Embed Size (px)
Citation preview
High-SPF sunscreens (SPF $ 70) may provideultraviolet protection above minimal recommended
levels by adequately compensating for lowersunscreen user application amounts
Hao Ou-Yang, PhD,a Joseph Stanfield, MS,b Curtis Cole, PhD,c Yohini Appa, PhD,a and Darrell Rigel, MDd
Los Angeles, California; Winston Salem, North Carolina; Skillman, New Jersey; and New York, New York
From
to
C
C
Fund
m
C
Discl
C
C
C
is
pe
122
Background: The manner in which consumers apply sunscreens is often inadequate for ultravioletprotection according to the labeled sun protection factor (SPF). Although sunscreen SPFs are labeled bytesting at an application density of 2 mg/cm2, the actual protection received is often substantially lessbecause of consumer application densities ranging from 0.5 to 1 mg/cm2. High-SPF sunscreens mayprovide more adequate protection even when applied by consumers at inadequate amounts.
Objective: We sought to measure the actual SPF values of various sunscreens (labeled SPF 30-100) appliedin amounts typical of those used by consumers.
Methods: Actual SPF values were measured on human volunteers for 6 sunscreen products with labeledSPF values ranging from 30 to 100, applied at 0.5, 1.0, 1.5, and 2.0 mg/cm2.
Results: There was a linear relationship between application density and the actual SPF; sunscreens withlabeled SPF values of 70 and above provided significant protection, even at the low application densitiestypically applied by consumers. Sunscreens labeled SPF 70 and 100 applied at 0.5 mg/cm2 provided anactual SPF value of, respectively, 19 and 27.
Limitations: The study was conducted in a laboratory setting under standardized conditions and resultsare extrapolated to actual in-use situations.
Conclusion: Sunscreens with SPF 70 and above add additional clinical benefits when applied by consumersat typically used amounts, by delivering an actual SPF that meets the minimum SPF levels recommended forskin cancer and photodamage prevention. In contrast, sunscreens with SPF 30 or 50 may not producesufficient protection at actual consumer usage levels. ( J Am Acad Dermatol 2012;67:1220-7.)
Key words: minimal erythema dose; sun protection; sunburn; sunburn protection factor; sunscreens;ultraviolet protection.
The harmful effects of ultraviolet (UV) radia-tion on the skin have been known for quitesome time. Exposure to UV radiation leads
not only to skin photodamage1 but, more
Neutrogena Corp, Los Angelesa; Suncare Research Labora-
ries LLC, Winston Salemb; Johnson and Johnson Consumer
ompanies, Skillmanc; and New York University Medical
enter.d
ed in full by Neutrogena Corp; the preparation of this
anuscript was sponsored in full by Johnson and Johnson
onsumer Companies.
osure: Drs Ou-Yang and Appa are employees of Neutrogena
orp, the manufacturer of two of the sunscreens tested. Dr
ole is an employee of Johnson and Johnson Consumer
ompanies, a sister company of Neutrogena Corp. Mr Stanfield
an employee of Suncare Research Laboratories, the inde-
ndent testing laboratory that received compensation for
0
importantly, to immunosuppression2 and skin can-cers3 such as squamous cell carcinoma,4 basal cellcarcinoma,5 and melanoma.6,7 To reduce the inci-dence of UV-related skin cancers, the American
conducting this study, and he is currently a consultant to
Galderma Laboratories LP. Dr Rigel is a consultant for Neu-
trogena Corp, Johnson and Johnson Consumer Companies,
Beiersdorf, and P&G.
Previously presented as a poster at the 69th American Academy of
Dermatology Annual Meeting, New Orleans, Feb. 4-8, 2011.
Accepted for publication February 17, 2012.
Reprint requests: Hao Ou-Yang, PhD, Neutrogena Corp, 5760 W 96
St, Los Angeles, CA 90045. E-mail: [email protected].
Published online April 1, 2012.
0190-9622/$36.00
� 2012 by the American Academy of Dermatology, Inc.
doi:10.1016/j.jaad.2012.02.029
J AM ACAD DERMATOL
VOLUME 67, NUMBER 6Ou-Yang et al 1221
Academy of Dermatology recommends, amongother measures, the generous application of a‘‘broad-spectrum, water-resistant sunscreen withsun protection factor (SPF) of at least 30 to allexposed skin.’’8
Many studies have shown that sunscreens canprotect fromUV-induced damage and skin cancer.9-12
CAPSULE SUMMARY
d Consumers typically apply sunscreensunevenly and in amounts lower thanrecommended, reducing the actualsunburn protection factor.
d Sunscreens with sun protection factor of70 and above yield significant protectioneven when underapplied in typicalconsumer use situations.
d Sunscreens with sun protection factor of70 and above may deliver the minimalSPF levels for skin cancer andphotodamage prevention, even whenmisused or under-applied.
