Embed Size (px)
Citation preview

REVIEW
High-mobility group box 1 (HMGB1) in childhood: from benchto bedside
Valeria Chirico & Antonio Lacquaniti & Vincenzo Salpietro & Caterina Munafò &
Maria Pia Calabrò & Michele Buemi & Teresa Arrigo & Carmelo Salpietro
Received: 16 January 2014 /Revised: 13 April 2014 /Accepted: 22 April 2014# Springer-Verlag Berlin Heidelberg 2014
Abstract High-mobility group box protein 1 (HMGB1) is anonhistone nuclear protein that has a dual function. Inside thecell, HMGB1 binds DNA, regulating transcription and deter-mining chromosomal architecture. Outside the cell, HMGB1activates the innate system and mediates a wide range ofphysiological and pathological responses. HMGB1 exertsthese actions through differential engagement of multiplesurface receptors, including Toll-like receptor (TLR)2,
TLR4, and receptor for advanced glycation end products(RAGE). HMGB1 is implicated as a late mediator of sepsisand is also involved in inflammatory and autoimmune dis-eases, such as rheumatoid arthritis and systemic lupus erythe-matosus. Interestingly, HMGB1 was associated with tumorprogression, becoming a potential therapeutic target, due to itsinvolvement in the resistance to chemotherapy. Its implicationon the pathogenesis of systemic vasculitis and inflammatorybowel diseases has also been evaluated. Moreover, it regulatesneuroinflammation after traumatic brain injuries or cerebralinfectious diseases. The aim of this review is to analyze thesedifferent roles of HMGB1, both in physiological and patho-logical conditions, discussing clinical and scientific implica-tions in the field of pediatrics. Conclusion: HMGB1 plays akey role in several pediatric diseases, opening new scenariosfor diagnostic biomarkers and therapeutic strategiesdevelopment.
Keywords Autoimmune disease . Cancer . Children .
High-mobility group box 1 (HMGB1) . Neurologicaldiseases . Newborn . Preterm born . Sepsis . Vasculitis
AbbreviationsAA Acute appendicitisAGE Advanced glycation end productsAN Anorexia nervosaANCA Anti-neutrophil cytoplasmic antibodiesCSF Cerebrospinal fluidCSS Churg–Strauss syndromeCRP C-reactive proteinCD Crohn’s diseaseDAMP Damage-associated molecular patternDCs Dendritic cellsHMGB1 High-mobility group box 1KD Kawasaki diseaseJIA Juvenile idiopathic arthritis
Communicated by David Nadal
V. Chirico (*) :V. Salpietro : C. Munafò :M. P. Calabrò :T. Arrigo :C. SalpietroDepartment of Pediatric Sciences, University of Messina,98100 Messina, Italye-mail: [email protected]
V. Salpietroe-mail: [email protected]
C. Munafòe-mail: [email protected]
M. P. Calabròe-mail: [email protected]
T. Arrigoe-mail: [email protected]
C. Salpietroe-mail: [email protected]
A. Lacquaniti :M. BuemiDepartment of Internal Medicine, University of Messina, Messina,Italy
A. Lacquanitie-mail: [email protected]
M. Buemie-mail: [email protected]
A. LacquanitiDepartment of Internal Medicine, Mediterranean Institute forTransplantation and Advanced Specialized Therapies, ISMETT,Palermo, Italy
Eur J PediatrDOI 10.1007/s00431-014-2327-1

IC Immune complexesIBD Inflammatory bowel diseasesIFN InterferonIL InterleukinMPA Microscopic polyangiitisMAPK Mitogen-activated protein kinasesNEC Necrotizing enterocolitisNOD Nonobese diabeticNF-κB Nuclear factor-kappa Bp-ANCAs Perinuclear anti-neutrophil
cytoplasmic antibodiesRAGE Receptor for advanced glycation end productsRA Rheumatoid arthritisSLE Systemic lupus erythematosusTIM-3 T cell immunoglobulin and mucin domain-3TLR Toll-like receptorTBI Traumatic brain injuryTGF Tumor growth factorTNF Tumor necrosis factorT1D Type 1 diabetesUC Ulcerative colitisWG Wegener granulomatosis
Introduction
High-mobility group box 1 (HMGB1) is one of the mostimportant damage-associated molecular pattern (DAMP) mol-ecules, initiating and perpetuating immune response in non-infectious inflammatory responses [27]. Its role, in fact, is toact as a “danger signal”, orchestrating a homeostatic defensiveresponse in challenged tissues [46].
The recent discovery of HMGB1, as a critical mediator ofinflammation, stimulated an increasing interest in inflamma-tion research field [8]. The study of this molecule may lead tothe identification of a new diagnostic biomarker for variousdiseases, having the inflammatory process as background.Furthermore, HMGB1 could open important scenarios fornovel therapeutic strategies [77]. The aim of this review is toanalyze the role of HMGB1, reporting its physiological func-tions, its receptor interactions, and its role in pathologicalfield. In particular, pediatric diseases and data obtained fromanimal models having important clinical and scientific impli-cations in the field of pediatrics, were discussed.
Physiological role of HMGB1
HMGB1 structure
HMGB1 was first described almost 30 years ago as a nonhis-tone chromosomal protein with high electrophoretic mobility
[49]. HMGB is a family of three nuclear proteins includingHMGB1 (previously named amphoterin or HMG1), HMGB2,and HMGB3 [14, 24]. HMGB1 is a single polypeptide chainof 215-amino-acid length that contains two positively chargeddomains referred as “HMG boxes A and B” [90]. The highlyconserved N and C terminal regions of the protein areenriched with basic and acidic amino acid residues,respectively [109, 119].
The functional role of HMGB1 depends upon its location.When inside the nucleus, HMGB1 acts as an architecturalprotein that binds DNA, whereas it exerts different roles andfunctions, once outside the cell, as a proinflammatorycytokine.
Apart from its localization, structural modifications, suchas acetylation or phosphorylation, can determine differentfunctions of HMGB1 [105].
Nuclear HMGB1 actions
HMGB1 is constitutively expressed in many cell types, and alarge “pool” of preformed HMGB1 is stored in the nucleus[16, 31]. “A” and “B” HMG boxes enable HMGB1 to bindchromosomal DNA and fulfill its nuclear functions, includingnucleosomal structure and stability, and regulation of geneexpression [25]. HMGB1 is also active in DNA recombina-tion, repair, and replication [24].
HMGB1 interacts with a wide range of proteins, such astranscriptional factors [80], steroid hormone receptors [18], ma-trix metalloproteinases 2 and 9 [100], viral components [37], andseveral components of the plasminogen activation system [87].
Cytosolic HMGB1 actions
HMGB1 acts as a cell-membrane form, promoting neuriteoutgrowth, smooth muscle cell chemotaxis, and tumor cellmetastasis [89]. Cytosolic HMGB1 promotes autophagy, aconserved programmed survival pathway induced by environ-mental and intracellular stress [103].
Moreover, it represents an important biosensor of nucleicacid inside the cells. DNA or RNA derived from viruses,bacteria, or damaged cells trigger innate immune responsesthrough HMGB1, which is required for subsequent recogni-tion by specific pattern receptors [63].
Extracellular HMGB1 actions
Macrophages, monocytes, dendritic cells (DCs), and T cellsactively release HMGB1 after stimulation with exogenousbacterial products such as endotoxin, or with endogenousproinflammatory cytokines, as well as tumor necrosis factor(TNF)-α, interleukin (IL)-1β, and interferon (IFN)-γ.
As an extracellular protein, HMGB1 exerts autocrine andparacrine effects including activation of nuclear factor-kappa
Eur J Pediatr

B (NF-κB), diffuse endothelial activation, systemic activationof inflammatory cells, stimulation of cell migration, facilita-tion of innate recognition of microbial products, and activa-tion of innate immune cells [71]. Moreover, HMGB1 also actson progenitor cells and may play a role in regeneration andrepair of injured tissue [85].
Bactericidal activity represents another property ofHMGB1, able to eradicate in culture more than 95 % ofbacteria within 5 min [123].
Simultaneously, the A box competes with full-lengthHMGB1 for binding sites, leading to an attenuation of theinflammatory cascade. This self-limiting action could repre-sent a negative feed-back for proinflammatory processes[116]. Table 1 summarizes the functions of HMGB1.
HMGB1 receptors
The receptor for advanced glycation end products (RAGE) andsome members of the Toll-like receptor (TLR) family, such asTLR2 and TLR4, have been involved in HMGB1 signaling [15].
After release, HMGB1 binds RAGE, activating of NF-κBand mitogen-activated protein kinases (MAPK) and, conse-quentially, several proinflammatory genes [98].
RAGE alone, however, cannot explain all observed effectsof HMGB1, suggesting the existence of additional receptorsrelevant to HMGB1 signaling.
