Embed Size (px)
Citation preview
D R D E N N I S O ’ C O N N O R
M . B . , B . S . D I P R A C O G D I P M U S C M E D G C H P E
HIP AND SHOULDER PAIN GP ASSESSMENT TIPS AND INJECTION TECHNIQUES
DISCLAIMER
LEARNING OBJECTIVES
• Review hip and shoulder assessment in a
general practice setting
• Apply a focused algorithmic approach to
hip and shoulder pain
• Explore evidence based medicine principles
in management
• Revise office based injection techniques for
common hip and shoulder problems
HOW COMMON?
• MSK conditions second most common presentation
to Australian GPs (10%)
• Shoulder symptoms 0.7% of consultations (third most
common MSK problem behind back and knee
complaints)
• Shoulder ultrasound 11.2 % of all ultrasound exams
and 4.2% of all imaging
• Hip symptoms < 0.6%* of consultations
• Hip ultrasound 2% of all ultrasounds
• (BEACH Data 2009-2010)
SIMILARITIES
• Lateral hip pain is termed the rotator cuff of the hip
• Anatomical similarities of short muscles inserting
onto a tuberosity or trochanter
• Overlying large strong muscles which attach distally
• Bursa intimately related to muscle/tendon/bone
interface
• Process of tendon degeneration and traction forces
and compression likely to be responsible for injury
• Propensity to chronic symptoms
HIP PAIN
LATERAL HIP PAIN (ADULTS)
GREATER TROCHANTERIC PAIN SYNDROME
Spectrum of conditions including trochanteric bursitis
and gluteal enthesiopathy and tendinitis, tendinosis
and tears of gluteus minimus and medius.
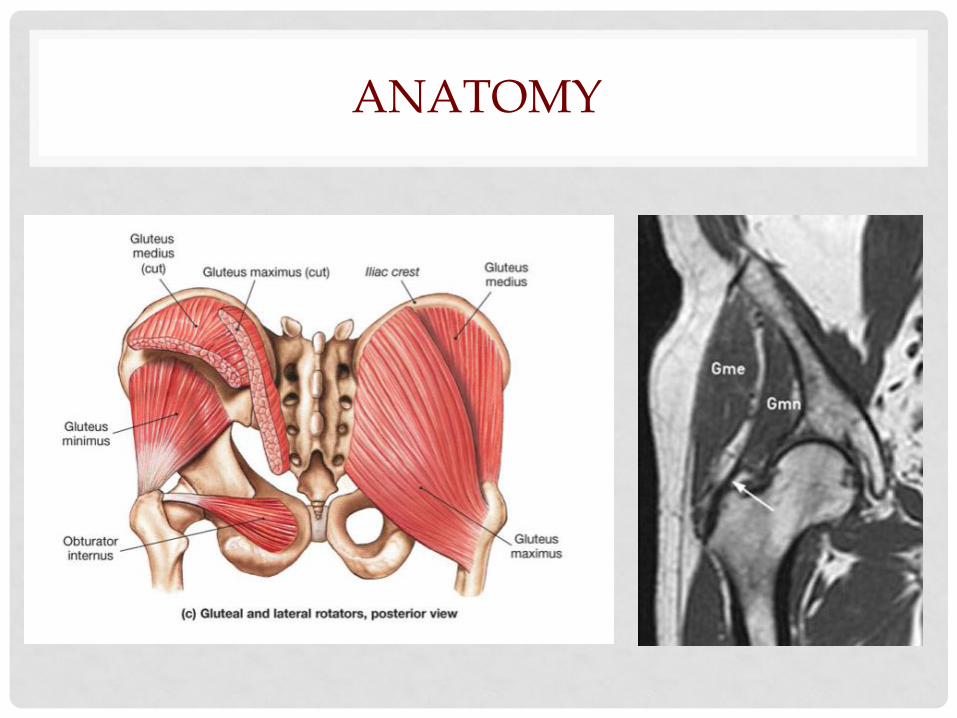
ANATOMY
HISTORY
• 40 - 60 y.o woman
• Pain in the lateral hip region
• Insidious onset
• Worse lying on that side at night
• Radiation of pain down lateral thigh (Pseudosciatica)
• Symptoms with prolonged standing
• Worse sitting with affected leg crossed
• Pain lying on contralateral side
CLINICAL TESTS
• Painless hip flexion and internal rotation
Then
• Point tenderness over the greater trochanter
And possibly
• Positive single leg stance for 30 seconds
• Painful resisted external derotation
• Positive FABER (Patrick’s) Test
• Positive Trendelenberg’s Test
WITH • Symptom relief from trigger point injection*
DIFFERENTIAL DIAGNOSIS
• Atypical hip joint pain
• L4/5 facet referred pain
• Meralgia paraesthetica
• Lumbar radiculopathy
• Iliotibial band syndrome
• Stress fracture femoral neck
• (Snapping Hip - Coxa Sultans)
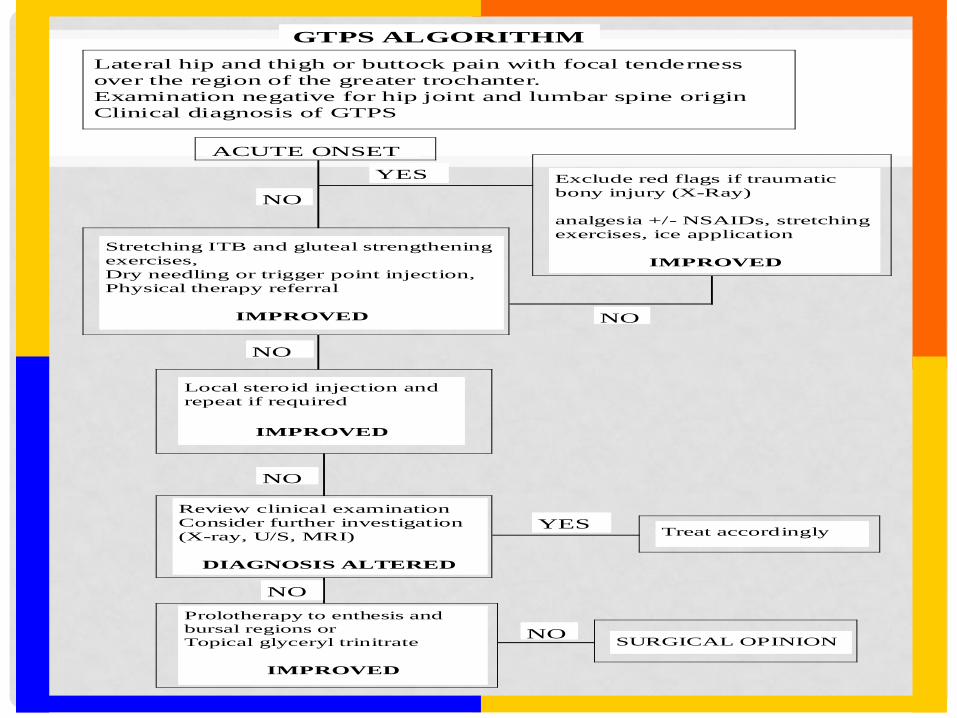
Lateral hip and thigh or buttock pain with focal tenderness
over the region of the greater trochanter.
