and epididymis, infant; H & E57B Hela cells, mitosis; H58B59B Spermatic cord with ductus deferens, human; H & E60B Seminal vesicle, monkey; H & E; plastic section6lB Seminal vesicle; H & E62B Bulbo urethral, adult rabbit; H & E63B Prostate, monkey; H & E64B Prostate; H & E65B Prostate, monkey; H & E; plastic section66B Penis, stillborn; H & OGE67B Bladder, monkey; H & E; plastic section68B Ovary, monkey; H & E; plastic section69B Ovary, corpus luteum, 25th day menstrual cycle; H & E70B Ovary, corpus luteum, first trimester; M7lB Ovary, infant; H & E72B Ovary, senile; H & E73B Ovary and uterine tube, small mammal; H & E74B Uterine tube, human, l7 years old; H & E75B Uterine tube; H & E76B Uterine tube; senile; H & E77B Uterus, early and late luteal phases; H & E78B Uterus, menstruating and follicular phases; H & E79B Uterus, 2 months pregnant, human; H & E80B Uterus, monkey; H & E; plastic section8lB Cervix and uterus, term human baby; H & E82B Cervix, adult; H & E83B Vagina, monkey; H & E; plastic section84B Vagina, 20 years; H & E85B86B Placenta, human, 2-month; H & E87B Placenta, human, full term; H & E88B Oviduct monkey; H & E; plastic section89B Placenta, human at parturition; tetrachrome90B Placenta, human, lst trimester; H & E9lB Placenta, human, early 2nd trimester; H & E92B Mammary gland, nonpregnant; H & E93B Placenta, human, 3rd trimester; H & E; plastic section94B Mammary gland, senile; H & E95B Mammary gland, lactating; H & E96B Umbilical cord, human, tetrachrome97B98B Eyelid, rabbit; H & E99B Mammary gland, monkey; resting; H & El00B Mammary gland, monkey; lactating; H & E
Box B

14
Indicate damaged or missing slides in the appropriate spaces below.A blank space after a number indicates that slide is present in the box and serviceable.
Box A
1. 26. 51. 76.
2. 27. 52. 77.
3. 28. 53. 78.
4. 29. 54. 79.
5. 30. 55. 80.
6. 31. 56. 81.
7. 32. 57. 82.
8. 33. 58. 83.
9. 34. 59. 84.
10. 35. 60. 85.
11. 36. 61. 86.
12. 37. 62. 87.
13. 38. 63. 88.
14. 39. 64. 89.
15. 40. 65. 90.
16. 41. 66. 91.
17. 42. 67. 92.
18. 43. 68. 93.
19. 44. 69. 94.
20. 45. 70. 95.
21. 46. 71. 96.
22. 47. 72. 97.
23. 48. 73. 98.
24. 49. 74. 99.
25. 50. 75. 100.
1. 26. 51. 76.
2. 27. 52. 77.
3. 28. 53. 78.
4. 29. 54. 79.
5. 30. 55. 80.
6. 31. 56. 81.
7. 32. 57. 82.
8. 33. 58. 83.
9. 34. 59. 84.
10. 35. 60. 85.
11. 36. 61. 86.
12. 37. 62. 87.
13. 38. 63. 88.
14. 39. 64. 89.
15. 40. 65. 90.
16. 41. 66. 91.
17. 42. 67. 92.
18. 43. 68. 93.
19. 44. 69. 94.
20. 45. 70. 95.
21. 46. 71. 96.
22. 47. 72. 97.
23. 48. 73. 98.
24. 49. 74. 99.
25. 50. 75. 100.
Box B

15
To intelligently use the slides in your slide collection, you should have at least some knowledgeof the histological technique that has gone into their preparation.
FixationThe first step in preparing slides of a specimen for light microscopy is fixation. Ideally thisaccomplishes the following important requirements for subsequent sectioning and staining:
Functions of a fixative
· Kills the tissue quickly.
· Preserves much of the chemical composition of the cell.
· Minimizes tissue swelling or shrinkage.
· Inactivates tissue proteases.
· Imparts rigidity to preserve the shape and location of the tissue compo-nents during sectioning.
· Mordant for some dyes used in staining.
Most fixatives act on the proteins of the tissue to render them insoluble. The followingfixatives are commonly used for light microscopy:
FormalinFormalin is an aqueous solution of formaldehyde. It is easily the most common fixative for routinelight microscopy, and functions by binding to certain side groups of amino acids to formmethylene bridges between protein molecules. Aldehydes allow lipid extraction, but theypenetrate tissues quickly and preserve structure quite well.
AlcoholAlcohol coagulates protein and penetrates rapidly but dehydrates tissue and causes shrinkage.Alcohol preserves glycogen and other water soluble components of tissues better thanaqueous fixatives.
Bouin's FluidBouin's fluid is a mixture of the following three fixatives: Formalin - same function as describedabove. Picric acid - offsets the tendency of formalin to harden tissue excessively and makescytoplasm more basophilic (affinity for basic dyes). The exact chemical effect of this fixativeis not known although it probably forms additive compounds with amino groups. Acetic acid- offsets tissue shrinkage associated with picric acid by breaking salt linkages between proteinchains and exposing hydrophilic groups to water.
Histological Methods

16
HISTOLOGICAL METHODS
Special Fixative Ingredients
Chromium saltsCertain chromium salts such as potassium dichromate, produces oxidation and chromiumlinkages between proteins and also binds phospholipids.
Mercuric chlorideMercuric chloride acts on sulfhydryl; carboxyl and amino groups of protein, producing mercurylinkages between the molecules.
Immersion and Perfusion FixationFixatives are occasionally perfused into tissues in vitro by way of the blood stream but in mostcases, small blocks of tissue are simply immersed in the fixative. This latter method often resultsin unequal fixation in the block. When you study slides, you will often notice that tissuepreservation, shrinkage and even staining will vary from the periphery of the section to the centeras a result of the rate of penetration and varying exposure to the fixative. Slide 23B in yourcollection shows an example of this; note how the shrinkage and staining artifact at the peripheryof this pituitary gland differs from the better-preserved and stained interior. The periphery wasover fixed.
Dehydration and EmbeddingAll of the sections in our slide collection were cut from tissues embedded in either a paraffin orplastic matrix. Some sort of solid embedding matrix is essential for slicing the tissue into sectionsof about l0 µm or less in thickness. One can simply freeze a block of fresh tissue in water (or otheraqueous medium) and cut frozen sections in a cryostat microtome. This method has certainadvantages: it avoids extracting lipids, allows histochemical procedures for localizing enzymesin tissues, and is a very quick method attractive to surgical pathologists. Ice as an embedmenthas several disadvantages however, including rather severe ice crystal artifact in the tissue(though very quick freezing will minimize this).
Fixed tissues are typically dehydrated in a graded series of alcohol and are cleared in xyleneor other nonpolar solvent. Xylene makes the tissue more translucent to light, but even moreimportantly, xylene is miscible with the embedding medium and thus allows its penetration intothe tissue block. Paraffin is the most common embedding medium, although many slides in yourset have been embedded in celloidin (nitrocellulose). You can distinguish slides prepared bythese two embedding methods by looking carefully at the section with the unaided eye. In acelloidin section you will often see a rectangular field of celloidin that extends slightly beyondthe perimeter of the specimen. Unlike paraffin, celloidin is not dissolved from the section beforemounting (compare slide 6A [celloidin] with 8A [paraffin]).

17
Sectioning
Paraffin and Celloidin SectionsMost of the slides in your class set are sections cut from a block of embedded tissue. Paraffinand celloidin sections are typically cut about 5-l0 µm thick with a razor sharp steel knife mountedon a microtome. Sectioning is necessary if one is to examine the interior of a block of tissue, ratherthan just its outer surface. More importantly, a thin section allows us to transilluminate thespecimen with light in the microscope. In a sense, the light microscope “optically sections” yoursection even thinner due to the limited depth of focus of the high power objectives. At 400xmagnification, for example, the depth of field is only a little over l µm. It is for this reason thatone generally keeps focusing up and down through the specimen as you study, say, a 7 µm thicksection.
After sectioning, one or more sections are carefully placed on a microscope slide where theyare made to adhere as wrinkle-free as possible. Wrinkles are often confused with some structuralfeatures of tissues by the beginning student. You can easily detect a wrinkle because they havevery straight edges and are both thicker (often three thicknesses) and darker than the rest ofthe section. Naturally, you will also find occasional tears or separations in your sections. Afterthe paraffin is dissolved from the section, it is stained with one or more of a wide variety of stains.
Thin Plastic SectionsSome slides in your class set are plastic sections. In this case the tissue was embedded in a ratherhard epoxy resin and sectioned about l.5 µm thick with knives made from broken pieces of thickplate glass. These very thin sections offer greater clarity as well as greater detail of cellcomponents. Compare a l.5 µm thick plastic section of monkey testis (55B) with a 7 µm thickparaffin section of monkey testis (54B).
Non-Sectioned TissueThere are a few slides in your class set that really are not sections at all. Blood smears and
marrow smears (32A), for example, are not sections. The intact white blood cells of a smear looksubstantially larger than they would in sections of these same cells — why is this so? Cellscultured on a coverslip may also be observed without sectioning (57B). Slide 39A is a teased-out spread of areolar connective tissue which, of course, has not been sectioned.
Staining Sections and TissuesWhile the examination of unstained viable cells and tissues is frequently informative (particularlywith polarizing, phase, dark-field and fluorescence microscopy), most sections of tissue mustbe stained with dyes to reveal detailed structure under the light microscope. Often, more thanone stain is employed on the same slide to differentiate two or more tissue elements. It mustbe remembered that no one stain or combination of stains can satisfactorily differentiate all tissueelements. Whereas the hematoxylin and eosin method is perhaps the most commonly used stainto show general tissue morphology, specific or selective stains are frequently required to showcertain elements to best advantage. It is, for example, impossible to see mitochondria with most
HISTOLOGICAL METHODS

18
HISTOLOGICAL METHODS
procedures, but they can be stained by Janus green B with supravital techniques. Frequentlyeven the fixation must be carefully selected to either adequately preserve the desired tissueelements, or to promote their staining with a particular dye.
The slides loaned to you for this course have been stained with a wide variety of stains. Itwill be helpful to consider the possible reasons the indicated stain was used for each tissue andwhat you might expect to see in it. Histological specimens are most easily interpreted when youunderstand the specific staining characteristics of the stain used in preparation. The glossaryat the end of the lab manual includes all of the stains you will encounter in this course and detailstheir dye affinities for cell and tissue components. The two most common stains are hematoxylinand eosin (H & E) and hematoxylin and orange G-erythrosin (H & OGE), described below.
· Hematoxylin and eosin (H & E) - The most common histologic stain used for routinestudy of general morphology. Stains nuclei blue and practically all cytoplasmic structuresred. Those constituents staining blue with the basic dye hematoxylin are commonly calledbasophilic and those staining red with the acidic dye eosin are called acidophilic. Pronouncedbasophilia in the cytoplasm of cells usually indicates a high level of RNA and proteinsynthesis such as is observed in developing organs in the embryo (or in cells of the adultorganism that are very actively engaged in protein synthesis, e.g., the pancreatic acinar cells).As a general rule, the basic components of a tissue stain with acidic dyes and so are calledacidophilic, whereas the acidic components stain with basic dyes and are called basophilic.
· Hematoxylin and orange G-erythrosin (H & OGE) - A general purpose stain formorphology. The hematoxylin primarily stains nuclei and other basophilic constituents ofthe cell, if any. Orange G is a rather strongly acid dye which stains acidophilic componentssuch as the cytoplasm, an orange-red color. The erythrosin is also an acid dye, but stainssome structures such as smooth muscle, a light pink.

19
u
NA = n × sine µ
Theoretical Considerations
ResolutionResolution is the closest distance that two points may be separated and still observed to be twoseparate points. The resolution of the unaided eye is normally about .2 mm. The resolution ofthe light microscope depends on the wave length of light used and the numerical aperture ofits lens (the latter is stamped on the side of the objective). The ultimate resolution of the lightmicroscope using visible light is about 0.2 µm.
The maximum theoretical resolution of a light microscope with a given objective lens isdetermined by the following formula:
rNA
=0 6. l
Where r = resolutionλ = wave length of illumination
NA = numerical aperture of lens
The wave length of visible light is typically not under the control of the microscopist. Thenumerical aperture (NA) is equal to the sine of ½ the angle of aperture (µ) times the refractiveindex (n) of the medium through which the light passes and varies with the objective used. Theangle of aperture is the angle between a point in focus and the margins of the first lens of theobjective.
NA = n × sine µ
As can be seen by an examination of this formula, objectives designed to resolve smallerobjects must either have a very broad diameter (impractical) or a closer working distance toincrease the size of µ. In any case, the sine of the angle of aperture can only approach a valueas great as 1. To achieve a NA greater than 1, an immersion medium with a high refractive index,typically oil, must be placed between the specimen and the front lens of the objective. Whatis not as obvious is that the effective NA of the microscope is the average of the NA of theobjective and that of the condenser. We should then write the resolution formula as follows:
r NA NAOBJ Cond=
+l
Put simply, unless the condenser is able to fill the objective lens with light, the NA of the lenswill be reduced because the angle of aperture will be reduced. Consequently, over-closing theiris diaphragm of the condenser will reduce the effective NA.
The Microscope

20
Study questions:
1. Assuming a mean wave length for light of 0.5 µm, calculate the optimumresolution of your microscope for each of the objectives (4x, 10x, 40x, and100x), using the NA value marked on each objective.
2. What effect would the magnification of the eyepieces have on resolution?
3. Could you resolve any of the following with your microscope:
· cell membrane
· cilium
· mitochondrion
· ribosome
THE MICROSCOPE
Cleaning the MicroscopeA dirty objective lens is a common cause of lack of resolution in microscopes. If you suspecta dirty objective, unscrew it from the lens turret and examine the surface of the lens with aneyepiece from your scope. If you look through the eyepiece the “wrong way” it can be usedas a fine quality loupe. This will reveal any deposit on the lens.
The most common way of dirtying an objective lens (especially the 40x one) is to accidentlydrag it through oil. This can be avoided by never rotating the lens turret after you have the oilin place and by using only the oil lens (l00x objective) on oiled slides. This lens, by the way,has a black ring around the lens barrel to make it easily distinguishable from the high dry lens(40x). If you must look at an oiled slide with the high dry lens, then lower (focus) the slide awayfrom the lens, blot up the bulk of the oil from the slide with lens tissue and then carefully rotatethe lens turret to bring in the 40x lens. The l0x and 4x objectives should clear any puddle of oil.
You must clean the oil off the oil immersion objective (or any accidently soiled objective) aftereach day’s use. If you leave it on, it will collect dust in the oil making a grinding compound whenyou finally wipe it off. The l00x oil immersion objective is fortunately easy to clean as follows:
Cleaning the oil immersion lens
1. Turn the lens turret so you can get at it.
2. Wipe off the oil as well as possible with dry lens tissue (lens tissue only -please).
3. Slightly dampen a clean piece of lens tissue with lens cleaning fluid andgently wipe lens with this. You might finish with another dry wipe. It isexceedingly important that you do not use an excess of lens cleaning fluid

21
Illumination of the Light MicroscopeImproper illumination of a microscope generally causes the greatest amount of difficultyencountered in the use of this instrument (dirty lenses run a close second). In order to properlyilluminate a microscope, it is necessary to understand that the function of a condenser is to focusthe light on the specimen in such a manner that the specimen acts as the source of illumination.The iris diaphragm of the condenser serves to eliminate stray light, not to reduce intensity!
The Olympus CH is relatively noncritical in its illumination, but the following procedure willinsure that you are getting the best possible image:
1. Focus on a specimen with the 4x l0x or 40x objective.
2. Focus the condenser on the light source.
Focus the condenser up and down until you see the sharpest possible image of the ground
as this can dissolve the cement between the lens elements and thus ruinthe objective.
If you get oil or residue of any kind on your dry lenses (the 40x is particularly susceptibleto this), lens tissue will usually not suffice. All of the dry objectives on your scope are of a specialflat field design (image is flat edge to edge) in which the first lens element is concave . Lens tissuejust glides over the central portion of this type of lens. You can see this with your eyepiece“loupe.” We have found that the dry lenses (especially l0x and 40x) are best cleaned withstyrofoam. We will provide each lab with white styrofoam “peanuts”, the kind used by shippersto pack fragile equipment. You simply break the styrofoam in two and use the freshly exposedfracture face to gently clean your objectives. These surfaces will absorb oil and clean the lensquite nicely if you use a few clean areas of styrofoam. It should not be necessary to use lenscleaner with this method. Do not use the styrofoam method on eyepieces.
Finally, you should never have to clean the lenses or prisms in the interior of your microscope.If you think you have a problem here, call it to the attention of your lab instructor. It shouldn’teven be necessary to clean the inner surface of the lens on your eyepiece, though you may havean occasion to clean the outer surface of your eyepiece lens. If so, first remove the sliding eyecup from the ocular. The cup (more accurately, tube) will not come completely off until you lineup a pin with a keyway - if you twist as you pull, the eye shade will come off. Naturally, youwill use lens tissue on this lens as well and if absolutely necessary your tissue may be dampenedwith a small amount of lens cleaner. NEVER use the air jets on the lab benches to blow dirt outof a lens - these air lines are full of oil and will inevitably make matters worse.
THE MICROSCOPE

22
glass diffusing plate (in the light source) superimposed on your focused specimen. Whenyou have accomplished this you should see a grainy field over your specimen. This will beeasy to see if you close the condenser diaphragm as far as it goes. While this is the idealcondenser focus you will want to eliminate the grainy field by defocusing your condenserabove its focal point until the grain disappears.
3. Adust the condenser diaphragm.
Now open the condenser diaphragm wide open. From its open position, slowly close thecondenser diaphragm until it just begins to darken the field. You might want to check youradjustment by removing one of the eyepieces, looking down the tube and insuring that thediaphragm is just beginning to encroach upon the disk of light at the back of the objective.
To insure maximum resolution, this procedure should be repeated for each objective as therequired adjustments are slightly different. This is especially true for the condenser diaphragmsetting. For special purposes you may wish to close the condenser diaphragm more than usualto increase contrast. This will result in some loss of resolution, but can actually help to visualizelow contrast features of the specimen such as fine fibers. To appreciate this effect, examine yourslide of heart muscle (l6A) with the condenser diaphragm wide open. This will produce light flarethat degrades specimen contrast, making it difficult to see the striations and intercalated disksof this tissue. Now slowly close the diaphragm. You will notice an increase in contrast that makesthe muscle striations and intercalated disks quite easy to see.
The Use of the Oil Immersion ObjectiveThe 100x objective, and only this objective, must be used with immersion oil. This objective isclearly marked with a black ring around it. Failure to use immersion oil with this objective willresult in substantially less resolution than with the dry 40x objective.
Never begin studying a slide with the 100x objective. The small field of view of this lens willmake the location of areas of interest in your slide very difficult. Always start your study witha lower power objective and work your way up in power as you focus your attention on detailsof interest. If you find that the magnification and resolution of the high dry lens (40x objective)is inadequate for resolving the required detail in a particular field, then, and only then, go to oil.
Assuming you have a field of interest in focus under the 40x objective, check to see that yourpre-focusing lever is set so as to prevent further upward travel of the stage with the coarse focus.This lever is just medial to the coarse focusing knob on the side opposite the light switch. Toset this lever, simply loosen it and retighten it. When correctly set, this will allow you to quicklyfind focus under oil without risk of running the 100x objective into the coverglass. The condensershould now be focused at its uppermost position.
Lower the stage as far as it will go with the coarse focus and turn the lens turret so that theobjective lenses are out of the way for the application of the oil to the slide. Then, carefully applyone small drop of oil to the coverslip over the area of interest illuminated by the condenser. Tryto avoid making bubbles in the oil as this can greatly reduce resolution.
Turn the turret to put the 100x objective in viewing position and slowly focus the stage upwith the coarse focus until it comes to a stop at the position previously set by your pre-focuslever. Look through the eyepieces and cautiously make any necessary fine focusing adjustmentswith the fine focusing knob to get the sharpest image.
Finally, remove an eyepiece and look down the body tube of the microscope. Adjust the
THE MICROSCOPE

23
condenser diaphragm so that it is just outside the field of the objective aperture. If you haveany bubbles in the oil, they will be easily seen (with the eyepiece removed) as refractile spheres.Noticeable bubbles should be removed from the oil as they can seriously degrade resolution.Bubbles can be removed by lowering the stage and gently sweeping the surface of the oil dropleton both the slide and the objective with a wisp of lens tissue. It is important to clean the oil offthe objective before you put the scope away (explained in next section). Also, wipe the oil offthe slide unless it is a blood smear with no coverslip.
The Dual-View Teaching HeadTwo students sharing a set of slides will typically share a single dual-view teaching head. Thisequipment consists of a dual body-tube (looks like rectangular boxes on either end of a 10" longtube), a special binocular head with dual focusing eyepieces, an Olympus electrical transformer(model TDO) and a pointer light/socket assembly with electrical cord (may already be attachedto the dual body-tube). Remove any plastic covers from the dual body-tube assembly and savethem with the bag or box for repacking when you turn it in.
Install the dual body-tube as follows:
1. Remove the binocular head from one of your microscopes by loosening the largeknurled knob.
2. Carefully place the end of the dual-body tube with the protruding black "joy-sticks"on the opening where you removed the binocular head (note that the silver label nextto the longer black joy-stick must be right side up for this assembly to fit properly).Orient the tube so that it extends out over the arm of the microscope (the part you grabwhen you pick up the microscope) and tighten the knurled metal knob to attach thedual-body tube to the microscope (you may need to tilt the assembly to get it seatedproperly before you tighten the knob).
3. Place the binocular head you removed (it should have only one focusing eyepiece)on top of the dual-body tube and tighten the knob on the dual-body tube to securethe head in place.
4. Slide the small beige plastic "kick-stand" on the dual-body tube so that it wedgesbetween the tube and the microscope arm (this is important because it relievesstrain on the body tube). We discourage orienting the dual-body tube in adirection that does not permit this support.
5. Attach the special binocular head with two focussing eyepieces to the other end ofthe dual-body tube.
6. Insert the bulb/socket assembly into the hole on the side of the dual-body tube (atthe end with the black joy-stick) and plug the other end of the wire into the back ofthe transformer.
THE MICROSCOPE

24
Proper Use of the dual teaching head
1. Place the scope with teaching head either on one of the center tables or on thepull-out "bread board" between adjacent carrels.
2. The binocular heads should ideally be facing away from one another so that bothobservers are face to face (this will ensure that each observer sees the same fieldin the same orientation).
3. The host (person operating the controls on the side of the tube to which themicroscope is directly attached) should focus on a slide with the nonfocusingeyepiece then adjust the focusing eyepiece on the same field.
4. The partner should then focus both eyepieces on the other end of the dual-bodytube so that this same field is in focus (no further adjustment should be necessaryby the partner as the host focuses on slides).
5. The pointer transformer should be plugged in and adjusted to low, medium or highlight intensity as desired. The pointer should be visible to both host and partnerin the same orientation. The color of the pointer can be changed between red andgreen using the black plastic slide near the long joy-stick. If the light does notlight, first check that the transformer is plugged in. If the pointer still doesn't lightup when you move the joy-stick about, then pull the pointer light out of its socket(follow the wire to the microscope) after loosening the set screw on the lightsocket. New lamps are available in the supply room (see your instructor).
6. Both host and partner can move the pointer. The host pointer is the longer of thetwo black joy-sticks. The partner may use the short joy-stick that protrudes at anangle from the host end of the dual-body tube. Both should find all controls,including the main focus and mechanical stage, to be easily accessible.
7. To avoid wear and damage, leave the dual viewing apparatus on the microscopethroughout the semester (unless you do not wish to use it all). You will find thatthe microscope with its teaching head will fit in your carrel locker if you merelyturn the two binocular heads 180 degrees so that their eyepieces are close to eachother.
THE MICROSCOPE

