Embed Size (px)
Citation preview

High-Dose Continuous Nebulized Levalbuterol for Pediatric StatusAsthmaticus: A Randomized Trial
Timothy Andrews, MD, Erin McGintee, MD, Manoj K. Mittal, MD, Lisa Tyler, RRT, Amber Chew, Xuemei Zhang, MS,
Nicholas Pawlowski, MD, and Joseph J. Zorc, MD
Objective To assess the use of high-dose continuous levalbuterol (LEV), the single active (R)-enantiomer of race-mic albuterol (RAC), in the treatment of status asthmaticus.Study design Children age 6 to 18 years with severe asthma exacerbation were enrolled in this randomized, dou-ble-blind trial if they failed initial emergency department (ED) therapy with RAC and systemic steroids. Subjects re-ceived equipotent doses of RAC (20 mg/hour) or LEV (10 mg/hour) within a standardized inpatient protocol. Bloodsamples for measurements of albuterol enantiomer, potassium, and glucose levels were obtained from the first 40subjects. The median time until discontinuation of continuous therapy was compared using the rank-sum test, andother outcomes were compared using general linear mixed models.Results A total of 81 subjects (40 in the RAC group and 41 in the LEV group) were enrolled; the 2 groups weresimilar at baseline. Both groups tolerated continuous therapy with similar changes in heart rate and serum potas-sium and glucose levels but higher serum (S)-albuterol concentrations in the subjects treated with RAC. The mediantime for continuous therapy was similar in the RAC and LEV groups (18.3 hours vs 16.0 hours), as were the otherclinical measures.Conclusions Substituting high-dose continuous LEV for RAC did not reduce the time on continuous therapy andhad similar adverse effects in children who had failed initial treatment with RAC. (J Pediatr 2009;155:205-10).
Asthma is a leading cause of health-related disability and hospitalization for children, and the prevalence of asthma hasincreased over recent decades.1 Costs related to asthma, a substantial proportion of which are associated with emergencyand inpatient care, also are increasing.2 Concerns about the increasing burden of hospital care for asthma have led to the
development of standardized treatment protocols using systemic corticosteroids and high-dose beta-agonists, such as albu-terol.3,4 Although standardization of care has led to reduced costs and lengths of stay, continued improvement in these pro-tocols is needed.5,6
In the past, albuterol was available as a racemic mixture of 2 enantiomers, (R)-albuterol and (S)-albuterol. Recently, a pu-rified form of (R)-albuterol, also known as levalbuterol (LEV), has become available commercially (Xopenex Inhalation Solu-tion; Sepracor, Marlborough, Massachusetts). (R)-albuterol binds the beta2-adrenergic receptors, producing the therapeuticbronchodilator effects of albuterol, along with such common adverse effects as tachycardia and tremor. The effects of (S)-albuterol remain controversial and were debated recently in 2 opposing editorials.7,8 In vitro studies suggest that (S)-albuterolincreases intracellular calcium, enhances airway hyperresponsiveness, and causes activation of eosinophils, all potentially det-rimental effects in acute asthma that may oppose the therapeutic effects of (R)-albuterol.9-11 Pharmacokinetic studies havefound that (S)-albuterol has a longer half-life than (R)-albuterol, resulting in accumulation of the (S) enantiomer after repeateddosing with the racemic mixture.12 Clinical studies assessing the effects of LEV and RAC on lung function in adults with stableasthma have yielded conflicting results. Some studies have demonstrated improved forced expiratory volume in 1 second(FEV1) from LEV compared with equivalent doses of RAC, suggesting that the presence of the S isomer may impair broncho-dilation;13,14 however, other studies have found no difference in lung functionbetween RAC and LEV.15,16 Data for acutely ill children are limited. Carlet al17 reported a reduced hospitalization rate after LEV was substituted forRAC in a clinical trial of ED treatment for asthma, but other investigators foundno difference in lung function or clinical score between the 2 treatments in other
See editorial, p 162
From The Children’s Hospital of Philadelphia,Philadelphia, PA and the Divisions of Allergy andImmunology (T.A., E.M., N.P.) and Pediatric EmergencyMedicine (M.M., A.C., J.Z.), Department of Pediatrics(L.T., X.Z.), University of Pennsylvania School ofMedicine, Philadelphia, PA
This investigator-initiated study was funded by an unre-stricted research grant from Sepracor Inc. The authorsdeclare no other affiliation, financial agreements, orinvolvement with this or any company that might beconsidered a conflict of interest.
ClinicalTrials.gov registration number: NCT00124176.
0022-3476/$ - see front matter. Copyright � 2009 Mosby Inc.
