Embed Size (px)
Citation preview
Anita Rajasekhar, MD, MS
University of Florida Health
Anne Rose, PharmD
University of Wisconsin Health
High Dose vs Low Dose: Duration of Therapy Debate
Presenters:
Disclosures
Anita Rajasekhar• Grants, Research or Clinical Trials: (institution receives support)
• Sanofi, Baxalta, Biomarin, Dimensions Therapeutics, Genetech, Janssen Pharmaceuticals, Roche, Bio Products laboratory, LTD, and Kedrion
Anne Rose• Grants, Research or Clinical Trials: Pfizer
Learning Objectives
By the end of this presentation the audience will be able to:
1. Recognize factors associated with increased risk of recurrent VTE2. Discuss appropriate duration of anticoagulation for VTE depending
on risk/benefit analysis3. Summarize evidence (or lack thereof!) on extended anticoagulation
in VTE associated with various clinical scenarios
Case 1: First Unprovoked VTE• 65 year-old man is diagnosed with a left femoral vein DVT. He has had
no recent travel, acute illness, hospitalization, surgery, trauma• PMHx: hypertension, hyperlipidemia, BMI 27• Labs including CBC and CMP are normal• Medications: ACE-I, statin• He was assessed to be at low risk of bleeding on anticoagulation. • He was on apixaban 10mg twice daily x 1 week followed by 5mg twice
daily thereafter• He returns to clinic at 3 months to discuss duration of anticoagulation• He is willing to continue long-term anticoagulation if needed
