Embed Size (px)
Citation preview

This article was downloaded by: [New York University]On: 09 October 2014, At: 05:22Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: MortimerHouse, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Psychoactive DrugsPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/ujpd20
Heroin Addiction: Neurobiology, Pharmacology, andPolicyAvram Goldstein aa Stanford UniversityPublished online: 20 Jan 2012.
To cite this article: Avram Goldstein (1991) Heroin Addiction: Neurobiology, Pharmacology, and Policy, Journal ofPsychoactive Drugs, 23:2, 123-133, DOI: 10.1080/02791072.1991.10472231
To link to this article: http://dx.doi.org/10.1080/02791072.1991.10472231
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) containedin the publications on our platform. However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose ofthe Content. Any opinions and views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be reliedupon and should be independently verified with primary sources of information. Taylor and Francis shallnot be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and otherliabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to orarising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Heroin Addiction: Neurobiology,
Pharmacology, and Policyt
Avram Goldstein*
Abstract- The neurobiology of drug addiction is being clarified. Research is revealing the anatomic pathways of primary drug reinforcement (reward) in the brain and the molecular architecture of the receptors on which addictive drugs act All addictive drugs mimic (or occasionally block) the actions of some neurotransmitter; in the case of heroin or methadone an endogenous opioid, probably ~!-endorphin. The groundwork is being laid for understanding Dole and Nyswander 's "metabolic disease" concept as a concrete neurochemical abnormality of the endogenous opioid system. Thus, a stronger basis is developing for regarding methadone maintenance as a means of replacing a neurohormonal deficiency. Three practical conclusions that can be drawn from this model are: (1) methadone dosage must be adequate (never less than 50-80 mg); (2) it should be more widely accepted that some patients may require lifelong methadone maintenance; and (3) longer-acting, better stabilizing methadone congeners, such as LAAM and its metabolites, should be brought into general use.
Keywords- addiction, heroin, LAAM, naloxone, neurobiology, methadone maintenance, opiates, public policy
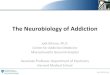
Twenty-four years ago Vincent Dole and Marie Nyswander proposed that heroin addiction was a "metabolic disease" (Dole & Nyswander 1967). Nyswander, a psychiatrist, had concluded that heroin addiction was entirely refractory to psychotherapy, in that respect resembling organic brain disease or the major psychoses. Heroin addicts spent all their waking hours seeking heroin, acquiring the means to buy it, and injecting it But when they were given the long-acting opiate methadone (once daily by mouth), they reduced substantially or discontinued altogether their use of heroin. This is well documented in numerous publications. Figure 1 (upper panel) presents data from my first methadone trial in San Jose, California, in 1970. The percent of urine tests positive for the heroin metabolite, morphine, is plotted for the first six months of treatment. Figure 1 (lower panel) is an independent study, initiated five years later. By then, to exclude anyone who was not a genuine "hard-core" addict, a naloxone test was being employed to confirm physical dependence on opiates (Judson, Himmelberger & Goldstein 1980); only those who tested positive were admitted. Urine
t Adapted from a paper presented at the Society for Neuroscience Symposium, St. Louis, October 29, 1990.
*Professor Emeritus of Pharmacology, Stanford University. Please address reprint requests to Avram Goldstein, 735 Dolores
Street, Stanford, California 94305.
JourNJl of Psychoacti11~ Drugs 123
tests were mandatory, conducted under rigorous, cheatproof conditions, and absences were recorded as positives.
Skeptics objected that this was not so remarkable because one opiate was just being substituted for another. Like Dole and Nyswander, we found that a great many of the addicts maintained on methadone changed their behavior radically. They began to function in a manner that could not be distinguished from nonnal controls either by tests of psychomotor or cognitive perfonnance or by observers blinded to a subject's condition (Dole 1988). Moreover, they seemed to do better and feel better on methadone than during periods of abstinence from any opiate. Thus, a possible interpretation was that methadone not only substituted pharmacologically for heroin (which it certainly did) but that it was acting as a surrogate for a missing honnone. According to that view, heroin self-administration had been an attempt at self-medication for some sort of deficiency syndrome. Heroin, however, is a poor drug for chronic administration because it is much too short-acting and requires intravenous (IV) injection several times daily. This pharmacokinetic defect makes heroin use difficult to reconcile with a nonnal, stable, productive life-style.
In the present article, the endogenous opioids and their receptors are briefly reviewed as well as their roles in reward and aversion and in emotions. The growing evidence
Vol. 23(2), Apr-Jun 1991
Dow
nloa
ded
by [
New
Yor
k U
nive
rsity
] at
05:
22 0
9 O
ctob
er 2
014

Goldstein Heroin Addiction
Q)
c \._
::)
Q)
> +-' (f)
0 (L
+-' c Q)
u \._
Q) (L
(f)
0 (L
+-' c Q)
u \._
Q) (L
100
90
8 0 Methadone 80 mg ( 1973) N=40
70
60
50
40
30
20
10
0
ol ~ '\_o~o--o---o~
0 0 5 10 15 20 25
100~~-----------------------------------------------,
90~ Methad on e/LMM N= 7 2 (1 979) 80
70
60 0
50
40
30
20 o---o~ 0 10
0+-----------~--------~-----------+----------~ 0 2 3 4
Treatment Week
Figure l. Test results for morphine in urine obtained in two surrogate-opiate maintenance programs five years apart. Treatment week zero is date of first dose of methadone (upper panel) or of methadone or LAAM (lower panel); Goldstein, unpublished data.
