Embed Size (px)
Citation preview

High altitude medicine
Charles Clarke*,1
National Hospital for Neurology and Neurosurgery and Whipps Cross Hospital,Queen Square, London WC1N 3BG, UK
Received 1 November 2004; accepted 2 November 2004Available online 1 April 2005
Introduction
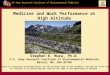
Over 10 million people live at altitudes above4000 m in a hypoxic environment throughout theirlives, often without evident clinical effects. How-ever, millions of lowlanders, i.e. sea level residentsor those usually residing below 3000 m travel highereach year. Some do so for pleasure, others foremployment, to engage in warfare or to go ontrekking, skiing or mountaineering trips. Theyfrequently develop various forms of high altitudeillness, the clinical syndromes caused by chronichypobaric hypoxia. Often separated into acutemountain sickness (AMS), pulmonary and cerebraloedema, these conditions have a common patho-physiological basis.1 The degree of hypoxia atvarious altitudes is illustrated in Fig. 1. Seriousclinical problems are seldom seen below 3000 m.
Acute mountain sickness is often no more than amild inconvenience, though sometimes distinctlyunpleasant. By contrast, the serious forms ofaltitude-related illness, pulmonary and cerebraloedema are potentially fatal. Since the latter havebeen recognised principally on mountaineeringexpeditions, there is a tendency to regard altitude
1477-8939/$ - see front matter Q 2004 Elsevier Ltd. All rights reservdoi:10.1016/j.tmaid.2004.11.006
* Tel.: C44 20 7837 3611.E-mail address: [email protected].
1 Charles Clarke has been climbing since the 1960s and hastaken part in many Himalayan expeditions including two toEverest.
medicine as a branch of wilderness medicine, or ofmountaineering itself. The reality is that altitudemedicine is of major importance to the travel andski industries, and to the military. It has economicand public health consequences far beyond climb-ing mountains. In addition, the study of sufferershas given us valuable insight into the effects ofhypoxia in the sea level population when they suffercardiac or respiratory disease.
The purpose of this article is to provide anoverview of the subject, with brief case reportsillustrating the reality of illness at high altitude.
History
From the earliest times it was clear that travel tohigh places could cause problems.2 Tookim, aChinese civil servant writing in the time of theEmperor Ching Te (37–32 BC) offered a sternwarning to General Wang Fung, preparing tomarch to the far west (towards Tibet and Xinjiang):
“The Chinese Commission will in such circum-stances be left to starve among the hills andvalleys. Again, on passing the Great HeadacheMountain and the Little Headache Mountain, theRed Land and the Fever Slope, men’s bodiesbecome feverish, they lose colour and areattacked with headache and vomiting. Theasses and cattle being all in like condition.”
Travel Medicine and Infectious Disease (2005) 3, 189–197
www.elsevierhealth.com/journals/tmid
ed.

Figure 1 Altitude, barometric pressure, air pressureand oxygen tension.
Plate 1 Mosso’s apparatus to measure transmittedpulsation through a post-traumatic skull defect (CharlesClarke Collection).
C. Clarke190
Death at altitude with foaming at the mouth wasalso recorded in later Chinese documents. In the17th century the Jesuit priest Jose d’Acostamentioned similar problems crossing the Andes.
It was Angelo Mosso, an innovative professor ofphysiology in Turin in the late 19th century whopioneered the study of altitude hypoxia. Whilst theEnglish speaking world dwelt on climbing exploits,for example those of Edward Whymper3 (first ascentof the Matterhorn, 1865) and Sir Martin Conway(Himalayas 1892), Mosso commissioned his ownlaboratory, the Capanna Margherita on the alpinesummit of Monte Rosa (4554 m). Ingenious physio-logical studies were undertaken (Plate 1). Therewas recognition of effects of hypoxia on both brainand lungs.4
Other early contributors were Haldane, Barcroftand colleagues (1910–1920) and the physiologistAlexander Kellas (1921). Later Dr Griffith Pugh andmany others from the 1950s onwards have exploredthe physiology of acclimatisation and the effects ofhypoxia. However in terms of practical medicine,the headaches and malaise of acute mountainsickness (AMS) remained the only recognisablecondition until 1960, when the climber and phys-ician Charles Houston described acute high altitudepulmonary oedema.
Figure 2 Effects of acute hypoxia.