All rights reserved. 10.1016/j.jpeds.2009.01.073
ED Emergency department
FEV1 Forced expiratory volume in 1 second
LEV Levalbuterol
NAEPP National Asthma Education and Prevention Program
RAC Racemic albuterol
205

THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 155, No. 2
ED-based trials.18,19 No studies have compared LEV andRAC in high-dose continuous therapy, as is recommendedfor children hospitalized with severe status asthmaticus.4
The objective of the present study was to compare LEV andRAC in a group of children hospitalized for severe asthmawho were receiving high-dose continuous beta-agonist ther-apy after failing to respond to standard ED therapy.
Methods
This was a randomized, double-blind, controlled trial con-ducted at an urban academic children’s hospital. Our hospi-tal’s Institutional Review Board approved the study protocolbefore the start of enrollment. Research staff members werepresent in the ED from 8 a.m. to midnight each day to enrollpotential study participants. To be eligible for the study, a pa-tient had to be at least 6 (the age at which LEV is approved foruse) and less than 19 years of age and have a diagnosis ofasthma, defined as at least 2 previous visits at which a health-care provider had prescribed a beta-agonist to treat acutesymptoms. Eligible subjects were those who had been treatedin the ED with a standardized protocol based on NationalAsthma Education and Prevention Program (NAEPP) guide-lines, including, during the first hour, three 5-mg doses ofnebulized racemic albuterol, two 500-mg doses of ipra-tropium, and a 2-mg/kg dose (to a maximum of 60 mg) oforal prednisolone or parenteral methylprednisolone.4
After this initial therapy, each patient was assessed by anattending physician. Those who demonstrated continuedsymptoms of respiratory distress requiring continuous albu-terol therapy were eligible for enrollment. Continuous albu-terol is given in inpatient units according to an existingstandard protocol that includes hourly assessments by a respi-ratory therapist; approximately 40% of patients admitted toinpatient units receive continuous therapy. To avoid con-founding by additional therapies, patients were excluded ifthey had been started on intravenous beta-agonists or werebeing admitted to the intensive care unit, where treatmentbeyond the standard protocol is often given. Patients withother lung diseases (eg, cystic fibrosis), sickle cell disease, car-diac disease, pregnancy, or a history of allergy or other con-traindication to albuterol also were excluded. Each subjectwas enrolled in the study only once.
After informed consent was obtained, the patients wererandomized to receive either RAC 20 mg/hour or LEV 10mg/hour in a continuous nebulized formulation. Prenum-bered sequential syringes containing the dose for the first6 hours were prepared in advance by the research pharmacyusing a randomization sequence of blocks of 6. Subsequentblinded doses were delivered to the inpatient unit by the phar-macy. The patients’ care was directed by the inpatient asthmaprotocol. Progression through the pathway was determinedby standardized assessments by a trained respiratory thera-pist; severity was categorized as ‘‘severe,’’ ‘‘moderate,’’ or‘‘mild.’’ Patients assessed as ‘‘severe’’ on continuous albuteroltherapy received continuous cardiorespiratory monitoring
206
and pulse oximetry and were assessed hourly for improve-ment with vital signs and a standardized respiratory assess-ment including a clinical asthma score, which has beendemonstrated to have good interobserver agreement in previ-ous research.20 In patients with 2 consecutive hourly assess-ments of ‘‘moderate’’ severity, the beta-agonist dose wasreduced by half and hourly assessments were continued.Those with 2 subsequent ‘‘moderate’’ assessments were ad-vanced to intermittent albuterol, given every 2 hours. Thestudy medication ended after discontinuation of continuoustherapy, and further treatments with nebulized open-labelRAC were given as needed. During the inpatient phase ofthe study, patients received oral prednisone/prednisolone orintravenous methylprednisolone 1 mg/kg up to a maximumof 30 mg every 6 hours. Ipratropium was not part of the stan-dard order set for the protocol but could be ordered by the ad-mitting physician. The inpatient protocol called forcontinuation of home medications, such as inhaled cortico-steroids, during hospitalization.
Study Measurements and OutcomesResearch assistants interviewed the study subjects at the timeof enrollment with a standard history form that assessed de-mographics, asthma history and severity, and medicationuse. Clinical measurements were obtained from standardizedrespiratory flowsheets. The study’s primary endpoint was theduration of continuous albuterol therapy; secondary out-comes included spirometry and a clinical asthma score, thePediatric Asthma Severity Score (PASS), which has beenshown to have reliability, discrimination, and responsivenessat our institution.21,22 The PASS was recorded hourly duringcontinuous therapy as part of the respiratory assessment.Asthma severity is graded on a 6-point scale, summing indi-vidual assessment values (0, none/mild; 1, moderate; 2, se-vere) for each of 3 items: wheeze, prolonged expiration,and work of breathing. Spirometry was performed by respi-ratory therapists using a KoKoMate portable spirometer(nSpire Health, Inc., Longmont, Colorado) at baseline andevery 4 hours during continuous therapy. The best of 3 com-pleted attempts was included in the subject’s data. To assessthe quality of the data, each flow-volume loop was reviewedin a blinded fashion by 2 investigators with subspecialty
Table. Baseline characteristics of the RAC and LEVgroups
RAC (n = 40) LEV (n = 41)
Male, n (%) 26 (65%) 25 (61%)Age, mean, years (SD) 10.4 (3.5) 10.7 (3.3)Race, African American, n (%) 35 (88%) 40 (98%)Oxygen saturation, mean % (SD) 94.4% (3.6%) 94.5% (3.7%)Respiratory rate, mean per minute (SD) 33.3 (9.7) 34.0 (11.2)PASS, mean (SD) 1.8 (1.3) 2.3 (1.0)Previous hospitalization for asthma, n (%) 36 (90%) 36 (88%)Previous inhaled corticosteroid use, n (%) 28 (70%) 27 (66%)Albuterol treatments during 4 hours before
ED, mean (SD)1.0 (1.2) 1.1 (1.2)
Use of levalbuterol at home, n (%) 5 (13%) 2 (5%)
SD, standard deviation.
