Embed Size (px)
Citation preview

1
HIE Community Meeting #3 2/1/2012
North Bay Administrative Center Fairfield
Introductions (In order of seating) Dave Minch, HIPAA/HIE Project Manager, John Muir Health (in the East Bay) Part of HealthShare Bay Area Getting MOU signed and getting our checks in Lyman: Dave Minch is here as subject matter expert on HIE. Dave is the chair of the national HIMSS HIE organization. Stephen Betz, Assistant Director, Solano County Health and Social Services Have task to implement EHR in Solano County. We have 2 systems, one for mental health and one for primary care clinics (Next Gen) Joined through Cal eConnect consortium of counties to build an HIE system to pull in lab results, public health lab results and share that. Our dream is to share at least with all EDs in the county the public health lab results. Rick Llewelyn, IT Director, Network Operations, NorthBay Healthcare. Justin Graham, Chief Medical Information Officer, NorthBay Healthcare Mark Street, Chief Technology Officer, Alliance Medical Center, Healdsburg Implemented EPIC last year Receiving lab results for past 3 years HIE facilitated by Will Ross, Redwood MedNet Soon to get ED summaries form local hospitals Challenge getting our data out of epic into HIE We have med history in HIE It is hard to work with vendors to get the data out Will Ross, Project Manager, Redwood MedNet, Ukiah Carl Spitzer, CMIO, Marin General Practicing ER doc Early in evaluation of HIE Kathy Horan, MD, Family Practice, EHR Champion, Sonoma and Lake County Regions fo Sutter in West Bay

2
Jack Horn, CEO, Partnership HealthPlan of California Medi-cal managed plan in 6 counties Interested in seeing what can be done We are a small part of most hospital and physician practices With more EMR coming, see an opportunity to capture information for better management of patient care. We are very supportive of this process. Robert Moore, Chief Medical Officer, Partnership HealthPlan of California Meg community health centetr contac costa planned parenthood all are in some stage of rolling out NextGen anxious to conntrect wiht epic and all of the other system Robert Sullens, EHR Project Manager, Solano County Mental Health Department Just implementing EHR system. Marty Malin, Interim Manager, Mental Health Services Act, Solano County I work with Robert Sullens. Kim Ortiz, Consultant, Work with Cal eConnect Formerly head of the Office of Health Information Technology for the State. Suzan Elliot, Clinic Administrator, Touro University Medical Center Soon merging with Solano County Clinics. Bring forward IT to our students and university. Use IT as education tool for our physicians of the future. Liz Gibboney, Chief Operating Officer, Partnership HealthPlan of California Laura Landry, Interim CEO, Cal eConnect Ran Western Health Information Network, nee Long Beach Network for Health, an HIE in LA and Orange Counties area Rim Cothren, Chief Technical Officer, Cal eConnect A developer of the NwHIN. We stitched together 3 different HIE's. The largest HIE implementation in the DoD. Rachel Olmedo, Cal eConnect Suzanne Ness, Regional Vice President, Hospital Council of Northern & Central California Juel Bortolussi, Project Manager, SJHS Sonoma County HIE projects

3
Kathy Ficco, Executive Director, St Joseph Health System, Sonoma County With Juel’s support we are in the process of connecting with some of our providers Currently delivering lab results. A goal we are working on is Allowing MD to place lab orders in the Meditech system. We don't want to see doctors printing orders and faxing them. We are actively engaged with Redwood MedNet to transfer discharge summaries. We as a group need to decide what is the “it“ we can do together to better take care of people. Cynthia Solomon, CEO, FollowMe, Inc. A personal health record company with a focus on PHR for vulnerable populations. Deal with foster youth. Many of our patients access many many health care systems and none of those connect so HIE is central for consumer-centric care. Cindy Melody, Executive Director, Marin Sonoma Medical Society Responsible for Marin, Sonoma, Mendocino and Lake medical societies. Maryann Eckhout, Executive Director, Napa and Solano Medical Society We have MDs in different modes of practice. They all can't talk to each other and THAT’S A PROBLEM. Elisa Ashton, California Health and Human Services We administer the grant that came from ONC to support HIE and incentive programs. California is one of 5 challenge states. We were drafted to participate in and take info we learn in settings like this to feedback to ONC so they understand why we aren't Rhode Island. Rhode Island has 100% of their 91 pharmacies and their 9 hospitals connected and we don't. We have weekly calls with them and with CMS. We will educate them on provider organizations. Not everything gets into small, medium and large organizations in California. They will get to listen to what real people are doing so we can educate the ONC why it's more challenging in California. Partners in e. Promoting the adoption of EHR technology if there is a safety component to it. Issues about e-Prescribing. Collect info about some of the unintended consequences of rapid adoption of technology. Connect to vendor or software. Building policy at state level around this adoption. Scott Christman, Health Informatics Director, Adventist Health Now focusing on hospital ambulatory. Will focus on clinics in St Helena region later this year. Melinda Miers, Adventist Health Focus on Cerner and affiliated MD EHRs.
4
John Wise, IT Manager, Sonoma County Department of Health Services Don Hitchcock, MD, Queen of Valley Medical Center Craig Lindquist, MD, PhD, Medical Director, HHS Clinics, Marin Health and Social Services Department of Health We are in the very early phase of thinking of HIE in Marin County. Carl Thomas, Interim Executive Director, Solano Coalition for Better Health Have most of the top leadership of health care delivery participating in Solano County Sundeep Desai, MD, CMIO, Sac Sierra Region, Sutter Health What will happen first? The enterprise HIE or the community one? Dan Glaze, Consultant, Program Manager for HIT Coordination for the State California Health and Human Services Create and fund organizations such as Cal eConnect Hope to continue to provide resources for this kind of meeting. You have lots of qualified experiences resources sitting all around this room. We have plenty of templates to work from. The issue is deciding what is right for this region and this unique configuration of trading partners. You are not the first ones to go through it. We are here to support such efforts. Cal eConnect has assembled through Laura’s leadership an excellent staff. They have the skill sets to provide assistance. Mark Elson, Chief Program Officer, Cal eConnect You are fortunate to have Lyman Dennis in the room to coordinate this process. Juel Bortolussi, Business Systems Analyst, Information Technology Services, St. Joseph Health System Lyman Dennis, Organizer and Facilitator, Principal, El Dorado Health Consulting
Service Areas for Inclusion in Project: Sacramento, Yolo, Other Lyman Dennis, Organizer / Facilitator The Dartmouth Atlas is a national database documenting healthcare regions by looking at Medicare referral patterns using two case types:
Major cardiovascular surgery

