Embed Size (px)
Citation preview

High-Dose Chemotherapy Followed by Peripheral Blood Stem Cell Rescue forMetastatic Rhabdomyosarcoma: The Experience at Chicago Children’s
Memorial Hospital
David O. Walterhouse, MD,1* Margo L. Hoover, MD,2
Mary Anne H. Marymont, MD,3 and Morris Kletzel, MD1
Background. Because outcome for meta-static rhabdomyosarcoma remains poor withstandard therapy, and because some patientswith extensive unresectable metastatic rhabdo-myosarcoma are unable to tolerate standardtherapy with the associated large radiationfields, peripheral blood stem cell rescue (PB-SCR) following high-dose chemotherapy wasoffered as consolidative therapy for patientswith Stage 4/Group IV rhabdomyosarcoma. Pa-tients and Methods. Eight patients with Stage4/Group IV rhabdomyosarcoma were diag-nosed from May, 1992, through November,1994. Consolidative PBSCR following thiotepa300 mg/M2 on days −7, −6, and −5; cyclophos-phamide 1,500 mg/M2 on days −5, −4, −3, and−2; and carboplatin 600 mg/M2 on days −3 and−2 was offered to those patients who achieveda complete remission with multimodalitytherapy. Patients with extensive metastatic dis-ease who did not receive full doses of radiation
to all sites of disease remained eligible for high-dose chemotherapy and PBSCR. Results. Fiveof eight patients achieved a complete response.Four patients underwent PBSCR. One of thefour patients is alive without evidence of dis-ease 53 months post-PBSCR. All other patientsdied of progressive disease. Conclusions. Theseresults, along with the existing literature, showno advantage of high-dose chemotherapy fol-lowed by PBSCR as consolidative therapy forpatients with Stage 4/Group IV rhabdomyosar-coma over standard dose chemotherapy, radia-tion, and surgery. For patients with extensive,unresectable disease at diagnosis who cannotreceive radiation to all areas of disease basedon concerns of marrow reserve, high-dose che-motherapy followed by PBSCR does not appearto provide adequate local control and cannotbe offered as curative therapy. Med. Pediatr.Oncol. 32:88–92, 1999. © 1999 Wiley-Liss, Inc.
Key words: metastatic rhabdomyosarcoma; radiation therapy; stem cell rescue;transplantation
The outcome of patients with Stage 4/Group IV rhab-domyosarcoma remains poor. The first, second, and thirdIntergroup Rhabdomyosarcoma Studies (IRS) report5-year, progression-free survival rates of 20%, 23%, and27–30%, respectively for Group IV patients despite in-tensification of chemotherapy and the addition of newagents [1–3]. The outcome for patients with bone marrowmetastases at diagnosis or metastases to more than oneanatomic region or tissue appears to be particularly poor[4–6]. Despite the poor ultimate outcome, over one-halfof all patients with Group IV rhabdomyosarcoma at-tained complete responses to multimodality therapy inIRS-II and IRS-III, suggesting that new therapeutic strat-egies to consolidate more effectively the remissions thatare achieved might be beneficial [2,3].
Horowitz et al. used autologous bone marrow trans-plant as consolidation therapy in 65 patients with high-risk localized or metastatic sarcoma, including 25 pa-tients with rhabdomyosarcoma [7]. Patients achieving acomplete response to induction chemotherapy, radiationtherapy, and surgery, received 8 gray (Gy) total bodyirradiation (TBI) followed by vincristine, doxorubicin,
and cyclophosphamide in preparation for autologousbone marrow transplant. A 6-year, event-free survivalrate of 14% was reported for patients with metastaticdisease. It was concluded that consolidation therapy us-ing this preparative regimen for autologous bone marrowtransplant failed to improve the outcome for this group ofpatients. Pinkerton et al. reported consolidation withhigh-dose melphalan followed by autologous bone mar-row transplant for 36 patients with rhabdomyosarcoma,12 of whom were metastatic [8]. Progression-free sur-
1Department of Pediatrics, Division of Hematology/Oncology, North-western University Medical School, Children’s Memorial Hospital,Chicago, Illinois2Pediatric Hematology/Oncology, Children’s Hospital of OrangeCounty, Orange, California3Division of Radiation Oncology, Northwestern University MedicalSchool; Children’s Memorial Hospital, Chicago, Illinois
*Correspondence to: David Walterhouse, Division of Hematology/Oncology, Children’s Memorial Hospital, Box 30, 2300 Children’sPlaza, Chicago, IL 60614. E-mail: [email protected]
Received 12 February 1998; Accepted 27 August 1998
Medical and Pediatric Oncology 32:88–92 (1999)
© 1999 Wiley-Liss, Inc.