Andrews et al
August 2009 ORIGINAL ARTICLES
training in spirometry interpretation. Only measurementsfor which there was agreement about the adequacy of thetracing were used for the analysis. In the first 40 patients,an intravenous line was placed and blood samples weredrawn at enrollment and every 6 hours during continuoustherapy for measurement of serum (R)-albuterol, (S)-albu-terol, and glucose concentrations and every 12 hours formeasurement of serum potassium concentration. Any potas-sium values deemed to be hemolyzed or grossly hemolyzed bythe laboratory were excluded from analysis.
Statistical Methods and Data AnalysisThe 2 study groups were compared at baseline for demo-graphic and clinical factors using the c2 test, t-test, or non-parametric rank-sum test, depending on the type anddistribution of each variable. The primary outcome of dura-tion of continuous therapy was compared using a nonpara-metric rank-sum test. Secondary outcome variables werecompared using repeated analysis of variance. Linearmixed-effects models were used to examine changes overtime and to account for different follow-up times, measure-ment times, and within-subject correlation.
Initially, the study’s sample size was calculated to detecta reduction in time on continuous therapy of 4 hours. Butthe Data and Safety Monitoring Board’s review of the proto-col determined that a 4-hour difference was not clinically sig-nificant; subsequently, the sample size was recalculated at 80subjects to detect a 6-hour difference between the groupsbased on pilot data estimating a mean duration of 14 hourswith a standard deviation of 8 hours (assuming 80% powerand using a 2-tailed test with a = 0.05). At the request ofthe Institutional Review Board, an interim analysis of safetydata only (vital signs and serum potassium and glucose)was conducted after 40 subjects were enrolled.
Results
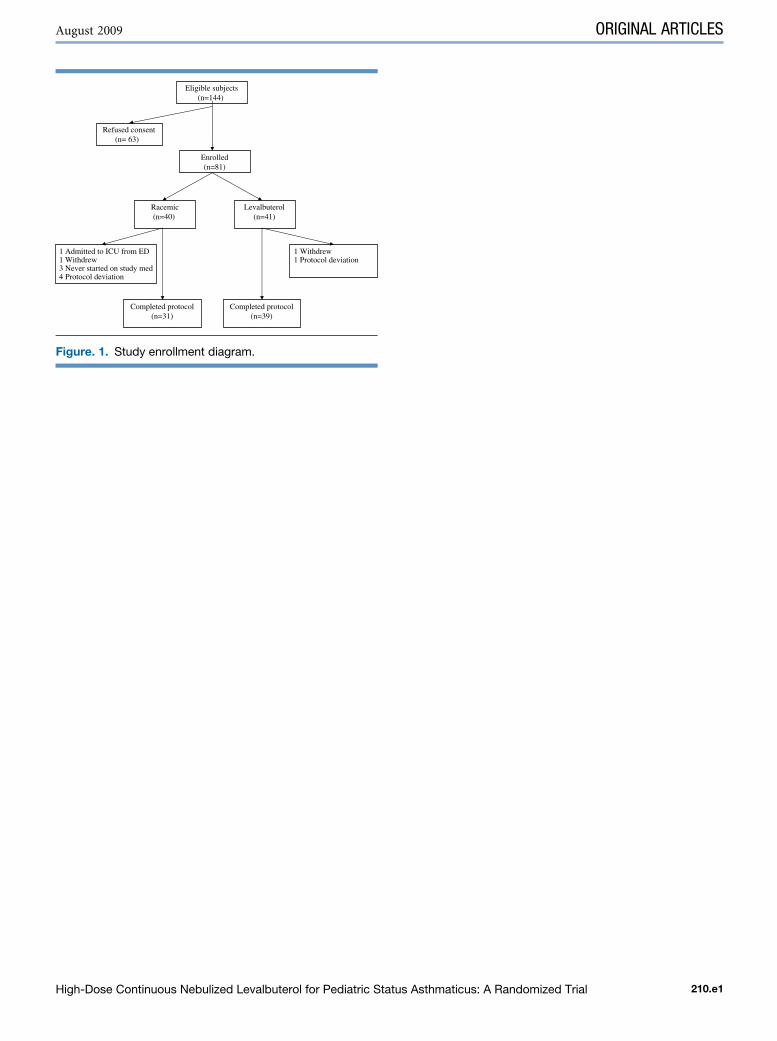
Between April 2004 and February 2006, 143 eligible subjectswere approached for enrollment in the study. Of these, 81provided informed consent and were randomized, 40 toRAC and 41 to LEV (Figure 1; available at www.jpeds.com).Several deviations from the planned protocol were recordedand accounted for in our data analysis. Of the 81 randomizedsubjects, 3 (all in the RAC group) never started on the studymedication, due