5
Neurosurgery Using this approach, the Dartmouth Atlas aggregates 3,436 hospital service areas into 306 hospital referral regions. In the slightly-simplified diagram below, several split counties are treated as full counties.
Sacramento is center of 10-county service area so inclusion of Sacramento in the NE Bay HIE project would require adding all the counties referring to Sacramento hospitals which would change the character of the project. Recommendation: Omit Sacramento County. Yolo County is part of the Sacramento service area per the Dartmouth Atlas. On the other hand, for Medi-Cal services, Yolo County is part of the Partnership HealthPlan of California service area. The Communicare community clinics use the Sonoma-based Redwood Community Health Network for their eClinicalWorks information system. Recommendation: Retain Yolo County.

6
We can expect in time that some HIEs will communicate readily with other HIEs serving the same or bordering areas. The areas will coalesce in due course. Jack Horn. “One possible approach is to continue reaching out to a larger group of counties until we solidify a plan and see the total scope of what is involved. Then counties may want to be in or out.” Lyman Dennis. Speaking of reaching out, we do have visitors from Marin and Sacramento at this meeting. Laura Landry, Cal eConnect. There is some activity going on in the Sacramento market now. Providers will shift around and select in or select out based on their business model or their organizational readiness. We may be surprised by what emerges.
Presentation by Peter Mathews, MD, Kaiser Permanente Napa. Health Information Exchange: What’s in it for Patients? A Physician’s Perspective. I am speaking from the perspective of a clinical informatics doctor which I have been doing in Kaiser for about 20 years half-time and from a person who has been an primary care physician, an internist, in Napa for the past 20 years. I have been dealing with patients who also have care in nursing homes, the VA facility, acute care hospitals and from their homes. They move all around with their clinical information and some of the information is legible and some of it isn’t. We will be discussing why what we are doing in this room and the community has importance for patient care. At the end, I will show you how the various Kaiser organizations share data with each other. Definition. HIE is the secure sharing of standardized healthcare information among individual patients, acute care hospitals, long-term care facilities, pharmacies, labs, and radiology organizations. For what purpose? To support quality, service and cost. We all know about the problem with ever-escalating cost of healthcare in our country. The ultimate goal is to improve the care of our members and our communities. I would like to make the case with some examples from my own practice as to how exchange can help in this way. The article being circulated, “Transforming Health Care – The Role of Health IT” is from the Internet. It was published in January. Link below: http://www.bipartisanpolicy.org/library/report/transforming-health-care-role-health-it This is a free 40-page report on the state of health informatics in this country. The key attributes of high-performing organizations are --
Organization wide focus on the needs of the patient

7
Strong organizational and clinical leadership Access to information to support EFFICIENT, COORDINATED CARE Timely access to care Emphasis on Prevention, Wellness and Healthy behaviors
The key opportunity among these five is the third, “Access to information to support EFFICIENT, COORDINATED CARE.” Patients move among all the different entities. They have lab work done here, they go see a primary care doctor, they go to a specialist, they might be in an acute care hospital for a few days, and then they might go to a skilled nursing facility. This is typical of the sick older patients. Then there are the younger patients who may have had their preventive care done in one place; then they lose coverage. When was their last Pap smear? When was their last mammogram? What were their last immunizations? Things fall through the cracks so we don’t really achieve efficient coordinated care. This is what we are trying to correct with the efforts at health information exchange. What we want to do is improve the quality of care so that unnecessary stuff is not done, so that the right stuff gets done, and we don’t do harm to our patients because we did not pick up information that the last healthcare provider knew about -- an allergy to a medication or overuse of a medication or a prior procedure that the patient had. If you share data, then you can do all sorts of fancy stuff, but I am going to skip that. What kind of patients will we take care of? Preventive care? Healthy care, basically. Patients up-to-date on Pap smears and mammograms, colorectal cancer screening, cholesterol screening. Changes in coverage may interfere. Does this make a difference? Well, it can, if you are the one who gets advanced breast cancer because you did not get your mammogram done. So the passing of routine, healthy preventive health information has value in preventing that kind of burden of unnecessary cancers and heart disease that could have been picked up if we did our screening lab work, immunizations, etc. If you move up the scale, the next most important group are the chronic disease patients. These are sicker patients who are going to utilize more costly resources, costing all our organizations more money, causing more side-effects for the patients. For diabetes, we have pretty good standards of care: the patient should have good blood sugar control, should have cholesterol under control, etc., etc. Well, again, patients don’t always stay with one healthcare organization so they can be in my organization, Kaiser, one year, and a few years later they can be somewhere else. Maybe they have their lab work done and maybe they don’t. Maybe their labs were under control and maybe they weren’t. But can we as a community capture when our members and our patients are overdue or out-of-control and intervene? Do patients remember this stuff themselves? Not necessarily. So getting this type of chronic disease information shared among our organizations will improve patient care. This will help control diabetes, high blood pressure, etc. Where most of us spend a lot of our time and where the high cost is for people in the last 6 months or the last 1 to 2 years of their lives. These are the patients who are constantly moving around our healthcare system – going from the primary care doctor to the specialist to the acute care hospital to the nursing home. They will invariably be seen in the ER and their record