vival was reported at only 20% for Group IV patients.Koscielniak et al., after a retrospective review, concludedthat high-dose chemotherapy followed by hematopoieticrescue is still of uncertain value in the therapy of poor-risk rhabdomyosarcoma and should be performed only aspart of controlled clinical trials [9]. In their series, 5 of 27patients (18.5%) with primary metastatic rhabdomyosar-coma were without evidence of disease, with a medianfollow-up of 57 months from diagnosis and 27 monthsfrom high-dose chemotherapy and hematopoietic rescue.
From May, 1992, through November, 1994, eight pa-tients with Stage 4/Group IV rhabdomyosarcoma werediagnosed at Children’s Memorial Hospital. Interest inusing peripheral blood stem cell rescue (PBSCR) follow-ing high-dose chemotherapy as consolidation therapy forthese patients arose from the fact that some of thesepatients would be unable to tolerate and receive standardmultimodality therapy because of extensive disease at thetime of diagnosis, prohibiting delivery of adequate radia-tion therapy to all areas of unresectable disease. PBSCRwas proposed as an alternative treatment approach forthese patients. In addition, based on their poor prognosisusing standard therapy, Stage 4/Group IV patients whowere able to receive standard radiation therapy withinIRS guidelines to all areas of unresectable disease alsowere offered PBSCR following high-dose chemotherapy.Consolidative PBSCR following thiotepa, cyclophospha-mide, and carboplatin was offered to those patients whoachieved a complete remission. This report summarizesthis prospective, single-institution experience.
PATIENTS AND METHODS
Eight consecutive Stage 4/Group IV patients diag-nosed with rhabdomyosarcoma from May, 1992, throughNovember, 1994, at Children’s Memorial Hospital weretreated with the intent of PBSCR if complete remissioncould be achieved with multimodality therapy (Table I).The patients ranged in age from 3 years to 17 years.There were three males and five females. Histologic clas-sification was alveolar in four cases, embryonal in threecases, and undifferentiated in one case. Primary sites
included the orbit, nasopharynx, pterygopalatine fossa,lower extremity, pelvis, and uterus; two patients had un-known primary tumors with widely disseminated disease.Metastatic sites included the lungs, lymph nodes, bonemarrow, bone, liver, and serosal surfaces. The indicationfor high-dose chemotherapy followed by PBSCR wasprimary metastatic rhabdomyosarcoma or undifferenti-ated sarcoma in all cases. None of the patients undergo-ing high-dose chemotherapy followed by PBSCR hadrecurrent or progressive disease.