Journal of Psychoactive Drugs 124 Vol. 23(2), Apr-Jun 1991
Dow
nloa
ded
by [
New
Yor
k U
nive
rsity
] at
05:
22 0
9 O
ctob
er 2
014

Goldstein Heroin Addiction
TABLE I THE ENDOGENOUS OPIOID PEPTIDESt
The Enkephalln Family [Met]enkephalin (YGGFM) [Met]enkephalin-RF (enkephalin heptapeptide) [Met)enkephalin-RGL (enkephalin octapeptide) Peptide E (YGGFMRRVGRPEWWMDYQKRYGGFL) Metorphamide (YGGFMRRV amide) BAM-12P, BAM-18P, BAM-22P (first 12, 18, or 22 residues of peptide E) Peptide F (YGGFMKKMDELYPLEVEEEANGGEVLGKRYGGFM) [Leu]enkephalin (YGGFL)
The Endorphin Family ~-Endorphin (YGGFMTSEKSQTPLVTLFKNAIVKNAHKKGQ; residues 61-91 of~-lipotropin) a-Endorphin (First 16 residues of ~-endorphin) y-Endorphin (First 17 residues of ~-endorphin)
The Dynorphln Family Dynorphin A (YGGFLRRIRPKLKWDNQ) Dynorphin A-(1-8) (YGGFLRRI) Dynorphin B (YGGFLRRQFKVVT) Dynorphin-32 (YGGFLRRIRPKLKWDNQ-KR-YGGFLRRQFKVVT) Leurnorphin (Dynorphin 829; dynorphin B extended at C-tenninus by -RSQEDPNAYYEELFDV) a-Neoendorphin (YGGFLRKPK) 13-Neoendorphin (YGGFLRKP)
tThree families of enkephalin-containing peptides are encoded by three different genes. Recent evidence also indicates the presence of dennorphins and (possibly) deltorphins, opioid peptides that do not contain the five-residue enkephalin sequence. Dennorphin is YaFGYPS amide; ala-<leltorphin I is YaFDVVG amide (see Moret al. 1990; Erspamer et al. 1989).
Single-leuer amino acid code: A=alanine; C=cysteine; D=aspartate; E=glutarnate; F=phenylalanine; G=glycine; H=histidine; !=isoleucine; K=lysine; L=leucine; M=rnethionine; N=asparagine; P=proline; Q=glutamine; R=arginine; S=serine; T=threonine; V=valine; W=tryptophan; Y=tyrosine. Lower-case letter signifies a D-amino acid.
for commonalities in the reinforcing effects of all seven families of addictive drugs is noted and some hypothetical possibilities are posed concerning neurochemical abnormalities in addiction. Finally, some implications of the neurobiology of opiate addiction for optimal maintenance treatment with a surrogate opiate are discussed as well as the implications for national policy concerning the treatment of heroin addicts.
THE ENDOGENOUS OPIOIDS
The discovery of the endogenous opioids and the characterization of their receptors provided a possible basis in neurobiology for the metabolic disease concept. The receptors on which opiates act to produce positive reinforcement (reward) are nonnally activated by endogenous opioid agonists. There are three families of enkephalin-containing opioid peptides: the enkephalins themselves, the endorphins (especially P-endorphin), and the dynorphins (see Table 1). These are encoded by three different genes and they all contain the N-tenninal pentapeptide sequence of either methionine-enkephalin or leucine-enkephalin, the molecular conformations of which bear a certain resemblance to morphine.
JowNJI of Psychoactive Drwgs 125
There is now evidence for a different group of opioid peptides in mammalian brain: the dermorphins and deltorphins, discovered by Erspamer in frog skin, the source of many neuropeptides (Moret al. 1990; Erspamer et al. 1989). These are extremely potent, with high selectivity for JJ.- and ~-opioid receptors, respectively. They all have N-tenninal tyrosine, but they do not contain the enkephalin sequence at all.
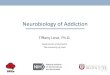
Finally, evidence has accumulated over the yearsfirst from Spector's group (see Donnerer et al. 1987 for a review) and then from mine (Weitz et al. 1986)- that morphine and related alkaloids are present in mammalian brain. The proof is unequivocal; gas chromatography-mass spectrometry establishes the chemical identities of morphine, codeine, and 6-acetylmorphine from that tissue (see Figure 2). Rigorous control procedures absolutely ruled out laboratory contamination. Inasmuch as morphine is synthesized from dopamine in the opium poppy, and as dopamine is so abundant in the brain, it is anra:tive to think that the morphine in the brain may be endogenous, may be a neurotransmitter or neurohonnone. However, the actual biosynthesis of morphine in the animal body remains to be demonstrated conclusively.
When Dole and Nyswander introduced methadone
Vol. 23(2), Apr-Jun 1991
Dow
nloa
ded
by [
New
Yor
k U
nive
rsity
] at
05:
22 0
9 O
ctob
er 2
014

>. -'iii c u .5 u ;>
; "E c u u ... u
Q.