TLR2 and TLR4 may mediate HMGB1 effects, includingchemotactic cell movement and release of proinflammatorycytokines [7, 86, 121]. HMGB1 acts also by TLR9 signaling,presenting several ligands, such as ssDNA or branched RNAstructures, to its receptor [104].
HMGB1may also suppress proinflammatory cytokine releaseinduced by HMGB1-TLR4 signaling, binding, and signalingthrough a bimolecular cell surface receptor complex formed byCD24 and Siglec-10 (in humans) or Siglec-G (in mice) [32].
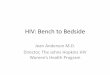
T cell immunoglobulin and mucin domain-3 (TIM-3) antag-onize HMGB1 receptor, suppressing innate immune responsesthrough the inhibition of the recruitment of nucleic acids bycytosolic sensors, such as HMGB1, via a galectin-9-independent mechanism [33]. Moreover, thrombomodulin, anendothelial thrombin-binding anticoagulant cofactor, bindsHMGB1 and sequesters HMGB1 from TLRs and other recep-tors. This binding mediates proteolytic cleavage of HMGB1 bythrombin [58]. Figure 1 better explains all these interactions.
HMGB1 in childhood pathology
Sepsis
Sepsis is one of the common causes of morbidity and mortal-ity in children [111]. Early recognition and prompt initiation
of therapy are the most important measures in reducing mor-tality, but a timely diagnosis remains difficult [76].
In contrast to early inflammatory mediators, such asTNF-α and IL-1β, HMGB1 is a late mediator of sepsis [1].Pavare et al. analyzed HMGB1 in children at different age andwith different grades of infections, underlying its low diag-nostic power to detect the bacteremia [88].
Several markers were studied by Carrol et al. to diagnosebacterial infection in Malawian children, highlighting thatprocalcitonin identifies severe sepsis better, when comparedwith other biomarkers such as C-reactive protein (CRP) orHMGB1 [28].
Therefore, no exciting data about the role of HMGB1 inpediatric sepsis were obtained in these studies, but later stagesof disease, in which HMGB1 could play a more importantrole, were not assessed. In fact, HMGB1 is secreted by mac-rophages 20 hin vitro after activation with endotoxin andin vivo 20–72 h after the onset of infection [75].
HMGB1 should be evaluated as a late prognostic factor orused as a marker of response to therapy, rather than an earlymarker of sepsis. Kato et al. demonstrated that edaravone, anovel free-radical scavenger, prolonged survival in a neonatalanimal model of sepsis, preventing HMGB1 elevation [65].
Studies of sepsis have been conducted principally on ani-mal models and adult humans, with few data about pediatricpopulation and further studies are necessary to assign a role toHMGB1.
Inflammatory bowel disease
Necrotizing enterocolitis
Necrotizing enterocolitis (NEC) is the most frequent andlethal disease affecting gastrointestinal tract of premature in-fant [45]. Although numerous risk factors including prematu-rity, hypoxia, bacterial infection, and intestinal ischemia havebeen implicated in the pathogenesis of NEC, the etiology isunclear but multifactorial [114].
Numerous inflammatory mediators have been involved inthe pathogenesis of NEC, such as fecal calpoprotectin, IL-6,TNF-α, or tumor growth factor (TGF)-β [120].
Zamora et al. examined HMGB1 in newborn rats withexperimental NEC and in inflamed intestine of human infantswith acute NEC, demonstrating its role as a mediator ofhypoxia-induced gut injury. Furthermore, the suppression ofHMGB1 with inhibitors, such as semapimod, a drug withimmunomodulatory and anti-inflammatory properties, partial-ly protected against intestinal epithelial cell death [122].
Crohn’s disease and ulcerative colitis
Crohn’s disease (CD), largely arising from a Th1 response,and ulcerative colitis (UC), mainly mediated by T cells or
Eur J Pediatr

natural killer T cells, are the most important inflammatorybowel diseases (IBD) [19]. Vitali et al. demonstrated increasedHMGB1 protein levels in the stools of patients with IBD,hypothesizing an active secretion of the protein stored in thenucleus rather than a "de novo" synthesis. In addition, highHMGB1 was also revealed in patients with inactive disease,suggesting that it might be a sensitive marker of mucosalinflammation, although the disease was clinically inactive[108].
Acute appendicitis
Acute appendicitis (AA) represents a common pediatric abdom-inal surgical emergency, with high rates, around 10–30 %, ofnegative appendectomy and perforated appendicitis [12].
Diagnostic traditional methods are rather nonspecific, and itis still controversial if the use of imaging applications signifi-cantly reduces these complications [50]. Therefore, the identi-fication of novel markers of AA is clinically highly desirable.
HMGB1 was assessed in AA patients, evaluating mRNAand protein levels. In particular, Albayrak et al. demonstratedthat HMGB1 levels were high in AA patients, also in thosewith normal white blood cell counts [5]. This observation wasalso confirmed by Wu et al. who demonstrated that HMGB1,in acute simple, acute suppurative and acute gangrenous ap-pendicitis groups, were significantly high and positively cor-related with the severity of the disease [115].
These data confirm that HMGB1 plays a crucial role in thepathophysiological process of inflammatory bowel diseases,but further studies are necessary to constitute HMGB1 as aclinical biomarker.
The main data about the role of HMGB1 in inflammatoryand infectious diseases are summarized in Table 2.
Autoimmune disease
HMGB1 has been implicated in the pathogenesis of a broadspectrum of autoimmune disease, identified as an auto-antigenrecognized by perinuclear anti-neutrophil cytoplasmic anti-bodies (p-ANCAs) [26].
Table 3 reports main pediatric diseases in which a physio-pathological role of HMGB1 has been demonstrated, under-lying possible mechanisms and future clinical prospects.
Type 1 diabetes
Autoimmune response during type 1 diabetes (T1D) develop-ment is a multifactorial and complex process that requiresgenetic predisposition to synergize with unknown exogenousand/or endogenous triggers. Once triggered by those factors,early stages are characterized by insulitis and infiltration of thepancreatic islets by DCs, macrophages, and T cells [29].
Han et al. demonstrated that HMGB1, actively secreted byDCs, contributed to insulitis progression and diabetes in
Table 1 Physiological functions of HMGB1 based on its localization
Localization Functions References
Membrane Neurites growth Raucci et al. [89]
Smooth muscle cell chemotaxis Raucci et al. [89]
Tumor cell metastasis Raucci et al. [89]
Nuclear Stabilize nucleosome structure Bustin et al. [25]
Gene transcription Bustin et al. [25]
DNA repair/replication Bustin et al. [24]
Interaction with transcriptional factors Nishitani et al. [80]
Interaction with steroid hormone receptors Boonyaratanakornkit et al. [18]
Interaction with matrix metalloproteinase Taguchi et al. [100]
Interaction with viral components Costello et al. [37]
Extracellular Dendritic cell stimulation Campana et al. [27]
Th1 polarization Messmer [74]
B cell activation/proliferation Avalos [11]
Activation of immune cells with induction of proinflammatory cytokine production Lotze et al. [71]
Regeneration and repair of injured tissue Palumbo et al. [85]
Bactericidal effects Zetterstrom et al. [123]
Osteoclast formation Sakai [93]
Negative inotropic effects on cardiomyocytes Hagiwara [51]
Chemotaxis/differentiation on stem cells Chavakis [30]
HMGB1 high-mobility group box 1
Eur J Pediatr

nonobese diabetic (NOD) mice. Moreover, HMGB1 signaledvia TLR4, the main receptor on β cells, to selectively damageβ cells during the development of T1D [69].
Pediatric T1D patients have high circulating levels ofHMGB1, which could trigger TLR2 and TLR4 activationand leading to a proinflammatory state [38].
The challenge for future studies would be the developmentof HMGB1 blockade drugs to evaluate the natural history ofT1D and its complications.
Systemic lupus erythematosus
Systemic lupus erythematosus (SLE) is a complex, chronicmultisystem autoimmune inflammatory disease [66]. Up to
20 % of cases are diagnosed during childhood with a lessfavorable prognosis [21]. Environmental triggers, such asinfectious agents, operate in the context of both susceptibilitygenes and epigenetic modifications, resulting in alterations inantigen presentation, lymphoid signaling, apoptosis, andantigen/immune complexes (IC) clearance [48].
HMGB1 is significantly elevated in lupus sera and hasbeen regarded as one of the components in DNA-containingIC that enhances cytokine production through TLR9 orRAGE ligation [70, 104].
These observations derived from adult studies, whereasthere are no data about HMGB1 in children with SLE, exceptGarcia-Romo’s evaluation of neutrophil proteins, includingHMGB1, in pediatric SLE patients [47].