Acute mountain sickness (AMS)
Stepping from an aircraft, road vehicle or ski-liftabove 3000 m, immediate breathlessness and faint-ness are common—the acute effect of hypoxia.

High altitude medicine 191
Sudden ascent to extreme altitudes can even leadto abrupt loss of consciousness (Fig. 2).
AMS describes more gradual malaise that devel-ops within some 6–24 h of arrival above 3000 m.Symptoms are rare below 2500 m, but almostinvariable following sudden ascent to 4000 m orabove, when they may be very unpleasant andsevere. The AMS syndrome is simply defined:headache in an unacclimatised person recentlyarrived above 2500 m, with one or more of thefollowing—anorexia, nausea, vomiting, insomnia,dizziness or fatigue.5
At 3500 m AMS seldom progresses much further.Resolution is usual without treatment within sev-eral days. At higher altitudes, more serious forms ofAMS are seen—at 4500–5000 m around 2% of sealevel visitors will suffer either severe disabling AMSor a high altitude oedema described below.
AMS follows a familiar pattern in individuals whogo high regularly. At 3600 m I feel slightly heada-chy, intensely lethargic, shivery, cold and faint forseveral days. I have heartburn and waterbrash. Inother people dizziness or headache predominate.
On recovery, one can expect to feel well ataltitude and continue to do so until extreme heightsabove 7000 m. Higher than this, deterioration setsin. Permanent human habitation is impossibleabove 6000 m.
Plate 2 Chest X-ray: high altitude pulmonary oedema(Charles Clarke Collection).
High altitude pulmonary and cerebraloedema
Typical clinical features
AMS is self-limiting, and essentially a problem to beendured. High altitude pulmonary and cerebraloedema are serious. They need early recognitionand prompt management.
Pulmonary oedema was identified clearly in1960, in a seminal case report6 by Charles Houstonin a skier in Aspen. Typically the patient had hadacute mountain sickness, and/or a minor respirat-ory infection but had failed to recover as expected.Breathlessness follows. At first the problem may besubtle, with an irritating dry cough and puffing atrest, or gasping whilst eating or talking, with adistinctly blue tinge around the lips. Later, withinhours or days, obvious severe dyspnoea follows.Copious frothy sputum is a late stage—cases areusually moribund by this time.
In the early stages, rales (audible crackles) in thechest soon develop, often beginning on the right.There is no need for a stethoscope—the cracklingcan be heard easily by resting an ear to the chest.
Signs of heart failure are absent, orthopnoeauncommon and haemoptysis rare. A mild feverbelow 38.5 8C is common.
Case 1. A man of 30 had struggled up on foot toEverest Base Camp at 5200 m. He had had AMS forseveral days and had never been ‘right’. Gradually,over a week at 5200 m he became slightly breath-less at rest. This first became obvious when he waseating. He became blue, but insisted he was wellenough to stay at altitude. There were crackles atboth lung bases. He recovered promptly whenescorted down below 4000 m during the day andwas entirely well (and indignant) on returning toKathmandu.
Patients with pulmonary oedema have soft, fluffyshadowing on chest X-ray (Plate 2)—often confinedto right in the early stages, a normal heart size,severe arterial hypoxaemia, pulmonary hyperten-sion and respiratory alkalosis.
Cerebral oedema is also usually a sequel ofunresolved AMS. It was recognised clearly in the1970s.7 Headaches persist, often postural andexcruciating. Unsteadiness develops. Unreasonablebehaviour is frequent. Double vision can develop,and vertigo. Later there is sleepiness, and coma.Seizures are uncommon. Downward herniation ofthe swollen brain (coning) is the cause of death, a

Plate 3 MRI in cerebral oedema (courtesy Dr Sui Wong, 2004).
C. Clarke192
distinct possibility by the time a patient hasbecome sleepy.
The finer points of neurological examinationcan be hard to delineate on a climb, in a tent, orhotel room. If someone at altitude acts oddly, oris ataxic on walking heel to toe, they have brainoedema until proven otherwise. Papilloedema isfrequent, cerebellar signs common, and a sixthnerve palsy (double visionCconvergent squint)the most evident cranial nerve sign. Stroke-like features are sometimes seen—a mildhemiparesis.
