Embed Size (px)
DESCRIPTION
Hernia
Citation preview

Volume 15 • Supplement 2 • May 2011
Abstract Book
33rd INTERNATIONALCONGRESSOFTHE EUROPEANHERNIA SOCIETY
Oral communications
Posters
GHENT, BELGIUMMay 10-13, 2011
The World Journal of Herniaand Abdominal Wall Surgery
Official Organ of the European Hernia Society (EHS-GREPA)Official Organ of the American Hernia Society (AHS)
Now indexed and included in
Science Citation Index Expanded Journal Citation Reports/Science Edition Current Contents®/Clinical Medicine
See complete list below the table ofcontents
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page 1

H
FOR LAPAROSCOPIC HERNIA REPAIR.
INTRODUCING
Unique design gives him a
from various deployment angles.1,2
Unique, absorbable, low profile “strap” design.1,3
Secure fixation at various deployment angles.2
Each strap deploys with equivalent force.4
Call 1-800-4ETHICON or visit www.ethiconsecurestrap.com.
1-4. Data on File. Ethicon, Inc. ©Ethicon, Inc. 2010 SEC-296-10-8/12
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page 2

Hernia
Founding EditorFounding Editor
Editors-in-ChiefEditors-in-Chief Associate EditorsAssociate Editors
Editorial BoardEditorial Board
J.H. AlexandreParis, France
P.K. AmidCalabasas, CA, USA
G. Champault Bondy, France
P.K. ChowbeyNew Delhi, India
F. CorcioneNapoli, Italy
M. DeysineGarden City, NY, USA
J.B. FlamentReims, FL, FranceD. van GeldereZwolle, The Netherlands
A.I. GilbertMiami, FL, USA
M. Hidalgo PascualMadrid, Spain
M. KurzerLondon, UK
K.A. LeBlancBaton Rouge, LA, USA
S.-Z. MaBeijing, China
C. MeyerStrasbourg, France
M. MiserezLeuven, Belgium
A. MontgomeryMalmö, Sweden
E. NicoloMcKeesport, PA, USA
E. NilssonMotala, Sweden
J.P. PalotReims, France
E.H. PhillipsLos Angeles, CA, USA
R. ReadRockville, IN, USA
R.K.J. SimmermacherUtrecht, The Netherlands
J.P. Chevrel††
Bobigny, France
V. Schumpelick, Aachen, Germany
R.J. Fitzgibbons Omaha, NE, USA
R. Bendavid, Netanya, Israel
A. Kingsnorth, Plymouth, UK
International Advisory BoardInternational Advisory Board
J. AbrahamsonHaifa, Israel
R. AlvarezChula Vista, CA, USA
G. ArltBerlin, Germany
O. ArmstrongNantes, France
M. ArreguiIndianapolis, IN, USA
H.P. BeckerKoblenz, Germany
J.M. BellonMadrid, Spain
C. BellowsNew Orleans, MO, USA
D. BergerBaden-Baden, Germany
R. BittnerStuttgart, Germany
G. CampanelliCastellanza-Varese, Italy
R. CeruttiBuenos Aires, Argentina
J. ConzeAachen, Germany
P. CurcilloFlourtown, PA, USA
S. DabrowieckiBydgoszcz, Poland
J. DeBordPeoria, IL, USA
A. de la TorreBuenos Aires, Argentina
G. FerzliStaten Island, NY, USA
M. FranklinSan Antonio, TX, USA
A.G. GreenburgBarrington, RI, USA
K. HaroldScottsdale, AZ, USA
B.T. HenifordCharlotte, USA
L. HerszageBuenos Aires, Argentina
L. IsraelssonSundsvall, Sweden
K. JungeAachen, Germany
N. KatkhoudaLos Angeles, CA, USA
M. KavicYoungstown, OH, USA
H. KehletCopenhagen, Denmark
J.F. KukletaZürich, Switzerland
J. LeroyStrasbourg, France
Z. MalazgirtSamsun, Turkey
V. MandalàCefalu, Italy
J.B. McKernanWoodstock, GA, USA
S.K. MittalOmaha, NE, USA
R. MoranFullerton, CA, USA
A. PansHerstal, Belgium
C. PeiperHamm, Germany
E. PélissierBesancon, France
J. PetersLos Angeles, CA, USA
B. RamshawColumbia, SC, USA
W. ReedMineola, NY, USA
S. RollSao Paulo, Brazil
M. RosenCleveland, OH, USA
L.T. SorensenCopenhagen, Denmark
S. TowfighLos Angeles, CA, USA
P. VerhaegheAmiens, France
G. VoellerMemphis, TN, USA
M. WexlerMontreal, Canada
R.M. ZollingerCleveland, OH, USA
A4
The World Journal of Hernia and Abdominal Wall SurgeryHernia
13
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page 3

“Hernia” was created in 1997 with thepurpose of promoting clinical studies andbasic research as they apply to groin hernias,internal hernias, the abdominal wall (anteriorand postero-lateral aspects), the diaphragmand the perineum. “Hernia” is the officialorgan of the European Hernia Society(GREPA), established in 1979, and of theAmerican Hernia Society (AHS) establishedin 1997. These associations have commonobjectives: the advancement of abdominal wall andhernia surgery in all aspects, the study of anatomical, physiological,pathological and therapeutic issues concerningthe abdominal wall and hernias, the creation of associated groups which willpromote research and teaching in this field, the development of interdisciplinary relations.“Hernia” is a journal written by surgeons whohave made abdominal wall surgery theirspecial field of interest.
Submission of a manuscript implies: that thework described has not been published before(except in form of an abstract or as part of apublished lecture, review or thesis); that it is notunder consideration for publication elsewhere;that its publication has been approved by all co-authors, if any, as well as - tacitly or explicitly -by the responsible authorities at the institutionwhere the work was carried out. The authorwarrants that his/her contribution is original andthat he/she has full power to make this grant.The author signs for and accepts responsibilityfor releasing this material on behalf of any andall co-authors. Transfer of copyright to Springer(respective to owner if other than Springer)becomes effective if and when the article isaccepted for publication. After submission of theCopyright Transfer Statement signed by thecorresponding author, changes of authorship orin the order of the authors listed will not beaccepted by Springer. The copyright covers theexclusive right and license (for U.S. governmentemployees: to the extent transferable) toreproduce, publish, distribute and archive thearticle in all forms and media of expression nowknown or developed in the future, includingreprints, translations, photographic reproductions,microform, electronic form (offline, online) orany other reproductions of similar nature.
All articles published in this journal areprotected by copyright, which covers theexclusive rights to reproduce and distribute thearticle (e.g., as offprints), as well as all translationrights. No material published in this journal maybe reproduced photographically or stored onmicrofilm, in electronic data bases, video disks,etc., without first obtaining written permissionfrom the publisher (respective the copyrightowner if other than Springer). The use of generaldescriptive names, trade names, trademarks, etc.,in this publication, even if not specificallyidentified, does not imply that these names are notprotected by the relevant laws and regulations.
An author may self-archive an author-createdversion of his/her article on his/her own website.He/she may also deposit this version on his/herinstitution’s and funder’s (funder’s designated)repository at the funder’s request or as a result ofa legal obligation, including his/her final version,provided it is not made publicity available until
after 12 months of official publication. He/shemay not use the publisher’s PDF version which isposted on www.springerlink.com for the purposeof self-archiving or deposit. Furthermore, theauthor may only post his/her version providedacknowledgement is given to the original sourceof publication and a link is inserted to thepublished article on Springer’s website. The linkmust be accompanied by the following text:“The original publication is available atwww.springerlink.com”.
The author is requested to use the appropriateDOI for the article (go to the Linking Options inthe article, then to OpenURL and use the linkwith the DOI). Articles disseminated viawww.springerlink.com are indexed, abstracted andreferenced by many abstracting and informationservices, bibliographic networks, subscriptionagencies, library networks, and consortia.
While the advice and information in thisjournal is believed to be true and accurate at thedate of its publication, neither the authors, theeditors, nor the publisher can accept any legalresponsibility for any errors or omissions thatmay be made. The publisher makes no warranty,express or implied, with respect to the materialcontained herein.
Special regulations for photocopies in the USA;Photocopies may be made for personal or in-houseuse beyond the limitations stipulated underSection 107 or 108 of U.S. Copyright Law,provided a fee is paid. All fees should be paidto Copyright Clearance Center, Inc.,222 Rosewood Drive, Danvers, MA 01923, USA,Tel.: +1-978-7508400, Fax: +1-978-6468600,http://www.copyright.com, stating the ISSN of thejournal, the volume, and the first and last pagenumbers of each article copied. The copyrightowner’s consent does not include copying forgeneral distribution, promotion, new works, orresale. In these cases, specific written permissionmust first be obtained from the publisher.
The Canada Institute for Scientific andTechnical Information (CISTI) provides acomprehensive, world-wide document deliveryservice for all Springer journals. For moreinformation, or to place an order for a copyright-cleared Springer document, please contact ClientAssistant, Document Delivery, CISTI, OttawaK1A 0S2, Canada, Tel.: +1-613-993-9251;Fax: +1-613-952-8243,e-mail: [email protected].
ISSN print edition 1265-4906ISSN electronic edition 1248-9204
Subscription ratesFor information on subscription rates pleasecontact Springer Customer Service Center GmbHThe Americas (North, South Central Americaand the Caribbean):[email protected]
Outside the Americas:[email protected]
Orders and inquiriesThe America (North, South, Central Americaand the Caribbean):Springer Journal FulfillmentP.O. Box 2485, Secaucus, NJ 07096, USATel.: +1-800-SPRINGER, (777-4643)Tel.: +1-201-348-4033 (outside US and Canada)Fax: +1-201-348-4505e-mail: [email protected]
Outside the Americas:via a bookseller orSpringer, Customer Service Center GmbHHaberstrasse 7, 69126 Heidelberg, Germany
Tel.: +49-6221-345-4304Fax: +49-6221-345-4229e-mail: [email protected] hours: Monday to Friday8 a.m. to 8 p.m. local time and on German publicholidays.
Cancellations must be received by September 30to take effect at the end of the same year.
Changes of address. Allow six weeks for allchanges to become effective. All communicationsshould include both old and new addresses (withpostal codes) and should be accompanied by amailing label from a recent issue. According to§4 Sect. 3 of the German Postal Services DataProtection Regulations, if a subscriber’s addresschanges, the German Post Office can inform thepublisher of the new address even if thesubscriber has not submitted a formal applicationfor mail to be forwarded. Subscribers not inagreement with this procedure may send awritten complaint to Customer Service Journalwithin 14 days of publication of this issue.
Back volumes. Prices are available on request.
Microform editions are available from ProQuest.Further information available athttp://www.il.proquest.com/umi/
An electronic edition of this journal is availableat springerlink.com
Springer FranceKarine PechResponsible22, rue de PalestroF-75008 Paris, FranceTel.: +33 1 53 00 98 73Fax: +33 1 53 00 98 61e-mail: [email protected]
Springer, Bernhard SchüllerJournal ProductionPostfach 105280D-69042 Heidelberg, GermanyTel.: +49-6221-487-8737Fax: +49-6221-487-68737e-mail: [email protected]
Director of the Publication:Dr. Guido Zosimo-Landolfo
Publishing Editor:Dr. Guido Zosimo-Landolfo22, rue de PalestroF-75008 Paris, FranceTel.: +33 (1) 53 00 98 71Fax: +33 (1) 53 00 98 61e-mail: [email protected]
TypesettersSPS Chennai, India
PrintersStürtz GmbH, Würzburg, Germany
Printed on acid-free paper
Springer is a part of SpringerScience+Business Mediaspringer.com
Ownership and Copyright© Springer-Verlag France 2010
HERNIAThe World Journal of Hernia andAbdominal Wall Surgery
1 Aims and Scope
2 Copyright
3 Subscription information
4 Electronic edition
5 Advertising and Partnership
6 Production
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page 4

Hernia (2011) 15 (Suppl 2): S1-S35
ABSTRACTS
© Springer-Verlag 2011
Oral communications
O-004Long-term incidence of incisional hernia afterabdominal surgery: A prospective randomized trialcomparing two suture materialsA. Bloemen, P. Van Dooren, B.F. Huizinga, A.G.M. HoofwijkOrbis Medical Centre, Surgery, Sittard-Geleen, Netherlands
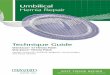
Background: Incisional hernia is a frequent complication of abdom-inal surgery, often requiring surgical intervention. Much researchcomparing suture-materials for closure of the abdominal fascia hasbeen performed, without clear consensus. This prospective random-ized trial was therefore performed.Methods: In 456 patients undergoing median laparotomy, the abdom-inal fascia was closed continuously with non-absorbable (Prolene®)or absorbable (Polydioxanone-s®) suture-materials. Follow-up was byphysical examination and ultrasonography at 6-month intervals. Mainoutcome measures were incisional hernia, surgical site infections andsuture sinus. Statistical analysis was performed with Kaplan-Meiersurvival analyses and Chi-squared and Student’s T-tests.Results: In 456 patients, the abdominal fascia was closed with non-absorbable (Prolene®) or absorbable (Polydioxanone-s®) sutures.Median follow-up was 31 months. Incidence of incisional hernia inProlene® and PDS® was 20.2% (n=45) and 24.9% (n=58) withoutsignificance (P=0.229). Kaplan-Meier curves showed a higher cumu-lative incidence for Prolene® and PDS®; 23.7 and 30.2%, withoutsignificance (P=0.222). When fascial dehiscence was considered anearly occurrence of incisional hernia, there no significant differencein incidence (P=0.088) and in Kaplan-Meier analysis (P= 0.072,Figure 1). Secondary outcome measures showed no significant dif-ferences, although fascial dehiscence occurred twice as often in thePDS®-group.Discussion and conclusion: The incidence of incisional hernia inboth groups was high when compared to the literature. This is dueto strict diagnostic methods and the performed Kaplan-Meier analy-ses. There are no significant differences in incidence of incisionalhernia, although there is a trend in favour of Prolene®. Appearanceof surgical site infections and suture sinus did not differ between thesuture materials.The incidence of incisional hernia appears higher than previouslyestimated. Although there is a trend in favour of Prolene®, no statis-tical significant difference between the two materials was found andno strong preference for either Prolene® or PDS® can be made basedon this study.
O-006One-year follow-up after incisional hernia treatment:Results of a prospective randomized studyL. Venclauskas, A. Maleckas, M. KiudelisDepartment of Surgery, Kaunas University of Medicine, Kaunas,Lithuania
Background: The incidence of incisional hernia after midline laparo-tomies ranges from 10 to 20%. The recurrence rate after this herniasurgery varies from 25 to 52% using autogenous tissue. The use ofprosthetic meshes can decrease the postoperative hernia recurrenceby up to 10%. The aim of this prospective randomized clinical studywas to analyze and compare the results of three different incisionalhernia surgical techniques.
Suture materialPDS®
Prolene®
PDS®-censoredProlene®-censored
Prop
ortio
non
heal
thy
parti
cipa
nts
Follow-up (months)0 6 12 18 24 30 36 42 48 54
1,0
0,9
0,8
0,7
0,6
PDS® 267 227 205 163 145 121 097 85 69 49Prolene® 256 224 204 178 150 123 106 87 66 39
Numbers at risk during interval
Fig. 1: Kaplan-Meier estimates for incidence of hernia.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S1

S2 Hernia (2011) 15 (Suppl 2): S1-S35
Materials and methods: One hundred and sixty-one patients whounderwent incisional hernia surgery were randomized into threegroups. The Keel technique was used in the first group, the “Onlay”technique (prosthetic mesh is fixed on the external abdominal mus-cle slip) in the second group, and the “Sublay” technique (prostheticmesh is placed on the posterior abdominal muscle sheath) in thethird group. Age, sex, hospitalization time, body mass index (BMI),intraabdominal pressure, postoperative complications, postoperativepain, normal physical activity recovery time, and recurrence rate werecompared between the groups. The postoperative follow-up periodwas 12 months.Results: Fifty-four patients in the Keel group, 57 patients in the“Onlay” group, and 50 patients in the “Sublay” group were oper-ated. Age, hospitalization time, and BMI were similar in all of thegroups. The operative time was significantly longer in the prostheticmesh groups compared with the Keel group. The intraabdominalpressure changes before and after surgery was significantly higherin the Keel group compared with the prosthetic mesh groups(5.66±2.5 mmHg vs. 1.88±1 mmHg vs. 1.76±1 mmHg; P<0.05). Thepostoperative wound complications rate was significantly higher inthe “Onlay” technique group compared with the Keel and “Sublay”technique groups (49.1% vs. 22.2% vs. 24%; P<0.05). Postoperativepain (VAS score) was significantly lower in the “Onlay” and“Sublay” groups (5.53±1.59 vs. 3.96±1.56 vs. 3.78±1.97; P<0.05).All of the patients in “Sublay” group recovered to normal physicalactivity during the 6 months follow-up period compared with 94.4%of patients in the Keel group and 98.3% of patients in the “Onlay”group. The recurrence rate was 22.2% in the Keel group, 10.5% inthe “Onlay” group, and 2% in the “Sublay” group during the fol-low-up period. The general complications rate after hernia surgerywas 5.6%. Postoperative pneumonia was the most frequent compli-cation, which appeared in 4.3% of patients. There was no postoper-ative death in our prospective study.Conclusions: Mesh repair is the first-choice technique for incisionalhernia treatment. The results of the “Sublay” technique are betterthan the “Onlay” technique.Reference:Hernia. 2010 Dec; 14(6): 575-82. Epub 2010 Jun 22.
O-008Long-term outcome after randomising Prolene HerniaSystem, Mesh Plug Repair and Lichtenstein foringuinal hernia repairS.W. Nienhuijs1, C. Rosman21 Catharina Hospital Eindhoven, Surgery, Eindhoven, Netherlands;2 Canisius-Wilhelmina Hospital, Surgery, Nijmegen, Netherlands
Background: Comparing three commonly used techniques for inguinalhernia repair revealed no clinical relevant differences in previous stud-ies, except the main complication of chronic pain. Whether this dimin-ishes or favours one technique over time was the subject of this study.Methods: Between 2001 and 2003, 334 patients were blindly andrandomly allocated to receive one of the three open hernia repairs:Prolene-Hernia-System, Mesh-Plug-Repair or the Lichtenstein proce-dure. 23 of them deceased or were untraceable. The remainingreceived postal questionnaire focussing on pain limitations and sen-sory disturbances.Results: In total 251 out of 311 patients completed the follow-up(80.7%). The majority of 191 patients had no pain. Forty-one patientsscored a VAS score below 30, nine scored 30 till 50 and anothernine above 50. Exactly the same 59 patients rated their pain as mild
(44), moderate (14) and severe (1). All but two regarded this painmaintainable. The frequency was monthly for 34 patients, weekly for14 and for 10 patients daily. The proportion of 13.5% experiencedlimitations for daily activities. 17 patients graded this as minimal, 14as moderate and 3 as severe. Reported sensory disturbances werenumbness (13.5%), feeling the mesh sometimes (27.1%) or regularly(5.2%). Eleven recurrences were reported (4.4%). No differencebetween the techniques were found.Conclusion: Chronic pain after inguinal hernia repair diminishesover time for all three techniques. After 7 years, however, 7% stillsuffers moderate/severe pain with limitations. This underlines theefforts surgeons are taking today to prevent this complication.
O-010 Best PaperInterim analysis of a comparative randomized study:Potential benefit of absorbatack™ absorbable fixationin the treatment of ventral hernia by laparoscopicapproachM. Lepere1, W. Cobb2, D. Giles3, U. Novitsky3, H. Scheuerlein4,V. Narula5, J. Ponsky6, B. Matthews7, T. Barthes8, H. Johanet9,M. Rosen101 Clinique Saint Charles, Laparoscopic surgery, La Roche Sur Yon,France; 2 Greenville Hospital System, France; 3 uconn Health Center,France; 4 Jena University, France; 5 The Ohio State University,France; 6 University Hospitals Case Medical Center, France;7 Washington University School of Medicine, France; 8 PoitiersPolyclinic, France; 9 Clinic Saint-Marie, France; 10 Case MedicalCenter, University Hospitals of Cleveland, France
Background: To avoid early mesh migration after ventral hernialaparoscopic treatment, fixation is recommended. However, postop-erative pain and mesh fixation may be correlated. An absorbable fix-ation device might provide adequate additional fixation strengthwhile reducing long term postoperative discomfort. To compareAbsorbaTack™ absorbable fixation versus ProTack™ permanent fix-ation during laparoscopic ventral hernia mesh repair, a prospectiverandomized multi-institutional study evaluating fixation efficacy andpostoperative pain has been conducted.Methods: 97 patients were randomized in 10 centers. 50 patientsunderwent laparoscopic hernia mesh repair with AbsorbaTack™ fix-ation (group A) and 47 with ProTack™ fixation (group P). Patientpain (PI-NRS pain scale) and other outcomes were assessed from thepreoperative visit to the six-month follow-up visit.Results: The demographic characteristics and the post operativecomplication rates were comparable between group A and group P.Two recurrences were observed at six months in group A (group P:0 recurrence; p=0.5). No mesh infection, migration nor fistula werereported. In group P, one small bowel obstruction was observed.However, despite randomization, the pain prior to surgery (meanPI-NRS score) was significantly higher in group A compared togroup P (1.9 vs 1.0, p=0.02). When compared to baseline, pain wasreduced at one month and six months in group A (difference of -0.5and -0.9, respectively). Compared to baseline, pain was reduced onlyat six months in group P (difference of -0.7).Conclusion: AbsorbaTack™ absorbable fixation shows a potentialbenefit when judged on the average postoperative pain level decreasefrom baseline. This potential benefit may be reinforced with the fullabsorption of the device. The two study groups showed comparabledegrees of efficacy and safety (based on recurrence rates and postop-erative complications). These promising results need to be confirmedwith longer follow-up.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S2