Questions to ask?
Why did he develop a DVT?
How should he be treated in the acute phase?
If long term anticoagulation is indicated, what should he be treated with?
How long should he be treated?
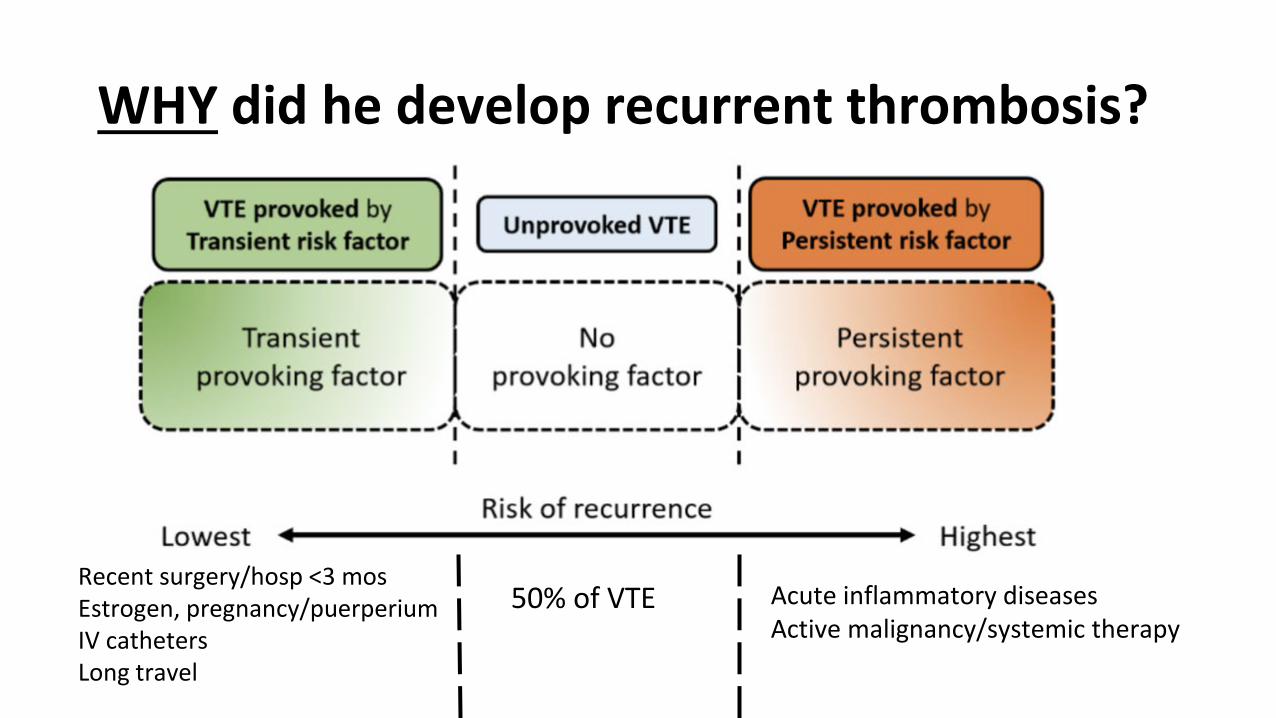
WHY did he develop recurrent thrombosis?
Recent surgery/hosp <3 mosEstrogen, pregnancy/puerperiumIV cathetersLong travel
Acute inflammatory diseasesActive malignancy/systemic therapy
50% of VTE
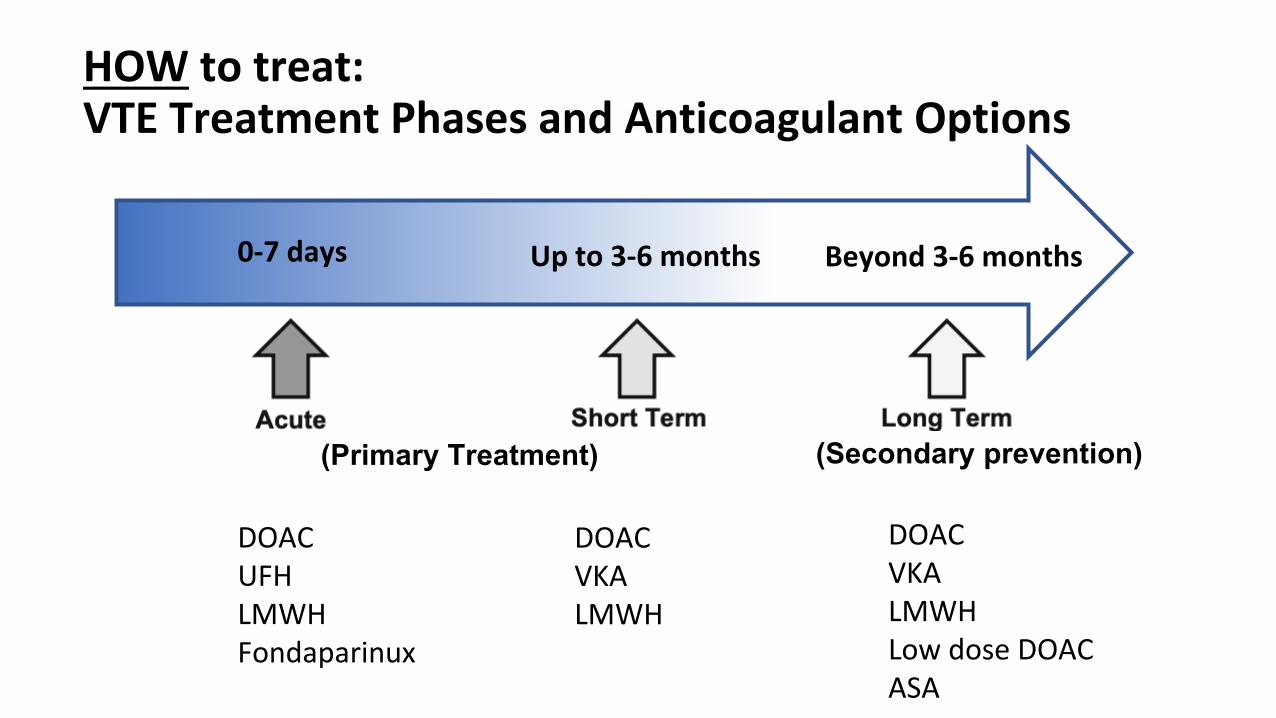
HOW to treat: VTE Treatment Phases and Anticoagulant Options
DOACUFHLMWHFondaparinux
DOACVKA LMWH
DOACVKA LMWH Low dose DOAC ASA
0-7 days Up to 3-6 months Beyond 3-6 months
(Primary Treatment) (Secondary prevention)
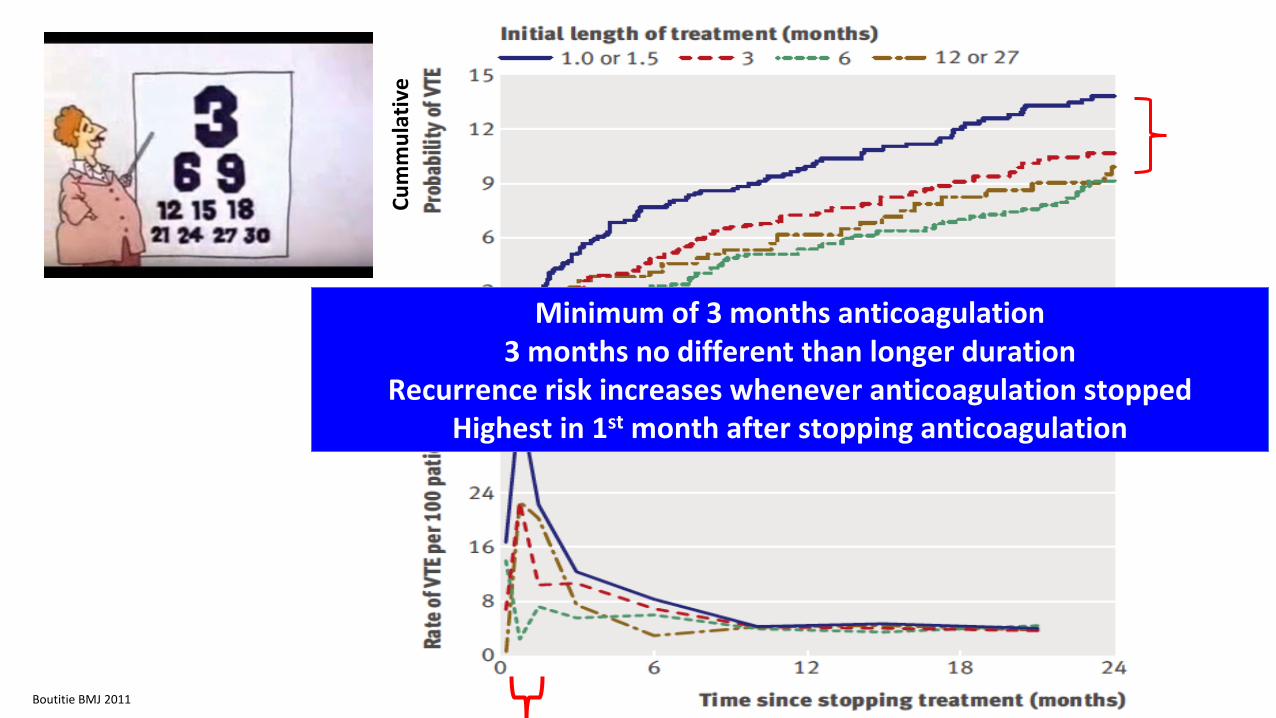
Minimum of 3 months anticoagulation3 months no different than longer duration
Recurrence risk increases whenever anticoagulation stoppedHighest in 1st month after stopping anticoagulation
Boutitie BMJ 2011
Cum
mul
ativ
e
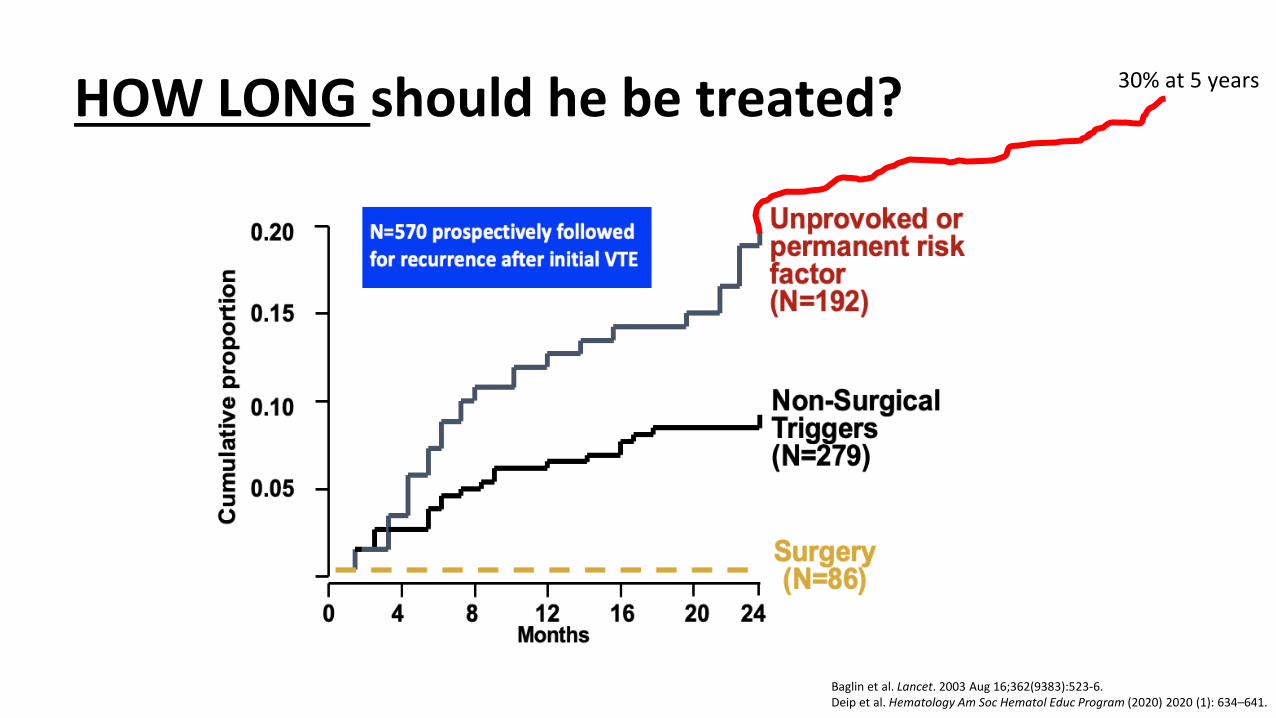
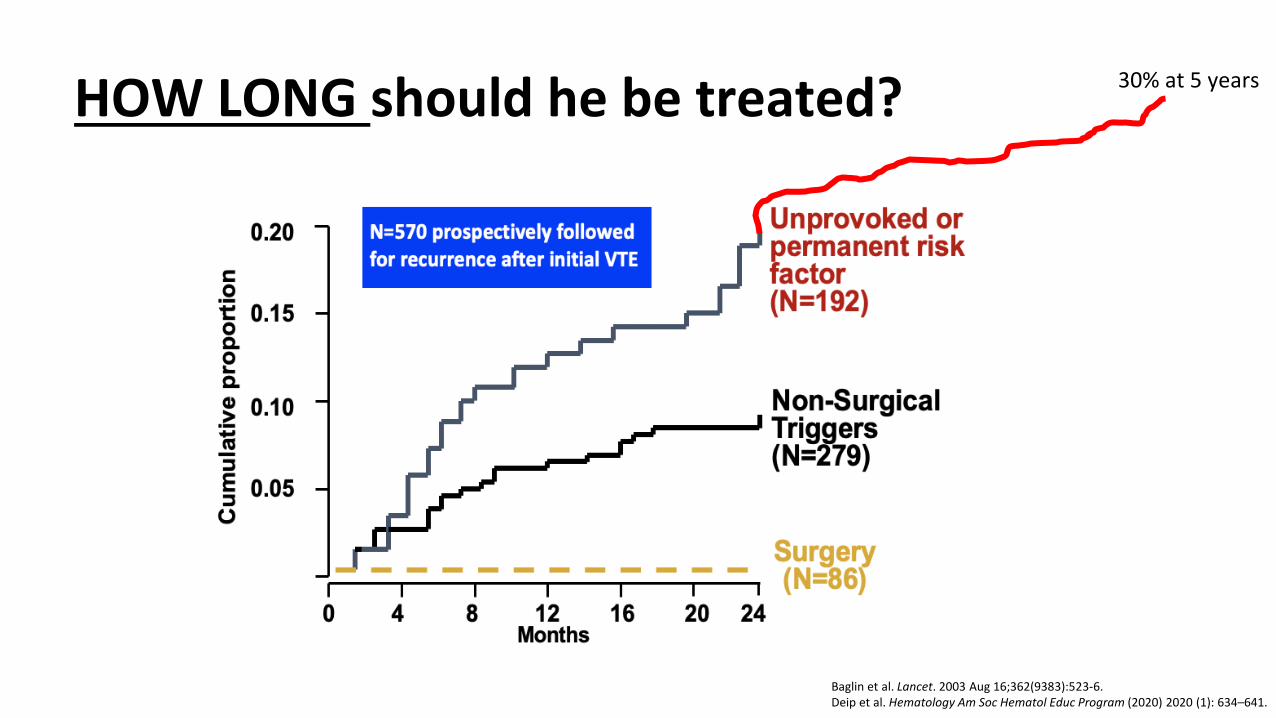
HOW LONG should he be treated?
Baglin et al. Lancet. 2003 Aug 16;362(9383):523-6.Deip et al. Hematology Am Soc Hematol Educ Program (2020) 2020 (1): 634–641.
30% at 5 years
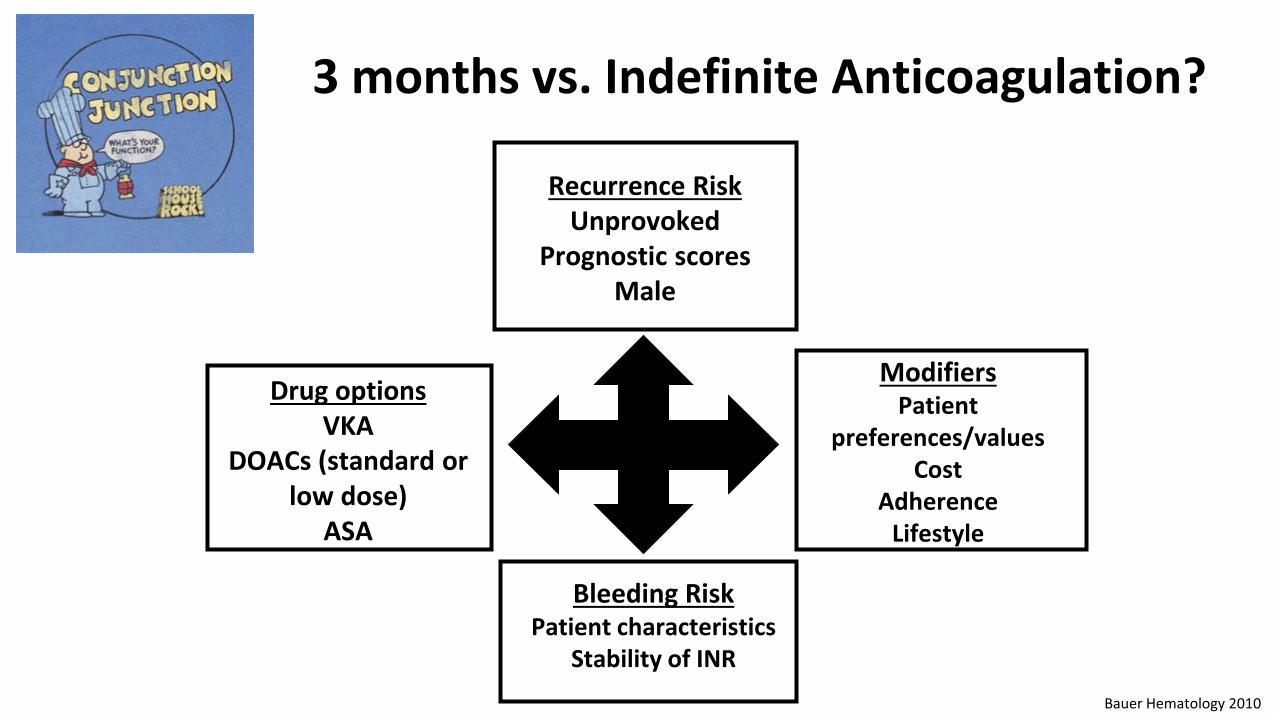
3 months vs. Indefinite Anticoagulation?