to clinical improvement before the initiationof continuous albuterol. One subject, also in the RAC group,worsened and was withdrawn from the protocol due to thedecision to admit to the intensive care unit and treat with in-travenous terbutaline and open-label continuous RAC. Onesubject in each group withdrew from the study treatmentshortly after enrollment; the subject in the LEV group with-drew because of vomiting and was subsequently treated withintermittent albuterol, and the subject in the RAC group wascontinued on open-label RAC. Three subjects (1 in the LEVgroup and 2 in the RAC group) were switched to open-labelalbuterol during the study because of an inability to obtain
High-Dose Continuous Nebulized Levalbuterol for Pediatric Sta
the study medication. One subject in the RAC group receivedthe study medication at a diluted concentration for 6 hoursat the end of the first day of treatment before discontinuationof continuous therapy. One subject in the RAC groupreceived LEV after the first 6 hours due to a pharmacy error.These subjects were included in their assigned group forintention-to-treat analysis. A subanalysis of subjects who suc-cessfully completed the protocol found similar results and isnot presented here.
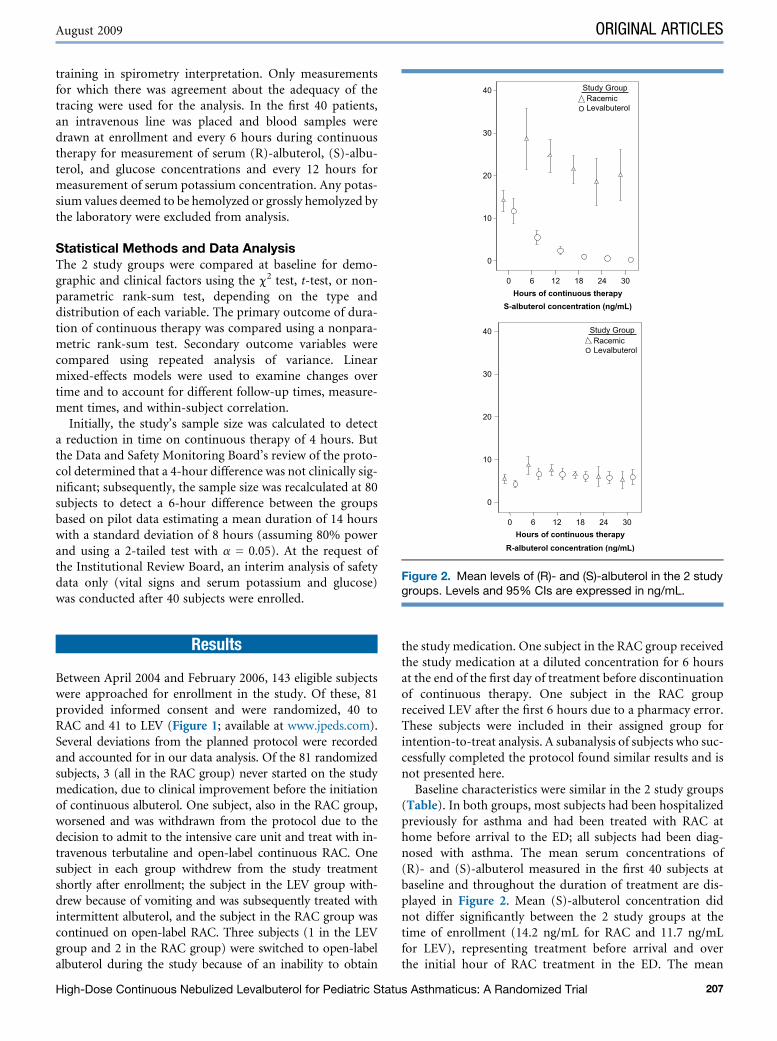
Baseline characteristics were similar in the 2 study groups(Table). In both groups, most subjects had been hospitalizedpreviously for asthma and had been treated with RAC athome before arrival to the ED; all subjects had been diag-nosed with asthma. The mean serum concentrations of(R)- and (S)-albuterol measured in the first 40 subjects atbaseline and throughout the duration of treatment are dis-played in Figure 2. Mean (S)-albuterol concentration didnot differ significantly between the 2 study groups at thetime of enrollment (14.2 ng/mL for RAC and 11.7 ng/mLfor LEV), representing treatment before arrival and overthe initial hour of RAC treatment in the ED. The mean
0 6 12 18 24 30Hours of continuous therapy
0
10
20
30
40
0 6 12 18 24 30Hours of continuous therapy
0
10
20
30
40
S-albuterol concentration (ng/mL)
R-albuterol concentration (ng/mL)
Study GroupRacemicLevalbuterol
Study GroupRacemic
O
O
Levalbuterol
Figure 2. Mean levels of (R)- and (S)-albuterol in the 2 studygroups. Levels and 95% CIs are expressed in ng/mL.