8
may not be available. Maybe someone in the healthcare system did a good job and captured what the patient wants in an advance directive, that they don’t want aggressive care, that they don’t want to be on a breathing machine, that they don’t want to have resuscitation, but unless we have the ability to capture and share that information, then bad things can happen. The patient can have a long hospitalization and intubation – which is both costly and not what the patient wanted – because we don’t capture and share that type of information. What information to capture first. I pretty much have a geriatric practice and I want to give you some examples. Patients come to me all the time – acutely ill. They were seen at the local emergency room and three days later I need to obtain their EKG because they are still having chest pain so I can compare it. You do it today by fax. Maybe they were seen in the emergency room and they were allergic to a medication but the patient doesn’t know what it is and they give him the same thing and he has a reaction and ends up in the hospital. In all these examples, we can improve the health of our patients and reduce cost and improve quality if we capture some basic information, eventually, lots of information, but there is high value in certain pieces of that information. I am going to give you my two cents as to what those early pieces of information should be that will really benefit the health of our community and reduce a lot of bad things that happen to patients because we don’t capture data properly. So, who needs the information? You all know who needs the information. The patient needs it. The primary care physician or nurse practitioner needs it. The referred-to specialists need it. Labs pharmacies and radiology, health plans, long-term care facilities and hospitals and emergency departments need it. The list goes on-and-on but these are main parties. It would be great if we had all the information. But where is the bang for the buck? What will make the most difference in the early days? We can add more and more over time. I think Dave Minch mentioned these at our last meeting:
Meds
Labs
Radiology These are a great place to start. That is where we started many years ago. Then
Problem list, especially if you can attach comments to it. What are the main illnesses the patient is dealing with? Maybe it is high blood pressure. Maybe it is diabetes. Maybe they have had gall bladder surgery. A simple problem list is a great place to start if it is accurate. If you can embellish that list, it is better. For example, the patient has coronary artery disease but they also had a stent put in at Queen of the Valley hospital in April 2009. That is better. And they are on Lovastatin to reduce cholesterol. That kind of staccato summary of the patient is tremendously valuable. Not a lot of information but very good.
Screening. A record of some of their screening results – Paps, mammograms – is very helpful. The last colorectal cancer screening, whether colonoscopy or hemoccult testing. Etc.

9
Advance directive. In elderly patients like the ones I see, at least a pointer to where the advance directive is available. In this era, for Medicare beneficiaries, some 25% of healthcare costs are expended in the last year of life. (Christopher Hogan, June Lunney, Jon Gabel and Joanne Lynn, Medicare Beneficiaries’ Costs Of Care In The Last Year Of Life. Health Affairs, Vol 31, No 1, January 2012.)
If good doctors and good health plans capture this information and make it available throughout the community, patients can get the care they prefer and not procedures they do not elect. If patients have filled out an advance directive and we have a good information architecture, when someone call “911” for the patient, then the patient doesn’t get intubated and they don’t get put in the ICU and they don’t get put on breathing machines. The patient’s wishes are respected and, guess what? It saves gazillions of dollars appropriately with good medical care. It is very delicate how you do this but it is very important.
Key transcriptions. Emergency room discharge summaries, hospital discharge summaries or nursing home discharge summaries are of disproportionate value.
If you have these pieces of information, you have a great deal of help. There are other things you can add on as you move further up the road – prior EKGs, etc. But if you start with this or a portion of this and build toward this, you are well on your way to improving care and reducing cost and reducing undue harm to all of our patients.
I have some scenarios here but I have already pretty much gone through them so I am going to skip them. So how do you sequence exchange in a way that make sense?
Labs
Radiology
Medications. Meds are harder because there are a lot of pharmacies. Then a little bit of clinical information. You are going to have to have providers feed that in in some fashion.
Allergies
Problem list – preferably a smart problem list. I will show you some examples in a moment.
These elements will be a great place to start community-wide.
Advance directives – somehow get these in very fast. They are really important for doing the right thing.
Key dictated items – discharge summary, operative note, history and physical. Any physician in this room that is looking through someone’s chart is looking for transcribed information that we can read. I received notes from a doctor in private practice yesterday. The doctor did not have good handwriting. I could not make anything out of it. The big bang for the buck: physicians in the room, you are looking first for transcribed stuff, right? First thing. That is the low-hanging fruit. Transcribed ED reports. Things like that.

10
This is the new world, right? We have smart phones, iPads, things like that. Social networking and things like that. Who knows where all this will be taking us beyond where we are with the electronic health record today. The world is changing very fast. It is a very exciting time as technology hits healthcare. Now I will show you some screen shots of shared data. We use the vendor Epic and we call our version Health Connect. The first screen is our snapshot screen, our summary clinical record.
This has the information I just mentioned, pretty much – problem list, immunizations, medications, habits, and allergies. It does not have lab results or radiology on this particular screen. This is an example for a fake patient I created of an an annotated problem list.