Drug optionsVKA
DOACs (standard or low dose)
ASA
Recurrence RiskUnprovoked
Prognostic scoresMale
Bleeding RiskPatient characteristics
Stability of INR
ModifiersPatient
preferences/valuesCost
AdherenceLifestyle
Bauer Hematology 2010
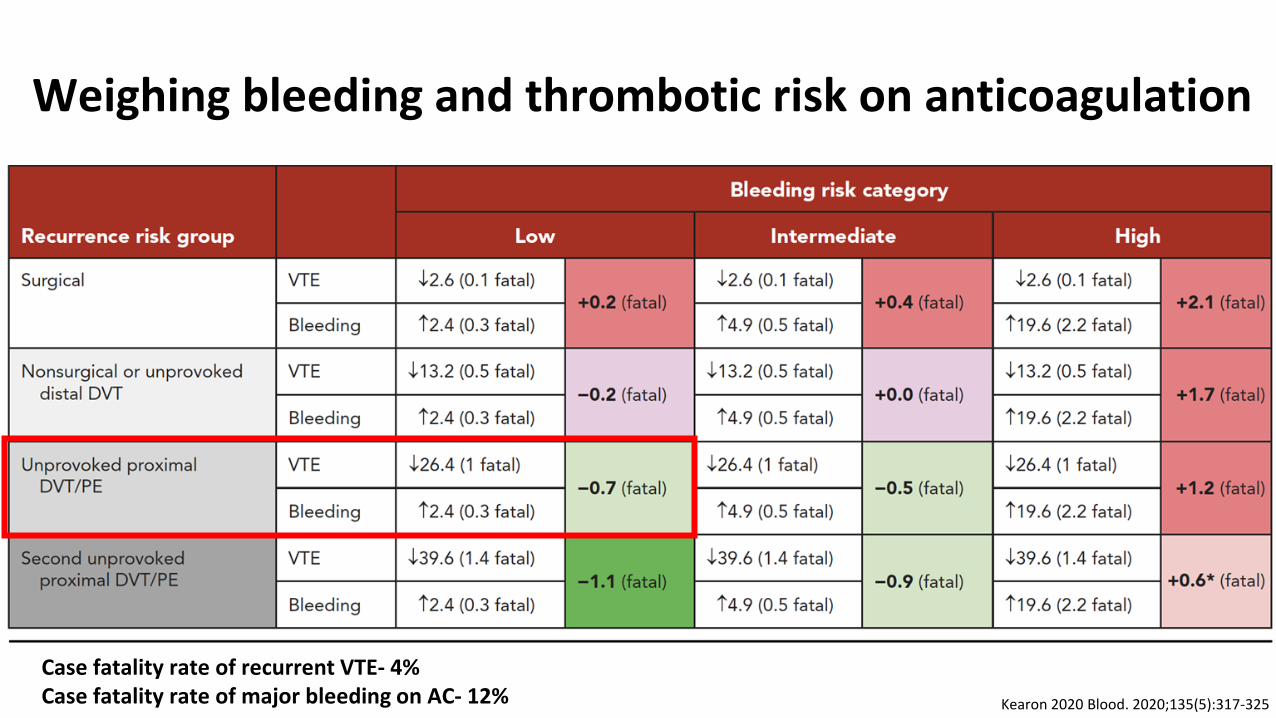
Weighing bleeding and thrombotic risk on anticoagulation
Kearon 2020 Blood. 2020;135(5):317-325
Case fatality rate of recurrent VTE- 4%Case fatality rate of major bleeding on AC- 12%
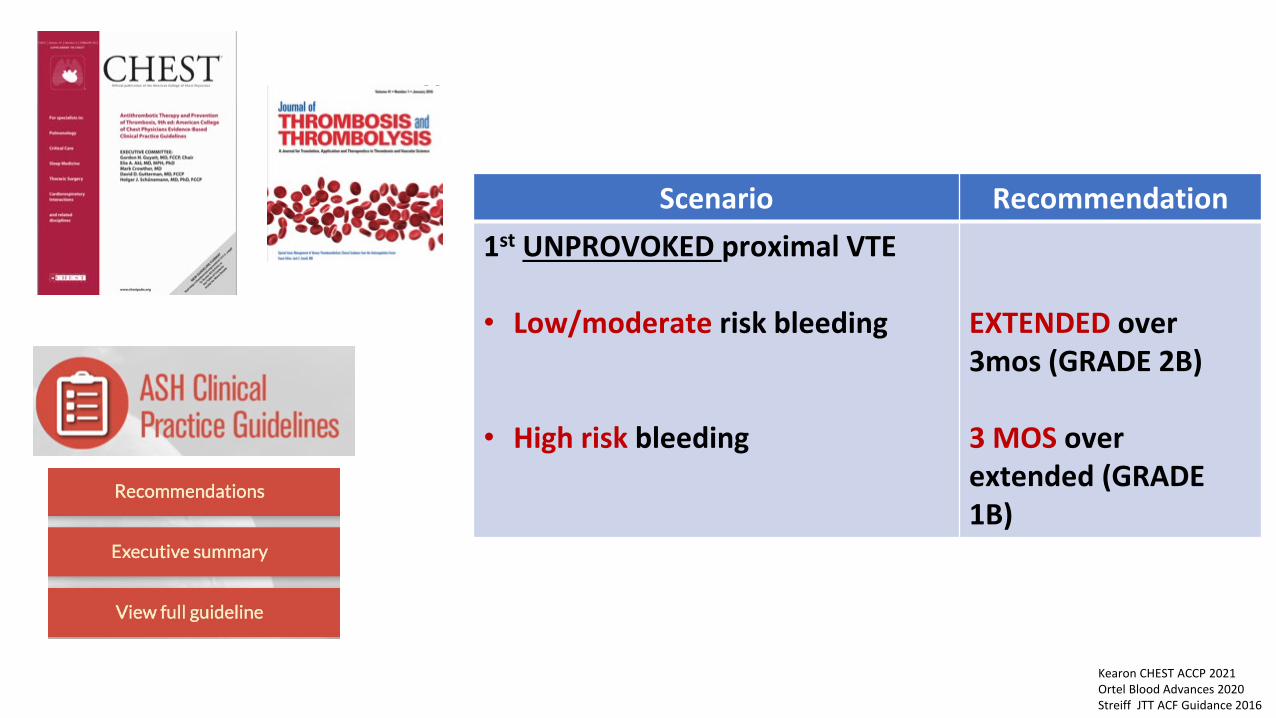
Scenario Recommendation1st UNPROVOKED proximal VTE
• Low/moderate risk bleeding
• High risk bleeding
EXTENDED over 3mos (GRADE 2B)
3 MOS over extended (GRADE 1B)
Kearon CHEST ACCP 2021Ortel Blood Advances 2020Streiff JTT ACF Guidance 2016
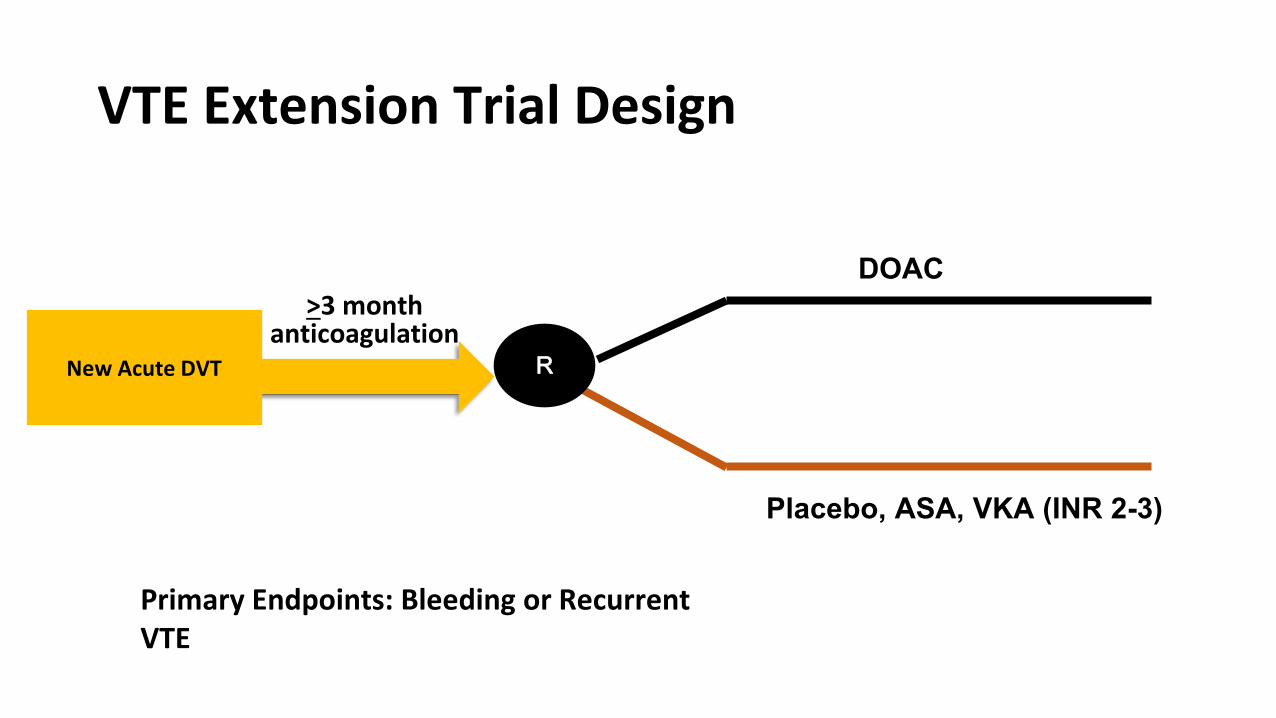
VTE Extension Trial Design
DOAC
Placebo, ASA, VKA (INR 2-3)
R
>3 month anticoagulation
Primary Endpoints: Bleeding or Recurrent VTE
New Acute DVT
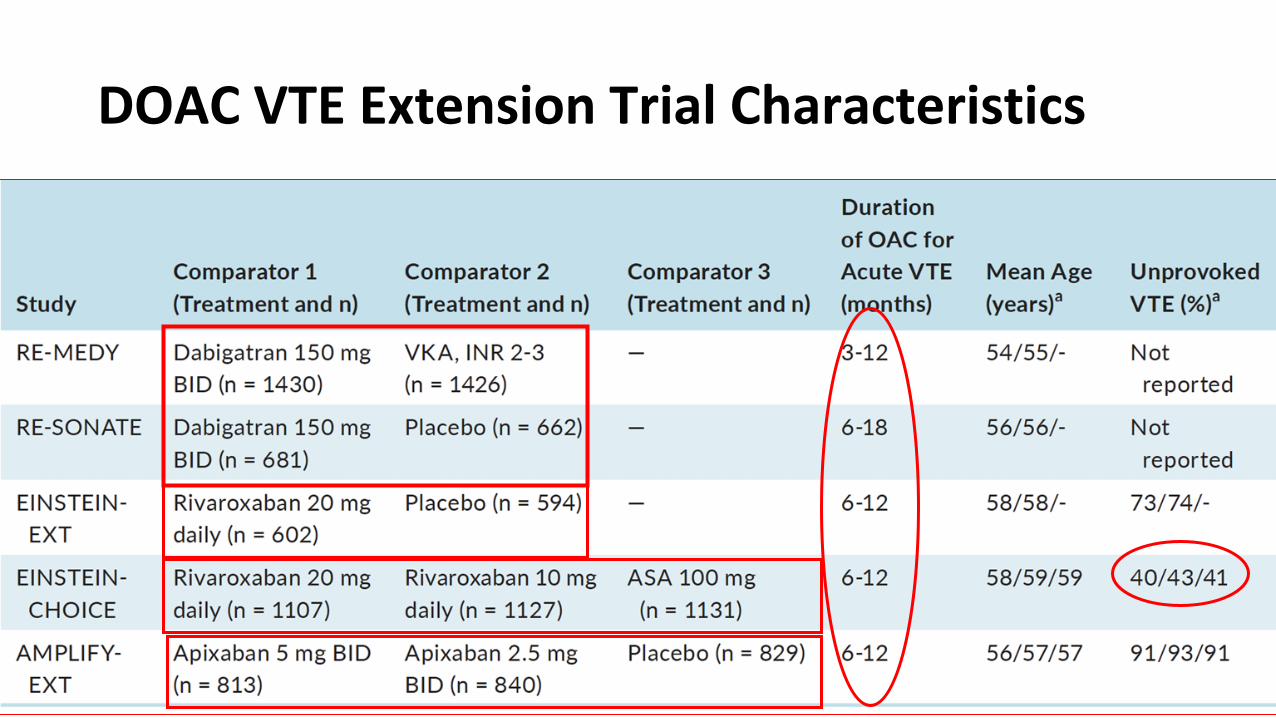
DOAC VTE Extension Trial Characteristics
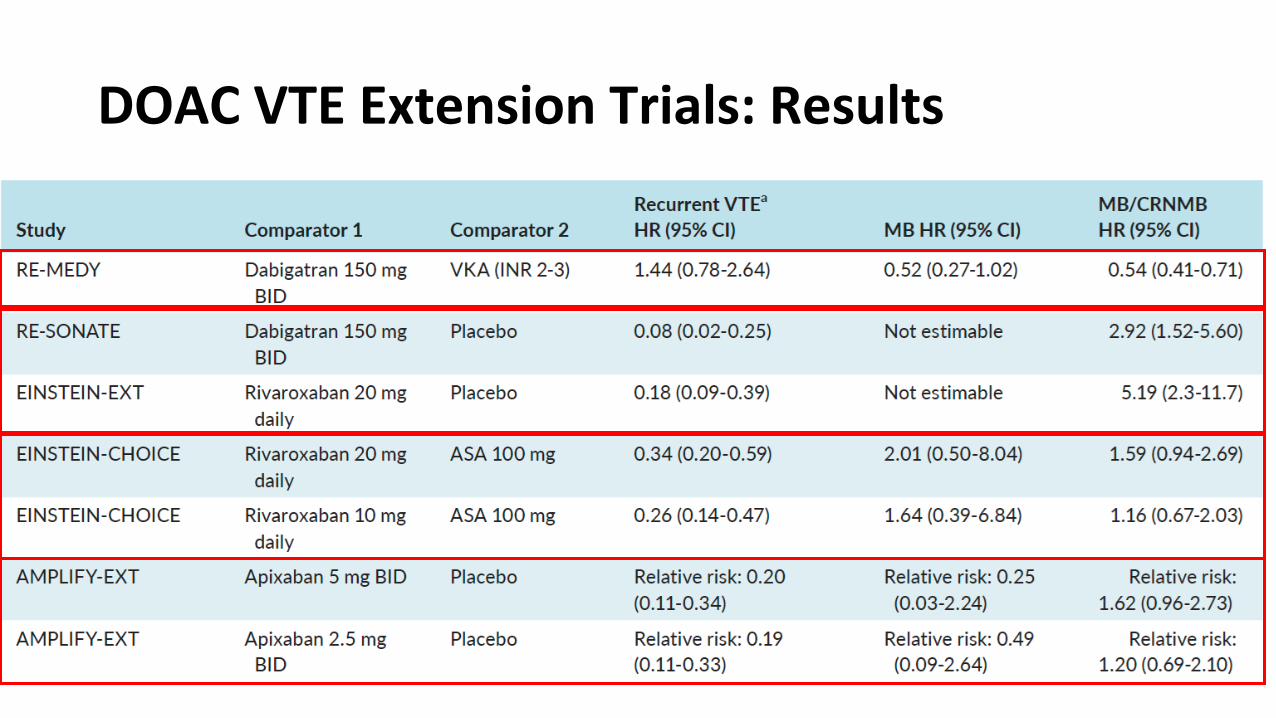
DOAC VTE Extension Trials: Results
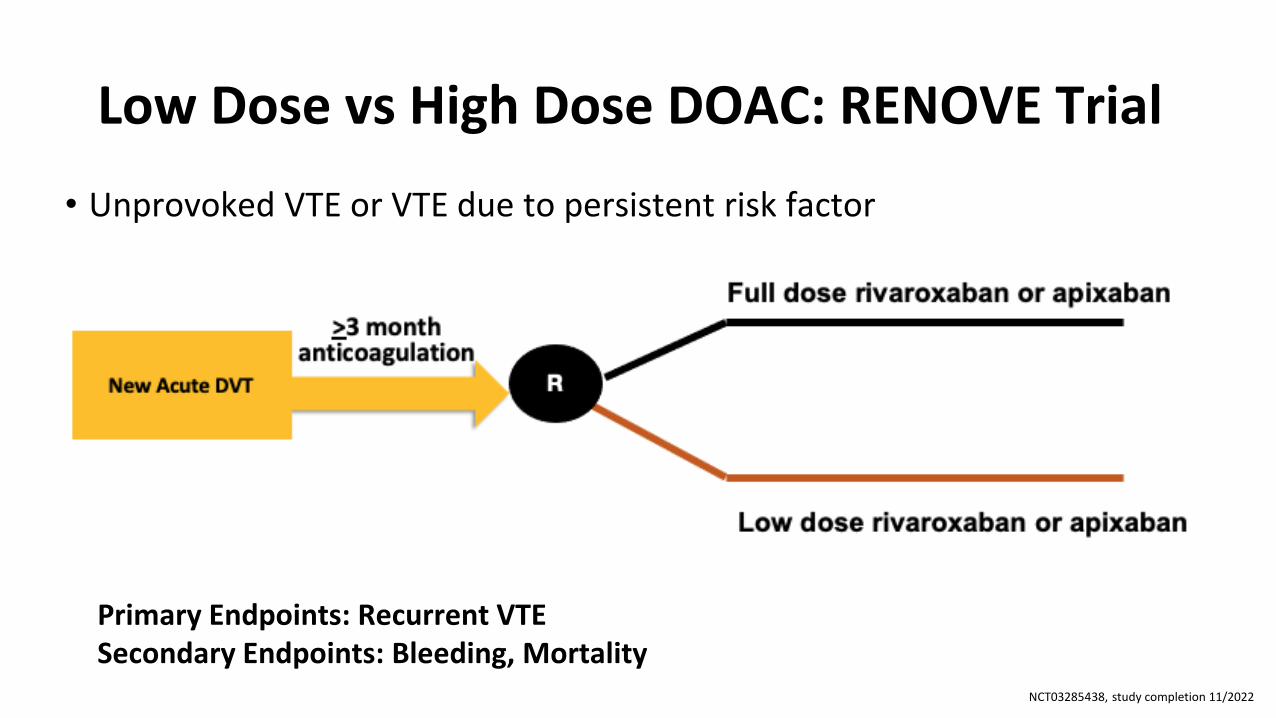
Low Dose vs High Dose DOAC: RENOVE Trial
• Unprovoked VTE or VTE due to persistent risk factor
Primary Endpoints: Recurrent VTESecondary Endpoints: Bleeding, Mortality
NCT03285438, study completion 11/2022

Case 1: Revisited