Hernia (2011) 15 (Suppl 2): S1-S35 S3
O-011 Best VideoRobotic single-port hernia surgery: The future is todayH.M. TranThe Sydney Hernia Specialists, Surgery, Sydney, Australia
Introduction: Single-port and robotic Freehand® represent the mostsignificant innovations in laparoscopic surgery in the last 20 years.While large scale adoption of single-port hernia surgery awaits resultsof prospective randomised controlled studies confirming its potentialbenefits there is enormous potential for robotic Freehand® to solvethe problem with the chronic lack of good camera assistants.However, there have been no published reports in robotic (single-port) hernia surgery.Aims: Assess the feasibility, safety and efficacy of combiningLaparo-endoscopic Single Site (LESS) Tri-port™ with roboticFreehand® in laparoscopic total extraperitoneal (TEP) inguinal her-nia repair.Materials and methods: Preliminary study in a swine model demon-strated the feasibility of single-port robotic hernia surgery using300/5.5 mm/52 cm laparoscope and straight dissecting instruments.The use of rigid ports such as SILS™ resulted in damaging bendingto the laparoscope. This was not experienced with the floppyTri-port™. Patients undergoing TEP inguinal hernia repair betweenOct-Dec 2010 were selected for robotic single-port hernia repair.Patient data include: age, sex, body mass index, American Associationof Anaesthesiologists classification, type of hernia, time spent clean-ing the laparoscope, patient satisfaction survey and recurrence.Results: There were 16 patients undergoing robotic single-port TEPinguinal hernia repair compared to 16 cases of conventional single-port inguinal hernia repair. Patients were matched for age, sex, BMI,ASA and types of hernia. Although operation time was comparablein both groups (48min vs 52min) time wasted for scope cleaning was1.5 minutes for robotic compared to 8.5 minutes for conventionalsingle-port surgery. There were no recurrences and patient satisfac-tion was high in both groups.Conclusion: Robotic single-port hernia repair is safe and efficient.In addition to negating the risks of trocar-induced bowel/vascularinjuries and producing scarless incisions it allows better utilisationof precious manpower resources. LESS™ Freehand® TEP repair rep-resents a new stratosphere for laparoscopic surgery.
O-012 Best PaperSubcutaneous Talc lowers the incidence of woundcomplications after open ventral hernia repair withpanniculectomyV.B. Tsirline, D.A. Klima, I. Belyansky, C.L. Carpenter,C.M. Hlavacek, S.B. Getz, B.T. HenifordCarolinas Medical Center, GI/MIS Surgery, Charlotte, United Statesof America
Introduction: Wound complications in patients undergoing largeventral hernia repair requiring extensive tissue dissection or pan-niculectomy (OVHR/PAN) occur in 18-50% of procedures. Thisstudy evaluates a novel concept of talc application in subcutaneoustissue of OVHR/PAN patients to decrease postoperative seroma for-mation and wound complications. The considerations of the associ-ated complications that are occasionally seen after talc administra-tion in the pleural space were also evaluated.Methods: Demographics, perioperative data, and outcomes of patientsundergoing OVHR/PAN were evaluated prospectively. Patients weredivided into those who received subcutaneous talc poudrage (Talc)and controls who had a conventional procedure (NoTalc).
Results: 180 patients met inclusion criteria, 74 in Talc group and106 in NoTalc group. Demographics were similar (p>0.05), follow-up was 1 to 73 months. Defect size was larger in Talc group(mean±SD) 258±195 vs 213±281cm2 (p=0.02). The Talc group hada significant reduction in seromas requiring intervention (20.8% to2.7%; p<0.001), cellulitis (39.6% to 20.5%; p=0.007) and antibioticuse (40.6% to 22.9%; p=0.02). Talc group also had significantly ear-lier drain removal from 25.6±19.1 to 14.6±7.0 days (p<0.001). Therewas no difference in the incidence of tachycardia (HR>100 bpm),hypotension (SBP<90 mmHg), tachypnea (RR>25 breaths/min), orhypoxia (O2 Sat<92%). Patients who received talc had a lower inci-dence of renal insufficiency (Cr>1.2) compared to controls, with sta-tistically significant differences on POD3 (6.1% vs 19.2% p=0.049)and POD4 (4.3% vs 17.4% p=0.035).Conclusions: Subcutaneous application of talc for OVHR/PANdecreases postoperative rates of cellulitis, antibiotic use, and complexseromas requiring intervention. Average drain duration was 11 daysshorter. Fewer patients developed renal insufficiency, likely due todecreased fluid shifts. No additional adverse effects were noted. Useof subcutaneous talc in patients undergoing OVHR/PAN may decreasepostoperative systemic and wound complications.
O-013 Best VideoPearls and pitfalls of abdominal wall anatomy incomponent separationZ.M. Hurwitz, J. O'Brien, R.M. DunnUniversity of Massachusetts Medical School, Surgery, Worcester, Ma,United States of America
Background: Complex ventral hernia repair (CVHR) requires anintimate working knowledge of the anatomy of the abdominal wallfor optimum outcome and a low rate of surgical complications.Advances in techniques of abdominal wall reconstruction (particu-larly component separation) continue to evolve and include laparo-scopic, endoscopic, and open variations. The surgical anatomy of theabdominal wall is difficult to appreciate and often overlooked dur-ing abdominal operations. This video highlights the anatomy of theanterior abdominal wall including the four muscles (rectus abdo-minis, extenal and internal obliques, and transversus abdominis) aswell as their aponeurotic connections, the neural and vascular sup-ply to these muscles and to the soft tissue of the abdominal wall.All of these components must be considered when performingcomplex ventral hernia repair.Methods: Cadaveric abdominal wall dissection via an “I” shapedincision was performed. The skin and subcutaneous tissues wereelevated to the mid-axillary line. Cutaneous perforators from therectus abdominis were identified and labeled during skin flap eleva-tion. The rectus abdominis muscles were elevated from the posteriorsheath to demonstrate segmental neural and vascular contributions.The external oblique aponeurosis was divided to demonstratecomponent separation technique. The intercostal nerves were identi-fied coursing deep to the internal oblique.Results: This cadaveric dissection highlights the abdominal wallanatomy as it pertains to use of component separation and CVR tech-niques. Structures identified include the cutaneous perforators, theanterior and posterior fascia, the arcuate line, the external and inter-nal oblique muscles and their aponeuroses, the blood supply to therectus muscles including the epigastric vessels and the segmentalintercostal vessels as well as the segmental innervations of the rec-tus via intercostal nerves.Conclusions: Detailed anatomic knowledge of the structural ele-ments of the abdominal wall are critical to effective CVHR withcomponent separation. Higher quality video will be available forpresentation.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S3

O-014 Best PaperLaparoscopic surgery (TEP) for sportsman’s herniais more effective than non-operative treatment.A randomized clinical trial with magnetic resonanceimaging of 60 patientsH. Paajanen1, T. Brinck1, I. Airo21 University hospital of Kuopio, Surgery, Kuopio, Finland;2 Deaconess Hospital of Helsinki, Surgery, Helsinki, Finland
Background: Sportsman’s hernia is a deficiency of the posterior wallof the inguinal canal. Endoscopic mesh repair may offer faster recov-ery for athletes with sportsman’s hernia compared to non-operativetherapy.Methods:A randomized, prospective study was conducted on 30 oper-ated and 30 conservatively treated patients with sportsman’s hernia.Clinical data and magnetic resonance imaging were collected on allpatients. After 3 to 6 months of groin symptoms, the patients wererandomized into operative or physiotherapy groups. Operation was per-formed by a placement of totally extraperitoneal endoscopic (TEP)mesh behind the symphysis and painful groin area. Conservative treat-ment included at least 2 months of active physiotherapy. The outcomemeasures were pre- and postoperative pain using a visual analoguescale and partial or full recovery to sport activity at 1, 3, 6 and12 months after randomization.
Results: The athletes in both treatment groups had similar charac-teristics and pain scores. Operative repair was more effective thannon-operative treatment to decrease chronic groin pain after onemonth and up to 12 months of following up (p<0.001). Twenty sevenof 30 athletes (90%) returned to sport activities after three monthsof convalescence compared to eight of 30 (27%) in the non-opera-tive group (p<0.0001). Seven athletes (23%) in the conservativegroup were later operated because of persistent groin pain.Conclusions: This randomized controlled study indicated that theendoscopic placement of retropubic mesh was more efficient thanconservative therapy for the treatment of sportsman’s hernia typepubalgia in athletes.ClinicalTrials.gov identifier: NCT00966589
O-015 Best VideoComplex abdominal wall reconstruction with acomponent separation technique in an ostomizedpatient with a loose of domain incisional herniaJ. López-Monclús1, M.A. García-Ureña1, P. López-Quindós1,D.A. Melero1, A. Pueyo1, L.A. Blázquez1, E. Enrique1, A. Galvan1,N. Palencia2, R. Barriga2, A. Robin1, A. Cruz11 Henares Hospital, General and Digestive Surgery, Coslada, Spain;2 Spain
Background: Management of loose of domain hernias in ostomizedpatients is always a surgical challenge. Our objective is to presentour eventroplasty technique for abdominal wall reconstruction in anureterostomized patient with a variation of the component separationtechnique.Methods: Fifty-nine years old male with previous history of openradical cystectomy with right ureterostomy two years ago who devel-oped a loose of domain incisional hernia. A variation of the compo-nent separation technique was done; retromuscular space was dis-sected by incising the posterior rectus sheath on both sides.Unfortunately there was not enough tissue to get a primaryclosure of the midline in the preperitoneal space, so an intrabdomi-nal bioabsorbable mesh of polyglycolic acid and trimethylene car-bonate was placed. After dissecating the lateral subcutaneous flaps,we desinserted the attachments of external oblique muscle to therectus sheet, partially in the right side where the ureterostomy waspresent. A very low density polypropylene mesh was then suturedto the external oblique muscle in the onlay position and an aspira-tive drain was placed in the subcutaneous space before ending thesurgery.Results: The patient was discharged in the fifth postoperative day.He developed a superficial wound infection which was managed inthe outpatient clinic with a complete healing of the wound after threeweeks after the surgery. After three months of follow up, the patientis asymptomatic.Conclusions: Massive incisional hernias in ostomized patients areusually a surgical challenge, due to the difficult dissection of the her-nial sac and the impairment of the muscular and fascial structuresnecessaries to mesh fixation. In cases of loose of domain hernias,the separation component technique enables us to enlarge the intrab-dominal volume. Nowadays, the combination of last generationpoypropylene meshes and the new biosynthetic meshes has widenedthe spectrum of choices to manage this surgery.
O-016 Best PaperGORE Bio-A Tissue Reinforcement for pelvic floordefects after laparoscopically-assistedabdominoperineal resectionT. Mussack, C. Chiapponi, U. Stocker, R. LadurnerKlinikum der Universität München, Department of SurgeryInnenstadt, München, Germany
Background: The 3 D GORE Bio-A Tissue Reinforcement (TR)consists of biocompatible synthetic polymers that are gradually absorbedby the recipient. The objective of this study was to evaluate GORE Bio-A TR in patients with laparoscopically-assisted abdominoperineal resec-tion due to low rectal or anal cancer for reinforcement of pelvic floor.Methods: Twenty-five consecutive patients (15 male, 10 female;mean age, 53 years [range 29-79]; mean ASA score, 2 [range 1-3])underwent laparoscopically-assisted abdominoperineal resection for
S4 Hernia (2011) 15 (Suppl 2): S1-S35
Fig. 1: Postoperative pain scales of the patients.
LaparoscopicNon-operative
Time (months)
Pain
scal
e
10
8
6
4
2
0Pre 1 3 6 12
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S4

Hernia (2011) 15 (Suppl 2): S1-S35 S5
low rectal adenocarcinoma (n=17) or squamous cell carcinoma of theanal canal (n=8). Twenty-one patients received preoperative chemora-diation, 4 patients had perforated tumors at time of surgery. Sixpatients with anal cancer suffered from HIV-infection, all otherpatients were immunocompetent. Before pelvic floor closure, GOREBio-A TR was inserted via the perineal route. The matrix was finallyfixed laparoscopically with interrupted absorbable sutures or tacks tothe pelvic floor. Three and twelve months after surgery, patients werereevaluated in terms of quality of life (SF-36) and pelvic floor mor-phology shown by cine 1.5T MRI.Results: The prosthesis was easy to configure and implant. Patientswith primary skin closure as well as secondary wound healing of theperineum finally revealed a pleasant clinical course. In 3 cases ofwound infection, GORE Bio-A TR allowed for infection resolutionwithout prosthetic removal. Three months after surgery, all physicaland mental SF-36 values were significantly lower than the norm val-ues for the age-stratified German norm population, most likelybecause of the postoperative chemotherapy according to the proto-col. Cine MRI revealed a complete integration of GORE Bio-A TRinto the pelvic floor without evidence of seroma, infection or per-ineal hernia.Conclusions: GORE Bio-A TR has proven to serve as a convincing tis-sue scaffold targeting pelvic floor reinforcement in cases of complicatedpelvic floor defects after laparoscopically-assisted abdominoperinealresection.
O-020NOTES: Less is more in hernia surgeryD. LomantoDepartment of Surgery, Yong Loo Lin School of Medicine, NationalUniversity Health System, National University of Singapore,Singapore
Surgery in the 21th Century seems to evolve further with the merg-ing of medical technology like flexible and rigid endoscopy, roboticdevices, sealing and IT technology aiming to offer a better clinicaloutcome and cure to our patients. Since the beginning, MinimallyInvasive Surgery have been associated with less pain, shorter hospitalstays, fewer complications and better cosmesis than conventionallaparotomy, with the merging of these technologies we aim to furtherimprove this benefits without affecting safety and outcome. The dremto have a bloodless and scarless surgery started by reducing both sizeand number of access; through minilaparoscopy, needlescopy orcombined endoscopic-laparoscopic approach we have reached the goldstandard in many surgical diseases but the development continues andin 2005 pioneer reported in early experimental study a new attractivetechnique called “Natural Orifice Translumenal Endoscopic Surgery”(NOTES) where a flexible endoscope is passed through a natural ori-fice such as the mouth, vagina or rectum to perform intra-abdominalprocedures as cholecystectomy, oophorectomy, tubal ligation andmore. Since then, NOTES has gained widespread interest and proba-bly in the 21th Century we will be at the verge of a totally newparadigm shift that could redefine modern surgery. Our experimentalexperience to evaluate the feasibility of NOTES, to recognize thepitfalls of the procedure, to assess its safety for potential human appli-cation and to develop new tools like the MASTER Robotic device tobetter perform this new attracting approach is ongoing. Dissection,retraction, navigation and orientation, intraperitoneal sepsis and inad-equate instrumentation are the challenges that we encounter and needto be solved before this new surgical approach can be fully utilizedin clinical setting.
In hernia surgery few report has been published in the literaturemostly in experimental setting showing the pros and cons of bothtransgastric and transvaginal approach for abdominal wall herniarepair. In our experience in an experimental survival study weassessed the feasibility and safety of the transluminal abdominal wallhernia repair using mesh for potential human application by specif-ically investigating the challenges using a transvaginal approach.NOTES although initial experimental and clinical study seemsencouraging should still be done in proper academic setting understrict controlled review to avoid inappropriate publicity. Trials shouldaim to objectively describe both adverse and favorable outcomes.Meantime we aim the research and development of both industriesand universities centers will further develop to improve the technolo-gies for this new approach.
O-021Classification of surgical meshes for hernia repairU. KlingeRWTH Aachen & Universitätsklinikum Aachen, Aachen, Germany
What for? If a unique device identifiers with complete follow-up ofevery device is available, this is not necessary. If we have the dataof such a compulsory registry we will get a precise ratio of failuresfor every single device. BUT do you believe it will be a realisticvision? A complete registry of all devices with complete follow-upfor several years? NEVER!What is the alternative, if there is any?In the moment we only have incomplete data. We have some num-bers of failures, but we do not know the percentage because we donot know the absolute number of implanted materials (supposinglymore than 1/2 million each year in Europe). We even have nocomplete follow up. But we have a voluntary registry and we havea voluntary collection of mesh explants. And we can learn from it.If you assume that there is no difference for the risk between thematerials, then the ratio of meshes with complications and mesheswithout complications should be similar for the many differentdevices. Or the ratio of meshes explanted for recurrence should becomparable to that explanted for infection or pain for the many dif-ferent devices. But if there are some significant differences, weshould think about it and it may indicate a relevant impact of thematerial.However, such an interpretation is hardly possilbe if you have > 200devices with > 300 trade names and perhaps 50 new developmentseach year. Therefore, any reliable interpretation of the data requiressome sort of grouping, a grouping considering relevant “major”differences. And what is a relevant “major” difference? A “Major”difference is a difference that can be or alrady has been objectifiedin a randomised controlled trial. RCT. Vice verse, if you do not havesignificant differences in a RCT, then these materials shouldhave only “minor” differences, and correspondingly belong to onejoint group.Among the many textile characteristics the only property that can beused today for grouping is the porosity. There is sufficient evidencethat small pore structures have a distinct outcome in comparison tolarge pore structures or the films without any pores. And there iswide agreement that there are some different meshes with additionalfeatures, e.g. for the use in the abdominal cavity, which shouldnot be compared with materials for the simple use in the groin.Therefore, there is another group of meshes covering specific require-ments, which in case of sudden extentsion may be even subdividedlater on.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S5

S6 Hernia (2011) 15 (Suppl 2): S1-S35
In a joint discussion with most of the major manufactures of meshmaterials we could agree on the following grouping of porous tex-tile structures:
Application Detailed Group 1 Group 2 Group 3 Group 4Application Advanced Basic Special Preshaped,
technology technology features preformed,3D
“large “small “prevention “pluggingpores” pores” of adhesion, the defect”
modified scarformation,bioactive, mesh,drug releaseetc.”
Groin Groin A A A AFemoral
Ventral Incisional A A A AParastomalEpigastricUmbilicalHiatalCongenitaldefect
Intraperitoneal
Proposal for grouping of textile porous meshes used for hernia repair, furhter subdivison possi-ble a = monofilament, b = multifilament, c = mixed polymers / fibres
This grouping is based on the assumption that meshes within a groupshows only minor differences, and minor differences are defined bythe impossibility to proove relevant differences in a RCT. It does notconsider so called biologicals, which should be evaluated as distinctdevice, perhaps as 2 additional groups or completely in a seperateanalysis. If in future there may be some meshes with bioactivecoating with approval as class III medical device a further groupmay be added. This grouping will be available on the webpages ofthe German and of the European hernia society. It will be revisedregularly, with addition of new devices if essentail information ofthe prodduct such as porosity is provided. This grouping is inten-dend to be used for analysis of the data from the registry of herniarepairs as well as of implant failures to detect major mesh materialrelated problems.
O-022Prospective randomized trial comparing polypropyleneand new biomaterials in plug and patch surgery foringuinal herniaA.M. Manno, A. Verbo, G. Rizzo, D.P. Pafundi, G. Mascianà,C. CocoCatholic University of The Sacred Heart, Surgery, Rome, Italy
Backgrounds: The aim of this study is to prospectively comparepolypropylene to new biomaterials in the treatment of inguinal her-nia, in order to evaluate if the last ones can show better biocompat-ibility and incorporation, recurrence rate being equal.Methods: Seventy consecutive patients affected by primary inguinalhernia were included. All patients were submitted to patch andplug operation after randomization to polypropylene (group A)or PTFE + PGA/TMC plug (group B). Postoperative pain according
to VAS scale was assessed at a 12 h, 24 h, 48 h, 7 days, 1, 3, 6and 12 months from the operation. Blood samples to test leucocytecount, fibrinogen, CRP and IL-6 levels were collected 24 h beforesurgery and 6, 24, 48 and 168 h postoperatively. Clinical evaluationand inguinal ultrasound (US) were performed at 1, 3, 6 and12 months.Results: There were 67 males and 3 females (median age 43 years),34 in group A and 36 in group B. VAS median score was significantlylower in group B in all the report during the study. Leucocite countat 6, 12, 24, 48h resulted higher in group A than in group B (100%vs 6%, 100% vs 36%, 96% vs 8% and 96% vs 2,5%). The same forCPR (96% vs 0%, 82,5% vs 8,5, 100% vs 30% and 85% vs 12%),and fibrinogen (41% vs 0%, 100% vs 47%, 100% vs 50% and 100%vs 53%). Il-6 resulted higher in group A at 24h (100% vs 47%). Ingroup A stronger inflammatory response was evidenced by US at1 month (70% vs 36% in group B). No recurrences in both groups.Conclusions: PTFE mesh and PGA/TMC plug seem able to guar-antee less inflammatory response and thus less postoperative painand better quality of life after hernia surgery.
O-023Preliminary results of a comparative randomized study(RCT): Benefit of self-gripping ParietexstudyProGrip™ mesh in open inguinal hernia repairA.N. Kingsnorth1, S. Nienhuijs2, E. Schülenberg2, P. Ziprin2,A. Eklund2, M. Gingell-Littlejohn2, M. Miserez2, E. Kullman2,S. Smeds21 Plymouth Hospitals NHS Trust, Hernia Service, Plymouth, UnitedKingdom; 2 Eindhoven, Netherlands
Background: The Lichtenstein method is the gold standard for openmesh inguinal hernia repair with low recurrences. However, an unre-solved problem is post-operative pain, which may be related to meshfixation. The aim of this study was to compare the self-grippingParietex ProGrip™ sutureless mesh repair vs Lichtenstein suturedmesh repair in a RCT evaluating postoperative pain.Methods: 390 patients were randomized in 9 centers and analyzedat 3-month (among whom, 215 patients reached the 1-year assess-ment). 197 patients were operated with Lichtenstein repair (L group)and 193 with Parietex ProGrip™ mesh (P group) with or withoutfixation. Patient pain (linear 150-mm VAS scale) and other outcomeswere assessed from the preoperative visit to the 1-year follow-upvisit. Post-operative pain was analyzed using difference between VASscore at each assessment and baseline.Results: The VAS difference analysis showed:• A lower pain in P than in L group at Discharge (respectively +2.57and +10.41, p=0.053) and Day-7 (-1.37 vs +5.96, p=0.048).
• No pain difference at 1-month post-surgery or later.In P group, throughout the 3-month post-operative period, the painwas lower in patients without fixation than in patients with 1-stitch:Infection rates were 5.6% in L group and 3.1% in P group, (p=NS).Surgery duration was significantly shorter in P than L group (34.4 minvs 40.7 min; p<0,001).No recurrence was observed in P group although 1.6% was observedin L group.Conclusion: These preliminary results show that surgery durationand early pain are significantly reduced with ProGrip™ comparedto Lichtenstein repair. The use of ProGrip™ is simple and fast,providing some better outcome measures for patients comparedwith Lichtenstein. These promising results and trends need to beconfirmed on a larger population.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S6