100 rx3 Peak 1 ~xa 3&4 ee TFA Derlv'atlve 477
97
115 152
0
.. 3~:~ M+·
Morphine NCH3
LX3 TFA Derivative CF3 go Lx9 100
100 200 300 400 500
m/z
Figure 2. Comparison of mass spectra of the trifluoroacetyl (fFA) derivatives of purified material from beef brain ("Peak 1," upper tracing) and of authentic morphine (inverted lower tracing) (Weitz et al. 1986) .
. : ·.·:
· .. :. : ......
·.:..: ........ ·Mu receptors + +
..... Transporters
N. Accumb. + Dopami nergi c +OPIATES
COCAINE
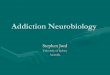
Figure 3. Meso limbic dopaminergic brain reward pathway. This cartoon depicts tonic irlhibition of dopamine neurons originating in the ventral tegmental area (VTA), and Jlopioid stimulation by suppression ofrelease of the irlhibitory neurotransmitter, possibly GAB A. Cocaine acts at terminals of the same neurons to block reuptake of dopamine by the dopamine transporter. Primary reinforcement (reward) is due to dopamine stimulation at nucleus accumbens through D1 dopamine receptors.
Dow
nloa
ded
by [
New
Yor
k U
nive
rsity
] at
05:
22 0
9 O
ctob
er 2
014

Goldstein Heroin Addiction
TABLE II THE OPIOID RECEPTORS
Receptor Type j.l
Preferred Endogenous Ligand ~-Endorphin
Exogenous Ligands DAGO,CTOP Casomorphin Morphiceptin PL0-17
1C
Dennorphins Morphine•
Enkephalins Deltorphins•
Dynorphins
Morphine, heroinb Other morphinans Fentanyl
DPDPE
Benzomorphans U50,488 and other arylacetamides Other 1C agonisu
•Present in brain but not yet demonstrated to be a neurotransmitter or neurohormone. bHeroin itself (3 ,6-{jiacetylmorphine) does not bind to opioid receptors but is converted in the body to active
products 6-acetylmorphine and morphine. •Present in frog skin, but not yet demonstrated in mammalian brain.
maintenance, the idea of a metabolic disease seemed farfetched, but now in view of the multiplicity of endogenous opioids there is an abundance of plausible disease possibilities. The opioid peptides are very widely distributed in numerous systems and pathways throughout the central nervous system (CNS) (Stengaard-Pedersen 1989; Way 1986). Not only are diverse physiologic actions mediated at different sites in the brain, they seem to be mediated by a far larger number ofpeptides than one might have expected from three genes. This is because different patterns of processing yield different active fragments in different tissues (see Table 1), with the processing patterns themselves subject to modification by altered conditions.
OPIOID RECEPTORS
There are three major types of opioid receptors- J..L,
~.and K- which have been very well characterized, and like the peptides, are widely distributed (Loh & Smith 1990). All opioids- alkaloids as well as peptides- can bind to all three receptor types, but with quite different affinities (see Table II). Neither morphine nor the endogenous peptides are very highly selective; not more than fiftyfold for a preferred over a next-preferred opioid receptor type. But synthetic ligands of extremely high selectivity are becoming available, and these are contributing to the evidence that each opioid receptor type may be differentiated into subtypes, as with virtually all other receptors; exactly how many subtypes is not yet clear.
Because morphine was always thought of primarily as a painkiller, the original expectation was that endogenous morphinelike peptides would be principally in-
JourNJI of Psychoactiv~ Drugs 1Z7
volved in regulating pain. However, it is now known that suppression of pain is only one of numerous functions of these substances. With respect to self-administration and addiction, the principal concern is primary reinforcement. Here a specific mesolimbic "reward pathway" (see Figure 3) has been identified in the brain (Bozarth 1987), and there are probably others. Doparninergic neurons originate in the ventral tegmental area (VTA), below the pons, and project forward to the nucleus accumbens and other forebrain areas. The release of dopamine from the terminals of these neurons onto dopamine receptors in nucleus accumbens produces positive reinforcement (Spanagel, Herz & Shippenberg 1990; Herz & Shippenberg 1989).
The doparninergic neurons appear to be under continuous inhibition in the VTA, perhaps by the universal inhibitory neurotransmitter y-aminobutyric acid (GABA). Endogenous opioids are abundant there, where they are thought to modulate the activity of the dopaminergic neurons by suppressing the release of the inhibitory neurotransmitter, thus causing stimulation by disinhibitiona typical mechanism in the brain. The opioid chiefly responsible is probably ~-endorphin, acting on J.Lreceptors, the same receptors to which morphine binds preferentially.
A different aspect of opiate addiction, the withdrawal disturbances, originate elsewhere: in the periaqueductal gray matter (Bozarth & Wise 1984). This anatomic separation of opiate effects emphasizes an important point about all the addictive drugs: the primary cause of compulsive self-administration is the reinforcing property, manifested in specific brain pathways that are quite different from those mediating other pharmacologic effects or the development of physical dependence. Confusion over this
Vol. 23(2), Apr-Jun 1991
Dow
nloa
ded
by [
New
Yor
k U
nive
rsity
] at
05:
22 0
9 O
ctob
er 2
014

Goldstein
distinction led to misunderstandings about whether or not certain drugs (e.g., nicotine, cannabis), which did not display a florid opiatelike withdrawal syndrome, were addictive. Indeed they are, with addiction being defined as compulsive drug self-administration, resulting from stimulation of a brain reward system.