The determination of theirSPF value is regulated bythe Food and DrugAdministration (FDA) andother internationally recog-nized testing standards,which all dictate that sun-screens be tested at an appli-cation density of 2 mg/cm2.13,14 However, several in-vestigations have shown thatconsumers typically applyless than 2 mg/cm2,15-20 thusreducing the actual protec-tion of the sunscreen.21-23 Inan open study conducted atthe beach on 42 volunteers,Bech-Thomsen and Wulf15
calculated that the average
sunscreen density applied by sunbathers was 0.5mg/cm2. Another group assessed the amount ofsunscreen applied by 10 women with photosensitiveskin conditions, as they would use it during a sunnyday; they found that the median application dose was0.5 mg/cm2, with site variations from 0 to 1.2 mg/cm2.16 Grosick and Tanner17 reported a study inwhich 700 women were given free access to varioussunscreens SPF 15 and higher to be used over 3 to 6weeks; the study found that the SPF achieved in actualuse was below that of the labeled SPF. Investigationson sunscreen application by beachgoers have furtherconfirmed that consumers rarely apply sunscreensuniformly and usually do not reapply them oftenenough, particularly after swimming.18,19In 2011, the FDA proposed to cap the labeled SPFat ‘‘501,’’ stating that there is insufficient evidencethat SPF values above 50 produce additional clinicalbenefits.24 However, a consumer in-use study con-ducted to compare the efficacy of a sunscreen withSPF 50 versus one with SPF 85 demonstrated that thehigher SPF sunscreen provided better sunburn pro-tection.25 In addition, it is widely presumed thathigh-SPF sunscreens may deliver an SPF adequatefor skin cancer and photodamage prevention evenwhen underapplied by consumers.
The purpose of this study was to test the actualSPFs of sunscreens with labeled SPFs 30 to 100 underthe reduced densities that are typically applied by
users, to determine if high-SPF products applied perconsumer behavior would still yield an SPF adequatefor skin cancer prevention,26 compared with lowerSPF products.
METHODSThis study evaluated the effects of various appli-
cation densities on the actualSPF values of 6 sunscreenproducts, with labeled SPFsranging from 30 to 100. Theinvestigation was designedwith a 2-step approach. Aninitial study (study A) wasconducted on 251 volunteersto determine the SPF value of6 sunscreens (labeled SPFfrom 30-100) at 4 differentapplication densities (0.5,1.0, 1.5, and 2.0 mg/cm2).The second study (study B),conducted on 76 volunteersafter the results of study Awere reviewed, was carriedout to compare the SPFvalues of the 6 sunscreens
at low application densities (0.5 and 1 mg/cm2) sideby side.
Both studies were single center, controlled, ran-domized, and evaluator blinded. Subjects weremale/female healthy volunteers with Fitzpatrickskin types I, II, and III.27 To facilitate estimation ofthe minimal erythema dose (MED), colorimetricmeasurements of each subject’s skin were obtainedaccording to the international SPF method, and theindividual typology angle value was computed.14
Both studies were conducted in accordance to theFDA final monograph on sunscreen products13,28
and to the Declaration of Helsinki principles; proto-cols and informed consent were approved by anindependent institutional review board.
Test sunscreen formulations and test sitesSix US-marketed sunscreen formulations were
tested (4 lotions and two sprays). The 4 lotionswere selected based on similar vehicles and types ofactive ingredients. The two sprays also containedsimilar types of active ingredients. The test productswere:(A) SPF 30 lotion sunscreen (Coppertone Sport 30,
SPF 30, Schering-Plough HealthCare ProductsInc, Memphis, TN).
(B) SPF 100 lotion sunscreen (Neutrogena UltraSheer Lotion SPF 100, Neutrogena Corp, LosAngeles, CA).
Abbreviations used:
FDA: Food and Drug AdministrationMED: minimal erythema doseSPF: sunburn protection factorUV: ultraviolet
J AM ACAD DERMATOL
DECEMBER 20121222 Ou-Yang et al
(C) SPF 100 spray sunscreen (Neutrogena UltimateSport Spray SPF 100, Neutrogena Corp, LosAngeles, CA).
(D) SPF 50 lotion sunscreen (Coppertone Sport501, SPF 501, Schering-Plough HealthCareProducts Inc, Memphis, TN).
(E) SPF 50 spray sunscreen (Coppertone Sport 50Continuous Spray, SPF 501, Schering-PloughHealthCare Products Inc, Memphis, TN).
(F) SPF 70 lotion sunscreen (Coppertone Sport701, SPF 701, Schering-Plough HealthCareProducts Inc, Memphis, TN).
The formulations were applied to the subject’sback using a pipette and delivered in small dropletswithin pre-outlined skin sites; the droplets werespread as quickly and uniformly as possible using afinger cot. For spray-on products, formulations werefirst sprayed into a beaker and swirled until nobubbles remained before being transferred to skin bypipette.