Hernia (2011) 15 (Suppl 2): S1-S35 S7
O-024Is it possible to prevent emergency surgery for femoralhernia by earlier intervention?U. Dahlstrand1, G. Sandblom1, S. Wollert2, U. Gunnarsson11 Karolinska University Hospital, Department of Surgery, Stockholm,Sweden; 2 Uppsala University Hospital, Department of Surgery,Uppsala, Sweden
Background: Femoral hernias are frequently operated on as emer-gencies. Emergency procedures for femoral hernia are associatedwith an almost ten-fold increase in mortality, while no increase isseen for elective procedures. The natural course of femoral herniasis not well known and it is uncertain whether the risk of femoralhernia incarceration can be reduced.Methods: 1,967 patients who had had a repair for a primary unilat-eral femoral hernia between January 1, 1997 and December 31, 2006were sent a questionnaire about hernia symptoms and contacts withthe health services regarding the hernia prior to surgery. Answerswere matched to data recorded in the Swedish Hernia Register andanalyzed.Results: The response rate was 1441/1967 (73.3%). 30.7% (442) ofthe responders were operated on as emergencies. The median age atsurgery was 58 years and the median time from surgery to complet-ing the questionnaire was 4.7 (range 1.4-11.8) years. 50.7% of thepatients who were operated on as emergencies, stated that they werenot aware that they had a hernia, prior to surgery. 31.3% of themhad not had any groin symptoms prior to surgery and 22.2% had nosymptoms at all.Conclusion: There is a considerable difference in complaintsbetween patients who have elective and those who have emergencyprocedures for femoral hernia. Patients who have emergencyprocedures are often unaware of their hernia. It is thus notreasonable to believe that screening programs would identifyand allow for elective repair in a sufficient number of femoralhernias to be effective in preventing mortality related to emergencyprocedures.
O-025Outcomes of emergency groin hernia surgery in adistrict teaching hospital: A 2-year studyV. Cijan, M.
v
Scepanovic, M. Brankovic, P. Bojovic, Z. Pudar,P. CabunacClinical Hospital Center “Zvezdara”, Department of surgery,Belgrade, Serbia
Background: While groin hernias in general remain a substantialpart of modern surgical practice, the special consideration of incar-cerated groin hernias has received relatively little attention to date.Of all inguinal and femoral hernia repairs 5,1% and 35,2 % respec-tively, present as emergencies accounting for significant morbidityand mortality, which have remained unchanged in the last fewdecades. The optimal technique for incarcerated groin hernia repairremains contentious. The aim of this study was to evaluate the out-comes of emergency groin hernia surgery performed in a districtteaching hospital for a 2-year period.Methods: A retrospective database of 163 patients who underwentemergency groin hernia repair between 2008-2010. year was main-tained. Demography, type of hernia and procedure categorized intissue approximation (Bassini, Lotheisen-McVay, Shouldice) andopen tension-free mesh repair (Lichtenstein) group, complications,hospitalisation and recurrence were recorded.
Results: 115 males and 48 females of mean age 68,3 with incarcer-ated groin hernia were evaluated; of these, 124 were inguinal and39 were femoral.There were 97 primary tissue repairs and66 Lichtenstein procedures with median hospitalisation of 6.65 days.Bowel resection was required in 27 patients.The overall postopera-tive mortality rate was 4.3%. 11 patients developed postoperativehaematoma, 10% had wound seroma and 6.1% wound infectionswithout mesh removal. Recurrent hernias had appeared in 7 patientsat one year follow-up.Conclusion: Emergency groin hernia surgery is associated withsignificant morbidity, mortality and longer hospitalization, comparedto elective hernia repair. Incarcerated hernias were more commonin men, but intestinal resection was required more often inwomen, mainly related to femoral hernia. Elective groin surgeryshould be preferred to avoid the complication of incarceration.Lichtenstein hernioplasty can be successfully used in the manage-ment of incarcerated groin hernias with good surgical outcome.
O-026Interim analysis of a comparative randomized study:Benefit of AbsorbaTack™ absorbable fixation in thetreatment of inguinal hernia by laparoscopic approachM. Lepere1, W. Cobb2, D. Giles3, U. Novitsky3, H. Scheuerlein4,V. Narula5, J. Ponsky6, B. Matthews7, T. Barthes8, H. Johanet9,M. Rosen101 Clinique Saint Charles, Laparoscopic Surgery, La Roche Sur Yon,France; 2 Greenville Hospital System, France; 3 Uconn HealthCenter, France; 4 Jena University, France; 5 The Ohio StateUniversity, France; 6 University Hospitals Case Medical Center,France; 7 Washington University School of Medicine, France;8 Poitiers Polyclinic, France; 9 Clinic Saint-Marie, France; 10 CaseMedical Center, University Hospitals of Cleveland, France
Background: To avoid mesh migration after inguinal hernia meshtreatment, mesh fixation is recommended. However, postoperativepain and permanent mesh fixation may be correlated. An absorbablefixation device might provide adequate initial fixation strengthwhile reducing long term postoperative discomfort. To compareAbsorbaTack™ (absorbable fixation) versus ProTack™ (permanentfixation) during laparoscopic inguinal hernia mesh repair, a prospec-tive randomized multi-institutional study evaluating fixation efficacyand postoperative pain has been conducted.Methods: 96 patients were randomized in 10 centers. 46 patientsunderwent laparoscopic hernia mesh repair with AbsorbaTack™fixation (group A) and 50 with ProTack™ fixation (group P). Patientpain (PI-NRS pain scale) and other outcomes were assessed from thepreoperative visit to the six-month follow-up visit.Results: The demographic characteristics and minor complicationrates were comparable. Two recurrences occurred in group P, nonein group A (non significant). No mesh migration nor infection werereported in both groups. On the other hand, despite randomization,pain prior to surgery was found significantly higher for group Acompared to group P (median 1 vs 0, p=0.03). When compared tothe baseline, the pain (PI-NRS) was reduced at one month and sixmonths (median difference -1 and -2, respectively) in group A. Whencompared to the baseline, the median difference was 0 in group Pat one month and six months.Conclusion: AbsorbaTack™ absorbable fixation shows a benefitwhen judged on the median post operative pain level decrease frombaseline. This benefit may be reinforced with the full absorption ofthe device. The two study groups showed comparable degrees ofefficacy and safety (based on recurrence rates and post operativecomplications). These promising results need to be confirmed withlonger follow-up.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S7

S8 Hernia (2011) 15 (Suppl 2): S1-S35
O-027Risk factors for complications in groin hernia surgery;a National Register StudyP. Nordin1, K.J. Lundström1, G. Sandblom2, S. Smedberg31 Östersund Hospital, Department of Surgery, Östersund, Sweden;2 Huddinge University Hospital, KI, Department of Surgery,Stockholm, Sweden; 3 Helsingborg Hospital, Department of Surgery,Helsingborg, Sweden
Background: The outcome of groin hernia surgery is evaluatedmostly comparing recurrence rates and long term pain. The aim ofthe present observational population-based registry study was toanalyze and identify risk factors for postoperative complications andanalyze the relative risk of reoperation for recurrence for respectivecomplication.Methods: Using data from the nationwide Swedish Hernia Registerbetween 1998 and 2009 150514 herniorraphies was analyzed withrespect to postoperative complications occurring within 30 days ofsurgery.Results: Risk factors significantly affecting the rate of postoperativecomplications were Laparoscopic repair (Odds Ratio OR 1.35, 95%confidence interval (CI) 1.24-1.47) and open pre peritoneal tech-niques (OR 1.31, CI 1.15-1.49) with open anterior mesh as referencecategory, general (OR 1.30, CI 1.23-1.37) and regional (OR 1.53,CI 1.43-1.63) anesthesia with local anesthesia as reference category,emergency procedures (OR 1.58, CI 1.47-1.71), recurrent herniarepair (OR 1.39, CI 1.27-1.52), femoral hernia (OR 1.30, CI 1.14-1.48), age > 65 years (OR 1.26, CI 1.21-1.31) and duration ofsurgery exceeding 50 minutes (OR 1.27, CI 1.22-1.33). Relativerisk (RR) for reoperation for recurrence related to complicationswere hematoma (RR 1.23, CI 1.05-1.45), severe pain (RR, 1.84,CI 1.39-2.45) and the group other complications (RR 1.69,CI 1.41-2.01).Conclusions: In groin hernia repair open anterior approach and localanesthesia are associated with less risk of postoperative complica-tions.
O-028Tailored Hernia Surgery with 3-D-Meshes –first results of a german multicenter study with1,467 patientsR.L. Lorenz1, A.K. Koch21 3Chirurgen, Hernia center, Berlin, Germany; 2 Chirurgische PraxisCoobus, Hernia center, Cottbus, Germany
Background: Large-scale data for the inguinal hernia repair in anambulant setting are rare. 16 german hernia centres in the ambula-tory sector with expierience using 3 dimensional and partlyresorbable Meshes for inguinal hernia surgery initiating an database for ambulatory hernia surgery. We analysed the data of1,467 patients for risk of reoperation and early postoperativeresults after 4 and 12 weeks including the risk of chronic inguinalpain.Methods: Prospective recording of all inguinal hernia repairs using3- D- meshes since 1st October 2009 till 30th September 2010 in aonline based Hernia Database (www.qs-leistenhernie.de). A clinicalfollow up was after 4, 12 and 52 weeks by the surgeon. We are pre-senting the first final results an analysis of 1,467 cases (1,271 malesand 158 females). There is a continuous registration of all consecu-tive operations.
Results: There are 1,271 males and 158 females. The average agefor males and for females was 53 years. The average operation timewas 38 minutes. About 10,8% of the procedures are recurrent her-nias. Ultrapro Hernia System (UHS, Gilbert Procedure) was used in56% and UPP (Ultra Pro Plug) in 44%. There were 6 infections(0.5%) and 6 early recurrences (0.5%) reported. Sensory disturbancewas reported after 4 weeks in 14% and after 12 weeks in 7%.Inguinal pain was found after 4 weeks in 7.0% and after 12 weeksin 3.7%.Conclusion: Although hernia repair with 3 dimensional partlyresorbable meshes was not associated with more perioperativecomplications, and less impairment of inguinal sensibility after12 weeks. Incidence of pain were comparable or less than othertechniques. The ongoing data base is feasible to perform a continu-ous documentation and quality control in hernia surgery as well inthe ambulatory sector.
O-029Complex ventral hernia reconstruction: Long-termresults after component separation and porcine biologicgraftR.M. Dunn, J.A. O’Brien, Z.M. HurwitzUniversity of Massachusetts Medical School, Division of Plastic andReconstructive Surgery, Worcester, United States of America
Background: Complex ventral hernias represent unique challengesin reconstructive surgery. The abdominal wall serves as both a struc-tural entity as well as a dynamic, functional one; both elements areimportant to consider in its reconstruction. Biologic implants haveprovided surgeons with reconstructive alternatives to successfullymanage complex ventral hernias when risk of wound complicationsassociated with synthetic mesh is excessive. This study reviews andevaluates our results using an acellular porcine dermal implant(Permacol Biologic Implant™) to restore both the structure and func-tion of the abdominal wall.Methods: This study is a retrospective review of thirty-five consecu-tive patients who underwent abdominal wall reconstruction by a sin-gle surgeon between 9/2006 and 9/2010 using Permacol™. Preoperative(age, BMI, and comorbidities), perioperative (hernia size, wound clas-sification, type/location of mesh, components separation, quiltingsutures, number/duration of drains) and postoperative variables (lengthof follow-up, complications including recurrence, enterocutaneousfistulae, and seroma) were examined.Results: Thirty-five patients underwent abdominal wall reconstruc-tion using Permacol™. Mean age and BMI were 54.2 years and 33.5,respectively. Most (86%) had overlay mesh placement with 74%undergoing component separation. Ten (29%) patients developedseromas, five required reoperation. Three of eighteen who had quilt-ing sutures developed seromas (17%) compared with seven seromas(44%) out of sixteen non-quilted patients. Mean mesh size was473 cm2. With an average follow-up of 18.7 months (range 0-48),there was one recurrence (2.9%).Conclusion: The combination of component separation techniquewith onlay of crosslinked acellular porcine dermis has provided sta-ble abdominal wall reconstruction in our series. We report a lowerrecurrence rate than typically reported. We primarily employed anoverlay technique, allowing reloading of the external oblique bysewing to its cut edges. We hypothesize that this maneuver, inconcert with re-medialization of the rectus muscles, allows for aphysiologic reconstruction of the abdominal wall.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S8

Hernia (2011) 15 (Suppl 2): S1-S35 S9
O-030No mesh related adverse events at 2 years in50 consecutive patients treated with Dynamesh IPOMtechniqueB. Smet1, P.R.L. Pattyn1, I. De Keukelaere2, J. Casaer2, P. Vuylsteke11 H. Hart Roeselare, Surgery, Roeselare, Belgium; 2 AZ Lokeren,Surgery, Lokeren, Belgium
Background: Polyvinylidene Difluoride-coated polypropylene meshescan be used in laparoscopic abdominal wall hernia repair. There arereports in the literature of high rate of early meshrelated adverse eventsleading to surgical re-interventions and even meshexplantation. Wehave looked at our own series of patients with lap placed Dynamesh.Methods: 50 patients were treated with lap IPOM technique usingDynamesh in a 2 year period in two centers. Patient demographicsand surgical procedures were equal in both centers.Results: With a mean of 1 year follow-up we report 1 mesh explantdue to a perop iatrogenic small bowel injury. We had no mesh relatedexplants nor surgical re-interventions due to mesh related obstruc-tion episodes. No clinical recurrences were seen.Conclusions: We cannot confirm earlier reports of high rate of earlymesh related complications requiring mesh explant.
O-031Prophylactic use of ventral patch mesh® in postrocarhernia in bariatric surgeryS. Morales-Conde, J. Cañete, M. Socas, A. Barranco, I. Serrano,I. Alarcón, J.A. Navas, D. Bernal, J.M. Cadet, F.J. PadilloUniversitary Hospital Virgen del Rocio, General and DigestiveSurgery, Innovation and minimal invasive surgery, Seville, Spain
Background: Given the risk involved in the development of herniain trocar site after laparoscopic surgery in morbid obesity patientsespecially (0.02-2.4%), the objective of this review is a prospectivestudy in morbid obesity patients undergoing bariatric surgery whichis applied prophylactically Proceed Ventral Patch mesh® hernia pre-vention in ports postrócar from 12 mm.Methods: Were collected bariatric surgery patients between theperiod from July 2009 until the date on which use Proceed VentralPatch mesh® for the prevention of post-trocar hernia at trocar mod-els most likely to develop a hernia (12 mm trocar in the vacuum leftby-pass and 12-mm trocar in the left upper quadrant where the pieceis removed in patients undergoing sleeve gastrectomy).Results: A total of 139 morbid obesity patients were operated in ourunit in which the mesh was used prophylactically. 67 of these patientswere for gastric bypass (48.2%), 68 to sleeve gastrectomy (48.9%),4 cases were performed in single port (5.8%) and 4 adjustable gas-tric banding (2.9%).The mean follow-up of patients after surgery is 6.32 months.The results showed a total of 5 surgical complications, including 3in which gateway Proceed Ventral Patch mesh® used correspondingto 2 wound seromas (1.43%) in gastric bypass and 1 superficial infec-tion injury, treated conservatively (0.7%) in a patient operated on forgastric bypass. The other two complications were seromas presentedat the other trocar wounds than prophylactic mesh (one for bypassand another to Sleeve).We do not present any incidence of trocar hernia during follow-upof our series in any trocars.Conclusions: Current data suggest that an individualized approachto the closure of the trocar is associated with a 0% incidence oftrocar hernia, similar morbidity among the trocars to which places amesh and those that do not close.
O-032Bio-absorbable meshes use in abdominal wallreconstruction and hernia repair in case ofcontaminated surgical fieldsL.J. Sanchez, M. Bernini, L. Bencini, M. Farsi, B. Boffi, R. MorettiCareggi Hospital, Chirurgia Generale Oncologica, Florence, Italy
Despite laparoscopy post-incisional abdominal hernias are still verycommon. Some patients (up to 20%) could potentially live with theirabdominal wall defect without any further problem, but the major-ity of abdominal wall hernias needs a repair, which is commonlyperformed with the use of synthetic prosthesis either throughlaparoscopy or open surgery.To date, there are some series in literature of huge and contaminatedcases repaired by means of absorbable biological meshes, with arecurrence rate ranging from 4% to 53%.In our experience we favour the laparoscopic repair even for verywide defects. Our recurrence rate is 13% at a 10-year follow-up. Ourindications for the use of biological or synthetic absorbable meshesare: contaminated surgical fields, infected meshes of previous repairsor a wide surgical wound dehiscence (burst abdomen).In the last two years we treated 8 patients using biological absorbablemeshes.6 of them had fistulas originating from an infection of a retromus-cular polipropilene prosthesis previously placed. In 2 cases we useda bovine pericardium biological mesh (TUTOMESH®). In theremaining 4 cases we placed a swine dermal biological prosthesis(Permacol™; Tissue Science Laboratories plc, Covington, GA,USA). While in 2 cases of midline abdominal wall hernias, in asso-ciation with a colostomy for neoplastic disease, we chose to placeabsorbable synthetic meshes (GORE®BIO-A® Tissue Reinforcement,W.L. Gore & Associates, Flagstaff, AZ).In 5 cases the mesh was put in a “sublay” manner, suturing rectusmuscles sheath above it, while in 3 cases it was placed in a “inlay”fashion, being sutured at the edges of the defect, since it was impos-sible to close the rectus muscles sheath.Results are encouraging. We didn’t register any surgical complicationand no infections developed even in very contaminated fields. Follow-up is still too short to draw any conclusion and will continue.
O-033A Belgian multicentre prospective evaluation of a largepore tissue separating mesh in laparoscopic ventralhernia repairF. Berrevoet1, T. Tollens2, L. Berwouts3, C. Bertrand4, P. Delvaux5,J. De Gols6, F. Muysoms7, T. Lafullarde8, E. Meir9, T. De Backer10,M. Ruppert11, B. Navez121 University Hospital Ghent, General and Hepatobiliary surgery,Ghent, Belgium; 2 Imelda Hospital Bonheiden, Belgium;3 St Vincentius Hospital Deinze, Belgium; 4 Centre Hospitalier deJoliment, Belgium; 5 AZ Klina Brasschaat, Belgium; 6 CAZMidden-Limburg, Belgium; 7 AZ Maria Middelares-St Jozef Gent,Belgium; 8 St Dympna Hospital Geel, Belgium; 9 St VincentiusHospital Mortsel, Belgium; 10 University Hospital Brussels, Belgium;11 University Hospital Antwerp, Belgium; 12 Hospital St Joseph, Gilly,Belgium
Background: A variety of tissue-separating meshes have becomeavailable to use inside the peritoneal cavity. Little is known aboutthe clinical features of a lot of them caused by the lack of prospec-tive gathered data. This analysis reports multicentre prospectiveclinical data evaluating the experience with the use of Proceed®-meshin laparoscopic ventral hernia repair.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S9

