Embed Size (px)
Citation preview

HERSHEY MEDICAL CENTER EXPERIENCE WITH TIGHT
GLYCEMIC CONTROL
Robert Gabbay, M.D., Ph.D.Associate Professor of Medicine
Co-Director, Penn State Diabetes Center

Diabetes in Hospitalized Patients
• Fourth most common co-morbid condition among hospitalized patients
• 10–12% of all hospital discharges
• 29% of all cardiac surgery patients
• 1–3 days longer hospital stay
Hogan P, et al. Diabetes Care. 2003;26:917–932.American Association of Clinical Endocrinologists. Available at:http://www.aace.com/pub/ICC/inpatientStatement.php. Accessed March 17, 2004.

The Increasing Rate of Diabetes Among Hospitalized Patients
Hospitalizations for Diabetes as a Listed Diagnosis
0
1
2
3
4
5
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001
Hospital Discharges (millions)
48%
Available at: http://www.cdc.gov/diabetes/statistics/dmany/fig1.htm. Accessed June 15, 2004.

Potential Benefits of Improving Glucose Control in the Hospital
• Improving inpatient glycemic control provides an opportunity to– Reduce mortality– Reduce morbidity– Reduce costs of care
• Length of stay (LOS)• Cost of inpatient complications• Fewer rehospitalizations• Reduced extended care


Intensive Insulin Therapy in Critically Ill Surgical Patients
• Setting: surgical intensive care unit in University Hospital, Leuven, Belgium
• Hypothesis: normalization of blood glucose levels with insulin therapy can improve prognosis of patients with hyperglycemia or insulin resistance
• Design: prospective, randomized, controlled study• Conventional: insulin when blood glucose > 215
mg/dL• Intensive: insulin when glucose > 110 mg/dL and
maintained at 80–110 mg/dLvan den Berghe G, et al. N Engl J Med. 2001;345:1359–1367.

Intensive Insulin Therapy in Critically Ill Surgical Patients
van den Berghe G, et al. N Engl J Med. 2001;345:1359–1367.
No serious hypoglycemic events.
Conventional Intensive
Mean AM blood glucose achieved (mg/dL)
153 103
% receiving insulin 39% 100%
% BG < 40 mg/dL 6 39

Intensive Insulin Therapy in Critically Ill Surgical Patients Improves
Survival
van den Berghe G, et al. N Engl J Med. 2001;345:1359–1367.Copyright ©2001 Massachusetts Medical Society. All rights reserved.
Conventional: insulin when blood glucose > 215 mg/dL.Intensive: insulin when glucose > 110 mg/dL and maintained at 80–110 mg/dL.
Survival in ICU (%)
100
96
92
88
80
0
84
0 20 40 60 80 100 120 140 160
Intensive treatment
Conventional treatment
Days After Admission

Intensive Insulin Therapy in Critically Ill Surgical Patients: Morbidity and Mortality
Benefits
van den Berghe G, et al. N Engl J Med. 2001;345:1359–1367.
-60
-50
-40
-30
-20
-10
0
Reduction(%)
Mortality Sepsis Dialysis PolyneuropathyBlood
Transfusion
34%
46%41%
44%50%
N = 1,548

IV Insulin Therapy in Critically Ill Surgical Patients: Safety
• A titration algorithm achieved and maintained blood glucose levels at < 110 mg/dL
• Insulin requirements were highest and most variable during first 6 hours of intensive care
• Normoglycemia was reached within 24 hours with a mean daily insulin dose of 77 IU; maintained with 94 IU on day 7
• Blood glucose was monitored every 4 hours by ABG • Statistically significant, but clinically harmless,
hypoglycemia was observed briefly
van den Berghe G, et al. N Engl J Med. 2001;345:1359–1367.