Two primary tumors were resected completely, onewas surgically debulked, and five were biopsied (TableII). One patient (patient 3) had a complete resection ofhis primary tumor and did not receive radiation to theprimary site. A second patient (patient 5) had a completeresection of a uterine primary; however, because of se-rosal seeding in the pelvis, this patient received 4,140-centigray (cGy) pelvic radiation. The remaining four pa-tients with known primary sites (patients 2, 4, 7, and 8)received radiation therapy within IRS-IV guidelines tothe primary sites. In addition, five patients (patients 1, 2,3, 5, and 8) received radiation therapy within IRS-IVguidelines to all metastatic sites. At the discretion of thetreating radiation oncologist (M.H.M.), three patients didnot receive full doses of radiation therapy to all sites ofmetastatic disease, because the protocol-specified radia-tion fields were felt to be too extensive to tolerate (pa-tients 4, 6, and 7). These patients remained eligible forhigh-dose chemotherapy and PBSCR. Two of the pa-tients (patients 2 and 5) received initial chemotherapy onthe IRS-IV protocol with vincristine and melphalan fol-lowed by vincristine, dactinomycin, and cyclophospha-mide, but they were removed from the IRS study withprogressive disease. Both patients were then treated withalternative chemotherapy in an attempt to achieve a com-plete response. Neither of these patients achieved a com-plete response to become eligible for high-dose chemo-therapy followed by PBSCR. One patient (patient 8) re-ceived induction chemotherapy on the IRS-IV protocol;however, the patient achieved only a partial response andwas not eligible for high-dose chemotherapy followed byPBSCR. Two patients (patients 6 and 7) received their
TABLE I. Stage 4/Group IV Patient Characteristics
Patient no. Age (years) Sex Histology Primary site Metastatic sites
1 17 F Alveolar Unknown Cervical, mediastinal, retroperitoneal nodes; pleuraland pericardial effusions
2 14 M Undifferentiated Pterygopalatine fossa Lungs3 3 M Alveolar Soleus Bone marrow, vertebral bodies4 14 F Alveolar Orbit Bone marrow, regional nodes, vertebral bodies5 17 F Alveolar Uterus Bone marrow, ribs, vertebral bodies6 13 F Alveolar Unknown Ascites, bone, liver, mediastinum, pleural
effusions, porta hepatis7 14 F Embryonal Pelvis Liver, lungs, serosal implants8 8 M Embryonal Nasopharynx Lungs, lymph nodes
Stem Cell Rescue for Rhabdomyosarcoma 89
initial chemotherapy on the IRS protocol for Stage 4patients with either vincristine and melphalan (patient 6)or etoposide and ifosfamide (patient 7), but they wereremoved from the IRS study, because the treating radia-tion oncologist (M.H.M.) felt that the protocol-specifiedradiation fields were too extensive to tolerate. Two pa-tients (patients 1 and 4) received induction therapy withvincristine, dactinomycin, and cyclophosphamide, andone patient (patient 3) received initial induction therapyon the IRS study but was removed from study by choiceof the treating physician and received ongoing inductiontherapy with vincristine, doxorubicin, and cyclophospha-mide.
Peripheral blood stem cells were harvested through adouble-lumen central line by continuous interface leu-kopheresis using the Cobe Spectra pheresis machine(Cobe, Denver, CO). A mean of 3.4 × 108 mononuclearcells (MNC)/kg (range 1.5–7.6 × 108 MNC/kg) werecollected per patient. Mobilization consisted of tumor-specific chemotherapy followed by granulocyte-colonystimulating factor (G-CSF) 5–10mg/kg. Pheresis wasundertaken at the time of white cell recovery. The pa-tients underwent a mean of 3.5 phereses (range 3–4).After collection, the pheresed cells were cryopreservedwith 10% dimethyl sulfoxide in a controlled-rate freezer
at 1°C/minute to −70°C and were then placed in liquid-nitrogen storage. Molecular studies were not used toidentify the t(2;13)(q35;q14) in the pheresed cells of thepatients with alveolar histology. For patients whoachieved a complete response, ablation therapy consistedof thiotepa 300 mg/M2 on days −7, −6, −5; cyclophos-phamide 1,500 mg/M2 on days −5, −4, −3, −2; and car-boplatin 600 mg/M2 on days −3 and −2. This was fol-lowed by unpurged PBSCR at a dose of 2.4–5.2 × 108
cells/kg. The protocol was approved by the Children’sMemorial Institutional Review Board, and written, in-formed consent was obtained for each patient. Patientswere supported according to institutional guidelines, in-cluding G-CSF 5mg/kg beginning on day 7 post-PBSCR,fluconazole prophylaxis, broad-spectrum antibiotics forfever, parenteral nutrition, and blood product support.Patients were maintained in High Efficiency Particle Air-filtration (HEPA) filter-positive pressure rooms.
