Embed Size (px)
Citation preview

HIGH COUNTRY NUCLEAR
MEDICNE CONFERENCE
February 27, 2016
BIG DATA AND PERSONALIZED MEDICINE
Robert C. Hendel, MD, FACC, MASNC
Professor of Medicine and Radiology
Associate Chief Medical Officer
Director, Cardiac Care Unit
University of Miami Hospital

BIG DATA IN HEALTH CARE
• Of the people, for the people, by the
people…..
• “Transition of data from refuse to riches” JAMA 2013; 309: 1351

A FEW EXAMPLES
• Astronomy
• Engineering
• Retail sales
• Entertainment
• Politics
• Medicine
–E. Coli outbreaks
–Cancer screening
–Drug surveillance

BIG DATA SUPPORTS IOM’S TRIPLE AIM
• Improve the health of the
population
• Enhance the patient
experience of care (including
quality, access, and reliability)
• Reduce, or at least control, the
per capita cost of care.

BIG DATA AND POTENTIAL IMPACT
ON HEALTHCARE
• Stimulate change that can improve patient
outcome
• Define further areas of investigation
• Better monitoring of safety and effectiveness
• Permit development of personalized medicine
leading to improved outcomes and efficiencies

THE FIVE “V’s” OF BIG DATA
• Volume –Massive amounts of data, with anticipated increase of 20-50 fold within
5 years [zetttabyte (1024 gigtabytes)]
–Strain capacity and capability for storage, management and retrieval
• Variety –Linkage of disparately formatted data
• Velocity –More flexibility and more rapidly using big data infrastructure
• Veracity –Data assurance (error-free)
• Value

COMPONENTS OF BIG DATA IN HEALTHCARE
• Notes
• Prescriptions
• Imaging
• Laboratory
• Pharmacy
• Insurance
• Administrative data
• EHR data
• Social media
• Monitoring feeds
–Vital signs
–HF data

APPLICATIONS OF BIG DATA IN HEALTHCARE
• Population characteristics
• Particularly value for evalution of social determinants
of health
• Identification of risk factors
• Development of predictive models
–Diagnostic
–Prognostic
• Comparison of different interventions (observational)
• Variation among providers
–Systems
–Individuals
• Fuel for research BJS 2015; 102: e93
JACC 2015; 66: 1898

POTENTIAL HEALTHCARE SAVINGS WITH BIG DATA ANALYTICS
$300 Billion
• Lost through waste and inefficiency
–Clinical operations: comparative effectiveness; CE strategies
–R & D: modeling, predictions, clinical trial design
–Public health: disease patterns,
• Additional contributions of big data analytics
–Evidence-based medicine
–Geonomic analytics
–Fraud analysis
–Device monitoring
–Patient profile analytics
Raghupathi W, Raghupathi V
HISS 2014; 2: 3

CLINICAL DATABASES
• Administrative
–Routinely collected
–Limited patient information
–Clinical management: usually episode of care
–Health insurance: claims data
• Clinical
–Specific collection process
–Relevant clinical data collected
–More data on outcomes and co-morbidities
–Disease-based: Primary focus on clinical quality
–Treatment-based: Value of intervention


BIG DATA APPLICATIONS
FOR HEALTH CARE QUALITY
• Generation of new knowledge
–Allows for observational evidence for clinical questions
not possible with RCT
–Enhance generalizability of trial findings
• Knowledge dissemination
–Dashboards, clinical alerts
• Translation into personalized medicine
• Empowerment of patients
Murdoch TB, Detsky AS
JAMA 2013; 309: 1351

BIG DATA AND CLINICAL RESEARCH
Need for New Thinking, Training and Tools
(Harlan Krumholtz, MD)
• THE PROBLEM
–Current medical research cannot keep pace with
the information needs of patients, clinicians,
administrators, and policy makers
• THE SOLUTION
–Data generated every day could serve as an
inexhaustible source of knowledge to fuel a
learning health system

BIG DATA CHALLENGES FOR CLINICAL RESEARCH
• Data quality
–Completeness: representative and comprehensive
–Accuracy: Valid and reliable •Data entry error
•Systemic inconsistencies and omissions
•Misclassification
–May be enhanced by incentives (i.e. reimbursement)