S10 Hernia (2011) 15 (Suppl 2): S1-S35
Methods: Two- hundred- ten adult patients treated laparoscopically in12 different centers in Belgium with a Proceed mesh were entered in aprospective registry. Antibiotic prophylaxis, surgical technique and meshoverlap was standardized according to protocol. Fixation of the meshwas with sutures, tacks or both according to the surgeons’ preference.Peri-operative morbidity and mortality was evaluated, as were recur-rence rate and quality of life after 1 year using a SF-36 questionnaire.Approval of the Ethical Committee was obtained for all centers.Results: The mean age was 48 years (range, 18-86 years). There wereno conversions to open repair and no mortality. Complications included27 seromas/hematomas (7 aspirated), and chronic pain in 14 patients.There have been no documented infections of the mesh. At one yearFU (n=147) there have been 9 recurrences (6.1%), with acceptable, goodor excellent quality of life in 79% of patients.Conclusions: This prospective registry shows safe and acceptable resultsusing a large pore tissue separating mesh (Proceed®) for ventral herniarepair. There were no complications directly related to the mesh.However, a nation-wide multicenter evaluation still shows higher recur-rence rates after 1 year than generally reported in the literature.
O-034Operation Hernia: Achievements in Ghana during5 yearsF.C. Oppong, A.N. KingsnorthPlymouth Hospitals NHS Trustl, Hernia Service, Plymouth, UnitedKingdom
Background: Operation Hernia (OH) has over the past 5 years run asuccessful humanitarian surgical project in Ghana. Founded by theauthors in 2005 [4], the aim has been to provide treatment of herniasand training in mesh repair. The project was cradled in the WesternRegion of Ghana but has expanded to Nigeria [5] and other parts ofAfrica, Ecuador in South America, Mongolia in Asia and even toMaldova in Eastern Europe. The success of OH is mainly due to theefforts of selfless teams of volunteers from Europe and America.Methods: OH Database was established in 2009 and includesKingsnorth Hernia Grading. Data from 2005-2008 was retrieved fromtheatre records. In 2007 mosquito nets were used safely [3] insteadof more expensive brand meshes.Results: From 2005 to 2010, 2,100 hernias have been repaired by32 teams with a morbidity of 0.15% and 3 deaths. One was due toan unrelated pathology. Prevalence of hernias in Ghana 7.7%. Lessthan 40% [3] are repaired resulting in a large pool of unrepaired her-nias which become large scrotal hernias. 37% of patients have hadtheir hernias for over 5 years. There are 10 times more scrotal her-nias in Ghana than there are in Plymouth, UK. 80% suffer signifi-cant disability from their hernias [2]. The economic impact is obvi-ous. Treatment restores their health. OH has therefore contributed tothe creation of relative “wealth” of their local communities. Localsurgeons and trainees from one teaching hospital have been success-fully trained in mesh repair.Conclusion: Mesh repair of hernias can performed safely in Ghana.Treatment of hernias in Ghana is cost effective [1]. Mosquito nets canbe used safely in hernia repair in Ghana [3]. Operation hernia has pio-neered in Ghana the routine use of mesh in the repair of hernias.References:1. S.D. Shillcutt, M.G. Clarke, A.N. Kingsnorth. ArchSurg. 2010;145(10): 954-961
2. D.L. Sanders, C.S. Porter, K.C.D. Mitchell and A.N. Kingsnorth.Hernia. 2008; 12(5): 527-529
3. M.G. Clarke, C. Oppong, R. Simmermacher, K. Park, M. Kurzer,L. Vanotoo, A.N. Kingsnorth. Hernia 2008
4. A.N. Kingsnorth, C. Oppong, J. Akoh, B. Stephenson, R. Simmer-macher. Hernia 2006; 10: 376-379
5. www.operationhernia.org
O-035Belgian mission to Ghana: Viewed by the surgeonC. SommelingWaregem Hospital, Waregem, Belgium
The Belgian Section of Abdominal Wall Surgery (BSAWS) hasbeen involved in “Operation Hernia” since 2008. The “OperationHernia Project” is an non governemental organization, started in 2005on the initiative of Prof Kingsnorth (Plymouth, UK), and is supportedby the EHS.The first Belgian Mission went to Takoradi (Ghana) with threesurgeons and two nurses. In one week (five days) we performed59 operations in 54 patients, mainly for groin hernias, but also forventral hernias.In 2009 a smaller Spanish-Belgian Mission (one surgeon and onenurse) operated in Takoradi. In 2010 a third Mission, consisting oftwo surgeons and one nurse, operated in two hospitals on 54 patients,again mainly on huge and demanding groin hernias. At that momentthere was a waiting list of more than 200 patients.Due to the engagement of Dr. Bernard Boateng-Duah, Head ofMedical Services at Takoradi Hospital, patients are preselected andscreened, and are scheduled for treatment. As visiting surgeons weonly have to check the indication, and to decide if the operation canbe performed under local, loco-regional or general anaesthesia.During the three years, that we work in Takoradi clearly improve-ments have been made in the use of loco-regional anaesthesia, dueto the development of the skills by the anaesthesia-nurses and thebetter availability of drugs, contributing to a better comfort of thepatients (in the sometimes timeconsuming repairs).Also the presence of better equipment in the operation theatres (i.e.new operation lights) made life easier. There however is still a short-age in suture-material, local anaesthetics, drapes and gloves. Thismaterial was brought to Ghana by ourselves.All groin hernias in adults were treated by a Lichtensteinrepair; westill used polypropylene and poly-ethylene meshes. In the futuremeshes made of mosquitonets (also called Indian meshes) will be pref-erentially used, because of the lower costs of this material; in severalforeign studies the reliability of these meshes has been proved.Although the effect on the general health of the local people atTakoradi may be small but for the individual patient the advantagesof a hernia repair are important; he can work again, will suffer nolonger of the complaints of a huge groin hernia, and does not risksthe lifetreathening complication of an incarceration.This is rewarding and motivates us to go back again to Ghana andtry to convince other surgeons to participate in the “Operation HerniaProject”, as it is expanding her activities to other African and evenAsiatic and South American regions.In March 2011 a new Belgian Mission will visit Takoradi, this timewith three surgeons.
O-036Operation Hernia: Viewed by the residentD. Sanders
In recent years surgery has been recognized as an essential compo-nent of global health. However, long-term investment in surgicalservices in low-income countries is still lacking. By participating inoverseas humanitarian surgical projects, European Surgical traineeshave the potential to aid in the provision of surgical services in coun-tries with unmet need. These opportunities provide a challenging andinteresting working environment and facilitate the development of per-sonal and professional competence. The presentation is a personalreport on the experience gained in three Operation Hernia Missionsin South America and Ghana.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S10

Hernia (2011) 15 (Suppl 2): S1-S35 S11
O-037Humanitarian hernia surgery in rural NigeriaP. NussbaumerSurgical Clinic, Spital Lachen AG, Lachen, Switzerland
Introduction: Humanitarian hernia surgery in Benue State, Nigeriastarted 2010. In January 2011 another mission through the OperationHernia Foundation was carried out again in a rural hospital by a Swissteam. The objectives of the mission were to treat as many patients aspossible and to teach contemporary surgical techniques to the local staff.Methods: The mission was carried out in St. Mary’s hospital inOkpoga, a 100 bed institution which belongs to the health services ofthe Catholic Diocese of Otukpo. The facilities were equipped with sup-port of Operation Hernia and donations in advance (e.g. generator, oper-ating lights and diathermy machines). The campaign was announcedin the local communities beforehand and eligible patients selected.The team was made up of four surgeons, one anesthetist and a scrubnurse originating from Switzerland and England. Surgical and anes-thesiological material was purchased locally if available or else wiseprovided by the team.Results: During six days 80 patients (64 male; 16 female) with amean age of 45 (3 6/12 - 80) years were operated on. Only very fewof the preselected patients with a misdiagnosis had to be refused sur-gery. A total of 90 procedures were performed for inguinal, femoral,epigastric and lumbar hernias and hydroceles. Of the mesh repairs94% were Lichtenstein procedures. There were 9 suture repairs forepigastric and children’s hernias. Half of the interventions wereaccomplished in local and one third in spinal anesthesia.There were no immediate postoperative complications and on read-missions reported so far for a superficial infection that was treatedsuccessfully by oral antibiotics.One of the three local doctors was trained to perform the procedureindependently.Conclusion: The mission has been judged as an equally rewardingexperience for both the expat team and the local staff. Focused mis-sions like the one described can help reduce the burden of surgicaldisease by treating a large number of patients in a short spell andtraining local staff at the same time.Due to the high prevalence of inguinal hernias in Africa the need forfurther dedicated teams and missions remains high.
O-042The use of uncoated soft polypropylene forreinforcement of components separation repair ofmidline ventral herniasG.A. DumanianDivision of Plastic and Reconstructive Surgery, NorthwesternUniversity, Feinberg School of Medicine, Chicago, Illinois, USA
Background: The search continues for the ideal repair of the midlineventral hernia, and the components separation technique has a low,but still concerning, hernia recurrence rate. It has been suggested thatreinforcement of the midline closure with mesh during componentsseparation reduces recurrence rates but there are concerns that the useof synthetic mesh, particularly in an underlay position, will result inunacceptably high rates of infection, adhesion, or fistula formation.This lecture aims to compare traditional unsupported components sep-aration with those reinforced with an underlay of polypropylene meshin terms of recurrence rates and complication profiles.Methods: In 2005, the presenter’s technique evolved from an unsup-ported components separation repair to one reinforced with an intraperi-toneal underlay of uncoated soft polypropylene mesh. Over a 5 yearstudy period, there were 67 cases of midline ventral hernias repaired witha reinforced components separation technique. The results of these cases
were compared to those obtained from a review of 158 unsupportedcomponents separation repairs performed between 1997 and 2005.Results: Unsupported components separation was associated witha 25 percent true recurrence rate that required reoperation (meanfollow-up, 20.1 months), whereas components separation supportedby soft polypropylene mesh had a significantly lower recurrencerate of 3 percent during a follow-up period of 21 months. In thepolypropylene-supported repairs there were no enterocutaneous fis-tulae or infections requiring mesh removal. Two patients were admit-ted and treated conservatively for post-operative small bowel obstruc-tions, with radiologic evidence suggestive of possible adhesions tothe polypropylene mesh underlay. Both patients improved withconservative management and neither patient required reoperation.Conclusion: The use of soft polypropylene mesh for reinforcementof components separation repair of midline ventral hernias demon-strates significantly reduced hernia recurrence rates and an accept-ably low complication profile.
O-043 - VIDEOTEP repair with a sticky mesh. Yes you can!M. Michiels, R. Ceulemans, I. JacobsH. Hartziekenhuis Mol, Abdominal surgery, Mol, Belgium
Totally extraperitoneal (TEP) laparoscopic inguinal hernia repairremains, although technically demanding, our first choice in technique.Ninety percent of these procedures are performed on a day case basis.We use lightweight meshes with a dimension of 15x13 cm. For largerdefects (> 3 cm) we prefer fixation of the mesh. This video demon-strates that using a self-fixating mesh (Parietex Progrip®, Covidien) isan appealing and feasable option as an alternative to tacker fixationwithout changing the techique or dimensions of the mesh.
O-044Transabdominal preperitoneal hernioplasty withmicrolaparoscopy and mesh fixation with biologicalglueA. Noceti, E.L. Ratto, O. Perata, A. PiccardoCairo Montenotte-Savona Hospital, General Surgery, CairoMontenotte-Savona, Italy
Background: We propose a new microinvasive technique for theTransabdominal Preperitoneal Hernioplasty (TAPP), with microla-paroscopy and with biological glue fixation of the mesh. Studying theefficacy, safety and the patient compliance of microlaparoscopic inguinalhernioplasty (TAPP), with biological glue fixation of the mesh.Methods: The basic steps of the surgical technique are: pneumoperi-toneum induction with Verres in periumbelical site; disposition ofone 5 mm trocar for 30 degree optic and two 5 or less mm trocarsin right and left lower abdominal quadrant; incision of the peritoneummust be large and high enough to open the preperitoneal space inaccordance with Stoppa’s principles; then dissection of the herniasac, with removal of any plug migrated; parietalization of the sper-matic cord; insertion into the abdomen of the mesh is with endobagwith personal technique; mesh placement fixed with biological glue;closure of the peritoneal incision with a continuous suture of monofil-ament 300 or self-locking suture.Results: 251 Transabdominal Preperitoneal Hernioplasty (TAPP)with microlaparoscopy and with biological glue fixation of the meshhave been performed from 2003 to 2011. The technique was appliedto the following selected cases: hernia recurrence, bilateral herniawith or without recurrence, hernioplasty during other laparoscopicinterventions and requested by patients performing sports activities;always been performed under general anesthesia; the hospital staywas one day surgery; the recurrence rate was 1,6%; we had no major
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S11

S12 Hernia (2011) 15 (Suppl 2): S1-S35
complications nor postoperative pain syndromes through the use offibrin sealant, we had post-operative seromas in 2.3% of casesresolved completely three months in 99% of cases; return to usualactivities is faster with good patient satisfaction.Conclusions: The microinvasivity in Transabdominal PreperitonealHernioplasty decreases postoperative pain, trocar-site hernias andbleeding, without compromising the results. The result is an improve-ment in patient satisfaction.
O-045 - VIDEOLaparoscopic totally extraperitoneal inguinal herniarepair: vascular complication after 72 casesA. Meyer1, D. Bellandi2, E. Berger2, M.A.A. Ranoya2, O. Monteiro2,P.A. Alonso2, L.M.V. Guimarães21 University of São Paulo, Gastroenterology, São Paulo, Brazil;2 Professor Edmundo Vasconcelos Hospital, Surgery, São Paulo,Brazil
Background: Demonstrate vascular complications after learning curve(40 cases), show changes in surgical technique that helped reducecomplication rates and show the reasons for continuing to use thelaparoscopic extra-peritoneal approach (TEP) for hernia repair.Methods: Male, 34 years, diagnosed with bilateral symptomaticinguinal hernia, scheduled elective surgery with complete preoperativeevaluation, ASA I. Technical - Veres needle is inserted in the midlinejust above the pubis in Retzius space (suprapubic). We used three tro-cars in the midline and 0° laparoscope to dissect the preperitoneal.Insufflation with a continuous set pressure not exceeding 12 mmHg.Results: During dissection of the hernia sac injury occurred in theright iliac vein causing bleeding. Punctiform lesion was quicklycompressed by laparoscopic forceps (Maryland) with appropriatecontrol and hemostasis of the lesion. Later, the sacs were identifiedand reduced bilaterally. The 3-D anatomical polypropylene mesh(Microval; Malmont, France) is introduced through the umbilicusport. The mesh is placed over the space created for covering all sitesof hernias (indirect, direct, femoral and obturator) and be largeenough to at least 10x14 cm. Because of its anatomy conformationis not necessary to use staplers avoiding neuralgia.Conclusion: The rate of complications with TEP procedure is low.Laparoscopic hernia repair is a reproducible and reliable technique. Inour experience, there are contraindications for the TEP procedure. Thetechnique must be careful to avoid intraoperative complications that mayoccur after the learning curve. Complications can occur even after thesurgeon has acquired substantial experience.
O-046 - VIDEOModified grid iron, (F. Ugahary), hernioplastie, using anew self expandable prothesisM. SolerClinique Saint Jean, Chirurgie, Cagnes Sur Mer, France
Grid- Iron hernioplasty represent one of the last evolution of the preperitoneal approach for the treatment of groin hernias.The main difficulty of the technique, was to unrolled the prosthesisin the pre peritoneal space through a 3,5 cm incision.Since 18 months years, the author uses a new self expandable pros-thesis.The movie show the grid iron procedure:• The specific technique of pre preperitoneal space dissection, usinga very simple but specific devices.
• The use of the new expandable prosthesis, with a rigid ring thatmake easier the placement of the prosthesis in the right positionin the preperitoneal space.
300 cases were performed, without recurrence or severe chronic pain.
O-048 - VIDEOMigration of an inguinal hernia mesh 17 years afterplacementJ.S.B. Bontinck, F.E. Muysoms, D.A. ClaeysAZ Maria Middelares, Surgery, Ghent, Belgium
We present a case report about a migrated inguinal hernia mesh17 years after placement.
O-049 - VIDEOFixation of the mesh by glue in TAPP laparoscopicgroin hernia repairJ. Jerabek, J. Cagas, I. CapovSt. Anne’s University Hospital Brno, 1st Department of Surgery,Brno, Czech Republic
We present our technique of mesh fixation by synthetic surgical gluein TAPP procedure. In the 1st Department of Surgery (St. Anne’sUniversity Hospital Brno, The Czech Republic) we used this proce-dure on 150 groin hernia patients. The recommended steps of TAPPprocedure are respected. Wide preperitoneal dissection- beyond themidline and bellow the lower margin of the ramus pubis is neces-sary. Adequate size (10x15cm) of light-weight mesh (PP MESH extralarge pore, VUP, Brno) is used to cover the entire Fruchaud’smyopectineal hole. For mesh fixation we used the synthetic surgicalglue (GLUBRAN 2, GEM, Italy). The glue is applying with the assis-tance of the epidural catheter (G16-18).
O-051A systematic review of methods for mesh fixationduring laparoscopic ventral hernia repairF. Berrevoet, E. ReynvoetDepartment of General and Hepatobiliairy Surgery, UniversityHospital Ghent, Ghent, Belgium
Introduction: The use of laparoscopy in ventral hernia repair isbecoming more and more fashionable. One of the remaining techni-cal difficulties remains fixation of the mesh. Fixation should bestrong enough to prevent rupture of the mesh from the tissue andmigration into the former defect. In the meantime, trauma to theabdominal wall tissue should be kept minimal to prevent postopera-tive pain and adhesion formation.Methods: All studies describing a series of at least 30 patients oper-ated laparoscopically for ventral hernia, using one well-defined fixa-tion technique and a follow-up of at least 12 months were included inthis systematic review. The reported technique of mesh fixation wascategorized into three groups: “tacks” only, “sutures” only and “tacksand sutures”. For each treatment group the overall recurrence rate,adjusted to the number of patients treated, was calculated. No overlapbetween two 95% confidence intervals was defined as a significant dif-ference. If noted, the existence of postoperative pain was indicated.Results: A total of 29 series were included for statistical evaluation.Thirteen trials used only tacks, 2 only used sutures and 14 used bothtacks and sutures with a mean follow-up of 32, 39 and 27 monthsrespectively. The weighted proportion of the recurrence rate was 4.15%(0.0326-0.0503) for tacks only, 0.85% (0.0036-0.0134) for sutures onlyand 3.28% (0.0258-0.0398) for tacks and sutures. The articles reviewedin this study were not able to prove that sutures lead to more pain.Pain levels described are still high for all techniques.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S12