• Male with unprovoked LE DVT high recurrence risk• Renal function normal, no antiplatelet low bleeding risk• On DOAC without AE• No drug interactions with DOAC• Patient willing to continue anticoagulation
Continue long-term DOAC; consider low dose
Case 2: The Tale of Mr. Morton
• 60-year-old male presents to the ED with acute onset left sided chest pain (5/10)
• PMH: NIDDM2; HTN; s/p right ankle fracture surgery 3 weeks ago
• Cardiac workup: negative• CT: right sided subsegmental PE w/o signs of right heart strain• Enoxaparin 120 mg x 1 given in the ED; Discharged on apixaban• Patient following up in clinic 3 months later to discuss length of
therapy
Questions to ask?
Was the VTE provoked by a transient risk factor?
What is the patient’s bleeding risk?
What is the patient’s preference?
How significant was the event?
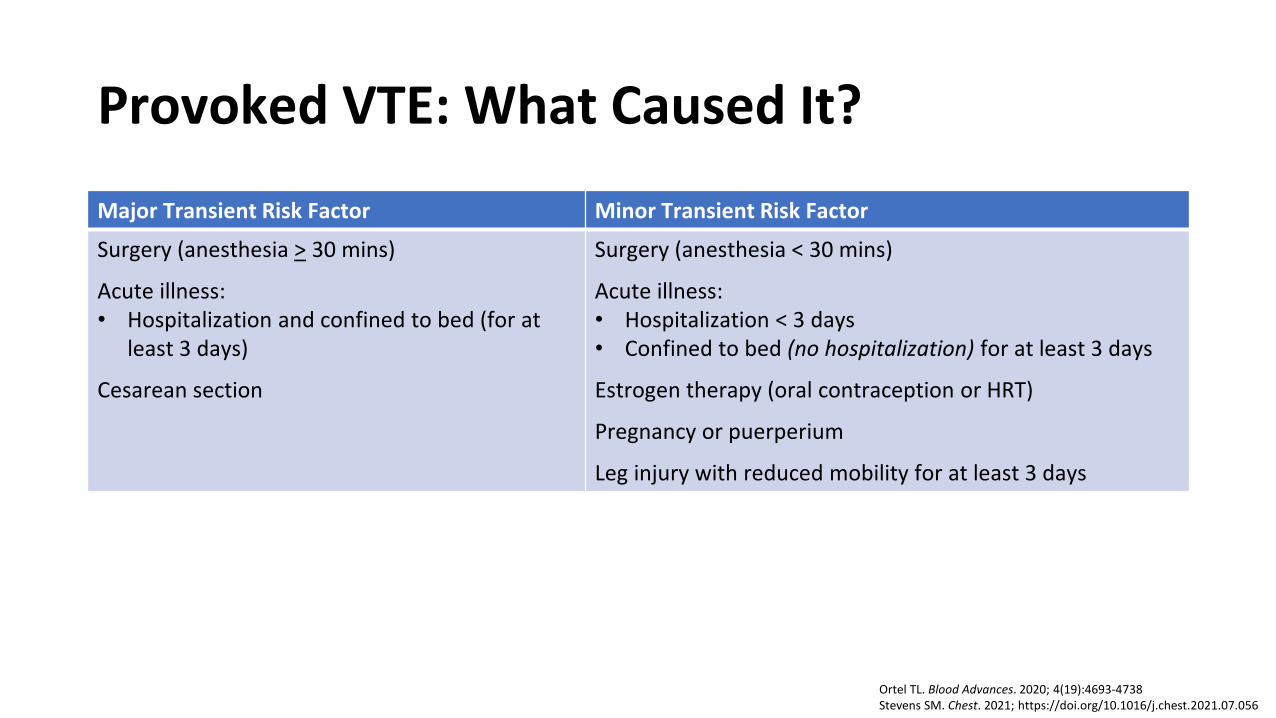
Provoked VTE: What Caused It?
Major Transient Risk Factor Minor Transient Risk Factor
Surgery (anesthesia > 30 mins)
Acute illness:• Hospitalization and confined to bed (for at
least 3 days)
Cesarean section
Surgery (anesthesia < 30 mins)
Acute illness:• Hospitalization < 3 days• Confined to bed (no hospitalization) for at least 3 days
Estrogen therapy (oral contraception or HRT)
Pregnancy or puerperium
Leg injury with reduced mobility for at least 3 days
Ortel TL. Blood Advances. 2020; 4(19):4693-4738Stevens SM. Chest. 2021; https://doi.org/10.1016/j.chest.2021.07.056
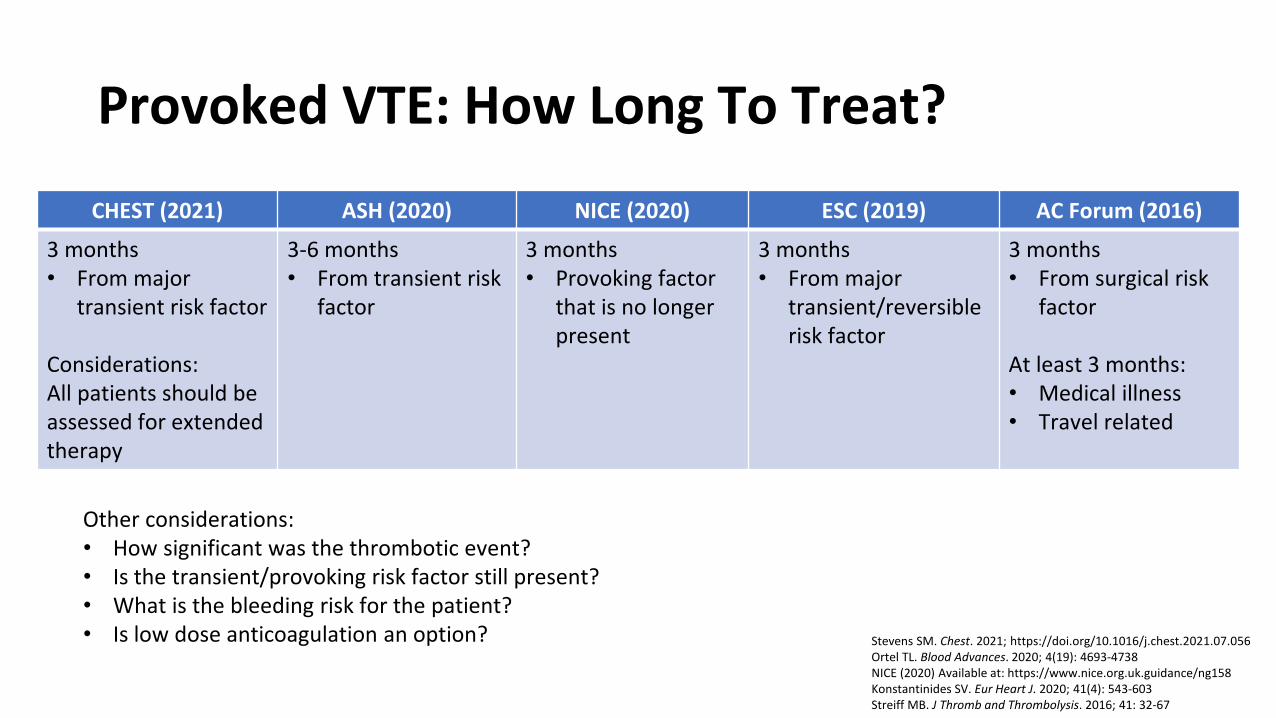
Provoked VTE: How Long To Treat?