11
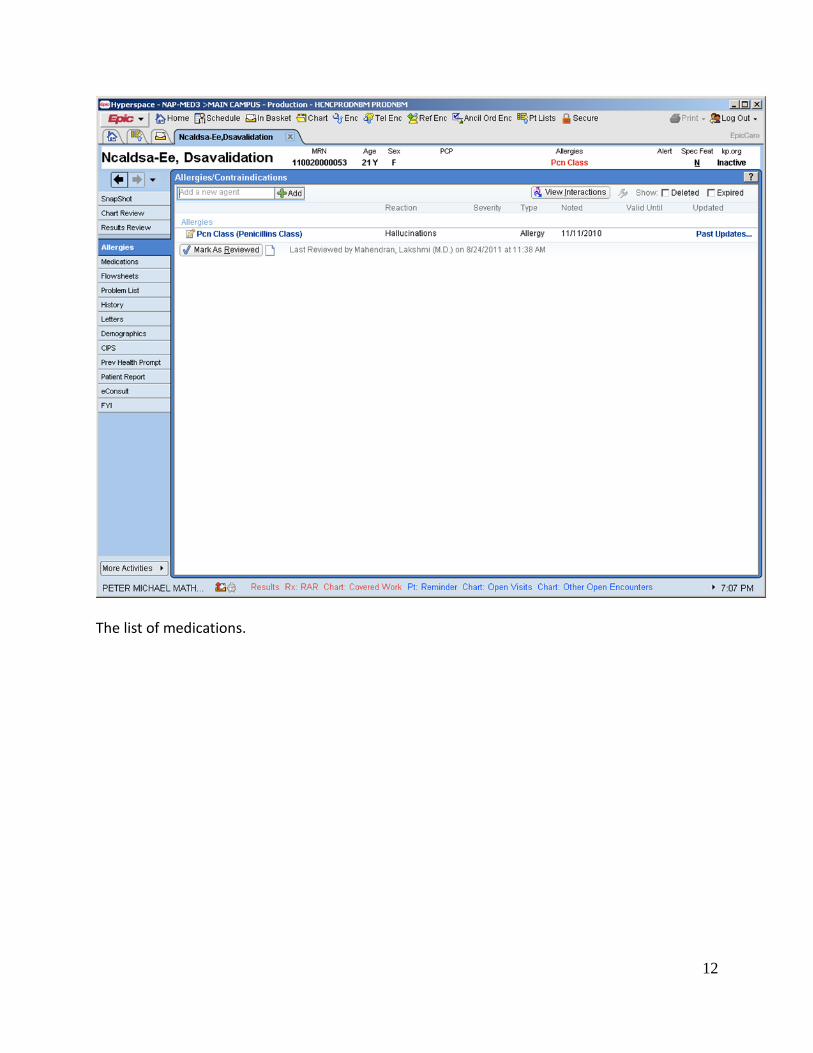
I put editorial comments about key things about this patient. I put down “Life Care Plan,” essentially the advance directive. This is a 21-year-old but pretend it is an 80-year-old. The existence of a Durable Power of Attorney for Health Care and their wishes could go there. Then the diabetes condition, their last blood sugar, their medications, etc. For hypertension, I recorded the medicines she is on. For screening, I indicated status on colonoscopy screenings, an example. This shows the bang-for-the-buck of having an annotated problem list for a patient. Then I have screens from our system. An allergy screen.
12
The list of medications.

13
Overuse of prescription medications is becoming an issue. We need to do a better job of assuring that we do not over-prescribe. Not just a list of medications but an indication of how often filled. If inhalers for asthma patients are filled too often, it means that they are not on appropriate other medications. This is a screen from our legacy preventive prompting system which is pretty much a list of last Pap, last mamo, last immunizations, blood pressure, and things like that. This shows when these interventions are next due as a guide to both the provider and the patient.

14
The immunization screen is particularly important for pediatric patients but for adults as well.
The next screen tracks vital signs – weight, blood pressure, lab results, etc. These are very simple to capture and very important.
The next screen is a comparison of cardiac studies. Very important when you are able to capture this information.

15
We capture the advance directive and then scan it into our system today. The fact that it exists in noted in the electronic health record and the actual directive can be read from the scanned form.

16
These are a few sections of our existing health care system as examples of good places to start in the community to make a difference in patient care. Data exchange at Kaiser. My last set of slides show something we implemented in the last three months or so. There are six Kaiser regions: Southern California, Northern California, Mid Atlantic, Colorado, Hawaii and Oregon. Each region has the same vendor, Epic, but when we went live, we could not initially exchange records. But we got to that point about three to four months ago. So now, if a Kaiser patient comes into my office who has previously been seen in another Kaiser region, I say, “great”. “I will pull up your record.” We have the advantage of sharing the same medical record vendor. Pretty much, we have a view of the entire medical record. I can’t write orders or notes in the Southern California region system, but I can pull up everything that has happened there. I will show you screen shots of what the clerk or I would do to pull up the record and then I will show you want the record looks like. Pulling up the record (2 slides):