Hernia (2011) 15 (Suppl 2): S1-S35 S13
Conclusion: The use of sutures was associated with significantbetter results regarding recurrence rates compared to the use of“tacks” or “tacks and sutures”. However, it has to be mentioned thatthese “suture” trials used “closure of the defect” in their series,possibly influencing the outcome. No technique was found yet to beeffective in reducing postoperative pain.
O-053Fixation of mesh to the diaphragm during laparoscopicparaesophageal hernia repairR.H. FortelnyDepartment of General, Visceral and Oncological Surgery,Wilhelminenspital, Vienna, Austria
Introduction: The use of hiatal meshes for the repair of giant parae-sophageal hernias is associated with a significantly decreased rate ofrecurrences compared to mesh free techniques. Migration of theimplant and trauma to neighboring organs due to perforating devices,such as sutures or tacks, present potentially lethal complications. Wepropose a laparoscopic application of a titanium-coated mesh(TiSure, GfE, Germany) designated for hiatal repair, with fibrinsealant fixation (Tissucol, Baxter, Austria).Methods: Initially we performed an experimental study in 7 pigs,designed to assess the efficacy of the fibrin sealant fixation of meshin experimental hiatal repair in pigs. After a precise dissection of theright and left crura and the crural commissure TiSure was implanted.For circular and three dimensional mesh fixation onto the diaphragmwe used fibrin sealant applied with the Easy Spray system. Animalswere sacrificed after 4 wk, and meshes were explanted after macro-scopical assessment of the correct position and tissue integration.Histology was performed.Results: All meshes showed excellent tissue integration and no signsof migration or dislocation. FS was completely degraded andreplaced by well vascularized fibroblastic tissue. Based on theseresults a patient (male, 59 y) presented at our outpatient departmentwith a giant paraesophageal hernia with an intrathoracic upside-downstomach. In elective laparoscopy, the stomach was repositioned andthe crura of the diaphragm were approximated with nonresorbablesutures. The defect was reinforced with a TiSure and fibrin sealantapplied with a laparoscopic spraying device. No perforating fixationdevice was used for mesh fixation itself. The patient has fully recov-ered, showing no recurrence or adverse effects 1 year postOP.Conclusion: Based on good results from own experimental trials, themesh sealing approach in hiatal hernia repair was performed clini-cally, yielding an excellent result in this case. Multicenter trials toassess the full impact of FS mesh fixation in combination withmacroporous hiatal meshes seem mandatory.
O-057Internally measured, individually tailored andgeometrically positioned laparoscopic mesh repair ofparastomal herniaA. Doka, I. Smith, M. KassaiMonklands Hospital, General Surgery, Airdrie, United Kingdom
Background: Parastomal hernia is considered to be an almostinevitable complication of stoma formation, with a reported incidenceof around 50%. Historically, repair has been discouraged due to highrecurrence rates. We describe our experience with a method of indi-vidually tailored and positioned laparoscopic mesh repair.Methods: After reduction of hernia content, intra-corporeal measure-ment of the defect is performed. The diameters of stoma and defectare measured. These are marked on a templating sheet (as supplied
with a commercially manufactured mesh) such that the defect iscentered on the mesh. The geometrical relationship between the anchorstitches and bowel cut-out is established. The corresponding anchorstitch positions are determined and marked intra-abdominally. If thedefect is more than 3cm greater than that required for the stoma, anadditional nylon “scaffolding” suture is placed prior to insertion of themesh. The mesh is deployed with anchor stitches placed at the markedpositions, thus ensuring close approximation of the mesh to the bowelwall, leaving only sufficient space for passage of the stoma. The meshis secured with a single crown tacking technique.Results: 17 patients underwent surgery over 26 months. 2 had no freeperitoneal cavity and therefore required conversion to open repair.Composite mesh with PTFE was used in 7 cases, collagen-coated in10. These 10 patients form our study group. A “scaffolding” supportsuture was placed in 5 cases. Average operating time was 65 minutes.One patient needed redo surgery 2 days later. Average blood loss was25 ml. No mesh infection was recorded. Average hospital stay was2.2 days. Follow-up ranged between 2 and 24 months. One recurrenceoccurred with each mesh type.Conclusions: Our initial results suggest that an internally measured,individually-tailored, and geometrically positioned laparoscopic meshrepair is safe and effective.
O-058Parastomal hernia - Inter observer agreement ofintrastomal 3D ultrasoundK. Strigård1, A. Gurmu1, P. Nasvall2, U. Gunnarsson11 Karolinska Institutet, Div. of suregery, Clintec, Stockholm, Sweden;2 Sundeby Hospital, Dept of surgery, Luleå, Sweden
Background: Parastomal hernia is usually diagnosed after clinicalexamination including intrastomal palpation during Valsalva.Sometimes a CT scan is conducted to further improve diagnostics.Even so the difference between a bulging, a parastomal hernia anda protrusion may be hard to judge. In attempt to develop an effec-tive diagnostic tool, a method using intrastomal ultrasound has beendeveloped. The aim of this study was to determine interobserveragreement and reliability of this new method.Methods:A ProFocus 2202 ultrasound machine with the BK Medicaltransducer 2050 was used with the setting 9 MHz and the probecovered with a water-filled balloon according to specifications deter-mined in an earlier study. Twenty patients with permanent colostomy,and suspected parastomal hernia based on clinical examination orpatients with stoma complaints were investigated by three differentphysicians from two different hospitals. One of the physicians wasexperienced whereas the other two had limited experience. Tostandardize the 3D ultrasonography examination a strict protocol wasfollowed. The protocol categorised results as normal, a bulge or aparastomal hernia. Identification of anatomical landmarks was indi-cated. The images from the examinations were copied to USB mem-ories, allowing all three physicians to make their own evaluationaccording to a given formulary. The statistics are evaluated withFleiss’ kappa and congruence between investigators.Results: Seventeen patients were investigated by all three investiga-tors and another three by two of the investigators. Inter observerFleiss’ kappa was 0.59. The overall agreement between two investi-gators was 72.2% and by three investigators 58.8%.Conclusion: Although two of the investigators had a short trainingperiod 3 D intrastomal ultrasound show good inter observer reliabil-ity and may be the tool of choice to differentiate between a bulge,a hernia or a protrusion. With a structured training program interobserver agreement would probably increase considerably.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S13

S14 Hernia (2011) 15 (Suppl 2): S1-S35
O-059Laparoscopic paracolostomal hernia repair: The totallynew lap-re-do techniqueQ.YaoHuashan Hospital, Fudan Hernia Center, Shanghai, China
Background: Paracolostomal hernia is a common postoperativecomplication of colostomies. Laparoscopic paracolostomal herniarepairs have been reported for at least five techniques so far withvariable and unsatisfactory follow-up results, especially for the highincident rate of postoperative recurrence. Herein we developed andapplied a totally new Lap-re-Do technique to laparoscopic para-colostomal hernia repair to reduce the postoperative complications,with the quietly different idea from current laparoscopic procedures.Methods We applied the Lap-re-Do technique to laparoscopic para-colostomal hernia repairs on 17 patients with PVDF mesh from May2009 to December 2010, including 2 single-incision laparoscopic sur-gical (SILS) procedures. The demographic, perioperative, and earlyfollow-up data prospectively collected for these patients are presentedin this report.Results: All the 17 operations were performed successfully, including13 patients under routine laparoscopic procedures (median operativetime, 101.5 min), 2 patients detected with incisional hernia beingrepaired simultaneously (median operative time, 140.0 min), and2 patients under SILS procedures (median operative time, 122.5 min).No in-hospital mortality occurred, and all the patients had a mediantime of 2.0 days for stoma production postoperatively. Postoperativerecovery was uneventful for all the 15 patients (88.2%), who had amedian hospital stay of 5.6 days. Surgical and nonsurgical complica-tions occurred, respectively, for one patient with mild stoma collapse(5.9%), and one patient with arrhythmia (5.9%). In 4 weeks afterdischarge from hospital, all the patient were reexamined by physicalexamination and computerized tomography scan, and the follow-upresults (median follow-up time, 8.5 months) indicated no recurrence,no severe seroma, no intractable pain, no complications of mesh-related infection and no dysfunction of defecation.Conclusions: Laparoscopic paracolostomal hernia repair with Lap-re-Do technique is feasible.
O-060Fixation of mesh to bone in pelvic and abdominal walldefects where conventional techniques are inadequate.Long term resultsS.G.G. SmedbergHelsingborg Hospital, Dep of Surgery, Helsingborg, Sweden
Background: Overlapping in sublay position and ingrowth of meshnormally provides the most efficient cure for abdominal wall defectsof any kind. When there is lack of tissues for overlapping or sutur-ing mesh and the pressure of abdominal contents is high, fixation ofmesh to bone is an alternative. Long term results of the treatment ofthree cases with anterior pelvic ring defects after tumour resectionsand one case with a neuromuscular disorder with degradation of theentire lower abdominal wall will be presented.Methods: In three male patients with anterior pelvic hernias afterpubic bone resection a hammock of prosthetic mesh bridging thedefect was fixated to the pelvic bone edges. The distance from thehernia defect to the rectum was 2 cm. A PTFE prosthesis was cho-sen, not tearing at the fixation points and allowing suturing close tothe rectum. In the patient with neuromuscular disease no muscle oraponeurosis was available for reconstruction till halfway between
umbilicus and xiphoid. On each side a 30x30 cm polypropylenemesh, for maximum ingrowth properties, was placed diagonallypreperitoneally, overlapping the pubic bones, iliopsoas muscle, andlaterally to quadratus lomborum, and fixated by screws to the pubicbone and iliac spine, fixation points reinforced by PTFE patches.Superiorly meshes were placed sublay in the rectus sheath. Themeshes were stretched, cut and sutured in the midline.Results: The firs and third patient with pelvic reconstruction do wellwith no recurrence after 18 and 7 years. The second patient died9 years postoperatively without recurrence. The abdominal wallreconstruction is stable 2 years postoperatively. Further subcostalmuscular degradation has been treated, mesh fixated to ribs.Conclusion: Fixation of mesh to bone has proven to be a long-last-ing and reliable way of reconstructing difficult pelvic and abdomi-nal wall defects.
O-063Repair and reconstruction of abdominal wall defectsafter excision of abdominal wall tumorsY. Gu, R. Tang, D.Q. GongDepartment of General Surgery, Shanghai Ninth Hospital, Herniaand Abdominal Wall Surgery Center, Shanghai Jiaotong UniversitySchool of Medicine, Shanghai, China
Repair and reconstruction of abdominal wall defects after abdomi-nal wall tumor resection often present the abdominal surgeon with avery challenging problem. Complete resection with tumor-free mar-gins is the primary goal, but this is usually attained with massivesoft tissue loss, and therefore, a large, complex abdominal wall defectresulted. This presentation will specifically focus on two aspects:classification of the abdominal wall defects and techniques used forabdominal wall repair and reconstruction which have had significantimpact on outcome of the abdominal wall tumor resection.The abdominal wall is a multilayer structure composed of severaldifferent tissues. According to the defective components of abdomi-nal wall, we categorized the defects after tumor resection into threetypes: Type I, defects involving only the loss of skin and subcuta-neous fascia when the tumor is shallow and dose not invade themyofascial layer; Type II, myofascial defects with intact skin cover-age; and Type III, myofascial defects without skin coverage. Besides,abdominal zones were assigned based on the location of the defect:Zone M: midline defect of the abdomen (subdivided to upper 1/3,middle 1/3 and lower 1/3 respectively); Zone U: upper quadrantdefect of the abdomen; Zone L: lower quadrant defect of theabdomen.Decisions regarding techniques used for abdominal wall repair andreconstruction are mainly based on an assessment of the defect byextent and location as described by classification. For Type I defects,primary sutures after adequately separating the subcutaneous tissueare preferred, free skin graft can be used only when there is a too-large defect or the patient is too thin to make suture. For type II-Mdefects, component separation with or without mesh reinforcementis preferred. For type II-U and II-L defects, a prosthetic or biologi-cal mesh, or alternatively a pedicled or vascularized autologous fas-cial substitute, is needed to replace the lost myofascial layer. Fortype III defects, the resulting full-thickness defect will require a pedi-cled or vascularized myocutaneous flap with or without a prostheticor biological mesh for abdominal wall reconstruction.Our techniques as well as detailed photos will be used to present ourrepair and reconstruction, rationale for classification and approachand the outcome of the patients in our center will be discussed.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S14

Hernia (2011) 15 (Suppl 2): S1-S35 S15
O-067Systemic injury of aponeurosis as the reason ofdevelopment of herniaK.M. MylytsyaZaporizhzhya Medical Academy of Postdiploma Education, Surgery,Zaporizhzhya, Ukraine
Background: Traditionally, the main reason for hernias development,is considered to be the sharp increase of intra-abdominal pressure orthe incorrectly executed operative intervention. The objective of thisstudy was to find the pathological mechanisms of hernia foundation.Methods: In our research we’ve undertaken a number of compara-tive histomorphologycal tests to specify the features of aponeurosiscondition with 60 patients. First group - 30 patients who have ven-tral hernia. Another group - 30 patients with normal abdominal wall.Results: The research results have shown that in first group all patientshave evidence of connective tissue dysplasia. Destructive and dys-trophic changes of aponeurosis as misarrangement of collagenic fibres,i.e. their fragmentation, lysis, nidal picrimophylia were observed.Infringed collagen synthesis also proves the decrease in functionalactivity of fiberplasts. Elastic fibres are or irregular thichkness, andare also fragmented and partially lysed. The quantity of sulphated gly-cosaminoglycan that provide fibrillar genesis and define the durabil-ity of connecting tissue is lowered, also as well as quantity of chon-droitin sulfate and hyaluronic acid, which reflects the sclerosisphenomenon of proves the increased confusion of connective tissue.Thus, in case of connective tissue dysplasia we can also observe adefinite morphologycally and histochemically confirmed infringementof aponeurosis structure, which forms the basis for development andformation of hernia, including progressive and recurrent one.The histomorphologycal tests of aponeurosis condition of secondgroup was absolutely contrary. Any significant changes of collagenicfibres or decrease in functional activity of fiberplasts were not found.Conclusion: If we admit the fact that hernia is not a mechanicaliatrogenic injury, but an innate pathology of connective tissue, thenthe need to alter the approaches to treatment and prevention of her-nias appears to be obvious. And, of course, the issue of terminologycomes up on the agenda.
O-068The efficacy of fibrin sealant fixation of hydrophobicimplants in experimental onlay repair in ratsS. Gruber-Blum1, A.H. Petter-Puchner2, J. Brand1, H. Redl1,K. Glaser2, R.H. Fortelny21 Ludwig Boltzmann Institute for Experimental and ClinicalTraumatology, Experimental Research, Vienna, Austria;2 Wilhelminenspital der Stadt Wien, II. Department of GeneralSurgery, Vienna, Austria
Background: Fibrin sealant (FS) mesh fixation has gained increasingpopularity in open and laparoscopic hernia repair and works especiallywell with hydrophilic implant materials, eg. titanized meshes. The aimof this study was the assessment of FS fixation of hydrophobicimplants. A polypropylene mesh coated with α-Ω fatty acid (CQ,c-qur lite®, Atrium) was tested in experimental onlay repair. Preservedpores facilitate FS fixation.Methods: 16 CQ (2x2 cm) were implanted in 8 male Sprague Dawleyrats. 2 different groups were investigated. Meshes were either fixedwith FS 4 I.U. only (treatment) or sutured only (control). Follow-upwas four weeks. Evaluation criteria were mesh dislocation, seromaformation, tissue integration and adhesion formation. Histology wasperformed (Hematoxilin Eosin staining and Cytokeratin staining).
Results: Despite the hydrophobic mesh coating and excessive move-ments of the animals during the observation period, FS alone yieldeda reliable fixation. No mesh dislocation occurred, no seroma wasdetected and mesh integration was excellent.Conclusion: Fixation of hydrophopic meshes with FS in onlay repairis feasible.
O-069Athletic pubalgia - anterior pelvic floor repair as antherapeutic optionA. Koch1, R. Lorenz21 Day Surgerey Center, Cottbus, Germany;2 3 Chirurgen, Berlin, Germany
Background: Recent publicity and some scientific reports suggestincreasing success in treating an entity called “sports hernia” - moreaccurately named athletic pubalgia. The former concepts do not takeinto account the likely mechanisms of injury or various patterns ofpain that these athletes exhibit. The author believes that the conceptof a “pubic joint” or “pubic dynamic complex” is fundamental tounderstanding the anatomy and pertinent pathophysiology in thesepatients. Many injuries can now be treated successfully. Some of theinjuries require surgery and others do not.The author is a generalsurgeon and team doctor of an 2nd league soccer team in Germany.Methods: The Approach to anterior pelvic floor repair is theunderstanding of this Complex. Most of the athlets can be cured bya conservative treatment including physiotherapy and sometimesinjections.Results: Between 1.1.2006 until 31.12.2010 352 Athletes presented andonly 46 received operative treatment (13.1%) 28 soccer players 4th-5thleague 6 soccer players 1st and 2nd league 5 soccer players 3rd leaue1 U21 national player 4 hockey Professionals 2 marathon runners46 Patients with anterior pelvic floor repair (7 bilateral, 39 unilateral).All 46 Patients returns after 8 Weeks to full play.Conclusion: The decision to an operative treatment is highly selec-tive. Revision of the inguinal canal is not enough. Anterior pelvicfloor repair is the most effective method with the lowest recurrencerate and the athlets can return to play fully after 2-3 months.
O-070Quality management in day case Hernia surgery inGermanyR. Lorenz1, A. Koch21 3Chirurgen, Hernia center, Berlin, Germany; 2 Chirurgische PraxisCoobus, Hernia center, Cottbus, Germany
Background: In Germany the health system is strictly separated inan ambulatory and a hospital sector. The percentage of day caseHernia surgery in Germany is very low comparing to the average ofthe industrial countries - last studies have shown a part of only 20%.The improvement of this part could save a lot of money.Methods: We developed a large multicenter study together with 16specialized hernia centers in Germany. This could be a first possiblestep in the development of a country covering database. This stepshould show that in the ambulatory sector the same high qualityresults are possible as in the hospital sector.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S15

S16 Hernia (2011) 15 (Suppl 2): S1-S35
Results: In our study we demonstrate that in average 60% of theinguinal hernias can be done as a day case. Hernia repairs in theambulatory sector are not associated with more perioperativecomplications or a higher recurrence rates. The incidence of pain iscomparable or less to other techniques.Conclusion: Day case surgery is feasible without a lower safety stan-dard for the patient. The quantity of day case Hernia surgery couldbe raised up to 60%. Ongoing data base are necessary for a contin-uous documentation and quality control.
O-071Long-term outcome after randomizing Kugel versusLichtenstein repairS.W. Nienhuijs1, J.F. Staal2, L.J.A. Strobbe3, C. Rosman31 Catharina Hospital Eindhoven, Surgery, Eindhoven, Netherlands;2 Slingeland Hospital Doetinchem, Surgery, Doetinchem,Netherlands; 3 Canisius-Wilhelmina Hospital, Nijmegen, Netherlands
Background: The open preperitoneal approach in inguinal herniarepair has shown to be a feasible alternative for the open anteriorapproach. In short-term results a tendency for less neuropathicwas seen. The objective of this study the review the long-termresults.Methods: A total of 172 patients have been blindly and randomlyallocated to receive open anterior (Lichtenstein) or open preperitoneal(Kugel) inguinal hernia between 2005 and 2006. This study groupwas sent a postal questionnaire focussing on pain limitations andsensory disturbances.Results: Two patients have died in the follow-up, another 7 wereuntraceable. 140 out of 163 patients completed the questionnaire(86%). Two recurrences were encountered in the Kugel groupversus 5 in the Lichtenstein group (p=.277). Three-quarters of thegroup reported no pain, 21.6% rated their [ain as mild. On a VerbalDescriptor Scale pain was graded some higher in the Lichtensteingroup (p=.021). The mean VAS pain score was 5.5 after posteriorand 7.3 after open approach (p=.477) of the total group. No patientused analgesics. Three patients rated their limitations on daily activ-ity as severe, five as moderate and the remaining mild/none. 16patients reported numbness after Lichtenstein versus one in the othergroup (p<.001). After a Kugel repair significantly less frequent feel-ing the mesh was reported (p=.008).Conclusion: Although some differences in pain parameters werefound, overall there is no clinically relevant difference in chronicpain after a Kugel and Lichtenstein repair. In the latter group signif-icantly more numbness and foreign body feeling was reported,confirming the initial finding a preperitoneal position of a mesh isless likely to cause sensory disturbances.
O-072Validation of Biodex system 4 for measuring musclestrength in patients with rectus diastasisP.M. EmanuelssonClintec, Of surgery, Stockholm, Sweden
Background: To investigate the validity and reliability of the BiodexSystem 4 in the assessment of abdominal strength in patients withrectus diastasis.
Material and methods: Ten healthy volunteers and ten patients withrectus diastasis of more than 3 cm were recruited. Test-retest relia-bility at 30°/s respectively 60°/s extension/flexion spinal angles aswell as isometric muscle strength with and without abdominal gir-dle were assessed. Reliability was calculated using the InterclassCorrelation Coefficient (ICC) method. Validity was evaluated by cor-relation with the International Physical Activity Questionnaire (IPAQ)and a Visual Analogue Scale (VAS) used for self-assessment ofabdominal muscle strength. The Kendall-Tau and Spearman statisti-cal tests were used.Results: Reliability was excellent with ICC values ranging between0.77 and 0.97. No significant difference in muscle strength was seenfor tests with or without a girdle except with 60° of extension. Theinternal validity assessed as correlation between VAS assessment andisometric strength measurements (p=0.0077) was excellent, whereasthere was no correlation to IPAQ.Conclusions: The Biodex System 4 has been shown to be a valu-able and reliable instrument to measure abdominal wall strength inpatients suffering from rectus diastasis. The internal validity is excel-lent. The incongruence between abdominal muscle strength, as meas-ured using the Biodex system 4 and IPAQ indicates that there is norelationship between general physical activity (IPAQ) and musclestrength in patients with rectus diastasis.
O-073Umbilical hernia repair with bioabsorbable plugdecreases recurrence rate at 31 monthsK.A. LeBlancMinimally Invasive Surgery Institute, Surgery, Baton Rouge, UnitedStates of America
Background: Adult umbilical hernias are routinely performed as aprimary repair and pose a higher risk for recurrences. A bioab-sorbable plug could provide benefits to reinforce the primary repair,without long-term complications associated with a permanent pros-thetic. This is the first study to evaluate the use of a fully biore-sorbable plug to repair umbilical hernias in terms of recurrence ratesspecifically.Methods: Patient selection for this prospective study was based onumbilical hernia defects less than 4 cm in greatest dimension in pri-mary or recurrent anterior abdominal wall hernias. Between June2006 and November 2008, 72 patients underwent open umbilical her-nia repair with GORE® BIO-A® Hernia Plug (W.L. Gore andAssociates, Newark, DE). The disc portion of the plug was placedthrough the fascial defect into the preperitoneal space and sutured inplace. The defect was closed over the plug with permanent suture.Early and late complications were analyzed.Results: Average defect size was 3.9 cm2 (1-9.9 cm2). Average fol-low up time was 31 months (1-50 months) through phone conversa-tion or office visits, with 81% of patients having followup of atleast 24 months. Minor complications occurred in the postoperativeperiod in 7 (9.7%) patients including seroma (1.4%), and wounddehiscence (2.8%). One (1.4%) recurrence was reported in long termfollow up.Conclusions: The results indicate that the use of GORE® BIO-A®
Hernia Plug alone to reinforce primary repair of umbilical defectsless than 3 cm in diameter can reduce the expected recurrence rateof 11-44% to 1.4%. This is a significant advancement in the repairof umbilical hernias. Permanent mesh may not be needed in themajority of these patients unless there appears an inherent weaknessin collagen synthesis. In our practice, it has become the standardrepair for these types of hernias.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S16