Case 2. A journalist and a doctor (myself) hadtravelled by jeep across Tibet to the region of theCho Oyu base camp at 5000 m. They both had hadmoderate AMS, mainly lassitude for a few days. At5000 m both became very sick with increasingheadache (excruciating on lying down). They wereslightly unsteady on their feet. The journalist hadno papilloedema. We were due to climb over a5400 m pass on foot the following day, but would beable to drop rapidly to 3600 m thereafter. Treat-ment with a single dexamethasone 8 mg dose bymouth resolved the headache and unsteadinesswithin several hours. Next day we crossed the highpass slowly, but uneventfully and had no recurrenceof the problem. We both had had mild cerebral
oedema, and had taken a substantial risk goinghigher in the way we did.
Investigation is rarely possible in the clinicalsetting of brain oedema, but where patients havebeen studied a posterior leucoencephalopathy ispresent—with a predeliction for changes in theposterior part of the corpus callosum on MRI(Plate 3).
Sudden cerebral and pulmonary oedemaat extreme altitude
We tend to regard altitude oedemas as severe formsof AMS—they often follow it and are part ofunresolved AMS and over-hasty acclimatisation.However one sometimes sees these conditionsdevelop suddenly at extreme altitudes above7000 m in fit, well acclimatised climbers.
Case 3. A sherpa who had been carrying loadsdaily for 2 weeks on the SW Face of Everest in 1975suddenly became ataxic with a headache at 7600 m.He was unable to stand. Severe papilloedema waspresent (Plate 4, taken on a portable retinal cameraat 6000 m). He made an uneventful rapid recoverywithin several days (descent and dexamethasone).
Case 4. A very fit well-acclimatised climber onanother Everest expedition, after a month of

Plate 4 The swollen optic disc in Case 3 (CharlesClarke, 1975).
High altitude medicine 193
intermittent visits above 7000 m, suddenly devel-oped a mild left hemiparesis whilst climbing. Hehad severe papilloedema. He recovered on descentwithin a week, and has since been back to highaltitude without ill effects.
Case 5. A highly experienced climber wasclimbing Kangchenjunga (8586 m) in winter withhis wife. He seemed entirely fit and acclimatisedand was about to attempt the summit from a campabove 7000 m. He suddenly began to cough upblood-stained sputum, and became gravely ill.Despite attempting to descend he deteriorated,developing features of both lung and brain oedema.He died high on the mountain within 1 day of theonset of symptoms.8
Pathophysiology
Much is now known about how these vascularoedemas develop, though some details remainelusive. The genetic basis for both individualsusceptibility and the tendency to recurrenceremains uncertain. Hypoxia causes over-perfusionof micro-vascular beds, high capillary pressure,endothelial leakage and hence, oedema. The pre-cise mediators in the brain may be nitric oxidesynthetase and vascular endothelial growth factor(VEGF). Headache follows stimulation of the trige-mino-vascular system (the cause of most headaches,anyway). There is evidence to suggest that everyoneat altitude develops some brain swelling, and hasover-perfused lungs. The acute altitude oedemasoccur when this delicate balance decompensates.
Management
This comprises a general approach to the issue,avoidance, drug prophylaxis and the treatment ofAMS and suspected/established high altitudeoedemas.
Despite the ready availability of information,9
many people seriously affected by altitude illnesssay that they had not been forewarned of thepotential dangers of hypoxia— of simply disregardgood advice. This accounts for serious cases seenregularly on Kilimanjaro (5895 m). It is prudent towarn travellers to altitude that AMS is common, andoften inevitable, though rarely serious, but con-versely that serious illnesses may happen, and ifthey do so they are not medical oddities.
Case 6. A 50 year medical professor decided toclimb Kilimanjaro over a long weekend fromLondon. He was strongly advised against this, butfelt he was in sufficiently good physical training todo it. Near the summit he became confused andunsteady, and felt very ill. He reached the top andreturned, unwell and exhausted to London. Onexamination he was probably slightly cognitivelyimpaired, and certainly disinhibited. He could givefew clear details of the summit. A severe haemor-rhagic retinopathy was present. He made a com-plete recovery over a week.
Prevention
Almost all serious altitude illness is preventable iftravellers go up slowly. Suggested guidelines above2500 m are deceptively simple. The height at whichone sleeps should increase by no more than500–600 m for each day’s ascent between 2500and 4000 m. Adding extras days is helpful.10 Thepracticality of following such an ideal regime rarelypresents itself.