In study A, the 6 test products at the 4 applicationdensities were randomized among skin sites andsubjects. Each subject received a standard sunscreen(homosalate 8%)28 and up to 3 test products, appliedat one of the 4 application densities (0.5, 1.0, 1.5, and2.0 mg/cm2) so that each test product was evaluatedat all 4 amounts on at least 20 subjects. The 8%homosalate control was obtained commercially andhad a labeled SPF of 4.
In study B, the SPF determination of the 6sunscreen formulations applied at 0.5 and 1.0 mg/cm2 was conducted in 3 parallel panels of at least 20subjects each. Each subject received 4 test products/densities tested side by side to allow within-subjectcomparisons of similar types of products (Table I);each panel received a fixed product/density combi-nation: one panel compared the two sprays at bothapplication densities; a second panel compared the 4lotions applied at 0.5 mg/cm2; and a third panelcompared the 4 lotions applied at 1.0 mg/cm2. Testproducts and/or densities were randomized withineach panel.
UV sourceSingle-port xenon arc solar simulators (model
16S, Solar Light Co, Glenside, PA) were used toadminister UV doses. Output spectra of the light
sources were calibrated using spectroradiometricmeasurements (model OL756 spectroradiometer,Optronic Laboratories, Orlando, FL) and were foundto meet the specifications for UV spectral distributionoutlined in the FDA proposed amendment to thesunscreen monograph13 and the international SPFmethod.14
ProceduresA total of 251 volunteers were enrolled in study A
and 76 volunteers were enrolled in study B. Study Bwas conducted after reviewing the results from studyA. Both studies followed the same procedures be-low, except where indicated.
Day 1eMED determination. On day 1, 5 UVdoses, progressively increasing by 25% increments,were applied to predetermined unprotected sites ofthe mid aspect of the back, as indicated in the FDAsunscreen monograph.28 Within 22 to 24 hours afterirradiation, subjects returned to the testing laboratoryfor evaluation of UV-induced skin responses. Ablinded trained evaluator graded the UV exposedsites for erythema using a warm fluorescent lampemitting 450 to 550 lux: the MEDwas the smallest UVdose in the series to produce the first mild erythemawith clearly defined borders.
Day 2eapplication of products and UV dosesfor static SPF determination. Study A. On day2, two to four 50-cm2 rectangles were marked on thesubject’s back between the belt line and shoulderblades. The number of sites depended on theexpected SPF: only two high-SPF products couldbe tested together at the higher dose levels, becauseof the long exposure times. A technician applied therandomized density (0.5, 1.0, 1.5, or 2.0 mg/cm2) ofone to three test products and the homosalatestandard sunscreen (2.0 mg/cm2) to the designatedrectangles on the subject’s back. Test product allo-cation was determined by randomization. After atleast 15 minutes from application, 7 progressive UVdoses were applied to determine the MED forsunscreen-treated skin sites. Dose series were calcu-lated by multiplying the expected SPF of eachformulation, the initial subject’s unprotected MED,and the following number: 0.76, 0.87, 0.93, 1.00,1.07, 1.15, and 1.32.28
Expected SPF values were based on in vitro mea-surements of each product at the 4 applicationdensities: they were anticipated to be approximately75%, 50%, and 25% of the labeled SPF for applicationdensities of 1.5, 1, and 0.5 mg/cm2, respectively.
Study B. On day 2, four 50-cm2 rectangles weremarked on the subject’s back between the belt lineand shoulder blades. A technician applied the ran-domized density (0.5 or 1.0mg/cm2) of the 4 selected

Table I. Test product allocation
Test products
Panel 1 (20 subjects) (E) SPF 50 spray at 0.5 mg/cm2 (C) SPF 100 spray at 0.5 mg/cm2
(E) SPF 50 spray at 1.0 mg/cm2 (C) SPF 100 spray at 1.0 mg/cm2
Panel 2 (20 subjects) (A) SPF 30 lotion at 0.5 mg/cm2 (D) SPF 50 lotion at 0.5 mg/cm2
(F) SPF 70 lotion at 0.5 mg/cm2 (B) SPF 100 lotion at 0.5 mg/cm2
Panel 3 (20 subjects) (A) SPF 30 lotion at 1.0 mg/cm2 (D) SPF 50 lotion at 1.0 mg/cm2
(F) SPF 70 lotion at 1.0 mg/cm2 (B) SPF 100 lotion at 1.0 mg/cm2
SPF, Sunburn protection factor.
J AM ACAD DERMATOL
VOLUME 67, NUMBER 6Ou-Yang et al 1223
test products in their designated rectangles. The testproducts to be applied were determined by a ran-domization code balanced by panel, applicationdensity, and site location, to the maximum extentpossible. At least 15 minutes after application, 7progressive UV doses were applied to determine theMED for sunscreen-treated skin sites. Dose serieswere calculated as in study A.