tus Asthmaticus: A Randomized Trial 207
THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 155, No. 2
(S)-albuterol concentration rose to 28.6 ng/mL at 6 hours inthe RAC group, compared with 5.5 ng/mL in the LEV group(P < .001); (S)-albuterol concentration continued to differbetween the 2 groups at each subsequent time point.
Additional therapies administered were similar in the 2study groups. Ipratropium was administered to 44% of thestudy subjects overall during continuous therapy (38% ofthe RAC group and 49% of the LEV group). Some 90% ofthe subjects remained on intermittent therapy after discon-tinuation of continuous albuterol therapy, while 9 patients(6 in the RAC group and 3 in the LEV group) were restartedon continuous therapy during hospitalization in response toa worsening respiratory assessment.
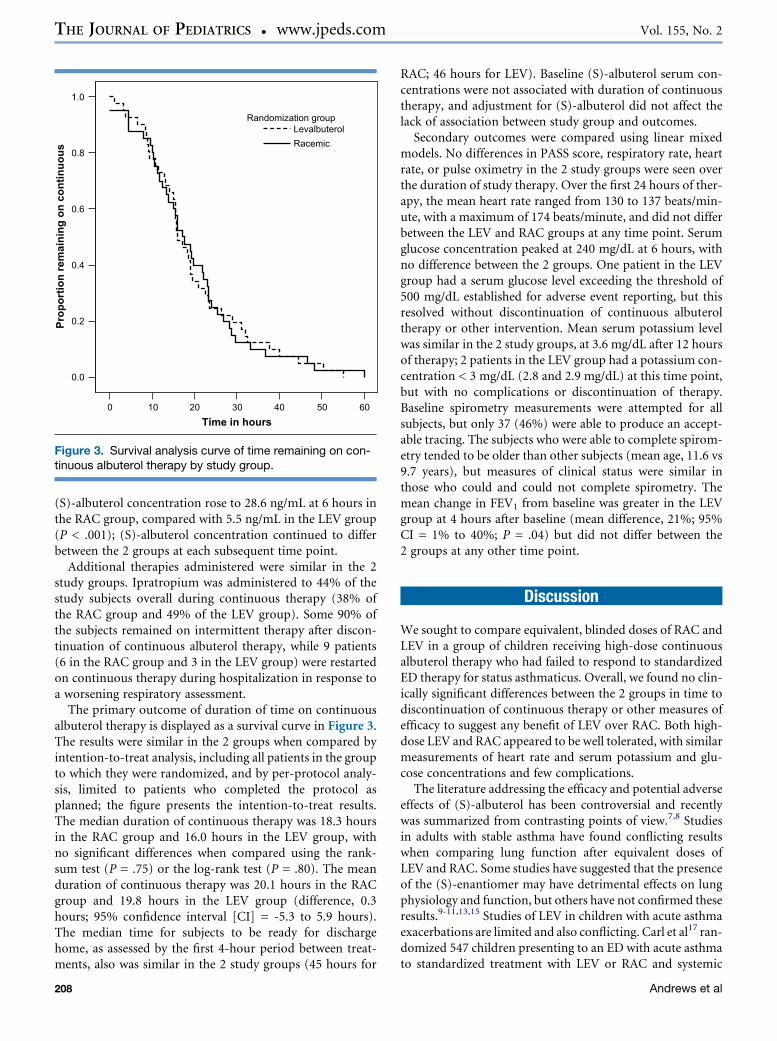
The primary outcome of duration of time on continuousalbuterol therapy is displayed as a survival curve in Figure 3.The results were similar in the 2 groups when compared byintention-to-treat analysis, including all patients in the groupto which they were randomized, and by per-protocol analy-sis, limited to patients who completed the protocol asplanned; the figure presents the intention-to-treat results.The median duration of continuous therapy was 18.3 hoursin the RAC group and 16.0 hours in the LEV group, withno significant differences when compared using the rank-sum test (P = .75) or the log-rank test (P = .80). The meanduration of continuous therapy was 20.1 hours in the RACgroup and 19.8 hours in the LEV group (difference, 0.3hours; 95% confidence interval [CI] = -5.3 to 5.9 hours).The median time for subjects to be ready for dischargehome, as assessed by the first 4-hour period between treat-ments, also was similar in the 2 study groups (45 hours for
0 10 20 30 40 50 60Time in hours
0.0
0.2
0.4
0.6
0.8
1.0
Pro
po
rtio
n rem
ain
in
g o
n co
ntin
uo
us
Randomization groupLevalbuterolRacemic
Figure 3. Survival analysis curve of time remaining on con-tinuous albuterol therapy by study group.