RESULTS
Two patients demonstrated progressive disease duringinduction therapy and died of progressive disease 12months (patient 5) and 15 months (patient 2) from diag-nosis. One patient achieved a partial response, clearing
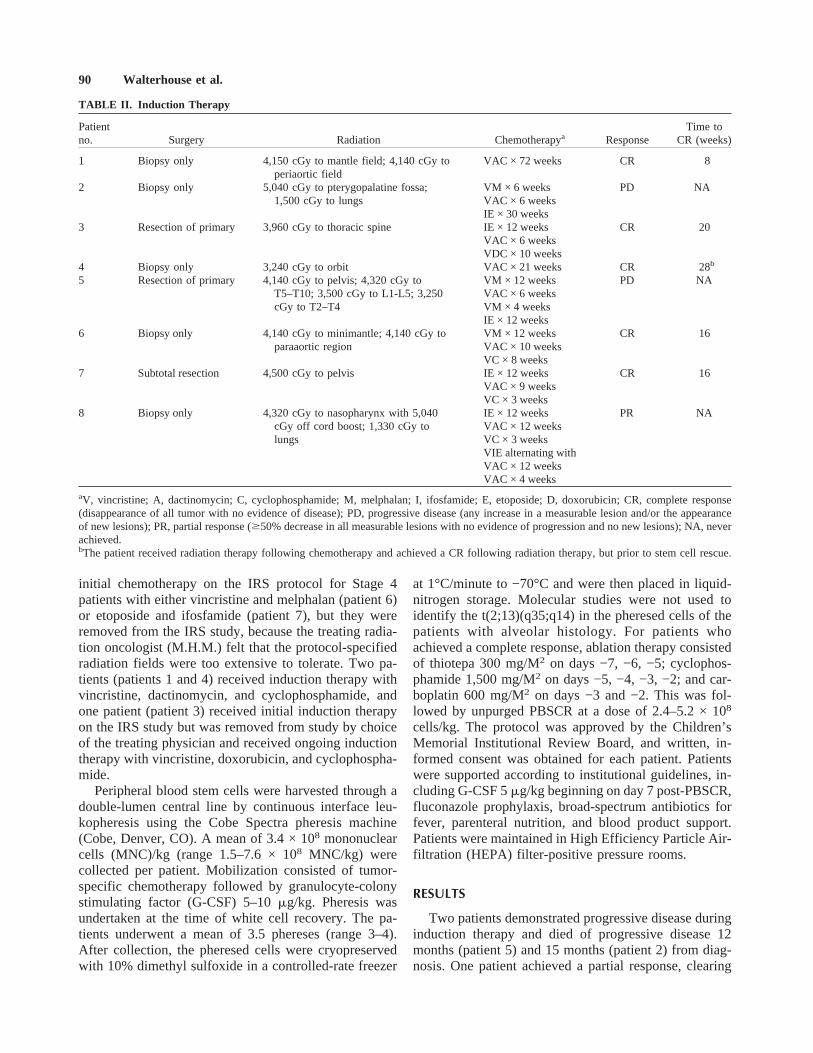
TABLE II. Induction Therapy
Patientno. Surgery Radiation Chemotherapya Response
Time toCR (weeks)
1 Biopsy only 4,150 cGy to mantle field; 4,140 cGy toperiaortic field
VAC × 72 weeks CR 8
2 Biopsy only 5,040 cGy to pterygopalatine fossa; VM × 6 weeks PD NA1,500 cGy to lungs VAC × 6 weeks
IE × 30 weeks3 Resection of primary 3,960 cGy to thoracic spine IE × 12 weeks CR 20
VAC × 6 weeksVDC × 10 weeks
4 Biopsy only 3,240 cGy to orbit VAC × 21 weeks CR 28b
5 Resection of primary 4,140 cGy to pelvis; 4,320 cGy to VM × 12 weeks PD NAT5–T10; 3,500 cGy to L1-L5; 3,250 VAC × 6 weekscGy to T2–T4 VM × 4 weeks
IE × 12 weeks6 Biopsy only 4,140 cGy to minimantle; 4,140 cGy to VM × 12 weeks CR 16
paraaortic region VAC × 10 weeksVC × 8 weeks
7 Subtotal resection 4,500 cGy to pelvis IE × 12 weeks CR 16VAC × 9 weeksVC × 3 weeks
8 Biopsy only 4,320 cGy to nasopharynx with 5,040 IE × 12 weeks PR NAcGy off cord boost; 1,330 cGy to VAC × 12 weekslungs VC × 3 weeks
VIE alternating withVAC × 12 weeksVAC × 4 weeks
aV, vincristine; A, dactinomycin; C, cyclophosphamide; M, melphalan; I, ifosfamide; E, etoposide; D, doxorubicin; CR, complete response(disappearance of all tumor with no evidence of disease); PD, progressive disease (any increase in a measurable lesion and/or the appearanceof new lesions); PR, partial response ($50% decrease in all measurable lesions with no evidence of progression and no new lesions); NA, neverachieved.bThe patient received radiation therapy following chemotherapy and achieved a CR following radiation therapy, but prior to stem cell rescue.