CHEST (2021) ASH (2020) NICE (2020) ESC (2019) AC Forum (2016)
3 months• From major
transient risk factor
Considerations: All patients should be assessed for extended therapy
3-6 months• From transient risk
factor
3 months• Provoking factor
that is no longer present
3 months • From major
transient/reversible risk factor
3 months • From surgical risk
factor
At least 3 months:• Medical illness• Travel related
Other considerations: • How significant was the thrombotic event?• Is the transient/provoking risk factor still present?• What is the bleeding risk for the patient? • Is low dose anticoagulation an option? Stevens SM. Chest. 2021; https://doi.org/10.1016/j.chest.2021.07.056
Ortel TL. Blood Advances. 2020; 4(19): 4693-4738NICE (2020) Available at: https://www.nice.org.uk.guidance/ng158Konstantinides SV. Eur Heart J. 2020; 41(4): 543-603Streiff MB. J Thromb and Thrombolysis. 2016; 41: 32-67
HOW LONG should he be treated?
Baglin et al. Lancet. 2003 Aug 16;362(9383):523-6.Deip et al. Hematology Am Soc Hematol Educ Program (2020) 2020 (1): 634–641.
30% at 5 years
Case 2 revisited. Mr. Morton
• Transient risk factor: surgery
• Bleeding risk: low
• VTE event: subsegmental PE
• Patient preference: wishes to stop anticoagulation
• Length of therapy: 3 months
Case 3: Antiphospholipid Syndrome• A 32-year-old woman with h/o late 2nd trimester
miscarriage 5 years ago now presents with an unprovoked lobar PE
• Medications: none• Labs: CBC and CMP normal• She is started on LMWH bridge to VKA• She is found to meet criteria for APLS (triple aPL
positive)• She returns after 3 months to discuss duration of AC• She is interested in a DOAC if long term AC is needed. • INRs well controlled (time in therapeutic range 75%)

Questions to ask?
Why did she have a thrombotic event?
How should she be treated in the acute phase?
If long term anticoagulation is indicated, what should she be
treated with?
How long should she be treated?
Why did she develop unprovoked PE?
• Antiphospholipid Syndrome is an autoimmune disorder characterized by clinical and laboratory criteria
• Recurrence risk off anticoagulation-conflicting data• VTE ~30% annual risk vs no significant increased risk
• Triple positive higher thrombosis risk than single aPL• VTE ~ 5% annual risk or 37% at 10 years
Garcia et al Blood. 2013;122(5):817-824Pengo et al Blood. 2011;118(17):4714-4718Galli er al Blood 2007; 118(17): 4714-4718
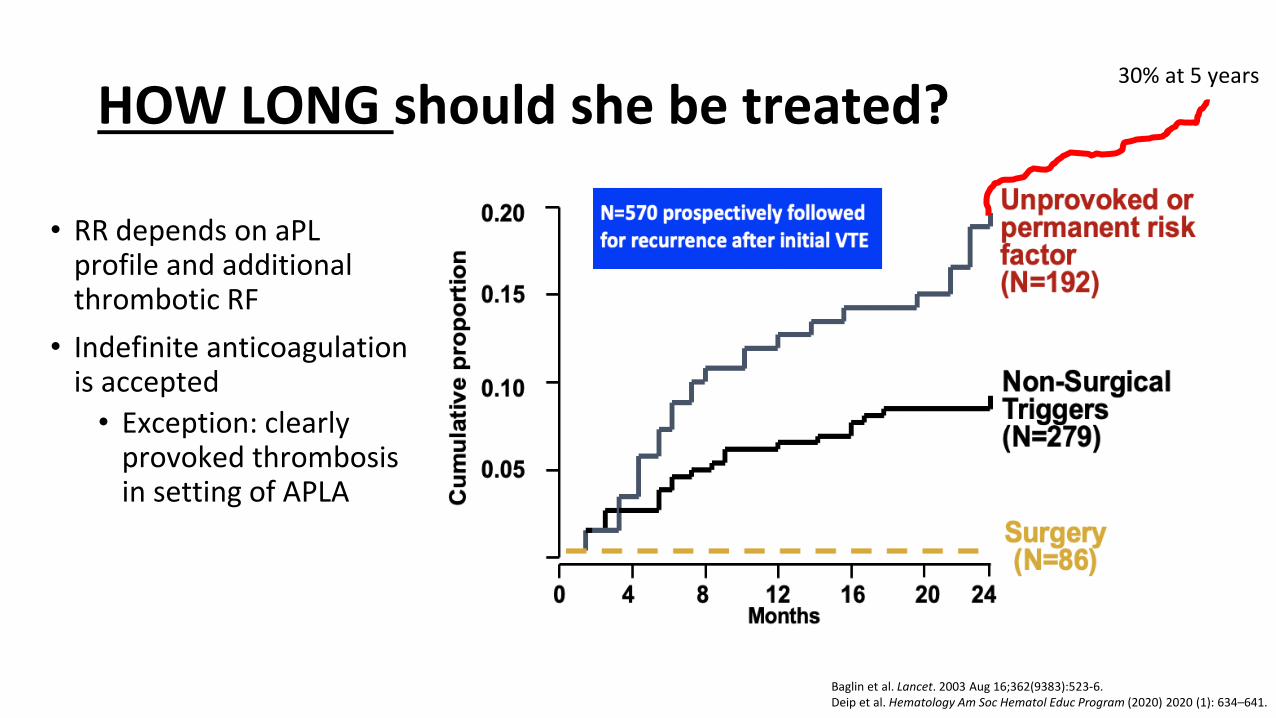
HOW LONG should she be treated?
• RR depends on aPL profile and additional thrombotic RF
• Indefinite anticoagulation is accepted
• Exception: clearly provoked thrombosis in setting of APLA
Baglin et al. Lancet. 2003 Aug 16;362(9383):523-6.Deip et al. Hematology Am Soc Hematol Educ Program (2020) 2020 (1): 634–641.
30% at 5 years
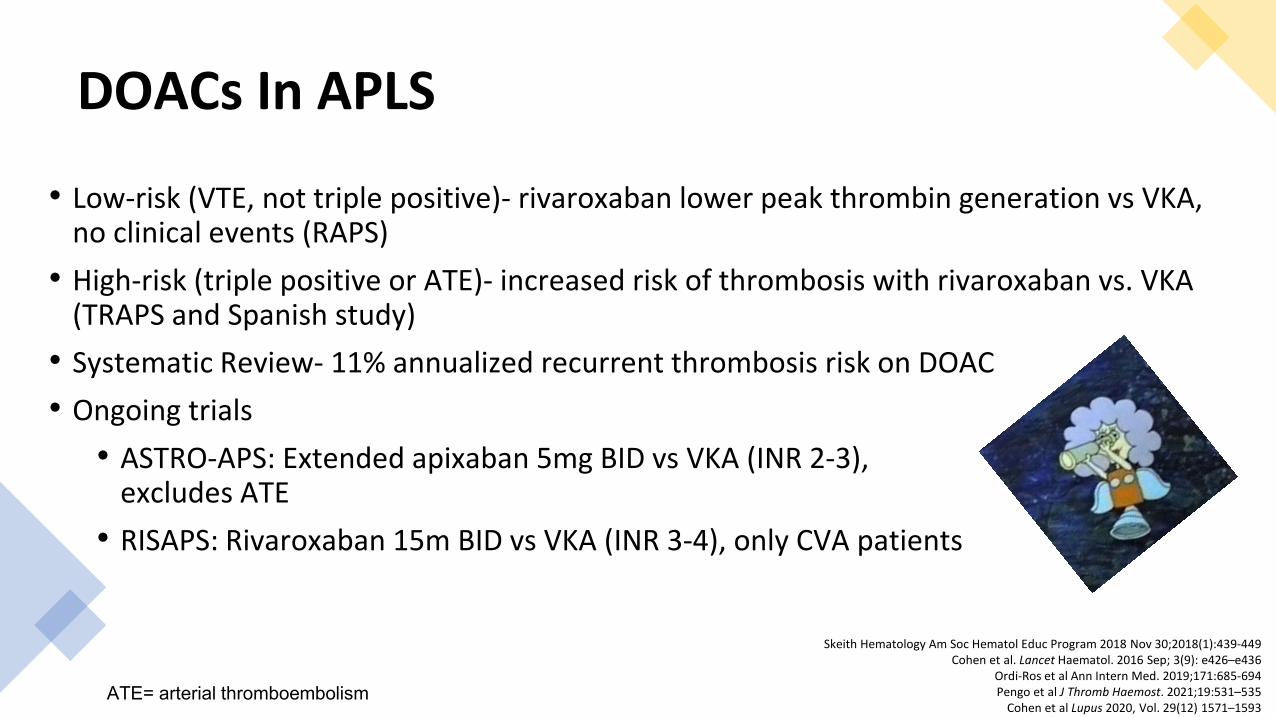
DOACs In APLS
• Low-risk (VTE, not triple positive)- rivaroxaban lower peak thrombin generation vs VKA, no clinical events (RAPS)
• High-risk (triple positive or ATE)- increased risk of thrombosis with rivaroxaban vs. VKA (TRAPS and Spanish study)
• Systematic Review- 11% annualized recurrent thrombosis risk on DOAC• Ongoing trials
• ASTRO-APS: Extended apixaban 5mg BID vs VKA (INR 2-3), excludes ATE
• RISAPS: Rivaroxaban 15m BID vs VKA (INR 3-4), only CVA patients
Skeith Hematology Am Soc Hematol Educ Program 2018 Nov 30;2018(1):439-449Cohen et al. Lancet Haematol. 2016 Sep; 3(9): e426–e436
Ordi-Ros et al Ann Intern Med. 2019;171:685-694Pengo et al J Thromb Haemost. 2021;19:531–535
Cohen et al Lupus 2020, Vol. 29(12) 1571–1593 ATE= arterial thromboembolism
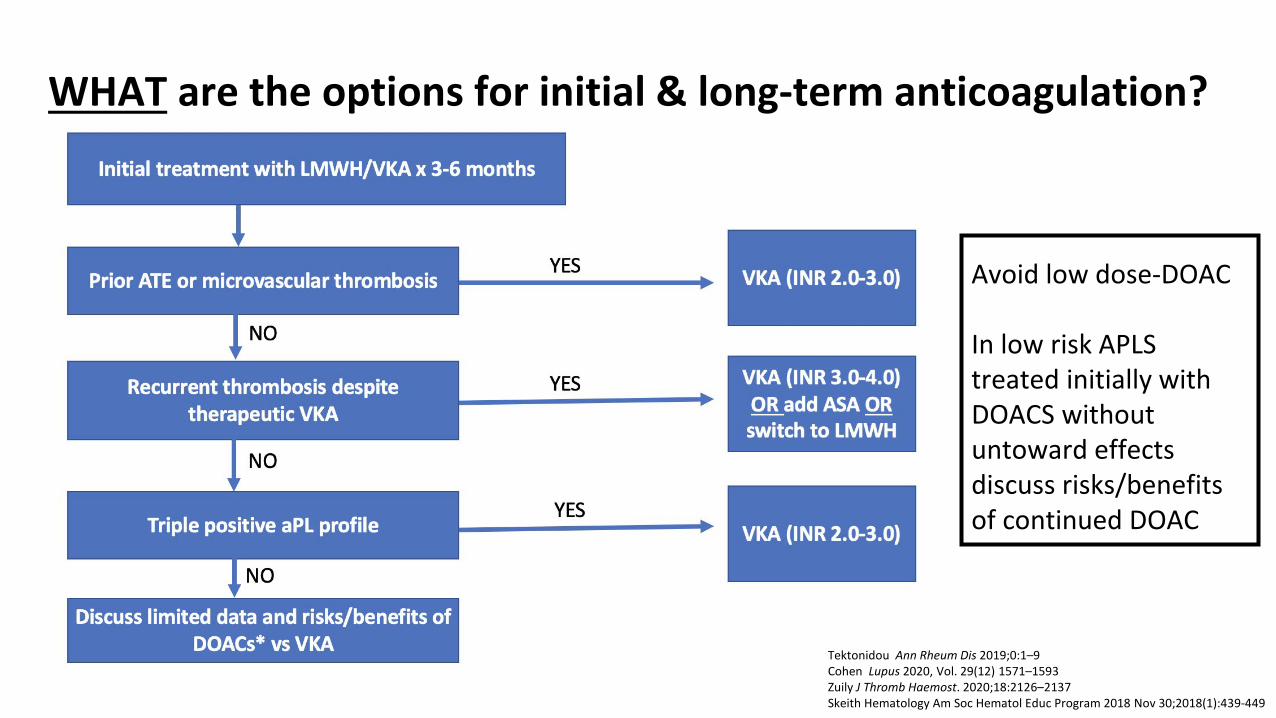
Avoid low dose-DOAC
In low risk APLS treated initially with DOACS without untoward effects discuss risks/benefits of continued DOAC
WHAT are the options for initial & long-term anticoagulation?