17
What the record looks like (3 slides):

18

19
The scenario is a Kaiser pateint from Southern California who visits Napa on vacation. He gets chest pain and visits a Kaiser doctor in Napa (me). I query Southern California regions through Care Epic, give a reason for the query, hit the button, and in about 2 minutes, the system pulls the medical record from Southern California into our system in read-only mode. We have decided that for these types of situations, we do not need a written authorization from the patient but we could requrire a written authorization. We end up with the record. The record is the ususal summary (slides shown above) followed by inpatient care, etc. This is the end game in short term. But the game is changing. The organization just bought us iPads. Today I did prescription refills from Starbucks. Members just in the last month have access to our website from smart phones. How will we eventually interact with Facebook, Twitter, etc.? We can make a real improvement in care if we just start working together and get these early pieces in. What are we going to accomplish? We are not going to do harm to patients because the next provider does not know what the previous provider did. The prior provider knew the patient was allergic to penecillium but we gave it to them anyway because we did not know. The patient had an advance directive but no one knew it so we intubated him. Stuff like that. The patient came in with an abnormal EKG but we don’t have access to the prior EKG so we don’t know that it is exactly like the last EKG. By working the system, we can get this, by calling over, but we are so busy…. And there are a lot of preventive things that fall through the cracks. The patient did not get a mammogram and presents with advanced breast cancer. The patient did not

20
get colorectal screening. The patient thinks it was three years ago but it was seven years ago and the patient gets cancer and dies. There is a lot of good stuff we could do to improve care, to reduce costs and make things better. So, begin at the beginning. Med. Lab. Pharmacy. Problem list. Allergies. That is not a bad list. We can do that. Then the next phase. Add some transacriptions. Start at the hospitals. Start in the ED. Thank you very much.
Mission Statements (Changed from “vision statements” as more “mission”-oriented) H. Martin Malin, PhD, MA, MFT Interim Mental Health Services Act Coordinator Solano County Health and Social Services Tim Wilson, PhD Epidemiologist Yolo County Health Department We looked at the mission statements of successful HIE's. The following is the start of a mission statement: To improve individual health outcomes in the NE Bay area
Support continuity of care
Promote appropriate clinical decision making at the point of care
Make information available and useful
Improve patient safety
Improve and enhance the patient/clinician experience
Support achievement of systematic goals such as o clinical analytics o population health management o implementation of best practices
Reduce adverse outcomes and cost associated with
Treatment decisions made based on incomplete or patient-recall data when better data is available
Lack of patient engagement in their own healthcare due to lack of understanding of key health drivers and test trends
Provide connector technology that Reliably exchanges Physical health

21
Mental health Alcohol and substance abuse information among providers Rapidly provides requested data Anticipate connection with other HIE's regionally and nationally
What do we want the group to accomplish? Lyman Dennis, Organizer / Facilitator
We need HIE for the 3 stages of meaningful use incentives.
We need HIE economically for ACO movement so that ACOs can have managed care across organizations and providers can earn incentives.
Providers need it to be competitive as patients like the benefits of electronic care: eMail providers, electronic lab results, online prescription refill, all medical records available in one place, preventive prompts,….
Providers need to reach Stage 7 of EMR adoption for quality improvements and cost savings.
Why HIE? Rationalize medical care
Allow continuity of care across providers
Provide all clinical data at point of care
Support evidence-based medicine by allowing review of more info about each case
Reduce duplicate testing
Support ACO reimbursement incentives Options for the Community Group 1. Do nothing - disband. 2. Set up full HIE organization and business. 3. Set up an organization to contract for HIE services. 4. Set up a collaborative to coordinate the contracting for services. Example: Solano Coalition for Better Health set up Partnership HealthPlan of California in 1994. Option 1. Do nothing.
HIE will develop chaotically and without plan for integration.
Analogous to unplanned ER services. Competition for victims or no ambulance when needed.
Likely to be o more expensive o contain gaps

22
o have unlinked HIE service silos Option 2. Build a full HIE organization and business
Time is past when a full-service HIE (like Santa Cruz HIE can gain all the exchange services for a county or group of counties. The counties already have distinct functions and HIEs operating.
Cost of a full HIE is relatively high – staff, policies and procedures, hardware, software, infrastructure, etc.
NOT NECESSARY AS LESS-EXPENSIVE ATERNATIVES AVAILABLE Option 3. Set up an organization to contract for HIE services
LIKE HIE set up in inland empire
Existing HIE and vendors provide this service
Having a community organization do this allows
negotiation leverage
economies of scale
a forum to agree on a common approach
a way to coordinate community resources related to HIE Option 4. Set up a collaborative to coordinate contracting for services
Light organization like the Solano Coalition for Better Health
Bring community together and develop a coordinated plan
Negotiate with each other on how it should be done
A community voice When we get to stage 3 of meaningful use, that will not be the end. Sharing the data you get from implementing EHR's. The true values of getting rid of the silos. Transformation in the way we pay for health care. Canada has a different perspective on health care. HIE has become their EPIC -- their clinical record. They refer to their HIE system as their electronic record system. They look to the HIE to be the longitudinal record. The way they assess health care. The way they manage life care as opposed to a given encounter. In performing life care, they have to look across the encounters. Once we understand what an ACO is and what information we need to pull together across different settings, many of which the ACO does not control.
23
Labs The business use case was to reduce the cost of transmission of lab results. There were costs associated with every one of those manual steps. We can deliver those results electronically to a portal and you can get all of those results in once place. We have to demo the real value. HIE Comments by Laura Landry All of the players in room have effective and efficient decision making process so HIE can develop at the speed it needs to in order to meet organizational needs. Mary individual organization needs to community decision making capacity and you want to drive them at the same level. Weigh efficient and effective nonpartisan decision making and also the development of trust. Everyone has their own business need. We will need to balance community health center needs against the large medical centers. These kinds of discussions are those we will need to address. How do we as a community come together and make decisions? Look at it from worst case scenario. When different parties have different points of view, how will you resolve the discussion? Harder to do if you don't have a corporate umbrella. In order to sign an agreement we needed an umbrella organization, a legal entity and a board with authority over the program. The group needs to address governance and decision making. Lyman Dennis. In the Inland Empire, the nonprofit medical society incubated the HIE. Justin Graham. The vast majority of HIE's have failed. The business model and decision making need to come to a common purpose as the first step. What are the reasons for failures? We want to determine that we are not on this path before we lend resources to it. If any of us want to build ACO's we will need some form of HIE Stephen Betz, Solano County. Economies of scale are an issue with us. If we could agree on one HIE structure it would save a lot of money. Solano County Board: “When will you have it?” The boards are interested in good patient management. Round 1 in San Francisco. Everyone at the meetings were in agreement, but no one briefed the CEOs. When time came to sign agreements, the CEOs said, “What is HIE?” and “Why didn't you tell me about it?” Round 2 with Alameda Contra Costa is proceeding better. Coordinating Committee. When you go back to your organization, TALK to your boss about what happened here so that we won't have another SF. At some point, the HIE organization will either have to pay for contracted HIE services or contribute in some other way.