25
Histology is the study of tissues, but no intelligent study of tissues can be made without at leasta basic knowledge of the cells of which tissues are comprised. Although there are many typesof cells unique to each organ (and these will be considered as the various organ systems arestudied), you will benefit at this stage by a brief consideration of the structure of cells in general.You will be studying cells as imaged in the light microscope, as well as in the transmission andscanning electron microscopes. In most cases you will be looking at sections through cells andtissues; however, there are a few exceptions. Slide 57B , for example, contains whole HeLa cellsin culture. Scanning electron micrographs also generally show whole cells rather than sections.
It is not always easy for a beginning student in histology to discern even such basicstructures as the nucleus , nucleolus and cytoplasm. This may be a good place for you to start.Pick any slide from your slide boxes and first familiarize yourself with what is cellular and whatis extracellular, (i.e., connective tissue and ground substance), and then finally what is nucleus,nucleolus (not always visible), and cytoplasm. Look through the electron micrographs availableto you (including, of course, your textbook) and study these same basic features. Don’t dismissthis as too obvious until you have tried a variety of samples.
Basophilic vs. AcidophilicThroughout this course cells will be frequently described as being basophilic or acidophilic withregard to the cytoplasm as stained by hematoxylin and eosin respectively. If you have notalready done so, you might read through the sections of this lab guide on Histologic Stains ,particularly under hematoxylin and eosin (H & E). Generally, acidic groups bind basic stains(like hematoxylin) and basic groups bind acidic stains (like eosin). Cellular basophilia usuallyindicates the presence of the RNA-containing free ribosomes or ribosomes in association withendoplasmic reticulum (rough endoplasmic reticulum). A high ribosome content generallytypifies a cell that is actively engaged in protein synthesis. Look at the section of pancreas onslide l2B. Pancreatic acinar cells often appear to be arranged in circular groups, much like thepieces of a pie. These cells exhibit basophilia, i.e., the acidic RNA stains with the basichematoxylin dye (bluish) in the region where ribosomes are concentrated around and below thenucleus. The area of the cell oriented toward the center of the circle is filled with secretiongranules; these granules are eosinophilic. Other cells associated with the duct system of thisgland will be distinctly nonbasophilic and are almost colorless.
If rough endoplasmic reticulum predominates, this usually indicates a cell which is synthe-sizing proteins for export out of the cell; conversely, if free ribosomes (polyribosomes in thecytoplasm but not associated with membranes of endoplasmic reticulum) predominate, theproteins are generally kept within the cell. Look through the electron micrograph (EM) collectionand determine for yourself if this is a good “rule of thumb.” See if you can find an EM of a plasmacell in your textbook. This is a basophilic cell; are the ribosomes free or bound to the endoplasmicreticulum? Does this fit our “rule of thumb”? Why? Ribosomes, by the way, are often confusedwith glycogen in electron micrographs; in particular polyribosomes are often confused withalpha glycogen. Your EM collection will provide examples of cells with glycogen andpolyribosomes; learn to distinguish these by differences in size, staining, and aggregation ofthe particles.
It should be pointed out that the nucleolus and the chromatin in the nucleus generally arebasophilic. Why? Some extracellular material is also basophilic (look at the cartilage “models”of bones in the foot of a human embryo on slide 57A). These cartilaginous “bones” stain soblue with the hematoxylin that you can see them clearly on the slide with the unaided eye. This
The Cell

26
is due to the glycosaminoglycans in cartilage which contain strongly acidic sulfate groups.
Membranous Structures in the CellWhen you look at EMs, you will soon realize that nearly everything you see consists ofmembranes, filaments or granules. Most of the organelles of the cell are largely membranousstructures. Membranes as such are not visible in the light microscope, being generally in therange of 7-l0 nm thick whereas the resolution of the light microscope is only 200 nm. You cansee where the border of the nucleus is in the light microscope, but you cannot see the membranesof the nuclear envelope. Study the nuclear envelope (a double layer of membranes) in EMs. Canyou find nuclear pores? Notice that the chromatin, which generally tends to adhere to thenucleoplasmic side of the nuclear envelope, is usually lacking wherever there is a nuclear pore.The nuclear membrane appears to fold back on itself around each nuclear pore. Ribosomes areusually attached to the cytoplasmic side of the nuclear envelope, but not to the nucleoplasmicside. Occasionally you may see a continuity of the endoplasmic reticulum with the nuclearenvelope. Nuclear pores probably function as channels for the passage of materials such asmessenger RNA, ribosomal subunits, etc., between nucleus and cytoplasm during interphase(i.e., when the cell is not dividing).
You will notice that in EMs of any membranous structure, the membrane may vary insharpness and apparent thickness from place to place. This is due to the plane of section; bearin mind that while the membrane is only about l0 nm thick, the thickness of the section you arelooking at is generally between 60 and l00 nm thick. If a membrane is oblique to the plane of thesection, it will appear thicker and very blurred. Look through the EMs; you will find abundantexamples of this in the plasma membrane, nuclear envelope and endoplasmic reticulummembrane. Occasionally, you will find a portion of membrane that is cut virtually parallel to theplane of section and appears as a broad sheet.
The cell membrane itself (plasma membrane) has a number of interesting specializations thatyou will encounter in your studies. If you look at EMs of closely packed cells, you will noticethat their plasma membranes rarely actually touch one another. There is generally an interveningspace no less than l5-20 nm. This space results at least in part from the presence of glycoproteinsand polysaccharides called the glycocalyx. Such coats may have antigenic properties, as wellas other roles in relation to the micro-environment around each cell. In some cells (i.e., on theapical ends of absorptive cells of the intestine), this glycocalyx is very highly developed. Theglycocalyx is part of the plasma membrane, in contrast to a layer of basal lamina (to be describedlater) which is not considered to be an integral structure of the plasmalemma.
Membrane JunctionsThe cells of a tissue, particularly those of an epithelium, tend to adhere to one another, bothselectively and tenaciously. While the glycocalyx is not easily seen, there are visible attachmentstructures including desmosomes, gap junctions, tight junctions, and apical junctional complexes(combination of different junctions). Only at tight junctions do the cell membranes actuallytouch, often becoming fused in those areas. Your EM collection of cell organelles will help youget started in discerning these junctional structures. These specialized cell junctions are eitherat the limit of or below the resolution of the light microscope, though evidence of their existencemay be seen in some epithelial tissues. In the epidermis of the skin, for example, there is a layerof cells called the spinous layer (so called because of the spiny shape of the epidermal cells).
THE CELL

27
The spiny shape results from shrinkage artifact in the histological technique. When theindividual cells shrink, they continue to “hang on” to one another at many points on each cellby means of the desmosomes, thereby producing the spiny appearance. Look at the epidermison slide 7A with either your 40x or 100x (oil) objective.
MicrovilliMany cells have, to a greater or lesser extent, small finger-like membrane bound cytoplasmicprocesses extending from the surface of the cell which apparently serve to amplify its surfacearea. These structures, called microvilli, are particularly abundant on absorptive cells such asthose in the small intestine and proximal convoluted tubules of the kidney. Very long specializedmicrovilli can be seen lining the lumen of the epididymis of the testis (54B). Look at the slidewith the unaided eye; you will see a large blue circular field that is the testis proper, and on oneside of this you will see a smaller red circular field. It is this field that will have the cross sectionsof the ducts, which are lined with long microvilli. These microvilli of the epididymis are calledstereocilia (non-motile cilia), but are actually not cilia.
CiliaTrue cilia are motile structures that can be seen lining the irregular lumen of the oviduct (88B).Cross sections of cilia in the EMs will be particularly useful in studying the interesting finestructure of the cilium. Unlike microvilli, cilia have a core of microtubules in a “9+2” arrangement.Flagella are similar in structure to cilia, but they are longer and usually there is no more thanone per cell. The best example of flagella can be found on the testis slide (54B). The luminaof the epididymis contain flagellated spermatozoa. Flagella also have the “9+2” microtubulararrangement. Curiously, many epithelial cells have been found to bear a single flagellum.
Endoplasmic ReticulumThere are two types of endoplasmic reticulum (ER): (l) rough ER and (2) smooth ER. The ERcan be considered a series of potentially interconnected labyrinthine channels runningthroughout the cytoplasm. The rough ER is studded with polyribosomes, which you shouldbe able to see in both cross sections and glancing surface views in appropriate EMs. Thesesurface views often show numerous small clusters of polyribosomes. The ribosomes of eachcluster are in a coiled linear arrangement that is related to one molecule of mRNA, and allowsthe simultaneous production of several polypeptides from one messenger RNA. The flocculent-appearing content of the rough ER represents synthesized protein that has gained access tothe cisternae of the ER, and from here may be carried to the Golgi complex for further processingand/or packaging. Cells in a very active state of protein synthesis will often have greatlydistended rough ER cisternae. Rough ER often has a tendency to occur in packed parallel arrays,while smooth ER has a much more irregular arrangement. Look for this in EMs. Nissl substancein the neuron is a particularly striking example of this. Though most cells have a mixture of roughand smooth ER, those cells producing largely proteins will have predominantly rough ER,whereas those cells producing steroids and with high lipid and cholesterol metabolism will havelargely smooth ER. Smooth ER lacks ribosomes, rarely occurs in the long flattened cisternaetypical of rough ER, and is more likely to be found forming continuous and discontinuouscontacts with the Golgi complex. You will find several examples of smooth (agranular) ER in yourEM collection.
THE CELL

28
GolgiIdentification of the membranous organelle known as the Golgi complex frequently gives thebeginning student trouble. The Golgi complex is big enough to be seen easily in the lightmicroscope, but unfortunately it resists being stained with nearly every dye and can bedemonstrated convincingly only with a special silver “stain”. One can, with experience, takeadvantage of its chromophobic nature and discern the Golgi zone as a clear or negative imagein many stained sections of cells. The Golgi will appear as a clear zone next to the nucleus. Evenin the EM it takes some experience to quickly find the Golgi complex. The EM collections andyour textbook should be helpful in this regard. The Golgi resembles smooth ER, but unlike thesmooth ER, its agranular membranous cisternae are stacked in closely associated layers. Thesestacks are often curved and close to the nucleus, and occasionally, even in a “pocket” indentedinto the side of the nucleus. Many cells, particularly those of a simple epithelium, have a polaritythat is often indicated by the position of the Golgi in the cell. The Golgi apparatus will usuallybe on the side of the nucleus toward that end of the cell from which the secretory products leave.
MitochondriaOne of the most striking of the membranous organelles of the cell is the mitochondrion. Thoughmitochondria are within the resolution of the light microscope, they are not usually stained incommon histological preparations. The iron hematoxylin-stained section of stomach (80A) doesshow mitochondria as small granular or rod-shaped structures in the parietal cells. Of the twosections on slide 80A, look at the black one. Look for cells arranged in rows. You will see twotypes of cells in these rows: white foamy-looking cells and grey-looking cells. The latter are theparietal cells containing the black-staining mitochondria. If the cytoplasm contains a highproportion of mitochondria and few ribosomes, the cytoplasm often stains with an acid dyeprimarily because of the mitochondria.
In the EMs, mitochondria can be seen to have a highly characteristic structural organizationand frequently have a characteristic size, morphology and location for a particular tissue. Thisfact will help you later to identify tissue in EMs, as well as understand the cellular physiologyof the tissues. For now, it will be helpful to look at a wide variety of EMs and learn to identifymitochondria, paying particular attention to their variations in morphology. Whereas mostmitochondria have lamellar-shaped cristae , those of steroid-secreting cells often have tubularcristae; your EM collection has an example of such a cell. Cardiac muscle mitochondria oftenhave cristae that are angular. In some cells (e.g., liver), the matrix of the mitochondrion is verydark. In many cells most mitochondria will occupy a particular position in the cell. For example,in some secretory and absorptive cells, the mitochondria are sandwiched between the folds ofa greatly infolded basal cell membrane. You will encounter examples of this when you study theproximal tubules of the kidney and the striated ducts of salivary glands. You might want to glanceat these in your textbook now.
Vesicles and vacuolesIn EMs most cells contain a variety of essentially round vacuoles or vesicles. These may formby an inpocketing of the plasma membrane or by budding off from other membranous organelleswithin the cell. Large invaginations of the surface of the cell often result in the uptake ofparticulate matter from the exterior (phagocytosis). In many cases, cytoplasmic processes (calledpseudopodia) extend out from the cell surface and surround particulate material in the
THE CELL

29
extracellular environment. The vacuoles formed as a result of phagocytosis are calledphagosomes. Invaginations at the surface of cells that imbibe fluid, participate in a type ofendocytosis called pinocytosis or micropinocytosis, thereby producing pinocytotic vesicles.The reverse of this process of pinocytosis, where vesicles fuse with the cell membrane and losetheir contents to the exterior of the cell, is called exocytosis. Such a process takes place in allsecretory cells in which the secretory product resides in vesicles which are derived from the Golgicomplex. A special type of micropinocytosis involves coated vesicles. The area of theinvaginating cell membrane is unusually thick, due to additional material (clathrin) on thecytoplasmic side of the cell membrane. Proteins in the exterior environment of the cell appearto selectively bind to the cell membrane at these coated portions of the cell membrane, and aresubsequently taken into the cell by micropinocytosis. Examples of coated vesicles can be foundin the EM collection.
LysosomesThe lysosome is a membrane-bounded vesicle in the cell which contains a number of hydrolyticenzymes active at an acid pH. This organelle has received considerable attention in recent yearsas a result of the interest in storage diseases. Lysosomes are electron dense, membrane-bounded structures about the size of the narrowest dimension of a mitochondrion. Theyoriginate as separate structures in the region of the Golgi complex. Lysosomes can fuse withthe phagosomes to form a phagolysosome or, as it is often called, a digestive vacuole. Lysosomescan also fuse with vacuoles containing organelles of the same cell, an autolysosome orautophagic vacuole. Both phagolysosomes and autolysosomes show evidence of membranous“debris” within them. In this way, the cell (by means of lysosomes) can digest both materialsbrought into the cell from outside as well as endogenous materials and effete organelles withinthe cell. Many examples of lysosomes and digestive vacuoles will be found in your study ofEMs. Occasionally, cells will accumulate indigestible material within a vacuole, which is thencalled a residual body. This indigestible material often includes the so called “myelin figures,”which look like rolled up membranes. Granules in neutrophils and eosinophils of the blood havebeen shown to be lysosomes. Those of the acidophilic leukocyte in particular are of sufficientsize, number and staining quality to be easily seen with the light microscope.
Filamentous and Tubular OrganellesAll cells contain various classes of fibrillar organelles, but you may not always see them in aparticular plane of section. The three main types in order of increasing diameter are microfilaments,intermediate filaments, and microtubules. These organelles are of indefinite length and, ingeneral, appear to participate in various types of mechanical activity within cells (such aslocomotion, particle transport, cytokinesis, chromosome movement and structural rigidity).
Microfilaments are about 5 nm in diameter, and often occur in skeins or bundles near theplasmalemma. They are similar, if not identical, to the actin filaments found in muscle cells. Thedrug cytochalasin B interferes with the operation of several mechanochemical processes thatappear to be dependent upon microfilaments. Cells treated with cytochalasin B fail to undergocytokinesis, and cell locomotion is reversibly inhibited.
Intermediate filaments are about l0 nm in diameter and usually occur singly or in loose tangles.They are prominent in neurons (neurofilaments) but can also be found in most other cells. Theircomposition in cells of different types is being investigated. Although they may appear similar
THE CELL

30
morphologically in different cell types, their chemical composition varies. Their functionincludes a mechanical-structural role as is indicated by the great abundance in the epidermis.
Microtubules are tubular structures of indefinite length, are remarkably straight, and measureabout 24 nm in diameter. Microtubules are generally surrounded by a zone of low electrondensity, free of ribosomes and other organelles. Microtubules are composed of the protein,tubulin, a dimer with a MW of ll0,000. The tubulin monomers (MW, 55,000) are about 5 nm indiameter. Thirteen subunits are arranged in a ring to form the cross section of the microtubule.Drugs such as colchicine and vinblastine block many microtubule-dependent processes bybinding to the tubulin dimers and preventing their assembly into microtubules. In addition totheir role in the movement of cilia and flagella, microtubules have been implicated in a varietyof other mechanical processes such as chromosome movement, transport of cytoplasmicorganelles and axoplasmic flow. Microtubules also serve a mechanical function as a sort ofcytoskeleton. The maintenance of the biconcave shape of some red blood cells, for example,is due in part to a ring of microtubules just under the cell membrane. Examples of microfilamentsand microtubules will be found in your EM collection.
CentriolesThe centriole is an organelle of the cell that consists primarily of microtubules. This curiousorganelle is discussed at length in your textbook. A fortuitous plane of section is required tofind one of these in an EM, as usually, there are not more than two per cell. Your EM collectionincludes a section of a centriole. Centrioles that are related to the bases of cilia are called basalbodies. Some rather oblique sections of basal bodies may be found in your EM collection. Returnto slide 88B,where the basal bodies may be seen as pink staining material just beneath the apicalcell surface.
THE CELL

31
In this laboratory, as in subsequent ones, be sure to examine the slide first by eye to gainfamiliarity with the orientation of the tissue. Then scan the tissue under the lower magnificationlenses. Only when you have found an area of interest should you proceed to the oil immersionlens, and then only if really necessary. If you are not familiar with the use of a light microscope,study the section on “Illumination of the Light Microscope” included in this laboratory manual.
An epithelium is an avascular sheet of contiguous cells (with very little intercellularsubstance), resting upon an extracellular basement membrane. An epithelium may consist ofa single layer of cells (simple epithelium), or may have two or more layers of cells (stratifiedepithelium). An oblique section through an epithelium may give the impression that there aremore layers than actually exist. Also, the presence of lymphocytes among columnar cells oftengives an erroneous impression of a pseudostratified rather than simple epithelium.
Simple EpitheliaSimple epithelia can be divided into four basic types for which there are many representativesin your slide collection. It should be noted that there is continuous gradation from type to type.
Simple Squamous EpitheliumThis type of epithelium comprises a single layer of flat cells in which the nuclei form a prominentbulge in the mid-portion of the free surface of each cell. Mesothelium is the name given to thetype of simple squamous epithelium lining the body cavities. Peritoneum consists of mesothe-lium and a thin layer of connective tissue. Slide 8lA gives a surface view of an unsectioned wholemounted sheet of mesentery with mesothelium on both surfaces of a connective tissue layer.In favorable areas the cells are outlined by a silver deposit. One of the commonest forms of simplesquamous epithelium is the type known as endothelium which lines the heart, blood vesselsand lymphatics (l00A). You should be able to find blood vessels on just about any slide in thecollection - - you might try your hand at identifying the endothelium on a few random slides.
Simple Cuboidal EpitheliaCuboidal - height of each cell is approximately equivalent to its width. In slide l3B,the bestexample is found surrounding the pink stained colloid in the thyroid follicles. Cells may varybetween cuboidal and columnar, depending upon the activity of the gland. In slides 44B and46B, cross sectioned kidney tubules provide an opportunity to compare squamous, cuboidaland tall cuboidal to columnar epithelium. Slide 46B is stained with PAS, which shows thebasement membrane (in red) surrounding each tubule. Study the parietal (or outer) layer ofBowman’s capsule as an example of squamous epithelium.
Simple Columnar epitheliaIn this type of epithelium, cells are taller than wide and often prismatic in shape. Frequently, theremay be a specialization of the apical cell surface where one may find cilia or microvilli. The simplecolumnar absorptive epithelium (which lines the greatly folded inner surface of the intestine),can be seen on slide 86A. Due to the many different planes of section, some areas may appearmulti-layered. In slide 88B,we see an example of the ciliated simple columnar epithelium liningthe uterine tube (oviduct). Stop down the condenser diaphragm to increase contrast in order
Epithelial Tissues

32
to see cilia. Basal bodies may be seen in some areas of the epithelium.
Pseudostratified EpitheliaComprises two or more layers of nuclei in simple columnar epithelium, and gives the appearanceof stratified epithelium. For example, in slide 36B the bases of all cells lining the trachea touchthe basement membrane, but not all the cells reach the surface. These cells are also ciliated.
Stratified EpitheliaThis type of epithelium is characterized by two or more layers of cells, and subdivided into thesquamous, cuboidal or columnar types (depending upon the shape of the surface cells as seenin cross section).
Stratified SquamousIn most cases, the lower layers of stratified squamous epithelium are more cuboidal, or evencolumnar as in skin (7A). In the case of skin, the uppermost squamous cells are cornified anddead. Note the gradual transition from columnar cells in the lower most basal layer to squamousin the superficial cornified layer. The lining of the esophagus (75A) is similar, even though thesuperficial squamous cells are living and contain nuclei. Compare lining epithelium of esophagusand trachea. How is each particularly suited for its function? Slide 83B of vaginal epitheliumis an example of stratified squamous epithelium that may prove confusing to you. Here thesuperficial cells are greatly swollen, and only lightly stained due to the dissolution of greatquantities of glycogen that had occupied these cells.
Stratified CuboidalThe ducts of sweat glands in the skin consist of a two-layered cuboidal epithelium. Slide 7A hasmany highly coiled sweat glands deep in the dermis, near a layer of skeletal muscle. The ductis that portion of the gland extending from the epidermis to the highly coiled secretory portiondeep in the dermis. The relatively straight sweat gland ducts will be occasionally observed incross section when their stratified (i.e., two-layer) nature will be more clearly seen.
Stratified ColumnarExamples of both stratified cuboidal and stratified columnar may be found in the ducts of salivaryglands (7lA). Stratified cuboidal and stratified columnar epithelium typically occur as a transitionbetween a simple epithelium and a stratified squamous epithelium. Does this “rule of thumb”fit the examples you have observed in slides 7A and 71A? Where else in the body might youexpect to find such a transition between a simple epithelium and stratified squamous epithelium?
EPITHELIAL TISSUES

33
TransitionalThis epithelium is limited to the urinary tract and is especially suited for the vast surfaceexpansion that develops in bladder, ureters and upper urethra. When the bladder is relaxed(67B), the epithelium appears multilayered and resembles stratified squamous, but the diagnos-tic superficial cells (called facet cells) are more biscuit-shaped. The facet cells are large polyploidcells that are highly modified to increase their membrane surface, while retaining their ability toserve as an ionic barrier. Several investigators have reported that all of the cells of transitionalepithelium (including the facet cells) are in contact with basement membrane and thus, shouldbe categorized as a type of simple epithelium. While you are on slide 67B, note the mesothelium(simple squamous) that covers the border of the bladder opposite the transitional epithelium.What is this layer called? In the distended bladder the superficial cells are flatter (5lB). Theremay be more than one nucleus per epithelial cell.
EPITHELIAL TISSUES

34

35
Blood
Wright’s Stained Smear of Peripheral Blood
Preparation of slide:
1. Clean slide with 95% alcohol. Slide must be completely dry.
2. Clean finger with 70% alcohol and cotton and allow to dry.
3. Puncture finger with a clean stylet. Wipe away the first drops.
4. Take the clean slide and gently touch it to a small drop of blood so thatthe blood is l-2 mm from right end of slide. Do not touch the slide with thisfinger. Spread drop right away.
5. Place slide on flat surface and hold edges of slide with fingers of your lefthand. Place one end of the spreader slide to the left of the drop of bloodand pull it to the right until it just comes into contact with the blood. Allowthe blood to spread along the end of the spreader slide. Then, with a firm,steady movement and holding the spreader slide at 30° angle, push thespreader slide to the left.
All of this must be done rapidly, before the blood clots. It is important to realize that you arepulling or dragging the blood across the slide -- not pushing it. It is important that the edgeof the slide not pass over the top of the blood, or it will damage the cells.
6. The thickness of the smear will depend upon (l) the angle of spreader slideand (2) the rapidity of the spreading movement. The smaller the angle ofinclination, the thinner the smear will be. The film is thicker if the spread-ing is done rapidly. Thinner smears are preferable.
7. Air-dry before staining.
Staining Method:
1. Place slide on a rack with the blood side up.
2. Add just enough Wright’s stain to cover the surface and allow to standfrom l to 3 minutes, depending on the stain.
3. Add an equal amount of water and blow on surface to mix until a greenishmetallic sheen appears on the top of the stain. Allow to stand 4 or 5minutes. Do not allow this to dry out at the edges; add more buffer ifnecessary.
4. Rinse with distilled water. Be sure to flood the stain from the preparation,
Proper position and angle ofspreader slide relative to bloodspecimen.