Expected SPF values were based on the in vitromeasurements of each product at the two applicationdensities (study A): they were anticipated to beapproximately 50% and 25% of the labeled SPF forapplication densities of 1.0 and 0.5 mg/cm2,respectively.
Day 2erepeated MED determination. On day2, 5 UV doses, progressively increasing by 25%increments, were also readministered to an unpro-tected area of the mid aspect of the back. The 5-doseseries was calculated based on multiples of theoriginal MED, as follows: 0.64, 0.80, 1.00 (originalMED), 1.25, and 1.56.
Day 3eevaluation of responses for SPF cal-culation and repeated MED. Skin responseswere evaluated 22 to 24 hours after administrationof UV doses (day 3), using the 7-point erythemagrading scale. Grading was conducted by a trainedevaluator, who did not participate in product appli-cations or administration of UV doses.
SPF computationAfter determination of the repeated MED as
detailed above, SPF values were calculated for eachsubject as follows: Individual SPF = MED of pro-tected skin/repeated MED of unprotected skin.
Mean SPF values and statistical information foreach test product and application density were thencalculated.28
Statistical analysisA one-way analysis of variance was performed
within samples to test for differences in SPF by dose,and orthogonal contrasts were constructed to testlinearity of the dose response. Within each dose
group, between-sample comparisons were analyzedby a one-way analysis of variance. Panel 1 data wereanalyzed by a mixed linear model, with dependentvariable SPF values, and random model term fordose (0.5, 1.0) and fixed term for sample (C, E), andthe interaction of dose and sample. Panel 2 (at dose =0.5) and panel 3 (at dose = 1.0) data analysis used arepeatedmeasures analysis of variance to test for SPFdifferences among samples. Summary statistics forthese statistical analyses include the least-squaresmean difference between sample pairs and 95%confidence intervals, using Tukey-Kramer adjust-ment for multiple comparisons. Statistical analysiswas conducted using SAS software (SAS Institute Inc,Cary, NC) Version 9.2 on an XP Pro platform.
RESULTSStudy A
A total of 237 subjects completed the study and233 were included in SPF calculations. Data for 4subjects were excluded because of protocolviolations.
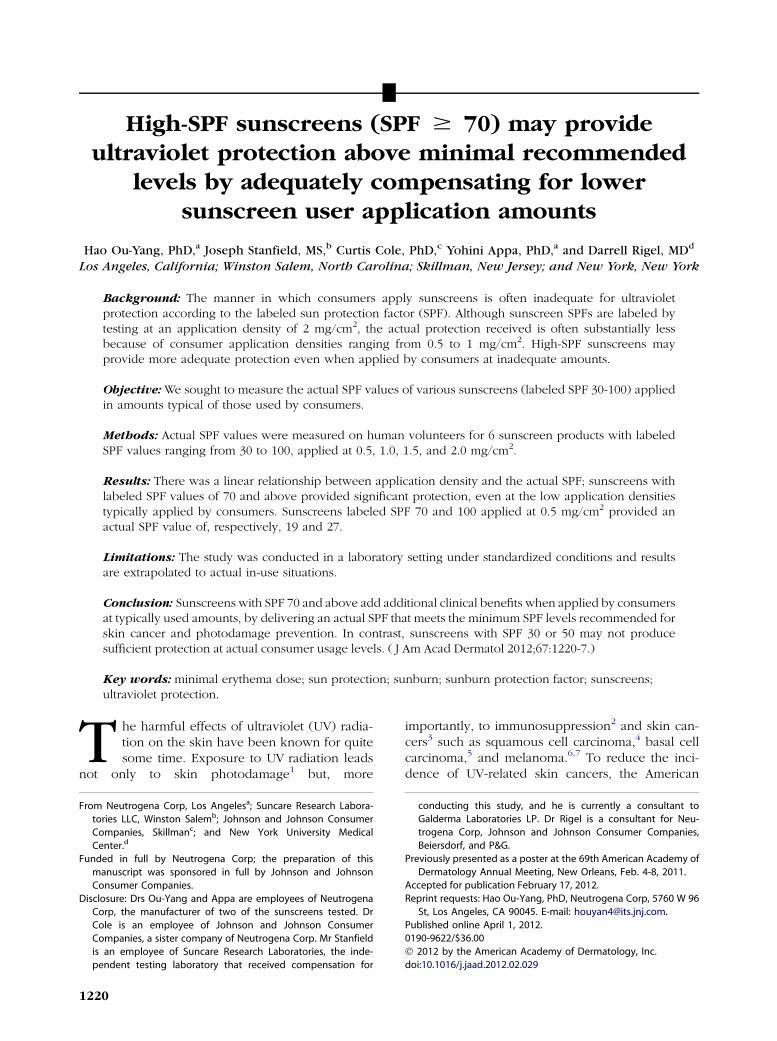
Mean SPF values and statistical information foreach test product and application density are pre-sented in Table II. For all 6 test sunscreens, the meanSPF value was progressively lower with lower appli-cation densities. However, reduced application den-sities yielded proportionately higher mean SPFvalues for products with higher labeled SPFs. SPFvalues for the 2.0-mg/cm2 application were slightlyhigher than labeled values. Measured SPF valueswere statistically different for sunscreens with differ-ent labeled SPF when tested at the same applicationdensity and were statistically different for the sameproduct when tested at different application densi-ties. Correlation coefficients (R2) for linear curve fitswere all greater than 0.99, suggesting a linear corre-lation between application densities of 0.5 to 2 mg/cm2 and SPF (Fig 1).