90 Walterhouse et al.

the primary site but not the lungs, and died of progressivepulmonary disease 22 months from diagnosis (patient 8).Five patients achieved a complete response and werecandidates for PBSCR. Time to complete responseranged from 8 weeks to 28 weeks from diagnosis (TableII). Complete response was determined by radiographicimaging studies in all cases. One patient refused trans-plant (patient 1), and four patients underwent PBSCRfollowing high-dose chemotherapy 28–36 weeks fromdiagnosis (patients 3, 4, 6, and 7). Extensive radiationfields affected marrow reserve in three patients (patients5, 6, and 7), resulting in chemotherapy delays duringinduction therapy.
All patients who underwent PBSCR following high-dose chemotherapy engrafted with a median time to anabsolute neutrophil count (ANC) of greater than 500 ×106/liter of 15 days (range 9–44 days) and a plateletcount greater than 20 × 109/liter of 21 days (range 9–93days). Peritransplant toxicities included sepsis in fourpatients, fungal infection in one patient, hemorrhagiccystitis in one patient, and acalculous cholecystitis in onepatient. There were no treatment-related deaths.
One patient, who presented with an extremity primarytumor and with bone and bone marrow metastatic sites, iswithout evidence of disease 53 months post-PBSCR (pa-tient 3; Fig. 1). Three patients died with recurrent diseaseat 10 months (patient 4), 12 months (patient 7), and 19months (patient 6) post-PBSCR and 19 months (patient4), 20 months (patient 7), and 29 months (patient 6),respectively, from diagnosis. The three patients who de-veloped recurrent disease recurred in known sites of dis-ease at the time of diagnosis, including a paraspinal/vertebral body recurrence (patient 4), a pulmonary recur-rence (patient 7), and recurrent peritoneal and pleuralimplants (patient 6). Two of these patients recurred inareas of known disease that had not been irradiated (pa-tients 6 and 7). The patient who refused transplant died ofprogressive disease in the lungs and bone marrow 30months from diagnosis (patient 1).
DISCUSSION
Horowitz et al., Pinkerton et al., and Koscielniak et al.failed to show an advantage of autologous bone marrowrescue following high-dose myeloablative chemotherapyover standard chemotherapy, radiation therapy, and sur-gery for patients with Stage 4/Group IV rhabdomyosar-coma [7–9]. It is possible, however, that different abla-tive regimens might consolidate more successfully theremissions that can be achieved in the majority of thesepatients. We used an ablative regimen consisting of thio-tepa 300 mg/M2 on days −7, −6, and −5; cyclophospha-mide 1,500 mg/M2 on days −5, −4, −3, and −2; andcarboplatin 600 mg/M2 on days −3 and −2. This regimenprovides myeloablation with minimal extramedullarytoxicity, and we recently reported that it is well toleratedduring transplantation of patients with neuroblastoma[10]. It has not been tested previously for treatment ofrhabdomyosarcoma; however, cyclophosphamide isknown to be an effective agent against rhabdomyosarco-ma, and carboplatin has been used as part of combinationchemotherapy for metastatic rhabdomyosarcoma and forrhabdomyosarcoma in the relapse setting [11]. There areno data evaluating the activity of thiotepa against rhab-domyosarcoma; however, its marrow toxicity makes it anideal agent for autologous transplantation.
Five of eight patients in our series achieved a com-plete remission, a number comparable to that in the IRSII and IRS III studies for Group IV patients [2,3]. Ourresults support the other studies showing no advantage ofhigh-dose chemotherapy followed by autologous PBSCRas consolidation therapy for patients with Stage 4/GroupIV rhabdomyosarcoma over standard-dose chemo-therapy, radiation, and surgery. One of four transplantedpatients is a long-term survivor, a number comparable tothe other studies and to the use of standard therapy.
