-
American Journal of Gastroenterology ISSN 0002-9270C 2008 by Am.
Coll. of Gastroenterology doi:
10.1111/j.1572-0241.2008.02149.xPublished by Blackwell
Publishing
ORIGINAL CONTRIBUTIONS
Endoscopy
High- Versus Low-Dose Proton Pump Inhibitors AfterEndoscopic
Hemostasis in Patients With Peptic UlcerBleeding: A Multicentre,
Randomized StudyAngelo Andriulli, M.D.,1 Silvano Loperfido, M.D.,2
Rosaria Focareta, M.D.,3 Pietro Leo, M.D.,4
Fabio Fornari, M.D.,5 Antonietta Garripoli, M.D.,6 Paolo Tonti,
M.D.,7 Sergio Peyre, M.D.,8
Antonio Spadaccini, M.D.,9 Riccardo Marmo, M.D.,10 Antonio
Merla, M.D.,1 Alessandro Caroli, M.D.,2
Gian Battista Forte, M.D.,3 Angelo Belmonte, M.D.,4 Giovanni
Aragona, M.D.,5 Gianni Imperiali, M.D.,11
Fabrizio Forte, M.D.,3 Fabio Monica, M.D.,2 Nazario Caruso,
M.D.,1 and Francesco Perri, M.D.1
Divisions of Gastroenterology, 1Casa Sollievo della Sofferenza
Hospital, IRCCS, San Giovanni, Rotondo,Italy, 2Regional Hospital,
Treviso, Italy, 3 S. Sebastiano Hospital, Caserta, Italy, 4P.O.
Annunziata Hospital,Cosenza, Italy, 5G. da Saliceto Hospital,
Piacenza, Italy, 6 Maria Vittoria Hospital, Torino, Italy,7Ospedali
Riuniti, Foggia, Italy, 8Ivrea Hospital, Ivrea, Italy, 9S. Pio da
Pietrelcina Hospital, Vasto, Italy,10L. Curto Hospital, Polla,
Italy, and 11Valduce Hospital, Como, Italy
BACKGROUND: The most effective schedule of proton pump inhibitor
(PPI) administration following endoscopichemostasis of bleeding
ulcers remains uncertain.
METHODS: Patients with actively bleeding ulcers and those with
nonbleeding visible vessel or adherent clotwere treated with
epinephrine injection and/or thermal coagulation, and randomized to
receiveintravenous PPIs according to an intensive regimen (80 mg
bolus followed by 8 mg/h ascontinuous infusion for 72 h) or a
standard regimen (40 mg bolus daily followed by saline infusionfor
72 h). After the infusion, all patients were given 20 mg PPI twice
daily orally. The primary endpoint was the in-hospital rebleeding
rate, as ascertained at the repeat endoscopy.
RESULTS: Bleeding recurred in 28 of 238 patients (11.8%)
receiving the intensive regimen, and in 19 of 236(8.1%) patients
receiving the standard regimen (P = 0.18). Most rebleeding episodes
occurredduring the initial 72-h infusion: 18 (7.6%) and 19 events
(8.1%) in the intensive and standardgroups, respectively (P =
0.32). Mean units of blood transfused were 1.7 2.1 in the intensive
and1.5 2.1 in the standard regimen group (P = 0.34). The duration
of hospital stay was
-
3012 Andriulli et al.
endoscopic hemostasis was conducted in 11 Italian centreson a
nonprofit, voluntary basis after the protocol receivedapproval by
local ethics committees. All study subjects gavewritten informed
consent and were enrolled between October2004 and March 2007. No
industry support in the ideation,planning, designing, and
conducting of the trial or in the anal-ysis of the experimental
data was pursued.