24
HIE is important to the future of the provider organizations. Cal eConnect will help the group with information about existing organizations. What is HIE? What should we do about it? Why should you think about HIE when you build your EHR?
Organization Approaches Carl Thomas Interim Executive Director Solano coalition for Better Health Lori Sklar Executive Director Redwood Community Health Network (not present) Nonprofit structure seemed to be the best structure to go with. It kept the influential stake holders involved in decision making. Allows application for grants. Nonprofits had proper balance of moving everyone along and taking into account everyone's needs equally. Data Sharing
What data is shared?
When it is shared?
Who would benefit from data sharing? Avoid pioneering
Build on experience of other groups.
Begin with available documents.
Don’t redevelop successful work of others.
Utilize best practices. Two board structures in California Cal eConnect has 22-24 board members. Board members all interested and engaged. Has good balanced mix of CIOs, CEOs

25
Redwood MedNet has 8 people on the board. A mix of skill sets and interests. You will have to figure out what works for this area. You may not have two Sutter groups.
HIE Service Offerings by Category Paul Alcala, VP CIO NorthBay Healthcare Dave Minch, HIPAA/HIE Project Manager, John Muir Health Kathy Ficco, Executive Director, St. Joseph Health System Justin Graham, MD, CMIO, NorthBay Healthcare Lyman Dennis, Organizer / Facilitator Basic “Core” Services Foundational Services
Master Patient Index
Record Locator
Provider Directory
Entity Directory (Hospitals, medical groups, etc.)
User Directory
Other Directors (clinics, public services, registries, non-participant message destinations, etc.)
Authentication/Authorization Methods
ATNA Standard Transaction and Use Logs Transaction services (hospital and ambulatory)
Inbound Interfaces EHR => HIE
Outbound Interfaces HIE => EHR Virtually all kinds of EHR's The community is more than hospitals and physicians. Touch on SNFs, schools for immunizations, public health immunization registries. Application Services
Consent Management (Opt-In, Opt-Out)
Secure Clinician-Clinician Messaging/Referrals
Gateways (NwHIN, other local HIE, state HIEs, Direct HISP, Immunization Registry, Public Health)
Portal To View Community Record
Results Distribution Specialty “Premium” Services

26
Physician EMR-Lite vs Costco EMR
Full EMR with HIE or Contracted Installation
Support
Other Physician Products (eRx, practice management, home device montiroing)
Personal Health Record (PHR)
Dictation Services
Disease Registries
Public Health and Immunization Reporting And Inquiry
Advance Directives
Group Purchasing Most HIE's started with grants. Some fail to engage the stakeholders and fail to find services that are of value to their constituents. Clinical Data & Workflow Clinical Information
Diagnosis / Problem List
Allergies
Laboratory Values
Radiology Transcription
Discharge Summary
Visit Summary
Immunizations
Medication Summary Workflow
Referrals
Authorizations
Encounters (ED, Ambulatory, Inpatient)
Transition of Care Support
Home Health Reporting
Image and Other Dx Reporting Physicians are really busy. EHR workflows can only be assisted with something integrated into the clinical and administrative workflows. More and more hospitals are choosing Epic. Why? Not because of the product itself but because Epic has studied clinical workflows very well and very deeply and Epic figured out how to make sensible workflow happen within the context of an EHR. Physicians use HIE almost as an extension of the EHR