Examination negative for hip joint and lumbar spine origin
Clinical diagnosis of GTPS
NO
YES
GTPS ALGORITHM
Exclude red flags if traumatic
bony injury (X-Ray)
analgesia +/- NSAIDs, stretching
exercises, ice application
IMPROVED
Stretching ITB and gluteal strengthening
exercises,
Dry needling or trigger point injection,
Physical therapy referral
IMPROVED
NO
Local steroid injection and
repeat if required
IMPROVED
NO
Review clinical examination
Consider further investigation
(X-ray, U/S, MRI)
DIAGNOSIS ALTERED
Treat accordingly YES
Prolotherapy to enthesis and
bursal regions or
Topical glyceryl trinitrate
IMPROVED
SURGICAL OPINION NO
NO
NO
ACUTE ONSET
INJECTION TECHNIQUES
Office based lateral hip injection techniques
• Dry needling
• Local Anaesthetic injection
• Steroid injection
DRY NEEDLING
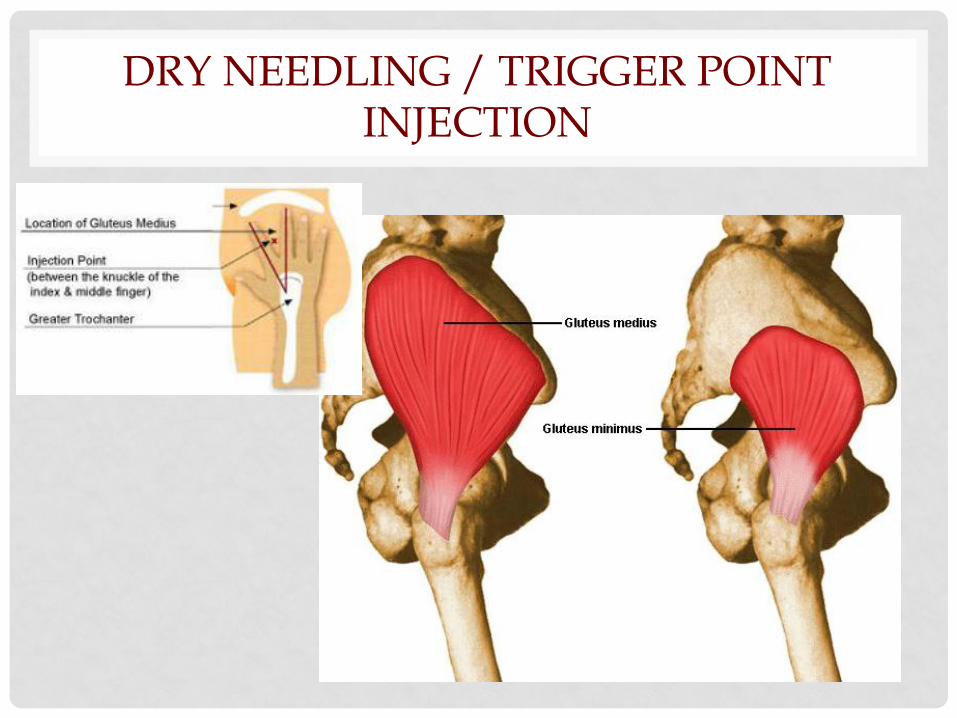