Study BA total of 65 subjects completed the study and all
were included in SPF calculations. The results are
Table II. Study A: sunburn protection factor results
AeLabel SPF: 30 DeLabel SPF: 501 FeLabel SPF: 701 BeLabel SPF: 100 EeLabel SPF: 50 spray CeLabel SPF: 100 spray
2 mg/cm2
Mean SPF 31.0 52.8 70.6 104.6 50.7 105.3SD 4.2 6.4 8.7 8.1 5.0 11.1n 20 21 20 20 20 2095% CI 1.9 2.7 3.8 3.6 2.2 4.9
1.5 mg/cm2
Mean SPF 21.8 41.3 54.4 79.3 38.6 75.0SD 2.4 4.2 5.0 7.4 4.3 8.0n 20 20 20 20 20 2095% CI 1.1 1.8 2.2 3.2 1.9 3.5
1 mg/cm2
Mean SPF 16.0 26.0 37.1 55.9 25.7 50.1SD 1.3 2.5 4.5 5.0 2.8 5.2n 20 20 20 20 20 2095% CI 0.6 1.1 2.0 2.2 1.2 2.3
0.5 mg/cm2
Mean SPF 8.8 13.9 19.3 27.1 12.6 22.4SD 1.1 1.5 1.4 1.6 1.5 3.1n 20 20 20 20 20 2095% CI 0.5 0.7 0.6 0.7 0.7 1.4
CI, Confidence interval; SPF, sunburn protection factor.
Fig 1. Correlation for study A. Correlation coefficients(R2) for linear curve fits were all greater than 0.99,suggesting linear relationship between applicationamount and sunburn protection factor (SPF ) for all testproducts.
J AM ACAD DERMATOL
DECEMBER 20121224 Ou-Yang et al
presented in Table III. The results confirmed thelinear relationship between amount of sunscreenapplied and static SPF value for the high-SPF sun-screens tested in study A, with the mean SPF valuefor 0.5-mg/cm2 applications resulting in approxi-mately 25% of the labeled SPF. At applications of 0.5
mg/cm2, the average SPF for labeled SPF 30was 9.11,for labeled 501 was 14.34, for labeled 701 was19.27, and for labeled 100 was 27.85. In thisside-by-side test, the sunscreens with the higherlabeled SPF values consistently provided statisticallybetter protection than the sunscreens with the lower-labeled SPF values at the application densities rele-vant to consumers.
DISCUSSIONIn recent years, advancements in sunscreen for-
mulations and access to photostabilized UV filtertechnology have allowed companies to manufactureproducts with SPF value up to 100. The marketing ofvery higheSPF products (SPF [50) has spurred anongoing debate questioning their added clinicalbenefits. Indeed, comparative investigations onvery higheSPF sunscreens are scant. Russak et al25
conducted a split-face, double-blind, randomizedstudy comparing an SPF 50with an SPF 85 product. Atotal of 56 skier/snowboarders applied each sun-screen once to the assigned side of the face during asunny day at high altitude and subjects were exposedto the sun during the snow activity for an average of5 hours. The results showed that the product withSPF 85 provided significantly more protectionagainst sunburn than the one with SPF 50.