Fig. 1 Release modalities, receptors, pathways, and actions of HMGB1.The full-length HMGB1 contains two homogenous domains (boxes Aand B) and an acidic C-terminal tail. HMGB1 is actively secreted byinnate immune cells in response to exogenous bacterial products (e.g.,endotoxin or CpG-DNA) or endogenous inflammatory stimuli (e.g., TNFand IFN-γ) and passively released by damaged or virus-infected cells.HMGB1 initiates cellular responses by interacting with several differentcell surface receptors. HMGB1 can associate with LPS and activateTLR4, or, when associated with the nucleosome, released during second-ary necrosis, TLR2 is preferentially engaged. HMGB1 also bind to IL-1βand signal through the IL-1R. HMGB1 can bind to DNA and RNA andsignal through RAGE. Engagement of these receptors results in receptor-dependent signaling via the MyD88-dependent pathway involvingNF-κB activation. Activated NF-κB migrates to the nucleus, where itdirectly upregulates the transcriptions of proinflammatory products,
including HMGB1. HMGB1 binds CpG-DNAs, ssRNAs, and dsRNAspromoting their recognition. These complex are endocytosed intoendosomal compartments where they engage the intracellular TLR9,TLR7, and TLR3 resulting in MyD88 and TRIF recruitment and thesubsequent immune response via NF-κB. TIM-3 and CD24/Siglec-10represent two inhibitory HMGB1 receptors. TIM-3, binding HMGB1,inhibits the recruitment of nucleic acids into endosomes and subsequentnucleic acid-mediated immune responses. The complex HMGB1-CD24/Siglec-10 determines a suppression of proinflammatory cytokine release.Abbreviations: HMGB1 high-mobility group protein B1, RAGE receptorfor advanced glycation end products, TLR toll-like receptor, IL interleu-kin, LPS lipopolysaccharide, MyD88 myeloid differentiation primaryresponse gene 88, TRIF TIR-domain-containing adapter-inducinginterferon-β, NF-kB nuclear factor-kappa B, TIM-3T cell immunoglobu-lin and mucin domain-3
Eur J Pediatr

Furthermore, recently it has been demonstrated thatHMGB1, significantly increased in juvenile SLE pa-tients with or without active nephritis, was positivelycorrelated with the disease activity, sustaining the in-flammatory action of interferon-α [62].
Studies assessing HMGB1, anti-HMGB1 and their com-plexes in the pathogenesis of SLE are needed in childhoodpopulation, to further elucidate the role of this novel inflam-matory protein. Therapeutic targeting of HMGB1 might opennew therapeutic opportunities.
Rheumatoid arthritis
HMGB1 is clearly involved in the pathogenesis of rheumatoidarthritis (RA), enhancing the expression of cytokines andother proinflammatory factors [68].
Juvenile idiopathic arthritis (JIA) is a group of chronicchildhood arthritides of unknown origin. While there areseveral observations that confirm the role of HMGB1 in adultarthritis, few studies are conducted in children, in which it wasdemonstrated that patients with JIA were characterized byantibodies direct against HMGB1 or HMGB-2 [92, 113].
It is plausible that HMGB1-binding antibodies might serveas a limiting overwhelming cytokine release, after tissue
damage. Furthermore, high levels of HMGB1 in inflamedjoints were demonstrated in children with JIA, with thehighest levels assessed in patients with a disease onset in earlyage (before age 10) [95].
These data confirm that HMGB1 represents a mediator ofinflammatory arthritis and may serve as a potential therapeutictarget. Further studies should be conducted in children withJIA to confirm the role of HMGB1 and to evaluate if phar-macological interference with this pathway can be an excel-lent strategy for pediatric arthritis.
Vasculitis
Kawasaki disease
Kawasaki disease (KD) is an acute, self-limited vasculitis,with potential cardiovascular complications, developing in∼15 to 25 % of untreated children [79].
Hoshina et al. measured HMGB1 levels in 27 childrenaffected by KD, demonstrating higher HMGB1 values thanhealthy controls. Furthermore, the highest values were detectedin early acute phase with a gradually decrement after deferves-cence [55]. In addition, analyzing KD patients after intravenousimmunoglobulin treatment, Eguchi et al. demonstrated that
Table 2 HMGB1 role in inflammatory and infective diseases
Disease HMGB1 Mechanisms Pediatric data (reference) Future prospects
Sepsis Serum ↑or→
Innate immune cells actively release HMGB1which can be released passively fromdamaged cells or cells infected by viruses.HMGB1 triggers an inflammatoryresponse
2 studies; Pavare [88] andCarrol [28] studied childrenwith different grades ofinfections, including sepsis
Late prognostic factor
Marker of therapy response
HMGB1 inhibition as therapy
IBD Stoolsand H↑↑
Intracellular localization of HMGB1with its active secretion storedin the nucleus rather than a"de novo" synthesis
1 study; Vitali [108] analyzedthe stools and bioptic tissuesof 19 children with CDand 21 with UC
Early fecal diagnostic marker
Marker of mucosal inflammation
Marker of therapy response
NEC H ↑↑ Over expression of HMGB1 andRAGE is related to the enterocyteapoptosis/necrosis cell death andhypoxia-induced gut barrier failureassociated with NEC
1 study; Zamora [122] studiedbiopsies in 7 infants andin newborn rats
HMGB1 inhibition as therapy
AA Serumand H↑↑
Bacteria invade and infect the wallof the appendix, causing releasingof bacterial endotoxin andproinflammatory cytokines, which activatemonocytes/macrophages to release HMGB1. HMGB1is also passively released from injuredor necrotic cells
2 studies; few adolescentswere enrolled with adultsin these studies [5, 108]
Diagnostic marker of appendicitis
Newborn infectionPRM,hypoxemia
AMF andUCB↑↑
In response to inflammatory or infectivestimuli, HMGB1 is secreted by fetalimmune cells, which triggerinflammatory responses
6 studies; HMGB1 wasevaluated in several newborndiseases [2, 23, 39, 77, 82, 94]
Diagnostic marker of inflammatoryor infective diseases in newborns
HMGB1 high-mobility group box 1,H histological data, CSF cerebrospinal fluid, IBD inflammatory bowel disease, CD Cronh’s disease,UC ulcerativecolitis,NEC necrotizing enterocolitis, AA acute appendicitis, AMF amniotic fluid,UCB umbilical cord blood,PRM prolonged rupture of the membranes,TLR toll-like receptor
Eur J Pediatr

poor-responder group was characterized by high HMGB1,representing a potential marker of therapy resistance [40].
Anti-neutrophilic cytoplasmatic antibodies–associatedvasculitis
The primary small-vessel systemic vasculitic disorders asso-ciated with anti-neutrophic cytoplasmic antibodies (ANCA)
include Wegener granulomatosis (WG), microscopic polyan-giitis (MPA), and Churg–Strauss syndrome (CSS) [60].
CSS is a vasculitis with a propensity for lung involvement,accompanied by asthma and an eosinophil-rich inflammatoryinfiltrate with granuloma formation [81, 125]. It is generallyconsidered a disease of adults, and its occurrence in childrenhas been reported infrequently [20].
Taira et al. revealed an involvement of HMGB1 in the path-ogenesis of CSSwith HMGB1 levels strictly related with ANCA
Table 3 HMGB1 involvement in autoimmune disorders and vasculitis
Disease HMGB1 Mechanisms Pediatric data (reference) Future prospects
T1D Serum ↑ Dendritic cells contributesto insulitis progression,secreting HMGB1 that,signaling via TLR4,selectively damages β cells
1 study; Devaraj [38]evaluated HMGB1levels in pediatric patients
HMGB1inhibitionas therapy
SLE Serum and H ↑↑ HMGB1 enhances cytokineproduction through TLR9or RAGE ligation. It is alsoinvolved in the abnormalhyperactivation of JAK-STAT1signaling pathway. HMGB1sustains the inflammatoryaction of interferon-α
2 studies; 1 in vitro studyconducted on neutrophilsisolated from the blood ofpediatric SLE patients [47] and1 in vivo study in juvenileSLE patients [62]
Therapeutictargeting ofHMGB1pathway
JIA Serum and SF ↑↑ Innate immune cells activelyrelease HMGB1 which canbe released passively fromdamaged cells or cells infectedby viruses. HMGB1 triggersan inflammatory response
2 studies; antibodies directagainst HMGB1 weredetected in ANA positivechildren. High HMGB1were recorded in synovialfluid [92, 115]
Diagnosticmarker of JIA
HMGB1inhibition astherapy
Vasculitis
KD Serum and H activephase (↑) andremission phase(↓)
HMGB1 is actively secretedby immune cells and passivelyreleased by injured and necroticcells. HMGB1 serum levelsreflect remaining low-gradeinflammatory activity ortissue damage
2 studies; different levelsof HMGB1 in acute orchronic vasculitis [38],before and after treatment [52]
Marker ofinflammationin vasculitisdisease
HMGB1inhibitionas therapy
Marker oftherapyresponse
ANCA-associated VASCULITIS
CSS Serum and H ↑ HMGB1 is a eosinophilchemotaxis inductor.Eosinophil are able torelease HMGB1
1 study; Taira [95] demonstratedthat eosinophils stainedpositive for HMGB1 positivelycorrelated with peripheraleosinophil counts
Diagnosticmarkerof CSS
WS Serum and H activephase (↑) andremission phase(↓)
HMGB1 is passively released bynecrotic and apoptotic cells.Furthermore, its high levels,especially during the active phase,are also due to immune cell activeproduction
2 studies; HMGB1 levels wereelevated in active Wegenercases [106] and WG withpredominant granulomatousmanifestations [51]
Diagnosticmarkerof WS
Prognosticmarker
HMGB1 high-mobility group box 1, T1D type 1 diabetes, TLR toll-like receptor, SLE systemic lupus erythematosus,H histological data,RAGE advancedglycation end products, JIA juvenile idiopathic arthritis, SF synovial fluid, IF immunofluorescence, ANA antinuclear antibodies,MGmyasthenia gravis,HSP Henoch–Schönlein purpura, BD Behcet’s disease, KD Kawasaki disease, CSS Churg–Strauss syndrome, WS Wegener’s syndrome, ANCA anti-neutrophilic cytoplasmatic antibodies
Eur J Pediatr

antibodies and higher values than those observed in asthmaticpatients.Moreover, eosinophils stained positive for HMGB1, oneof themost important eosinophil chemotaxis inductor, which wasalso positively correlated with peripheral eosinophil counts [101].