Hernia (2011) 15 (Suppl 2): S1-S35 S17
O-074Laparoscopic versus Open incisional hernia repair:A randomized clinical trialH.H. Eker1, B.M.E. Hansson2, M. Buunen1, P.J. Klitsie1,I.M.C. Janssen3, E.G.J.M. Pierik4, W.C. Hop1, H.J. Bonjer5,J.F. Lange1, J Jeekel11 Erasmus Medical Center, Department of Surgery, Rotterdam,Netherlands; 2 University Medical Center Nijmegen and CanisiusWilhelmina Hospital Nijmegen, Department of Surgery, Nijmegen,Netherlands; 3 Rijnstate Hospital, Department of Surgery, Arnhem,Netherlands; 4 Isala Clinics, Department of Surgery, Zwolle,Netherlands; 5 VU Medical Center, Department of Surgery,Amsterdam, Netherlands
Background: The ongoing debate about the merits of endoscopicversus open incisional hernia repair prompts the need for a level 1randomized clinical trial. In this multicenter randomized clinical trial,quality of life outcomes, postoperative pain, operative data, hospitaladmission and recurrence rates in the two different techniques areanalyzed.Methods: Ten hospitals randomized 206 patients to laparoscopic oropen mesh repair. Patients with an incisional hernia larger than threecm and smaller than 15 cm, either primary or recurrent, wereincluded. Quality of life was assessed with EuroQoL, SF-36 ques-tionnaires and Visual Analogue Scales for pain and nausea. Operativedata were documented according the study protocol. For recurrencerates and influencing factors, follow-up controls at the outpatientclinic have been performed.Results: Quality of life questionnaires, completed at least five daysbefore surgery and at one and four weeks postoperatively, showedno significant differences between the groups. Blood loss during theoperation was less (39 ml vs 63 ml, p=0.04), as well as the numberof patients receiving a wound drain in the laparoscopic group (3%vs 43%, p<0.001). The theatre time for the laparoscopic group waslonger (96 min vs 72 min, p<0.001). At a follow-up period of44 months a recurrence rate of 16% was reported in the open arm,and 17% in the laparoscopic (p=0.32). The size of the defect wasfound to be an independent predictor for recurrence (<0.001).Conclusions: Laparoscopic surgery appears to have no advantage inhealth related quality of life compared to open surgery. During theoperation there is less blood loss and less often need for a wounddrain. The theatre time, however, is longer in the laparoscopic group.Recurrence appear to be equal with both techniques. Defect size isfound to be an independent factor for recurrence of incisionalhernia.
O-075What can we expect from tissue separating patches forumbilical and ventral hernia repair: 12 monthoutcomes using the international hernia mesh registryF. Berrevoet1, J. Mitchell2, L. Lin3, L. McRoy31 University Hospital Ghent, General and Hepatobiliary surgery,Ghent, Belgium; 2 Ethicon UK, division of J&J Medical Limited,Belgium; 3 Ethicon INC, Belgium
Background: The use of three dimensional tissue separating patchesfor umbilical hernia repair has recently been questioned in a reportof three cases. Small series of case reports as a basis for surgicaldecision making should be abandoned in favor of prospectively col-lected data. The International Hernia Mesh Registry was designedto obtain longitudinal outcome data for hernia repair with anymesh or technique. This report presents 12 month data for tissueseparating patches designed for repair of umbilical and smallventral defects.
Methods: Established in 2007, the IHMR has enrolled over 3,200patients at 37 sites in 10 countries 18 years of age and older, under-going herniorrhaphy with a mesh. Data is collected by surgeons atpre-, peri- and post-operative time points. Patients self-report Qualityof Life Outcomes using a validated instrument (Carolinas ComfortScore™) at baseline and at 1 and 6 months and 1, 2, 3, 4 and5 years post-surgery.Results: Ventral Patch*Number of cases 87Male / Female ratio (%) 65.5 / 34.5Age (mean ± SD) 52.6 ±16BMI (mean ±) 29.9 ±6Umbilical/epigastric % 79.3Ventral/incisional % 20.7Defect diameter median (cm, range) 2.0 (0.5-5.1)Mesh size 34% small, 66% mediumPatient reported recurrences (confirmed/false(+) /unknown)(true positive rate) 8(3/1/4) 3.4%Defect diameter for recurrences 4 cm, 3 cm, 3.5 cmCases with at least one AE 10%* Proceed Ventral Patch (Ethicon, n=73) and Ventralex (Bard, n=14)Conclusion: Observed recurrence rate at 12 months is 3.4 %.Confirmed recurrences involved defects with a diameter greater than2 cm with < 2 cm overlap onto healthy fascia circumferentially.Surgeons should follow the standard of care for overlap of mesh ontohealthy tissue to minimize risk of recurrence.
O-076High fascial closure rate after open abdomen treatmentwith vacuum assisted wound closure andmesh-mediated fascial traction - a multicenterprospective studyT. Bjarnason1, S. Acosta1, B. Pålsson1, A. Wanhainen2, M. Svensson3,K. Djavani4, M. Björck2, U. Petersson11 Skåne University Hospital, Surgery, MalmÖ, Sweden; 2 UppsalaUniversity Hospital, Vascular Surgery, Uppsala, Sweden; 3 FalunHospital, Surgery, Falun, Sweden; 4 Gävle Hospital, Surgery, GÄVle,Sweden
Background: Damage control surgery and open abdomen (OA) ther-apy has been widely adopted in both trauma and non-trauma situa-tions. Several techniques for temporary abdominal closure have beenused. In an attempt to increase fascial closure rates in elderly, non-trauma patients, we developed a technique combining vacuum-assistedwound closure and mesh-mediated fascial traction (VAWCM). TheV.A.C.® system from KCI was used. A polypropylene mesh wasdivided and sutured to the fascial edge on each side. The visceral pro-tective layer of the V.A.C.® system was placed intra-abdominally andthe mesh halves sutured together in the midline. Two polyurethanesponges were placed above the mesh. The wound was covered withair-tight drapes and then connected to the negative pressure unit.Every 2-3 days the abdomen was opened, the dressing changed andthe mesh tightened. When possible, the mesh was removed and thefascia closed.Methods: Prospective, multicenter study, including consecutivepatients treated with OA and VAWCM between 2006 and 2009.Results: There were 111 patients included. Median age was 68 years.Underlying pathologies were visceral (51%), vascular (41%) andtrauma (8%). Median duration of OA therapy was 14 days (4-87).Median SOFA score at admission was 8. In-hospital mortality was30%. Eight patients (7%) developed intestinal fistula, of whom sevenhad intestinal ischemia. Definitive abdominal closure was achieved in93 of 95 patients (98%) surviving until abdominal closure, in whom
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S17

S18 Hernia (2011) 15 (Suppl 2): S1-S35
mesh reinforcement was needed in 8. Complete fascial closure wasnot possible due to cartilage formation in two patients. Four patientsdeveloped an intra-abdominal abscess after fascial closure and weretreated with percutaneous drainage. One year follow-up regardingabdominal wall function is under analysis.Conclusions: The VAWCM method provided a high rate of primarydelayed fascial closure after long-term OA treatment in mainlyelderly, non-trauma patients. Technique-related complications werefew.
O-077Laparoscopic ventral hernia repair using fibrin glueas mechanism of fixation in selected patients(defect diameter < 7 cm)G. Cesana, S. Olmi, E. CrocePoliclinico San Marco, Surgery, Zingonia - Osio Sotto, Italy
Background: Laparoscopic treatment of incisional hernia could beperformed using different types of fixation devices and prosthesis.Some author point out classical fixation mechanisms (e.g. clips andtacks) as the cause of postoperative persistent pain, postoperativeadherences and consequently intestinal obstruction, and intestinalperforation. The aim of this study is to verify the safety and feasi-bility, as well as the patient outcome, of incisional hernia laparo-scopic repair using fibrin glue as mechanism of prosthesis’ fixationin ventral defects with diameter lower than 7 cm.Methods: Since November 2006 to December 2010, 106 patientswith ventral hernias lower than 7 cm of diameter (33 incisional her-nias and 73 primary ventral hernias) underwent laparoscopic repairusing dual-side meshes (19 Hi-Tex - Textile Hi-Tec - France and87 Parietex - Covidien - USA) fixed to abdominal wall by fibringlue (Tissucol - Baxter - USA and Quixil - Ethicon - USA). Surgicalcomplications and patients’ outcome were assessed with a clinicalfollow-up.Results: Mean operative time was 32.5 minutes, depending on lysisof peritoneal adherences. We did not have to convert any of thelaparoscopic procedures. The mean time of discharge was 1 day, themean time of recovery for physical or working activities was 7 days.With a mean follow-up of 30 no seromas, no relapses, no neuralgiasno intestinal obstructions were reported.Conclusion: In selected patients, Hi-tex allows laparoscopic repairof incisional hernia using fibrin glue with a better patient outcome,especially in terms of post-operative pain.
O-078Optimizing hernia surgery in patients with advancedliver disease and ascites waiting on livertransplantation: Tips for successF. Berrevoet, A. Vanlander, P. Deseyne, X. Rogiers, R. TroisiUniversity Hospital Ghent, General and Hepatobiliary surgery,Ghent, Belgium
Background: Umbilical, epigastric or incisional hernias are a com-mon problem in cirrhotic patients. A herniorraphy is associated witha significant morbidity, mortality and recurrence rate. Although thebetter clinical outcomes with a prosthetic hernioplasty in the generalpopulation, in cirrhotic patients with ascites, its recommendations orcriteria are not standardised.Methods: Twenty-two patients (19 for umbilical, 2 for epigastricand 1 for incisional hernia) with decompensated cirrhosis wereoperated on. The indication for operation was repeated incarceration in
8 patients, while 7 patients with umbilical hernias had ulceration andnecrosis of the overlying skin. Four patients were operated for signif-icant pain. Pre-operatively, aggressive medical therapy of ascites wasconducted at the hepatology unit. Umbilical hernias were treated withthe classic Mayo repair, without mesh, in case ulceration or necrosiswas involved. Preperitoneal mesh repair was performed if no futureliver transplantation seemed indicated. On 16 patients an intra-abdom-inal drainage was performed up to 10 days to permit a tension freehealing.Results: One patient without intra-abdominal drainage developedpersistent ascites leak. Another one developed a wound infectionwith the need for removal of the mesh and suffered a severe coagu-lopathy and died due to liver insufficiency. All patients were followedup for 9-42 months. Six patients were subsequently successfully trans-planted and developed no recurrence of their hernia till that date.No other recurrences have been observed after a median follow-up of14 months.Conclusions: Symptomatic or infectious hernias in patients withdecompensated cirrhosis may be repaired safely on an elective basis,even selectively using a mesh. However, postoperative control ofascites by intra-abdominal drainage, obtaining a tension free repair,is vital for success. Liver transplant candidates, even with decom-pensated liver cirrhosis, can be safely operated on and benefit froma hernia repair after preoperative medical support.
O-079Open parastomal hernia repair: Techniques and resultsJ. ConzeRhenish Westfalian Technical University, RWTH Aachen, SurgicalDepartment, Aachen, Germany
Parastomal hernia repair remains a persisting problem in herniology.Irrespective from the type of surgical approach the follow-up revealhigh recurrence rates. Local repair shows recurrence rates of 46-100%,stoma relocation shows recurrence rates of 30-50%. Different surgicalprocedures using non-absorbable mesh in open or laparoscopicapproach were described and reported promising results with recur-rence rates at 0-30%, knowingly the limitations of small number ofpatients and follow up. Looking at the recent literature it seems thatit has become a domain of laparoscopy.But wasn’t it Israelsson who showed amazing results in placing pro-phylactic meshes during the index operation. He performed an openretromuscular mesh augmentation. Why is it so difficult to achievethese results also in parastomal hernia repair? The open approachstill has several advantages: the mesh is placed in the extraperitonealposition, reducing the risk of mesh or tack induced adhesions andother complications, no need for expensive barrier meshes and fixa-tion devices. At the same time the hernia sac can be removed andresected, the fascia ring can be narrowed by suture and last not leastthe midline also receives a mesh augmentation.Main drawback in the retromuscular approach is the limitation of themesh placement by the anatomy of the rectus sheath. The lateral bor-der of the rectus sheath restricts a sufficient mesh size, reducing theobtainable lateral overlap. When we see recurrences after meshrepair, we detect the defect usually there. Therefore we now aim fora sufficient overlap by extension of the mesh to the lateral compart-ment of the abdominal wall. This can be achieved by incision of thelateral rectus sheath reaching the layer between m. oblique externeand m. oblique interne, the Ramirez layer. In our experience this isa possible alternative for a non-laparoscopic repair. The surgical stepsand first results are presented.Beside all options and limitations for parastomal hernia repair, theprophylactic use of mesh in the index operation seems to be the mostpromising approach!
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S18

Hernia (2011) 15 (Suppl 2): S1-S35 S19
O-080Laparoscopic keyhole techniques: why they fail?B.M.E. HanssonNijmegen, The Netherlands
Introduction: The laparoscopic key-hole technique is a way torepair parastomal hernias. A mesh with a central key-hole is drapedaround the stoma loop and tacked to the abdominal wall as shownin figure A. The operation is performed by laparoscopy.Results: In the literature several studies have been published regard-ing this technique.In most studies the hernia opening was narrowed with a nonre-sorbable suture, then a 15x19 cm PTFE-mesh was fashioned with acentral keyhole defect of 2 cm and eventually 2 small radial inci-sions to create a funnel-like shape for fixation to the bowel.Recently, composite parastomal meshes are available consisting ofpolypropyleen+polyvinyledinefluoride (Dynamesh), polyester withcollagen layer (Parietex composite parastomal patch), or polypropy-leen + PTFE (Bard parastomal patch).Reviewing the literature, the keyhole technique shows an overallrecurrence rate of 20.8% with a follow-up of at least 12 months [2].We can conclude that the key-hole technique failed!Why?There are probably multiple reasons for the high failure rate as foundin the reviewed literature. First of all, most patients with hernias areprobably affected by underlying defects in wound healing and col-lagen metabolism.This explains why the narrowing of the stoma opening with nonre-sorbable suture as performed in our technique will only have a tem-porary effect, as has already been noticed by the failure rate of upto 100% when relying on tissue repair alone. Therefore, the repairof the hernia depends completely on the presence of an adequatepositioned mesh. Ideally such a mesh should achieve rapid ingrowthin the abdominal wall while being inert to the bowel. Furthermorea mesh should be highly resistant to bacterial infections. Currentlymeshes made of expanded polytetrafluoroethylene (ePTFE) are con-sidered most suitable for this purpose since they are soft and pliableand anchor to the abdominal fascia when fixed with sutures or tacks.A major disadvantage of the mesh appeared to be its tendency toshrink, as observed in almost all patients who were reoperated for arecurrent parastomal hernia in our study [1].At reoperation, the mesh appeared smaller, the central opening wider,and the funnel-shaped part everted probably due to the intra-abdomi-nal pressure and disrupture of the non-absorbable sutures (Figure B).This results in a widening of the central key-hole and is held respon-sible for the recurrence because the intra-abdominal pressure andthe tangential forces working on the abdominal wall will resultin ongoing widening of the defect according to Laplace’s law(T=PxR/2).
Conclusion: The failure of the keyhole technique is based on theprogressive widening of the central opening due to intra-abdominalforces working on it, resulting in an inacceptable high recurrencerate on the long-term.Other patches or other techniques must be investigated and RCTshould be initiated before definitive conclusions can be drawn.
References:1. Laparoscopic parastomal hernia repair using a key-hole techniqueresults in a high recurrence rate; bme hansson-rp bleichrodt-ih dehingh; surg endosc (2009) 23: 1456-1459
2. Surgical techniques for parastomal hernia repair: a systematicreview of the literature; bme hansson - nj slater - ap schouten vander velde - hmm groenewoud - or buyne - ihjt de hingh - rp ble-ichrodt; submitted annals of surgery
O-083Prevention of parastomal hernias with meshreinforcement during open surgeryT. BrandsmaNijmegen, The Netherlands
As we all know the incidence of parastomal hernias is 30 to 50%depending on the type of stoma and time of follow-up. If weconcentrate on end colostomy’s the rates are as high as 48%.Most parastomal hernias develop in the first years after surgery andabout 30% needs a surgical correction due to pain or leakage.Treatment is mandatory when obstruction or strangulation of herniacontent occurs.The surgical approach with the local tissue repair is mainly aban-doned because of the high recurrence rates. The disadvantage of thestoma relocation technique is the risk of developing a new paras-tomal hernia or an incisional hernia at the old ostomy side or mid-line incision. Recurrence rates of mesh repairs range from 7% to17%.The last decade there is more and more focus on the prevention ofparastomal hernia’s. There have been a few observational studiesinvestigating the feasibility of placing different kind of meshes in anonlay or sublay position. Because of the promising results the firstrandomised controlled trials have been published in the last years.There are a few other RCT’s currently open for inclusions.The RCT’s published so far are all in favour of mesh placement. Butdue to the limited amount of trials and the small number of patientsthere is still some doubt regarding long term follow-up and morbid-ity and safety regarding mesh placement. At this moment there area few trials open for inclusions in Europe and the United States ofAmerica. In the Netherlands we are currently performing thePreventtrial, a multicentre RCT which is investigating the place-ment of a lightweight polypropylene mesh in a sublay position dur-ing open surgery.We will discuss the different techniques and trial results of meshreinforcement with open surgery. Current trials open for inclusionswill, if possible, be briefly discussed.
O-087Fixation of the mesh during Lichtenstein groin herniarepairG. Campanelli, F. Ceriani, M. Canziani, M. Cavalli, V. BertocchiInsubria University of Varese, Multimedica Hospital, Castellanza,Italy
Introduction: After the isolation and reduction of the hernia sac, theoriginal technique requires the placement of a polypropylene mesh,tailored on the inguinal channel and fixed along the inguinal liga-ment with a polypropylene running suture and fixed on the conjointligament with two or three absorbable stitches. The Lichtenstein tech-nique, is widely used because it is easy to learn and is associatedwith a low rate of recurrences and complications.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S19