Patient PopulationPatients who presented with overt
gastrointestinal bleeding ora recent history (
-
Proton-Pump Inhibitors After Endoscopic Hemostasis 3013
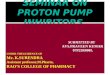
243 Assigned toan intensive regimen
239 Assigned tostandard regimen
238 included in analyses
236 included in analyses
5 Excluded from
analysis
3 Withdrew
voluntarily
2 Had warfarin
anticoagulation
3 Excluded from analysis
1 Withdrew voluntarily
1 Had a final diagnosis of
pancreatic gastrinoma
1 Had warfarin anticoagulation
482 Randomly assigned
to a study group
943 Excluded:
125 declined participation
383 F2c / F3 ulcers
74 MalloryWeiss or gastric erosions
33 cancer ulcers
12 unstable condition or moribond
84 Had begun to receive PPI
27 unable to provide written informed
consent
43 on anticoagulation therapy
22 failed endoscopic therapy
140 Excluded for other reasons
1425 Evaluated
Figure 1. Flow chart of patients throughout the study.
Statistical AnalysisAll patients who took at least one dose of
drugs were includedinto the analysis. Categorical data were
expressed as propor-tions (%), and continuous data as means
standard deviation(SD). P values for the primary end point were
obtained fromthe two-sided 2 Pearsons test. For other P values, the
two-sample t-test was used for continuous variables and the
Fisherexact test used for discrete variables.
A prediction model for rebleeding was developed includ-ing the
following covariates: Rockall score ( or
-
3014 Andriulli et al.
Table 1. Characteristics of the 474 Patients Included in the
Analysis
Intensive Regimen Standard RegimenCharacteristic (N = 238) (N =
236)Ageyr 66.3 15.6 66.8 16.7Age > 70 yrno. (%) 116 (48.7) 121
(51.3)Menno. (%) 151 (63.4) 156 (66.1)Hemoglobing/dL 9.1 2.4 9.5
2.2Patients with hemoglobin 10 g/dLno. (%) 155 (65.1) 146
(61.9)
Shock at presentationno. (%) 20 (8.4) 35 (14.8)Rockall score
Mean SD 4.7 1.3 5.0 1.56 pointsno. (%) 64 (26.9) 81 (34.3)
Severe comorbidityno. (%) 19 (8.0) 30 (12.7)Bleeding during
hospitalization
no. (%) 10 (4.2) 15 (6.4)Risk factors for bleeding peptic
ulcerno. (%)
Use of NSAID 75 (31.5) 74 (31.4)Use of aspirin 72 (30.3) 82
(34.7)
Time from bleeding to endoscopy6 h 77 (32.4) 76 (32.1)Between 6
and 12 h 74 (31.1) 78 (32.2)Between 12 and 24 h 55 (23.1) 49
(20.8)>24 h 32 (13.4) 33 (13.9)
Previous ulcer diseaseno. (%) 32 (13.4) 36 (15.3)Previous
bleedingno. (%) 25 (10.5) 14 (5.9)Peptic ulcer as source of
bleedingno. (%)
Duodenal ulcer 150 (63.0) 143 (60.6)Gastric ulcer 88 (37.0) 93
(39.4)
Ulcer size 20 mmno. (%) 21 (8.8) 15 (6.4)Forrest classification
of endoscopic stigmata of hemorrhageno. (%)
1 aspurting 25 (10.5) 25 (10.6)1 b oozing 82 (34.5) 73 (30.9)2
anonbleeding visible vessel 81 (34.0) 85 (36.0)2 badherent clot 50
(21.0) 53 (22.5)
Endoscopic hemostasis modalityno. (%)Unimodal 119 (50.0) 136
(57.6)Multimodal 119 (50.0) 100 (42.4)
Type of PPI administeredno. (%)Omeprazole 167 (70.2) 163
(69.1)Pantoprazole 71 (29.8) 73 (30.9)
NSAID = nonsteroidal anti-inflammatory drug; PPI = proton pump
inhibitor; SD = standard deviation.
therapy (Table 1): two-thirds of patients were men, abouthalf
were older than 70 yr, and a majority had taken aspirinor
nonsteroidal anti-inflammatory drugs before hospitaliza-tion.