Interest in using autologous transplant in this group ofpatients was generated by the treating radiation oncolo-gist’s feeling that some of the patients would not be ableto tolerate standard radiation therapy in terms of marrowreserve. This approach was considered as a possible al-ternative to standard chemotherapy, radiation therapy,and surgery. Although the numbers are small, two ofthree patients who did not receive standard radiationtherapy and underwent high-dose chemotherapy fol-lowed by PBSCR developed recurrent disease in areas ofknown disease that were not irradiated. Indeed, the initialrecurrence in each patient undergoing PBSCR in our se-ries was in a site of known disease at diagnosis. High-dose chemotherapy followed by PBSCR, as carried out inthis series of patients, did not provide adequate localcontrol for the majority of the patients. For patients withextensive, unresectable disease at diagnosis who cannotreceive radiation to all areas of disease based on concerns
Fig. 1. Flow diagram of the outcome of patients with Stage 4/GroupIV rhabdomyosarcoma. CR, complete response.
Stem Cell Rescue for Rhabdomyosarcoma 91

of marrow reserve, high-dose chemotherapy followed byPBSCR does not appear to provide adequate local con-trol, and high-dose chemotherapy followed by PBSCRcannot be offered as curative to these patients.
The single surviving patient had several poor prog-nostic factors, including an extremity primary, metastaticinvolvement of the bone marrow and bone, and alveolarhistology. The time to achieve a complete response forthis patient was not particularly rapid at 20 weeks.Whether this patient benefited from the high-dose che-motherapy followed by PBSCR above and beyond thestandard chemotherapy, surgery, and radiation therapy isunclear.
REFERENCES
1. Maurer HM, Beltangady M, Gehan EA, et al. The IntergroupRhabdomyosarcoma Study-1. A final report. Cancer 1988;61:209–220.
2. Maurer HM, Gehan EA, Beltangady M, et al. The IntergroupRhabdomyosarcoma Study-II. Cancer 1992;71:1904–1922.
3. Crist W, Gehan EA, Ragab AH, et al. The Third Intergroup Rhab-domyosarcoma Study. J Clin Oncol 1995;13:610–630.
4. Ruymann RB, Newton WA, Ragab AH, et al. Bone marrow me-tastases at diagnosis in children and adolescents with rhabdomyo-sarcoma. Cancer 1982;53:368–373.
5. Raney RB, Tefft, M, Maurer, HM, et al. Disease patterns andsurvival rate in children with metastatic soft-tissue sarcoma. Can-cer 1988;62:1257–1266.
6. Koscielniak E, Rodary C, Flamant F, et al. Metastatic rhabdomyo-sarcoma and histologically similar tumors in childhood: a retro-spective European multi-center analysis. Med Pediatr Oncol 1992;20:209–214.
7. Horowitz ME, Kinsella TJ, Wexler LH, et al. Total-body irradia-tion and autologous bone marrow transplant in the treatment ofhigh-risk Ewing’s sarcoma and rhabdomyosarcoma. J Clin Oncol1993;11:1911–1918.
8. Pinkerton CR, Groot-Loonen J, Barrett A, et al. Rapid VAC highdose melphalan regimen, a novel chemotherapy approach in child-hood soft tissue sarcomas. Br J Cancer 1991;64:381–385.
9. Koscielniak E, Klingebiel TH, Peters C, et al. Do patients withmetastatic and recurrent rhabdomyosarcoma benefit from high-dose therapy with hematopoietic rescue? Report of the German/Austrian Pediatric Bone Marrow Transplantation Group. BoneMarrow Transplant 1997;19:227–231.
10. Kletzel M, Abella EM, Sandler ES, et al. Thio-tepa and cyclo-phosphamide with stem cell rescue as consolidation therapy forchildren with high risk neuroblastoma. A Phase I/II study of thePediatric Blood and Bone Marrow Transplant Consortium. J Pe-diatr Hematol Oncol 1998;20:49–54.
11. Frascella E, Pritchard-Jones K, Modak S, et al. Response of pre-viously untreated metastatic rhabdomyosarcoma to combinationchemotherapy with carboplatin, epirubicin and vincristine. Eur JCancer 1996;32:821–825.
92 Walterhouse et al.