WG typically occurs in early adolescence, and glomerulone-phritis and pulmonary disease are common at the diagnosis [4].
Wibisono et al. reported increased serum HMGB1 levelsonly in active WG, suggesting that HMGB1 could vary withthe amount of necrotic tissue [112].
These data were confirmed by Henes et al. who demon-strated that HMGB1 serum levels were significantly high inWG with predominant granulomatous manifestations, corre-lating with the volumes of pulmonary “granuloma” [54].
HMGB1 may be used as a marker of inflammation invasculitis disease, but further studies are necessary to betterunderstand its physiopathological functions and to confirm itsdiagnostic and prognostic role. Furthermore, if HMGB1 isproven to be an inflammatory mediator in vasculitis (in par-ticular, if anti-HMGB1 antibodies will diminish the diseaseactivity in ANCA-associated vasculitis models), reducingHMGB1 expression may be an interesting new drug target.
Cancer
The involvement of HMGB1 in cancer is complex, with itsimplication in tumor formation, progression and in the re-sponse to chemotherapeutics [41] (Fig. 2).
Expression of HMGB1 is upregulated in nearly everytumor type and involved in the regulation of invasive tumorcell migration [44].
Autophagy has recently attracted increasing attention for itsrole in conferring resistance to various commonly used anti-cancer therapies [59].
The balance between apoptosis ("programmed cell death")and autophagy ("programmed cell survival") is important intumor development and response to therapy. HMGB1 and p53form a complex that regulates the balance between tumor celldeath and survival, with a pivotal role of HMGB1 in autoph-agy regulation [56].
Anticancer agents, including doxorubicin, cisplatin, andmeth-otrexate, induce HMGB1 upregulation in human osteosarcomacells, determining an increased drug resistance mediated byautophagy. Therefore, HMGB1 represents a critical factor forthe development of chemoresistance, as a regulator of autophagy,offering a novel target for improving osteosarcoma therapy [57].
In addition, Yang et al. found that HMGB1 was expressedabundantly in various kinds of both leukemia and nonbloodcancer cell lines, and its expression was positively correlatedwith clinical status in childhood leukemia. In leukemia cells,autophagy was induced by HMGB1, enhancing leukemia cellchemoresistance [117].
Another implication of HMGB1 in childhood oncologywas provided by Kang et al. who explored the clinical
significance of HMGB1alterations in acute lymphocytic leu-kemia, one of the most common malignancies in childhood,demonstrating its prognostic role [64].
Further studies are needed to verify if HMGB1 blockagecan be used to improve cancer treatments.
Neurological diseases
Autistic disorders
Autism is a neurodevelopmental disability characterized byimpairments in verbal communications, reciprocal social in-teractions, and restricted repetitive stereotyped behaviors [84].
Dysregulated immune function is a recurrent finding, includ-ing evidence of brain reactive antibodies, altered cytokine levelsin the brain, and altered function of innate immune cells [96].
HMGB1 receptors are involved in the pathophysiologicalmechanisms of autism. Enstrom et al. described abnormal sen-sitivity of peripheral blood monocytes, isolated from childrenwith and without autism, to TLR ligands, suggesting a dysfunc-tion in monocyte pathogen recognition and/or TLR signalingpathways [43]. Junaid et al. showed high incidence of A-allelehomozygosis in theGLO1 gene, with reduction in Glo1 activity[61]. This condition determines an accumulation in the brain ofmethylglyoxal, leading to the formation of advanced glycosyl-ated end products (AGE), which ultimately induces the RAGE-mediated downstream signaling cascade [13]. Autistic childrenare also characterized by abnormal serum levels of HMGB1when compared with healthy controls [42].
High serum levels of HMGB1 may be a biomarker of theimpai red rec ip roca l soc ia l in te rac t ions in th i sneurodevelopmental disorder.
Anorexia nervosa
Anorexia nervosa (AN) is a serious disorder affecting adoles-cents and young adults, decreasing quality of life over longperiod [97]. Several findings from clinical and animal studiesindicate that proinflammatory cytokines are involved in path-ophysiological mechanisms of eating disorders [36].
Agnello et al. demonstrated that administration of HMGB1into cerebral ventricles in rats reduces food intake; whereas, ina model of endotoxemia, passive immunization with anti-HMGB1 antibodies attenuated the development ofhypophagia [3]. In addition, HMGB1 was evaluated in pa-tients with AN at baseline and after nutritional rehabilitationand cognitive behavior therapy, with high HMGB1 valuesobserved in AN patients who did not respond to therapy [118].
Further studies with a larger sample size are needed toinvestigate the relationship between serum HMGB1 and path-ogenic mechanisms of anorexia.
Eur J Pediatr

Traumatic brain injury
Traumatic brain injury (TBI) is a leading cause of morbidityand mortality in children [14].
HMGB1 in part reflects the degree of necrosis and apopto-sis present after TBI, contributing to cell death and neurolog-ical morbidity [99].
Anti-HMGB1 monoclonal antibodies may provide a noveland effective therapy for TBI by protecting against blood–brainbarrier disruption and reducing the inflammatory responses in-duced by HMGB1 [83]. Moreover, adult observations highlight-ed that HMGB1 levels and Glasgow Coma Scale score providedsimilar prognostic information, in patients with severe TBI [110].
Only one pediatric study was performed to evaluateHMGB1 levels in ventricular cerebrospinal fluid (CSF) afterTBI, demonstrating that increased CSF levels of HMGB1were associated with poor outcome [10].
Targeting HMGB1 signaling may be a promising therapeu-tic approach for the treatment of TBI in pediatric and adultpopulation, but further studies are needed to better understandthe physiopathological role of this molecule in TBI.
Neurological infectious disease
Inflammation plays an important role in the neuropathologicalchanges induced by bacterial meningitis [17]. Moreover,
Fig. 2 Different roles of HMGB1 in the tumor microenvironment. Stim-ulated secretion of HMGB1 from tumor cells and passive release bynecrotic, dying tumor cells into the extracellular milieu has both pro-and anti-tumorigenic effects. The anti-tumorigenic effects are as follows:(1) Acute release of HMGB1 after antitumor treatments stimulates mat-uration of DCs through interactionwith TLR4 and RAGE. Activated DCsdetermine a clonal expansion of tumor antigen-specific T cells withimmune antitumor responses. (2) HMGB1 enhances chemotaxis andpromotes migration of monocytes, DCs, and Tcells. The pro-tumorigeniceffects are as follows: (1) Angiogenesis—persistent hypoxia in growingtumors leads to necrosis and apoptosis, causing a chronic release ofHMGB1, which activates protumor responses promoting angiogenesisand tumor growth through the recruitment of endothelial precursor cells(EPCs) and activation of local endothelial cells through RAGE signaling.Furthermore, activated macrophages synthetizes pro-angiogenetic fac-tors, such as VEGF. (2) Autophagy induction—during low oxygen,
HIF-1α initiates TLR4 transcription, which can then be engaged byHMGB1. The engagement of TLR4 results in signaling through adaptormolecules MyD88 and TRIF which both inhibit the interaction of Bcl-2with Beclin 1. Cytosolic HMGB1 disrupts the interaction betweenBeclin1 and Bcl-2 by competitively binding to Beclin1, inducing autoph-agy. HMGB1 induces autophagy by its direct binding to the RAGE andactivating ROS and NF-kB pathways. Autophagy improves the tumorgrowth inducing chemotherapy resistance, inhibiting apoptosis, and en-hancing cell survival. Abbreviations: HMGB1 high-mobility group pro-tein B1, RAGE receptor for advanced glycation end products, TLR toll-like receptor, IL interleukin, TNF tumor necrosis factor, EPCs endothelialprogenitor cells, VEGF vascular endothelial growth factor,HIF1 hypoxiainducible factor-1,MyD88myeloid differentiation primary response gene88, TRIF TIR-domain-containing adapter-inducing interferon-β, Bcl-2 Bcell lymphoma 2, ROS reactive oxygen species, NF-kB nuclear factor-kappa B
Eur J Pediatr

tissue damage secondary to meningeal inflammation is in-duced by TLR signalling activation [53, 67, 94].