Tektonidou Ann Rheum Dis 2019;0:1–9Cohen Lupus 2020, Vol. 29(12) 1571–1593Zuily J Thromb Haemost. 2020;18:2126–2137Skeith Hematology Am Soc Hematol Educ Program 2018 Nov 30;2018(1):439-449
Case 3: Revisited
• APLS patient with VTE • Triple aPL positive• No prior arterial thrombosis• High time in therapeutic range (TTR) on warfarin• Low risk bleeding• Patient willing to continue anticoagulation
Continue long-term VKA
Case 4.
• 28-year-old female presents to the ED with LLE swelling and pain in foot. She is unable to bear weight on her foot.
• PMH: factor V Leiden (heterozygous), depression, generalized anxiety• Additional information: patient on oral contraception x 3 years• Doppler US: extensive DVT from left popliteal vein to common femoral vein• IR: thrombectomy• Patient started on rivaroxaban• Follow up with PCP 2 weeks after hospital discharge
Questions to ask?
Was the VTE provoked by a transient risk factor?
What is the patient’s bleeding risk?
What is the patient’s preference?
How significant was the event?
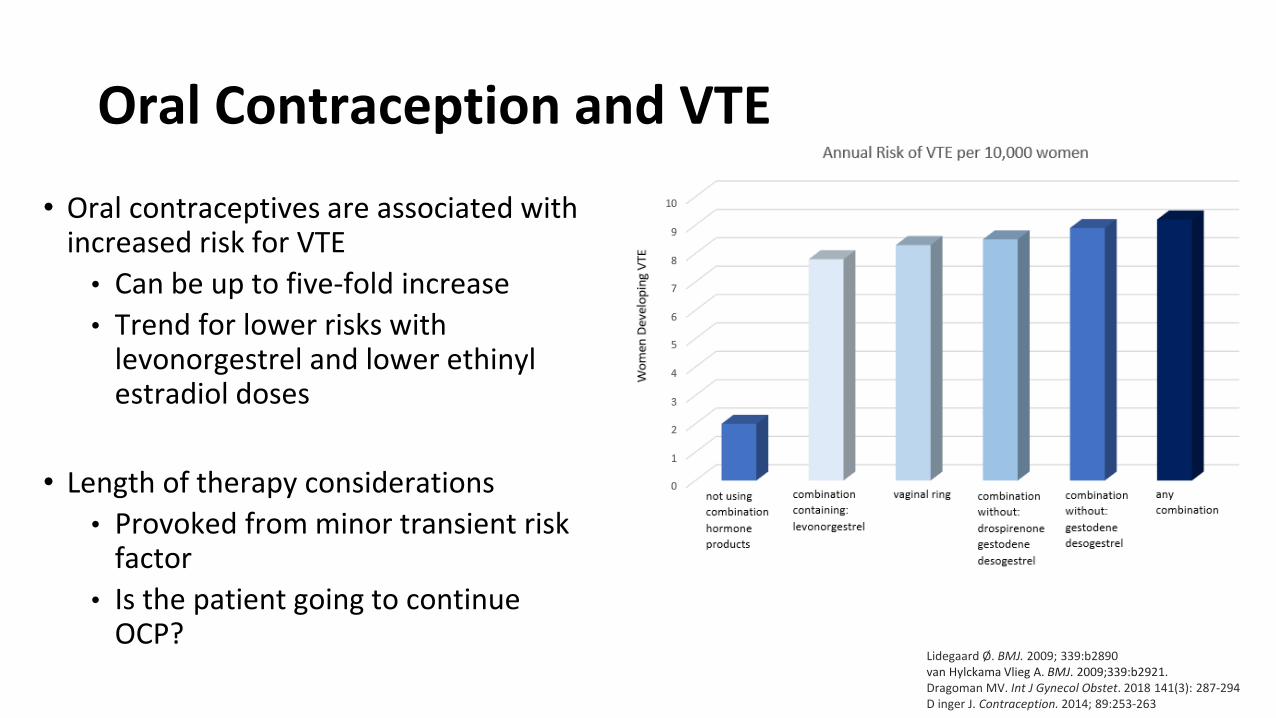
Oral Contraception and VTE
• Oral contraceptives are associated with increased risk for VTE
• Can be up to five-fold increase • Trend for lower risks with
levonorgestrel and lower ethinyl estradiol doses
• Length of therapy considerations• Provoked from minor transient risk
factor• Is the patient going to continue
OCP?Lidegaard Ø. BMJ. 2009; 339:b2890van Hylckama Vlieg A. BMJ. 2009;339:b2921.Dragoman MV. Int J Gynecol Obstet. 2018 141(3): 287-294D inger J. Contraception. 2014; 89:253-263
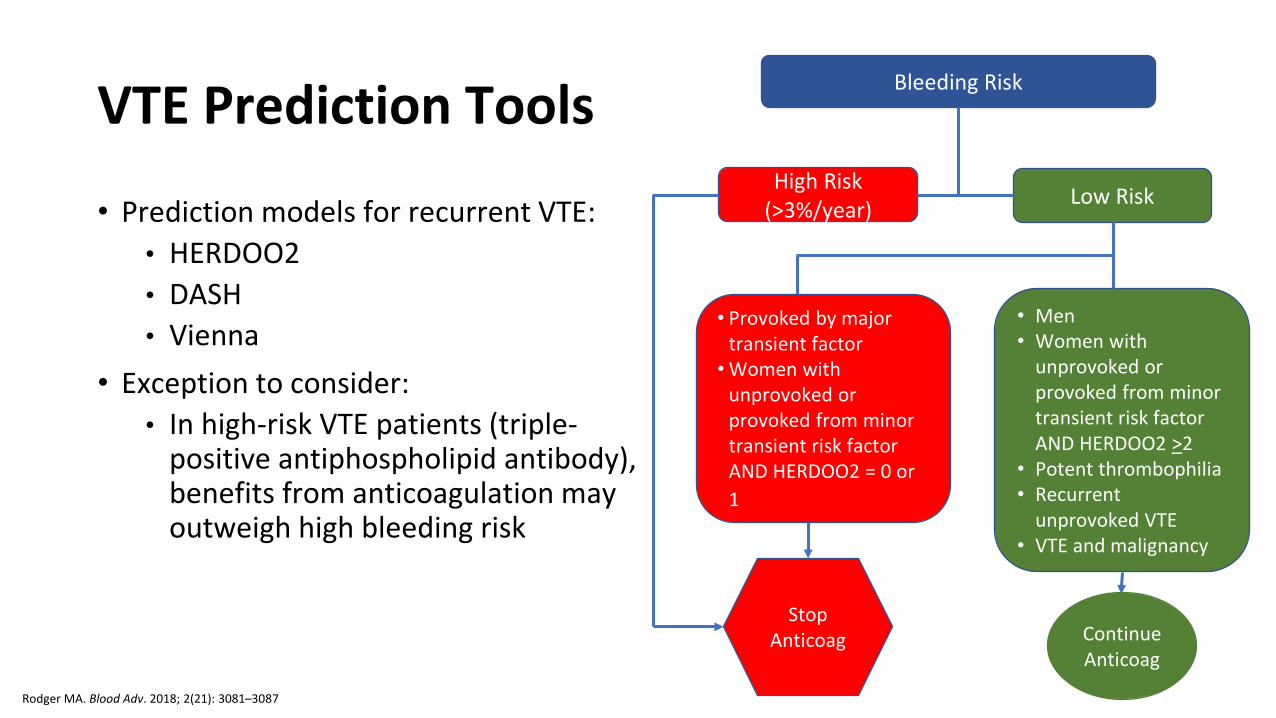
VTE Prediction Tools
• Prediction models for recurrent VTE:• HERDOO2• DASH• Vienna
• Exception to consider:• In high-risk VTE patients (triple-
positive antiphospholipid antibody), benefits from anticoagulation may outweigh high bleeding risk
Bleeding Risk
High Risk (>3%/year) Low Risk
• Provoked by major transient factor
• Women with unprovoked or provoked from minor transient risk factor AND HERDOO2 = 0 or 1
• Men• Women with
unprovoked or provoked from minor transient risk factor AND HERDOO2 >2
• Potent thrombophilia• Recurrent
unprovoked VTE• VTE and malignancy
Rodger MA. Blood Adv. 2018; 2(21): 3081–3087
Stop Anticoag Continue
Anticoag
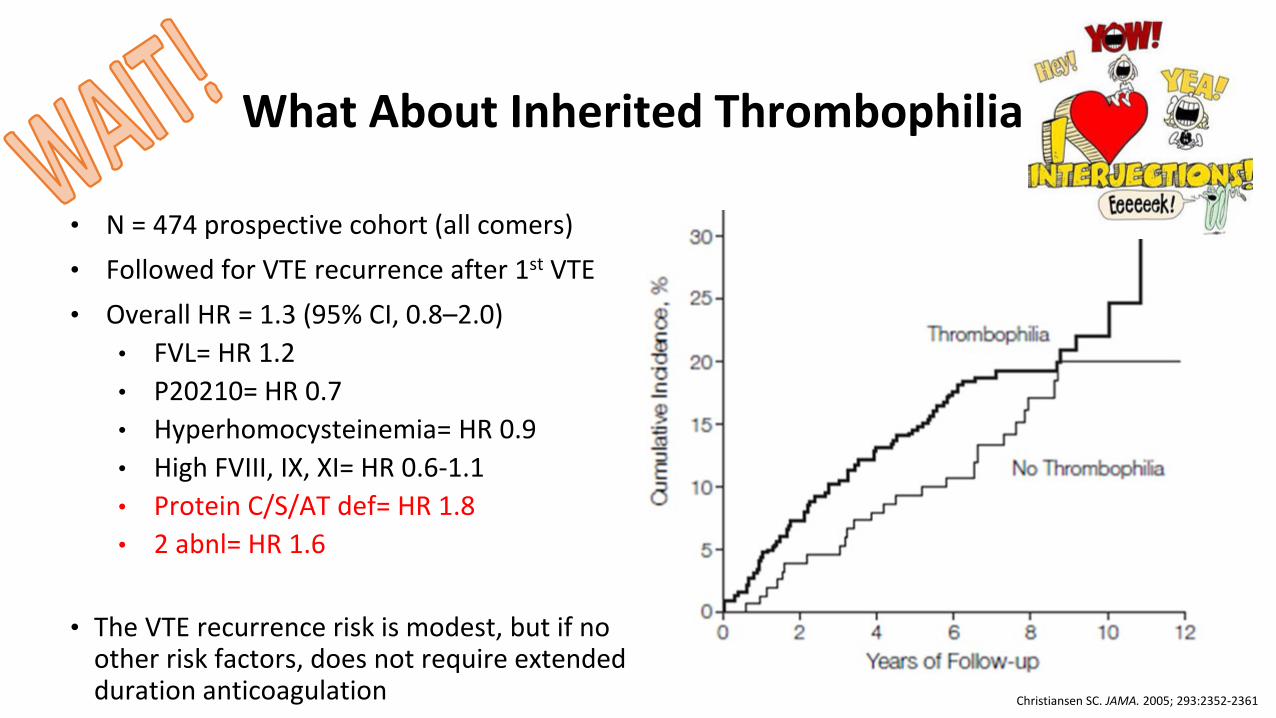
What About Inherited Thrombophilia
• N = 474 prospective cohort (all comers)• Followed for VTE recurrence after 1st VTE• Overall HR = 1.3 (95% CI, 0.8–2.0)
• FVL= HR 1.2• P20210= HR 0.7• Hyperhomocysteinemia= HR 0.9• High FVIII, IX, XI= HR 0.6-1.1• Protein C/S/AT def= HR 1.8• 2 abnl= HR 1.6