S20 Hernia (2011) 15 (Suppl 2): S1-S35
In the last years surgeons paid attention to reduce recurrence ratewith good success, so now the new object in the primary hernia sur-gery should be reduce disabling complication such as chronic pain.Estimates of chronic pain vary considerably from 0 to 53%.The European Hernia Society has defined the Pain Complex Syndromeafter hernia repair which include at least one of these aspects: numb-ness and/or groin discomfort and/or chronic pain.In terms of percentage, the incidence of Pain Complex Syndrome isassumed to be about 25% of patients undergoing inguinal hernia repair.Material and methods: Following the idea that Pain ComplexSyndrome could be caused by use of suture and fixation devices,after an observational study (186 patients consecutively enrolled fromSeptember 2004 and September 2006), we designed and played amulticenter, prospective, controlled, randomized, patient and evalua-tor blinded study: the TI.ME.LI (Tissucol for Mesh fixation inLichetenstein technique).The aim of this study is to evaluate pain and further disablingcomplications in patients undergoing Lichtenstein technique for pri-mary inguinal hernia repair by fixing the mesh with fibrin sealantversus sutures (control group).325 adult males requiring a unilateral tension-free hernioplasty wereincluded in the study and divided in two equal group from February2006 and March 2007.In the fibrin sealant group a small spot (1 ml) of Tissucol was appliedon the pubis under the mesh without spray then the remaining part(3 ml) over the mesh on the entire surface in a thin uniform layerby spray. In the control group, the mesh was fixed with Lichtensteintechnique.Results:A closed follow-up was planned (1 week, 1 month, 6 monthsand 1 year) and it finished in April 2008. At 1 year the percentageof patients with at least 1 disabling complication was significantlylower in the fibrin sealant group than in the sutures group.Compared with sutures, Fibrin sealant led to lower level of pain,numbness, and groin discomfort and to a lower use of analgesics.Fibrin sealant did not induce more recurrences than sutures in thispatient population and patients satisfaction was significantly higherwith FS than sutures.Conclusions: Fibrin sealant is safe and well tollerated by patients.It can be considered a good, if not the first, choice for the fixationof the mesh.
O-091Progrip inguinal hernia repair: a prospective study ofileoinguinal nerve perservation or neurectomyM.G. Muzi, C.I. Ciangola, F. Andreoli, C. Nigro, E. de Luca,G. TucciPoliclinico Tor vergata, Chirurgia Generale, Rome, Italy
Background: Lichtenstein technique has become the most frequentlyprocedure for inguinal hernia repair. Chronic pain is one of the mostsignificant complications. Causes of chronic pain related to hernior-rhaphy can be divided into neuropathic and non neuropathic. Theneuropathic causes include nerve entrapment by mesh, nerve entrap-ment by sutures or staples and neuroma formation. Peroperative iden-tification and subsequent division or preservation of the inguinalnerves during open hernia repair may influence the incidence ofchronic postoperative pain. The purpose of this report is to evaluatethe outcomes of neuralgia, paraesthesia and chronic pain followingroutine inguinal nerves excision compared to nerves preservationusing an innovative, partly resorbable polypropylene mesh with self-gripping properties the ProGrip™ Mesh.
Methods: Between October 2007 and December 2009, 258 patientsundergoing Progrip hernia repair were divided in two groups: groupA undergone nerves identification Group B undergone prophylacticileoinguinal neurectomy in case of “nerve at risk”. All operationswere performed by the same surgeon (MGM) under local anesthe-sia. The end points were the incidence of chronic groin pain at 6and 12 months, incidence of groin numbness, postoperative sensoryloss at the groin region, and quality of life.Results: In none of the two groups were registered cases of chronicpain; no significant intergroup differences were found regarding theincidence of groin numbness, postoperative sensory loss or changesat the groin region, and quality of life measurement at 1, 3, 6 and12 months after the operation.Conclusions: The study shows there is no differences between twogroups. It is important the identification of ilioinguinal nerve andsurgeon’s choice to remove it only in the cases of nerves at riskseems to be a good choice. Moreover the neurectomy does not affectnegatively the post operative outcomes.
O-092A randomised controlled trial of the effects oflightweight meshes in laparoscopic inguinal herniarepair on male fertility aspects up to 3 yearspostoperativelyE. Peeters, M. MiserezUZ Leuven, Leuven, Belgium
Background: Recently it was demonstrated that the use of light-weight meshes in laparoscopic inguinal hernia repair may signifi-cantly impair sperm motility 1 year after surgery. A longer follow-up up to three years postoperatively was undertaken to determinewhether these baleful effects of lightweight meshes on sperm motil-ity remain, decrease or increase further.Methods: 59 male patients with a primary, unilateral or bilateralinguinal hernia were randomised to laparoscopic inguinal herniarepair (TEP) using a standard polypropylene mesh (Marlex®) or alightweight mesh (VyproII®, TiMesh®). Male fertility aspects wereassessed preoperatively and 1 and 3 years after surgery, by means ofsemen analysis and scrotal ultrasonography.Results: Of the fifty patients that attended follow-up 1 year postoper-atively 13 patients were lost to follow-up at 3-year follow-up. Threeyears after surgery, sperm motility was slightly decreased in patientsoperated on with a VyproII® and TiMesh® mesh compared to theMarlex® group (-8.5% and -8% versus -2.8%; p = 0.87). Other semenparameters (sperm concentration, morphology, and α-glucosidase level)were comparable between the three groups. Furthermore, except for anon-significant decrease in sperm motility in the Marlex® group, semenanalysis results were unchanged at 3-year follow-up compared to 1 yearafter surgery. Finally, with regard to the results of the scrotal ultrasound,no significant differences could be noted between the heavyweightand lightweight groups and there was no significant improvementor worsening 3 years after surgery compared to one year postopera-tively.Conclusion: Our data suggest that the negative effects of the use oflightweight meshes in laparoscopic inguinal hernia repair on spermmotility do not increase further 3 years after surgery vs. 1 year aftersurgery. This result might be partially related to the lower samplesize.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S20

Hernia (2011) 15 (Suppl 2): S1-S35 S21
O-093The routine widespread use of bioprosthetic mesh is notnecessaryJ.M. Souza, G.A. DumanianDivision of Plastic and Reconstructive Surgery, NorthwesternUniversity, Feinberg School of Medicine, Chicago, Illinois, USA
Background: Mesh reinforcement of a midline ventral hernia repairhas been shown to minimize recurrence, but there is debate over whichmaterial offers the best combination of strength and complication pro-file. The Ventral Hernia Working Group (VHWG) recently proposeda grading system to assist surgeons in selecting the appropriate meshbased on an individual patient’s risk of developing a postoperativecomplication. Using this instrument, the VWHG suggests an advan-tage to the use of bioprosthetic mesh for all but low risk patients, andrecommends against the use of synthetic material due to concerns forincreased rates of infection, adhesions, and enterocutaneous fistulae.In this study, the VHWG grading scale was used to evaluate the inci-dence of these complications in 100 consecutive midline ventral her-nias repaired with uncoated mid-weight polypropylene mesh.Methods: A retrospective review was conducted of 100 consecutivecases of midline ventral hernia repair using an intra-abdominal under-lay of uncoated mid-weight polypropylene to reinforce a direct repairor components separation between July 2005 and May 2010. Therewere no “bridged” repairs. In all cases, the width of the mesh was8 cm for the length of the repair. The average duration of follow-upwas 26 months.Results: The mean BMI of the study population was 31.8 kg/m2,with an average hernia diameter of 9.6 cm. Graded according tothe VHWG scale, 51 percent of cases were considered Grade 2(“co-morbid”), with 25 percent considered Grade 3 (“potentiallycontaminated”). The remaining cases were Grade 1 (“low-risk”).Overall, there was a 7 percent rate of hernia recurrence. There wereno enterocutaneous fistulae or infections requiring mesh removal.Two patients were admitted for post-operative small bowel obstruc-tions. Both patients improved with conservative management and nei-ther patient required reoperation.Conclusion: The use of uncoated polypropylene mesh for reinforce-ment of midline ventral hernia repairs was not associated withincreased rates of infection, fistula formation, or clinically signifi-cant adhesions. These findings challenge the recommendation by theVHWG to avoid synthetic repair material in patients with co-mor-bidities or in “potentially contaminated” fields.
O-094Fixation free open ventral hernia repair using a newmesh with integrated placement strapsG. Amato1, G. Gulotta1, A. Agrusa1, G. Romano1, G. Salamone1,V.A. Saladino1, T. Goetze2, V. Paolucci31 University of Palermo, General Surgery, Urgency, and OrganTransplantation, Palermo, Italy; 2 Ketteler Krankenhaus, Dept. ofGeneral and Visceral Surgery, Offenbach, Germany; 3 KettelerKrankebhaus, Dept. of General and Visceral Surgery, Offenbach,Germany
Introduction: Mesh fixation and mesh overlap represent key issuesin ventral hernia repair. We have developed a modified technique forventral hernia repair using a new implant with integrated strapsdesigned to eliminate point fixation. Midterm follow-up in a cohortof patients indicates an overall reduction of complications as well asno recurrences.
Material and methods: A unique geometrically shaped light weight,large porous polypropylene mesh consisting of a large central bodyand eight radiating arms was used to repair ventral or incisional her-nia. The implant, previously tested in animal models, was placed in30 patients via open technique in sublay (preperitoneal or retromus-cular). A proprietary needle was tunneled laterally through the trans-verse and oblique muscles to capture the straps and retrieve them asa means of securing the mesh in place.Results: With this new method and prosthetic implant we achieveda simplified and faster surgical procedure. In all patients a defectoverlap of at least 30% was achieved. There were no intraoperativecomplications to report. In a midterm follow up from 30 to 36 months(mean 33 months) we recorded 3 seromas and 1 infection which weresuccessfully managed without mesh removal. Ultrasound follow-upshowed the mesh to be in place. No hematoma, chronic pain or recur-rence have been reported to date.Conclusions: The straps integrated to the prosthetic device allowedfor much smaller incisions and eliminated the complicated maneu-vers required for suturing the mesh in place, ensuring the mesh stayedcorrectly orientated. The inherent elongation of the straps absorbedforces placed on the implant during early recovery, thus helping toavoid mesh dislodgement before tissue ingrowth has occurred.Following advantages are clearly demonstrated: fixation free meshplacement, simplified procedure, broader coverage of the abdominalwall, shortening of the operative time and decreased intra- and post-operative complications.
O-095The dynamic parietal closure: Initial experience of anoriginal parietal closure procedure for treatment ofabdominal wound dehiscenceF. Browet1, Q. Qassemyar2, M. Robbe2, P. Verhaeghe1,J.M. Regimbeau11 Department of Digestive and Metabolique surgery, North Hospital,University of Picardy Medical Centre, Amiens France; 2 Departmentof plastic, reconstructive and aesthetic surgery, North Hospital,University of Picardy Medical Centre, Amiens, France
Background: After midline laparotomy, wound abdominal dehis-cence (WAD) is a common (0.2 to 10%) and strong (mortality: 44%,morbidity: 67%) complication. Actually, there is no clever solutionto prevent and treat WAD. Then, we developed an original proce-dure: the “dynamic parietal closure” (DPC).
Fig. 1: The mesh with integrated straps placed in sublay.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S21

S22 Hernia (2011) 15 (Suppl 2): S1-S35
Methods: DPC is a strengthening (with vascular loops) of the clas-sical aponeurotic closure. It is simple, fast and inexpensive and fea-sible whatever the need of stoma(s) or peritoneal drains. This tech-nique possesses the advantages without the pitfalls of retentionsutures techniques and parietal plasty.Along the entire length of the median laparotomy a successive massclosure was realized with silicone loops (vascular loop) placedtransfascially across the wound to obtain a suture like a U. Weadjusted the tension. It repulsed the digestive tract and closes theaponeurotic edges for a tension free classical continuous suture.The system was removed 21 days later by surgeon in consultationroom.Results: Prospectively, from January 2009 to December 2010, six-teen patients developed a WAD (2.06%) after midline laparotomyand were treated with DPC. The data from 16 patients were ana-lyzed prospectively. The WAD recurrence rate was 0%. Medianoperative time was 60 min [40-300]. The median morbidity score(Clavien’s classification) was 1.5 [0-IVa] (no IIIb and IVb, incisionalhernia: 25%). The median hospital stay was 18 days [6-54]. Themedian follow-up was 154 days [17-377]. Material cost: less than17 € per patient.Conclusions: DPC is an original, easy, cheap, efficient and promis-ing procedure but should be evaluated with a larger number.
O096Reconstruction of the front abdominal wall in herniacases following TRAM procedureM. Smietánski1, J. Wałecka1, W.J. Pokora2, J. Kitowski11 District Hospital Puck, Department of Surgery and Hernia Center,Puck, Poland; 2 Medical University of Gdansk, Department of Plasticand Reconstructive Surgery, Gdansk, Poland
Introduction: Both ventral hernia and the epigastric bulge are themost troublesome post-operational complications in patients afterTRAM flap breast reconstruction. The two pathologies of the frontabdominal wall following the procedure are caused by the absenceof the rectal-abdominal muscle. Authors examined patients afterTRAM procedure to point out the possibilities of the repair in dif-ferent cases and stages of the defect.Methods: Between 123 patients undergoing TRAM procedure 11were identified as postoperative hernia cases. All the patients werereoperated. Anatomical measurements were done. Possibilities ofreconstruction were described according to localization and width ofthe defect. In one year follow up recurrence were examined as a pri-mary end-point.Results: Two different localization of hernia/bulge was observed.Upper abdomen hernias were identified as a defect with a need forseparate incision repair. Lower abdomen hernias can easily be per-form via previous incision (not to influence the cosmetically effectof previous operation). All meshes were implanted in sub-lay posi-tion with a margin of min. 5 cm both sides. Defects brighter than5-6 cm need component separation technique on the involved side.In our series 3 cases of laparoscopic repair was observed. In all 3the repair was not sufficient according to persistent bulge and weak-ness of the abdominal wall.Conclusion: Bulge and hernia following TRAM procedure shouldbe operated with the open mesh technique (sub-lay). Extendeddefects need large muscle flap reposition before mesh implantation.Laparoscopic IPOM technique is not sufficient to obtain a goodcosmetically result. Patients in the follow-up period did not demon-strate recurrence and were satisfied with the aesthetic results of theoperation.
O-097Fascia closure during the acute phase of open abdomentreatmentU. PeterssonDepartment of Surgery, Malmö and Lund University, Malmö/Lund,Sweden
Background: This presentation will be part of a symposium onreconstruction of the abdominal wall after open abdomen treatmentand will focus on fascia closure during the acute phase. Loweringan increased intra-abdominal pressure is without doubt advantageousand sometimes life-saving. If non-surgical measures are insufficient,decompressive laparotomy and open abdomen treatment is indicatedin patients with abdominal compartment syndrome. In damagecontrol situations for trauma or in septic conditions, or when a sec-ond-look operation is planned, or as a prophylactic means for pre-vention of post-operative intra-abdominal hypertension, shorter orlonger periods of open abdomen treatment are also motivated.Many difficulties associated with an open abdomen have to be over-come in order to ensure a safe and positive out-come for these patients.The temporary abdomen closure (TAC) technique used during the openabdomen period should be safe in terms of complications and providehigh fascia closure rates. There are numerous retrospective reportsfrom series of various sizes presenting results for different TAC tech-niques. The number of prospective studies is increasing, providing abroader scientific base for open abdomen treatment.Results from prospective studies: Mortality ranges from 0-43%,fascia closure from 25-85% and fistula formation from 0-21%. Thismost certainly reflects patient heterogeneity but probably also differ-ent possibilities with the various TAC techniques used. The favouredTAC technique in many of the prospective studies includes the useof negative pressure, alone or combined with fascial traction. Fascia
Prospective studies including ≥≥ 20 patients treatedwith one specified TAC technique
Author Year n Dominating TAC Age Mort FC Fistulaetiology % % %
Aprahamian 1990 20 Tr AB 30 20 75 –
Wittman 1990 100 P FT – 24 80 –
Sugrue 1998 49 ACS Mesh 57 43 55 6
Miller 2004 53 Tr VAFC 36 15 72 2
Perez 2007 37 P+ACS V.A.C.® 58 38 70 3
Bee* 2008 51 Tr V.A.C. (31)/ 44/37 25/26 29/25 21/25Mesh (20) ns
Teixeira 2008 93 Tr V.A.C.® 33 14 85 15
Tieu 2008 29 Tr AB 45 24 72 0
Amin 2009 20 P V.A.C.® 59 0 75 10
Subramonia 2009 51 WD V.A.C.® 60 23 61 4
Shaik 2009 42 P V.A.C.® 68 9 52 5
Cheatham 2010 478 Tr VAFC 43 39 72 5
Pliakos* 2010 40 P RSSFC+V.A.C.® (21)/ 75/58 22/19 71/53 –V.A.C.® (19)
Acosta 2011 111 P+V VAWCM 68 30 84 7
* = randomized study. Tr = trauma. P = peritonitis. ACS = abdominal compartment syndrome. WD = wound dehiscence. V = vascular. TAC = temporary abdominal closuretechnique. AB = artificial burr. FT = fascial traction. VAFC = vacuum assisted fascial closure. V.A.C.® = vacuum assisted closure with abdominal dressing system from KCI.RSSFC = retention sutured sequential fascial closure. VAWCM = vacuum assisted woundclosure and mesh-mediated fascial traction with abdominal dressing system from KCI.FC = successful delayed primary fascial closure with the technique ± mesh or biologicmaterial on intention-to-treat basis. – = information not available.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S22

Hernia (2011) 15 (Suppl 2): S1-S35 S23
closure rates appear to be among the highest also when applied innon-trauma patients without an increase in fistula rates.Conclusion: Open abdomen treatment should be utilized with theprimary aim of controlling damage and saving lives in severely illor injured patients. What TAC technique to use in each individualpatient may vary according to the circumstances. The preference fornegative pressure therapy alone or combined with fascial tractionseems safe and provides high fascia closure rates, minimizing thenumber of patients debilitated by large planned hernias.
O-098Management of incisional hernia following openabdomen treatmentA. MontgomeryDepartment of Surgery, Skåne University Hospital, Lund University,Sweden
Background: Fascia closure in the acute phase after open abdomentreatment is not possible in all patients and the end result is in somepatients is a huge secondary hernia where also skin grafting isrequired in order to cover the intestines. There has been an increasein fascia closure using the temporary abdomen closure (TAC) tech-nique and it is now reported to be between 25-85%. This will ofcourse potentially reduce the postoperative convalescence phase sub-stantially. The frequency of a later development of and incisionalhernia that needs to be dealt with later is not known. It is probablyhigh due to the compromised healing conditions in these severely illpatients. Of course the magnitude of a later incisional hernia is prob-ably reduced since the adoption of the rectal muscles has beenachieved at closure of the open abdomen.Methods for closure and preventing hernias: The method of mesh-mediated facial traction in combination with vacuum assisted closurehas been described by Petersson et al 2007. This technique is basedon the use of a temporary mesh for stepwise traction and has resultedin a high closure rate of 84% reported in 111 patients by Acosta etal in 2011. In order to prevent a later incisional hernia a new tech-nique using a permanent retro muscular polypropylene mesh for trac-tion is proposed also bridging a gap that could not be closed. Conclusion: Vacuum assisted closure together with temporary mesh-mediated facial traction results in a high primary closure rate in theopen abdomen treatment. A further development of this techniqueusing a permanent mesh might be an option to prevent the develop-ment of a later secondary hernia.
O-106 - VIDEOLaparoscopic repair for voluminous hiatal hernia in anold female patientE. Cocozza, L. Livraghi, M. Berselli, L. Latham, V. Bianchi,L. Farassino, E. GuffantiAzienda Ospedaliera Ospedale di Circolo e Fondazione Macchi,Surgery, Varese, Italy
Background: Repairing of voluminous hiatal hernias in elderlypatients is still a controversial surgical topic. If patients begin sinpto-matic surgical approach can be considered to correct anatomical alter-ation and to relief the patients from the symptoms.
Methods: An eighty years old female patient was admitted to ourhospital for vomiting and dyspepsia. An upper digestive X-rayexamination with the contrast and a thorax and abdomen CT scanwere performed. The exames showed a voluminous hiatal herniawith dislocation of the stomach and of the omentum in mediastinum.A conservative treatment was started because the important co-mor-bility of patient (diabetes mellitus, hypertension and heart disease)and no presence of important complications related to hiatal hernia.In the following months however symptoms persisted and abingestis pneumonia occurred. Patient was readmitted in our Unitof Surgery: laparoscopic hernia reduction, repair with placementof absorbible prothesis and Nissen fundoplicatio were performed. Results: Post-operative days were clinically silent. In second post-operative day a X-ray with Gastrographin was performed, thatshowed a regular canalizzation without stenosis or extraluminal leaks;after a regular beginning of progressive oral intake the patient hasbeen discharged in eighth post-operative day in good clinical condi-tions. Three months later the patient is still asimptomatic and in goodhealth. Conclusion: This video shows as voluminous simptomatic hiatal her-nia in an old patient can be successfully treated with a low surgicalimpact in an experienced laparoscopic surgicalcentre. Minimally invasive approach can reduce the perioperative trauma andhas to be considered to minimalize the surgical impact in old patientswith important comorbility and benign patology.
O-107 - VIDEOTransfasial sutures are needed in laparoscopic lumbarhernia repair?J.B. Luque1, J.G. Jurado1, J. Suarez Grau1, J. Gomez Menchero2,I. Durán Ferreras1, J. García1, A. Bellido Luque3, D. Tovar11 Riotinto Hospital, General and Digestive surgery departament,Minas De Riotinto, Riotinto, Spain; 2 Spain; 3 USP clinica SagradoCorazón, Sevilla, Spain
We present a 67 years old patient who went to our hospital suffer-ing recurrent lateral pain with mass associated. This patient under-went a right nefrectomy 10 years ago, due to traffic accident. Afterexplorations, a large lumbar incisional hernia is diagnosed, andlaparospic approach was indicated one 10 mm trocar in umbilicalposition and two 5 mm trocar were used to perform the surgery.Hepatic flexure is included in the defect, so the first step is removethis structure.The second step is clear the lateral edge of the defect trying toimprove the mesh fixation on the lateral wall. Is necessary to iden-tifie the iliac crest and the last right ribs, because of the fixation.When the mesh is placed in the right position, the craneal edgeis fixed on the last ribs, and the caudal is fixed on the iliaccrest, using helicoidal sutures in doble crown technique. The laststep is to cover the tacker with autologus fibrin trying to diminishas much as possible the posibility of adhesion formation to the tackers. The patients was discharged in the first postoperative day, andno complications have been seen, only a postoperative seroma.this seroma was absorbed in the first postoperative month. Withthis video, we try to say that transfascial sutures are not neccesaryin laparoscopic lumbar hernias repair, avoiding the complicationcaused by using it, like chronic pain with no high recurrencerate.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S23