27
Clinical Management
Clinical Quality Reporting
Clinical Disease Registries
Chronic Disease Management and Reporting
Immunization Registries
Syndromic Surveillance Reporting and Monitoring
Clinical Decision Support Management Analytics
Insurance Claims Analytics
Regional Population Analytics
Clinical Trials Data Base
Public Health Case Mgmt
ACO Metrics Dave Minch. John Muir Health started its own HIE with a vendor in 2007. We connect all of our IPA physicians and we connect with Hill and share a lot of data with them. It's a private HIE. We decided 2 years ago that we would not achieve community integration of clinical content by running our own private HIE. Now, John Muir Health is with HealthShare Bay Area (HSBA) setting up community HIE in a way very similar to what you are doing now. This involves community building and interest building. It's a difficult undertaking but it is very worthwhile. We know we will have to play in ACO world. Data Accessibility Patient Community Record
Hospitals / Acute Care
Ambulatory / Outpatient Clinics
Home Health / Rehab
SNF / Long-Term Care
Care Continuum -- Merged Encounter Data Financial and Administrative Services
Claims Processing to Payers -- Emdeon claims clearinghouse
Eligibility Verifications
Remittance Advice Processing
Physician Credentialing Services
Billing Services
Attachments
28
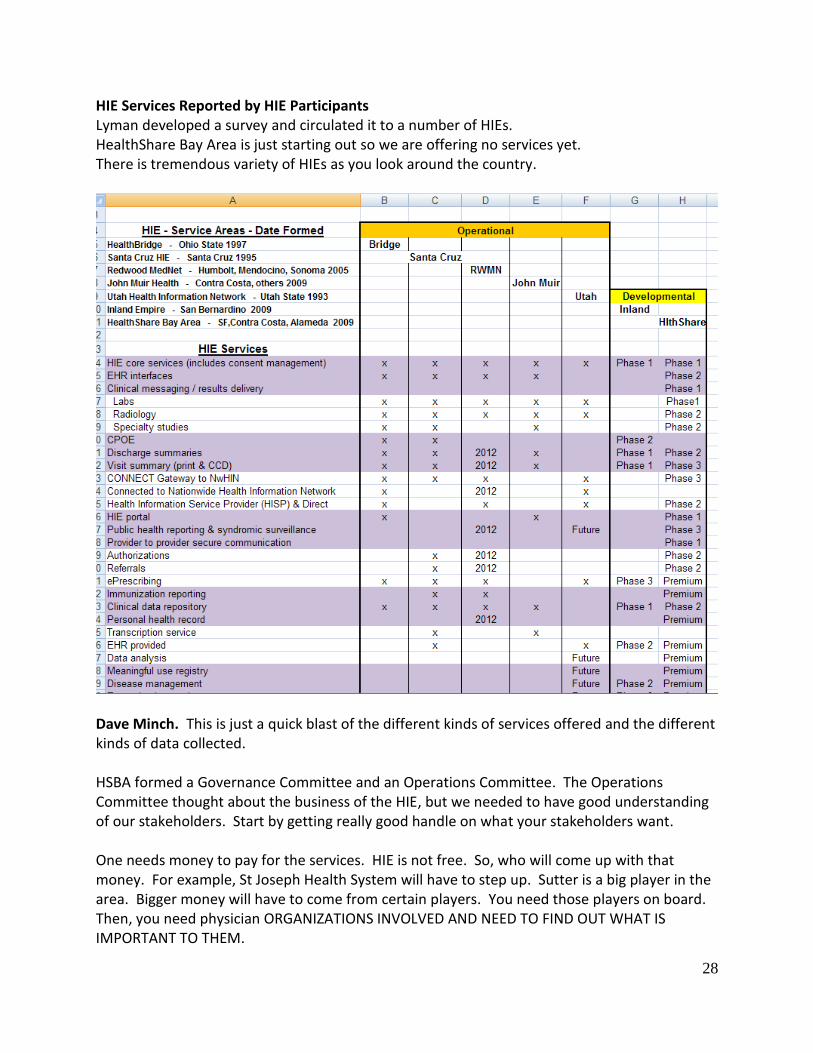
HIE Services Reported by HIE Participants Lyman developed a survey and circulated it to a number of HIEs. HealthShare Bay Area is just starting out so we are offering no services yet. There is tremendous variety of HIEs as you look around the country.
Dave Minch. This is just a quick blast of the different kinds of services offered and the different kinds of data collected. HSBA formed a Governance Committee and an Operations Committee. The Operations Committee thought about the business of the HIE, but we needed to have good understanding of our stakeholders. Start by getting really good handle on what your stakeholders want. One needs money to pay for the services. HIE is not free. So, who will come up with that money. For example, St Joseph Health System will have to step up. Sutter is a big player in the area. Bigger money will have to come from certain players. You need those players on board. Then, you need physician ORGANIZATIONS INVOLVED AND NEED TO FIND OUT WHAT IS IMPORTANT TO THEM.

29
Then, after understanding those two things, you can start putting a business plan together. When HSBA got back to business plan, the process went much more smoothly. Laura Landry. Everyone starts form a different place. Utah started with a claims clearinghouse. Prior to the clearinghouse, doctors weren't paid for 60-90 days. They had that pain point. They prioritized prompt payment and cut payment time down to 5 days. Everyone has problems with long-term care transitions. Start by looking at the edges of your systems and the pain points you have there. Everyone has some of the same problems. Many organizations don't have the right technology to support some functions. Home Health agencies don't have the required technology. If John Muir can't get what it needs at the edges of its system, that's a very personal organizational thing. That’s where you will start. What are your 1 to 5 pain points in your organization? You will make progress on one thing that will bubble for a while. Then you make progress on another thing. If everyone identifies 3 to 5 issues, you probably will have 2 to 5 overlaps. Don’t forget your payers. Your payers have problems that they would like for you to solve. In order to solve a problem for them, you have to understand how they would like it to be solved. That's how you cut out some of the time from the 18-20 months of planning. Ask the right questions first.
Models for Funding HIE Activities Suzanne Ness Regional Vice President Hospital Council of Northern & Central California Funding for Project
Assume beginning as a collaborative or contracting entity, not a formal startup HIE.
Long organizational road to be a full HIE & not necessary.
Better to
Contract for services or
Coordinate provider services so community exchange model makes sense. Funding Models (for Full HIEs, as that is what is out there) HealthBridge, Cincinnati
Founded 1997 with $1.75M in unsecured loans from