Case 7. Whenever I fly into Lhasa (3600 m), I feelexhausted for several days. I usually decide to staythere for three nights, before leaving by road forthe highlands of the Tibetan plateau—a day’s driveto c.5000 m. Once there, I continue to feel unwellfor about a week. Intense tiredness is my usual AMSproblem. For others it is headaches.
On one occasion my wife came too, she felt awfuland rarely left our hotel room in Lhasa for 5 days.
Rest is itself preventative. When Indian troopsare taken to Ladakh in preparation for action on theSiachen Glacier, I gather they are under orders tostay in bed for several weeks after reaching 3000 m.
Prophylaxis with acetazolamide (Diamox) hasbeen long known to be helpful in reducing AMSsymptoms (probably 125 mg twice daily is

Table 1 Suggested drug regimes for AMS prevention.
Drug Suggested dose Duration Comment
Acetazolamide 125 mg twice daily 5 days before reaching3500 m
Tingling common, serious effects rare
Dexamethasone 2 mg three timesdaily
3 days before reaching3500 m
Usual steroid effects—heartburncommon
ginkgo biloba 120 mg twice daily 5 days before reaching3500 m
Preparations vary
Notes: 1. I avoid taking drugs, and having used acetazolamide several times, prefer my predictable AMS; 2. If drugs are needed, testdoses for a day several weeks before a trip are useful; 3. 2 mg dexamethasone allows for an increase in dose if cerebral oedemadevelops.
C. Clarke194
sufficient), see Table 1. Dexamethasone has alsobeen shown to be effective, and perhaps surpris-ingly, gingko biloba. Anyone taking these drugsneeds to know their potential unwanted effects.
There are several myths about AMS. Physicalfitness and overhydration do nothing to prevent it(and may be counterproductive). Similarly, tobaccosmoking, cannabis and alcohol have no knowneffects either way. Sleeping pills, which might beexpected to make matters worse by depressingrespiration and exacerbating hypoxia, do not seemto be a problem. Zopiclone 3.75 mg is a useful, safedrug.
Treatment
The axioms are simple:
†
RECOGNISE altitude oedemas: differentiate fromAMS†
Avoid going higher † Avoid exercise † Descend, and certainly do so if deteriorating † Use drugs and oxygen.Typically the practical, diagnostic issue is thatAMS causes a profusion of complaints withoutphysical signs, whilst pulmonary and cerebraloedema can steal up on both the patient anddoctor. Whilst this is an over-simplification, failureto differentiate AMS from, and act upon, emergingaltitude oedemas has led to fatalities that mightwell have been avoided. Breathlessness at rest (weare all breathless on exercise) is the earliest sign ofpulmonary oedema, and ataxia the hallmark ofbrain oedema.
Acute mountain sicknessTreatment
‘Put them to bed, and give them aspirin,paracetamol and plenty of tea. They’ll soon bebetter’ is a reasonable attitude in most cases. Most
AMS is on the way to recovery within 3 days.However, the lethargy and malaise of AMS can beintense, and the headaches severe. In this situationmore enthusiastic treatment is certainly an option.
Descent—as little as 500 m or more can becurative within a matter of hours—is sometimespossible, but clearly not from an airport. Descent isalso administratively difficult and unpopular in theearly stages of a trek. Oxygen helps AMS quickly,and is often available (at a price) in up-markethotels. AMS is rarely severe enough to need aportable pressure chamber (see below), but theycan be used.
Both acetazolamide (250 mg twice daily forseveral days) and dexamethasone (see Prevention)are helpful. I often give a single large dose ofdexamethasone 4–8 mg by mouth, followed byanother if necessary at 4 h, if someone needstreatment for bad AMS.
These measures, with the passage of several daysare usually sufficient to resolve most cases of AMS.If they have failed to do so, or if a patient isdeteriorating, it is wisest assume that eitheraltitude oedema is present (pulmonary, cerebralor both) or that some other condition is the cause ofthe problem. It is obvious that there are manycauses of breathlessness, headache or ataxia. If oneof these situations prevails, the safety of thepatient and their immediate care must take priorityover the wishes and aspirations of fit members of aparty. A trivial illness (AMS) has become a seriousemergency.
Pulmonary and cerebral oedemaAction is essential. Experience has shown thatestablished brain and lung oedema rarely resolvewithout treatment. Oxygen is helpful, but descenteven better. Even a drop of several hundred metresis worthwhile. Sitting in a tent and waiting is a lastresort. Portable hyperbaric chambers are helpful,but they have a habit of being elsewhere when oneneeds them. They need to be carried (one porter

Plate 5 Portable hyperbaric chamber in use at 4000 m in Tibet (Charles Clarke, 1997).