Nineteen and 30 patients in the intensive and standardregimen
groups, respectively, presented with a severe comor-bidity (P =
0.09). Equal proportions of patients bled duringtheir hospital stay
for unrelated illnesses. Signs of hemody-namic instability were
more frequent in the standard regimen:shock was more common, mean
Rockall score higher, andmore patients had a Rockall score 6. An
equal number ofpatients had duodenal and gastric ulcers, and
prevalence ofactive arterial bleeding, oozing, nonbleeding visible
vessel, oradherent clot was not significantly different. (Table 1).
Abouthalf of ulcers were injected with epinephrine solution, and
theremaining received epinephrine in association with
thermaltherapy (bipolar electrocoagulation or argon plasma
coagula-tion) or apposition of clips. In the two treatment groups,
70%of patients received omeprazole and the remaining patients
received pantoprazole. All patients completed the
assignedschedule of PPIs administration. No drug-related side
effectswere reported in either group.
Bleeding recurred in 28 patients (11.8%, CI 7.616.0) inthe
intensive regimen group and in 19 (8.1%, CI 4.511.5)in the standard
regimen group; a difference of 3.8% (CI 1.7to 9.1%) (P = 0.18)
(Table 2). At the repeat endoscopy, 9lesions were spurting ulcers,
20 oozing, 13 had a nonbleed-ing visible vessel, 3 an adherent
clot, all but 2 of previouslesions were successfully controlled by
a second attempt atendoscoscopic hemostasis; the remaining 3
lesions were clas-sified as Forrest 2c or 3 and were not treated
endoscopically.Recurrent bleeding was most common during the period
ofintravenous administration: within the first 3 days, 16 pa-tients
(6.7%, CI 3.59.9) in the intensive regimen group and22 (9.3%, CI
5.513.1) in the standard regimen experiencedrebleeding (P = 0.32).
Between the two treatment groups,rebleeding rates did not differ
for gastric and duodenal ulcers
-
Proton-Pump Inhibitors After Endoscopic Hemostasis 3015
Table 2. Clinical Outcomes for the 47 Patients Included in the
Analysis
Intensive Regimen Standard RegimenCharacteristic (N = 238) (N =
236) P ValueRebleedingno. (%) 28 (11.8) 19 (8.1) 0.18Rebleeding
according to Forrest classification of endoscopic stigmata of
hemorrhageno. (%)
1 aspurting 5 (2.1) 5 (2.1)1 boozing 11 (4.6) 8 (3.4)2
anonbleeding visible vessel 7 (2.9) 5 (2.1)2 badherent clot 5 (2.1)
1 (0.4) 0.61
Rebleeding according to time from index endoscopyno. (%)24 h 13
(5.5) 10 (4.2)>24 h to 7 days 15 (6.3) 9 (3.8) 0.68
Rebleeding according to Rockall score: no. (%)
-
3016 Andriulli et al.
11.8% and 8.0% of patients, respectively, with a correspond-ing
3.8% (CI 1.7 to 9.1%) difference in proportions. The sta-tistically
equal rebleeding rate between the two intravenousPPI strategies is
of relevance considering that patients treatedwith bolus PPIs
presented more frequently with shock andsigns of hemodynamic
instability, two predictors of worseoutcome (12, 14). Our negative
results are in keeping withnegative data from four previous trials
that compared thetwo PPI strategies (710), but are at odds with the
Lin re-port (15). Therefore, we cannot endorse the reccommen-dation
issued by two consensus statements on the routineuse of the
intensive PPI regimen for peptic ulcer bleeding(2, 3).
The 11.8% and 8.1% rebleeding rates with intensive orstandard
regimens, reported in this study, are in keeping withthe 13.2%
probability of rebleeding reported in a pooled anal-ysis of data
from eight trials on high-dose PPI infusion (13).Consequently, the
divergent results between our study andprevious trials are unlikely
to reflect major differences in pa-tients populations or endoscopic
interventions. Reasons forthe discrepancy might be revealed by
carefully inspectingthe comparator used in previous trials:
whenever endoscopichemostasis was not applied, intravenous PPI
therapy reducedthe rate of rebleeding when compared with placebo
(16, 17)or H2-receptor antagonists (18). However, in patients
whounderwent simultaneous endoscopic hemostasis, two trialsreported
opposite results with the intensive PPI dosing ver-sus placebo (5,
6), a single report showed a benefit of high-dose PPI therapy in
comparison to H2R antagonists (1921),and four studies did not show
a significant difference be-tween an intensive regimen and standard
bolus PPI injections(710).