36
because pouring it off will cause a precipitate to be found on the smear.Once there, it cannot be washed off.
5. Drain with the thin end of the smear pointed upward.
6. Air dry. Remember, water and immersion oil to not mix.
ExaminationUsing the low and high dry lenses, find a relatively thin area of the smear (i.e., where the red cellsare plentiful but not touching or aggregated). Then switch to the oil immersion objective. Thedetails necessary for adequate assessment of the formed elements in the peripheral blood canonly be seen at this magnification. The oil drop should be placed directly on the smear. Nocoverslip is needed.
Begin by examining the red cells. Normal erythrocytes appear as uniformly sized, smoothcontoured discs (7.2 to 7.9 µm in diameter), with a rim of pink stain (due to hemoglobin) and aclear central area. The clear area represents the thin central portion of the biconcave disc, whichcontains less stained hemoglobin; it normally occupies just a little less than half the cell diameter.
Abnormalities of erythrocytes
. Size (larger than normal, smaller than normal, or nonuniformity)
· Shape
· Staining properties reflecting one or more of the following:
· Shape changes
· Altered hemoglobin concentration and distribution within the cell
· Unusual elements, such as RNA in reticulocytes
· Inclusions
These abnormalities can contribute to the diagnosis of many disease states. Examples of manysuch abnormalities are shown in the Upjohn monograph. It should be noted that trueabnormalities of these red cell parameters typically do not affect 90-l00% of the cells, and thosecells that are abnormal are found roughly evenly distributed on a slide. If you find red cellsuniformly deviant in a field, check other fields to rule out artifact. Artifacts may appear in somepart of nearly every blood film.
Common artifacts in blood smears
· Precipitated stain
BLOOD

37
· Red cell vacuolation, usually central
· Loss of central pallor due to overstaining
· Irregularly occurring abnormally shaped red cells.
PlateletsNext, look for platelets (thrombocytes). These tend to occur in clumps, since contact with glasstriggers aggregation. They appear as small blue bodies (¼ diameter of RBC), with striking redor purple granules. The granules are usually central. There should be roughly one platelet perl0-20 RBC. The platelet content is judged to be adequate or not by this criterion in the routineexamination of a blood smear; an actual platelet count is not routinely done, unlike RBC and WBCcounts. If you look carefully for the presence of the granules and the surrounding bluecytoplasm, you are not likely to mistake precipitated stain for platelets.
LeukocytesLeukocytes are often found towards the edge of the blood film. Begin by identifying examplesof each type of leukocyte. You may not find a basophil. Neutrophils are the easiest to identify.Their granules are fine and inconspicuously stained against a background of pink cytoplasm.The nuclear morphology is not obscured by overlying cytoplasmic granules. Mature neutro-phils have highly segmented nuclei (2-3 lobes) while the bands have horseshoe-shaped nuclei.The drumstick in neutrophils of females represents the “shut off” X chromosome. Not findingit after viewing l00-200 neutrophils is no denial or confirmation of your phenotypic sex.
Sometimes, when the entire blood film is overstained, the neutrophil granules may look darkbrown or black like basophil granules. The small size of the granules, three lobed nuclei, evidenceof overstaing (in RBCs, platelets and neutrophil cytoplasm) and excessively high "basophil"counts, should tip you against erroneous identification.
Eosinophils and BasophilsEosinophils and basophils contain coarse granules, stained bright red-orange and brown-blackrespectively. The granules tend to fill up the cytoplasm and often overlie the nucleus, obscuringtheir bilobed morphology. When you encounter these cells, there is generally no doubt in yourminds as to their identity.
Lymphocytes and MonocytesThe most difficult distinction you will have to make is between lymphocytes and monocytes.Start by finding the classical small round lymphocyte, with its nucleus filling up most of thevolume and only a thin rim of blue cytoplasm. The chromatin is distributed in coarse masses,which confers the typical “clumpy” dark purple staining of the nucleus. Other lymphocytes mayhave more cytoplasm, but the nuclear and cytoplasmic staining will be generally similar to thatof this clearly identifiable small lymphocyte. The large lymphocyte (infrequent in blood) has arelatively less clumped chromatin pattern, but the cytoplasmic features can often differentiateit from a monocyte. The monocyte has more abundant cytoplasm of a grayish-blue cast, andthe nucleus has a relatively finely-dispersed chromatin pattern (which is stained red rather than
BLOOD

38
deep purple). The presence of cytoplasmic vacuoles usually suggests a monocyte, if the nuclearand cytoplasmic appearance fit. A truly “folded” nucleus identifies a monocyte, but both celltypes can show nuclear indentation. Both cell types can have cytoplasmic granules. Monocytegranules are numerous, purple or lilac, and fine (hence hard to see), while lymphocyte granulesare red (azurophilic), few, and coarser.
White Blood Cell DifferentialNow that you can recognize each cell type, classify l00-200 successive WBCs and record theirnumbers in the table provided at the end of this chapter. This means that every WBC in eachrandomly selected field (in a good area) must be included in the count. Do not include brokencells, where either the cytoplasmic or the nuclear membrane has ruptured. Such a count is calledthe “differential count.” An increase in the relative percentage of particular WBC types ischaracteristic of many disease categories.
The specific examination of blood cells is routinely done with special stains (Wright’s andGiemsa). You have performed such an examination. You also need to be able to identify these
cells when they are located within tissues you will be studying under routine H & E staining.For all practical purposes, platelets can’t be seen, and RBCs simply appear as eosinophilic spotsof appropriate size. They can be seen edge on, in stacks or singly, and their shapes can bedeformed when squeezed by other structures. Of the WBCs, only lymphocytes and neutrophilsare seen with frequency. Monocytes are difficult to distinguish from lymphocytes, unless theyshow an unequivocal folded nuclear morphology or cytoplasmic vacuolization. Lymphocytesand neutrophils are easy to spot by their nuclear morphology, regardless of stain. Eosinophilsretain the bright red stain of their granules under H & E; they differ from mast cells by their nuclearmorphology. The similar granules of mast cells are displaced to the side of the nucleus, unlikethe eosinophil granules. Look at slide 27A. Within the arterial lumen, you should be able tosee several examples of lymphocytes and neutrophils among the RBCs.
BLOOD
White Blood Cell Differential Distribution
Cell Type Size:
Microns
PerCent
Neutrophilic bands 10-13 2-10
Neutrophils 9-12 60-70
Eosinophils 10-14 1-3
Basophils 8-10 0.5-1
Lymphocytes 6-10 20-40
Monocytes (saddle
nucleus)
12-15 2-10
Erythrocytes 7.5 ---

39
BLOOD
Study questions on EMs.
l) How can an eosinophilic leukocyte be distinguished from the other granu-locytes?
2) At the LM level, small lymphocytes do not show nucleoli. Does the EMsuggest otherwise?
3) In what ways would you expect the EM of a large lymphocyte to differfrom that of a small one?
4) The Golgi apparatus is situated in a characteristic site in all the WBCs.One of the EM pictures shows this location. Do you know the location?
Your Differential Count
Cell Type Score Expected
Neutrophilicbands
2-10
Neutrophils 60-70
Eosinophils 1-3
Basophils .5-1
Lymphocyte 20-40
Monocytes 2-10
Score 100 leucocytes by making counter marks in the table provided below.Assuming your blood sample is normal, your count should fall in the rangeindicated in the "expected" column.

40

41
Fibrous connective tissue is arbitrarily classified as either loose or dense. Loose connectivetissue is found virtually throughout the body (serving as the “excelsior of life”), while denseconnective tissue is more confined to the capsules, tendons, ligaments and dermis of the body.Both tissues are characterized by abundant collagen fibers and, usually, scattered elastic andreticular fibers. The difference is primarily one of packing density of the constituent fibers.Loose connective tissue is also much more cellular than dense connective tissue, and it isthrough the ground substance in the interstices of its fibers that water, salts, gases and variousmetabolites freely diffuse. Dense connective tissue serves more of a mechanical function thana diffusional one. Examine slide 8A of skin with your lowest power objective to appreciate thedifference between dense and loose connective tissue. Just deep to the stratified squamousepithelium (epidermis) is a layer of eosinophilic loose connective tissue (papillary dermis) anddeep to this is a thicker, denser and less cellular layer of irregular dense connective tissue(reticular dermis). Within the dermis you will see cross sections of numerous glands and hairfollicles; all of these are invested in a layer of loose connective tissue. Can you think of anyreasons for this mixture of dense and loose connective tissue? Deep to the dermis is a fatty layer(hypodermis) that is known as an adipose connective tissue, but is really a special case of looseconnective tissue.
Loose Connective TissueSlide 39A is a whole mount of loose connective tissue (perhaps fascia) that has been teasedout on a slide, and stained with H & E and Weigert’s resorcin-fuchsin for elastin. The looselytangled collagen fibers are eosinophilic. In contrast, the dark purple elastic fibers are straightand branching and appear to be under tension in this teased specimen. These elastic fibers donot stain well in the typical H & E section and, thus, are usually not obvious in sections. Thetissue is very cellular, but cytological detail is not very good in a whole mount of this type.
Slide 83B from the vagina provides an excellent opportunity to see the loose fibrousarchitecture of sectioned loose connective tissue. Look just deep to the stratified squamousepithelium. The rich cellularity of this connective tissue contrasts sharply with denseconnective tissue. The most abundant cell is the fibroblast with its elongate nucleus and veryelongate (though indistinct) cytoplasm. Numerous lymphocytes are also in evidence with smalldark round nuclei and no visible cytoplasm. Plasma cells are much less common, but shouldbe easy to identify. They are among the largest cells in the connective tissue, with a round tooval nucleus having a distinctive “clock face” chromatin pattern. The nucleus is typicallyeccentrically placed in an abundant basophilic cytoplasm. Mast cells are not numerous in thispreparation, but stand out quite well with their distinctive small red cytoplasmic granules. Themast cell nucleus is similar to the plasma cell nucleus, but is usually more centrally-placed in thecell. Macrophages can be very large irregularly shaped cells, but are not always easy to identify,unless the cytoplasm contains ingested material which appears as irregular eosinophilicgranules.
Now look at 88A of small intestine. Loose connective tissue forms much of the wall of thegut; however, do not confuse the collagen with the brighter red staining smooth muscle cellsin the gut wall. You should find all of the cell types previously mentioned. Mast cells areparticularly abundant in the gut and often appear close to blood vessels. In many preparations(particularly paraffin sections), mast cell granules are often lost or dissolved in the commonhistological fixatives making them difficult to identify. In these 1.5 µm thick plastic sections thegranules have lost heparin, but have retained histamine and are thus eosinophilic.
Fibrous Connective Tissue

42
Reticular Connective TissueThis is another special case of loose connective tissue. Reticular tissue is characteristic oflymphoid and hematopoietic organs and can be seen in slide 43A of the spleen (where thereticular fibers have been stained black with silver). Reticular fibers are a type of collagen andcan only be identified in sections, with certainty, after special silver techniques.
Adipose TissueA specialized type of loose connective tissue that is widespread in the body. Plastic sectionsof unilocular (common/yellow) adipose tissue (100A) show a dense-packing of bubble-like fatcells (adipocytes) in a scant loose connective tissue stroma. The adipocytes consist of a largeleached-out lipid droplet which has pushed aside the nucleus, and compressed the cytoplasmto a very thin periphery. Can you distinguish the adipocyte nuclei from nuclei of endothelialand fibroblast cells? The large framework into which the fat cells are packed consists of denseirregular connective tissue septa carrying muscular arteries, other blood vessels and myelinatednerves. A set of finer partitions extend out from these septa in the form of a rich network ofcapillaries and reticular fibers (not stained in this preparation).
Dense Connective TissueDense connective tissue is of two types: irregular dense connective tissue and regular denseconnective tissue. The former is found in the dermis and organ capsules; the latter in ligamentsand tendons. In regular dense connective tissue, the collagen fibers are tightly packed and allare oriented in approximately the same direction; in irregular dense connective tissue, there oftenappears to be no special organization of the fibers (In fact, the fibers are often highly organizedin “irregular” dense connective tissue as well, but are woven in a complex way that influencesthe important anisotropic biomechanical properties of the tissue).
Dense Regular Connective TissueIn dense regular connective tissue (such as ligaments and tendons), the only cellular elements(fibroblasts), are highly flattened, lying in interrupted rows between the fibers. The cytoplasmis scanty and attenuated so that only the nuclei are visible. In longitudinal section, the nucleiare plate-like, whereas when they have been transversely sectioned they are oval. Examineplastic section 49A in which small amounts of cytoplasm may be seen adjacent to the nuclei ofthe tendon fibroblasts. Slide 10A shows a tendon in a musculotendinous junctions. Most ofthe tissue is muscle, with thin bands of tendon attached in several areas, especially at the taperingend of the tissue. The muscle is slightly pinker than the collagen, and the nuclei of muscle anddense regular connective tissue differ in shape. Try to visualize the cross striations of muscleby closing the iris diaphragm of the condenser. Compare this section with slide 12A of skeletalmuscle. Ligaments can be seen connecting the bones of the knee joint in slide 60A (This slideis diagrammed in the section on “Cartilage”). You may find separating the different types ofconnective tissue difficult in this preparation until you gain some familiarity with cartilage,
FIBROUS CONNECTIVE TISSUE

43
fibrocartilage and bone.
Irregular Dense Connective TissueExamples of irregular dense connective tissue may be found in any slide of skin (1A) byexamining the dermis, and in the capsule of the testis on slide 54B. This type of connective tissueis more cellular than regular dense connective tissue but much less cellular than looseconnective tissue. There are two sections on most specimens of slide 1A. One section is stainedwith H & E and the other is stained with aldehyde-fuchsin, fast green and orange G. In the latterpreparation, elastin fibers are stained purple by the aldehyde-fuchsin, collagen fibers are stainedby the fast green (as usual) and also orange G (thus, collagen may be green or yellow). Comparingthese two sections will show you how unnoticeable elastic fibers can be if they are not speciallystained. The blood vessels have been injected with red carmine. Again, portions of the dermisare loose connective tissue but the bulk of the dermis is dense.
Embryonic Connective TissueThis type of tissue (found in embryos), is also called mesenchyme, and develops from mesodermand neural crest ectoderm. Many examples of this type of tissue can be found in slide 55A ofthe fetal thorax. These stellate-shaped cells are enmeshed in very fine and scattered collagenfibers together with extensive ground substance. The mesenchymal cells are particularlyevident in the developing kidney and just deep to the epidermis in this specimen. Mucousconnective tissue is similar to mesenchyme, but the ground substance is more abundant andthe fibrous component even less obvious. One of the few examples in the body is the Wharton’sjelly of the umbilical cord (slide 96B), which helps to keep the umbilical vessels from beingpinched off.
Electron MicrographsThe fine structure of fibroblasts and collagen is illustrated in the notebook of electronmicrographs, as is that of tissue macrophages. What are two striking characteristics of sucha macrophage? Which peripheral blood granulocyte does the mast cell resemble? Osteocytes,osteoclasts, and osteoblasts are shown in a light photomicrograph included in the notebook.
FIBROUS CONNECTIVE TISSUE

44

45
Hyaline CartilageCartilage is generally classified by the amount and type of its fiber content. The most ubiquitoustype is hyaline, in which the collagen and elastic fiber content of the matrix is insufficient to giveit a fibrous appearance in ordinary preparations. Start your examination of this type of cartilagewith slide 56A of the ribs of a stillborn. Ignore (for now) the bony ribs, and study only the costalcartilages. The two costal cartilages on the slide are large greenish-blue elliptical areas as seenby eye. In this slide (as for others), examine by eye first, and then study at low magnificationbefore using high dry lens.
In young cartilage, the chondrocytes are small and close together, but do not cluster ingroups. In growing cartilage, there is a gradation from small closely-packed cells in the area ofappositional growth beneath the perichondrium (dense fibrous connective tissue), to the olderand larger cells in the center of the cartilage. In older cartilage, the chondrocytes and their lacunaeare larger and typically tend to cluster in isogenous nests . The cells of these nests are daughtercells, and reflect interstitial growth.
The fetal foot (57A), and knee joint (60A) (see diagram of 60A at the end of this section),show excellent examples of hyaline cartilage with all stages of chondrocyte maturation.Articular cartilages are also hyaline (as can be seen in these slides), but are unusual becausethey lack a perichondrium. Slide l8A of the bronchi shows the more intense staining of thechondroitin sulfate immediately surrounding the individual lacunae; this is referred to as thecapsule. You can spot the location of the cartilage by eye by finding the areas of darkest stainingon the slide. The presence of the sulfated mucopolysaccharide in cartilage ground substanceis responsible for the staining with hematoxylin or basic dyes; the ground substance is thereforesaid to be basophilic. Aldehyde fuchsin is not specific for chondroitin sulfate or elastin, butfor the sulfate or disulfide moieties in these substances.
Elastic CartilageElastic cartilage is not widely distributed, but is important for its flexibility in the external earand epiglottis. Slide 33B of epiglottis shows the elastic fibers of this elastic cartilage particularlywell. You will notice a broad lamina of lipid containing cells in the center of this cartilage, crossedby strands of collagen (red) and elastic fibers (black). A lipid filled center is common in elasticcartilage plates (such as the ear and epiglottis), and may contribute to the mechanical propertiesof these structures. Without a special stain for elastin, elastic cartilage may be difficult todistinguish from hyalin cartilage.
FibrocartilageFibrocartilage may be difficult to discern in histological sections, since it resembles densefibrous connective tissue. There is no perichondrium. The major clue to its identification is thepresence of lacunae and capsules around the chondrocytes. The presence of these lacunaeindicates that the matrix is cartilaginous. In slides 5lA and 52A of the intervertebral disc,fibrocartilage joins the ends of adjacent vertebrae. This band of fibrocartilage (annulus fibrosus)encloses a cavity filled with gelatinous material (nucleus pulposus). In slide 60A the ligamentor tendon inserts into the bone via fibrocartilage.
A unique feature of cartilage is that it is not vascularized, and yet in slide 57A you will find
Cartilage

46
blood vessels which have invaded this cartilage. These vessels occupy areas that will soonbecome centers of ossification as the cartilage is replaced by highly vascularized bone. Youshould also have noticed that bone stains a very different color than cartilage.
Electron MicrographsElectron micrographs of cartilage cells may be found in the connective tissue notebook. Theyshow that cartilage cells contain large amounts of glycogen and have a rather distinctiveappearance. Note that the collagen fibrils in cartilage matrix are extremely fine. How does thecollagen of cartilage differ chemically from that of, say, the dermis or bone?
CARTILAGE

47
Bone
Ground Bone PreparationsSlide 59A is a specimen of ground dried bone, and is particularly good for demonstrating theinorganic matrix. This is a rather thick piece of bone and, thus, should be examined mainly withthe 4x and l0x objective. If you use the 40x objective be very cautious -- the working distancewill be close. It will help you in the examination of this slide if you increase the contrast by closingthe condenser diaphragm a little more than usual. You can identify osteons, lacunae, andcanaliculi within these osteons, as well as the Haversian canals, and an occasional Volkmann’scanal. Note the circumferential arrangement of the lamellae at the periosteal surface of the bone.Using the vernier scale on your mechanical stage (graduated in millimeters) and the pointer inyour eyepiece, calculate the maximum distance you can find between an outermost osteocyteof a circular (cross sectioned) osteon and the center of its Haversian canal. This is probablyclose to the upper limit for metabolite diffusion in the canalicular system of compact bone. Theother preparations which you will examine are sections of decalcified bone. When bone isdemineralized, one is left with mostly collagen; this “bone” stains about the same color as thesurrounding fibrous connective tissue.
Endochondral OssificationMost bones of the body develop first as hyaline cartilage models. These cartilage models areeventually invaded by blood vessels, and calcification of the cartilage quickly follows. Calcifiedcartilage then serves rather like a scaffolding on which true bone matrix and, finally, bone isdeposited. All calcified cartilage is eventually eroded away by osteoclasts. The developmentof the bones of the fetal foot (57A) provide a good example of these stages. With your 4xobjective, you will note that the calcaneus and cuneiform “bones” are still largely or entirelyhyaline cartilage, whereas the metatarsals and phalanges are part bone (red) and part cartilage(blue). One of the first stages in bone formation may be seen in the calcaneus and cuneiform“bones,” where blood vessels may be seen to invade these cartilage models. The lighter colorof the matrix surrounding these vessels is calcified cartilage. There is significant bonedevelopment in the diaphyseal portions of the metatarsals, and most of the phalanges. Theepiphyseal ends are cartilaginous, and the articular surfaces in the joints will remain so in theadult. Some of the phalanges may show an early stage of bone formation as a bone collardevelops around the mid diaphysis of the cartilage model; note that the chondrocytes are veryhypertrophic and vacuolated in this region. Notice how holey and irregular the bone appearscompared to the cartilage. The general mechanism for bone development you have seen in slide57A is called endochondral ossification.
By holding slide 60A up to the light and using your eyepiece as a loupe, you can readilysee the marrow cavity, diaphysis, epiphyseal plate, epiphysis and articular cartilage. Thedrawing of 60A in the previous section will aid you in orienting yourself on this slide. Usingyour microscope, examine the epiphyseal plate and identify the zone of proliferating cartilagecells , maturation zone of hypertrophic cartilage cells and zone of provisional calcification.Identify the periosteum, osteocytes, osteoblasts, osteoclasts , and, if possible, lamellae andHaversian systems. The sequence of maturation during growth in length of a long bone is nicelyexhibited in the epiphyseal and metaphyseal parts. There are rows of chondroblasts, showingprogressive proliferation and maturation in the epiphyseal plate. These chondrocytes becomehypertrophic, and the plates of cartilage between them calcify. Notice the irregular trabeculaeof calcified cartilage (grey) on which bone (red) is being deposited by osteoblasts. Osteoclasts

48
in Howship’s lacunae can usually be seen in relation to the trabeculae proximal to the epiphysealplate. The calcified cartilage matrix may stain intensely with hematoxylin, depending upon thepreparation; if the proteoglycan has been modified during decalcification, there will be littlebasophilic staining. The thin band of uncalcified matrix recently produced by osteoblasts(osteoid), stains with eosin, but to a lesser extent than does the mature bone matrix.
Intramembranous OssificationIn membrane bone formation, first osteoblasts and then bony spicules begin to appear in a regionof mesenchymal tissue without any cartilaginous precursor. Slide 6lA provides an example of“membrane” bone. Here, a lamina (“membrane”) of mesenchymal cells has differentiated intovery basophilic osteoblasts, which have begun to produce bone by a process called intramem-branous ossification. No cartilage model is formed in this type of bone formation. The differentcolors (blue and red) probably reflect a difference in the maturation of the bone matrix. Whatbone do you think this specimen came from? Membrane bone formation is also shown in slide54A of the infant jaw (see diagram on next page for help in orientation).
A modified form of membrane bone formation is called periosteal ossification, because, theosteoblasts are restricted to a region just under the fibroblastic connective tissue of theperiosteum. In this process, osteoblasts appear surrounding a volume of cartilage, and beginto form an enlarging jacket of bone without invading the volume of cartilage (although the lattergenerally breaks down). The connective tissue around the bone-jacketed cartilage changes fromperichondrium to periosteum, since it now contains bone forming cells. In long bones, growthin the length is by the endochondral method through growth and maturation of the epiphysealplate. Circumferential enlargement of the diaphysis, however, is technically a form of membranebone formation. Periosteal ossification can be seen at the periphery of the developing ribs ofa fetus in slide 55A. In this slide, a red basic dye stains cell nuclei and a green acid dye stainsthe bone (collagen). Do not be misled just because the warm color represents the basic dye andthe cool color an acid dye (in contradistinction to hematoxylin and eosin). You can observenormal hyaline cartilage in some developing ribs, but in others the cartilage is being envelopedby forming bone (within the periosteum), and the cartilage cells have begun to swell and die. Alater stage in the development of the ribs may be seen on slide 56A.
BONE