Several studies demonstrated a pivotal role of HMGB1 inmeningitis. In particular, CSF levels of HMGB1were elevatedin children with bacterial and aseptic meningitis, with thehighest values revealed in bacterial infection. Furthermore, asignificant correlation between white blood cell counts, glu-cose levels, and HMGB1 was underlined, confirming a diag-nostic role of this protein in meningitis [102].
These observations were confirmed by Asano et al., whoanalyzed HMGB1 in different infectious neurological disease.A marked elevation of HMGB1was seen only in bacterial andaseptic meningitis, concluding that HMGB1 was a poor dis-ease marker for acute encephalopathy [9]. In addition, Allevaet al. revealed a pathogenetic role of HMGB1 in childrenshowing cerebral symptoms as a consequence of severefalciparum malaria. Malarial patients were characterized byhigher HMGB1 levels than controls, and strictly related withpatient’s survival [6].
However, further studies about HMGB1 and its receptorare needed to reveal its exact role in pediatric meningitis.
Epilepsy
Febrile seizures are themost common form of childhood seizures[52]. Experimental studies provide evidence that induction ofspecific proinflammatory pathways in forebrain mediatesproconvulsive effects, and their pharmacological modulation rep-resents a potential strategy to reduce seizure activity [106, 107].
In particular, recent data, obtained from different experi-mental models of acute and chronic seizures, identified thecrucial role played by the activation of HMGB1-TLR4 sig-naling in the hippocampus in the generation and recurrence ofseizures [73]. Choi et al. demonstrated that active inflamma-tion, including HMGB1 and proinflammatory cytokines, oc-curred in children with febrile seizures and pediatric epilepsy[34]. Zurolo et al. evaluated the role of HMGB1-TLR4 axis inpediatric, adolescent, and adult patients who underwent
Table 4 Neurological diseases and HMGB1 involvement
Disease HMGB1 Mechanisms Pediatric data (reference) Future prospects
Autism Serum ↑ Dysregulated immune functionis a recurrent finding in autisticchildren. In addition, the TLRand RAGE signaling pathwaysare altered with a dysfunctionin monocyte pathogen recognition
4 studies; atudies [13, 43, 61]investigated TLR and RAGEpathway dysfunction in children.HMGB1 levels were assessed inautistic children [42]
Diagnostic marker of autism
AN Serum→or ↑
Proinflammatory cytokines playroles in AN. administration ofHMGB1 into the cerebral ventriclesin rats decreases food intake, whilea passive immunization withanti-HMGB1 antibodies attenuatedthe development of hypophagia
No evidence in children. Only 1study evaluated HMGB1 in youngadults affected by AN. It analyzed basalHMGB1 values and after treatment [118]
Diagnostic marker of AN
Marker of therapy resistance
TBI Serumand H↑
HMGB1 in part reflect the degreeof necrosis and apoptosis presentafter TBI. RAGE and HMGB1expression increased in microgliain the region surrounding thecontused area
1 study; HMGB1 was evaluated in CSFof children with TBI, highlighting itsprognostic role [10]
HMGB1 inhibition as therapy
Prognostic marker
Meningitis CSF ↑↑ HMGB1, massively released intothe cerebrospinal fluid, acts as aninflammatory cytokine throughTLR pathway, mediating meningealinflammation. MeningococcalCpG-DNA-HMGB1 enters inthe cells by endocytosis and thenbinds to TLR9, inducing activation ofinflammatory cytokines
4 studies; in pediatric populations,the physiopathological role ofHMGB1 has been studied inmeningitis and other neurologicalinfectious diseases
Diagnostic marker of meningitisbut not for acute enchephalothy
Prognostic marker
Marker of therapy response
Epilepsy Serumand H↑
Active neuroinflammation and markedcellular injury occur in pediatricepilepsy.The activation of HMGB1-TLR-RAGEsignaling plays a pivotal role in thegeneration and recurrence of seizures
2 studies; children with epilepsypresented an active inflammationstate and high HMGB1 levels [34].Histologically, it assessed anoverexpression of HMGB1 and itsreceptors in cerebral bioptic tissue [124]
HMGB1 inhibition as therapy
Prognostic marker
HMGB1 high-mobility group box 1, TLR toll-like receptor, H histological data, RAGE advanced glycation end products, AN anorexia nervosa, TBItraumatic brain injury, CSF cerebrospinal fluid
Eur J Pediatr

therapeutic surgical resection for refractory epilepsy, demon-strating an intralesional overexpression of HMGB1, TLR2,TLR4, and RAGE [124].
A pharmacological modulation of HMGB1-TLR/RAGEaxis with receptor antagonists or inactivating antibodies mayrepresent a potential novel antiepileptic strategy.
All information concerning HMGB1 involvement in pedi-atric neurological disorders has been reported in Table 4.
Prematurity born
The poor outcome observed in many preterm children is notentirely dependent on their gestational age at birth, but severalrisk factors are significantly associated with an increased riskof cerebral palsy, such as hypoxia, intra-amniotic infection,and inflammation [23].
It is well known that the host’s response to microbial path-ogens involves a series of carefully orchestrated mechanisms,including DAMP peptides, such as HMGB1, and their receptorpathways. A significant change in expression of RAGE andHMGB1 was demonstrated in the setting of inflammation-induced preterm birth, indicating that these peptides may beimportant mediators of cellular injury in fetus delivered [22].
Moreover, Romero et al. demonstrated high amniotic fluidHMGB1 concentrations in newborn with intra-amniotic infec-tion and preterm prelabor rupture of membranes [39, 91].HMGB1 levels were also high in infants born before 32 weeksof gestation and requiring mechanical ventilation, with a strictlycorrelation with the development of bronchopulmonary dyspla-sia or death [2]. HMGB1 was also investigated in neonates,with higher levels in unscheduled than scheduled caesariandelivery and associated with ischemic reperfusion injury [78].
Moreover, in neonates with asphyxia, it has been suggestedthat the elevation of HMGB1 might be associated with abnor-mal inflammatory responses, involving the excessive produc-tion of proinflammatory cytokines [82].
The important role of HMGB1 in fetal immune system hasbeen corroborated by data demonstrating that HMGB1 trig-gers inflammatory responses through upregulation of adhe-sion molecules and release of soluble proinflammatory medi-ators from endothelial cells [72]. Furthermore, HMGB1 exertsan essential role of neonatal immune responses with importantbiological functions, as a bridge between innate and adaptiveimmune responses [35].
Conclusion and future prospects
HMGB1 represents a common causal agent for various typesof diseases and may serve as a future target molecule poten-tially useful for understanding disease processes. Future stud-ies will define the pathways for HMGB1 release, elucidate themost effective strategies for blocking the effect of this
mediator and determine the nature of any side effects devel-oped when HMGB1 levels are reduced. Certain substances,able to inhibit the release or inactivate HMGB1 protein, areunder investigation. The study of HMGB1 should open newscenarios for diagnostic biomarkers and therapeutic strategies,both in childhood and in adult patients.
Funding source No external funding was secured for this study.
Financial disclosure The authors have no financial relationships rele-vant to this article to disclose.
Conflict of interest The authors have no conflicts of interest todisclose.