BIG DATA CHALLENGES FOR CLINICAL RESEARCH
• Application of causality (causal interpretation)
–Must use caution, as with all observational studies
–Situations of excessive variation •Concern with administrative database
• Incomplete data, patient differences, violation of modelling
assumptions, secular trends, chance
–Comparison of outcomes •Variation of treatment groups beyond treatment received (bias)
–Analytics •Multiple regression
•Propensity scores

BIG DATA CHALLENGES FOR CLINICAL RESEARCH
• Application of causality (causal interpretation)
–Must use caution, as with all observational studies
–Situations of excessive variation •Concern with administrative database
• Incomplete data, patient differences, violation of modelling
assumptions, secular trends, chance
–Comparison of outcomes •Variation of treatment groups beyond treatment received (bias)
–Analytics •Multiple regression
•Propensity scores
Whenever a causal interpretation is applied to data from
complex observational studies, such as those with big
data, “it cannot be overemphasized that ….data need to
be interpreted with a high degree of caution”
Ejerhed J et al, 2014
Lancet: 384: 303


BARRIERS FOR APPLICATION OF BIG DATA
• Privacy
–Cultural and ethical issues related to patient privacy
–Need for robust, integrated security for databases
–Blurred boundaries of research (consent required) and quality
improvement (exempt form consent)
–Concern raised in English Parliament caused suspension of
big data collection (BMJ 2015; 35: 351)
• Lack of expertise (data scientists, IT, etc)
• Time and expense
• Lack of acceptance
–Scientific community
–Clinicians
–Regulators

PERSONALIZED MEDICINE
The Wikipedia Definition
Medical model that separates patients into different
groups with medical decisions, practices, interventions
and/or products being tailored to the individual patient
based on their predicted response or risk of disease.
The terms personalized medicine, precision medicine,
stratified medicine and P4 medicine are used
interchangeably to describe this concept though some
authors and organizations use these expression
separately to indicate particular nuances,

PRECISION MEDICINE INITIATIVE (PMI)
• Announced during State of the Union
address on January 20, 2015
• $215 million support in FY 2016
–$70 for cancer genomics
–$130 M for cohort program
• Involves 1,000,000 participants
• EHR, genomics, patient engagement
• Disease focus but also prevention
• Goal of understanding complex
mechanisms of a patient’s health, disease
or condition and better predict which
treatments will be most effective.

Biv
al P
erc
ent
(%)
0
10
20
30
40
50
60
70
80
90
100
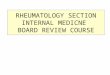
Bleeding Risk
" Low Risk Mod Risk High Risk "
Individual Operator Bival Use by Risk
doc_1033161138
doc_1154324127
doc_1265435101
doc_1265516223
doc_1275675027
doc_1326127267
doc_1447369368
doc_1457373656
doc_1508837287
doc_1578586533
doc_1588844245
doc_1598842601
doc_1619970532
doc_1659455335
doc_1669559480
doc_1720165640
doc_1780651497
doc_1891882965
doc_1942323944
doc_1982604914
Bival Use across Operators
Opportunity to be
more Efficient by
Reducing Use
Opportunity to
Improve Safety by
Increasing Use

Implementing Tools at
Point-of-Care
0 1 1
1 1
0 1 1
= 1
1 1 = 2 , , where
1
1
= 1
1
,
( )
1
(LO
T n T n
T n T n
i i i T i n T n
i i
i
i si ji iij
i
i sjj
x x
x x
x x
12 2
0 0 02 1
1
0
1 2
1
1
)HI
T
T T
T
F
n
n
n n nn
c cx
x x
c cx
Risk Models