49
BONE

50

51
Skeletal MuscleSlide l0A illustrates the junction of skeletal muscle fibers with tendon. Note the position of thenuclei. What is the actual nature of the junction between tendon and muscle fiber? In slide l3A(a cross-section of dog skeletal muscle), the shape of the individual skeletal muscle fibers isreadily seen. The differential effects of fixation can also be appreciated. Note for example, thedifference in fibers at the periphery, as opposed to those at the middle of the bundle. Since thevessels and nerves of skeletal muscle tend to parallel fiber direction, cross sections of thesestructures are seen in the perimysium. Many of your slides will also have muscle spindles inthis location. If your slide does not have one, look at that of a neighbor. In cross section, youshould be able to recognize the connective tissue capsule and intrafusal fibers of the spindle.The muscle spindle acts as a sensor in the feedback system that serves to maintain muscle tone.While studying slide l3A, compare the skeletal muscle fibers with the smooth muscle cells foundin blood vessels.
The plastic section ( l2A, H & E) of skeletal muscle in longitudinal section shows the in-registerpatterning of myofibrils and also fibers (cells) of the same muscle. In most sections, part of theperimysium septa surrounding groups of fibers can be seen; frequently, the septa, containblood vessels. This specimen allows you to see the various bands of striated muscle. You shouldbe able to see the H and Z bands , as well as A and I bands . The H stands for Hensen’s band (orzone), the light area in the center of the A band. The Z is taken from the German wordZwischensheibe, and is used to denote the band or line (disc) defining the terminal boundariesof the sarcomere (the disc between 2 sarcomeres). The designations A and I refer to the termsanisotropic and isotropic, and are derived from observations made with the polarizing microscope.The A bands appear dark in the light microscope, and correspond to areas in which both actinand myosin filaments run parallel to one another; the I bands are light in appearance, and areregions of the sarcomere adjacent to the Z line containing only actin fibers.
In your electron micrographs, please take note of these more overt cytological features ofstriated skeletal muscle (as well as those structures such as transverse tubules and thesarcoplasmic reticulum that are not visible at the light microscope level, but are essential tomuscle function).
Smooth MuscleSlides 86A (intestine), and 94A (colon) are probably the best preparations in which to observethe shape of smooth muscle fibers. Both smooth and skeletal muscle can be seen on slide 76A;smooth muscle is associated with the trachea cartilage (completing the circle) and, dependingupon the level at which the esophagus was sampled, skeletal muscle may be present in the outerwall of the esophagus. Another good preparation for comparing smooth and striated muscleis slide 99A of the recto-anal junction.
In some regions of this slide, you will see some contracted or partially-contracted smoothmuscle fibers in which the nuclei have assumed a characteristic spiral or corkscrew configuration.This nuclear configuration is one of the criteria that can be used to distinguish smooth musclecells at the light microscope level.
One of the fine structural characteristics of smooth muscle is the presence of numeroussurface invaginations or caveolae. What other features would you use to distinguish smoothmuscle cells from fibroblasts at the electron microscope level? How would you distinguishbetween areas of smooth muscle and dense connective tissue on the same slide?
Muscle

52
Cardiac MuscleSlide l7A (monkey heart) contains portions of both the atrium and ventricle, and may includepart of an atrioventricular valve. The atrial myocardium is thinner and contains more connectivetissue than the ventricle. Look for a place where there is a good cross-section of the cardiacmuscle fibers. Note the centrally-situated nuclei, the irregular curved outlines of the fibers, andvariation in fiber size.
The cardiac muscle plastic sections (slide l6A) are longitudinal sections with occasionalcross-sections, and frequent oblique sections at the edges. That the irregular columns of cells“branch and anastomose” can be seen by carefully following a length of fiber. The cells arejoined end-to-end at the intercalated disk. The richness of the capillary supply is apparent atl0x. At 40x, the one or two central nuclei in their spindle-shaped packet of sarcoplasm (rich ineosinophilic mitochondria) are well seen. Note also that the individual myofibrils are separatedby rows of mitochondria. Many of the longitudinally sectioned nuclei have indented margins.Why? Intercalated disks and the out-of-register sarcomeric banding of myofibrils are obviousat 40x.
At one edge of slide 20A (embedded in the loose connective tissue of the endocardium), arethe Purkinje fibers (cells designed more for conduction than for contraction). They consistof a group of large cells several times the diameter of ordinary myocardial cells. The myofibrilsare sparse and confined to the periphery of the cell. The central region contains the nucleusand cytoplasm, rich in glycogen (not seen in this preparation). The large, basophilic structuresin the myocardium of this slide are sections of parasites.
MUSCLE

53
Peripheral nervous tissue, like that of the central nervous system, is composed of cells activelyinvolved in impulse conduction and neurotransmitter production, and release (neurons) andhelper cells (termed satellite cells if adjacent to neuron cell bodies, and Schwann cells if relatedto axons). Schwann cells are also called neurilemmal cells. Peripheral nerve tissue differs fromcentral nerve tissue because (with the exception of the enteric plexuses), it is interspersed withconnective tissue components, giving it its substantial tensile strength.
Peripheral neurons are generally gathered in aggregates called ganglia. Within ganglia,individual neurons are recognized by their large cell bodies, or perikarya, usually containing alarge vesicular nucleus containing a prominent nucleolus. In the case of autonomic ganglia,these cell bodies will support both dendrites and an axon; in the case of sensory ganglia a singleprocess is dispatched from the soma (which then divides into a peripherally and a centrallydirected axon). You will encounter neuronal perikarya in many of your histology slides in theautonomic ganglia associated with visceral organs.
Slide l8B, of most sets, contains a large ganglion external to the adrenal gland (this is oneof the coeliac ganglia that receives preganglionic input from the splanchnic nerve; it providesadrenergic innervation for the gut and does not innervate the adrenal gland). Note that eachperikaryon is surrounded by encapsulating cells. The innermost of these are the satellite cells .They, in turn, are surrounded by flattened connective tissue cells. To gain a better idea of theactual shape of autonomic neurons, examine slide 93A (which is a magnificent flattened, silver-stained preparation of Auerbach’s plexus). In spite of poor preservation, you can observe thegeneral organization of a spinal ganglion on slide 48A; the nerve cell bodies and their investingsatellite cells have been separated artifactually.
The ganglia contributing to the Myenteric plexus of Auerbach are located between the innercircular and outer longitudinal muscle layers of the alimentary tract (slide 94A). The plasticsection of the intestine (86A) shows these ganglion cells particularly well, and also shows theganglion cells of Meissner’s plexus (located in the connective tissue just inside the musclelayers). Do you see typical satellite cells here?
Most of the nerve trunks that you will encounter in your slides contain large numbers ofmyelinated nerve fibers. See slide 25A (carotid sheath). In a “typical” H & E tissue preparation(e.g., in the perimysium of muscle, slide l3A) you should be able to see axons, myelin sheaths,Schwann cell nuclei, perineurium and epineurium. After standard fixation procedures, theaxon of myelinated peripheral nerves is surrounded only by remnants of myelin sheath, whichhas had its lipids extracted. This remnant material is termed neurokeratin.
Thus, in order to see fine details of nerve trunk structure, you must study your class electronmicrographs. Only here can it be seen that unmyelinated axons are also surrounded by thecytoplasm of a Schwann cell. Note that in contrast to the one-to-one relationship seen in themyelinated nerve fiber-Schwann cell unit, a single Schwann cell may invest several unmyelinatedfibers. Both myelinating and nonmyelinating Schwann cells are surrounded by a basal lamina.The endoneurium consists of the scattered connective tissue cells and fibers (collagen andreticular) which immediately surround the nerve fiber-Schwann cell unit of peripheral nerve.Nerve fibers are grouped or bundled together, and are surrounded by a connective tissue layertermed the perineurium (derived from fibroblasts). Larger and thicker nerves consist of severalperineurium-bound smaller nerves, held together by a coat of connective tissue (termed theepineurium). In nerves containing only one fascicle, the perineurium cannot be distinguishedfrom the epineurium. When peripheral nerve fibers penetrate epithelia, they typically lose theirSchwann cell sheath and basement lamina.
Slide 92A is a Sudan black fat stain of a sensory ganglion in tissue culture containing somemyelinated and many unmyelinated nerve fibers in the outgrowth zone. DO NOT USE OIL ON
Peripheral Nerves

54
THIS SLIDE (40x objective is adequate for viewing). The outgrowth also contains many othercell types (including many phagocytes) scattered over the top of the culture, and underlyinglayers of fibroblasts. The culture was prepared from a single dorsal root ganglion taken froma mouse fetus. No myelin was present at the time of explantation into culture. Several hundredneurons of the ganglion survive in the central mass of tissue, often stained too intensely to see.Sometimes, individual neurons of distinctively different sizes can be maintained in culture.Axons grow outward to form an outgrowth, along with accompanying Schwann cells, prolifer-ating fibroblasts and many phagocytes. The myelin present has formed in culture.
Can you identify in slide 92A:
1. Individual myelin segments (called myelin internodes).
2. The myelin-related Schwann cell nucleus related to each segment. Notethat this is a fat stain and the nucleus is not stained. It appears as avesicular void in the Schwann cell cytoplasm adjacent to the myelin.
3. Nodes of Ranvier between myelin segments.
4. Myelin segments still being formed (found in the more peripheral regions),or (rarely) extremely short myelin segments (called intercalated segments)interposed between myelin segments of normal length.
5. Branching in a myelinated fiber. What happens to the myelin sheathhere?
6. Non-myelinating Schwann cell nuclei related to fascicles of unmyelinatednerve fibers. These are best found in nerve fiber fascicles in the periph-eral regions.
7. Regions in the most peripheral parts of the outgrowth where the axonshave not yet acquired Schwann cell ensheathment and are growing overthe surfaces of very flattened fibroblasts.
8. Fat cells (sometimes present); phagocytes; stress fibers in the fibroblasts atthe culture periphery; satellite cells of neurons (if nerve cells are individu-ally visible).
Before leaving today’s laboratory also review the fine structure of the myoneural junction (seethe muscle set of EMs). In what ways does this structure resemble a synapse terminating onanother neuron? Correlating your knowledge of the peripheral nervous system from GrossAnatomy, the Neuroscience Course and Histology, can you answer the following:
PERIPHERAL NERVES

55
PERIPHERAL NERVES
7. Which ganglion would you culture in order to obtain noradrenergicneurons in a culture preparation?
8. Which neurons of the peripheral nervous system are not related to typicalSchwann cells?
9. How would you expect the histology of the vagus nerve and the phrenicnerve to differ?
10How would you expect the histology of the dorsal and ventral root to differfrom each other and from the standard peripheral nerve trunk?
Integrative questions in neuroanatomy
1. Some Schwann cells form myelin, and others only “loosely” ensheathenon-myelinated axons. Does the axon or the Schwann cell specify thisrelationship?
2. What is the relationship between nerve fiber diameter and myelin inter-node length in vivo? Why does cultured nerve tissue have only very shortmyelin segments?
3. Which ganglionic neurons (sensory, sympathetic, or parasympathetic) aresources of myelinated (as opposed to unmyelinated) nerve fibers?
4. What embryonic structures are the sources of Schwann cells? What cellsform the perineurium?
5. There are several types of axons which are myelinated by both Schwanncells and oligodendrocytes. Where are these located?
6. What neurotransmitters would you expect to find in the neurons of thedorsal root ganglion culture you have examined? How would you demon-strate the presence of a neurotransmitter system in these neurons?

56

57
Arteries and VeinsBegin your study of vessels with the largest elastic artery, the aorta. There should be twosections on your slide of the human aorta (23A). Study the H & OGE section first. All bloodvessels (with the exception of capillaries) are constructed of three main layers or tunics: thetunica intima, the tunica media and the tunica adventitia. These layers stand out distinctly on23A; starting from the lumen, there is a thick (pathologically thick) t. intima containing theendothelial lining, and a significant amount of connective tissue. Surrounding this, there is thet. media which is comprised mainly of circularly-arranged smooth muscle, interspersed withfenestrated laminae of elastin. Surrounding all is the t. adventitia, which is composed of a ratherloose connective tissue with scattered elastic fibers. Large vessels such as these are alsosupplied by blood vessels called the vasa vasorum; these small vessels may be seen in both thet. adventitia and t. media. Why do these vessels extend no deeper into the wall of the aorta thanthe outer t. media? Now, if you look at the other section on slide 23A stained for elastin, youwill see the elastic components of the t. media and t. adventitia quite easily.
Slide 33A of the monkey aorta is a plastic section and shows more cytologic detail. Note thetenuous endothelium and very thin connective tissue layer of the t. intima. The outer most limitof the t. intima is clearly indicated by a wavy pink-stained lamina of elastic tissue (called theinternal elastic membrane). The t. media comprises most of the wall of the artery. You can seethe nuclei of the smooth muscle cells that make up the wall; some run circumferential and somerun longitudinal. The elastic laminae of the media are wavy (why?), and stand out quite well eventhough this is an H & E. The adventitia shows some evidence of the vasa vasorum.
Slide 24A has several muscular arteries and an elastic artery; can you tell the difference? Youwill probably find a vein or two, as well. How might you identify the vein? Slide 27A will servewell for demonstrating the differences between an artery and a vein. Fortunately, arteries andveins usually run in parallel throughout the body, so that when you see one in section youusually see the other (as you do here). In general, veins are distinguished by their deformability,their comparatively thin and indistinctly layered wall, and the presence (in large veins) of valves.In 27A, the vessel with the thicker wall and yet smaller lumen is the artery. Compare the relativethickness and composition of the tunics between these vessels. Slide 25A is nicely stained forelastin. Note the striking difference in the development of the internal elastic membrane betweenthe artery and vein. There are significant differences in the elastic laminae of the t. media as well.
Many of the slides of specific organs provide excellent examples of smaller blood vessels.Slide 82A (pyloro-duodenal junction), for example, contains a wide range of vessel sizes. Youshould be able to find longitudinal sections of arterioles and capillaries in this preparation (Anarteriole has only one or two layers of muscle cells outside the intima). What type of sectionof the individual smooth muscle fibers would you expect to obtain in a cross section of a mediumsized vein? Slides l5B (neck organs) and l00A (adipose tissue) contain blood vessels ofdifferent sizes.
LymphaticsLymphatic vessels can be recognized in most tissues by their relatively large size, irregularshape, and thin wall (which may consist of little more than an endothelium). The small lymphaticvessels can be distinguished in different tissues by their irregular contour and thin walls withattenuated endothelial cells. Nice examples of lymphatic vessels are present in the plasticsections of monkey ovary (68B) and the human ileum (88A); they are readily distinguishable
Cardiovascular System

58
from the blood cell-filled blood vessels in these preparations. They can be found in the dermisin slide 50A of the dog ear. Lacteals are fat-absorbing lymphatic capillaries located in the villiof the small intestine. Lacteals in the collapsed state can be found with difficulty by carefulexamination of slides from the series on the intestine (e.g., slide 9lA of the cat ileum). Lymphaticvessels can also be found in the area of the lymph node in slide l5B of neck organs.
HeartSlide l5A (from the heart of a small mammal) shows a portion of the left ventricle, the left and rightauricles, and segments of the aorta and pulmonary artery between the right and left auricles. Theventricle is covered by a layer of mesothelium and connective tissue, the epicardium. Theendocardium lines the inner surface of the heart. Note its dense layer of connective tissueimmediately below the endothelial cells. A portion of papillary muscle extends into the ventricle.Between these two layers, one can see the arrangement of the myocardial cells. Note thedifference in the thickness of the walls of the right and left auricle. Aortic valves project fromthe inner walls of the aorta. The surface of the valves is covered by endothelial cells. Denseconnective tissue and a few cells which resemble chondrocytes are seen in these valves. Theconnective tissue and “chondroid” (the substance secreted by the chondrocyte-like cells),provide rigidity for the valves.
Slide 16A. Note the distribution of myofibrils, and location of nuclei in the cardiac musclecells. The intercalated discs which join one muscle cell to another are very well preserved in 16A.Note the wavy contour of the discs and the many small blood vessels among the myocardial cells.From what large vessel are they derived?
Slides 20A and 21A demonstrate Purkinje cells . Note their location below the endocardiumin the intraventricular septum. The cells are very easy to distinguish in the section of beef heart.They are shorter and broader than typical cardiac muscle cells, and have fewer myofibrils thanthe typical cardiac muscle cell. Can you find any abnormalities in the structure of the cardiacmuscle cells or in the blood vessels in the section of the human heart?
CARDIOVASCULAR SYSTEM

59
Slides 28A and 32AThis laboratory is intended to familiarize you with the myeloid elements, and to introduce youto the differentiating cells in bone marrow which give rise to cellular elements of the peripheralblood. Identification of the various cell stages depends upon cell size, the size and shape ofthe nucleus, the presence of cytoplasmic basophilia and the number and staining characteristicsof the cytoplasmic granules. The goal of this laboratory is to be able to identify various stagesin the development of erythrocytes and granulocytes on the basis of understanding the changesin differentiation.
Study slide 28A to gain an impression of the organization of marrow in conventionally stainedand sectioned material. Cells are clustered between sinusoids. You will note numerous “holes”in the marrow; what causes this? You might be able to identify some cells, but do not spendmuch time in this endeavor; the marrow stained with Wright’s stain is best for cell identification.Megakaryocytes are very large and may be easily seen in any preparation of marrow.
Slide 29A is a section through an intact plug of dog marrow, which has been separated fromits investing bone. With your 4x objective, note the large central longitudinal vein into whichthe sinusoids drain. Next to this vessel is a large central longitudinal artery and other smallerarteries. Note that the central vascular compartment of the marrow is more fatty, and theperipheral compartment is more hemopoietic. At higher magnification, you can find numerousmegakaryocytes in this hyperplastic marrow. With high dry, you ought to be able to discernsinusoids, fat cells and the reticular cells that (together with reticular fibers), make up the stromaof the marrow. You will be able to discern various stages in the development of granulocytes(neutrophils and eosinophils), but a detailed study of hemopoiesis is much better done onmarrow aspirates or touch preparations.
Most of your laboratory time should be spent looking for examples of different developmentalstages in the red and white blood cell series in the slide of human bone marrow (32A). Thispreparation was made by aspiration, which destroys much of the normal relationships youobserved in sections but gives much better cytological detail. The reticular stroma and fat cellsare either missing or destroyed. Use oil immersion. Do not try to identify every cell youencounter; instead look for good examples of each cell stage. Choose thin areas where cells arenicely spread out for your perusal. It is sometimes helpful to start identifying the more maturestages first and then carefully work your way back through the more immature stages. Don’tforget that, in the case of the more advanced developing granulocytes, the term basophilic oreosinophilic refers to the cytoplasmic granules, not the cytoplasmic staining per se. The overallcytoplasm is more basophilic for any type of granulocyte in the early developmental stages.Refer to the lecture handout for aid in identifying the various stages in erythrocyte andgranulocyte differentiation.
By examining 32A under oil, you should be able to find basophilic erythroblasts,polychromatophilic erythroblasts, normoblasts and both immature and mature erythrocytes.Look for promyelocytes with only a small cluster of granules and otherwise basophiliccytoplasm. What is the name of these granules? Their nuclei are not indented. Myelocytes showa wide variation in numbers of granules, are often quite large, and display a less basophiliccytoplasm. Metamyelocytes with horseshoe shaped nuclei are readily seen, and are a terminalstage which forms the mature polymorph by differentiation without further division. Thebasophilic metamyelocytes have large purple granules and are relatively rare, but can be found
Hemopoiesis

60
in occasional preparations. Look for band forms. Other cell types that you will find aremegakaryocytes, lymphocytes, fat cells , plasma cells and reticulum cells . The cells with themost prominent dark blue cytoplasm might be either plasma cells or basophilic erythroblasts.At what stage can you first distinguish between developing neutrophils, eosinophils andbasophils? There are several characteristics which distinguish a plasma cell. The eccentrically-placed nucleus has a cartwheel appearance due to the arrangement of the chromatin and aprominent nucleolus. The cytoplasm is highly basophilic (why?) except for a light area in thecenter of the cell next to the nucleus. What is in this lighter region? The plasma cell often containsa prominent vacuole in the cytoplasm. After studying plasma cells, how would you distinguishthem from basophilic erythroblasts? How can you distinguish immature, but anucleate,erythrocytes from mature ones?
Do not confuse the term reticulum cell with reticulocyte. The latter refers to an immatureerythrocyte, which has been made highly visible for quantitative purposes by staining withbrilliant cresyl blue or other dyes which stain ribonucleoprotein (RNP). The name reticulocytederives from the fact that these special stains precipitate the RNP in immature erythrocytes intoa darkly staining network (i.e., reticular arrangement), which otherwise would have stainedhomogeneously for hemoglobin (e.g., pink) in more mature cells. The reticulum cell, on the otherhand, is one of the larger cells you will see in a marrow smear (the even larger megakaryocytesand fat cells are often destroyed in preparation). The reticulum cell has abundant and ratherirregularly granular cytoplasm and a large, lumpy nucleus, often with a distinctive pale bluenucleolus. The reddish-blue chromatin of the nucleus generally has a “ropy” appearance.Reticulum cells are believed to represent the reticular cells of intact marrow.
Electron MicrographsTry to work out the characteristics of the differentiative processes in these cell lines from bothyour observations in the light microscope and your perusal of the electron micrographs. Forinstance, how does the chromatin change as the cells mature? The compaction of the nuclearelements is correlated with decreasing synthetic activity of the cell. In picture #l, you shouldcompare the nuclei of the myelocyte and the polymorphonuclear leukocyte. What organellesreside in the cytoplasm that occupies an area indenting the nucleus of a monocyte? Correlatethe light microscopic appearance and the fine structure of the plasma cell. Do the same for thedeveloping erythrocytes.
HEMOPOIESIS

61
ThymusBegin by looking under low power (4x) at the plastic section of a young human thymus (37A).Note that the connective tissue septa separating the lobules are very thin. The intensely bluecortex is thick, relative to the medulla. In some areas, the medullary regions of several lobulescan be seen to coalesce (actually all the medullary regions connect with each other). Under l00x,you can see that the homogeneously-stained pink spots and streaks represent vessel lumenscontaining plasma and RBCs. There are also numerous cells with bright red granules, which aremast cells. They are found mostly in connective tissue around vessels near the cortical-medullary junction, where the larger vessels distribute (drain) small branches to (or from) thecortex and medulla. The medulla appears lighter in color because of the relatively largerpercentage of the big epithelial-reticular cells . First, find one of the larger Hassall’scorpuscles . These consist of concentrically arranged, flattened epithelial-reticular cells invarious degrees of “degeneration”. Many contain dark staining granules. In some of the largerones, the outermost few epithelial reticular cells appear quite intact. These will show you thevery euchromatic, large, roughly oval nucleus and bright red nucleolus (or 2 nucleoli)characteristic of these cells. Now you can identify many other such nuclei throughout themedulla as probably belonging to epithelial- reticular cells. Most of the other cells in the medullaare lymphocytes (small and medium), endothelial cells, and macrophages. The macrophages alsohave rather euchromatic, large nuclei, and are almost impossible to distinguish from epithelial-reticular cells with certainty unless you see intracytoplasmic debris or vacuolization. At the EMlevel they can be distinguished. Do you know the criteria?
Within the cortex, the lymphoblasts, macrophages and epithelial-reticular cells cannot bedistinguished from each other with certainty, since they all have large, euchromatic nuclei. Thepredominant cell type is the small lymphocyte, which has very clumped chromatin and scantcytoplasm. Intermediate sized lymphocytes (between the small and the blastic lymphocyte)exhibit intermediate degrees of chromatin clumping and amount of cytoplasm. Do you seeHassall’s corpuscles in the cortex? Do you see mitotic figures? Do you expect to see mitoticfigures within the medulla? Could the metaphase mitotic figure you think you see be a neutrophilor a pyknotic nucleus? Can you see any plasma cells? Should there be any?
In slide 38A from a human infant, it is rather difficult to distinguish the cortex from the medulla.Slide 42A shows an involuted thymus from a small mammal. Under low power, observe theconsiderable widening of the interlobular connective tissue spaces and their replacement byfatty tissue. The cortex is thinner (relative to the medullary region) and total thymic tissue isdecreased. Under high power, you can see the same distribution of cell types. The cortex isstill packed with small lymphocytes. Occasional clear-cut mitotic figures can be found,consistent with the current view that the thymus continues to function well into adulthood and,perhaps, old age.
Peripheral Lymphoid Tissue
Diffuse Lymphocytic AccumulationsThe simplest form of lymphoid tissue consists of mere unorganized accumulations of lympho-cytes and some associated cells (such as macrophages, plasma cells). These may be diffuseor nodular. They are found in many organs, e.g. the submandibular salivary gland (7lA), the
Lymphatic Tissue