References
1. Abraham E, Arcaroli J, Carmody A, Wang H, Tracey KJ (2000)HMG-1 as a mediator of acute lung inflammation. J Immunol 165:2950–2954
2. Aghai ZH, Saslow JG, Meniru C et al (2010) High-mobility groupbox-1 protein in tracheal aspirates from premature infants: relation-ship with bronchopulmonary dysplasia and steroid therapy. JPerinatol 30:610–615
3. Agnello D, Wang H, Yang H, Tracey KJ, Ghezzi P (2002) HMGB-1, a DNA-binding protein with cytokine activity, induces brain TNFand IL-6 production, and mediates anorexia and taste aversion.Cytokine 18:231–236
4. Akikusa JD, Schneider R, Harvey EA et al (2007) Clinical featuresand outcome of pediatric Wegener′s granulomatosis. ArthritisRheum 57:837–844
5. Albayrak Y, Albayrak A, Celik M et al (2011) High mobility groupbox protein-1 (HMGB-1) as a new diagnostic marker in patientswith acute appendicitis. Scand J Trauma Resusc Emerg Med 19:27
6. Alleva LM, Yang H, Tracy KJ, Clark IA (2005) High mobilitygroup box 1 (HMGB1) protein: possible amplification signal inthe pathogenesis. R Soc Trop Med Hyg 99:171–174
7. Andersson U, Wang H, Palomblad K et al (2000) High mobilitygroup 1 protein (HMG1) stimulates proinflammatory cytokine syn-thesis in human monocytes. J Exp Med 192:565–570
8. Arrigo T, Chirico V, Salpietro V et al (2013) High-mobility groupprotein B1: a new biomarker of metabolic syndrome in obesechildren. Eur J Endocrinol 168:631–638
9. Asano T, Ichiki K, Koizumi S et al (2011) High mobility group box1 in cerebrospinal fluid from several neurological diseases at earlytime points. Int J Neurosci 121:480–484
10. Au AK, Aneja RK, Bell MJ et al (2012) Cerebrospinal fluid levelsof high-mobility group box 1 and cytochrome C predict outcomeafter pediatric traumatic brain injury. J Neurotrauma 29:2013–2021
11. Avalos AM, Kiefer K, Tian J, Christensen S, Shlomchik M, CoyleAJ et al (2010) RAGE-independent autoreactive B cell activation inresponse to chromatin and HMGB1/DNA immune complexes.Autoimmunity 43:103–110
12. Bachur RG, Hennelly K, Callahan MJ, Chen C, Monuteaux MC(2012) Diagnostic imaging and negative appendectomy rates inchildren: effects of age and gender. Pediatrics 129:877–884
13. BaruaM, Jenkins EC, ChenW, Kuizon S, Pullarkat RK, JunaidMA(2011) Glyoxalase I polymorphism rs2736654 causing theAla111Glu substitution modulates enzyme activity-implicationsfor autism. Autism Res 4:262–270
Eur J Pediatr

14. Berger RP, Bazaco MC, Wagner AK, Kochanek PM, Fabio A(2010) Trajectory analysis of serum biomarker concentrations facil-itates outcome prediction after pediatric traumatic and hypoxemicbrain injury. Dev Neurosci 32:396–405
15. Bierhaus A, Humpert PM, Morcos M et al (2005) UnderstandingRAGE, the receptor for advanced glycation end products. J MolMed 83:876–886
16. Bonaldi T, Talamo F, Scaffidi P et al (2003) Monocytic cellshyperacetylate chromatin protein HMGB1 to redirect it towardssecretion. EMBO J 22:551–560
17. Bonthius DJ, Karacay B (2002) Meningitis and encephalitis inchildren. An update. Neurol Clin 20:1013–1038
18. Boonyaratanakornkit V, Melvin V, Prendergast P et al (1998) High-mobility group chromatin proteins 1 and 2 functionally interact withsteroid hormone receptors to enhance their DNA binding in vitro andtranscriptional activity inmammalian cells.MolCell Biol 18:4471–4487
19. Bouma G, Strober W (2003) The immunological and genetic basisof inflammatory bowel disease. Nat Rev Immunol 3:521–533
20. Boyer D, Vargas SO, Slattery D, Rivera-Sanchez YM, Colin AA(2006) Churg–Strauss syndrome in children: a clinical and patho-logic review. Pediatrics 118:e914–e920
21. Brunner HI, Gladman DD, Ibañez D, Urowitz MD, Silverman ED(2008) Difference in disease features between childhood-onset andadult-onset systemic lupus erythematosus. Arthritis Rheum58:556–562
22. Buhimschi CS, Baumbusch MA, Dulay AT et al (2009)Characterization of RAGE, HMGB1, and S100beta ininflammation-induced preterm birth and fetal tissue injury. Am JPathol 175:958–975
23. Buhimschi CS, Dulay AT, Abdel-Razeq S et al (2009) Fetal inflam-matory response in women with proteomic biomarkers characteristicof intra-amniotic inflammation and preterm birth. BJOG 116:257–267
24. Bustin M (1999) Regulation of DNA-dependent activities by thefunctional motifs of the high mobility group chromosomal proteins.Mol Cell Biol 19:5237–5246
25. Bustin M (2002) At the crossroads of necrosis and apoptosis:signaling to multiple cellular targets by HMGB1. Sci STKE 51:E39
26. Bustin M, Reisch J, Einck L, Klippel JH (1982) Autoantibodies tonucleosomal protein; antibodies to HMG-17 in autoimmune dis-ease. Science 215:1245–1247
27. Campana L, Bosurgi L, BianchiME,Manfredi AA, Rovere-QueriniP (2009) Requirement of HMGB1 for stromal cell-derived factor-1/CXCL12-dependent migration of macrophages and dendritic cells.J Leukoc Biol 86:609–615
28. Carrol ED, Mankhambo LA, Jeffers G et al (2009) The diagnostic andprognostic accuracy of five markers of serious bacterial infection inMalawian children with signs of severe infection. PLoS One 4:e6621
29. Charre S, Rosmalen JC, Pelegri C et al (2012) Abnormalities indendritic cell and macrophage accumulation in the pancreas ofnonobese diabetic (NOD) mice during the early neonatal period.Histol Histopathol 17:393–401
30. Chavakis E, Hain A, VinciM, Carmona G, BianchiME, Vajkoczy Pet al (2007) High-mobility group box 1 activates integrin-dependenthoming of endothelial progenitor cells. Circ Res 100:204–212
31. ChenG, Li J, QiangX et al (2005) Suppression of HMGB1 release bystearoyl lysophosphatidylcholine: an additional mechanism for itstherapeutic effects in experimental sepsis. J Lipid Res 46:623–627
32. Chen GY, Tang J, Zheng P, Liu Y (2009) CD24 and Siglec-10selectively repress tissue damage-induced immune responses.Science 323:1722–1725
33. Chiba S, Baghdadi M, Akiba H et al (2012) Tumor-infiltrating DCssuppress nucleic acid-mediated innate immune responses throughinteractions between the receptor TIM-3 and the alarmin HMGB1.Nat Immunol 13:832–842
34. Choi J, Hyun JM, Jeon-Soo S (2011) Increased levels of HMGB1and pro-inflammatory cytokines in children with febrile seizures. JNeuroinflammation 8:135
35. Ciucci A, Gabriele I, Percario ZA, Affabris E, Colizzi V, Mancino G(2011) HMGB1 and cord blood: its role as immuno-adjuvant factorin innate immunity. PLoS One 6:e23766
36. Corcos M, Guilbaud O, Paterniti S et al (2003) Involvement ofcytokines in eating disorders: a critical review of the human litera-ture. Psychoneuroendocrinology 28:229–249
37. Costello E, Saudan P, Winocour E, Pizer L, Beard P (1997) Highmobility group chromosomal protein 1 binds to the adeno-associated virus replication protein (Rep) and promotes Rep-mediated site-specific cleavage of DNA, ATPase activity and tran-scriptional repression. EMBO J 16:5943–5954
38. Devaraj S, Dasu MR, Park SH, Jialal I (2009) Increased levels ofligands of Toll-like receptors 2 and 4 in type 1 diabetes.Diabetologia 52:1665–1668
39. Dubicke A, Andersson P, Fransson E et al (2010) High-mobilitygroup box protein 1 and its signalling receptors in human pretermand term cervix. J Reprod Immunol 84:86–94
40. Eguchi T, Nomura Y, Hashiguchi Tet al (2009) An elevated value ofhigh mobility group box 1 is a potential marker for poor response tohigh-dose of intravenous immunoglobulin treatment in patients withKawasaki syndrome. Pediatr Infect Dis J 28:339–341
41. Ellerman JE, Brown CK, de Vera M et al (2007) Masquerader: highmobility group box-1 and cancer. Clin Cancer Res 13:2836–2848