As opioid receptor types and subtypes are better characterized, and especially when they are finally cloned, one can expect to learn- for each separate aspect of opiate addiction- for which endogenous opioid an exogenous opiate substitutes, on which opioid receptor subtype it acts, and at which specific synapses. The same combination of biochemical, pharmacologic, and anatomic mapping will be necessary for addictive drugs of every other family.
Herz and Shippenberg (1989) showed that K opioid agonists, such as the dynorphin peptides, activate an aversion system that seems to counterbalance the rewarding effects of ~-endorphin. Moreover, K opioids in humans produce intense dysphoria and psychotomimesis (Pfeiffer et al. 1986). Presumably, therefore, a dysphoric state could be due to excessive production and release of dynorphins, to unregulated overproduction of K opioid receptors or their signal transduction systems, to deficiency of Pendorphin, or to a defect in the synthesis, membrane insertion or signal transduction systems of )..l opioid receptors. Any of these abnormalities would be expected torespond favorably to )..l opioids, such as heroin and methadone.
NALOXONE
Psychiatrists have noted anhedonia as a common accompaniment of opiate and other addictions. Anhedonia is an inability to experience life's normal pleasures and satisfactions. I wondered if pleasurable emotional states might be mediated by endogenous opioids, and tested this notion with naloxone in volunteer subjects (Goldstein 1980). This experiment was conducted 10 years ago and the results were published in a rather obscure journal; no one has yet replicated or extended it.
The antagonist naloxone has played a key role in determining if a certain physiologic process is mediated by an endogenous opioid system. Naloxone is very highly selective for opioid receptors as a class, but only about tenfold selective for the )lover the .11 or K type. Thus, a phenomenon blocked by naloxone is deduced to operate through an opioid receptor, but it is not possible to specify which type. It is noteworthy that the very first hint of the existence of an endogenous opioid pain-regulatory system (Akil, Mayer & Liebeskind 1972) came from naloxone blockade of the analgesia produced by stimulating the periaqueductal gray matter. The literature since that time is rich with similar examples. More recently, for example, naloxone was used as an effective tool to expose a phys-
JourfiOI of Psychoactive Drugs 128
Heroin Addiction
iologic role of endogenous opioids in suppressing luteinizing hormone-releasing hormone release in the hypothalamus; in sexually mature rats naloxone caused a large increase in plasma luteinizing hormone (Cicero et al. 1988).
What emotional response could be brought under experimental control in the laboratory in order to test the effect of naloxone? There is a well-known phenomenon called a thrill, which accompanies emotionally arousing experiences in many people. It is a pleasant tingling vibration that starts at the back of the neck and travels down the spine, sometimes also sweeping over the arms and down the legs. It is often accompanied by tears, sighs, a catch in the throat, and gooseflesh. The language itself has incorporated the concept of this particular bodily expression of emotions, for the term "thrill" means both a physical vibration and an emotionally arousing experience.
Thrills are evoked by many stimuli. Some people get them from certain passages of music; in opera lovers they are usually elicited by the great dramatic arias. One could reason that if thrills induced by music were mediated by the release of endogenous brain opioids, they should be blocked by naloxone.
The volunteer subjects in my previously mentioned study listened to musical passages that they knew were emotionally arousing for them, and they reported the number and intensity of the thrills. Ten subjects were tested at 10 sessions each. Sometimes they received an IV injection of naloxone, sometimes a placebo; and, of course, the whole experiment was conducted in a double-blind manner. In direct discrimination tests, human subjects are unable to distinguish naloxone from placebo after a single IV injection (Grevert & Goldstein 1978, 1977).
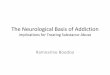
Overall, naloxone significantly attenuated the thrills, but not in all subjects. In some, however, it did so dramatically, as shown in Figure 4 for one subject at a single session as he listened to a passage from Gounod's Faust. Thrills were totally abolished at a repeat of the same musical passage after the naloxone injection. Repeating a musical passage without an injection or after a placebo injection yielded undiminished thrill activity. This study ought to be repeated with higher doses of naloxone- the doses used were only marginally effective, but higher doses are now known to be safe- and with more subjects. Nevertheless, the outcome here does suggest that endogenous opioids play a role in eliciting a purely emotional response, perhaps through a known reward pathway.
GENETIC PREDISPOSITION
All addictive drugs share a common characteristic: they interact with receptors for some endogenous neurotransmitter, as summarized in Table III. It will be interesting to learn if these drug families all converge in their actions onto the same dopaminergic reward pathway.
Vol. 23(2), Apr- Jun 1991
Dow
nloa
ded
by [
New
Yor
k U
nive
rsity
] at
05:
22 0
9 O
ctob
er 2
014

Goldstein
3
2
0
3
2
0
0
SUBJECT 12 PRE
INJ 2~1
100 200
SECONDS
300
Heroin Addiction
Figure 4. Blockade of music-induced thrills by naloxone in a responsive subject. Record of thrills is shown for a six-minute passage from Gounod 's Faust. Reported intensity of thrills (y-axis) is on an arbitrary scale of 0 to 3. Preinjection (upper panel); postinjection of naloxone (lower panel); unpublished data from Goldstein's 1980 study, see also Goldstein ( 1980).