62
gastrointestinal tract (99A) and the bronchial tree. You are not yet familiar with the histologyof these organs, but the lymphoid accumulations can be easily spotted under low power asrelatively dense concentrations of very dark, heterochromatic nuclei. Under high dry, you canappreciate that the small and medium lymphocytes predominate, thereby conferring thatcharacteristic appearance. From these slides, you will note that lymphoid accumulations oftendevelop beneath mucous membranes and in connective tissue surrounding ducts of glands.
Lymphoid NodulesNext in order of complexity are the lymphoid nodules (also called follicles) that are found inspecific locations associated with the gut. Germinal centers are frequently present in thesenodules. The tonsils are such nodules of lymphoid tissue underneath the mucosal epithelium.They are massively developed in the oral pharynx (slide 30A). The pharyngeal tonsils containextensive epithelial crypts (tonsillar crypts) which are infoldings of the epithelium. Theepithelium can be very thin over the large lymphoid nodules. Peyer’s patches constitute theother main group of such accumulations in the ileum (9lA). Similar collections can be seen inthe colon (94A) and the appendix (96A).
Lymph NodesLymph nodes represent highly organized and encapsulated collections of lymphoid and relatedcells. The silver impregnated section (the black and blue one) on slide 36A shows the generalarchitecture of lymph nodes best. The reticular fibers appear as black threads and the cell nucleihave been counterstained blue. The subcapsular, intermediate and medullary sinuses standout as relatively more open spaces, containing fewer reticular fibers and fewer cells. In contrast,the cortex and medullary cords are densely packed with cells. All the vessels are clearly outlinedby a ring of reticular fibers , as are the connective tissue trabeculae. In the cortex, there are manygerminal centers . One can see the typical appearance of a cap (or ring) of densely packed smalllymphocytes over the more lightly stained oval area. Within the light area of the germinal centers,many large lymphocytes and blasts are found. The medullary cords constitute a highly branchednetwork of solid tissue going from the cortex to the hilum of the node. In some sections, smallsegments of the afferent lymphatics can be seen to empty into the subcapsular sinus, and thelymphatic valves, sometimes can be seen outlined by reticular fibers.
In some areas of the sinuses, you can clearly see rosettes of grayish-tan color attached tothe reticular fibers criss-crossing the sinus lumen. These are sinus macrophages engorged withphagocytosed red cells. Such macrophages are seen in the subcapsular, intermediate andmedullary sinuses. RBCs do not normally enter the lymph, so this node represents a pathologicalsituation. Lymph node macrophages will phagocytose RBCs, although many other types ofmacrophages will not gobble up normal RBCs (absolutely essential in the liver since themacrophages are in blood sinuses).
Now turn to the other section on the same slide. You will again see the RBC (bright orange)engorged sinus macrophages. Within the sinuses you can identify some of the reticular cellsas having large, oval, euchromatic nuclei and cytoplasmic processes which stretch somedistance across the lumen. They can be most easily seen in the subcapsular sinuses. Consistentwith the abnormal blood extravasation into the lymph sinuses, you can also find manyneutrophils in the sinus lumen. They are also not normally found there. Within the cortex, youcan see a full range of euchromatic and heterochromatic nuclei. The larger and more euchromaticnuclei belong to lymphoblasts, large lymphocytes, macrophages and reticular cells. The ones
LYMPHATIC TISSUE

63
with smaller and more clumped chromatin belong to small and medium lymphocytes. The largelymphocytes and blasts are mostly found within germinal centers. Mitotic figures are also foundprimarily there. True plasma cells are rare around germinal centers, but some cells with abundantbasophilic cytoplasm and heterochromatic nuclei (representing transitional cells on their wayto becoming plasma cells) can be found within the cortex near the corticomedullary border. Themedullary cords can be clearly seen to be covered by a layer of reticular cells. The cords containlymphocytes and many plasma cells. The finding of neutrophils outside of vessels in the cords(as seen here) is abnormal. Reticular cells forming the scaffolding meshwork for holding thelymphoid cells within the cortex, and cords are not distinguishable in most instances fromlymphoblasts, large lymphocytes and macrophages.
Distinctive structures found in lymph nodes are the high endothelial postcapillary venules,which are the sites where blood lymphocytes enter the lymph node parenchyma. These arefound within the cortex, largely in the deeper portion of the cortex. The height of the endothelialcells vary somewhat with tissue preparation. Therefore, on any given slide, you should firstlocate some typical capillaries and note their lumen size, the flatness of their endothelial cellnuclei and the almost indiscernible layer of cytoplasm. Usually you can see only one (at mosttwo), very flat nuclei in a capillary cross section. Then, within the deep cortex, find vessel lumensof similar size which are lined by thicker cells. Since these endothelial cells are roughly cuboidaland cover less territory than the usual squamous endothelial cell, there are usually 2-3 or moreof these nuclei per cross section of these vessels. In longitudinal section, the nuclei can be seento be spaced more closely together than the usual endothelial cell nuclei, and have a morerounded shape (rather than the usual long oval shape of endothelial nuclei). Moreover, you canmake out some cytoplasm around the nuclei, unlike the usual endothelium. Sometimeslymphocytes can be found in passage between the endothelial cells, which may make the initialrecognition of the endothelium harder, but help the identification in the end.
Slide 34A is a plastic section of a lymph node. If your section is cut near the hilum, you cansee a concentration of muscular arteries and veins and, perhaps, a collapsed thin walledlymphatic vessel, all within rather extensive connective tissue spaces. As is characteristic ofplastic sections, the “open” spaces seen on paraffin sections seem to have disappeared.However, one can still appreciate relatively less cellular appearance of the various sinuses.Apply the description of slide 36A to this section except for the following: i.e. there are onlyrare RBC-engorged macrophages and a few neutrophils in the lymphatic sinuses. The few RBC-engorged macrophages must be carefully distinguished from the well preserved and conspicu-ous mast cells. Are the latter present in sinuses, in both the cortex and medullary cords? Unlikethe paraffin section, the many macrophages can be clearly identified in the cortex and cords bytheir cytoplasmic debris and vacuolization (especially in germinal centers). The identificationof the high-endothelial postcapillary venule is both easier and harder. Although the cuboidalnature of the endothelial cells is better preserved, the lumen in most instances are filled withlymphocytes (and some other blood cells). Many are caught in longitudinal-oblique sectionand show lymphocytes in passage through the endothelium.
LYMPHATIC TISSUE

64
SpleenHistologically, the spleen is the most complex lymphoid organ. The general structural plan canbest be seen on the H & E section on 43A. Under very low power, you can easily identify eachof the following regions and then examine them under high dry:
White PulpThe white pulp areas (WP) are the dense collections of small lymphocytes around a relativelysmall muscular artery, i.e., the periarterial lymphatic sheath (PALS), its central artery andlymphatic nodules (with or without germinal centers). The PALS is the collection of mainly smalllymphocytes, which are roughly symmetrically arranged around the central artery. The nodulesare roughly spherical structures, arranged to the side of the central artery. So in a cross sectionthrough a nodule, the central artery appears eccentric within the total area of lymphocyteaccumulation (nodule + PALS). How do T and B lymphocytes distribute within the nodulesversus the PALS? The nodules contain densely packed small lymphocytes. When germinalcenters develop within them, a lighter center is seen in the nodules, as is typical of all germinalcenters. Why are germinal centers more lightly stained? There are very few on this side. Underhigh power, you can see the smooth muscle cells of the central artery wall and its endothelium.With careful focusing you can also discern some of the pink streaks of reticular cell cytoplasmbetween the numerous lymphocytes. The lymphocytes are mostly small and medium types,except in germinal centers. The large, euchromatic nuclei belong to macrophages and reticularcells. Where and when are you likely to find plasma cells in the spleen?
Red PulpThe Red Pulp (RP) consists of the bulk of the space between the WP areas. They include thesplenic sinuses (venous sinusoids) and the splenic cords (of Billroth) in between the sinuses.The former are blood sinuses with large and free lumen (no fixed cells or fibers crossing it). Theblood has been largely removed from this spleen before fixation, so the sinus and vessel lumensappear as “empty” spaces, only occasionally containing a few blood cells. The sinuses can bedistinguished from the pulp veins which drain them by their peculiar endothelial cells. The roundendothelial nuclei are irregularly spaced around the sinus, and tend to protrude into the lumen.The pink cytoplasm of these endothelial cells can be seen in the spaces between the nuclei. Theendothelial cells of the splenic sinusoid are long spindle-shaped cells that are arranged in thewall of the sinus like the staves of a barrel. In some oblique sections, you can see the “candystripe” appearance of these cells. Many blood cells can be seen in passage between theendothelial cells. This is called “diapedesis.” Immotile cells (RBC and platelets) pass throughalso, but the term is not applied to them. The pulp veins are easily identified by their usual hard-to-see squamous endothelium, the scarcity of connective tissue surround, and their large lumen(especially relative to wall thickness). Between the sinuses are the cords. These are filled withall the formed elements of blood, as well as resident macrophages and free plasma cells. Thestroma is formed by the reticular cells and their meshwork of fibers. Many of these various cellscan be identified by criteria already familiar to you.
Vascular Organization of the SpleenSlide 45A of the dog spleen is particularly good for showing the vascular organization of the
LYMPHATIC TISSUE

65
spleen. Scattered throughout the spleen are sections through the numerous connective tissuetrabeculae. These radiate from the splenic capsule and branch throughout the substance ofthe spleen. Major vessels enter and leave in them. In the connective tissue trabeculae of thisdog spleen, one can find many smooth muscle cells running parallel to and mixed in theconnective tissue collagen, as well as smooth muscle cells forming the walls of the trabeculararteries and trabecular veins. In human spleens, the smooth muscle component is much lessoutside the vessel walls. The trabecular arteries give rise to branches which leave the trabeculaeas central arteries , while the pulp veins drain into the trabecular veins. Found within the cordsare the arterioles and capillaries of the red pulp. The central artery terminates as it leaves thewhite pulp, branching to form the penicillar vessels of the red pulp. Different portions are givenspecific class names, as the penicillar vessels branch and rebranch to supply the red pulp. Theinitial portion (right after they leave the WP) is the pulp artery. These short segments stillpossess a thin muscular coat, but much attenuated relative to that of the central artery. As theirbranches become capillary sized, they often acquire a sheath of concentrically-arrangedphagocytic cells. These are called the sheathed arterial capillaries. They are plentiful in thedog spleen, as can be seen on this slide. They stand out by virtue of the intensely eosinophilicstaining of the cytoplasm of the sheathing cells, and the remarkable thickness of this coat ofcells around a capillary-sized clear lumen. In human spleens, there are fewer of these sheathedcapillaries and the coat is not as well developed. The terminal portion of the penicillar vesselsare simply ordinary capillaries, although they are specifically designated as arterial capillaries.The sheathed arterial capillaries terminate as arterial capillaries after they emerge from thesheath. Usually such terminations are bell-shaped and open-ended, so that the lumen mayappear somewhat wider than the usual capillary seen in other organs. Alternatively, the arterialcapillaries may derive directly from the pulp artery without an intervening segment of sheathedarterial capillary. (Note: Unfortunately “pulp arteries” is also sometimes used loosely todesignate all arteries and capillaries of the red pulp, i.e., synonymous with “penicillar vessels”).
Marginal Zone The marginal zone (MZ) is the area immediately surrounding the White Pulp areas. It representsthe transition between WP and RP. It is mostly easily discerned under low power (4x and l0x),as the relatively cellular zone surrounding the densely cellular WP area but which also containssome small sinusoids. Under high power, the MZ can be seen to contain cords between smallsinuses. The cells in the cords include blood cells (conspicuously, neutrophils and RBCs)lymphocytes, macrophages, reticular cells and plasma cells.
Now turn to the silver stained section on slide 43A for a quick look at the dense mesh-likestroma formed by the reticular fibers. Relate the outlined structures here to the other sectionwhich you have now examined in great detail. All the trabeculae and larger vessel walls are darklystained. Why is that? The white pulp areas have a looser mesh of fibers (especially the lymphoidnodules). The sinusoid lumens, like the vessel lumens, are free of fibers. One can also appreciatethat the MZ has a denser mesh of fibers than the WP, and the sinusoids outlined by the reticularfibers are smaller than in the RP. Of particular interest is the circular investment of the sinusesby the reticular fibers, which assume a relationship to the endothelial cells like that of thestrapping to barrel staves. The basement membrane of the sinusoid contains reticular fibers,so this “strapping” arrangement holds for the basement membrane as well. This discontinuousarrangement of the basement membrane may aid diapedesis.
LYMPHATIC TISSUE

66
SinusoidsNext, look at slide 47A (the plastic embedded section of a primate spleen). Identify the WP, RPand MZ under low power. In some of your slides, there is one trabecula with a large vessel init. Note that the WP areas appear lighter because the RP sinusoids and vessel lumens are filledwith deeply eosinophilic RBC and plasma. The MZ is less distinct than in the previous slide,but can be seen as the area with smaller sinusoids roughly concentrically placed around the WPareas. Under high power, the cellular components of all the regions can be seen in greater detailin this section. Starting with the WP, you can see that the central arteries are all partly collapsed.The lumens are constricted and appear only as small areas of deep pink in the middle of a thickwall of smooth muscle cells. The endothelial cells appear thick and crowded rather thansquamous due to the collapse. Find the germinal centers present in some lymphoid nodules.Within the germinal centers, you should be able to identify some macrophages, mitotic figuresand many small lymphocytes. An occasional reticular cell can be identified with certainty bytheir large euchromatic nucleus, and long extended cytoplasmic processes. Within the RP, youshould be able to identify the complete outline of many sinusoids with their thick endotheliumand wide (but filled) lumen. Identify some of the many examples of leukocytes undergoingdiapedesis. The cords can be found immediately adjacent to each sinusoid you delineate. Theycan be seen to contain many more cells, and the spots of pink (RBC) are less continuous thanin the lumen of the sinusoids (where plasma between the RBC also stain). Some of the cord cellscan be clearly identified as lymphocytes, neutrophils, eosinophils, plasma cells and macroph-ages.
Slide 44A is an “unwashed” spleen which is still full of blood. If you compare the amountof blood in the red and white pulp areas, you will readily understand the derivation of thesenames.
LYMPHATIC TISSUE

67
Epidermis and Dermis
The most obvious feature of cross sections of this organ is that it consists of two distinct strata,a superficial epidermis and the underlying dermis. The epidermis is a stratified squamousepithelium in which the most superficial cells are dead squamous cells, devoid of most cellorganelles and filled with filamentous and amorphous proteins called keratins . The generalprocess by which keratins are produced in the cytoplasm of cells is called keratinization, andmay also be seen in the epithelium of the vagina, esophagus, oral cavity and thymic corpuscles.In these cases, however, keratinization normally does not result in a discrete dead layer of cellsdevoid of organelles (called the stratum corneum), but rather the cells retain their nuclei andmay be living. This type of incomplete keratinization is called parakeratinization and may occurin human skin in certain pathological conditions. Since a form of keratinization occurs in manyepithelial tissues, it is helpful to use the word cornification for that process that results in a deadand relatively impermeable stratum corneum. Epidermal cells which synthesize keratin are calledkeratinocytes.
Slide lA is digital skin from a monkey. The H & E section shows the greatly thickenedepidermis in this area. Note the well developed stratum corneum which is virtually free of nucleior basophilia. Just deep to the stratum corneum is the stratum granulosum. The cells in thislayer are filled with basophilic (blue) keratohyalin granules , which participate in the formationof keratin that will fill the horny cells of the stratum corneum. Note how sudden the transitionis from living cells in the granular layer to the dead flattened cells in the stratum corneum. Theepidermis, deep to the stratum granulosum, is called the stratum spinosum (stratum Malpighii).The deepest layer of the epidermis consists of low columnar cells, with nuclei squeezed veryclose together. This layer is called the basal layer, or occasionally the stratum germinativumsince most (if not all) of the mitotic activity occurs here. The irregular form of the deep rete ridgesis due to the plane of section. Melanin granules are abundant in the basal cells of the rete ridges.Stem cells are located in these areas, and are protected from actinic radiation by the supernuclearlocation of their melanin. You may occasionally see the dendritic processes of a melanocytein the basal layer.
The dermis is stained very lightly in this section, but in the other section on this slide (stainedwith aldehyde fuchsin, orange G and fast green), the yellow stained collagen and purple elasticfibers are evident. Most of the nuclei are in fibroblasts. Note the many cross sections of bloodvessels in the dermis. The ridges formed on the under surface of the epidermis are called reteridges . Note that the ducts of the sweat glands always contact the epidermal surface at the crestof these ridges. Coiled sweat glands and blood vessels are abundant. Can you find the sweatducts in the epidermis? The duct goes through the stratum corneum in a spiral path (Somesections of the aldehyde fuchsin specimen on lA will show a parasitic round worm embeddedin the epidermis). In some sections, there are a few onion-like nerve endings (called Paciniancorpuscles) located in the dermis. These pressure receptors consist of concentric layers ofsquamous epithelial cells around a central nerve fiber. Finger-like dermal extensions extendingup between the rete ridges are called dermal papillae. Within these papillae are blood capillariesand nerve endings. In the Bodian silver preparation of monkey digital skin (slide 2A), specializednerve endings (Meissner’s corpuscles) will be seen at the apex of some dermal papillae. Alsonotice that the deep dermis has many nerve trunks consisting of many fibers in bundles, andthat fibers often terminate in association with the eccrine sweat glands (probably representingthe sympathetic innervation of these structures). If you compare the two sections on this slide,
Integumentary System

68
you will find that it would be impossible to identify elastic fibers in this section without a suitablestain such as aldehyde fuchsin.
The plastic section (7A) is best for observing keratohyalin and melanin granules, the spinycells of the stratum spinosum, and both the secretory and duct portions of the eccrine sweatglands. The occasional clear cells in the basal layer containing scattered melanin granules aremelanocytes. These cells are responsible for the synthesis of melanoprotein. You will note thatmost of the melanin in the basal layer is actually in pink stained keratinocytes, rather than in clearmelanocytes or the more superficial keratinocytes. The keratinocytes of the basal layerphagocytize the tips of the dendritic process of melanocytes and, in this way, take on melaningranules. Once inside the keratinocyte, there is a directed movement of melanin granules, suchthat they come to occupy a supranuclear position; this provides an effective solar screen forthe DNA in these cells. You should see evidence of this preferential location in your slides ofpigmented skin. As the keratinocytes ascend to a higher level in the epidermis, most of theirmelanin is broken down and is no longer visible. Some pigment may persist in the stratumcorneum of darker skinned humans and animals. The spiny-looking cells of the stratum spinosumare easily discerned in the middle layers of the epidermis. This spiny appearance is actually ashrinkage artifact which reveals the scores of desmosomal attachments on the surface of eachkeratinocyte (keratin-producing cell in epidermis). The stratum granulosum is easily visible.Between this granular layer and the stratum corneum, you will find occasional transitional cellswith pyknotic nuclei. These cells are dying and will become corneocytes. Notice that thecorneocytes have little “peg and socket” elaborations between cells that appear to givemechanical integrity to the stratum corneum; this is typical of epidermis from the palms or soleswhich are high wear areas.
HairThe bodies of nearly all mammals are covered with hair. Slide 3A shows growing (anagen) hairfollicles in the human scalp. The hairs (like the sweat glands) are of epidermal origin thougha little tuft of dermis, called the hair papilla, in the deepest part of the hair follicle, is necessaryfor growth and differentiation of the hair. Longitudinal sections of hair follicles often show thedermal papilla surrounded by the bulb of the hair follicle like a claw. Hair follicles grow at arelatively uniform angle to the epidermis. Because of the plane of section, it is not always possibleto see the whole length of some hair follicles. The hair itself is yellow with black pigment granulesin the cortex, the living portion of the follicle stains blue, and the inner root sheath stains red.The melanocytes that produce the melanin are adjacent to the hair papilla, as can be observedin a longitudinal section through the hair bulb (bulb-shaped end of follicle). The mitotic activitythat supports hair growth occurs only in the hair matrix in the interior of the bulb. As thesematrix cells move up the follicle, they differentiate into the keratinized layers of the inner rootsheath as well as the hair shaft. As in the stratum corneum, part of this differentiation involvescell death (Consult your histology book for details of hair follicle structure; Ham is particularlygood in this respect). About one-third of the way down the follicle, on the side that forms anobtuse angle with the epidermis there is generally a bulge of vacuolated cells comprising thesebaceous gland. When the cells in the interior of this gland break down, their detritus (calledsebum) slips out between the inner root sheath of the follicle and the hair ( pilosebaceous canal)shaft to the surface of the skin. Some of the cytological details of this breakdown process canbe seen in electron micrographs in the integument collection. You may observe some “resting”(telogen) hair follicles. These follicles are shorter than anagen follicles and the deep end of the
INTEGUMENTARY SYSTEM

69
follicle is enlarged and has a rather spiny appearance from which it gets its name -- club hair.Slide 3A also shows the cutaneous blood supply to good advantage. Note the capillary loopsin the dermal papillae and the close association of blood vessels with both hair follicles and theeccrine sweat glands in the subcutaneous fat.
Slide 63A (lip) has well stained cross and longitudinal sections of hair follicles. The largesthair follicles in the lip are sinus hairs which derive their name from the fact that the bulbousportion of the follicle is suspended in a large blood sinus. These follicles produce the vibrissaeor “whiskers” of rodents, cats, etc., where they have a highly developed sensory function.
Slide 4A is from the bald human scalp and reveals that hair follicles and growing hairs areas numerous as in slide 3A. The hairs and hair follicles of the bald scalp are much smaller,however, and are called vellus hairs . These are the kind of hairs we find on our nose andforehead. Note the well-developed sebaceous glands that add insult to injury in baldness bymaking a “shiny pate.” These tiny hairs are common on the human body and give the mistakenimpression that man is largely “hairless.”
Slide 6A has two sections of adult thigh skin, the red staining H & OGE for collagen and theblack Verhoeff’s hematoxylin for elastic fibers. The epidermis is stained poorly on both sections.On the H & OGE preparation, the superficial papillary layer of the dermis is rather sharplydemarcated from coarser fibers in the reticular layer of the dermis. The reticular layer mergeswith the subcutaneous fat.
Sweat Glands
Eccrine Sweat GlandsSlide 7A is particularly well suited to study the histological detail of both the secretory and ductportions of eccrine sweat glands. The secretory portion of the sweat glands is readilydistinguished by the presence of myoepithelial cells, which give a scalloped appearance to thetubules in cross section. This is the only slide in which the mucus-producing dark cells andthe serous fluid-forming light cells can be readily discerned. The dark cells appear to be nearthe lumen and have distinct red granules, whereas the light cells comprise the bulk of thesecretory segment. Actually both the dark and light cells rest on the basement membrane. Theduct, on the other hand, is clearly a stratified cuboidal epithelium. Note the various cell types(including mast cells) that populate the dermis.
In slide 6A, the coiled secretory portion of the sweat glands and a good portion of the sweatducts lie in the reticular layer of the dermis. Note that the epithelium of the duct of the sweatglands is two cell layers thick and is darkly stained, while the epithelium of the secretory portionis one cell layer thick (although it may appear thicker) and lightly stained. Also notice themyoepithelial cells that are associated with the secretory portion. What function do they have?
Apocrine Sweat GlandsSlide 8A of axillary skin has been included in your collection to show the two types of sweatglands that exist in this area. You have seen eccrine sweat glands in most of the previous slides.Apocrine sweat glands are much more limited in distribution. There are two obvious differencesin the histology of these glands. The secretory part of the apocrine gland is larger in diameterand consists of a simple columnar epithelium. You will occasionally see a yellow lipofuscin
INTEGUMENTARY SYSTEM

70
material in these cells. The myoepithelial cells are well developed and, therefore, can be easilyseen on the apocrine and eccrine sweat glands. Apocrine glands are also found on the slide ofthe recto-anal junction (99A); this slide is also very good for studying sebaceous glands, hairfollicles, and Pacinian corpuscles.
The Meibomian glands (slide 98B) of the eyelid are of interest because they develop inassociation with hair follicles and are greatly enlarged and modified sebaceous glands. Whatfunction might these glands serve?
INTEGUMENTARY SYSTEM

71
Respiratory System
Nasal CavityIn examining the respiratory system from nares to alveoli, try to think of the ways in which thestructural adaptations of each part serves its function(s). The nose contains two nasal cavitiesseparated from one another by the nasal septum. Each nasal cavity is divided into two parts:(l) the vestibule, a slight dilation inside the opening of each nostril, and (2) the respiratoryportion, the remainder of the cavity.
Slide 28B is a frontal section through half of a cat nose. Orient yourself by examining theslide without the microscope (see diagram).
Note that the borders are the nasal septum (medial) and the wall of the maxillary sinus (lateral),while the hard palate forms the floor of the nasal cavity (as well as the roof of the oral cavity).The conchae (turbinates) are curled plates of bone extending from the lateral wall into the cavityand greatly increase the surface area over which air passes; they are more complex in the catthan in the human. Evidence for continuing bone deposition can be found on this slide. Theepithelium covering most of the nasal mucosa is pseudostratified ciliated columnar epitheliumwith numerous goblet cells. Venous plexuses are prominent beneath the epithelium of theconchae.
Olfactory EpitheliumOlfactory epithelium covers a portion of the surface of the upper conchae. This epithelium istall pseudostratified columnar, and consists of supporting (sustentacular) cells whose nucleiare generally nearest the free surface and bipolar nerve cells (called olfactory cells) whose nucleioccupy a wide zone deep to those of the supporting cells. Venous plexuses, the olfactory glandsof Bowman (serous), and bundles of nerve fibers are found beneath the epithelium.