208
RAC; 46 hours for LEV). Baseline (S)-albuterol serum con-centrations were not associated with duration of continuoustherapy, and adjustment for (S)-albuterol did not affect thelack of association between study group and outcomes.
Secondary outcomes were compared using linear mixedmodels. No differences in PASS score, respiratory rate, heartrate, or pulse oximetry in the 2 study groups were seen overthe duration of study therapy. Over the first 24 hours of ther-apy, the mean heart rate ranged from 130 to 137 beats/min-ute, with a maximum of 174 beats/minute, and did not differbetween the LEV and RAC groups at any time point. Serumglucose concentration peaked at 240 mg/dL at 6 hours, withno difference between the 2 groups. One patient in the LEVgroup had a serum glucose level exceeding the threshold of500 mg/dL established for adverse event reporting, but thisresolved without discontinuation of continuous albuteroltherapy or other intervention. Mean serum potassium levelwas similar in the 2 study groups, at 3.6 mg/dL after 12 hoursof therapy; 2 patients in the LEV group had a potassium con-centration < 3 mg/dL (2.8 and 2.9 mg/dL) at this time point,but with no complications or discontinuation of therapy.Baseline spirometry measurements were attempted for allsubjects, but only 37 (46%) were able to produce an accept-able tracing. The subjects who were able to complete spirom-etry tended to be older than other subjects (mean age, 11.6 vs9.7 years), but measures of clinical status were similar inthose who could and could not complete spirometry. Themean change in FEV1 from baseline was greater in the LEVgroup at 4 hours after baseline (mean difference, 21%; 95%CI = 1% to 40%; P = .04) but did not differ between the2 groups at any other time point.
Discussion
We sought to compare equivalent, blinded doses of RAC andLEV in a group of children receiving high-dose continuousalbuterol therapy who had failed to respond to standardizedED therapy for status asthmaticus. Overall, we found no clin-ically significant differences between the 2 groups in time todiscontinuation of continuous therapy or other measures ofefficacy to suggest any benefit of LEV over RAC. Both high-dose LEV and RAC appeared to be well tolerated, with similarmeasurements of heart rate and serum potassium and glu-cose concentrations and few complications.
The literature addressing the efficacy and potential adverseeffects of (S)-albuterol has been controversial and recentlywas summarized from contrasting points of view.7,8 Studiesin adults with stable asthma have found conflicting resultswhen comparing lung function after equivalent doses ofLEV and RAC. Some studies have suggested that the presenceof the (S)-enantiomer may have detrimental effects on lungphysiology and function, but others have not confirmed theseresults.9-11,13,15 Studies of LEV in children with acute asthmaexacerbations are limited and also conflicting. Carl et al17 ran-domized 547 children presenting to an ED with acute asthmato standardized treatment with LEV or RAC and systemic
Andrews et al

August 2009 ORIGINAL ARTICLES
corticosteroids. The children in the LEV group had a lowerrate of hospitalization (36% vs 45%), suggesting a benefit ofsingle enantiomer treatment. But Qureshi et al18 studieda similar group of 129 pediatric ED patients and found no im-provement in clinical asthma score or spirometry in the LEVgroup; the study was not powered to measure a difference inhospitalization rate. In addition to the difference in outcomemeasures, those 2 studies used different doses (RAC 5 mg inolder children in the study of Qureshi et al vs 2.5 mg in thestudy of Carl et al), which may account for the differences ob-served. We are unaware of any previous systematic reviews ormeta-analyses that have attempted to reconcile the availabledata or to conduct a cost-benefit assessment to assess thepotential cost differences due to the higher cost of nebulizedLEV compared with RAC.
Likewise, no previous study has prospectively studiedhigh-dose continuous LEV therapy in children. Expert panelguidelines for asthma published by the National Heart, Lungand Blood Institute recommend initiating continuous albu-terol for patients with poor response to ED therapy andnote the absence of data for high-dose continuous LEV.4
Our results expand the data regarding the use of LEV in treat-ing pediatric status asthmaticus.