30
Two healthplans
Five hospitals $250k each
All loans repaid on time, continuous operation 14 years
Sustainable without grants (5% to 8% annual return; only 3% from grants) Santa Cruz HIE
Bill Beighe, CIO
Founded in 1995 by Physicians Medical Group of Santa Cruz, Dominican Hospital and Unilab (now Quest) as a for-profit
$300k to $500k from each partner, given to Axolotl to develop software.
Driven by physicians. Hospitals, clinics, the jail, and behavioral health pay in. 70 points of care, each contributing. Redwood MedNet Will Ross, Project Manager Western Health Information Network (nee Long Beach Network for health) Laura Landry, CEO (now Interim CEO of Cal eConnect)
Both had grant-funded startup.
Cal eConnect provided matching funds to both.
Both still grant-dependent but moving to user funding Funding Options
Grants – not sustainable permanently (CareSpark in Tennessee went under when its grants ran out.)
Transaction-based fees – discourage use of services
Subscriptions – best. No volume restrictions. HealthBridge, Santa Cruz HIE, Utah Health Information Network
Need insurers and labs at the table. In one model, first dollar saving goes to the insurers. Per MD per month core services - one methodology Examples of Subscription Charges (composite of several HIEs)
Per MD per month: core services, with additional cost for EHR ‘lite.’
Hospitals: by bed or occupancy, per month charge
Community clinics: a single MD rate, per location
Free clinics: free
Home health: annual cost based on revenue
Ambulatory surgery: based on number of MDs
Long-term care/post acute: annual based on number of beds
Independent labs: per ordering provider per month, per lab (Quest, LabCorp, others)

31
Pharmacy: per year, per location Sale of “Premium” Services One of the key sources of HIE income is “premium” services that can carry a charge to providers. See the list on the top of page 26. The sustainable HIEs offer a variety of “premium” services and are always developing more. What can the HIE do more efficiently than each EHR and charge enough to contribute to the bottom line but not so much that the service is not attractive to the providers. Vendor HIE Market There's a reason why our vendors don't want to connect to other systems. The vendors want to become HIEs. One vendor quadrupled the price for its HIE subscription in a few months. When there is growing market and customer demand, prices go up. Sonoma would like to hitch up with Cal eConnect because it is driving prices down, forcing vendors to draw down cost to grant funded programs. We demanded that we would be able to engage with other organizations in negotiations with the vendor. This community group will have much more leverage if we combine forces. Kaiser in the Bay area. Kaiser would not be a participant in HSBA for now. Kaiser has a closed environment. Kaiser pretty much control all of the different pieces of the care process. Dave Minch. An organization controls fewer of the pieces than you think you do. John Muir Health provides radiation oncology for the East Bay. But, patient docs want to know what we've done on radiation oncology. And John Muir docs want to know what other care radiation oncology patients are receiving. We have a lot of need for HIE. KP is one of the pioneers with HIE. They have active connection with VA in San Diego. They are sharing info with other organizations through Care Everywhere. They are sharing records. I see that sharing expanding. We will see at some point that Kaiser realizes they should join in community HIE. Kaiser is co-founder of CCC to accelerate the dissemination of HIE standards throughout the country.
New HIE Resources Dave Minch

32
HIMSS HIE guides and toolkit
eHI (eHealth Initiative)
Markle (Connecting for Health) all on the web - great legal section Alan Briskin and Jerry Hinkley.
NeHC University (National eHealth Collaborative)
Vendors (Webinars and supplied docs) vendors have pretty good compendium
NwHIN DURSA (Data Use and Reciprocal Services Agreement) - This will be foundation for HIE to inter-operate within California.
Information from other HIEs (on HIE web sites and in contributed documents) There is no single answer to HIE but there are a lot of approaches and a lot of ways to think about things. Lyman. Thanks to Dave Minch for all of his help. He always is available and he helps out cheerfully.
Next meeting Lyman Dennis Homework Look at mission, organization and budget for a couple of alternatives:
Contracting organization or
Collaborative organization Discuss alternatives and implications. We need to talk to each of the participating organizations to find t their priorities. We did this in the Inland Empire. Such conversations also attract interest in the alternatives. We could send out a questionnaire that looks at potential services. But it is probably better to sit down and talk with people to see what their pain points are. Dave Minch. We did leverage medical societies in the Bay Area and we always invited hospital council representatives. What would I have done differently? I would try to leverage the relationships the hospital council had with the chief executives to find out from the executives their hot buttons. What important issues are on their plates? Jack Horn. Could we get a table of contents for a business plan? Lyman. Will send out. We have to decide what problems we are solving and what problems we are going to address first.

33
Jack Horn. What kind of commitments will people have to make? Laura Landry. Down in LA, at each of our meetings we made it a point of having 1 hour of open discussion. The problem we were having was unanticipated problems. Some things could be solved without any technical intervention. You had to have the right people talking to EACH OTHER. You can develop business value in these meetings. Here is what we are struggling with. There are opportunities here. You can bring a lot of structure but there is also a requirement for less structure so you can see what comes up. If this was a science, we'd be doing it already. This is an art and we have to learn to do it. The impact of changed reimbursement associated with healthcare reform is a motivator for moving this along expeditiously. Every hospital across the nation is gearing up for the new payment model. We have to save 20% of our current expenses. Lyman. The incentives under the ACO model will be up to 10% of revenue. This REALLY MEANS THAT THE ACO will own your profit margin.



![Monitoring INMM-SNF 020112.ppt ... – Use of armed escorts ... Microsoft PowerPoint - Monitoring_INMM-SNF_020112.ppt [Compatibility Mode] Author:](https://img.pdfslide.us/doc/110x75/5ae9bbe57f8b9a585f8b6c79/monitoring-inmm-snf-use-of-armed-escorts-microsoft-powerpoint-monitoringinmm-snf020112ppt.jpg)

