72
PalateThe palate extends posteriorly so as to form a partial division between the nasal and oral portionsof the pharynx, and consists of an anterior 2/3 (hard palate) and a posterior l/3 (soft palate). Slide34B is a section through a portion of the palate. The hard palate can be identified by the presenceof bone, covered superiorly by the mucous membrane of the nasal cavity and inferiorly by theoral mucosa.
Proceeding from above downward in the hard palate, one finds: l) nasal epithelium; 2) a laminapropria containing a few small, primarily mucous, glands; 3) bone; and 4) stratified squamousepithelium of the oral surface. Posteriorly in the soft palate, bone is absent and dense regularCT, muscle and large mucous glands are found. Palatine tonsils indicate that this section is lateraland caudal. Note that the passageways which carry only air have a pseudostratified columnarepithelium with goblet cells, while those which convey food or both food and air are lined bya stratified squamous epithelium.
TracheaSlide 35B represents a portion of the wall of the trachea cut in cross section. Although theepithelium is poorly preserved, the mixed nature of the tracheal glands is well shown. Study theplastic section (36B) in which the trachea is much better preserved, including the cilia.
LungSlide l8A shows the lobar bronchi, which supply air to one lobe of the lung. These bronchi arein the lung, but the histology of the lung parenchyma is poorly preserved. Slide 37B isparticularly useful for studying the intrapulmonary branching of the bronchial tree. Bronchi canbe easily discerned under low power by the presence of isolated pieces of cartilage deep to thesubmucosa. More distally in the tree, the cartilage is lost giving rise to the bronchioles. Theaccompanying diagram will be of assistance in locating the various portions of the peripheralairway. Respiratory ducts and alveolar ducts are easily visible in this preparation. The aldehydefuchsin section is especially useful since it emphasizes the cartilage, elastin and mucus of thegoblet cells. All of the blood vessels in the lung are rather thin-walled, making arteries difficultto distinguish from veins. In general the pulmonary and bronchial arteries are close to and branchwith the bronchial tree, whereas the veins (carrying oxygenated blood) run in the septa betweenadjacent bronchi. The pulmonary arteries have better developed elastica interna and externathan do the bronchial arteries.
Slide 32B is a thinner section of lung and, therefore, best for studying many of the finer details;in this preparation elastin and cell nuclei are black, cell cytoplasm is yellow, and collagen andcartilage are red. Look for the various air passages; cilia are particularly well preserved. Studythe alveolar wall; how would you characterize the pattern of the fine elastic fibers which are verynicely shown? Leukocytes also can be identified easily in this preparation. Of what is the visceral
RESPIRATORY SYSTEM

73
pleura composed?Slide 3lB (a plastic section) will reward your careful study with an appreciation of many
structural details of the alveolus and alveolar ducts. The aggregates of smooth muscle cells thatcomprise the helical wall of the alveolar duct are very well shown as a knob-like structure betweenalveoli (when the muscle cells are cut in cross section). Greater alveolar cells (septal cells, typeII pneumocytes) are also clearly visible among the type I pneumocytes in the alveolar wall. Thegreater alveolar cell bulges into the lumen of the alveolus, and is highly vacuolated due toextraction of its lipid rich multilamellar bodies (cytosomes). Note how closely the capillaries mayapproach the alveolar lumen. Elastin is unstained in this slide, but may still be discerned nearthe smooth muscle in the wall of the alveolar ducts. Ciliated cells may be present in some of theslides. Leukocytes are easily seen.
Slide 37B is a relatively thick section from a lung collapsed by pneumothorax. However, moreof the blood has been retained in the capillaries, and the pulmonary epithelium is in a better stateof preservation. Knobs of smooth muscle marking the walls of alveolar ducts can be recognized.Study the thick section (39B) in order to obtain a three-dimensional impression of the terminalairways. Try to distinguish alveolar ducts from alveoli. Under high-dry, the cellular compositionof some of the alveoli can be seen in a “whole mount” view. If you study the surface of the alveolarwall, you will be able to see the alveolar pores which are holes l0-l5 µm in diameter betweenadjacent alveolus; these serve as accessory communications between alveoli. Alveolarmacrophages (dust cells) may also be seen on the luminal surface of the alveolar wall.
Electron MicrographsIn EMs of the lung, identify the squamous pulmonary epithelial cells, greater alveolar cellswith their “laminated bodies,” and endothelial cells of the capillaries. Examine the air-blood“barrier” and identify all the components of that barrier in thick and thin areas.
EMs of the trachea show the typical appearance of ciliated columnar epithelial cells. Notethe appearance of cilia and microvilli in longitudinal and cross section. Also present are portionsof goblet cells with many mucigen droplets in the apical part of the cell.
RESPIRATORY SYSTEM

74
RESPIRATORY SYSTEM

75
The digestive system consists of a long epithelial-lined muscular tube, beginning at the lips andending at the anus. At both ends of the tube, the moist mucosal epithelium of the digestivetract abruptly joins the cornified integument at a mucocutaneous junction. That portion of thetube extending from the pharyngeoesophageal junction to the recto-anal junction is known asthe alimentary canal, and has a common structural plan throughout.
LipsSlide 54A shows the mucous and cutaneous surface of the lip of a 4-5 month fetus. Theepithelium on the cutaneous surface is cornified (though most of the stratum corneum is lost),whereas that on the mucous surface is simply keratinized. The epidermal cells are much largeron the mucous surface than the cutaneous surface and, naturally, lack hair follicles and sweatglands. The mucous surface of the lip and gingiva is quite similar. Mucus-secreting labial glandsare just developing under the mucosa of the lip. A diagram of this slide appears in the sectionon “Bone.”
Slide 63A shows the mucocutaneous junction of the lip in the adult human. Note the suddenchange in the thickness and appearance of the epidermis at the vermilion border of the lip (theunhaired portion of the cutaneous surface of the lip). Some of the hairs of the lip are sinus hairs,having a large loose capsule filled with blood. Note the mature labial salivary glands . Try tofind their ducts.
TeethSlide 54A also shows the early development of the teeth. The tooth is embedded in a connectivetissue space of the alveolar bone. You should be able to find the outer epithelium (simplecuboidal) of the enamel organ which surrounds the stellate reticulum. The enamel organ isinitially shaped like a ball with its bottom pushed in. The resulting concave surface is the innerenamel epithelium. The stellate reticulum is derived from the internal cells of the enamel organthrough an accumulation of gelatinous intercellular substance. In your slide, the inner enamelepithelium cells have elongated into tall columnar cells called ameloblasts (enamel producing)which are separated from the stellate cells by a layer of cuboidal cells, the stratum intermedium.
The whole cap-shaped enamel organ sits on the dental papilla. The mesenchymal cells ofthis papilla immediately adjacent to the ameloblasts also form tall columnar cells calledodontoblasts (will form dentin). Dentin production precedes enamel production, and a thin grayarea of dentin may be visible just under the ameloblasts. As dentin is laid down, theseodontoblasts recede centripetally, narrowing the pulp cavity. The enamel will grow centrifu-gally. In neither case are cells incorporated into the calcified tissues, although the odontoblastsleave a cell process in the dentin.
A mature tooth is visible in slide 64A. Note the cornified gingiva. The enamel has been lostin this decalcified preparation (enamel is about 95% inorganic). The pulp cavity, dentin, dentinaltubules, cementum and the periodontal ligament are visible.
Oral Cavity

76
TongueThe dorsal epithelium of the anterior part of the tongue has two types of papillae. Both the cone-shaped and cornified filiform papillae and the mushroom-shaped fungiform papillae can beobserved on slide 65A. The junction of the epithelium and lamina propria is greatly folded intopapillae, much as in the skin.
Taste BudsTaste buds will be visible in the epithelium at the apex, rather than on sides, in most fungiformpapillae. The sustentacular and taste cells are difficult to distinguish. In fact, the taste buds aredifficult to distinguish from secondary papillae in this preparation. In some taste buds you willbe able to see the taste pore.
The lamina propria of the tongue is clearly delineated from the muscular layer. Both serousand mucous lingual salivary glands are prominent in the posterior portion of the tongue. Youmay observe lymphoid tissue surrounding epithelial crypts at the posterior of the tongue; theseare the lingual tonsils . The muscle layer of the tongue is greatly interwoven, facilitating complexmovements.
Slide 66A is a particularly fine section of the tongue showing a circumvallate papilla. Notethe taste buds on the lateral wall of this papilla. You should be able to see a taste pore in a favorablesection. The papilla is surrounded by a marginal cleft into which the ducts of the serous glandsof von Ebner secrete their watery product.
PalateThe hard palate (slide 34B) consists of a bony roof over the mouth with its connective tissueand epithelium. The stratified squamous and cornified epithelium has conspicuous posteriorly-directed folds called rugae. The lamina propria is continuous with the periosteum of the bone.The soft palate continues posteriorly from the hard palate. This transition is visible on slide 34B.Note the difference in the epithelium on the oral side of the soft palate, and on the nasal side.For further explanation of the palate refer to the lab exercise on the respiratory system.
Salivary GlandsThe three major salivary glands are parotid gland (slides 67A ), the submandibular gland (70A-72A) and the sublingual gland (74A).
Parotid GlandThe parotid gland is described as a “pure serous” gland, but it does secrete some glycoproteins.Two classes of ducts are readily visible: the interlobular ducts which occur in the connectivetissue septa, and the intralobular ducts surrounded by acini. Note the relationship of thevasculature to these ducts. Myoepithelial cells (basket cells) are particularly evident on theducts and acini which have been superficially “nicked” in the plane of section. The nuclei ofthese contractile cells are spindle-shaped. Distinguish the secretory striated ducts and theintercalated ducts. Both of these ducts are intralobular in location. The basal striations of the
ORAL CAVITY

77
striated duct are best seen in slide 67A. What causes the striation and what is its functionalsignificance? Accumulation of fat cells in the connective tissue septa is characteristic of theparotid gland.
Submandibular GlandThe submandibular gland is a mixed gland having both serous and mucous components,
though it is largely serous. The alveoli are either entirely serous, or they are mucous with acrescent-shaped patch of a few serous cells (called serous demilunes and best seen in slide72A). In slide 70A, the mucous cells show a strongly positive response to PAS. Slides 7lA and72A are good for studying the ducts. You will find all of the types of ducts that you found inthe parotid glands, except that in the submandibular gland, the striated ducts are longer, andthus more frequently observed. The intercalated ducts are quite short. Note the abundanceof lymphoid tissue around some of the ducts in slide 7lA.
Sublingual GlandThe sublingual glands (74A) are mixed glands that are largely mucous, with some areas beingentirely mucous. Serous demilunes, separated from the lumen by mucous cells, are frequentlyfound. The gland lacks a capsule. The secretory portions of the ducts are very short and,therefore, rarely seen; the striated ducts are not found at all.
ORAL CAVITY

78

79
The alimentary tract consists of a basic structural plan throughout its length. From the lumenoutward this includes mucosa, submucosa, muscularis and adventitia. The mucosa differs ineach segment and is, hence, useful for identification. It is subdivided into a superficial epithelium,lamina propria, and a thin muscularis mucosae . The epithelium is often elaborated into glandsextending into the lamina propria, which often contains accumulations of lymphocytes. Thesubmucosa is a connective tissue layer containing blood vessels. The muscularis may bedifferentiated into as many as three layers, characterized by the orientation of the muscle fibers.The thin adventitia is often lost during preparation of the sections.
EsophagusSlides 75A and 76A. Beginning from the lumen there is: l) a thick stratified squamous epitheliumwith a papillated lower border; 2) a thin lamina propria with an occasional accumulation oflymphocytes; 3) a broad muscularis mucosa consisting of longitudinal muscle fibers; 4) thicksubmucosa with an abundance of elastic fibers; 5) a muscularis externa having an inner circularlayer and an outer longitudinal layer. At what level of the esophagus were these sections taken?Slide 75A may include ducts or secretory cells of the submucosal mucous glands.
StomachSlide 77A is a longitudinal section of the junction of the esophagus and stomach. The transitionfrom stratified squamous to simple columnar epithelium of the gastro-intestinal tract is abrupt.The stratified squamous epithelium of the esophagus may appear uncommonly tall because ofthe oblique plane of section. For the same reason, the gastric pits may appear as small roundpink-lined holes rather than tubes. These pits lead to the cardiac glands . The surface mucouscells cover the entire surface of the stomach and line the pits. These cells are stained pink inslide 77A, due to the presence of mucus.
Terminology for Glands of the StomachThe terminology with regard to glands of the stomach is somewhat confusing. For example, theterm gastric glands might be thought to indicate that these glands occur throughout the stomach,whereas they are absent from a narrow zone around the cardia and from the lower part of thepyloric region. A synonym (fundic glands) is even more misleading, for it indicates that theseglands are limited to the fundic region, whereas they are much more widespread. We can considerthat there are three types of glands: l) gastric glands , distributed throughout the greater partof the gastric mucosa; 2) cardiac glands , found in the cardiac region of the stomach near itsjunction with the esophagus; and 3) pyloric glands , confined to the region immediately abovethe pylorus.
Gland Cell TypesChief cells are probably so-called because they are the most numerous gland cell. Thesignificance of “parietal” is more obscure. The word means a wall surrounding a cavity or volume.
Esophagus and Stomach

80
In ordinary fixation techniques, the zymogen granules of chief cells are not well preserved.Thus, these protein-rich cells have an unexpectedly empty or foamy interior, in contrast to thedenser and more uniform parietal cells, where the mitochondria and other internal membranes(visible in stomach EM #5) are numerous and more readily preserved. In better preservedmaterial, chief cells will clearly show many large, moderately dense granules and a basalbasophilic region as the result of extensive rough endoplasmic reticulum (see stomach EM #5)and the nucleus. Parietal cells will show numerous, much smaller granules that prove to beacidophilic mitochondria, surrounding a central nucleus.
Slide 78A is a cross section of the fundic stomach, which shows the branched tubular gastricglands which open into the gastric pits . You should be able to find the surface mucous cells ,parietal cells and chief cells . The neck mucous cells occur at some distance below the surfacemucous cells, and contain a distinct type of mucigen granules as can be seen in stomach EMs#l and #2. Neck mucous cells are easily seen only in the PAS-stained part of slide 80A. Thelamina propria is relatively thin between the gastric glands, but contains smooth muscle cells(as well as most of the usual connective tissue elements). The muscularis mucosae consistsof an inner circular and an outer longitudinal layer, and is closely applied to the lamina propriaat the bottom of the gastric glands. The submucosa contains blood vessels, nerves andlymphatics. The muscularis externa consists of three muscle layers: an outer longitudinal, amiddle circular, and an inner oblique. Slide 80A is an exceptionally thin preparation of mucosafrom the fundus. The gray, iron hematoxylin stained section shows the mitochondria (black)of the cells. Mitochondria are particularly abundant in the parietal cells, which stand out rathernicely in this preparation (Some of these preparations contain spirochetes). The blue stained(PAS) portion of the slide makes it easy to distinguish virtually all of the cell types of the gastricglands, including the neck mucous cells (which are violet, compared to the blue of the surfacemucous cells). This section was cut from plastic-embedded material with the ultramicrotome,and is extremely thin. The same is true for the section on slide 79A. This H & E section isparticularly good for studying the composition of all the layers of the stomach. Several typesof enteroendocrine cells are evident in this section. These cells are located in the bottom endsof the glands, and have a scattering of small eosinophilic granules in a relatively clear cytoplasm.These cells are part of the glandular epithelium and, as such, occur within the surrounding basallamina which they face; this can be seen in stomach EM #4. Enteroendocrine cells should notbe confused with mast cells, which have many large red granules and occur in the lamina propria.
ESOPHAGUS AND STOMACH

81
DuodenumSlide 83A shows the abrupt pyloroduodenal junction in longitudinal section. Note how muchdeeper the gastric pits are in the pyloric mucosa than in the mucosa of the fundus. The pyloricglands, like the cardiac glands, are of the mucous type. Many solitary lymph nodules are evidentin this region. Note the large circular sphincter muscle at this junction. The muscularis mucosaeappears to ride up over the Brunner’s (duodenal) glands , and comes to lie just under the cryptsof Lieberkuhn. The muscularis mucosae does break up, however, and send branches downaround the glandular elements. The slide also contains sections of lymph nodes and pancreas.Both the pyloric glands and the Brunner’s glands are mucus secreting (mucin stains pink). Alsonote the abundance of goblet cells in the mucosa. Low broad villi are observed for the first timein the duodenum. The microvilli (striated border) on the absorptive epithelia are coated with PAS-positive material. Neurons and nerve fibers of the myenteric (Auerbach’s) plexus can beobserved between the inner circular and outer longitudinal muscle layers throughout the smallintestine. For a whole mount view of this plexus, see slide 93A.
Note in studying the slides for this laboratory that the epithelium of the villus containsabsorptive cells, goblet cells and enteroendocrine cells . In the epithelium of the crypt or gland,Paneth cells are located at the bottom of the crypt, and are most numerous in the duodenum andjejunum, less frequent in the ileum and absent in the colon. The duodenal cell types are mostclearly distinguished in the plastic section 87A. Above the Paneth cells are the stem cells (someof which may be seen dividing), and above them are cells in the process of differentiating intoabsorptive and goblet cells. Lymphocytes may be found scattered throughout the lamina propriaof the villi at all levels.
JejunumIn the jejunum (85A), goblet cells are much more abundant than in the duodenum. There are alsoeosinophilic Paneth cells at the bottom of the crypts of Lieberkuhn. Lymphocytes are abundantbetween the epithelial cells of the absorptive mucosa. The plastic section 86A is best forstudying some of the finer structural details (e.g., the entire length of the goblet cell often canbe seen, the striated border is well preserved, and the Paneth cell granules are nicely shown).The size of these granules can be contrasted with those of mast cells which are easily found withinthe muscle. Look for mitotic figures in the crypts on slide 86A. Some of the villi may havestreamers of exfoliated cells at the tip, indicating the location of the extrusion zone.
IleumThe ileum (slides 88A and 9lA) is distinguished by its few short, club-shaped villi and poorlydeveloped plicae. As one proceeds through the small intestine, there is an increasing numberof goblet cells; thus, the lining of the ileum contains a large number of them. Aggregates oflymphatic nodules (Peyer’s patches) are particularly abundant in slide 9lA of the ileum (Slide9lA is from a cat and contains globular leukocytes, a cell type not found in man). These cellshave small dark nuclei and large eosinophilic granules and are of uncertain function. The striatedborder, goblet cells, enteroendocrine cells and some Paneth cells can be seen in the plasticsection 88A.
Intestine

82
ColonSlide 94A The colon differs histologically from the small intestine in that it lacks villi, havingonly tubular pits for glands (glands of Lieberkuhn). We can observe that the number of gobletcells is continuing to increase as we go down the alimentary canal. Paneth cells are rare. Thesubmucosa contains some fat cells. There are numerous solitary nodules of lymphatic tissue.The outer longitudinal layer of the muscularis is grouped into three thick bands (taeniae coli),parts of which will be visible in your slides. This is not to imply, however, that there is nolongitudinal muscle between the taeniae. Longitudinal fiber bundles from the taeniae can beobserved to interrupt the circular layer.
AppendixThe appendix (96A) has a relatively small lumen. The mucosa is only slightly folded and hasan epithelium which is largely goblet or mucous cells. The abundance of lymphatic nodules isthe most striking feature. The muscularis mucosa is poorly developed.
RectumSlide 95A The glands of the rectum consist almost entirely of goblet cells. The longitudinaland circular layers of the muscularis are uninterrupted.
Recto-anal JunctionSlide 99A It has been a long way since we left the integument at the vermilion border of the lipuntil we pick it up again at the anus (about 9 meters actually). The epithelium changes abruptlyfrom the simple columnar epithelium we have observed in the whole gastro-intestinal tract, toa stratified cuboidal and then, finally, cornified - stratified squamous epithelium of the anus.Goblet cells are very abundant in the long broad glands of Lieberkuhn of the rectum. Theintegument of the anus contains hairs with sebaceous glands, eccrine sweat glands and thecircumanal glands which are similar to the apocrine sweat glands that you observed in the axilla.The circumanal glands are not present in all the slides; you may have to look at a neighbor’spreparation.
Electron MicrographsThe apical surface of columnar absorptive cells of the intestine have numerous microvilli. Thevery regular nature of the microvilli accounts for the striated border seen in the light microscope.The glycoprotein coat (“fuzz”) present on the microvilli accounts for the intense PAS stainingof the apical surfaces, as seen in your light microscope preparations. Mitochondria are rathernumerous in the columnar absorptive cells. Granular endoplasmic reticulum is not welldeveloped, but agranular ER is often conspicuous in the apical cytoplasm.
The apical cytoplasm of intestinal goblet cells is filled with mucigen droplets. The granularendoplasmic reticulum is extensively developed in the basal and perinuclear cytoplasm. Incontrast to the absorptive cells, the apical border of goblet cells has only a few microvilli.
INTESTINE