As intravenous PPI therapy is expensive, to be cost-effective
the extra cost of the medication must be offset bya reduction in
the occurrence of important adverse clinicaloutcomes. In our study,
patients who received the high-dosePPI regimen had no advantage
with respect to transfusion re-quirement, need for surgery, length
of hospital stay, or deathrate. Moreover, cost-effectiveness
analyses have yielded con-trasting results regarding which of the
two PPIs administra-tion strategies, oral (22) or intravenous (23),
is more effectivein patients who have received concomitant
endoscopic treat-ment. Standard PPI dosing has the obvious
advantage of re-duced cost and was not shown to increase the risk
of nonulcerdeaths (15, 17).
The rationale for the need for profound gastric acid
sup-pression in peptic ulcer bleeding is extrapolated largely
fromin vitro evidences that an acidic environment impairs
plateletfunction and clot stabilization (3, 4). These in vitro data
havebeen taken as supportive evidences for the in vivo
clinicalbenefit. However, in healthy non-Asian volunteers, who
aretypically Helicoacter pylori negative and rapid PPI
metabo-lizers, the currently accepted high-dose PPI regimen
main-tained intragastric pH above 6 for only 30% of the time
(24,25), thus raising the possibility that we may not be achiev-ing
the theoretically desirable pH even with intensive therapy.
Findings from this investigation indicate that we may not
needintragastric pH maintained at
-
Proton-Pump Inhibitors After Endoscopic Hemostasis 3017
What Is New Here
We report the results of a multicentre randomizedcontrolled
trial comparing an intensive high-doseacid-inhibiting regimen
versus a low-dose standardregimen in the management of high-risk
peptic ulcer-related bleeding after performance of appropriate
en-doscopic hemostasis: no significant difference in out-comes was
registered between the two regimens. Thesedata demonstrate that
3-day PPI infusion can be re-placed with a once-daily intravenous
bolus, support-ing the use of a low-dose regimen for its
cost-savingpotential.
Reprint requests and correspondence: Angelo Andriulli,
M.D.,Division of Gastroenterology, Casa Sollievo della Sofferenza
Hos-pital, IRCCS, 71013, San Giovanni, Rotondo, Italy.
Received November 9, 2007; accepted May 5, 2008.
REFERENCES
1. British Society of Gastroenterology Endoscopy Commit-tee.
Non-variceal upper gastrointestinal hemorrhage: Guide-lines. Gut
2002;51(Suppl 4):iv16.
2. Barkun A, Bardou M, Marshall JK, for the NonvaricealUpper GI
Bleeding Consensus Conference Group. Con-sensus recommendations for
managing patients with non-variceal upper gastrointestinal
bleeding. Am Intern Med2003;139:84357.
3. Green FW Jr., Kaplan MM, Curtis LE, et al. Effect of acidand
pepsin on blood coagulation and platelet aggregation.A possible
contributor prolonged gastroduodenal mucosalhemorrhage.
Gastroenterology 1978;74:3843.
4. Patchett SE, Enright H, Afdhal N, et al. Clot lysis by
gastricjuice: An in vitro study. Gut 1989;30:10747.
5. Schaffalitzky de Muckadell UB, Havelund T, Harling H,et al.
Effects of omeprazole on the outcome of endo-scopically treated
peptic ulcers. Scand J Gastroenterol1997;32:3207.
6. Lau JYW, Sung JJY, Lee KKC, et al. Effect of
intravenousomeprazole on recurrent bleeding after endoscopic
treat-ment of bleeding peptic ulcers. N Engl J Med
2000;343:3106.