Cocaine does, and recent evidence suggests that nicotine and alcohol do as well. By using selective antagonists, Spanagel, Herz and Shippenberg (1990) have implicated D1 as the dopamine receptor subtype most likely to be involved.
A neurochemical abnormality that played a role in driving addictive behavior could, of course, be consequent to (and caused by) chronic drug administration. A key point, however, should not be forgotten: from a medical standpoint, it is easy to detoxify addicts from the drugdependent state, and therefore addicts should be easy to cure. On the contrary, however, the real problem in addiction is relapse after successful detoxification and even after long periods of abstinence, which suggests that the neurochemical disturbances, if they are consequent to chronic drug self-administration, represent long-lasting irreversible dysfunction. Regulatory adaptations are typ-
Journal of Psychoactiv~ Drwgs 129
ically reversible on removal of the stimulus (e.g., drug or hormone) that induced them. For example, in experimental animals, drug-induced physical dependence is completely reversible within days after withdrawal of an addicting drug. What neurochemical mechanism can be invoked to account for the apparently irreversible relapse tendency?
Alternatively, one has to consider seriously the possibility that the postulated abnormality is antecedent to first use of an addictive drug; that is, a genetic predisposition to addiction. This can be dramatized by the following scenario, albeit a fictitious one. Imagine, before the discovery of insulin, an adolescent diabetic who knows he is ill, but does not know why. A drug dealer comes around, peddling an extract of pancreas, which the young diabetic and his friends decide to try out of adolescent curiosity. The friends become faint and ill as their blood sugar drops, and they swear never to take it again. But the
Vol. 23(2), Apr-Jun 199i
Dow
nloa
ded
by [
New
Yor
k U
nive
rsity
] at
05:
22 0
9 O
ctob
er 2
014

Goldstein Heroin Addiction
TABLE Ill THE ADDICTIVE DRUGS
Drug Family
Barbiturates Benzodiazepines Ethyl alcohol
Cocaine Amphetamines
Heroin Morphine Other 11 opiates
Nicotine
Caffeine
Cannabinoids (marijuana, THC)
PCP LSD Other hallucinogens
Brain Neurotransmitter Mimicked
GABA
Dopamine, norepinephrine
Enkephalins, ~-endorphin"
Acetylcholine (at nicotinic sites)
Adenosineb
Possible endogenous cannabinoid?
Unknown
01C agonists, mimicking the dynorphins, are aversive, thus not addictive.
bCaffeine is an antagonist at adenosine receptors.
diabetic feels normal for the flrst time in his life. From that moment on, he will probably run any risk to acquire the magic remedy. Anecdotal reports, especially from heroin addicts, cannot be given much credence, but inquiry does discover at least some who claim to recall just such a feeling of well-being for the flrst time in their lives, after their initial dose of heroin.
The concept of genetic predisposition to addiction is often misunderstood, as though it excluded a role for environmental influences. Predisposition means an exceptional vulnerability to those influences. Thus, in stressing possible biologic precursors, one cannot ignore the disproportionate burden of addiction on underprivileged groups in society. Nevertheless, one should not forget that even in the most wretched environs of inner cities, most people do not become addicts, even when the illicit addictive drugs are readily available. Moreover, most people, in all socioeconomic groups, do not become addicted to the legally available drugs. A general rule applies to all addictive drugs: when people are flrst exposed, some do not like them and do not become users at all; many use them thereafter in moderation; and some (the smallest portion) become compulsive users. The question is, Why is there this innate difference, which certainly precedes frrst contact with a given drug?
The frrst solid indication of genetic predisposition to an addiction comes from studies on alcoholism. The most persuasive evidence, Cloninger's adoptee studies (Devor
Journal of Psychoactive Drugs 130
& Cloninger 1989), suggested that heredity makes a major contribution to the probability of becoming an alcohol addict. In brief, a typical adoptee of alcoholic parentage, raised from birth by a normal family, is much more likely than his stepbrothers to become an alcohol addict. And even more striking, a typical adoptee of normal parentage, raised by alcoholics, is likely to grow up normal even though his stepbrothers become alcohol addicts. Findings such as these are changing views with respect to the roles of childhood experience, family environment, stress, and other psychologic influences on the genesis of alcoholism. Similar studies are very much needed for the other addictions, but opiate addiction presents formidable obstacles to such research because its illicit status makes valid information so difficult to come by.
Regardless of whether the postulated neurochemical abnormalities are consequent or antecedent to chronic drug use, it is now becoming technically feasible to see if they exist at all in the human brain. Positron emission tomography (PET) scans in living brains provides a promising avenue for approaching this fundamental question. For example, PET scans of deoxyglucose uptake have been used to visualize the brain sites at which nicotine specifically stimulates neuronal activity through nicotinic acetylcholine receptors (London, Szikszay & Dam 1986). Are there differences in nicotine addicts? If so, are those differences evident before they start to smoke? Direct ligandbinding studies are also possible by PET scanning; for ex-
Vol. 23(2), Apr- Jun 1991
Dow
nloa
ded
by [
New
Yor
k U
nive
rsity
] at
05:
22 0
9 O
ctob
er 2
014

Goldstein
ample, of a high-affinity J.L-selective opioid ligand in the living human brain (Frost et al. 1985). This technique may even be capable of indicating the extent of release of an endogenous ligand by its competition with the positronemitting ligand. The ligand-binding PET scan has not yet been used to address the question of receptor abnormalities or defective release of endogenous opioids in addicts.