42. Emanuele E, Boso M, Brondino N et al (2010) Increased serumlevels of high mobility group box 1 protein in patients with autisticdisorder. Prog Neuropsychopharmacol Biol Psychiatry 34:681–683
43. Enstrom AM, Onore CE, Van de Water JA, Ashwood P (2010)Differential monocyte responses to TLR ligands in children withautism spectrum disorders. Brain Behav Immun 24:64–71
44. Fages C, Nolo R, Huttunen HJ, Eskelinen E, Rauvala H (2000)Regulation of cell migration by amphoterin. J Cell Sci 113:611–620
45. Ford HR, Sorrells DL, Knisely AS (1996) Inflammatory cytokines,nitric oxide, and necrotizing enterocolitis. Semin Pediatr Surg 5:155–159
46. Gallucci S, Matzinger P (2001) Danger signals: SOS to the immunesystem. Curr Opin Immunol 13:114–119
47. Garcia-Romo GS, Caielli S, Vega B et al (2011) Netting neutrophilsare major inducers of type I IFN production in pediatric systemiclupus erythematosus. Sci Transl Med 3:73ra20
48. Ge Y, Brown MG, Wang H, Fu SM (2012) Genetic approach tostudy lupus glomerulonephritis. Methods Mol Biol 900:271–290
49. Goodwin GH, Sanders C, Johns EW (1973) A new group ofchromatin-associated proteins with a high content of acidic andbasic amino acids. Eur J Biochem 38:14–19
50. Güller U, Rosella L, McCall J, Brügger LE, Candinas D (2011)Negative appendicectomy and perforation rates in patients undergoinglaparoscopic surgery for suspected appendicitis. Br J Surg 8:589–595
51. Hagiwara S, Iwasaka H, Uchino T, Noguchi T (2008) High mobilitygroup box 1 induces a negative inotropic effect on the left ventriclein an isolated rat heart model of septic shock: a pilot study. Circ J 72:1012–1017
52. Hauser WA (1994) The prevalence and incidence of convulsivedisorders in children. Epilepsia 35:S1–S6
53. Hemmi H, Takeuchi O, Kawai T et al (2000) A Toll-like receptorrecognizes bacterial DNA. Nature 408:740–745
54. Henes FO, Chen Y, Bley TA et al (2011) Correlation of serum levelof high mobility group box 1 with the burden of granulomatousinflammation in granulomatosis with polyangiitis (Wegener′s). AnnRheum Dis 70:1926–1929
55. Hoshina T, Kusuhara K, IkedaK,MizunoY, SaitoM, Hara T (2008)High mobility group box 1 (HMGB1) and macrophage migrationinhibitory factor (MIF) in Kawasaki disease. Scand J Rheumatol 37:445–449
56. Huang J, Liu K, Yu Y et al (2012) Targeting HMGB1-mediatedautophagy as a novel therapeutic strategy for osteosarcoma.Autophagy 8:275–277
Eur J Pediatr

57. Huang J, Ni J, Liu K et al (2012) HMGB1 promotes drug resistancein osteosarcoma. Cancer Res 72:230–238
58. Ito T, Kawahara K, Okamoto K et al (2008) Proteolytic cleavage ofhigh mobility group box 1 protein by thrombin–thrombomodulincomplexes. Arterioscler Thromb Vasc Biol 28:825–830
59. Janku F, McConkey DJ, Hong DS, Kurzrock R (2011) Autophagyas a target for anticancer therapy. Nat Rev Clin Oncol 8:528–539
60. Jennette JC, Falk RJ, Andrassy K et al (1994) Nomenclature ofsystemic vasculitides: proposal of an international consensus con-ference. Arthritis Rheum 37:187–192
61. Junaid MA, Kowal D, Barua M, Pullarkat PS, Sklower-Brooks S,Pullarkat RK (2004) Proteomic studies identified a single nucleotidepolymorphism in glyoxalase I as autism susceptibility factor. Am JMed Genet A 131:11–17
62. Kanakoudi-Tsakalidou F, Farmaki E, Tzimouli V et al (2014)Simultaneous changes in serum HMGB1 and IFN-α levels and inLAIR-1 expression on plasmatoid dendritic cells of patients withjuvenile SLE. New therapeutic options? Lupus 23:305–312
63. Kang R, Livesey KM, Zeh HJ, Lotze MT, Tang D (2011) Metabolicregulation by HMGB1-mediated autophagy and mitophagy.Autophagy 7:1256–1258
64. Kang R, Tang DL, Cao LZ, Yu Y, Zhang GY, Xiao XZ (2007) Highmobility group box 1 is increased in children with acute lympho-cytic leukemia and stimulates the release of tumor necrosis factor-alpha in leukemic cell. Zhonghua Er Ke Za Zhi 45:329–333
65. Kato S, Hussein MH, Kakita H et al (2009) Edaravone, a novel freeradical scavenger, reduces high-mobility group box 1 and prolongssurvival in a neonatal sepsis model. Shock 32:586–592
66. Klein-Gitelman M, Reiff A, Silverman ED (2002) Systemic lupuserythematosus in childhood. Rheum Dis Clin N Am 28:561–577
67. Koedel U (2009) Toll-like receptors in bacterial meningitis. CurrTop Microbiol Immunol 336:15–40
68. Kokkola R, Sundberg E, Ulfgren AK et al (2002) High mobilitygroup box chromosomal protein 1: a novel proinflammatory medi-ator in synovitis. Arthritis Rheum 46:2598–2603
69. Li M, Song L, Gao X, Chang W, Qin X (2012) Toll-like receptor 4on islet β cells senses expression changes in high-mobility groupbox 1 and contributes to the initiation of type 1 diabetes. Exp MolMed 44:260–267
70. Li J, Xie H, Wen T, Liu H, Zhu W, Chen X (2010) Expression ofhigh mobility group box chromosomal protein 1 and its modulatingeffects on downstream cytokines in systemic lupus erythematosus. JRheumatol 37:766–775
71. Lotze MT, Tracey KJ (2005) High-mobility group box 1 protein(HMGB1): nuclear weapon in the immune arsenal. Nat RevImmunol 5:331–342
72. Luan ZG, Zhang H, Yang PT, Ma XC, Zhang C, Guo RX (2010)HMGB1 activates nuclear factor-κB signaling by RAGE and in-creases the production of TNF-α in human umbilical vein endothe-lial cells. Immunobiology 215:956–962
73. Maroso M, Balosso S, Ravizza T et al (2010) Toll-like receptor 4and high-mobility group box-1 are involved in ictogenesis and canbe targeted to reduce seizures. Nat Med 16:413–419
74. Messmer D, Yang H, Telusma G, Knoll F, Li J, Messmer B et al (2004)High mobility group box protein 1: an endogenous signal for dendriticcell maturation and Th1 polarization. J Immunol 173:307–313
75. Miksa M, Wu R, Dong W et al (2009) Immature dendriticcell-derived exosomes rescue septic animals via milk fatglobule epidermal growth factor–factor VIII. J Immunol183:5983–5990
76. Mishra K, Jacobs SE, Doyle LE, Garland SM (2006) Newer ap-proaches to the diagnosis of early onset neonatal sepsis. Arch DisChild Fetal Neonatal Ed 91:F208–F212
77. Musumeci D, Roviello GN, Montesarchio D (2014) An overviewon HMGB1 inhibitors as potential therapeutic agents in HMGB1-related pathologies. Pharmacol Ther 141:347–357
78. Nakamura T, Yamada S, Yoshioka T (2012)Measurement of plasmaconcentration of high mobility group box1 (HMGB1) in earlyneonates and evaluation of its usefulness. Clin Chim Acta 413:237–239
79. Newburger JW, Takahashi M, Gerber MA et al (2004) Committeeon Rheumatic Fever, Endocarditis, and Kawasaki Disease, Councilon Cardiovascular Disease in the Young, American HeartAssociation. Diagnosis, treatment, and long-term management ofKawasaki disease: a statement for health professionals from theCommittee on Rheumatic Fever, Endocarditis, and KawasakiDisease, Council on Cardiovascular Disease in the Young,American Heart Association. Pediatrics 114:1708–1733
80. Nishitani C, Mitsuzawa H, Hyakushima N, Sano H, Matsushima N,Kuroki Y (2005) The Toll-like receptor 4 region Glu24-Pro34 iscritical for interaction with MD-2. Biochem Biophys Res Commun328:586–590
81. Noth I, StrekME, Leff AR (2003) Churg–Strauss syndrome. Lancet361:587–594
82. Okazaki K, Kondo M, Kato M et al (2008) Elevation of high-mobility group box 1 concentration in asphyxiated neonates.Neonatology 94:105–109
83. Okuma Y, Liu K, Wake H et al (2012) Anti-high mobility groupbox-1 antibody therapy for traumatic brain injury. Ann Neurol. doi:10.1002/ana.23602
84. Ozonoff S, Iosif AM, Baguio F et al (2010) A prospective study ofthe emergence of early behavioral signs of autism. J AmAcad ChildAdolesc Psychiatry 49:256–266