DRY NEEDLING / TRIGGER POINT INJECTION
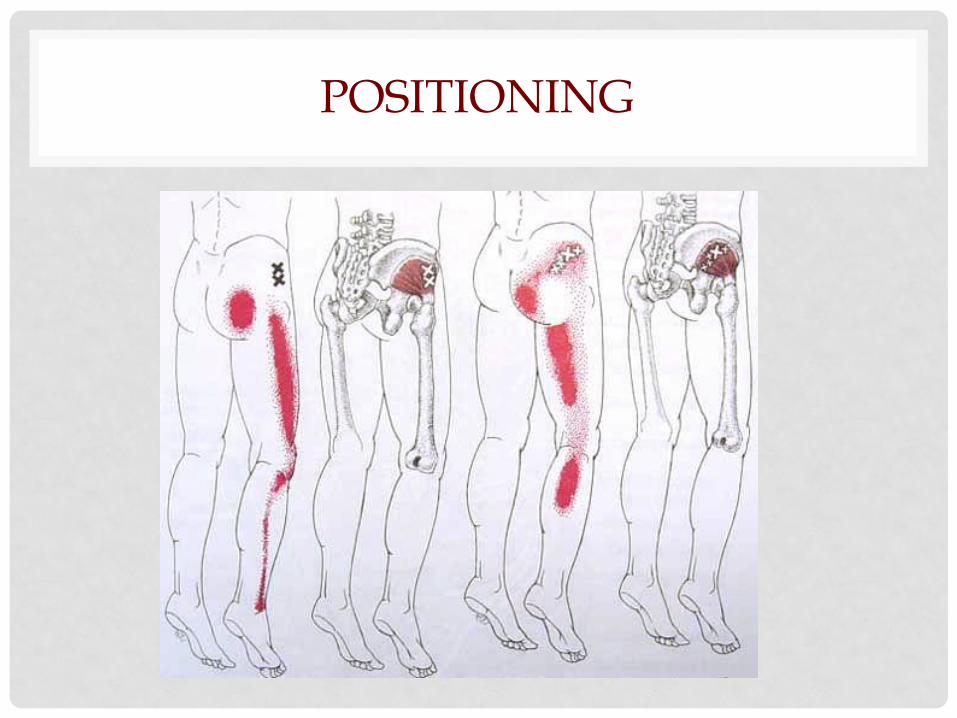
POSITIONING
STEROID INJECTION

TECHNIQUE
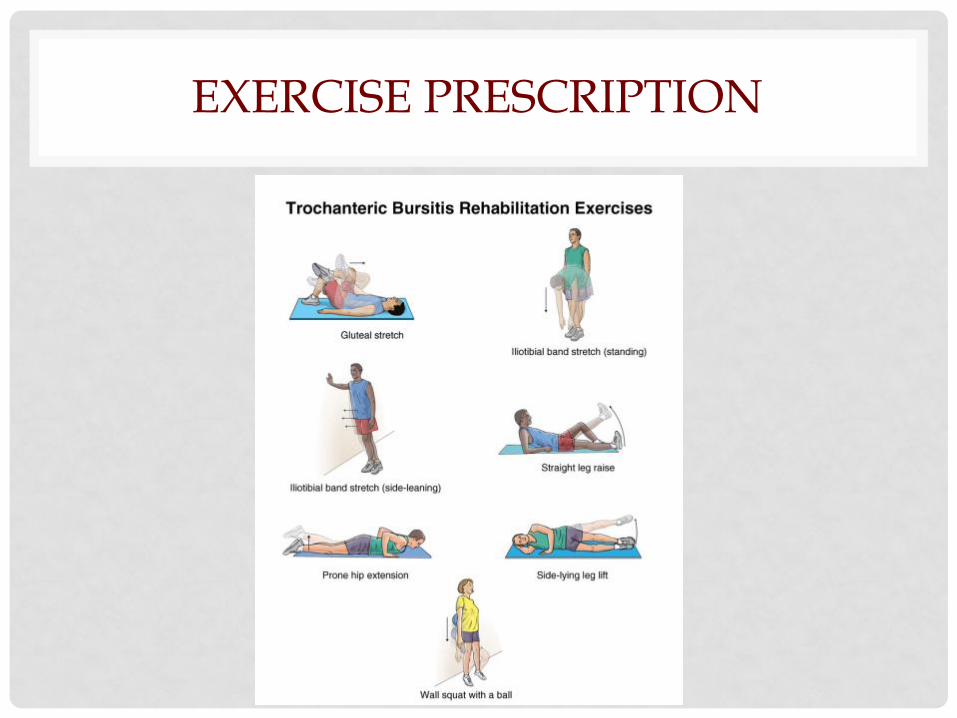
EXERCISE PRESCRIPTION


EXERCISES
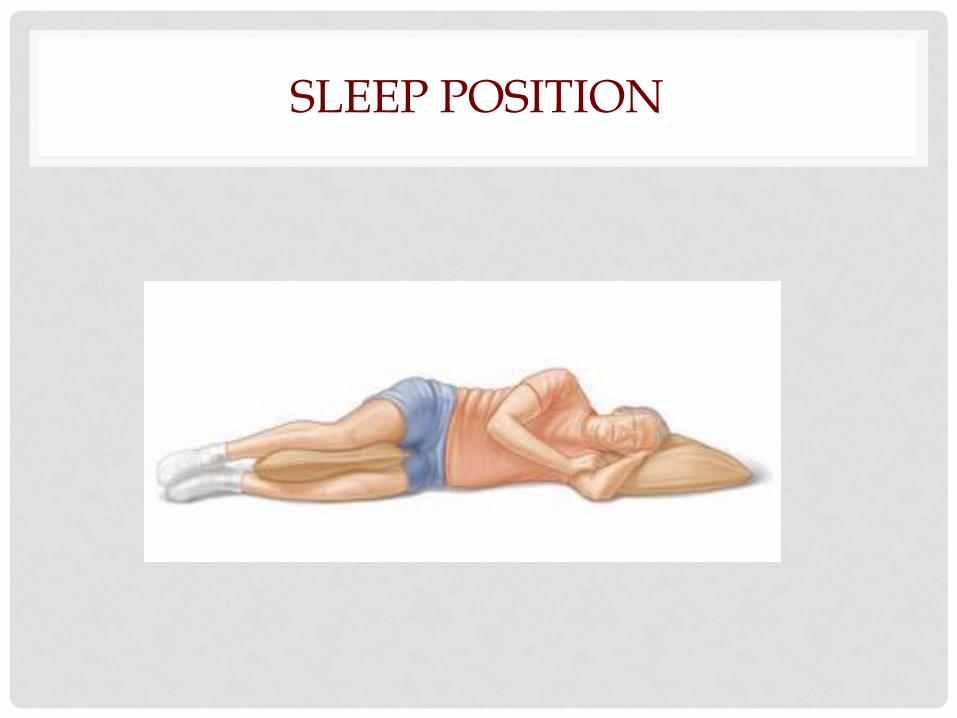
SLEEP POSITION
GP TIPS
• This tends to be a chronic condition
• Often patients present late, having tried other remedies
• A focused history and directed examination is time efficient for GPs
• Local anaesthetic injection can assist in diagnosis
• Steroid injections give good short term benefit
• Prescribe, describe and scribe a range of simple exercises
• Modify activities and postures which worsen the problem
• Sleep with a pillow between legs
SHOULDER PAIN
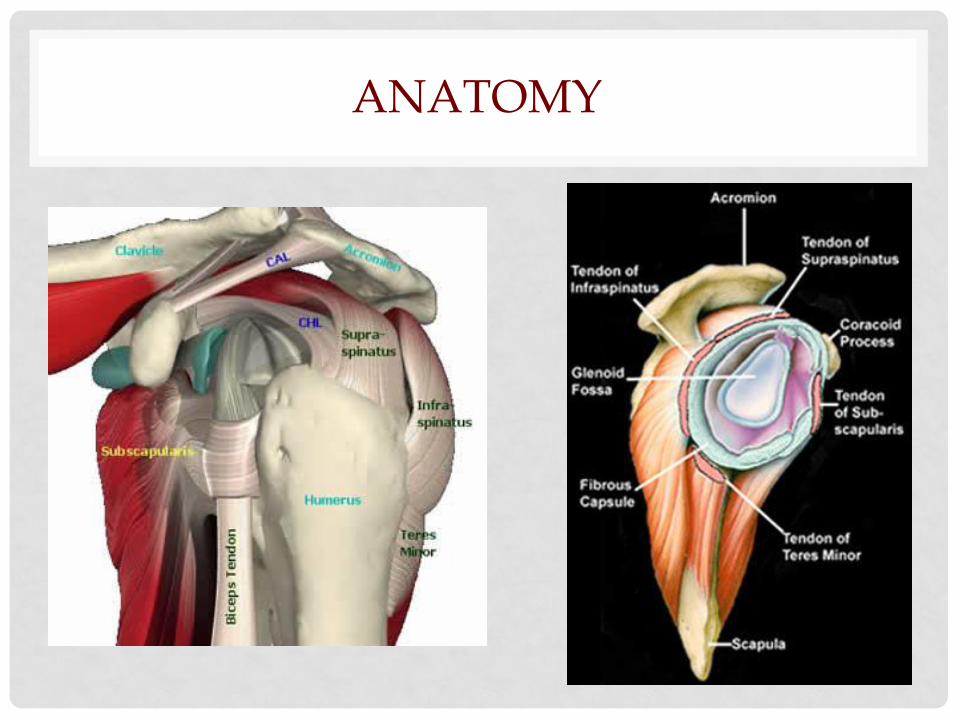
ANATOMY
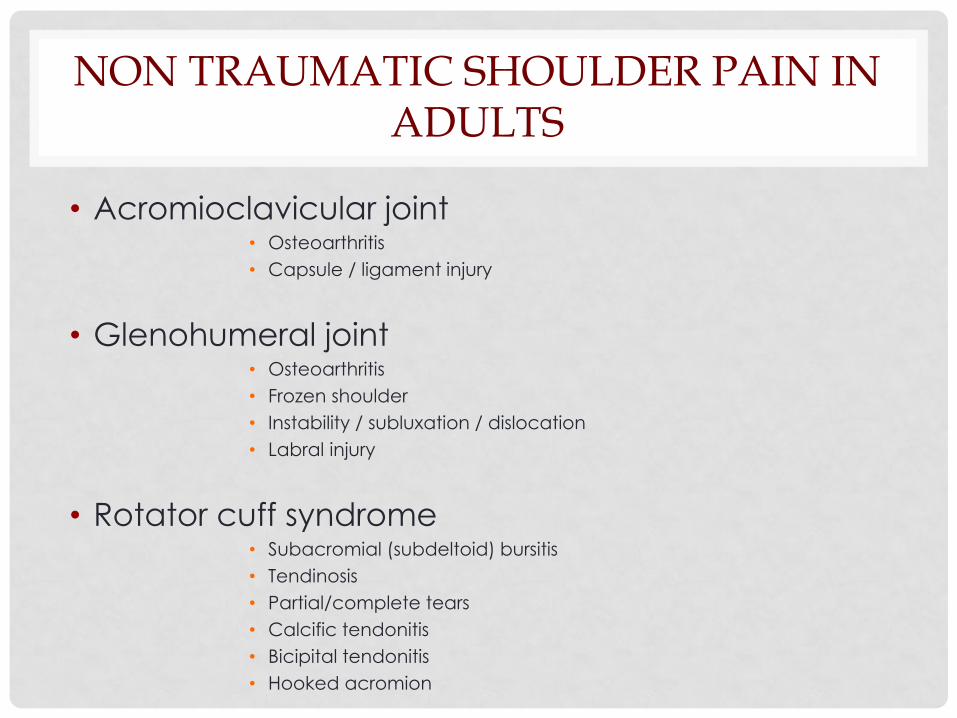
NON TRAUMATIC SHOULDER PAIN IN ADULTS
• Acromioclavicular joint • Osteoarthritis
• Capsule / ligament injury
• Glenohumeral joint • Osteoarthritis
• Frozen shoulder
• Instability / subluxation / dislocation
• Labral injury
• Rotator cuff syndrome • Subacromial (subdeltoid) bursitis
• Tendinosis
• Partial/complete tears
• Calcific tendonitis
• Bicipital tendonitis
• Hooked acromion
ROTATOR CUFF SYNDROME
ROTATOR CUFF SYNDROME
Spectrum of conditions including subacromial
bursitis, rotator cuff enthesiopathy and
tendinitis, tendinosis and tears in the rotator
cuff muscles
HISTORY
• >35 y.o
• Pain in lateral upper arm region
• Worse with abduction and/or rotation
• Often catching pain with certain movements
• Aching pain at night
• Repetitive overhead activities or heavy lifting
• Maybe history of prior minor injury
• Absence of ‘red flags’
CLINICAL TESTS
• 105 documented tests for shoulder region !