• The VTE recurrence risk is modest, but if no other risk factors, does not require extended duration anticoagulation Christiansen SC. JAMA. 2005; 293:2352-2361
Case 4 revisited
• Transient risk factor: oral contraceptives
• Bleeding risk: low
• VTE: extensive DVT
• Patient preference: wishes to stop anticoagulation
• Length of therapy: • At least 3 months• Consider 6 months• Consider low dose
-6
Case 5: Malignancy
• A 52-year-old male with stage 4 lung cancer on palliative chemotherapy presents with acute PE
• Labs reveal mild anemia (Hb 10.5 g/dL) but otherwise normal. • His bleeding risk is judged to be moderate• He is started apixaban 10mg BID for 1 week followed by 5mg BID• He returns for 3-month follow-up visit and would like to discuss
duration of anticoagulation• He is agreeable to staying on anticoagulation, if needed
Questions to ask?
Why did he have a thrombotic event?
How should he be treated in the acute phase?
If long term anticoagulation is indicated, what should he be treated
with?
How long should he be treated?
WHY Did Patient Develop Thrombosis?
• Malignancy is the most common persistent VTE risk factor
• Cumulative incidence recurrence up 20% at 12mos
• VTE risk influenced by cancer type, stage, treatment, and patient-related factors
• Challenges to anticoagulation include thrombocytopenia, drug interactions, liver/renal disease from metastasis or therapy adverse effects, malabsorption, poor PO intake

HOW to treat in cancer patient:VTE Treatment Phases and Anticoagulant Options
DOAC (Apix, Riva) LMWH
UFHFondaparinux
DOACLMWH
VKA
DOACLMWH
VKA (INR 2-3)Low dose DOAC Nothing
0-7 days Up to 3-6 months Beyond 3-6 months
Lyman et al. Blood Advances 2021; 5(4): 927-974; Key et al. J Clin Oncol. 2020;38(5):496-520; Farge et al. Lancet Oncol. 2019;20(10):e566-e581; https://www.nccn.org/professionals/physician_gls/default.aspx#supportive
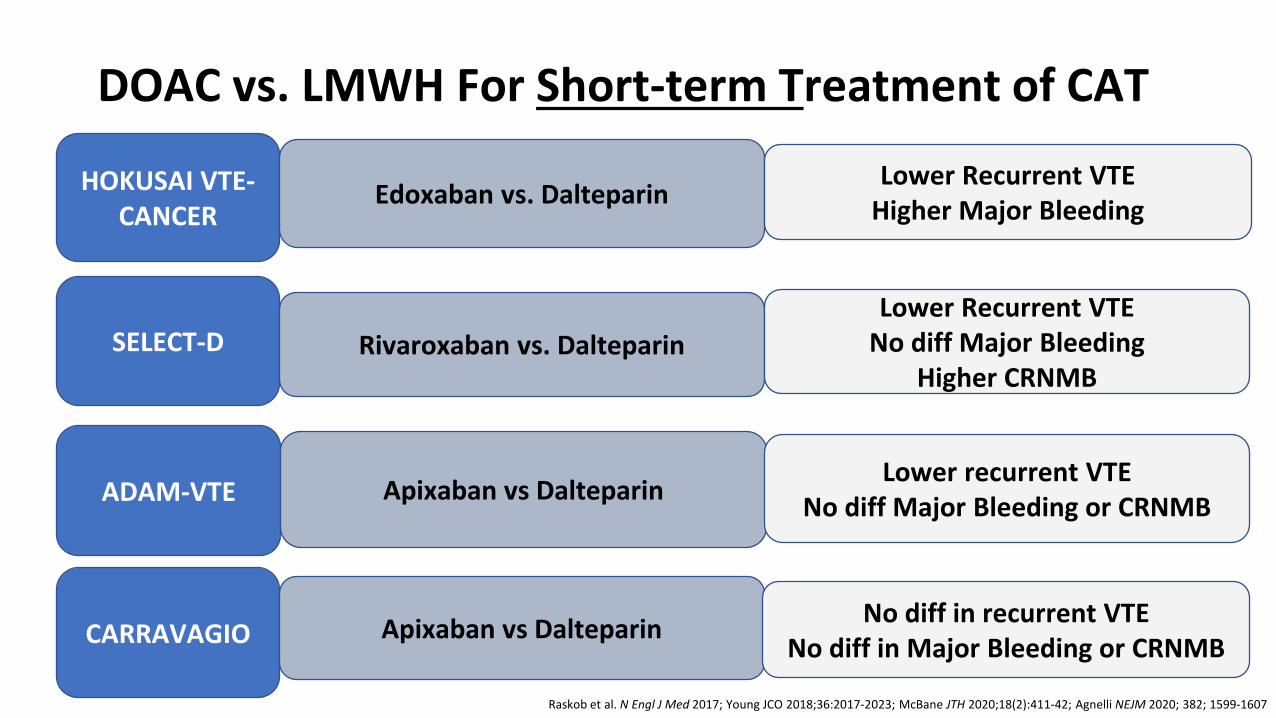
SELECT-D
HOKUSAI VTE-CANCER
ADAM-VTE
Edoxaban vs. Dalteparin
Rivaroxaban vs. Dalteparin
Apixaban vs Dalteparin
DOAC vs. LMWH For Short-term Treatment of CAT
CARRAVAGIO Apixaban vs Dalteparin
Lower recurrent VTENo diff Major Bleeding or CRNMB
Lower Recurrent VTEHigher Major Bleeding
Lower Recurrent VTENo diff Major Bleeding
Higher CRNMB
No diff in recurrent VTENo diff in Major Bleeding or CRNMB
Raskob et al. N Engl J Med 2017; Young JCO 2018;36:2017-2023; McBane JTH 2020;18(2):411-42; Agnelli NEJM 2020; 382; 1599-1607
2 Decision Points After Short-term Treatment
1. Continue beyond 6 months?
• How do we risk stratify?
2. Which anticoagulant to use?
• LMWH vs DOAC vs VKA?