Keys to Van den Berghe succcess
• 1 nurse to 2 pts
• Need IV glucose
• Benefit most for > 5 days in ICU (1/3)
• Number needed to treat = 29
• Karnofsky scores better after 6 and 12 months
• Studies in Europe in NICU, PICU, MICU

Indications for Intravenous Insulin Therapy: Summary
• Diabetic ketoacidosis• Nonketotic
hyperosmolar state • Critical care illness
(surgical, medical)• Postcardiac surgery• Myocardial infarction or
cardiogenic shock• NPO status in Type 1
diabetes
• Labor and delivery• Glucose exacerbated
by high-dose glucocorticoid therapy
• Perioperative period • After organ transplant • Total parenteral
nutrition therapy
American Association of Clinical Endocrinologists. Available at: http://www.aace.com/pub/ICC/inpatientStatement.php. Accessed March 17, 2004.

GETTING STARTED (1998)
• Define the problem
• Evaluate the evidence—CABG
• Evaluate Current Care
• Identify the Stakeholders
• Identify Barriers

Portland Diabetes Project: Mortality
Reprinted from Furnary AP, et al. J Thorac Cardiovasc Surg. 2003;125:1007–1021 with permission from American Association for Thoracic Surgery.
CII
10
8
6
4
0
Mortality(%)
87 88 89 90 91 92 93 94 98 99 00
Year
Patients with diabetes
Patients withoutdiabetes
2
95 96 97 01

Anthony Furnary MD 1999 CCNM
0.0
0.5
1.0
1.5
2.0
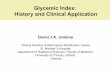
SQI CII
Deep Wound Infection Rate (%)
Furnary AP, et al. Ann Thorac Surg. 1999;67:352–362.
2.0%
0.8%
P = 0.01
SQI = subcutaneous insulin; CII = continuous insulin infusion.
Rate of DSWI Rates With Different Ins Protocols

CURRENT STATE OF CARE
• The infamous sliding scale
• Benign neglect
• Endocrinology consults on occasion
• Typical glucose monitoring every 4-6 hours

IDENTIFY STAKEHOLDERS
• CT Surgery
• Anesthesia
• Nursing Team
• Outcomes Research Team
• Endocrinology and Diabetes
• The hospital/payors

IDENTIFY BARRIERS
• Glucose monitoring
– Who?
– How?
• Understanding the rationale
• Nursing time and effort

DEVELOPMENT OF THE INSULIN INFUSION GLYCEMIC CONTROL PROTOCOL (IGCP)
• Multidisciplinary team led by Endocrinology
• Glucose meters needed to be available
• Goal 120-200 mg/dL
• Grand rounds and educational programs
• Evaluate outcomes

Endocrine Practice 10:112 (2004)

HMC IGCP Intervention
• All pts undergoing CABG
• Start IV insulin when present to anesthesia
• Continue IV insulin by protocol until taking po
• Endo consult to adjust insulin
• Multi-disciplinary team- nurses, anesthesia, CT surgery, outcomes research team, endo
Endocrine Practice 2004





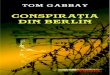
Histogram of all glucose levels in non-drip group and
insulin drip protocol
0%
5%
10%
15%
20%
25%
0 50 100
150
200
250
300
350
400
450
500
Glucose
Per
cen
t
No Drip
Drip

Our Analysis
• Financial data
• Costs incurred in 1999 normalized to the year 2000 (3% adjustment)
• Data collected from hospital’s cost accounting database and included following additional costs of IGCP:
– More frequent BG monitoring
– Pharmacy expenditures
– Routine endocrine consultation

COSTS
• Underestimated :
• Readmission
• Indirect costs, i.e., patient satisfaction, negative publicity and reduced referrals
• Risk of litigation


Mean
Variable No Drip (N=81) Drip (N=107)
Total Cost $21,442 $21,076
Total LOS 8.64 8.25
LOS (Surgery to D/C)
5.98
5.48
DSWI 4.94 % 4.63%