• Most tests for rotator cuff pathology are inaccurate
and cannot be recommended for clinical use
• Combination of physical tests at best raise the
clinical suspicion of impingement
PREDICTORS OF PERSISTENT SHOULDER PAIN
• Duration of complaint before presentation
• Gradual (insidious) onset
• Psychological complaints
• Repetitive movements
• Intensity of pain at presentation
• Degree of disability at presentation
MANAGEMENT
• Evidence is lacking for benefit of one mode of
treatment over another
• This includes conservative, injection therapy and
surgical treatment
• Subacromial steroid injection reduces pain and
improves function early (common theme)

INJECTION TECHNIQUES
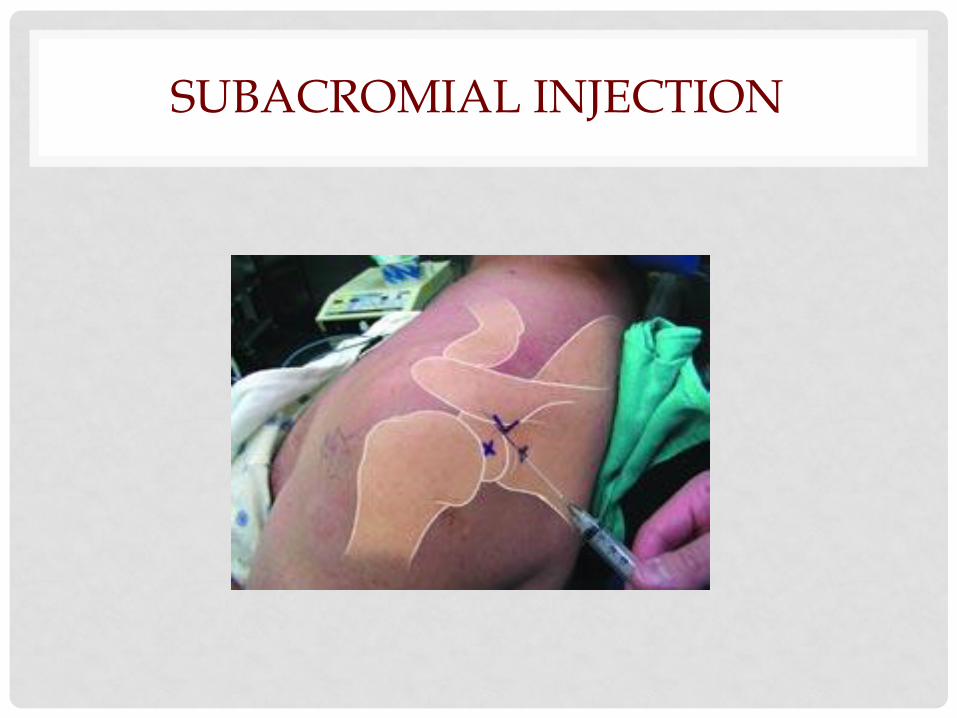
SUBACROMIAL INJECTION
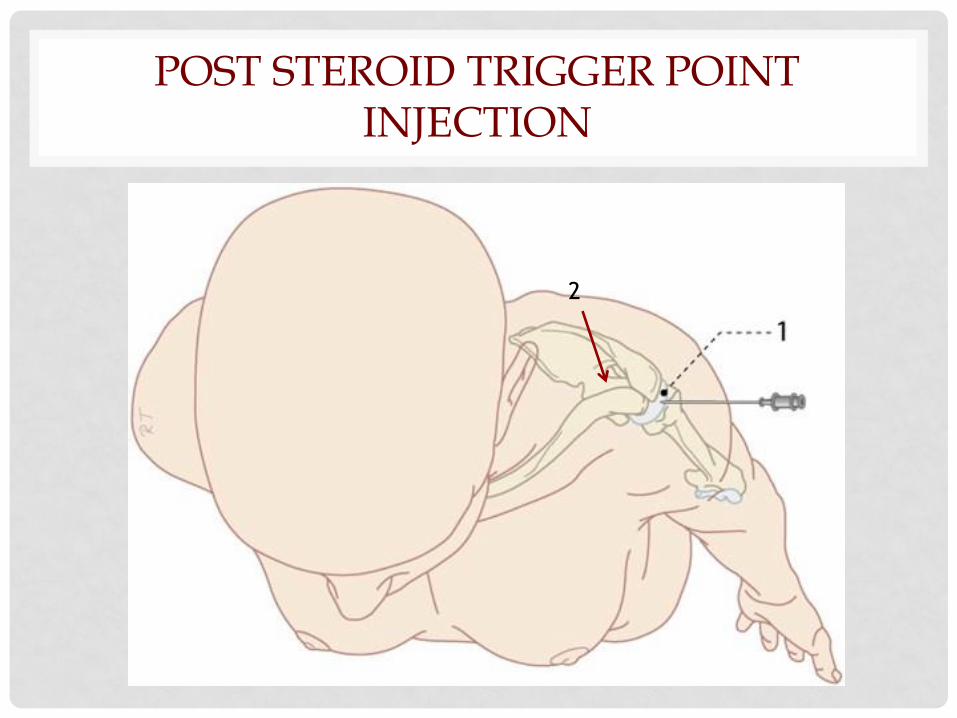
POST STEROID TRIGGER POINT INJECTION
2
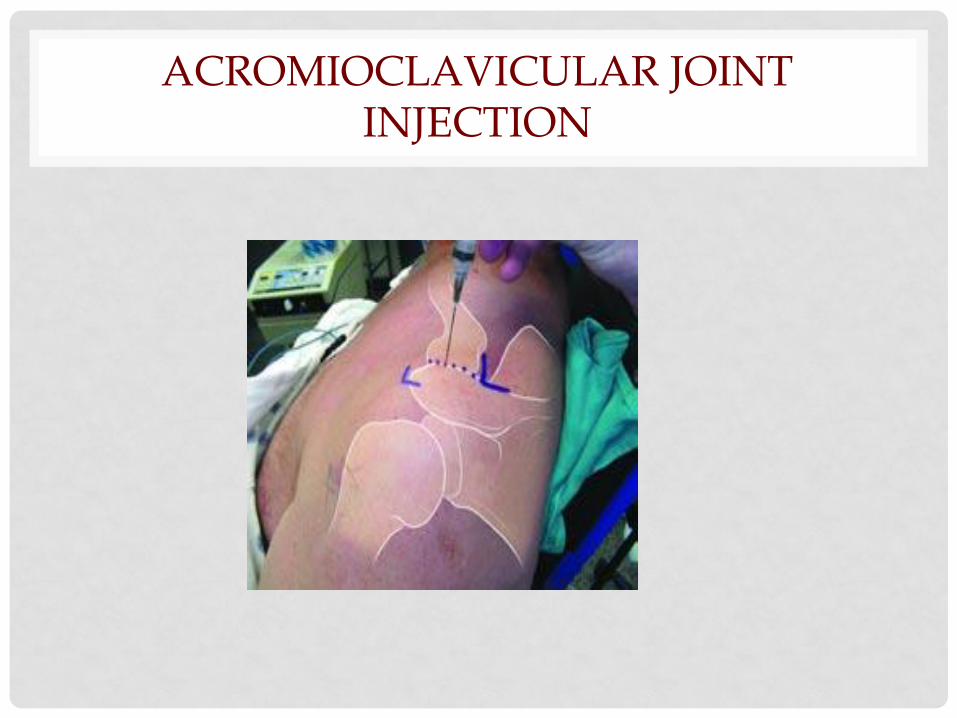
ACROMIOCLAVICULAR JOINT INJECTION
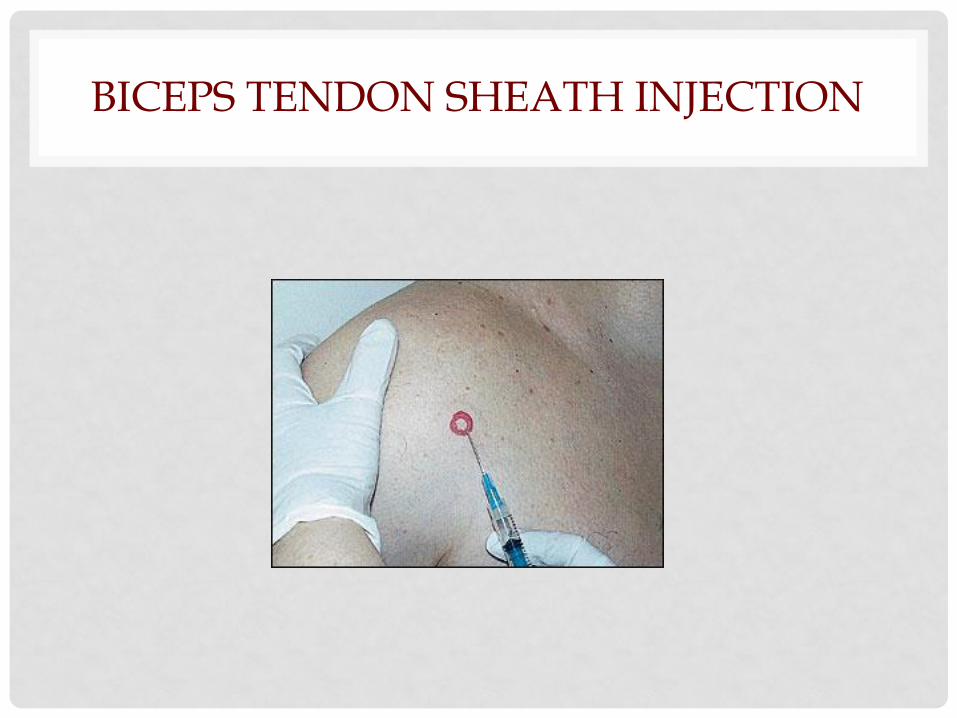
BICEPS TENDON SHEATH INJECTION
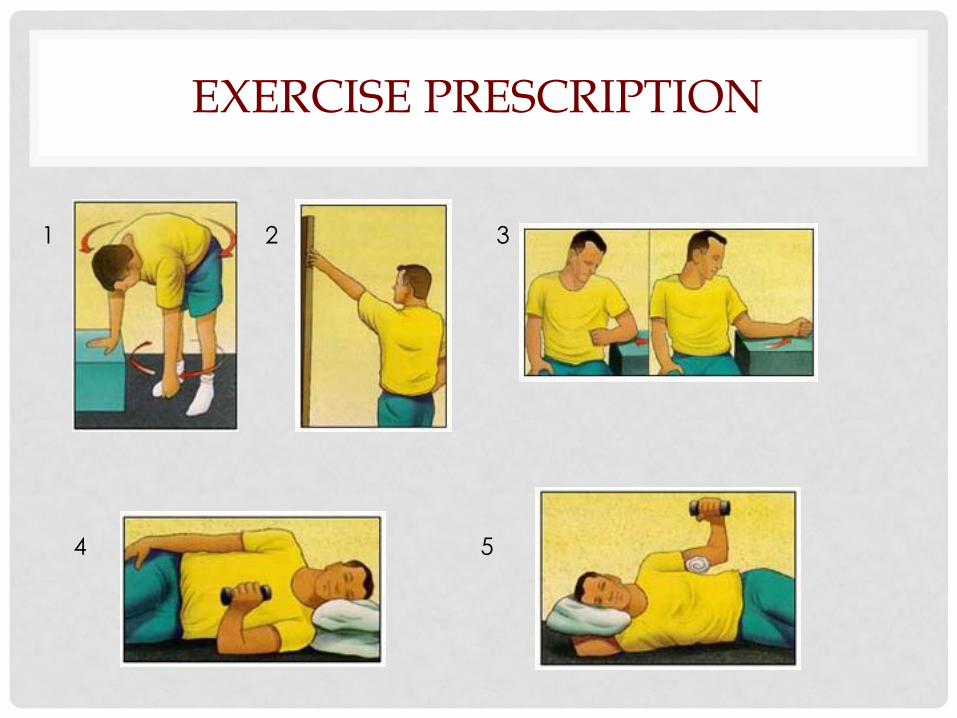
EXERCISE PRESCRIPTION
1 2 3
4 5



MY CHOICE
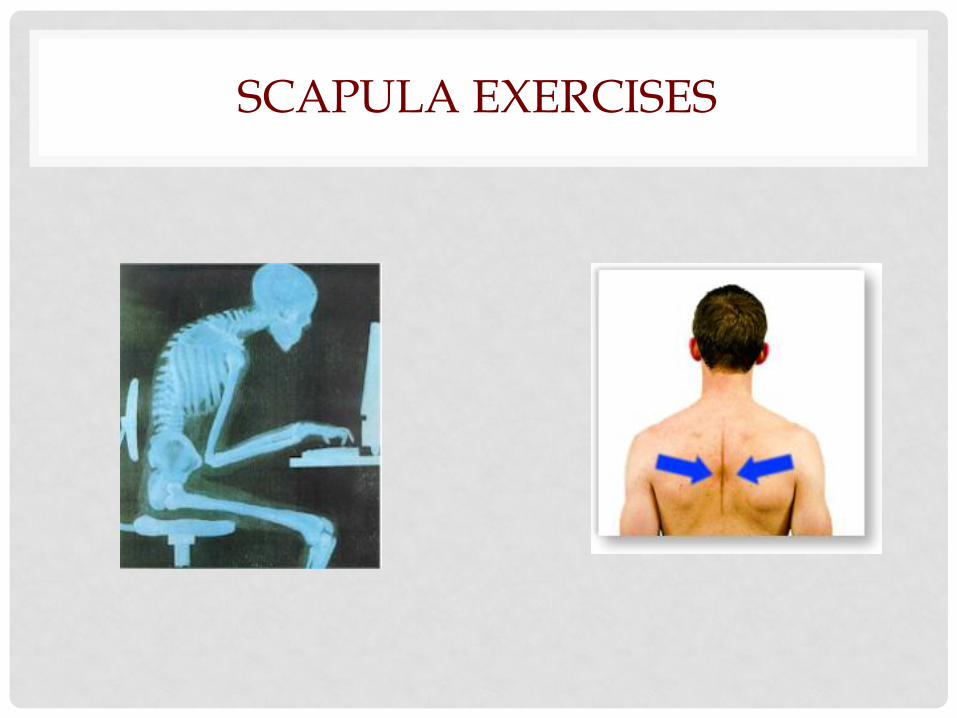