7. Schonekas H, Ahrens H, Pannewick U, et al. Comparisonof two
doses of intravenous pantoprazole in peptic ulcerbleeding.
Gastroenterology 1999;116:A305.
8. Udd M, Miettinen P, Palmu A, et al. Regular-dose
versushigh-dose omeprazole in peptic ulcer bleeding: A prospec-tive
randomized double-blind study. Scand J
Gastroenterol2001;36:13328.
9. Dokas SM, Lazaraki GI, Kontoninas Z, et al. Bolus
intra-venous omeprazole b.i.d vs. continuous intravenous
omepra-zole infusion combined with endoscopic hemostasis in
thetreatment of peptic ulcer bleeding. Preliminary results.
Gut2004;53(Suppl VI):A290.
10. Bajaj JS, Dua KS, Hanson K, et al. Prospective,
randomizedtrial comparing effect of oral versus intravenous
pantopra-zole on rebleeding after nonvariceal upper
gastrointestinalbleeding: A pilot study. Dig Dis Sci
2007;52:21904.
11. Andriulli A, Annese V, Caruso N, et al. Proton-pump
in-hibitors and outcome of endoscopic hemostasis in bleeding
peptic ulcer: A series of meta-analysis. Am J
Gastroenterol2005;100:20719.
12. Rockall TA, Logan RF, Devlin HB, et al. Risk assess-ment
after acute upper gastrointestinal haemorrhage.
Gut1996;38:31621.
13. Leontiadis GI, Sharma VK, Howden CW. Proton pump in-hibitor
treatment for acute peptic ulcer bleeding. CochraneDatabase Syst
Rev 2006;1:CD0020947.
14. Saeed ZA, Ramirez FC, Hepps KS, et al. Prospective
vali-dation of the Baylor bleeding score for predicting the
like-lihood of rebleeding after endoscopic hemostasis of
pepticulcers. Gastrointest Endosc 1995;41:5615.
15. Lin HJ, Lo WC, Chen YC, Perng CL. Role of
intravenousomeprazole in patients with high-risk of peptic ulcer
bleed-ing after successful endoscopic epinephrine injection:
Aprospective randomized comparative trial. Am J Gastroen-terol
2006;101:5005.
16. Hasselgren G, Lind T, Lundell L, et al. Continuous
intra-venous infusion of omeprazole in elderly patients with
pep-tic ulcer bleeding: Results of a placebo controlled
multicen-ter study. Scand J Gastroenterol 1997;32:32833.
17. Khuroo MS, Farahat KL, Kagevi IE. Treatment with pro-ton
pump inhibitors in acute non-variceal upper gastroin-testinal
bleeding: A meta-analysis. J Gastroenterol Hepatol2005;20:1125.
18. Cardi M, Muttillo IA, Amadori L, et al. Omeprazole ver-sus
ranitidine intraveineux dans le traitment de lulce`reduodenal
hemorragique: Une etude randomisee prospective.Ann Chir
1997;51:1369.
19. Labenz J, Peitz U, Leusing C, et al. Efficacy of primed
infu-sions with high dose ranitidine and omeprazole to maintainhigh
intragastric pH in patients with peptic ulcer bleeding:
Aprospective randomised controlled study. Gut 1997;40:3641.
20. Fried R, Beglinger C, Meier R, et al. Comparison of
intra-venous pantoprazole with intravenous ranitidine in
pepticulcer bleeding. Gut 1999;45(Suppl V):A100.
21. Lin HJ, Lo WC, Lee FY, et al. A prospective
randomisedcomparative trial showing tat omeprazole prevents
rebleed-ing in patients with bleeding peptic ulcer after
endoscopictherapy. Arch Intern Med 1998;158:548.
22. Spiegel BM, Dulai GS, Lim BS, et al. The
cost-effectivenessand budget impact of intravenous versus oral
proton pumpinhibitors in peptic ulcer hemorrhage. Clin
GastroenterolHepatol 2006;4:98897.