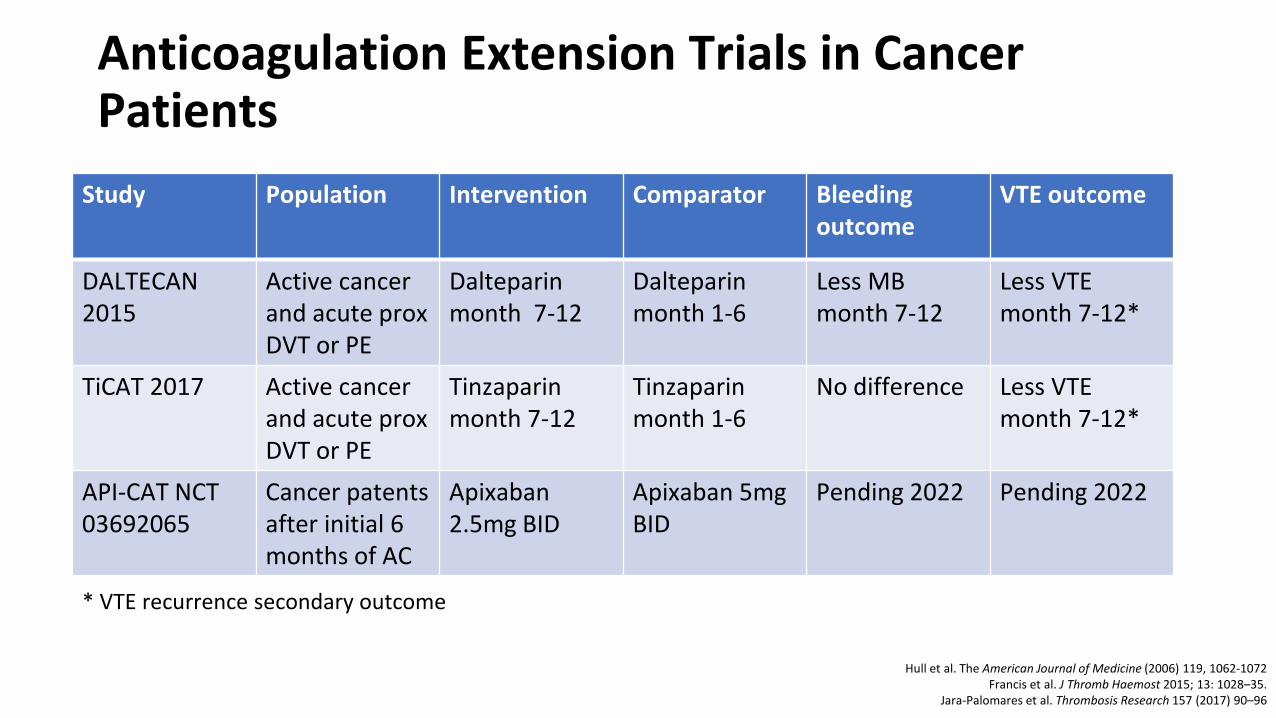
Anticoagulation Extension Trials in Cancer Patients
Study Population Intervention Comparator Bleeding outcome
VTE outcome
DALTECAN 2015
Active cancer and acute prox DVT or PE
Dalteparin month 7-12
Dalteparin month 1-6
Less MB month 7-12
Less VTE month 7-12*
TiCAT 2017 Active cancer and acute proxDVT or PE
Tinzaparin month 7-12
Tinzaparin month 1-6
No difference Less VTE month 7-12*
API-CAT NCT 03692065
Cancer patents after initial 6 months of AC
Apixaban 2.5mg BID
Apixaban 5mg BID
Pending 2022 Pending 2022
* VTE recurrence secondary outcome
Hull et al. The American Journal of Medicine (2006) 119, 1062-1072Francis et al. J Thromb Haemost 2015; 13: 1028–35.
Jara-Palomares et al. Thrombosis Research 157 (2017) 90–96
Bottom Line in Cancer-Associated Thrombosis • No study definitive on 3-6 months vs. longer
• Decision to extend beyond 6 months multifactorial
• Metastatic disease, active disease with ongoing systemic therapycontinue
• Remission, cure, no ongoing therapy, catheter remove stop
• Drug of choice for long-term anticoagulation unknown
Lyman et al. Blood Advances 2021; 5(4): 927-974Key et al. J Clin Oncol. 2020;38(5):496-520
Farge et al. Lancet Oncol. 2019;20(10):e566-e581https://www.nccn.org/professionals/physician_gls/default.aspx#supportive
Case 5 revisited
• Metastatic malignancy and ongoing therapy high risk recurrence• Bleeding risk judged to be moderate• On preferred AC with DOAC without AE• Not GI/GU tumor• No drug interactions with DOAC• Patient willing to continue anticoagulation
Continue long-term DOAC; for now, full dose
Case 6. What’s Happening? • 68-year-old male diagnosed with unprovoked right lower lobe PE
• Discharged on LMWH bridge to warfarin for long term anticoagulation therapy (due to DOAC $$)
• PMH: HTN, HLP, IDDM2; CKD (Scr 1.8; CrCl ~40 mL/min)
• Additional info: GIB – 2 months after starting warfarin (INR 2.3); reversed with PCC, hospitalized for 4 days
• Colonoscopy and upper endoscopy performed• Gastric ulcer with bleeding; treatment with epi and clips
• 2-week PCP follow up after hospitalization• Discussion of resumption and length of anticoagulation
Questions to ask?
Was the VTE provoked by a transient risk factor?
What is the patient’s bleeding risk?
What is the patient’s preference?
How significant was the event?
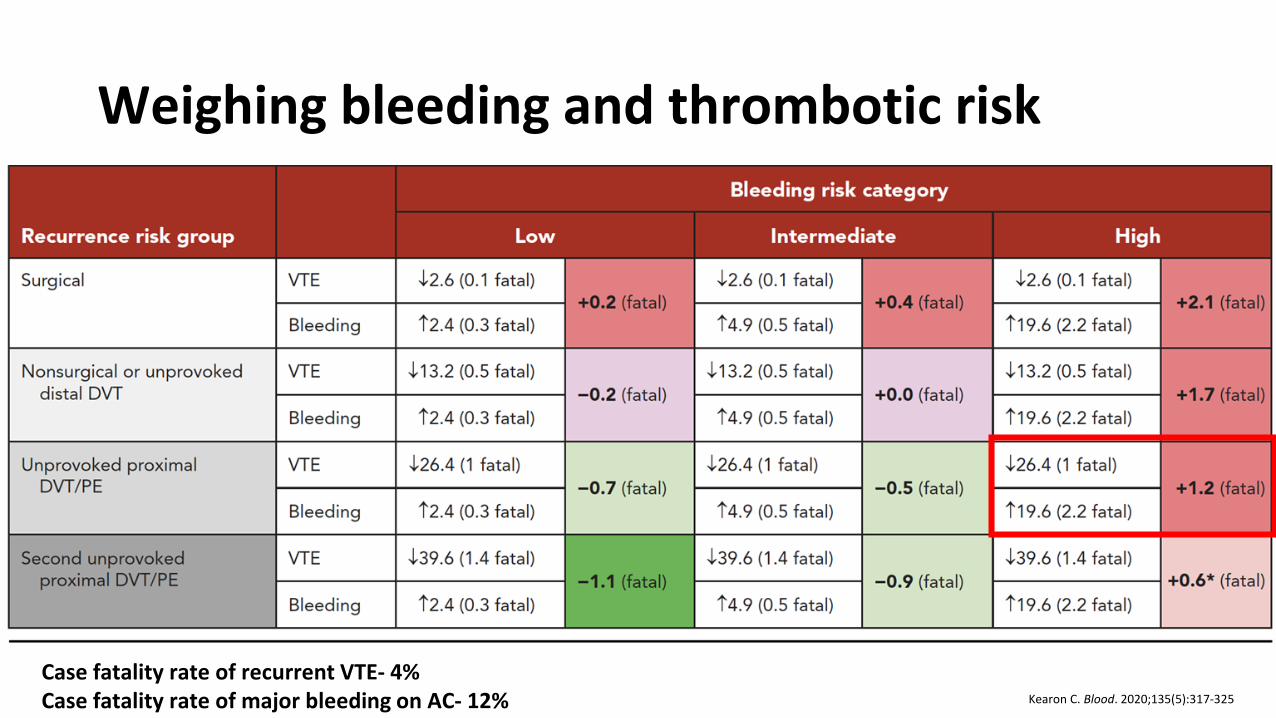
Weighing bleeding and thrombotic risk
Kearon C. Blood. 2020;135(5):317-325
Case fatality rate of recurrent VTE- 4%Case fatality rate of major bleeding on AC- 12%
Case 6 revisted. How Long To Treat?
• Transient risk factor: none identified
• Bleeding risk: high
• VTE: PE
• Patient preference: unsure, looking to PCP to decide
• Length of therapy: • At least 3 months• Consider stopping based on high bleeding risk• Consider low dose
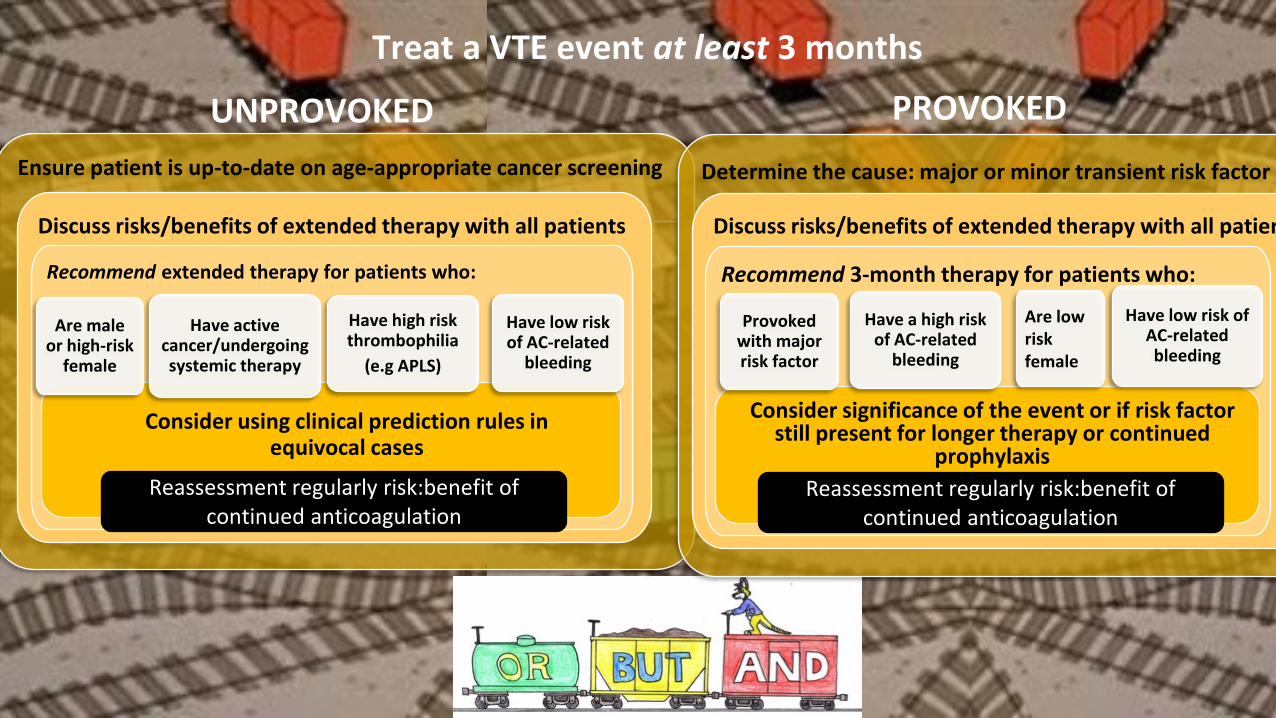
Ensure patient is up-to-date on age-appropriate cancer screening
Discuss risks/benefits of extended therapy with all patients
Recommend extended therapy for patients who:
Are male or high-risk
female
Have active cancer/undergoing systemic therapy
Have high risk thrombophilia
(e.g APLS)
Have low risk of AC-related
bleeding
Determine the cause: major or minor transient risk factor
Discuss risks/benefits of extended therapy with all patien
Recommend 3-month therapy for patients who:
Provoked with major risk factor
Have a high risk of AC-related
bleeding
Are low risk female
Have low risk of AC-related bleeding
Consider significance of the event or if risk factor still present for longer therapy or continued
prophylaxis Reassessment regularly risk:benefit of
continued anticoagulationReassessment regularly risk:benefit of
continued anticoagulation
Treat a VTE event at least 3 months
PROVOKEDUNPROVOKED
Consider using clinical prediction rules in equivocal cases
My Hero, Zero
• Take Home Points:• Risk for recurrent VTE and bleed will
never be 0%
• Regular reassessment of risk:benefit
• Special thanks to School House Rocks





