As the amino-acid sequences of the receptors that mediate the reinforcing effects of each drug family are identified, researchers will be in a position to compare mutations and polymorphisms in the genomic DNA of addicts and normals, using readily available material, as from leukocytes or hair roots. Unfortunately, no opioid receptor has yet been cloned, but it is already possible to study the GABA-receptor complex (a chloride channel on which alcohol acts), the cocaine-sensitive dopamine transporter (which accounts for the pharmacologic action of cocaine), and the adenosine receptors that are putative targets for caffeine action. The recent cloning of a 7 -helix G-proteincoupled cannabinoid receptor (Matsuda et al. 1990) opens new prospects for understanding the psychoactive effects of marijuana and hashish, and perhaps for discovering an endogenous cannabinoid ligand.
PUBLIC POLICY
Does the growing body of knowledge of the neurobiology and pharmacology of opiate addiction provide any guidance for drug policy? The broader aspects of this question were addressed at length in a recent issue of Science (Goldstein & Kalant 1990). There is no single simple cause of opiate addiction. Given that heroin is a primary reinforcer, the net contributions of the following three main factors will determine the incidence and prevalence of the addiction.
Individual Predisposition to Use Heroin Repeatedly and Consequently to Become Addicted
If it could be determined who is especially at risk, preventive efforts might be focused on those individuals early in life, and thus prevent addiction more efficiently. All addicts believe, at the outset, that they can use their drug safely and in moderation. At least for the present, therefore, the safest course is to discourage first use of all addictive drugs, licit and illicit. Regardless of the cause of an addiction, no useful purpose seems to be served by criminalizing addicts for their addiction alone. To the extent that future research implicates predisposition or an irreversible drug-induced abnormality in addictive behavior, society will be more inclined to regard addicts as victims of a disease, rather than simply as criminals. Treatment ought to be universally available, and it is probably cost-effective for society, as compared to relying on the criminal justice system alone (Hanlon et al. 1990).
IourNJI of Psychoactive Drv.g:r 131
Heroin Addiction
Moreover, if treatment is universally available, law enforcement (with respect to real personal and property crimes) can be more stringent because defense attorneys will no longer be able to argue "need for the drug" as an excuse for crimes committed to support a drug habit.
External Facilitatory and Inhibitory Influences External facilitatory and inhibitory influences include
societal, family, religious, and cultural traditions in addition to legal restraints, stressful or tranquil conditions of life, and alternative sources of satisfaction. These multiple influences offer many options for societal policies to reduce the incidence and prevalence of addiction.
Drug Availability There are ample data to show that legal restrictions
of many kinds and gradations can reduce drug consumption. As heroin is already totally prohibited, the maximum reduction in its availability that can be accomplished by means of formal legal restrictions has probably already been achieved. However, more efficient law enforcement strategy and tactics might be possible. Some argue that legalization would ameliorate the problems related to criminality and lack of quality control; but legalization could also be expected to expand the user pool, and therefore would be likely to make matters worse rather than better (Goldstein & Kalant 1990). Sweeping policy changes affecting addictive drugs are oftentimes advocated by politicians, political scientists, sociologists, economists, and others who typically lack knowledge about the drugs themselves.
METHADONE MAINTENANCE
Although the neurobiologic basis of methadone maintenance is incompletely understood, its therapeutic value is well established. The main goal is to stabilize the patient by establishing a nearly constant saturation of the opioid receptors at a substantial level of tolerance. This tolerance (sometimes confusingly called blockade} will make ordinary doses of IV heroin ineffective (i.e., unrewarding). And as methadone is taken by mouth, IV self-administration can be discontinued, which is especially important now for AIDS prevention in this high-risk group. According to the opioid deficiency (metabolic disease) theory, continuous exposure of the brain to methadone will effectively replace a defective component of an endogenous opioid system.
Two fundamental operational principles follow from the above, and although they have been well stated elsewhere (Dole 1988), they are not always understood and applied consistently.
1. As with any drug, the methadone dosage must be adequate or the desired therapeutic result cannot
Vol. 23(2), Apr-Jun 1991
Dow
nloa
ded
by [
New
Yor
k U
nive
rsity
] at
05:
22 0
9 O
ctob
er 2
014

Goldstein
be expected. It is abundantly clear from rigorous double-blind dosage comparisons (Ling et al. 1976; Goldstein & Judson 1974) as well as from practical experience that for most people the optimum dosage range is about 50 to 80 mg daily, certainly no lower. A large person-to-person variability suggests that careful dosage titration, with measurements of blood levels, should be considered in any refractory case. Arbitrary limitation to lower dosages- whether by official regulation or by the misguided feelings of patients or staff that less is better- is bound to be counterproductive. Moreover, in evaluating the success of methadone maintenance programs, dosage policies should be taken into account., and low-dose (e.g., 40 mg) programs should be excluded from the analyses.