SCAPULA EXERCISES
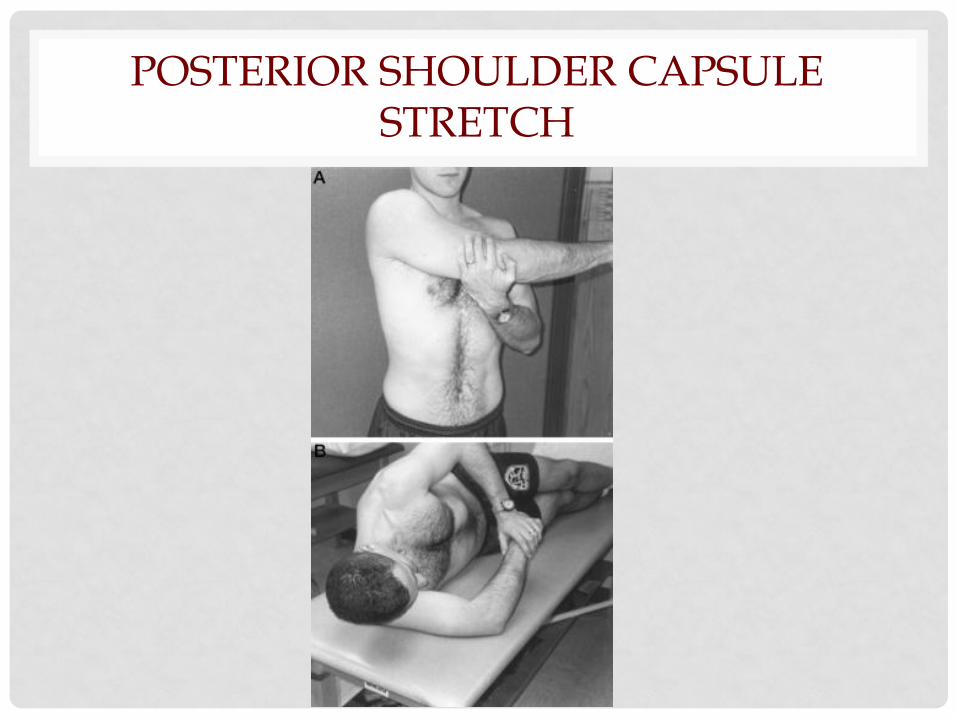
POSTERIOR SHOULDER CAPSULE STRETCH
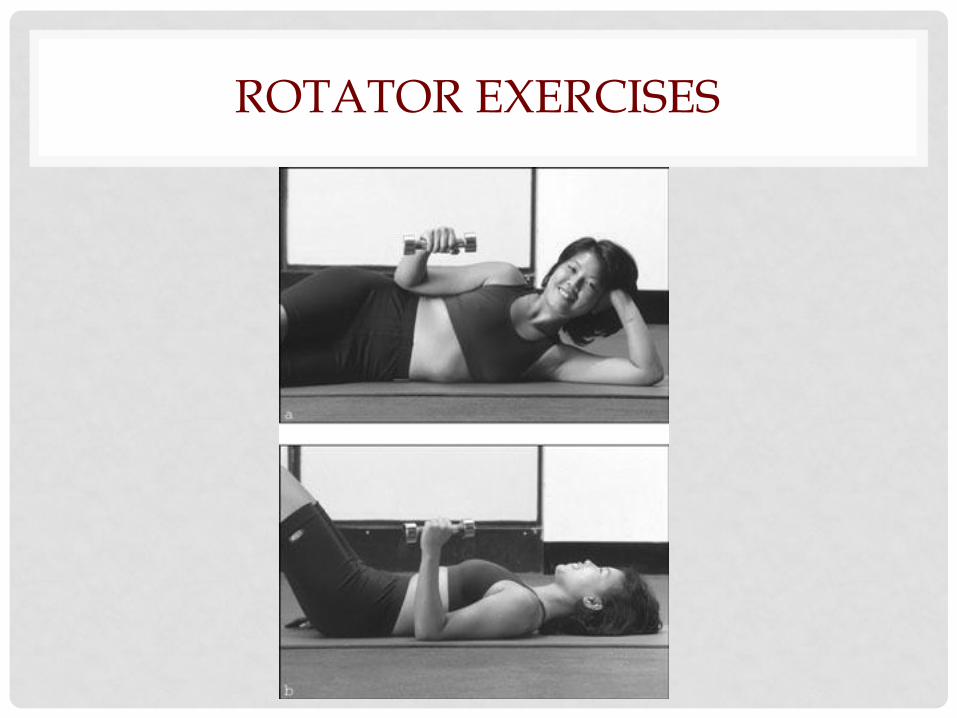
ROTATOR EXERCISES
GP SHOULDER TIPS
• Calcific tendonitis presents as acute severe non
traumatic pain and responds best to steroid injection
• Treat shoulder impingement early to reduce pain and
allow exercise rehabilitation
• Give advice to improve posture
• Avoid overhead activities and precipitating activities
• Prescribe, describe and scribe exercises to stretch the
GH capsule and strengthen the small shoulder muscle
stabilisers
• Future techniques to treat tendinosis likely to emerge
SUMMARY
• Exclude red flags
• A focused algorithmic approach can be useful
• Treat early and aggressively to reduce chronicity
• An injection doesn’t cure the problem but helps
reduce pain at least initially.
• Prescribe, describe and scribe stretch and
strengthening exercises in order to improve
function.
• Rehabilitation exercises need to be ongoing.
• Investigate if it will alter your management.
• Allow yourself time ( both for assessment and
management)
REFERENCES