83
Exocrine Pancreas(Slides l0B-l2B)
The exocrine portion of the pancreas can be seen in all the slides. The pancreatic tissue in generalis surrounded by an accumulation of fat. The human pancreas also contains much connectivetissue, which separates the exocrine portions into lobules. The exocrine portion of the pancreasis a compound tubuloalveolar gland composed of serous secretory units. Note the location ofthe zymogen granules in the apical portion of the cell and the intense basophilia in the basalportion. This is nicely shown in the H & E stained plastic section (l2B).
Duct SystemThe lumen of each pancreatic acinus is continuous with a small duct called the intercalated duct.This duct is distinguished by its pale staining simple cuboidal cells (which often extend into theacinus itself) as individual pale-staining cells called centroacinar cells . These ducts aretributaries of larger interlobular ducts, lined by columnar epithelium containing a few gobletcells. The interlobular ducts, in turn, join the two main pancreatic ducts. Many 83A slides havea large section of pancreas, in which the goblet cells of the major ducts are clearly seen.
Endocrine PancreasIdentify the pancreatic islets. Differentiation of the alpha, beta and delta cells is not possiblein H & E stained sections. In the aldehyde fuchsin stained pancreas, the beta cells (whichsynthesize insulin) have fine purplish stained granules. The alpha cells (which synthesizeglucagon), have a yellowish appearance in these islets. This stain permits one to identify smallgroups of isolated beta cells in the pancreas. Delta cells cannot be identified in thesepreparations. The rich blood supply to the islets is difficult to see but, in an ideal section, underoil immersion, the capillaries can sometimes be distinguished.
Electron MicrographsIn your microscope slides, pancreatic exocrine cells were characterized by the zymogen granulesin the apical cytoplasm while the basal cytoplasm was strongly basophilic. In the electronmicrographs, numerous dense zymogen granules are present in the apical cytoplasm, while thebasal cytoplasm contains extensive granular endoplasmic reticulum indicative of active proteinsynthesis. Centroacinar cells are readily identified by the low density of their cytoplasm, andthe paucity of cell organelles, as well as by their position.
Pancreas

84

85
LiverThe basic functional unit of the liver is the acinus, but the classical lobule is usually the easieststructural unit to discern. The connective tissue capsule (Glisson’s capsule) which surroundsthe liver is continuous with some of the connective tissue of the portal canals. In the human(and many other mammals) this connective tissue incompletely separates the lobules, whereasin other animals (such as the pig), it completely separates each lobule. The hepatic lobule hastwo main constituents: an epithelial parenchyma made up of hepatic cells arranged inanastomosing plates or sheets, and a system of blood channels. The blood supply to the liveris unusual in that a portion of it is a PORTAL SYSTEM. A portal system is one in which blood,after being collected from one set of capillaries, passes through a second set of capillary-likevessels before it returns to the systemic circulation. In the hepatic portal system, blood collectedfrom the capillaries of the stomach, most of the intestine, the pancreas and the spleen isconducted by way of the portal vein to the liver, where it passes through the sinusoids beforeentering the inferior vena cava (by way of the hepatic veins).
In the slides which follow, note the portal tracts (also known as portal triads or portal canals).
Contents of the portal tract
l Preterminal (interlobular) branches of the portal vein
2 Preterminal (interlobular) branches of the hepatic artery
3 Branch of the bile duct (lined by cuboidal epithelium) all in a commoninvestment of connective tissue which may, in addition, contain lymphat-ics. From these branches of the portal vein and hepatic artery arise theterminal branches.
These, in turn, empty their blood into the hepatic sinusoids which, in turn, empty into thecentral veins (the terminal branches of the hepatic vein). Note that preterminal branches areparallel to the central vein and terminal branches are perpendicular.
In slide 5B of the liver, the blood supply of the liver is delineated by dye injected into the vascularbed. Central veins may be identified as the dense red areas from which sinusoids radiate towardthe periphery of the lobules. After studying the terminal branches of the portal vein in thissection, you should have little trouble discerning the acinar arrangement in a section ofnoninjected liver.
Now study slide 2B, (human liver). Note that although a complete connective tissue capsuleis lacking for each lobule, the lobules can nevertheless be defined by the presence of the centralvein in the center and the portal triads at the periphery. Note also the characteristic pattern ofthe parenchymal cells in this, and other slides, and their relation to sinusoids .
Slide 3B is from a dog injected in vivo with carbon black, and slide 4B is from a rat injectedwith Trypan Blue. These substances are taken up by the phagocytic Kupffer cells, which areclearly identified. Note the variation in shape of Kupffer cells from flat, squamous-like cells tolarge ones which bulge into the lumen. In slide 4B, tissue macrophages in the interlobular CThave also phagocytosed the dye.
Slide 3B also shows good lobulation, dilated sinusoids, prominent nuclei and nucleoli of liver
Liver and Gallbladder

86
parenchyma. Compare nuclear size and number in liver cells on slide 3B.The thinner plastic section (7B) is best for studying cellular detail. In the sinusoid wall,
Kupffer cells can be distinguished from endothelial cells by the abundance of granules(lysosomes) resulting from the greater phagocytic activity of the Kupffer cell. In perisinusoidalspaces, you will observe a number of cells with vacuoles which represent areas of extracted fatdroplets; these are “fat-storing cells” which are stellate in shape. They tend to be morenumerous in intermediate and peripheral portions of the lobule than in central zones. Theirfunctional significance is not yet understood but it is known that vitamin A may accumulate inthe lipid droplets. Circulating white blood cells are nicely shown; the neutrophils appear smallerbecause they have been sectioned (rather than spread out, as in a smear). Using oil immersion,search the membranes between adjacent liver cells for evidence of bile canaliculi, which areminute canals formed by the membranes of two adjacent cells. The cell membrane delineatingthe bile canaliculi can be stained with silver; look at slide lB to see areas where canaliculisurrounding individual liver cells are stained in this manner. What do you notice about the sizeof parenchymal cell nuclei?
Slide 6B is a section of regenerating rat liver and, consequently, shows an unusually largenumber of mitotic figures. The variability in size of the parenchymal nuclei reflects the varyingdegree of polyploidy present in the mammalian liver. Although all of the parenchymal cells ofthe mammalian liver are diploid at birth, 80% of the nuclei are tetraploid by the time the animalhas reached maturity. Note also the cytoplasmic basophilia evident in the cells.
GallbladderBegin your study of gallbladder with slide 9B. Note that the mucosa is thrown into numerousfolds (which probably are not present when the gallbladder is distended), and has a tall columnarepithelium. This epithelium is responsible for reabsorption of much of the water from thecontents of the gallbladder. A layer of smooth muscle and associated collagen and elastic fiberssurround the gallbladder. The epithelium rests on a lamina propria of loose CT; there is no truemuscularis mucosae. There is often a layer of fat cells between the underlying connective tissueof the serosa and the muscular layer.
The plastic section of gallbladder (8B) is a circle-shaped transverse section displaying thethree layers: (l) mucosa, a simple columnar epithelium situated upon a lamina propria; (2) a thinmuscularis coat of interlacing bundles of smooth muscle; and (3) an adventitial outermost coatof irregular connective tissue containing nerves, blood vessels, and scattered adipose cells.Where the gallbladder is not overlain by liver tissue, a serosa is present. In the lamina propriaare a conspicuous number of capillaries, mast cells, and, in these slides, a great abundance ofplasma cells. Is a striated border present on the epithelial cells? Do not spend much time studyingthe muscularis which is difficult to discern in certain areas; its extent can be best appreciatedat low magnification.
Electron Micrographs of LiverIn the electron micrographs identify the hepatic sinusoids . Note the thin lining of these vessels.The space of Disse lies between the cells lining the sinusoids and the surface of the liverparenchymal cells. Numerous irregular microvilli project from the surface of the liver cells intothe space.
LIVER AND GALLBLADDER

87
Within the hepatic cells are dense accumulations of glycogen, numerous mitochondria andboth granular and agranular ER. Some micrographs may also show some crystalloid-containingmicrobodies (peroxisomes). Also identify bile canaliculi; note that a canaliculus is merely anexpansion of the intercellular space rather than a completely separate duct. The juncture of abile canaliculus with a branch of the bile duct is shown on one of the micrographs.
LIVER AND GALLBLADDER

88

89
KidneyThe kidney is a highly-organized structure, whose morphology is more obviously related to itsfunctional activity than in many other organs. The arrangement of the cortex of the kidney canbe clearly seen in slide 43B (unilobar kidney, rabbit). Portions of the medulla extend into thecortex as medullary rays; a medullary ray surrounded by its immediate cortical substanceconstitutes a lobule. The cortex, with its medullary pyramid, is called a lobe. Portions of the cortexextend downward between the medullary pyramids. On most of your slides, the continuity ofthese medullary rays with the medullary tissue extending to a minor calyx (at the apex of apyramid) can be seen. However, only a few of the slides will actually show the area cribrosawhere the papillary ducts open into the minor calyx.
Blood SupplyThe general pattern of organization of the kidney blood vascular system is not readily apparent.To simplify identification of all the blood vessels, look for them at the lowest magnification, andalso try to find continuities from one type to another. Be sure to distinguish the arteries fromthe veins as you follow them in the kidney. Continue with slide 43B, but also turn to 46B asnecessary. Find the corticomedullary junction and identify the arcuate vessels . Only rarely isthe section in a plane which permits the arcuate vessels to be observed in longitudinal section.However, multiple cross sections of these vessels can be seen ranging in depth from the edgeof the cortex to about a third of the distance into the cortex from the medulla. Interlobar vessels(from which the arcuate vessels arise) are larger and may be surrounded by connective tissuein contrast to the arcuate vessels; the interlobar vessels leave the connective tissue space, enterthe renal columns and course towards the corticomedullary junction, where they branch intoarcuate vessels. Radially directed interlobular vessels are readily seen in a number of the slides(particularly 43B and 46B). The afferent arterioles arise from interlobular arteries and enterthe renal corpuscle as the glomerular capillaries. The peritubular capillaries arise from efferentarterioles which exit from the cortical glomeruli (at some distance from the medulla), whereasthe vasa recta arise from the efferent arterioles of the more juxtamedullary glomeruli. These canbe seen accompanying the loops of Henle and collecting tubules in the medullary portions. Lookfor peritubular capillaries and vasa recta in the sections from injected animals (43B, 46B). Howdo peritubular capillaries differ in their fine structure from glomerular capillaries? The vasa rectahave a counter current arrangement which plays an essential role in the formation of a hypertonicurine.
Renal Corpuscle & JG CellsThe detailed histology of the kidney (including glomerulus , nephron, and collecting tubules),can be seen most readily in the injected rabbit kidney (slide 46B), and in the plastic section (44B).Study the structures first in slide 46B and then more closely in slide 44B. At the vascular poleof the renal corpuscle is the juxtaglomerular apparatus. This consists of a portion of theafferent and efferent arterioles (along with associated mesangial cells ) in intimate contact witha specialized portion of the distal tubule (the macula densa, see below). Juxtaglomerular cellsare modified smooth muscle cells in the wall of the afferent arteriole and can be seen to containgranules (which are known to contain renin). These granules, visible under oil immersion, arePAS-positive (46B), but may also be stained after H & E alone (44B). You may find them moreeasily in slide 46B, but don’t spend too much time searching for them. The parietal layer of
Urinary System

90
Bowman’s capsule is readily apparent. Mesangial cells cannot be distinguished in this type ofpreparation, but can be seen in appropriate EMs. The relationship of the foot process of thepodocytes, the sieve areas of the endothelial cells and the basement lamina of the glomerulusshould also be studied in appropriate EMs. What layers does the glomerular filtrate cross in itspassage from the blood stream to the urinary space?
Tubular NephronThe conduit pathway of the nephron consists of the space between the visceral and parietalwalls of Bowman’s capsule (the visceral wall of podocytes being closely applied to theglomerular capillary), the proximal convoluted tubule, the loop of Henle, and the distal convolutedtubule. The latter ends by joining a collecting tubule. The straight descending portion of theproximal tubule and the straight ascending portion of the distal tubule, together with the thinwalled recurrent tubule which joins them, constitute the hairpin-shaped conduit segment knownas the loop of Henle. The straight portions are sometimes called descending or ascending limbsof the loop. The predominant type of tubule near the glomeruli is the proximal convoluted tubulewhich is distinguished by greater thickness of the cells, eosinophilic cytoplasm, and PASpositive material in the brush border (46B). In scattered areas in certain slides, more distalportions of proximal convoluted tubules contain very large PAS-stained granules; thesegranules are presumed to be greatly enlarged lysosomes, specifically telolysosomes or brownishlipofuscin pigment granules. Electron micrographs of these cells reveal not only the brushborder, but also many absorption tubules and lysosomal derivatives. PAS positive material canalso be seen in the thick segments of the descending loops of Henle. The thin segments of theloops of Henle generally show only three or so nuclei in cross section, and the cells are lowcuboidal to squamous in shape. These cells are not as flat as the endothelial cells of the vasarecta and, hence, their nuclei do not bulge into the lumen as those of endothelial cells do. Thischaracteristic is particularly well shown in 44B.
The ascending loop undergoes a transition from a thin to a thick segment well before it entersthe distal convoluted tubule. If you carefully examine cross sections of the tubules in the medullaon slide 46B, you will note that ascending thick segments and thin segments are numerous, butyou will find few descending thick segments. How can you account for this? It may help youto make a longitudinal drawing of the loops of Henle in the medulla. The wall of the distalconvoluted tubule is modified in the area of apposition to the vascular pole of the glomerulus(specifically, the afferent arteriole); this modification is known as a macula densa, a region inwhich the nuclei of the distal convoluted tubule cells appear more crowded and elongated (46B).A characteristic feature of distal convoluted tubule cell (as well as of proximal convoluted tubulecell) fine structure is the interdigitation of basal folds containing prominent mitochondria. Theseinfoldings (plus aligned mitochondria) account for basal striations.
Collecting DuctThe point of passage of the distal convoluted tubule into the curved collecting tubules may bedifficult to find in histological preparations. Straight collecting tubules (in medullary rays) canbe distinguished from the proximal and distal tubules, in part, by the visibility of the lateral cellborders and the regularity in the spacing of nuclei. The tubule wall is composed of two cell types,“light” and “dark” (44B). The light cells are more numerous and appear gray; the less numerousdark cells stain pink, presumably because of the higher number of mitochondria. Dark cells arenot seen in the papillary region. On slide 46B, the region where the collecting tubules come
URINARY SYSTEM

91
together to form papillary ducts can be seen only in cross section.
Immature KidneyExamine the kidney sample in slide l7B, which is very immature and, thus, simplified in structure.Here the nephron is shorter and the glomerulus is smaller. The metanephric nephrons of thisfetal human kidney show many stages of development. Look for different stages in thedevelopment of the renal corpuscle. You will see examples where the visceral layer of thecorpuscle is just beginning to invaginate and develop into podocytes. The loops of Henle arestill quite short, and many have not extended down into the medulla.
Ureter & BladderExamine the ureter (48B) and bladder (5lB, 67B). The lining epithelium of these structures istransitional epithelium. This epithelium, unique to the urinary system, is well suited to therequirement for dramatic expansion and contraction. Most of the examples you will see in theseslides are highly contracted and folded. In a distended epithelium, the cells become greatlyflattened parallel to the surface, with the consequence that the layer of transitional epitheliumis thinner. One of the two sections on slide 5lB is from a stretched bladder and one is from arelaxed bladder. It is this ability of transitional epithelium to change in morphology withstretching that gives it its name. Some of the superficial transitional epithelial cells contain twonuclei; it is known that there is a progression from diploidy to octaploidy as you approach theepithelial surface. The nature of the granules present is not known. There are no true glandsin these passages of urinary secretion.
Both the ureter and bladder are composed of three layers.
Layers of ureter and bladder
1. Mucosa layer, consisting of transitional epithelium supported by a rela-tively prominent and dense lamina propria. There is no submucosa.
2. Muscularis layer, usually consisting of three layers of smooth muscle in alongitudinal, then circular, then longitudinal orientation.
This is not always visible but this arrangement may be seen on slide 67B (In the upper 2/3 of the ureter, the outer longitudinal layer of smooth muscle is not present). The layers ofsmooth muscle differ from those of the GI tract in that they are penetrated by connective tissueand, thus, are divided into bundles.
3. Adventitial layer, external to the muscularis, composed of irregular denseconnective tissue.
In 67B, peritoneal mesothelium is seen at the abluminal rim; this layer of simple squamousepithelium (plus a thin layer of supporting connective tissue) is termed serosa. Serosa coversthe upper part of the bladder whereas the remainder is covered by a fibrous adventitia.
URINARY SYSTEM

92

93
HypophysisIn all these slides, one should note the rich capillary supply and their close relationship to thesecretory cells of these endocrine glands. In the EM book, do you find evidence of fenestratedcapillaries in these glands?
Slide 26B is a sagittal section of hypothalamus and pituitary of the cat. In this material youcan see part of the third ventricle of the brain, and the infundibular stalk surrounded by parstuberalis (notice the many colloid cysts in this region and the portal blood vessels). Theposterior lobe (pars nervosa) is almost completely surrounded by intermediate lobe (parsintermedia ). A narrow cavity that represents the original lumen of Rathke’s pouch cansometimes be seen between the anterior and intermediate lobes. Both acidophilic and basophilicsecretory cells can be identified in the anterior lobe (pars distalis). The blood vascular bed inthe anterior lobe is of the sinusoidal type.
Slide 23B This human pituitary sample contains anterior, intermediate and a small part ofthe posterior lobe. Note the colloid cysts in the intermediate lobe, and acidophilic and basophiliccells in the anterior lobe. This material was probably obtained at autopsy and, consequently,it shows considerable shrinkage and fixation artifact.
Slide 24B Human hypophysis Masson’s trichrome stain (acid fuchsin, aniline blue, lightgreen). Note the thin capsule of connective tissue that surrounds the gland. Basophils staina deep lavender. Note the number and organization of these cells; most of them synthesize TSHor gonadotropins. The acidophils, which stain reddish-brown, are smaller than the basophilsand have relatively large nuclei. These cells synthesize growth hormone. The chromophobes(the small number of cells that are unstained) synthesize ACTH or represent degranulatedacidophils or basophils.
ThyroidThe thyroid slides show sections of thyroid follicles with their central, homogeneously stainedcolloid surrounded by epithelial cells. Follicles are variable in size. Within the scantinterfollicular connective tissue are found the usual vascular elements, fibroblasts, mast cellsand macrophages.
The abundance of colloid and size (especially the height) of the thyroid follicular cells varywith the functional state of the gland. The C-cells are difficult to identify without special staining(e.g., silver or antibody to calcitonin). In routine stains, the C-cells generally exhibit more lightly-stained cytoplasm, larger size (both whole cell and nucleus), eccentric nuclei, and are charac-teristically located in connective tissue spaces or in abluminal positions within the follicularepithelium. The latter situation is not always clear at the LM level. The best procedure torecognize the C-cells is to first register the staining and size of the numerically dominant follicularcell nuclei and cytoplasm. Then, proceed to identify cells with larger nuclei and less clumpedchromatin surrounded by lighter cytoplasm (relative to the thyroid follicular cells). Find themfirst within the more interfollicular spaces, then in the follicular epithelium.
Slide l3B shows a slightly more active gland. The slight basophilia of the follicular epitheliumis apparent. The C-cell cytoplasm here does not exhibit the same basophilia. In some follicles,there are follicular cells with pyknotic nuclei. These are found even within normal glands. Oneof your EM pictures shows such a “degenerating” cell among other healthy follicular cells.
Slide l4B contains both a section of the thyroid gland and the closely applied parathyroidgland. The parathyroid gland is surrounded by a thin layer of connective tissue that constitutes
Endocrine System

94
its only separation from the thyroid gland. The cells of the parathyroid are relatively uniformin size, with nuclei smaller and more basophilic than those of the thyroid cells. There are nooxyphils in the dog parathyroid gland.
The follicles are lined by cuboidal to low columnar cells. Careful examination may reveal somephagocytosed colloid within these cells. The vacuoles in the pink colloid are fixation artifacts.Occasionally, “C” or “calcitonin” cells can be found in the interfollicular spaces or wedgedbetween two follicular cells. With the slightly different stain combination used on this slide, thecytoplasm of some C-cells are slightly more orangish pink than other C-cells and the follicularcells. If you apply the criteria of size, nuclear staining and location suggested above foridentifying C- cells, you will successfully distinguish them from the follicular cells.
Slide l6B shows a highly active thyroid. Much of the colloid has been mobilized; some hasbeen lost during fixation. As the result of both colloid depletion and hypertrophy (andhyperplasia) of the follicular cells, the epithelium shows infolding. There is also vascularengorgement accompanying the increased glandular activity.
ParathyroidThe section of human parathyroid on slide 22B shows many oxyphils scattered throughout thegland and much fatty tissue. What does that tell you about the age of the ex-owner of the gland?The oxyphils are easy to spot, due to their smaller nuclei and their more abundant andeosinophilic cytoplasm. The increased acidophilic staining is due to what organelle within theircytoplasm? Sometimes similarly stained cells can be seen in pathological thyroid glands. Thesealso exhibit greatly increased numbers of the same cytoplasmic organelle. They are referred toas oxyphils also, or as “Hurthle cells.”
Adrenal GlandSlides l9B and 20B demonstrate the histologic organization typical of the adrenal in mostmammals. The gland is covered by a connective tissue capsule, which contains many branchingarteries and nerve fiber bundles. Some sections may contain cross sections or oblique sectionsof the preganglionic nerve fibers coursing through the cortex to innervate adrenal medulla cells.The cortex is not innervated. Most of the capsular arteries branch and enter the cortex in theform of fenestrated capillaries. Some of these capillaries may be collapsed; others distended withred cells. The capillaries extend from the zona glomerulosa to the cortico-medullary junction,and enter into the medullary bed via a few small vessels. In slide 20B, you may find an exampleof a medullary artery that goes directly from the capsule to the medulla without branching. Themedulla receives blood indirectly from the cortical capillaries and directly from the medullaryarteries. Note the large branches of veins which eventually anastomose with the large centralveins in the medulla. The cortex is divided into three zones: glomerulosa, fasciculata andreticularis . Note the size, shape, and organization of the cells in the three zones. Which zoneis the largest? Are the zones easily identified?
ENDOCRINE SYSTEM

95
Adrenal MedullaThe adrenal medulla in the central portion of the gland (slides l9B and 20B) contains largepolyhedral-shaped cells (often referred to as pheochromocytes because they react with chromesalts to give the chromaffin reaction). The cells are arranged in cords or aggregates which aresurrounded by capillary networks. Preganglionic sympathetic nerve fibers (which penetrate themedulla) synapse with the pheochromocytes, which are thus homologous with sympatheticganglion cells. On careful inspection, one can see a small number of sympathetic ganglion cellsscattered among the adrenal medullary cells.
ENDOCRINE SYSTEM

96

97
TestisSlide 54B, of the monkey testis is particularly useful for studying the organization of the testis.Under low power, the parenchyma of the testis is seen to consist of coiled seminiferous tubules,separated in groups from one another to form lobules bounded by septa of connective tissue.These lobules appear to radiate from the mediastinum testis, a region of vascular connectivetissue, which lies close to and parallels the epididymis (However, since your section is not ina precise mid-sagittal section, the mediastinum will be internal and to one side). Within themediastinum is the rete testis , a labyrinthine system of large spaces lined by a simple cuboidalepithelium. The rete is continuous with the seminiferous tubules via straight tubules whichcourse within the septa. The junctions of the straight tubules with the seminiferous tubules aredifficult to find. The straight tubules are lined by a simple cuboidal epithelium. Note the plexusof venules which is also located within the mediastinum.
The rete testis is drained by ductuli efferentes. These are not present on your slides. They leadto the tortuous epididymis (a highly-coiled tubule lined with a very tall pseudo-stratifiedcolumnar epithelium, whose cells have the long microvilli classically called “stereocilia”). Findalso the ductus deferens characterized by a larger lumen, a lower epithelium which shows afestooned outline and an appreciable amount of smooth muscle. Masses of spermatozoa anddesquamated cells of the seminiferous epithelium will be seen within the lumina of the epididymisand ductus deferens.
Male Reproductive System

98
MALE REPRODUCTIVE SYSTEM
Interstital TissueThe relative and absolute amounts of interstital tissue show wide variations among mammals.In slide 55B, from an adult monkey, interstitial cells are present in small clusters. The foamyappearance of the cytoplasm of the inerstitial cells results from the extraction of lipid duringhistological preparation.
Seminiferous TubulesThe seminiferous tubules (slides 54B and 55B), because they are coiled, will be seen cut atvariuos angles to their long axes. Enveloping the basal surface of the tubules are cells withelongated cork-screw shaped nuclei which belong to the myoid layer. In many instances,however, these nuclei cannot be distinguished from those of immediately adjacent fibroblasts.The plastic section (55B) is especially good for studying spermatogenesis. The seminiferousepithelium varies considerable in appearance depending upon the particular stage of thespermatogenic cycle as well as the plane of section of the specific tubule. Begin by identifyingcells in various stages of spermatogenesis and then consider the entire epithelium with respecttothe grouping of cells undergoing spermatogenesis in various segments of the seminiferoustubules. In this type of material, it is not possible to identify every cell, but it is possible to identifytypical expamples of most cell types.
Sertoli CellsThe nuclei of Sertoli cells tend to be elongated and folded and to contain a large prominentnucleolus. The scanty heterochromatin of Sertoli nuclei is frequently seen as elongated threadsparallel to the nuclear long axis. The highly branches and attenuated cytoplasm is not usuallydiscernible but when seen appears as tufts of acidophilic cytoplasm. The cell nucleus generallylies adjacent but perpendicular to the boundary layer or among the primary spermatocytes. Lookfor Sertoli cells in slides 54B, and 55B.
SpermatogoniaVirtually all nuclei located at the base of the epithelium which are not in Sertoli cells arespermatogonial. Typically, these nuclei are large and contained either distinctly stainedchromatin or large chromatin masses representing poor fixation of mitotically dividing cells. Youmay be able to distinguish light and dark spermatogonia.
Primary SpermatocytesThese cells are located in 2 or3 layers central (luminal) to the spermatogonia and contain muchlarger nuclei than those of the spermatogonia. The nuclei exhibit various stages of the prophaseof the first meiotic division.