Biv
al P
erc
ent
(%)
0
10
20
30
40
50
60
70
80
90
100
Bleeding Risk
" Low Risk Mod Risk High Risk "
Individual Operator Bival Use by Risk
doc_1043497241
doc_1134185390
doc_1174580773
doc_1265498323
doc_1306888144
doc_1386601235
doc_1396701066
doc_1508035163
doc_1528026374
doc_1730260456
doc_1831147420
SLH 2012
Biv
al P
erc
ent
(%)
0
10
20
30
40
50
60
70
80
90
100
Bleeding Risk
" Low Risk Mod Risk High Risk "
Individual Operator Bival Use by Risk
doc_1043497241
doc_1134185390
doc_1174580773
doc_1265498323
doc_1306888144
doc_1386601235
doc_1396701066
doc_1508035163
doc_1528026374
doc_1730260456
doc_1831147420
SLH 2013
• Predicted Bleeding Rate in 2013: 6.5%
• Observed Bleeding in 2013: 2.4%
• A third of predicted!
Impact of Accountability

The Benefits of Precision Medicine
Incidence of PCI-Related Bleeding Incidence of PCI-Related Acute Kidney Injury
Incidence of Rarely Appropriate Elective PCI

Total Cost Savings over 1 Year @
BJH
Savings from a reduction in PCI complications $1,235,000
Increased revenue from improved outcomes
(QHIP) $884,000
Increased revenue from Medicare (VBP) program $600,000
Savings from Same Day Discharge (SDD) program $452,000
Savings on PCI medications / Pharmacy savings $494,000
Estimated total savings $3,665,000

USING TO IMPROVE CARE
Prospective Data
Collection
Creation of
Predictive Models
Prospectively
Improve Health
Requires a IT Solution
Periodic Benchmark
Reports for Quality
Assurance
Courtesy of J Spertus



PRECISION MEDICINE (Wikipedia)
• Precision medicine….proposes customization of
healthcare, with medical decisions, practices and/or
produces being tailored to the individual patient
• Diagnostic testing...for selecting appropriate and optimal
therapies based on the content of a patient’s genetic
content and other molecular or cellular analysis.
• Much overlap wtih the term “personalized medicine”
• An approach to discover and develop treatments for
disease prevention and deliver superior outcomes by
integrating “big data”, clinical, molecular, environmental
and behavior informaotni, thereby leading to better
selection of theraeputic targets and novel prevention
strategies

ADVANCED
ANALYTICS Deals with smaller datasets but
uses advanced techniques to
analyze the impact of future
scenarios.
BASIC
ANALYTICS Relies on historical observations to
help avoid past mistakes and
duplicate past success.
BIG DATA
COMPUTING From a systems perspective, data
becomes more consolidated while
analytic workflows are more
streamlined and automated.
BIG DATA
ANALYTICS Can fuse different data types on a
massive scale resulting in
predictive and real-time analysis
capabilities.
An
aly
tic C
om
ple
xity
Size of Data
Small amounts of data or samples
(megabytes to gigabytes)
Large (or all) Amounts of data
(gigabytes to petabytes)
Predictive and real-time analytics capabilities
Accurate historical observations

Open Data: Examples Of Recently Released Data • Provider Utilization and Payment Data
• Public use files and interactive dashboards at the
state, HRR, and county level
– Chronic conditions
– Geographic variation
66
– Hospital Inpatient
– Hospital Outpatient
– Physician and other Supplier

Data-Sharing Programs: Virtual Research Data Center
ACCESS(
PRIVACY(
SECURITY(• (No(shipping(of(data(on(external(media((• (Users(only(see(data(files(with(the(data(they(need(to(conduct(their(project((• (CMS(can(track(and(monitor(use(of(the(data(
• (Users(can(perform(their(own(analyses(and(data(manipulaGon((in(
the(virtual(environment(
• (Secure(File(Transfer(System(allows(users(to(upload(their(own(data(and(download(output(files(efficiently(and(securely(
DATA(&(ANALYSIS(
• (Researchers(use(own(laptop(to(securely(access(data(remotely((
• (Increases(efficiency(of(data(sharing(and(reduces(infrastructure(costs(for(data(users((
• (Users(may(only(remove(aggregated(output(files;(no(granular(idenGfiable(output(may(be(taken((
Out(of(the(VRDC(• (CMS(encrypts(all((beneficiary(idenGfiers(
67

PATIENT-POWERED RESEARCH NETWORKS
PCORI
• PCORnet launched in 2014
• Goal: Improve speed, efficiency and cost-
effectiveness of clinical research by engaging
patients and leveraging EHR
• Better evidence will lead to improved patient
health outcomes