2. The sole criterion of success is substantial reduction (ideally, cessation) of heroin use, which often opens the way to functional integration into society (e.g., improved family life, employment), especially if adequate counseling and other kinds of help are made available. Sometimes cessation of heroin use is accompanied by reduction in use of other drugs, sometimes not. Termination of methadone maintenance is never a criterion of success, although it is usually sought (often unwisely) by patients. Relapse to heroin use after discontinuance of methadone calls for prompt return to the maintenance regimen. Arbitrary limitation of the duration of maintenance, like dosage limitation, is counterproductive.
Heroin Addiction
Methadone itself should have been superseded long ago by /-cx-acetylmethadol (LAAM, methadyl acetate) (Judson & Goldstein 1979). LAAM and its active metabolites (nor-LAAM or di-nor-LAAM) are surrogate opiates with much longer durations of action than methadone. Taken by mouth only three times weekly, LAAM establishes a more stable plasma level than methadone. Surveys have shown that the resulting better stabilization is recognized and appreciated by patients (Judson & Goldstein 1982; Trueblood, Judson & Goldstein 1978). Years of bungling by the National Institute on Drug Abuse and obstructionism by the Food and Drug Administration, which have frustrated attempts to bring LAAM into general use, are scandals that an angry public would never have tolerated were this drug intended for treatment of a more societally respectable disease.
CONCLUSION
Increased understanding of the neurobiology of addiction will lead to new diagnostic tests, new means of prevention, and new therapies, including novel pharmacologic approaches to normalizing regulatory dysfunctions. Thus, research on the neurobiology of addiction should receive high priority in the budget for the War on Drugs. Unfortunately, 70% of that budget is committed to supply reduction (interdiction and enforcement) and only 30% to all demand-reduction activities (i.e., prevention, treatment, and research). Those proportions should be approximately reversed.
REFERENCES
Akil, H.; Mayer, D.J. & Liebesk.ind, I. C. 1972. Comparison chez le rat entre l'analgesie induite par stimulation de Ia substance grise periaqueductale et l'analgesie morphinique. Comptes Rendus de /'Acatkm~ tks Sciences Vol. 274: 3603-3605.
Bozarth, M.A. 1987. Ventral tegmental reward system. In : Engel , J . & Oreland, L. (Eds .) Brain Reward Systems and Abuse. New York : Raven.
Bozarth, M. & Wise, R.A. 1984. Anatomically distinct opiate receptor fields mediate reward and physical dependence. Science Vol. 224: 516-517 .
Cicero, T.J.; Meyer, E.R .; Miller, B.T. & Bell, R.D. 1988. Age-related differences in the sensitivity of serum luteinizing hormone to prototypic mu, kappa and delta opiate agonists and antagonists. Jownal of Pharmacology and Experimental TherapeuJics Vol. 246: 14-20.
Devor, EJ. & Cloninger, C.R. 1989. Genetics of alcoholism. Annual Review of Genetics Vol. 23: 19-36.
Dole, V.P. 1988. Implications of methadone maintenance for theories of narcotic addiction. Jownal of the American Medical Association Vol. 260: 3025-3029.
Dole, V.P. & Nyswander, M. 1967. Heroin addiction- a metabolic disease. Archives of Internal Medicine Vol. 120: 19-24.
Donnerer, J.; Cardinale, G.; Coffey,J.; Lisek, C.A.; Jardine, I. & Spector, S. 1987. Chemical characterization and regulation of endogenous morphine and codeine in the rat. Journal of Pharmacology and Experimental TherapeuJics Vol. 242: 583-587.
Journal of Psychoactive Drugs 132
Erspamer, V.; Melchiorri, P.; Falconieri-Erspamer, G.; Negri, L.; Corsi, R.; Severini, C.; Barra, D.; Simmaco, M. & Krell , G. 1989. Deltorphins: A family of naturally occurring peptides with high affinity and selectivity for delta opioid binding sites. Proceedings of the National Academy of Sciences Vol. 86: 5188-5192.
Frost, J.J.; Wagner, H.N., Jr.; Dannals, R.F.; Ravert, H.T.; Links, J .M. ; Wilson, A.A.; Bums, H .D.; Wong, D.F.; McPherson, R .W.; Rosenbaum, A.E.; Kuhar, MJ. & Snyder, S.H. 1985. Imaging opiate receptors in the human brain by positron tomography. Journal of CompuJer Assisted Tomography Vol. 9: 231-236.
Goldstein, A. 1980. Thrills in response to music and other stimuli . Physiological Psychology Vol. 8: 126-129.
Goldstein, A. & Judson, B.A. 1974. Three critical issues in the management of methadone programs. In: Bourne, P.G. (Ed.) Addiction. New York: Academic Press.
Goldstein, A. & Kalant, H. 1990. Drug policy: Striking the right balance. Science Vol. 249 : 1513-1521.
Grevert, P. & Goldstein, A. 1978. Endorphins: Naloxone fails to alter experimental pain or mood in humans. Sc~nce Vol. 199: 1093-1095.
Grevert, P. & Goldstein, A. 1977. Effects of naloxone on experimentally induced ischemic pain and on mood in human subjects. Proceedings of the National Acatkmy of Sciences Vol. 74: 1291-1294.
Hanlon, T.E.; Nurco, D.N.; Kinlock, T.W. & Duszynski, K.R. 1990. Trends in criminal activity and drug use over an addiction career. American Journal of Drug and Alcohol Abuse Vol. 16: 223-238.