CONCLUSIONS
• Mean blood glucose improved from 241 to 183 (first 48 hours)
• Average number glucose determinations was 23.8 vs. 8
• Revenue neutral despite endocrine consults, pharmacy costs, pharmacy
• Cost offset by clinical improvement and overall cost savings
• Wide acceptance by nursing and docs

EVERYTHING CHANGES WITH THE VAN DEN
BERGHE STUDY

Intensive Insulin Therapy in Critically Ill Surgical Patients Improves
Survival
van den Berghe G, et al. N Engl J Med. 2001;345:1359–1367.Copyright ©2001 Massachusetts Medical Society. All rights reserved.
Conventional: insulin when blood glucose > 215 mg/dL.Intensive: insulin when glucose > 110 mg/dL and maintained at 80–110 mg/dL.
Survival in ICU (%)
100
96
92
88
80
0
84
0 20 40 60 80 100 120 140 160
Intensive treatment
Conventional treatment
Days After Admission

Getting to a Lower Goal

GETTING LOWER
• This should be easy?
• Shortcuts are not always shortcuts
• Better evidence
• Glucose monitoring a problem again
• Getting back to basics?

HMC New insulin drip protocol
• Based on evidence based work from Van den Berghe (NEJM)
• Refined by multi-disciplinary team

Key changes of new protocol
• Target BG range (80-120mg/dl)
• D10 NS at maintenance rate 50 ml/hour
• No automatic endo consult

Blood Glucose (BG)
mg/dl
Regimen #1For BG 110-219 mg/dl
Usual insulin dose <30 units/day orpatients using only oral agents whose glycohemoglobin is <8 or current blood glucose 110-219 mg/dl or
non-diabetics
Regimen #2For BG >220 mg/dl Usual insulin dose >30 units/day or patients using only oral agents whose glycohemoglobin is >8 or unknown orcurrent blood glucose > 220 mg/dl
Starting dose 2 units/hour 4 units/hour
If Initial BG decreases by
>50%
Decrease to 1 unit/hour Decrease to 2 units/hour
>140 Increase by 1unit/hour Increase by 2units/hour
121‑140 Increase by 0.5 unit/hour Increase by 1 unit/hour
80-120 Unchanged Unchanged
65-79 Reduce rate by 1 unit/hour Reduce rate by 1 unit/hour
40-64 Administer 12.5 ml of D50 IV, stop infusion, call physician, and re‑check BG in 15‑30 minutes. When BG >64 mg/dl, re‑start infusion at 50% lower rate.
Administer 12.5 ml of D50 IV, stop infusion, call physician, and re‑check BG in 15‑30 minutes. When BG >64 mg/dl, re‑start infusion at 50% lower rate.
<40 Administer 25 ml of D50 IV, stop infusion, call physician, and re‑check BG in 15‑30 minutes. When BG >64 mg/dl, re‑start infusion at 50% lower rate.

Coming to an ICU near you!

Lessons Learned:
Key things to think about before you try this at home!

The Ideal IV Insulin Protocol
• Easily ordered (signature only)
• Effective (gets to goal quickly)
• Safe (minimal risk of hypoglycemia)
• Easily implemented

Protocol Implementation
• Multidisciplinary team• Administration support• Pharmacy & Therapeutics Committee
approval• Forms (orders, flowsheet, med kardex)• Education: nursing, pharmacy, physicians
& NP/PA• Monitoring/QA

Bedside Glucose Monitoring
• Strong quality-control program essential!
• Specific situations rendering capillary tests inaccurate– Shock, hypoxia, dehydration– Extremes in hematocrit– Elevated bilirubin, triglycerides– Drugs (acetaminophen, dopamine, salicylates)
Clement S, et al. Diabetes Care. 2004;27:553–591.

Limitations of current system
• Nurse autonomy?
• GLUCOSE MONITORING
– Continuous
• Likely the first prototypes to be approved
• Closed loop
• Strengthening the business case for good glycemic control