85. Palumbo R, Sampaolesi M, Marchis FD et al (2004) ExtracellularHMGB1, a signal of tissue damage, induces mesoangioblast migra-tion and proliferation. J Cell Biol 164:441–449
86. Park JS, Svetkauskaite D, He Q et al (2004) Involvement of TLR2and TRL4 in cellular activation by high mobility group box 1protein (HMGB1). J Biol Chem 279:7370–7376
87. Parkkinen J, Rauvala H (1991) Interactions of plasminogen andtissue plasminogen activator (t-PA) with amphoterin. Enhancementof t-PA-catalyzed plasminogen activation by amphoterin. J BiolChem 266:16730–16735
88. Pavare J, Grope I, Kalnins I, Gardovska D (2010) High-mobility groupbox-1 protein, lipopolysaccharide-binding protein, interleukin-6 and C-reactive protein in children with community acquired infections andbacteraemia: a prospective study. BMC Infect Dis 10:28
89. Raucci A, Cugusi S, Antonelli A et al (2008) A soluble form of thereceptor for advanced glycation endproducts (RAGE) is producedby proteolytic cleavage of the membrane-bound form by thesheddase a disintegrin and metalloprotease 10 (ADAM10).FASEB J 22:3716–3727
90. Read CM, Cary PD, Crane-Robinson C, Driscoll PC, Norman DG(1993) Solution structure of a DNA-binding domain from HMG1.Nucleic Acids Res 21:3427–3436
91. Romero R, Chaiworapongsa T, Alpay Savasan Z et al (2011)Damage-associated molecular patterns (DAMPs) in preterm laborwith intact membranes and preterm PROM: a study of the alarminHMGB1. J Matern Fetal Neonatal Med 24:1444–1455
92. Rosenberg AM, Cordeiro DM (2000) Relationship between sex andantibodies to high mobility group proteins 1 and 2 in juvenileidiopathic arthritis. J Rheumatol 27:2489–2493
93. Sakai E, Shimada-Sugawara M, Nishishita K, Fukuma Y, Naito M,Okamoto K et al (2012) Suppression of RANKL-dependent hemeoxygenase-1 is required for high mobility group box 1 release andosteoclastogenesis. J Cell Biochem 113:486–498
94. Sanders MS, van Well GT, Ouburg S, Morré SA, van Furth AM(2012) Toll-like receptor 9 polymorphisms are associated withseverity variables in a cohort of meningococcal meningitis survi-vors. BMC Infect Dis 12:112
95. Schierbeck H, Pullerits R, Pruunsild C et al (2012) Evaluation of thedanger signal HMGB1 as a potential biomarker in juvenile
Eur J Pediatr

idiopathic arthritis (JIA): a preliminary study using the novelbiobank jabba. Ann Rheum Dis 71:A10–A11
96. State MW, Neuroscience ŠN (2012) The emerging biology ofautism spectrum disorders. Science 337:1301–1303
97. Steinhausen HC (2002) The outcome of anorexia nervosa in the20th century. Am J Psychiatry 159:1284–1294
98. Stern D, Yan SD, Yan SF, Schmidt AM (2002) Receptor for advancedglycation endproducts: a multiligand receptor magnifying cell stressin diverse pathologic settings. Adv Drug Deliv Rev 54:1615–1625
99. Su X, Wang H, Zhao J, Pan H, Mao L (2011) Beneficial effects ofethyl pyruvate through inhibiting high-mobility group box 1 ex-pression and TLR4/NF-κB pathway after traumatic brain injury inthe rat. Mediat Inflamm 2011:807142
100. Taguchi A, Blood DC, del Toro G et al (2000) Blockade of RAGE-amphoterin signalling suppresses tumour growth and metastases.Nature 405:354–360
101. Taira T, Matsuyama W, Mitsuyama H et al (2007) Increased serumhigh mobility box-1 level in Churg–Strauss syndrome. Clin ExpImmunol 148:241–247
102. Tang D, Kang R, Cao L et al (2008) A pilot study to detect highmobility group box 1 and heat shock protein 72 in cerebro-spinal fluid of pediatric patients with meningitis. Crit CareMed 36:291–295
103. Tang D, Kang R, Coyne CB, Zeh HJ, Lotze MT (2012) PAMPs andDAMPs: signal 0 s that spur autophagy and immunity. ImmunolRev 249:158–175
104. Tian J, Avalos AM, Mao SY et al (2007) Toll-like receptor 9-dependent activation by DNA-containing immune complexes ismediated by HMGB1 and RAGE. Nat Immunol 8:487–496
105. Urbonaviciute V, Furnrohr BG, Meister S et al (2008) Induction ofinflammatory and immuneresponses byHMGB1-nucleosome com-plexes: implications for the pathogenesis of SLE. J Exp Med 205:3007–3018
106. Vezzani A, Balosso S, Maroso M, Zardoni D, Noe′ F, Ravizza T(2010) ICE/caspase 1 inhibitors and IL-1beta receptor antagonists aspotential therapeutics in epilepsy. Curr Opin Investig Drugs 11:43–50
107. Vezzani A, Granata T (2005) Brain inflammation in epilepsy: ex-perimental and clinical evidence. Epilepsia 46:1724–1743
108. Vitali R, Stronati L, Negroni A et al (2011) Fecal HMGB1 is a novelmarker of intestinal mucosal inflammation in pediatric inflammato-ry bowel disease. Am J Gastroenterol 106:2029–2040
109. Walker JM, Gooderham K, Hastings JR, Mayes E, Johns EW(1980) The primary structures of non-histone chromosomal proteinsHMG1 and 2. FEBS Lett 122:264–270
110. Wang KY, Yu GF, Zhang ZY, Huang Q, Dong WQ (2012) Plasmahigh-mobility group box 1 levels and prediction of outcome inpatients with traumatic brain injury. Clin ChimActa 413:1737–1741
111. Watson RS, Carcillo JA (2005) Scope and epidemiology of pediatricsepsis. Pediatr Crit Care 6:3–4
112. Wibisono D, Csernok E, Lamprecht P, Holle JU, GrossWL,MoosigF (2010) Serum HMGB1 levels are increased in active Wegener’sgranulomatosis and differentiate between active forms of ANCA-associated vasculitis. Ann Rheum Dis 69:1888–1889
113. Wittemann B, Neuer G, Michels H, Truckenbrodt H, Bautz FA(1990) Autoantibodies to nonhistone chromosomal proteinsHMG-1 and HMG-2 in sera of patients with juvenile rheumatoidarthritis. Arthritis Rheum 33:1378–1383
114. Wu SF, Caplan M, Lin HC (2012) Necrotizing enterocolitis: oldproblem with new hope. Pediatr Neonatol 53:158–163
115. Wu C, Sun H, Wang H et al (2012) Evaluation of high mobilitygroup box 1 protein as a presurgical diagnostic markerreflecting the severity of acute appendicitis. Scand JTrauma Resusc Emerg Med 20:61
116. Yang H, Ochani M, Li J et al (2004) Reversing established sepsiswith antagonists of endogenous high-mobility group box 1. ProcNatl Acad Sci U S A 101:296–301
117. Yang L, Yu Y, Kang R et al (2012) Up-regulated autophagy byendogenous high mobility group box-1 promotes chemoresistancein leukemia cells. Leuk Lymphoma 53:315–322
118. Yasuhara D, Hashiguchi T, Kawahara K et al (2007) High mobilitygroup box 1 and refeeding-resistance in anorexia nervosa. MolPsychiatry 12:976–977
119. Yotov WV, St-Arnaud R (1992) Nucleotide sequence of a mousecDNA encoding the nonhistonne chromosomal high mobility groupprotein-1 (HMG1). Nucleic Acids Res 20:3516
120. Young C, Sharma R, Handfield M,Mai V, Neu J (2009) Biomarkersfor infants at risk for necrotizing enterocolitis: clues to prevention?Pediatr Res 65:91R–97R
121. Yu M, Wang H, Ding A et al (2006) HMGB1 signals through Toll-like receptor (TLR) 4 and TLR 2. Shock 26:174–179
122. Zamora R, Grishin A,Wong C et al (2005) High-mobility group box1 protein is an inflammatory mediator in necrotizing enterocolitis:protective effect of the macrophage deactivator semapimod. Am JPhysiol Gastrointest Liver Physiol 289:G643–G652
123. Zetterstrom CK, Bergman T, Rynnel-Dagöö B et al (2002) Highmobility group box chromosomal protein 1 (HMGB1) is an antibacte-rial factor produced by the human adenoid. Pediatr Res 52:148–154
124. Zurolo E, Iyer A, Maroso M et al (2011) Activation of toll-likereceptor, RAGE and HMGB1 signalling in malformations of corti-cal development. Brain 134:1015–1032
125. Zwerina J, Eger G, Englbrecht M, Manger B, Schett G (2009)Churg–Strauss syndrome in childhood: a systematic literature re-view and clinical comparison with adult patients. Semin ArthritisRheum 39:108–115
Eur J Pediatr