High altitude medicine 195
load) and pumped up. The inmate can becomeclaustrophobic (Plate 5).
Since it is often difficult to sort out whether brainor lung oedema is the most prominent, I usuallyassume both are present. Dexamethasone can bedramatically effective in cerebral oedema in amatter of hours, and nifedipine in pulmonaryoedema (Table 2).
Like AMS, when altitude oedemas begin toimprove, generally they continue to do so, andresolve completely.
Other high altitude phenomena
Peripheral oedema
Facial and upper limb swelling sometimes appearsduring acclimatisation. It is of little consequence.
Retinal haemorrhages
In the 1970s, symptomless retinal haemorrhageswere noted at altitude on several expeditions.11
Table 2 Suggested treatments for severe altitude illness.
Drug/treatment Dose &c
Descent 300 m often helpsDexamethasone 8 mg, then 4 mg every 6 hNifedipine 10 mg, then 20 mg slow r
12 hourlyOxygen 2–4 L/min by mask/cannuPortable hyperbaric chamber pump, to 2–4 psi for 2 h
Presumably these are due to retinal over-perfusion.Dramatic haemorrhages are sometimes seen, par-ticularly during acclimatisation. Rarely they inter-fere with vision.
Case 8. Plate 6 shows a large symptomlesssubhyaloid haemorrhage in one of the fittestclimbers on the Everest SW Face expedition in1975. He had been climbing in the icefall (below6000 m) for a week. The haemorrhages resolvedspontaneously (and he did not ‘go off sick’).
Sometimes a florid retinopathy develops in thecontext of cerebral oedema:
Case 9. An Argentinian climber developedblurred vision and severe headaches whilst climbingAconcagua (6959 m). I have little clinical data onthis case (Britain was at war with Argentina at thetime) other than the dramatic retinal photos(Plate 7) and the knowledge that visual losspersisted. Presumably the man had this retinopathyin the setting of cerebral oedema.
Stroke
Strokes have been recorded in travellers to alti-tude, perhaps more frequently than in the sea level
Comments
Mandatory, if at all possible(oral, IM, IV) Sometimes effective within minutes
elease
la Always helpsHelpful; claustrophobia an issue; notreally portable

Plate 6 Symptomless retinal haemorrhage in Case 8(Charles Clarke, 1975).
C. Clarke196
population. The high haemoglobin level (it mayexceed 20 G/dl) that develops in response tohypoxia after several weeks at altitude, withincreased blood viscosity are obvious factors:dehydration is another. Cerebral oedema is men-tioned above.
‘Funny turns’
Episodes of loss of consciousness, ‘blackouts andfunny turns’ are common diagnostic issues.
Fainting may occur during acclimatisation. Sei-zures are an occasional feature of cerebral oedema,and occasionally appear to be provoked at altitudein patients who already suffer from epilepsy,presumably from brain swelling/fluid retention.There have been several case reports of braintumours being recognised during AMS.
Plate 7 Florid retinopathy in Case 9 (Charles ClarkeCollection).
Some ‘funny turns’ at altitude are less easy tosort out. Migrainous events mimicking thrombo-embolic TIAs, or TIAs themselves have beenreported. Non-epileptic events (pseudo-seizures)may occur.
Children and elderly people at altitude
Children suffer problems similar to those seen inadults.12 Provided risks are understood there is noreason why they should not go high. Elderly peoplewho are otherwise well often tolerate hypoxiabetter than younger folk—perhaps because they donot rush around.
Deterioration at extreme altitude
Permanent human habitation is impossible above6000 m, though climbers and physiologists havestayed for some months at this altitude without aproblem.
Above 7000 m deterioration sets in, and soonbecomes rapid and evident over several days,especially as one gets near 8000 m summits withoutbottled oxygen.
Appetite falls, weight loss is substantial andfatigue extreme. Cognition becomes impaired andjudgement poor. This is the setting of many fatal-ities at great heights, when climbers are at theirphysiological, hypoxic limits. Survival, briefly, ispossible for acclimatised humans at the summit ofEverest (8848 m) without bottled oxygen. Intercur-rent illness or even a fall in barometric pressure cantip the balance in this fragile setting. The wary stayas briefly as possible above 7000 m.