Many studies have demonstrated that consumerstend to use significantly less product than recom-mended (0.5-1.0 mg/cm2) and in uneven applica-tions,15-20 with a decrease in actual sunburn
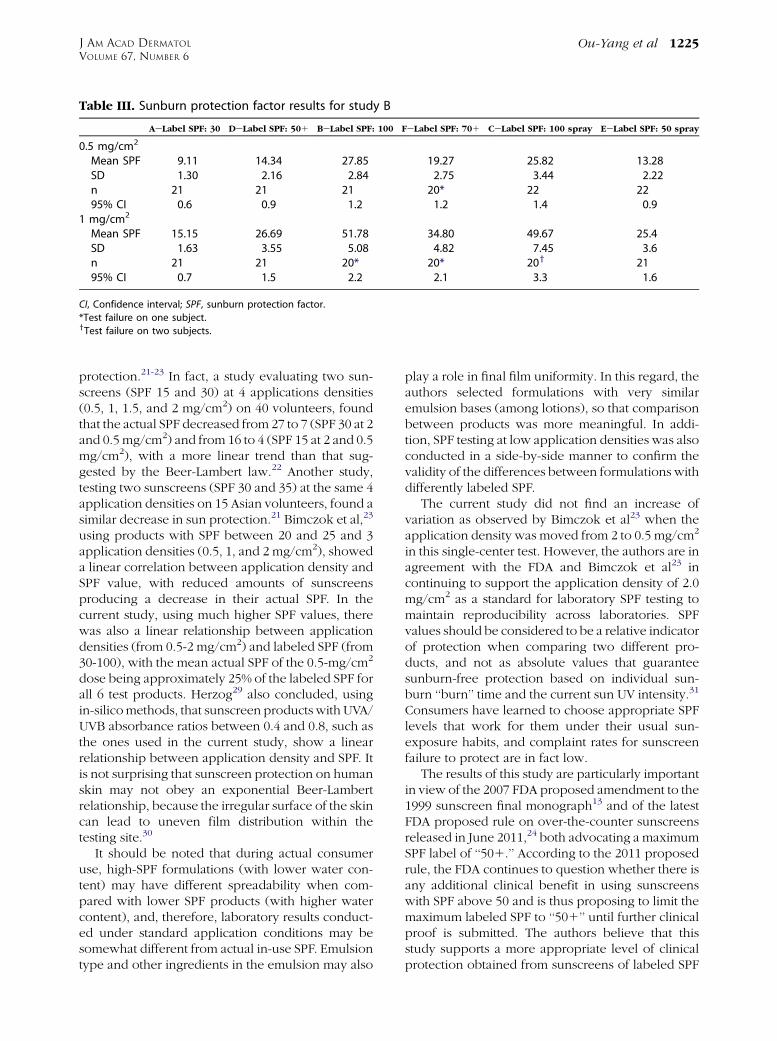
Table III. Sunburn protection factor results for study B
AeLabel SPF: 30 DeLabel SPF: 501 BeLabel SPF: 100 FeLabel SPF: 701 CeLabel SPF: 100 spray EeLabel SPF: 50 spray
0.5 mg/cm2
Mean SPF 9.11 14.34 27.85 19.27 25.82 13.28SD 1.30 2.16 2.84 2.75 3.44 2.22n 21 21 21 20* 22 2295% CI 0.6 0.9 1.2 1.2 1.4 0.9
1 mg/cm2
Mean SPF 15.15 26.69 51.78 34.80 49.67 25.4SD 1.63 3.55 5.08 4.82 7.45 3.6n 21 21 20* 20* 20y 2195% CI 0.7 1.5 2.2 2.1 3.3 1.6
CI, Confidence interval; SPF, sunburn protection factor.
*Test failure on one subject.yTest failure on two subjects.
J AM ACAD DERMATOL
VOLUME 67, NUMBER 6Ou-Yang et al 1225
protection.21-23 In fact, a study evaluating two sun-screens (SPF 15 and 30) at 4 applications densities(0.5, 1, 1.5, and 2 mg/cm2) on 40 volunteers, foundthat the actual SPF decreased from 27 to 7 (SPF 30 at 2and 0.5 mg/cm2) and from 16 to 4 (SPF 15 at 2 and 0.5mg/cm2), with a more linear trend than that sug-gested by the Beer-Lambert law.22 Another study,testing two sunscreens (SPF 30 and 35) at the same 4application densities on 15 Asian volunteers, found asimilar decrease in sun protection.21 Bimczok et al,23
using products with SPF between 20 and 25 and 3application densities (0.5, 1, and 2 mg/cm2), showeda linear correlation between application density andSPF value, with reduced amounts of sunscreensproducing a decrease in their actual SPF. In thecurrent study, using much higher SPF values, therewas also a linear relationship between applicationdensities (from 0.5-2 mg/cm2) and labeled SPF (from30-100), with the mean actual SPF of the 0.5-mg/cm2
dose being approximately 25% of the labeled SPF forall 6 test products. Herzog29 also concluded, usingin-silicomethods, that sunscreen products with UVA/UVB absorbance ratios between 0.4 and 0.8, such asthe ones used in the current study, show a linearrelationship between application density and SPF. Itis not surprising that sunscreen protection on humanskin may not obey an exponential Beer-Lambertrelationship, because the irregular surface of the skincan lead to uneven film distribution within thetesting site.30
It should be noted that during actual consumeruse, high-SPF formulations (with lower water con-tent) may have different spreadability when com-pared with lower SPF products (with higher watercontent), and, therefore, laboratory results conduct-ed under standard application conditions may besomewhat different from actual in-use SPF. Emulsiontype and other ingredients in the emulsion may also
play a role in final film uniformity. In this regard, theauthors selected formulations with very similaremulsion bases (among lotions), so that comparisonbetween products was more meaningful. In addi-tion, SPF testing at low application densities was alsoconducted in a side-by-side manner to confirm thevalidity of the differences between formulations withdifferently labeled SPF.