Vol. 23(2), Apr- Jun 1991
Dow
nloa
ded
by [
New
Yor
k U
nive
rsity
] at
05:
22 0
9 O
ctob
er 2
014

Goldstein
Herz, A. & Shippenberg, T.S. 1989. Neurochemical aspects of addiction: Opioids and olher drugs of abuse. In: Goldstein, A. (Ed.) Molecular and Cellular Aspects ojtM Drug Addictioi'IS. New York: SpringerVerlag.
Judson, B.A. & Goldstein, A. I 982. Symptom complaints of patients maintained on methadone, LAAM (methadyl acetate}, and naltrexone at different times in their addiction careers . Drug and Alcohol Depenlhnce Vol. 10: 269-282.
Judson, B.A. & Goldstein, A. 1979. Levo-alpha-acetylmethadol (LAAM) in the treatment of heroin addicts. I. Dosage schedule for induction and stabilization. Drug and Alcohol Dependence Vol. 4: 461-466.
Judson, B.A.; Himmelberger, D.U. & Goldstein, A. 1980. The naloxone test for opiate dependence. Clinical Pharmacology and TMrapeutics Vol. 27: 492-501.
Ling, W.; Charuvastra, C.; Kaim S.C. & Klen, C.J. I 976. Methadyl acetate and methadone as maintenance treatments for heroin addicts: A Veterans Administration cooperative study. Archives of General Psychiatry Vol. 33: 709-720.
Loh, H.H. & Smith, A.P. I 990. Molecular characterization of opioid receptors. Annual Review of Pharmacology and Toxicology Vol. 30: 123-147.
London, E.D. I 990. Effects of nicotine on cerebral metabolism. Ciba Foundation Symposium Vol. 152: 131-140.
London, E. D.; Szikszay, M. & Dam, M. 1986. Metabolic mapping of the cerebral effects of abused drugs. In: Harris, L.S. (Ed.)Problems of Drug Dependence, 1985. National Institute on Drug Abuse Research Monograph 67. Rockville, Maryland: National Institute
Journal of Psychoactive Drugs 133
Heroin Addiction
on Drug Abuse. Matsuda, L.A.; Lolait, S.J.; Brownstein, MJ.; Young, A.C. & Bonner,
T.l. 1990. Structure of a cannabinoid receptor and functional expression of the cloned eDNA. Nature Vol. 346:561-564.
Mor, A.; Pradelles, P.; Delfour, A.; Montagne, J.J.; Quintero, F.L.; Conrath, M. & Nicolas, P. I 990. Evidence for pro-dermorphin processing products in rat tissues. Biochemical and Biophysical Research Communicatioi'IS Vol. 170: 30-38.
Pfeiffer, A.; Brantl, V.; Herz, A. & Emrich, H.M. 1986. Psychotornimesis mediated by kappa opiate receptors. Science Vol. 233: 774-776.
Spanagel, R.; Herz, A. & Shippen berg, T.S. I 990. The effects of opioid peptides on dopamine release in the nucleus accumbens: An in vivo rnicrodialysis study. Journal ofNeurocMmirtry Vol. 55: I 734-17 40.
Stengaard-Pedersen, K. 1989. Opioid peptides and receptors. Localization, interactions and relationships to other molecules in the rodent brain, especially the hippocampal formation. Progress in HistocMmistry and Cytochemirtry Vol. 20: I -119.
Trueblood, B.; Judson, B.A. & Goldstein, A. 1978. Acceptability of methadyl acetate (LAAM) as compared with methadone in a treatment program for heroin addicts. Drug and Alcohol Dependence Vol. 3: 125-132.
Way, E.L. I 986. Sites and mechanisms of basic narcotic receptor function based on current research. Annals of Emergency Medicine Vol. 15: 1021-1025.
Weitz, CJ.; Lowney, Ll.; Faull, K.F.; Feistner, G. & Goldstein, A. 1986. Morphine and codeine from mammalian brain. Proceedings of tM National Acalhmy ofScumces Vol. 83: 9784-9788.
\\>1. 23(2), Apr-Jun 1991
Dow
nloa
ded
by [
New
Yor
k U
nive
rsity
] at
05:
22 0
9 O
ctob
er 2
014
![Neurobiology of Addiction presentation [Autosaved] · PDF file• Relieve boredom • Rebel ... • Genetic Factors ... Microsoft PowerPoint - Neurobiology of Addiction presentation](https://img.pdfslide.us/doc/110x75/5aa1de0e7f8b9a46238c53f4/neurobiology-of-addiction-presentation-autosaved-relieve-boredom-rebel.jpg)

![Heroin maintenance for chronic heroin-dependent individualsharmreductionactioncenter.org/HRAC_DOCUMENTS/ADDICTION AND... · [Intervention Review] Heroin maintenance for chronic heroin-dependent](https://img.pdfslide.us/doc/110x75/5b87383e7f8b9a1a248c3f66/heroin-maintenance-for-chronic-heroin-dependent-individualsharmr-and-intervention.jpg)


















![Neurobiology of Addiction presentation [Autosaved]](https://img.pdfslide.us/doc/110x75/61df190bd25d6301594124e7/neurobiology-of-addiction-presentation-autosaved.jpg)