99
MALE REPRODUCTIVE SYSTEM
Secondary SpermatocytesThese cells are appreciably smaller than primary spermatocytes. They are much less frequentlyseen because of the relatively short duration of this stage compared to others. It is not worthwhilesearching for these cells unless you have a special interest in spermatogenesis.
SpermatidsMost tubules contain two generations of spermatids. The younger generation lies adjacent tothe spermatocytes, and consists of cells with rather small nuclei containing a uniform dispersionof chromatin. The second generation of spermatids consists of maturing spermatozoa (recognizedby the dense chromatin of the nucleus) which forms the head of the spermatozoan. intermediatestages are easily identified. Note that for any given stage of spermiogenesis, there is the sameset of stages in that portion of the tubule.
Locate a region of the tubule that contains early spermatids adjacent to primaryspermatocytes near the basal side. Find the acrosomal granule, a small eosinophilic organellebeside the nucleus. Does the granule face the basal or adluminal side? Which way does theacrosome face in the mature spermatids?
The structure of sperm per se is better appreicated in electron micrographs, as is theassociation of the acrosome with the Golgi region in spermatids, and the mitochondrialdifferences between Sertoli cels and the germ cell line.
Accessory Reproductive Structures
ProstateSlides 64B and 63B. The prostate consists of 30 to 50 compound tubuloalveolar glandsabout the prostatic portion of the urethra (64B), in a bed of dense fibroelastic connectivetissue containing appreciable amounts of smooth muscle. Each gland is lines by a simplecuboidal or columnar epithelium in some regions and more often by pseudostratifiedepithelium in others. It is continous with the urethra at the sides of the colliculus seminalis(verumontanum), a longitudinal eminence in the posterior wall of the p rostatic urethra. Thesecretion of the prostate frequently (and normally) collects in the lumen of the gland as aneosinophilic onion-like mass termed a concretion. Such concretions are often found inseminal fluid and may calcify in situ. The relationships of the prostate are best send in slide64B. The ejaculatory ducts are not present on your slides. EMS of the prostatic cells showthe abundant RER of typical protein exporting cells. Slides 65B is a plastic section of theprostate of a young monkey, which is a much more active-looking gland than the olderspecimens we hve seen. In particular, it lacks the distended alveoli and concentrationswhich seem to accompany aging. The tall columnar shape of the secretory cells and theirnumerous apical secretory granules suggest that this is an actively secreting gland.Surrounding the tube-alveoli is a fibroelastic stroma containing smooth muscle cells (whichis a characteristic feature of this gland). The smooth muscle cells stain bright red while theelastin is conspicous by its lack of stain.

100
MALE REPRODUCTIVE SYSTEM
Prostate Gland: Slide 64B
Spermatic CordThis slide (59B) shows the contents (not the coats) of the spermatic cord (the bloodvessels are extraordinarily thick-walled in this sample). In this slide the three layers ofmuscle in the ductus deferences may be seen.
Seminal VesicleThe seminal vesicles (slide 61B) are saccular outgrowths of the ductus deferens.The individual saccules have a highly folded mucosa which further subdivides thecontinous lumen of these organs. However, since all of the pockets of the lumenthus formed communicate directly, the folding consitutes an increase of surface ofthe mucosa rather than separate glands. The epithelium of the mucosa of theseminal vesicles is generally considered to be columnar to pseudostratifiedcolumnar. Pigment can occasionally be seen in the epithelial cells. Note theabundance of smooth muscle beneath the mucosa. Slide 60B of monkey seminalvesicles is a plastic section which shows the well preserved (and highly secretory)columnar epithelium of this gland. Note the numerous sperm that have foiund theirway into the labyrinthine lumens of this gland.
Bulbo Urethral Gland

101
MALE REPRODUCTIVE SYSTEM
Examine briefly this compound tubuloalveolar gland (62B). The tubular nature of some at theglandular endings is apparent, but that it secretes a polysaccharide-rich secretion is lessobvious. This section does not contain the urethra.
PenisSlide 66B. The following structures can be seen on this slide: corpora cavernosa, septum,tunica albuginea, corpus spongiosum, dorsal vein, central arteries, helicine arteries,numerous nerves, and the penile urethra.

102

103
Female Reproductive System
OvaryIn slide 68B of a monkey ovary, numerous oocytes are seen at the periphery of the ovary. Thecovering epithelium can be seen on the surface of the ovary, underlain by a substantial tunicaalbuginea. When the granulosa cell layer is flattened and only one cell layer thick, the folliclesare primordial follicles; when the granulosa cells become cuboidal and prolierate rapidly to forma stratified epithelium, the follicles are called primary follicles. Secondary follicles (containinga fluid-filled cavity -- the antrum) are numerous in this ovary. The larges follicles which approachovulation are termed Graafian follicles. If there are advanced follicles on your slide, the large,vacuolated, estrogen-secreting cells of the theca interna will be nicely shown in this plasticsection. You may also be able to discern the basement membrane separating the follicle cellsfrom the theca interna. The zonal pellucida is prominent in this preparation; it is seen in bothdeveloping and atretic follicles. Some of the very large atretic follicles (because they appearmainly acellular) may at first appear to be corpora albacantia, but of course the corpora wouldnot contain residual zona pellucida (because the zona would have left with the egg at ovulation).Purple strands in the primary oocyte nuclei are the somewhat condensed chromosomes, arrestedin the meiotic prophase stage. Large lymphatic vessels are clearly distinguishable from theerythrocyte-loaded blood vessels in the ovarian medulla; in particular, distinguish betweenvenules and lymphatic vessels by content and frequency of endothelial nuclei.
The section of corpus luteum of the 25th day of menstrual cycle (slide 69B), illustratesthe folding that occurs in the folidng that occurs in the human corpus luteum and the way in whichthe lutein cells reflect the streaming of the granulosa cells at ovulation. Note also the hyaloidnature of the corpus albicans from a previous cycle. The antral follicles present at this stage areall undergoing atresia. Compare the size of the lutein cells with the granulosa cells of the atreticfollicles. In pregnancy (slide 70B), the lutein cells increase further in size and theca lutein cells(derived fro the theca interna) can be distinguished in clusters at the periphery of the corpusluteum. The follicles (both in the ovary with the active corpus luteum and in the contralateralovary) are in various stages of atresia, except for the primordial and primary follicles.
Many of the stages of follicular development and atresia can be seen in slide 73B. youmay find it useful to exchange slides with your neighbors to see various stages. Pick a moderatesized antral follicle and examine it closely. Note that a basement membrane separates theperipheral granulosa from the theca interna. Note the vascularity of the theca interna, and thepresence of glandular thecal cells in this layer (but not in the theca externa). in favorable sections,the stalk of granulosa cells and the group of granulosa cells surrounding the oocyte (cumulusoophorous) will also be seen. At various places in the slide, the hypertrophy of the theca internaas it converts to interstitial tissue is apparent. Although a similar hypertrophy occurs in thehuman ovary (especially during pregnancy), the interstitial tissue formed is more transitory thanin most other species.
UterusSlide 80B is a plastic section of monkey uterus in the resting stage of its estrous cycle. Themyometrium comprises a thick layer of interlacing smooth muscle bundles. Many examples ofthe rather thick-walled intramural branches of the uterine artery may be seen. The endometriumcontains numerous simple tubular uterine glands in the midst of a very cellular stroma. Scatteredmitotic figures are found among the stromal cells as well as in the simple columnar epithelium

104
FEMAILE REPRODUCTIVE SYSTEM
of the uterine glands.
Proliferative PhaseOn the left side of slide 78B, you will find a portion of a uterus from the proliferative phaseof the cycle. Note that the glands are simple tubular structures, are relatively short, andhave few branches. The stroma is dense. The epithelial cells are crowded columnar, andthe lumina of the glands are relatively devoid of secretion.
Luteal (Secretory) PhaseOn the right side of slide 77B is a portion of a uterus from the early luteal phase. Note thatthe glands are becoming coiled. Many of the nuclei are displaced from the base of the cells,which contain a basal vacuole where glycogen has been washed from the cell. Note alsothat there is secretion in the lumina of the glands, and the stroma is not quite as dense as inthe previous stage.
At the left of slide 77B, can be found a late luteal stage. Note that the glands arenow highly irregular. The glandular epithelial cells are ballooned and vacuolated. In manyregions the stroma is edematous and is highly vascular. Beneath the luminal epithelium thestroma shows the hypertrophy of the fibroblasts typical of the pseudodecidual reation andsome leukocytic infiltration.
Menstrual PhaseOn the right side of slide 78B is endometrium from early in the menstrual period. Note theextravasation of blood into the stroma, and the general loosening up and disintegration ofmuch of the functionalis of the endometrium. Note, however, that some of the glands in thebasalis are still relatively compact. It is from these twists of gland that regneration occurs.Slide 79B shows the endometrium in the first trimester of pregnancy. The conversion ofstromal cells into large spherical decidual cells is clearly seen here. Note also that theglands have become relatively inconsequential.
Immature UterusSlide 81B is a section of the uterus of a term fetus. It includes both the body and cervix ofthe uterus. The transition from a stratified squamous epithelium to a mucous-secretingepithelium can be seen where the exocervix and vaginal epithelium come together.Following the epithelium into the endocervix, one eventually comes to a simple columnarmucous epithelium. The glands of the cervix are relatively simple infoldings. In the body ofthe uterus, more complex infoldings give an indication of the rich glandularity that willeventually characterize the endometrium. The muscle layers of the uterus are divided (forpedagogical purposes) into an inner oblique, middle circular, and outer longitudinal layer,but the fiber directions are not so clear cut as the designationn of layers would suggest.Between the circular layer and longtudinal layer, is a region through which the majorvessels pass, the area vasculosa.

105
Slide 82B is of one wall of the adult cervix. At this stage, stratified squamous epithelium extendsinto the external OS where it changes abruptly to the simple columnar epithelium of the cervicalcanal. The endocervical glands are well developed. In the vaginal portion of the cervix (porticovaginalis), the stratified squamous epithelium may occasionally obstruct the opening of thecervical glands, resulting in so-called Nabothian cysts. You may find a few places on your slidewhere the cervical glands open through the stratified squamous of the portico vaginalis.
VaginaSlide 83B of monkey vagina shows that the more superficial epithelial cells appear empty (exceptfor nuclei), because the high glycogen content (which is characteristic of this type of epithelium)has been washed out by the histological technique.
OviductOn slide 75B, you can see the typical folds of the mucosa of the oviduct. Note that the mucosaruns directly down to the muscularis, without the intervention of a submucosa. Note also thedense stroma. Both the complex folding of the mucosa and the numerous cilia indicate that thissection is in the ampullary portion of the oviduct. Slide 74B includes sections of the isthmicand ampullary portions of the oviduct. The muscular organization and the well-developedciliated columnar epithelium of the monkey oviduct are shown by slide 88A.
PlacentaNowhere in the class Mammalia is there an organ more variable in structure than is the placenta.Within genera (and in most cases families) the variation is not very great, but the differencebetween orders and, in some instances, suborders is pronounced. One of the bases by whichthe different types of placenta are characterized is the relationship of the maternal tissues to theFemale Reproductive System
FEMALE REPRODUCTIVE SYSTEM

106
FEMALE REPRODUCTIVE SYSTEM
fetal trophoblast or chorion. When the fetal trophoblast is in direct contact with maternal blood,the placenta is called hemochorial. The human is an example of villous hemochorial chorioallan-toic placenta.
An understanding of the complex interactions that take place in the establishment of theplacenta cannot be achieved by examining a few representative sections. It should be possible,however, for you to see some of the changes with age that occur in the human placenta.
First Trimester PlacentaSlide 90B passes through part of the myometrium, the endometrium and into the intervillousspace. There is a spongy zone of dilated endometrial glands beneath the compact region ofenlarged stromal cells (decidual cells). At the surface of the basal plate, you can see adiscontinuous layer of red fibrin and many giant cells (clumps of syncytial trophoblast). Inaddition, there are regions where anchoring villi form portions of the basal plate. Syncytialtrophoblast is not interposed between cytotrophoblast and maternal tissue at the bases of theanchoring villi. The cytotrophoblast cells nearest the connective tissue stroma of the anchoringvillus are basophilic and compact, but as the cells extend toward the maternal side of the basalplate, they become vacuolated and are more loosely arranged. Numerous free villi are seen inthe intervillous space, but the section does not extend through the entire thickness of theplacenta to the chorionic plate . Slide 86B is useful for studying the free villi of the early placenta.The characteristics of the early placenta shown include a nearly complete cytotrophoblast layer(Langhans layer) underlying the syncytial trophoblast, numerous Hofbauer cells (vacuolatedmacrophages characteristic of the early placenta), and many nucleated erythrocytes.
Midtrimester and Term PlacentaThe general topography of the placenta may be appreciated by examining slide 9lB of the mid-trimester, and 89B of the term placenta. The narrow margin of both of these sections is theedge of the placental disc where the chorion frondosum becomes chorion laevae, (and whereconsequently, the basal and chorionic plates are closely apposed). Note the increased fibrinin the chorionic plate of the term placenta, and that the residual anchoring villi at the basal plateare fibrotic and largely devoid of cytotrophoblast.
Examine the free (terminal) villi of the term placentas in slide 87B. Note that there are relativelyfew cytotrophoblast cells, and the nuclei of the syncytium are clumped. Blood vessels are closeto (and even indenting) the syncytium. There is an increased density of the connective tissue,and in many regions fibrotic areas can be seen. Slide 93B dramatically demonstrates thefunctioning of the 3rd trimester placenta in counter-current exchange between fetal and maternalcirculations. Careful examination of the epithelium will reveal only occasional cytotrophoblastcells (lighter cytoplasm), and many syncytial knots.
The Umbilical CordThe umbilical cord (slide 96B) carries two muscular arteries and one muscular vein. The vesselslack elastica internae and adventitia, their muscular coats being embedded directly in the thickcylinder of mucous connective tissue in which they are carried. This tissue consists of stellatefibroblasts, scattered through a gelatinous ground substance known as Wharton’s jelly. The

107
FEMALE REPRODUCTIVE SYSTEM
mechanical properties of the ground substance and the vessel walls permit the umbilical to betwisted and, occasionally, even knotted without occlusion of the circulation.
The Female Breast
Nonlactating Mammary GlandSlides 92B, 94B, and 95B include three different functional states of the human mammary gland.The gland of a nonpregnant adult (92B) consists largely of a connective tissue stroma and fattylobules. Sections through the tubular epithelium of the ducts appear blue, because of the closeproximity of nuclei in these areas. During this stage, the non-functional mammary gland consistsof islands of ducts in a loose connective tissue stroma surrounded by dense interlobularconnective tissue stroma. There is substantial lymphocyte infiltration in this preparation. Slide94B is an involuted gland (postmenopausal), consisting of scattered large ducts and connectivetissue with very little fat. Both the columnar epithelium and myoepithelial cells remain healthy.
Lactating Mammary GlandThe lactating gland (95B) shows the expanded alveoli filled with a pink-staining secretorymaterial. The dense connective tissue is considerably reduced between the glandular lobes.The interlobular ducts are large, and have stratified columnar epithelium. Some of these sectionscontain a portion of the base of the nipple, showing several lactiferous sinuses surrounded bya dense connective tissue matrix.
Slides 99B and l00B are from monkey, and provide another opportunity to compare theresting and functional state of the mammary gland. The alveoli in slide l00B are congested withmilk. What hormone could you give to cause emptying of these alveolar spaces? What typesof stimulation cause this hormone to be secreted in the nursing mother? Do you see evidenceof mitotic activity in the alveolar cells in the lactating gland? How might this be related to reportsof lower incidence of breast cancer in women who have experienced extended periods oflactation? Locate the myoepithelial cells. Would you expect to find nerve endings on these cellsin studying electron micrographs of these regions?

108

109
Glossary
AAlcian blue - Stains complex carbohydrates rich in free acidic groups. Connective tissue mucins,most epithelial mucins and mast cell granules are stained a turquoise blue color.
Aldehyde fuchsin - Stains elastic fibers violet to purple. Secretory granules in mast cells, gastricchief cells, pancreatic B cells, beta cells of the pituitary, and mucins also stain purple.
BBodian silver - A technique for impregnating nerve axons with reduced silver (black). The nucleiand Golgi of most cells also stain with this method.
CCarmine - A basic dye used as a counterstain for vital dyes, in the Mucicarmine technique, andfor coloring gelatin used to inject blood vessels.
Copper-chrome hematoxylin (CCH) - Stains mitochondria deep blue against a yellowishbackground.
FFast green - An acid dye used as a counter stain (rarely used alone) that stains connective tissuea light green.
Formalin - The most common fixative for routine light microscopy, consisting of an aqueoussolution of formaldehyde. Works by binding to certain side groups of amino acids to formmethylene bridges between protein molecules. Aldehydes allow lipid extraction but penetratetissues quickly.
HHematoxylin and eosin (H & E) - The most common histologic stain used for routine study ofgeneral morphology. Stains nuclei blue and practically all cytoplasmic structures red. Thoseconstituents staining blue are commonly called basophilic and those staining red, acidophilic.Pronounced basophilia in the cytoplasm of cells usually indicates a high level of RNA and proteinsynthesis (such as is observed in developing organs in the embryo, or in cells of the adultorganism) e.g., the pancreatic acinar cells. As a general rule, the basic components of a tissuestain with acidic dyes and so are called acidophilic whereas the acidic components stain withbasicdyes and are called basophilic.
Hematoxylin and orange G-erythrosin (H & OGE) - A general purpose stain for morphology.The hematoxylin primarily stains nuclei and other basophilic constituents of the cell, if any.Orange G is a rather strongly acid dye which stains acidophilic components (such as thecytoplasm) an orange-red color. The erythrosin is also an acid dye, but stains some structures(such as smooth muscle) a light pink.

110
IIron hematoxylin (IH) - This stain is particularly useful for secretory granules, but in additionstains chromatin, nuclei, mitochondria and cross striations of voluntary muscle an intense blue.The stain is not specific for anything other than dense protein in any tissue. The iron (ironammonium sulfate) actually serves as a mordant, to which the hematoxylin can bind.
MMallory trichrome (M) - This stain consists of three dyes: acid fuchsin, aniline blue and orangeG. Stains collagen an intense blue, mucus and amyloid various shades of blue; and nuclei,cytoplasm, elastic fibers, neuroglia, myoglia and fibrin red. Erythrocytes and myelin sheathsstain yellow to orange.
Metachromasia - A shift in the absorption spectrum of a basic dye, such as thionin or toluidineblue. This results from interaction between dye molecules when they are bound close enoughtogether (within .5-.7 nm‹) to a series of uniformly-spaced negative sites such as exist in heparin,other acid mucopolysaccharides and nucleoproteins. Tissue substances that are stainedmetachromatically do not appear to be the same color as the dye used but, rather, acquire areddish shade.
Methylene blue - A common basic dye and counterstain.
Mucicarmine (Muci) - An aluminum carmine compound that stains mucins a bright red.
PPAS-PTH - A combination stain of periodic acid Schiff and phosphotungstic acid hematoxylin.It allows the simultaneous staining of mitochondria, muscle fibers, etc., with basementmembrane, glycogen, etc.
Periodic acid Schiff (PAS) - A histochemical technique which stains structures rich inpolysaccharides, mucopolysaccharides, glycoproteins and glycolipids. The periodic acidselectively oxidizes l,2 glycols and l,2- amino alcohols, thus splitting off free aldehydes (whichare then detected in situ by forming a stable complex with the Schiff reagent to form areddish-purple color). Tissue constituents which are stained various shades of red by thistechnique include glycogen, basement membranes of epithelia, mucins, and colloids of thyroidand anterior pituitary. It is most frequently used in your slide collection to show basementmembranes and the glycocalyx.
Phosphotungstic acid hematoxylin (PTAH) - A common technique for staining mitochondriaa deep blue. Collagen and ground substance of cartilage and bone stain yellow to brownish-red. Many fibrous elements of tissue (such as fibroelastic fibroglial, myoglial and neuroglialfibrils, striated muscle fibers and fibrin) stain blue. Coarse elastic fibers may stain purple.
GLOSSARY

111
RResorcin-fuchsin (RF: Weigert’s resorcin fuchsin) - A stain for elastic fibers, deep purple toviolet. Nuclei stain paler red, cartilage matrix stain violet and cytoplasm yellow.
SSilver methods - All of the silver techniques entail the impregnation of blocks or sections oftissue with silver compounds (AgNO3) and a subsequent reduction of the so-called argyrophilictissue elements to free silver. The various techniques are used to demonstrate nerve axons,reticular fibers and melanin.
TTetrachrome - A mixture of hematoxylin, orange G, fast green, and chromotrope 2R, an acid dyethat stains the cytoplasm mildly pinkish. The orange G stains the erythrocytes orange in thispreparation.
VVerhoeff’s hematoxylin (VH) - An empirical stain which stains elastic fibers a clear blue-blackor black. Fibroglia, myoglia, neuroglia and fibrin may stain pink.
WWright’s stain - A mixed stain containing eosin and a series of methylene blue derivatives,especially azure B. Used almost exclusively for blood smears, marrow smears, etc. When handledproperly, this mixture stains myloid cells as follows:
Erythrocytes - pink; nuclei - deep blue; basophilic granules - deep purple.Eosinophils - granules red to red-orange, bluish cytoplasm.Neutrophils - granules - reddish brown, pale pink cytoplasm.Monocytes -azure granules.Lymphocytes - granules more reddish than monocyte granules, sky blue cytoplasm.Platelets - violet to purple.
GLOSSARY