The current study did not find an increase ofvariation as observed by Bimczok et al23 when theapplication density was moved from 2 to 0.5 mg/cm2
in this single-center test. However, the authors are inagreement with the FDA and Bimczok et al23 incontinuing to support the application density of 2.0mg/cm2 as a standard for laboratory SPF testing tomaintain reproducibility across laboratories. SPFvalues should be considered to be a relative indicatorof protection when comparing two different pro-ducts, and not as absolute values that guaranteesunburn-free protection based on individual sun-burn ‘‘burn’’ time and the current sun UV intensity.31
Consumers have learned to choose appropriate SPFlevels that work for them under their usual sun-exposure habits, and complaint rates for sunscreenfailure to protect are in fact low.
The results of this study are particularly importantin view of the 2007 FDA proposed amendment to the1999 sunscreen final monograph13 and of the latestFDA proposed rule on over-the-counter sunscreensreleased in June 2011,24 both advocating a maximumSPF label of ‘‘501.’’ According to the 2011 proposedrule, the FDA continues to question whether there isany additional clinical benefit in using sunscreenswith SPF above 50 and is thus proposing to limit themaximum labeled SPF to ‘‘501’’ until further clinicalproof is submitted. The authors believe that thisstudy supports a more appropriate level of clinicalprotection obtained from sunscreens of labeled SPF
J AM ACAD DERMATOL
DECEMBER 20121226 Ou-Yang et al
values above 50 when used at doses more consistentwith consumer behavior. In fact, sunscreens with SPF70 and above, when broad spectrum, can provide amargin of safety for consumers by yielding at least anSPF 19 in this study even at concentrations as low as0.5 mg/cm2, exceeding the minimal requirement ofSPF 15 and thereby decreasing the subsequent risk ofskin cancer and photodamage, based on currentFDA recommendations,26 whereas sunscreens at orbelow SPF 50 may not produce enough protection atthe same dose (actual SPF 13-14 in this study). It isnoteworthy that the SPF 30 sunscreen deliveredactual mean SPFs 15.15 and 9.11 when applied,respectively, at 1 and 0.5 mg/cm2, thus providinginadequate effectiveness at 0.5 mg/cm2 based oncurrent recommendations for decreasing skin cancerrisks.
In summary, sunscreens with SPF 70 and aboveadd additional clinical benefits when applied byconsumers at typically used concentrations by deliv-ering an actual SPF that meets the minimum SPFlevels recommended for skin cancer and photo-damage prevention. In contrast, sunscreens with SPF30 or 50 may not produce sufficient protection atactual consumer use levels.
The authors would like to thankDr Alessandra Pagnoni,of Pagnoni Consulting LLC, for her writing and editorialassistance in the preparation of this manuscript. DrPagnoni is a consultant for Johnson and JohnsonConsumer Companies and Neutrogena Corp. The authorswould also like to thank Mark Van Buskirk, of DataReduction, for statistical analysis of the study data. MrVan Buskirk is a consultant for Johnson and JohnsonConsumer Companies.
REFERENCES
1. Gilchrest BA, Szabo G, Flynn E, Goldwyn RM. Chronologic and
actinically induced aging in human facial skin. J Invest
Dermatol 1983;80:81S-5S.
2. Aubin F. Mechanisms involved in ultraviolet light-induced
immunosuppression. Eur J Dermatol 2003;13:515-23.
3. Rigel DS. Cutaneous ultraviolet exposure and its relationship
to the development of skin cancer. J Am Acad Dermatol 2008;
58:S129-32.
4. English DR, Armstrong BK, Kricker A, Winter MG, Heenan PJ,
Randell PL. Case-control study of sun exposure and squamous
cell carcinoma of the skin. Int J Cancer 1998;77:347-53.
5. van Dam RM, Huang Z, Rimm EB, Weinstock MA, Spiegelman
D, Colditz GA, et al. Risk factors for basal cell carcinoma of the
skin in men: results from the health professionals follow-up
study. Am J Epidemiol 1999;150:459-68.
6. Ortonne JP. Photobiology and genetics of malignant mela-
noma. Br J Dermatol 2002;146:S11-6.
7. Markovic SN, Erickson LA, Rao RD, Weenig RH, Pockaj BA,
Bardia A, et al. Melanoma Study Group of the Mayo Clinic
Cancer Center. Malignant melanoma in the 21st century, part
1: epidemiology, risk factors, screening, prevention, and diag-
nosis. Mayo Clin Proc 2007;82:364-80.
8. American Academy of Dermatology. Melanoma. Available
from: http://www.aad.org/media-resources/stats-and-facts/
conditions/melanoma/melanoma. Accessed December 8,
2011.