• Strauss, E.J et al .Greater Trocahnteric Pain
Syndrome. Sports Med Arthrosc Rev. Vol 18, No 2,
June 2010
• Williams BS and Cohen SP. Greater trochanteric
pain syndrome: a review of anatomy, diagnosis
and treatment. Anesth Analg. 2009; 108:1662-1670
• Shbeeb MI, Matteson EL. Trochanteric bursitis (
greater trochanter pain syndrome) Mayo Clin
Proc.1996;71:565-569
• Collee G. Greter trochanteric pain syndrome
(trochanteric bursitis) in low back pain.
Scandinavian Journal of Rheumatology
1991;20:262-266
• Lievense a, Bierma-Zeinstra S, SchoutenB, Bohnen A,
Verhaar J, Koes B. Prognosis of trochanteric pain in
primary care. British Journalof General Practice
2005; 55(512): 199-204
• Del Buono A, PapaliaR, Khanduja V, Denaro V and
Maffuli N. Management of the greater trochanteric
pain syndrome: a systematic review. British Medical
Bulletin 2012: 102: 115-131
• Brinks A et al. Corticosteroid Injections for greater
trochanteric pain syndrome: A randomised
controlled trial in primary care. Ann Fam Med
2011;9:226-234
• Hughes P, Taylor N, Green R. Most clinical tests
cannot accurately diagnose rotator cuff
pathology: a systematic review. Aust Journal of
Physio 2008 Vol 54, 159-170
• Silva L et al. Accuracy of physical examination in
subacromial impingement syndrome.
Rheumatology 2008; 47: 679-683
• Kuijpers T et al. Clinical prediction rules for the
prognosis of shoulder pain in general practice.
Pain120(2006) 276-285
• Masters S, O’Doherty L, Mitchell G, Yelland M. Acute
shoulder pain in primary care. An observational
study. AFP Vol36,No6,June 2007
• Crawshaw DP et al. Exercise therapy after
corticosteroid injection for moderate to severe
shoulder pain: large pragmatic randomised trial.
BMJ 2010;340:c3037
• Stitik TP, Foye PM, Fossati J. Shoulder injections for
osteoarthritis and other disorders. Phys Med Rehab
Clin N Am;15 (2004) 407-446
• Holmgren T, Hallgren HB, oberg B, Adolfsson Land
Johanssen K. Effect of specific exercise strategy on
need for surgery in patients with subacromial
impingement syndrome: randomised controlled
study. BMJ 2012;344:e787
• Codsi M. The painful shoulder: when to inject and
when to refer. Cleveland Clinic Journal of
Medicine. Vol 74:7; (2007); 473-488