We found no clinically significant difference in the dura-tion of continuous therapy or other clinical outcomes inthe children treated with LEV and those treated with RAC.Several limitations of our study should be considered whenapplying our findings to the clinical setting, however. First,all of the patients in our study failed initial treatment withRAC and thus had an elevated baseline serum (S)-albuterolconcentration measured at enrollment. We designed ourprotocol in this manner because most patients respond tostandard albuterol therapy, and we would have needed to en-roll many more patients on arrival to obtain a sample of thissize that required continuous therapy. In addition, we soughtto select a group of patients who had failed to respond toRAC therapy hypothetically due to an accumulation of (S)-albuterol. We reasoned that these patients might be mostlikely to benefit from substitution with LEV. Previous re-search in adults has suggested that (S)-albuterol concentra-tions may be related to response to LEV;23 however, wefound no difference after adjusting for (S)-albuterol mea-surements. But if (S)-albuterol has detrimental physiologicaleffects on the airway, these effects possibly may have alreadybegun during treatment before the ED visit, during initial EDtherapy, and during the hours it took for the level to fall. Wealso chose to use doses of LEV and RAC containing the sameamount of the (R) isomer, to ensure that these severely ill pa-tients received adequate doses of the active enantiomer. It ispossible that lower doses of LEV (or RAC) might be as effec-tive, with fewer adverse effects. Further study of LEV initiatedearlier in treatment of severe asthma and at other doseswould help clarify these issues.
Our study was a convenience sample conducted in a singlecenter with a single approach to asthma therapy and thusmay not be widely generalizable. We studied only patientswith asthma of sufficient severity to merit continuous bron-
High-Dose Continuous Nebulized Levalbuterol for Pediatric Sta
chodilator therapy (about 40% of the admitted patients atour institution). Evidence supporting continuous versus in-termittent albuterol is limited, and further research could ex-plore the intermittent use of RAC and LEV.24 Although ourprotocol is standardized and based on national asthma guide-lines, different results may be found using other measures ofimproved asthma severity. We supplemented our clinical as-sessment with spirometry to increase objectivity, but foundthat only some of these very ill children were able to performspirometry, as reported previously.25 We chose to exclude themost severely asthmatic patients, because many receive addi-tional therapies in the intensive care unit that would bedifficult to control. Concurrent conditions, such as pneumo-nia, were not systematically assessed, and may have differedbetween the 2 study groups. Finally, other agents, such asipratropium, were prescribed for a subset of patients enrolledin our study; however, the rate of ipratropium use was similarin the 2 study groups, and the recent NAEPP guidelines statethat ipratropium is not effective in hospitalized patients withasthma. Thus, this is unlikely to act as a confounder.4
In conclusion, we found no benefit of substituting contin-uous high-dose LEV for RAC in a group of children who hadfailed initial therapy for severe asthma with RAC. Future stud-ies should assess initial therapy with LEV in severe asthma andexplore other therapies for pediatric status asthmaticus. n
Submitted for publication June 25, 2008; last revision received Dec 16, 2008;
accepted Jan 30, 2009.
Reprint requests: Joseph J. Zorc, MD, Division of Emergency Medicine,
Children’s Hospital of Philadelphia, 34th Street and Civic Center Boulevard,
Philadelphia, PA 19104-4399. E-mail: [email protected].
References
1. Mannino DM, Homa DM, Pertowski CA, Ashizawa A, Nixon LL,
Johnson CA, et al. Surveillance for asthma–United States, 1960-1995.
MMWR CDC Surveill Summ 1998;47:1-27.
2. Weiss KB, Sullivan SD, Lyttle CS. Trends in the cost of illness for asthma
in the United States, 1985-1994. J Allergy Clin Immunol 2000;106:493-9.
3. Schuh S, Reider MJ, Canny G, Pender E, Forbes T, Tan YK, et al. Neb-
ulized albuterol in acute childhood asthma: comparison of two doses.
Pediatrics 1990;86:509-13.
4. National Asthma Education and Prevention Program. Expert Panel
Report 3: Guidelines for the Diagnosis and Management of Asthma.
Bethesda, MD: National Institutes of Health; 2007.
5. Johnson KB, Blaisdell CJ, Walker A, Eggleston P. Effectiveness of a clin-
ical pathway for inpatient asthma management. Pediatrics 2000;106:
1006-12.
6. McDowell KM, Chatburn RL, Myers TR, O’Riordan MA, Kercsmar CM.
A cost-saving algorithm for children hospitalized for status asthmaticus.
Arch Pediatr Adolesc Med 1998;152:977-84.
7. Ameredes BT, Calhoun WJ. (R)-albuterol for asthma: pro [a.k.a. (S)-
albuterol for asthma: con]. Am J Respir Crit Care Med 2006;174:965-9.
8. Barnes PJ. Treatment with (R)-albuterol has no advantage over racemic
albuterol. Am J Respir Crit Care Med 2006;174:969-72.
9. Handley D. The asthma-like pharmacology and toxicology of (S)-iso-
mers of beta agonists. J Allergy Clin Immunol 1999;104:S69-76.