9. Kligman LH, Akin FJ, Kligman AM. Sunscreens prevent ultra-
violet photocarcinogenesis. J Am Acad Dermatol 1980;3:30-5.
10. Roberts LK, Beasley DG. Sunscreen lotions prevent ultraviolet
radiation-induced suppression of antitumor immune re-
sponses. Int J Cancer 1997;71:94-102.
11. Sambandan DR, Ratner D. Sunscreens: an overview and
update. J Am Acad Dermatol 2011;64:748-58.
12. Green AC, Williams GM, Logan V, Strutton GM. Reduced
melanoma after regular sunscreen use: randomized trial
follow-up. J Clin Oncol 2011;29:257-63.
13. Sunscreen drug products for over-the-counter human use.
proposed amendment of final monograph proposed rule for
over-the-counter human use. Federal Register 21 CFR Parts
347 and 352. Sunscreen drug products 2007;72:49070-122.
14. COLIPA, CTFA-SA, JCIA, CTFA. COLIPA guidelines; interna-
tional sun protection factor (SPF) test method, 2006. Available
from: http://www.colipa.eu/publications-colipa-the-european-
cosmetic-cosmetics-association/guidelines.html?view=item&id=
21. Accessed December 8, 2011.
15. Bech-Thomsen N, Wulf HC. Sunbathers’ application of sun-
screen is probably inadequate to obtain the sun protection
factor assigned to the preparation. Photodermatol Photo-
immunol Photomed 1992-1993;9:242-4.
16. Azurdia RM, Pagliaro JA, Diffey BL, Rhodes LE. Sunscreen
application by photosensitive patients is inadequate for pro-
tection. Br J Dermatol 1999;140:255-8.
17. Grosick T, Tanner P. Efficacy as used, not as tested, is true
measure of sunscreen performance. J Am Acad Dermatol
2004;50:P31.
18. Lademann J, Schanzer S, Richter H, Pelchrzim RV, Zastrow L,
Golz K, et al. Sunscreen application at the beach. J Cosmet
Dermatol 2004;3:62-8.
19. Wright MA, Wright ST, Wagner RF. Mechanisms of sunscreen
failure. J Am Acad Dermatol 2001;44:781-4.
20. Reich A, Harupa M, Bury M, Chrzaszcz J, Starczewska A.
Application of sunscreen preparations: a need to change the
regulations. Photodermatol Photoimmunol Photomed 2009;
25:242-4.
21. Kim SM, Oh BH, Lee YW, Choe YB, Ahn KJ. The relation
between the amount of sunscreen applied and the sun
protection factor in Asian skin. J Am Acad Dermatol 2010;62:
218-22.
22. Schalka S, dos Reis VM, Cuc�e LC. The influence of the amount
of sunscreen applied and its sun protection factor (SPF):
evaluation of two sunscreens including the same ingredients
at different concentrations. Photodermatol Photoimmunol
Photomed 2009;25:175-80.
23. Bimczok R, Gers-Barlag H, Mundt C, Klette E, Bielfeldt S,
Rudolph T, et al. Influence of applied quantity of sunscreen
products on sun protection factorea multicenter study orga-
nized by the DGK task force sun protection. Skin Pharmacol
Physiol 2007;20:57-64.
24. Revised effectiveness determination; sunscreen drug products
for over-the-counter human use; proposed rule. Federal Reg-
ister 21 CFR Part 201. Revised 2011;76:35672-8.
25. Russak J, Chen T, Appa Y, Rigel DS. A comparison of sunburn
protection of high-sun protection (SPF) sunscreens: SPF 85
sunscreen is significantly more protective than SPF 50. J Am
Acad Dermatol 2010;62:348-9.
26. Labeling and effectiveness testing; sunscreen drug pro-
ducts for over-the-counter human use; final rule. Federal

J AM ACAD DERMATOL
VOLUME 67, NUMBER 6Ou-Yang et al 1227
Register 21 CFR parts 201 and 310. Labeling 2011;76:
35620-65.
27. Fitzpatrick TB. The validity and practicality of sun-reactive skin
types I through VI. Arch Dermatol 1988;124:869-71.
28. Sunscreen drug products for over-the-counter human use;
final monograph. Federal Register 21 CFR parts 310, 352, 700
and 740. Sunscreen 1999;64:27666-93.
29. Herzog B. Understanding sunscreeneinfluence of amount of
application on performance determined by in vivo and in
silico experiments. J Am Acad Dermatol 2007;56:AB40.
30. O’Neil JJ. Effect of film irregularities on sunscreen efficacy.
J Pharm Sci 1984;73:888-91.
31. Diffey B. Has the sun protection factor had its day? BMJ 2000;
320:176-7.

















![Compensating Teams[1]](https://img.pdfslide.us/doc/110x75/577d27c61a28ab4e1ea4cb06/compensating-teams1.jpg)