23. Barkun AN, Herba K, Adam V, et al. The cost-effectivenessof
high-dose oral proton pump inhibition after endoscopy inthe acute
treatment of peptic ulcer bleeding. Aliment Phar-macol Ther
2004;20:195202.
24. Netzer P, Gaia C, Sandoz M, et al. Effect of repeated
injec-tion and continuous infusion of omeprazole and ranitidine
onintragastric pH over 72 h. Am J Gastroenterol 1999;94:3517.
25. Metz DC, Amer F, Hunt B, et al. Lansoprazole regimens
thatsustain intragastric pH >6: AN evaluation of
intermittentoral and continuous intravenous lansoprazole or
ranitidine.Aliment Pharmacol Ther 1999;23:98595.
26. Welage LS, Berardi RR. Evaluation of omeprazole,
lan-soprazole, pantoprazole, and rabeprazole in the treatmentof
acid-related diseases. J Am Pharm Assoc 2000;40:5262.
27. Chilovi F, Piazzi L, Zancanella L, et al.
Intravenousomeprazole and pantoprazole after endoscopic treatmentof
bleeding peptic ulcers. Gastrointest Endosc 2003;57:AB150.
28. Marmo R, Rotondano G, Piscopo R, et al. Dual ther-apy versus
monotherapy in the endoscopic treatment of
-
3018 Andriulli et al.
high-risk bleeding ulcers: A meta-analysis of controlledtrial.
Am J Gastroenterol 2007;102:27989.
29. ASGE guideline: The role of endoscopy in acute non-variceal
upper-GI hemorrhage. Gastrointest Endosc 2004;60:497504.
30. Pilotto A, Franceschi M, Longoa MG, et al. Helicobacter
py-lori infection and the prevention of peptic ulcer with
protonpump inhibitors in elderly subjects taking low-dose
aspirin.Dig Liver Dis 2004;36:66670.
31. Jensen DM, Pace SC, Soffer E, et al., and members of the
315Study Group. Continuous infusion of pantoprazole
versusranitidine for prevention of ulcer rebleeding: A U.S.
multi-center randomized, double-blind study. Am J
Gastroenterol2006;101:19919.
CONFLICT OF INTEREST
Guarantor of the article: Angelo Andriulli, M.D.Specific author
contributions: Angelo Andriulli designedthe study, wrote the
original draft of the protocol, discussedit with the Ethics
committee of the coordinating centre, acted
as the coordinator of the entire study, supervised the
statisti-cal analysis of trial data, and wrote the manuscript.
SilvanoLoperfido discussed and amended the original draft of
theprotocol, presented and discussed the study with the localEthics
committee, enrolled patients to the study, and reviewedthe final
version of the manuscript. Rosaria Focareta, PietroLeo, Fabio
Fornari, Antonietta Garritoli, Paolo Tonti, Ser-gio Peyre, Antonio
Spadaccini, Riccardo Marmo, Alessan-dro Caroli, Gian Battista
Forte, Angelo Belmonte, GiovanniAragona, Gianni Imperiali, Fabrizio
Forte, Fabio Monica,Nazario Caruso agreed on the final version of
the protocol ofthe study, discussed the protocol with their local
Ethics com-mittees, enrolled patients to the study, and agreed on
the finalversion of the manuscript. Antonio Merla enrolled
patientsto the study, collected data from contributing
investigators,and managed the electronic database. Francesco Perri
ran thestatistical analysis of experimental data.Financial support:
None.Potential competing interests: None.


![sNDA Approval [Rx ONLY] (COR-SNDAACTION-05) · Oral Hypoglycemics 7.13 . Proton Pump Inhibitors, H2 Blockers, Antacids 7.14 . Warfarin 7.15 . Concomitant Drugs That Do Not Need Dose](https://img.pdfslide.us/doc/110x75/5f024d097e708231d4039636/snda-approval-rx-only-cor-sndaaction-05-oral-hypoglycemics-713-proton-pump.jpg)