10. Mitra S, Ugur M, Ugur O, Goodman HM, McCullough JR,
Yamaguchi H. (S)-albuterol increases intracellular free calcium by mus-
carinic receptor activation and a phospholipase C-dependent mecha-
nism in airway smooth muscle. Mol Pharmacol 1998;53:347-54.
tus Asthmaticus: A Randomized Trial 209

THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 155, No. 2
11. Volcheck GW, Kelkar P, Bartemes KR, Gleich GJ, Kita H. Effects of (R)-
and (S)-isomers of beta-adrenergic agonists on eosinophil response to
interleukin-5. Clin Exp Allergy 2005;35:1341-6.
12. Gumbhir-Shah K, Kellerman DJ, DeGraw S, Koch P, Jusko WJ. Pharma-
cokinetics and pharmacodynamics of cumulative single doses of inhaled
salbutamol enantiomers in asthmatic subjects. Pulm Pharmacol Ther
1999;12:353-62.
13. Nelson HS, Bensch G, Pleskow WW, DiSantostefano R, DeGraw S,
Reasner DS, et al. Improved bronchodilation with levalbuterol com-
pared with racemic albuterol in patients with asthma. J Allergy Clin
Immunol 1998;102:943-52.
14. Milgrom H, Skoner DP, Bensch G, Kim KT, Claus R, Baumgartner RA.
Low-dose levalbuterol in children with asthma: safety and efficacy in
comparison with placebo and racemic albuterol. J Allergy Clin Immunol
2001;108:938-45.
15. Lotvall J, Palmqvist M, Arvidsson P, Maloney A, Ventresca GP, Ward J.
The therapeutic ratio of R-albuterol is comparable with that of R(S)-al-
buterol in asthmatic patients. J Allergy Clin Immunol 2001;108:726-31.
16. Berger WE, Milgrom H, Skoner DP, Tripp K, Parsey MV,
Baumgartner RA. Evaluation of levalbuterol metered dose inhaler in pe-
diatric patients with asthma: a double-blind, randomized, placebo- and
active-controlled trial. Curr Med Res Opin 2006;22:1217-26.
17. Carl JC, Myers TR, Kirchner HL, Kercsmar CM. Comparison of racemic
albuterol and levalbuterol for treatment of acute asthma. J Pediatr 2003;
143:731-6.
210
18. Qureshi F, Zaritsky A, Welch C, Meadows T, Burke BL. Clinical efficacy
of racemic albuterol versus levalbuterol for the treatment of acute pedi-
atric asthma. Ann Emerg Med 2005;46:29-36.
19. Hardasmalani MD, DeBari V, Bithoney WG, Gold N. Levalbuterol ver-
sus racemic albuterol in the treatment of acute exacerbation of asthma in
children. Pediatr Emerg Care 2005;21:415-9.
20. Stevens MW, Gorelick MH, Schultz T. Interrater agreement in the
clinical evaluation of acute pediatric asthma. J Asthma 2003;40:
311-5.
21. Gorelick MH, Stevens MW, Schultz TR, Scribano PV. Performance of
a novel clinical score, the Pediatric Asthma Severity Score (PASS), in
the evaluation of acute asthma. Acad Emerg Med 2004;11:10-8.
22. Gorelick MH, Stevens MW, Schultz TR. Comparability of acute asthma
severity assessments by parents and respiratory therapists. Arch Pediatr
Adolesc Med 2002;156:1199-202.
23. Nowak R, Emerman C, Hanrahan JP, Parsey MV, Hanania NA, Claus R,
et al. A comparison of levalbuterol with racemic albuterol in the treat-
ment of acute severe asthma exacerbations in adults. Am J Emerg Med
2006;24:259-67.
24. Camargo CA Jr., Spooner CH, Rowe BH. Continuous versus intermit-
tent beta-agonists for acute asthma. Cochrane Database Syst Rev 2003;
4:CD001115.
25. Gorelick MH, Stevens MW, Schultz T, Scribano PV. Difficulty in obtain-
ing peak expiratory flow measurements in children with acute asthma.
Pediatr Emerg Care 2004;20:22-6.
Andrews et al
August 2009 ORIGINAL ARTICLES
Refused consent(n= 63)
Enrolled(n=81)
Racemic(n=40)
Levalbuterol(n=41)
Completed protocol(n=31)
Completed protocol(n=39)
1 Withdrew 1 Protocol deviation
1 Admitted to ICU from ED 1 Withdrew 3 Never started on study med 4 Protocol deviation
Eligible subjects(n=144)
Figure. 1. Study enrollment diagram.
High-Dose Continuous Nebulized Levalbuterol for Pediatric Status Asthmaticus: A Randomized Trial 210.e1

















![Status asthmaticus - pdfs.semanticscholar.org · Status asthmaticus influenced by reduced exposure to stimuli and by regular effective treatment [8]. C currently pathologists have](https://img.pdfslide.us/doc/110x75/5e0e2e4f584564357a38ccc6/status-asthmaticus-pdfs-status-asthmaticus-influenced-by-reduced-exposure-to.jpg)