High altitude native populations
There is a common myth that hill people—porters,sherpas and camp staff—suffer AMS less than theiremployers. The reality is that unless they live athigh altitude (well above 2500 m) or are alreadyacclimatised they share the same risk as anyoneelse.13 They are often poorly equipped and becomevery miserable when asked to carry heavy loadswhen they have AMS.
Chronic mountain sickness (CMS, Monge’sDisease)
For completeness, this condition seen in highaltitude residents is mentioned briefly here. In1925 Dr Carlos Monge reported a case of poly-cythaemia in a man from Cerro de Pasco (4300 m).CMS consists of vague but real complaints

High altitude medicine 197
(headache, fatigue, poor concentration, dyspnoeaon exertion) in high altitude residents, typicallywith excessive haemoglobin levels. Largely seen inSouth America, CMS has now been reported in Asia.Characteristically symptoms reverse on descent tosea level, and return on re-ascent.
Pre-existing medical illnesses
In contrast to the dramatic presentations of thealtitude oedemas and the substantial changes intissue oxygenation at altitude, underlying medicalillnesses under control at sea level are generally welltolerated. My general advice is to avoid draconianrestrictions, provided risks are clearly understood.
Asthma behaves variably. Long-standing suf-ferers with evident allergies often improve above4000 m. Late onset asthma tends to betroublesome.
The blood pressure tends to fall slightly duringacclimatisation (it may be rather labile). Treatedhypertension carries no substantial risk.
Diabetes and epilepsy pose no great risk ataltitude. Brittle diabetes may become hard tocontrol, and the anorexia of AMS may be a problem.Epilepsy control is not often an issue.
People with mild angina or following successfulbypass surgery have gone to altitude withoutevident ill effects. Cardiac failure and chronicrespiratory impairment are however likely tocause substantial problems above 3000 m.
In general, a pragmatic assessment of risk needsto be carried out for any condition. One man withmalignant glioma of the brain was keen to go toEverest before he died, accepted the risks—andsurvived an expedition in reasonable shape.
Returning to altitude after seriousaltitude illness
‘Will it be safe to return?’ is a common questionafter someone has had pulmonary or cerebral
oedema. There is no easy answer. There arecertainly individuals who tend repeatedly todevelop severe AMS or altitude oedema.
I warn of the distinct possibility of recurrencebut point out that many climbers have had oneepisode of pulmonary or cerebral oedema and thenreturned to extreme altitudes without any obviousill-effects. For a holidaymaker/trekker the notionof a future, recurrent, potentially fatal illness issufficient to deter most—but the determinedmountaineer, by nature more anarchic and lessrisk averse, rarely heeds cautious advice—andusually gets away with it.
References
1. Hackett PH, Roach CR. High-altitude illness. N Engl J Med2001;345:107–14.
2. Clarke CRA. Three journeys to high altitude: medicine,Tibetan thangkas, and Sepu Kangri. J R Coll Physicians Lond1999;33:78–84.
3. Braham T. When the Alps cast their spell. Glasgow: The InPinn; 2004.
4. Mosso A. Life of man in the high Alps. London: Fisher Unwin;1898.
5. Roach RC, et al. The Lake Louise AMS scoring system. In:Sutton JR, Houston CS, Coates G, editors. Hypoxia &molecular medicine. Burlington, Vt: Charles S. Houston;1993. p. 272–4.
6. Houston CS. High altitude pulmonary oedema. N Engl J Med1960;293:478–80.
7. Houston CS, Dickinson J. Cerebral form of high altitudeillness. Lancet 1975;2(7945):758–61.
8. Coffey M. Where the mountain casts its shadow. London:Hutchinson; 2003.
9. British Mountaineering Council Information Service: www.thebmc.co.uk
10. Purkayastha SS, Ray US, Aroroa BS, et al. Acclimatisation athigh altitude in gradual and acute induction. J Appl Physiol1995;79:487–92.
11. Clarke C, Duff J. Mountain sickness, retinal haemorrhagesand acclimatisation on Everest in 1975. Br Med J 1976;2(6034):495–7.
12. Pollard AJ, et al. Children at altitude: an internationalconsensus statement. High Alt Med Biol 2001;2(3):389–403.
13. Basnyat B, Murdoch DR. High-altitude illness. Lancet 2003;361(9373):1967–74.