S24 Hernia (2011) 15 (Suppl 2): S1-S35
O-108 - VIDEOProceed ventral partch in the prevention of trocarhernia site in bariatric surgeryS. Morales-Conde, I. Serrano, M. Socas, A. Barranco, J. Cañete,J.A. Navas, M.D. Casado, J.M. Cadet, F.J. PadilloUniversitary Hospital Virgen del Rocio, General and DigestiveSurgery. Innovation and minimal invasive surgery., Seville, Spain
Background: There is a risk of developing a trocar site hernia (TSH)after laparoscopic surgery, but data are sparse and based mostly onretrospective studies with a short and poorly defined follow-upperiod. Surgical approaches and patient-related co-morbidity, as obe-sity, have also been suggested as risk factors for development ofTSH. TSH appears most often (96%) in trocar sites of 10 mm, locatedmostly in the umbilicus region (82%) and in places where the inci-sion is extended for the removal of surgical specimen. Aims: The aim of this paper/report is to show a new method of clo-sure, (based on our experience), to prevent developing of a trocarsite hernia in morbid obesity patients in those trocars with higherrisk of developing a TSH (the 12 mm trocar at the left flank aftergastric by-pass and the 12 mm trocar at the left hypocomdrium aftera sleeve gastrectomy through where we remove the surgical speci-men) by placing a preformed plug (proceed ventral patch). Method: We place a single stitch knoted at both flaps of the mesh.Then we introduce the mesh rolled up into the abdominal cavity,using an endoclinch, through the 12 mm after removing the valve.Once the mesh is inside, we remove the trocar and the mesh isexpanded under direct vision, covering the entire hole. Afterwards,we attach the previous stitch to the subcutaneous cellular tissue. Results: According to our experience we have had no cases of tro-car hernia site at these 12 mm trocar closed by the plug, neither atthe others, which we did not close.
O-109 - VIDEOPreliminary experience of a new technique inlaparoscopic ventral hernia repair: mesh fixation withfibrin sealant (tissucol®)A. Noceti, E.L. Ratto, O. Perata, A. PiccardoCairo Montenotte-Savona Hospital, General Surgery, CairoMontenotte-Savona, Italy
Background: We present a preliminary experience of a new tech-nique of mesh fixation with fibrin sealant in laparoscopic ventral her-nia repair. Performed after the good results of experimental studiesin ventral hernia repair and of case studies of inguinal hernioplasty(IPOM) with fibrin glue. Methods: The basic steps of the surgical technique are: pneumoperi-toneum induction with Verres in left upper quadrant; disposition of10 mm optical trocar and two 5 mm trocars in the left anterior axil-lary line; 5 mm 30 degree optic for mesh introduction viewing; adhe-siolisis (cold blade near bowel); transparietal placement markers tosign an overlap > 4 cm; measurement of “teilored mesh”; just useddiluited fibrin sealant (tissucol®) whit spray set for mesh fixation;just used Parietex™ Composite (PCO) mesh, circular model, with aresorbable collagen barrier on one side to limit visceral attachments.No Pro Tack and no transfascial sutures. Ten minutes without pneu-moperitoneum are required to control the perfect adhesion of themesh. If this does not occur we use pro tack. Patients with herniasize > 2 cm are excluded from this technique. Results: We performed 11 operations: middle hernia size 1,8 cm(1,5- 2 cm), 4 female and 7 male, average age of 60,5 years old(40 and 89). 2 incisional hernias, 5 umbilical, 4 epigastric. Averageoperative time: 30 minutes (20-40 min). No postoperative complica-
tions. Reduction in postoperative analgesic assumption of 90%.Average hospital stay 30 hours. Relapse rate (F.U. < 24 months):0%. Conclusions: No Pro Tack, no pain. We consider this technique veryinteresting, effective and safe and a very important step towards themicro invasiveness with great advantage for the patients. More caseswith longer follow-up will be useful to expand indications for thistechnique.
O-110 - VIDEONew personal technique in microlaparoscopic ventralhernias repair: Two-trocar and biological glue A. Noceti, E.L. Ratto, O. Perata, A. PiccardoCairo Montenotte-Savona Hospital, General Surgery, CairoMontenotte-Savona, Italy
Background: Eighteen years after the first series of 5 laparoscopicincisional hernias repair, this technique is standardized. We want tointroduce a new microinvasive technique: “two-trocar technique withthe use of biological glue”, to further reduce the traumatism. The aimof the study is to further reduce the invasiveness through the reductionin number and size of the trocar and the reduction of traumatic fixa-tion with the use of biological glue and no use of transfascial sutures. Methods: The basic steps of the surgical technique are: pneumoperi-toneum induction with Verres in left upper quadrant; disposition of 2trocars, one 10 mm optic for mesh introduction and one 5 mm in theleft anterior axillary line; 5 mm 30 degree optic; transparietal place-ment markers to sign an overlap > 4 cm; measurement of “teiloredmesh”; mixed fixing reducing traumatism (biological glue and half ofthe usual of titanium or resorbable spirals). Preoperative assessmentof patient using US and eventually CT of abdominal wall. Patientswith significant peritoneal adhesions are excluded from this technique. Results: 51 operations have been performed from 2007 to 2011: middle lesion size 4 cm (2-6 cm), 12 pt. (34,2%) with BMI>30,24 female and 27 male, middle age of 60,5 years old (35 and 89).25 incisional hernias (8 recurrent and 4 complex defect treated withdouble mesh), 16 umbilical, 9 epigastric and 1 Spigelian. Middleoperative time: 45 minutes (25-85 min). No postoperative complica-tions. Reduction in postoperative analgesic assumption of 57%.Middle hospital stay 30 hours. Relapse rate (F.U. > 24 months): 0%. Conclusions: Less Pro Tack, less port. This means less pain and lesscomplication without affecting the results. We consider this techniqueeffective and safe and another step towards the micro invasiveness,with great advantage for the patients.
O-111 - VIDEOGiant incisional hernias – Combining laparoscopicassisted components separation technique and sublaymesh implantationO. Doebler, B. StechemesserVivantes Auguste Viktoria Clinic, Berlin, Germany
Introduction: Giant incisional hernias are a challenge for the surgeon.It is often necessary to reconstruct the abdominal wall combiningautologous and non-autologous techniques. Prosthetic mesh implanta-tion can reduce the postoperative hernia recurrence by up to 10%.Implanting prosthetic mesh in sublay technique has shown advantagesover onlay or ipom implantation. In case of giant incisonal hernias itis necessary to tighten the fascia edges to stabilize the abdominal wall.With components separation technique it is possible to approximatethe rectus fascia to the midline up to 10 cm. To reduce the mobiliza-tion trauma for the abdominal wall which endangers the skin and
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S24

Hernia (2011) 15 (Suppl 2): S1-S35 S25
subcutaneous blood supply components separation technique can beperformed with laparoscopic assistance.Methods: In this study we reconstructed giant incisional herniascombining laparascopic assisted components separation techniqueand mesh-implantation in sublay technique. Patient demographics,secondary diagnosis and preoperative risk factors, postoperative complications and clinical outcome were reviewed. Results: 14 Patients with giant midline incisional hernias were recon-structed with laparoscopic assisted components separation techniqueand sublay mesh implantation. All defects were larger than 10 cm(EHS – classification W3). The median BMI was 33.3. The meanOperation time was 194 min. Bioprosthetic meshes were implantedin 50% of the patients. In the other half of the patients conventionalmonocryl-prolene – composite mesh was used. 6 of 7 patients withbioprosthetic meshes showed a postoperative seroma whereas one ofthe conventional group develop a postoperative seroma too. None ofthe patients required a graft removal because of wound infection.The follow up of six months showed no lack of stability or relapsehernia.Conclusion: Reconstruction of giant incisional hernias often needs acombination between autologous and non-autologues techniques.Linking up component separation technique and prosthetic meshimplantation in sublay technique is a promising combination to recon-struct and stabilize the abdominal wall. Performing a laparoscopicassisted components separation reduces the mobilization trauma of theabdominal wall evidently and shows advantages in postoperativepatients outcome. Short time follow up showed good results. Howeverlong time studies are necessary to prove relapse prophylaxis.
O-112 - VIDEOSurgical treatment of a meshoma producing a nonneuropatic postoperative painM.A. García-Ureña, J. López-Monclús, D. Melero, P. López Quindós,A. Pueyo, N. Palencia, R. Barriga, A. RobinHenares Hospital, Surgery, Madrid, Spain
One of the sources of postoperative hernia pain is non-neuropathic.This pain can be caused by mechanical pressure of a folded o waddedmesh. We present in this video the surgical treatment to solve a caseof postoperative non-neuropatic pain. This is a 69 years with a previous history of umbilical hernia. In 2006,she was operated for a Spiegel hernia with mesh placement. One yearlater was reoperated urgently for an incarcerated recurrent hernia in theleft quadrant with primary repair. The patient was referred to our clinicfor constant invalidating pain with important impairment in her qualityof life. On exploration, pain was denoted on palpating a specific areaunder the previous incision. A CT was obtained and showed an imageof a mass between external and internal oblique muscles. The patientaccepted surgical re-exploration. Under spinal anesthesia an incision wasmade on the previous scar. A lot of scar tissue was found and a com-plete dissection of the different planes was achieved but no sign ofchronic infection was seen. Finally a meshoma was found and was completely resected. There was no bacterial growth in the specimen. The patient was discharged on the following day of the procedure.There was no complication. After one year of follow-up, the patient´spain has diminished but not completely disappeared. She reportsa satisfactory quality of life and is pleased with the procedure. Acontrol CT on 12th month showed a return to normal postoperativefindings. Postoperative hernia pain is a disabling condition that needs to beconsidered. A CT should be performed in patients suffering invali-dating pain to differentiate the source of this pain. Surgical reoper-ation is a useful option that must be offered to this patient in clin-ics dedicated to abdominal wall.
O-114Tailoring the midline and subxiphoidal incisionalhernia repairJ. ConzeRhenish Westfalian Technical University, RWTH Aachen, SurgicalDepartment, Aachen, Germany
For a standard procedure you need a standard hernia. Are all herniasthe same? So far we do not really differentiate, not in location of thehernia, not in size of hernia, not even in the condition of the patient,and not in the different surgical techniques. The reimbursement sys-tem doesn`t differentiate either, the DRG for small hernias is thealmost the same as for large hernias, making the repair of the real bigones economically loss-making and therefore totally unattractive. The retromuscular mesh augmentation seems to be an ideal procedureto reconstruct the anatomy and physiology of the abdominal wall. Thistechnique facilitates a readaption of the rectus muscles that cover themesh prosthesis and reduces the risk of mesh infection by closure ofthe anterior fascia in front of the mesh. It keeps the prosthesis out ofthe intraabdominal position, preventing possible mesh induced com-plications, such adhesions and fistula formation.But hernias are not all the same, some are located close to thexiphoid, some have a large transverse diameter by lateral retractionoften associated with a loss of domain. There is a risk of an abdom-inal compartment syndrome or respiratory constraint depending onthe patient condition. In these cases, where a closure of the anteriorrectus sheath cannot be obtained, you need a plan B... sometimeseven a plan C or D. We have developed an algorithm, tailoring the procedure to thepatient’s condition and anatomical findings. This algorithm regardsthe considerations and advantages of the open retromuscular meshaugmentation, to achieve a ventral fascia reconstruction and preven-tion of mesh contact to the intestine and the subcutaneous tissue asmuch as possible. Only at the end of the algorithm we perform anopen IPOM – bridging technique ensuring a broad subduction tofacilitate a sufficient contact area between the intraabdominal meshand host tissue. We need standardisation but tailored to the patientsanatomy and condition.
O-116Tailoring of open suprapublic incisional hernia repairP. Verhaeghe1, Ch. Sabbagh1, J.B. Deguines1, E. Mensah2,J.M. Régimbeau11 Department of digestive and metabolic surgery, CHU Amiens,Amiens, France; 2 Department general surgery, University ofParakou, République du Bénin
Incisional hernia repair has been greatly modificated by the Stoppa& Rives works during the 20° Century. The aim is a reinsertion ofthe rectus magnus muscle by insertion of an inert prosthesis behindthe muscles and in front of the peritoneum. This prosthesis must notto be in contact with the bowel (avoid migration risk). A width of 4to 6 cm (Stoppa), 5 cm (Schumpelick) out of the internal border ofthe muscle is needed to get a strong enough repair.Supra pubic incisional hernia belongs to the group of boundaries her-nias: they get this name for they get on one side a solid limit withimpossibility to fix the prosthesis at the good distance.Suprapubic hernia must be diffentiated from umbilical incisional her-nia with incision getting infra umbilical which don’t reach pubis areeasier to repair. A good preoperative analysis of parietal wall defect
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S25

S26 Hernia (2011) 15 (Suppl 2): S1-S35
is obtained by CT scan (or RMI); the defect mechanism can be dif-ferent between median incision, horizontal rectus magnus desinser-tion (Gynecologist Mouchel incision), worth when anteriorly wereperformed both incision with a real lost of tissue. Larger supra pubichernia can put in communication median supra pubic hernia andinternal inguinal hole.The intervention begins by a scar excision, often wide and ugly, fora better cosmetic result. Second step is opening to look for internalborder of rectus magnus and separate rectus magnus from peritoneumtaking car that under linea alba there is a thin sheet to protect epi-gastric vessels and no thick aponeurosis. If the rectus magnus is ofgood quality, dissection is stopped on Spigel line and if there is muscular lost, the linea alba is crossed and dissection prolongedbetween lateral muscles. Infra pubic dissection is performed inRetzius space (same space used by Stoppa for GPRVS). This can bevery difficult, either impossible, if anteriorly cystotomy was per-formed for prostate surgery or multiple pelvis broken with very thickfibrosis. A pre-existent laparoscopic inguinal repair (TAPP or TEP)make the dissection more difficult (adhesion to epigastric vessels)but can be done if the prosthesis is left fixed on the peritoneum.Mensuration of the prosthesis cut in a large sheet of mersilen(prolen?). Prosthesis is fixed by transmuscular shrouds with shortskin incisions on both sides. Non absorbable separate knot fixed theprosthesis at the posterior side (Cooper ligament) of the ilio pubicbranch leaving a large surface of prosthesis free under the fixation.Drain is not systematics. The patient wears an abdominal belt dur-ing one month after repair. This open technique gets two advantageson laparoscopic one: cosmetic one by scar excision and avoidingmedian bubble and more important avoid direct contact betweenbowel and prosthesis.
O-117Tailoring suprapubic hernia repair – The laparoscopicapproachA.M. CarbonellThe Hernia Center of the Greenville Hospital System UniversityMedical Center Greenville, South Carolina, USA
Suprapubic incisional hernias are located in close proximity to thepubic bone and arise from urologic, gynecologic, or orthopedic pro-cedures. The repair of these hernias is difficult due to the complex-ity of dissection and their anatomic proximity to the bladder, bony,vascular and nerve structures. In select patients, these hernias can be repaired laparoscopically withthe benefit of decreased wound complications and less pain.Suprapubic hernias better approached open, on the other hand, arethose with thin-wide scars, associated pressure ulceration of the skin,and massive rectus diastasis.There are three critical steps in the laparoscopic repair of suprapu-bic hernias. First, the prevesical space is entered, exposing thepubic bone, Cooper’s ligaments, and the inferior epigastric vesselsbilaterally. Second, an appropriate size mesh is introduced andaffixed to the abdominal wall with sutures and tacks. Third, sincetheir is very little fascia above the pubic bone available for meshfixation, laparoscopy requires durable, permanent fixation ofthe mesh to the pubic bone utilizing bone-anchored sutures andtacks.With proper patient selection, a clear understanding of the pelvicanatomy and experience with permanent fixation to bone, the laparo-scopic repair of suprapubic incisional hernias is a viable alternativeto the traditional open approach.
O-118Tailoring the repair of lateral incisional herniasF. MuysomsAZ Maria Middelares, Ghent, Belgium
Lateral incisional hernias are less frequent than midline incisionalhernias. For the midline incisional hernias standardized techniqueshave been described using either open or laparoscopic approaches.For the lateral hernias much less literature and evidence is available.According to the EHS-consensus classification for incisional hernias,the lateral hernias are defined as: subcostal hernias, flank hernias,iliac hernias and lumbar hernias [1]. Care should be taken when read-ing the available literature because flank hernias and lumbar herniashave been used as synonyms [2, 3]. When deciding in a particular patient whether to use an openapproach or a laparoscopic approach, we cannot rely on evidencedliterature, therefore we will decide using our personal experience asa guide. I have found a preoperative CT scan very helpful in guid-ing this decision. It allows us to estimate the size of the hernia defect,the distance of the defect to the bony borders of the abdominalwall and the size of the hernia sac. Moreover we can evaluate thecontent of the hernia sac. When choosing for a laparoscopic approach we must be sure that anadequate overlap of the mesh over the hernia defect can be achieved.For hernias close to the bony borders of the abdomen, fixation ofthe mesh to the bony structures must be achieved in order to avoidrecurrences between the mesh and the bony borders [3]. When performing open repair for lateral hernias specific knowledgeof the anatomy of the abdominal wall muscles lateral to the rectussheath is necessary if we want to perform a retromuscular or sublaymesh repair. Therefore we can recommend the cadaver study per-formed by Stumpf et al. from Aachen [2]. For lateral flank and lumbar incisional hernia repair the planebetween the musculus obliquus externus and internus is the mostsuitable, because of the presence of neurovascular structures in theplane between the transversus abdominis and the obliquus internusmuscles on the lateral side. For iliac lateral incisional hernias the mesh will be positioned cra-nially in between muscle layers and below the linea arcuata in thepreperitoneal plane. A good overlap underneath the iliopubic tractcan be achieved by blunt dissection.For subcostal hernias cranially the mesh will be positioned either ontop or below the ribs and the costal margin, to achieve adequate over-lap. If positioning underneath the costal margin is needed the attach-ment of the musculus obliquus internus to the costal margin has tobe sectioned. In alignment with the trend to use large pore, lightweight meshes inmidline sublay repair, we can choose the same for lateral herniarepair. In large lateral hernias I nevertheless prefer a heavyweightsmall pore mesh. Another question is if the mesh should be fixedwith sutures, which I have used up till now. Alternatively no fixa-tion or fixation with glue could be an option. I think that the new self-fixating meshes, will be my personal choicefor these indications, when meshes of appropriate sizes will becomeavailable. References:1. Classification of primary and incisional abdominal wall hernias.F. Muysoms et al. Hernia (2009) 13: 407-414
2. The lateral incisional hernia: anatomical considerations for astandardized retromuscular sublay repair. M. Stumpf, J. Conze,A. Pescher, K. Junge, C. Krones, U. Klinge, V. Schumpelick.Hernia (2009) 13: 293-297
3. Laparoscopic transperitoneal repair of flank hernias: a retrospec-tive review of 27 patients. C. Edwards, T. Geiger, K. Bartow,A. Ramaswamy, N. Fearing, K. Thaler, B. Ramshaw. Surg Endosc(2009) 23: 2692-2696
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S26

Hernia (2011) 15 (Suppl 2): S1-S35 S27
O-120Lysostaphin treated porcine mesh dramaticallyimproves animal survival and increases tissueintegration in the presence of high bacterial inoculumI. Belyansky1, T.R. Martin1, V.B. Tsirline1, J. Shipp1, A.E. Lincourt1,A. Vertegel2, B.T. Heniford11 Carolinas Medical Center, Carolinas Laparoscopic and AdvancedSurgery Program, Charlotte, United States of America; 2 ClemsonUniversity, Bioengineering, Clemson, South Carolina, United Statesof America
Background: Lysostaphin (LS), a naturally occurring anti-Staphylococcal endopeptidase, has the ability to penetrate biofilmand aggressively kill Staph aureus, even MRSA. In this study weexamined the tensile strength of LS bound porcine mesh-fascial inter-face and its histological appearance in infected field. Methods: On-lay PMs were implanted in select groups of rats. GroupA (n=10) had LS-PM with no bacteria. Group B (n=15) had PM and10^6 S. aureus without LS. Group C (n=15) had PM, 10^8 S. aureusand no LS. Group D and Group E (n=10/each group) had LS-PMinoculated with 10^6 and 10^8 CFU S. aureus respectively. Meshwas explanted at 60 days, tested for tensile strength, bacterial cul-ture, and histologically scored (scale 1-5) by blinded evaluators. Results: Groups B and C had 93% mortality due to infection. Othergroups had sterile cultures at 60 days, normal appearing mesh,and no mortality. Mean pull-off strength in Group A was 5.0 N,Group D – 4.9 N, and Group E – 6.7 N (p=0.01 vs. Group A). Tissueingrowth and fibroblast content scores were 2.10 and 2.38 respec-tively in controls (Group A), while Group D was 1.67 (p=0.007) and1.93 (p=0.11) and Group E was 2.75 (p=0.014) and 3.1 (p=0.008)compared to controls. Conclusion: Inoculated rats without LS had 93% mortality due toinfection. In contrast, LS-bound PM withstood S. aureus inoculation(10^6 and 10^8), resulting in 100% survival and sterile cultures aftermesh implantation. Histologic evaluation showed complete resolu-tion of infection in inoculated, LS treated groups. Of note, the high-est inoculum group (10^8) showed higher tensile strength, greatertissue ingrowth, and fibroblast content. This difference may be dueto an amplified immune response without infection, causingimproved mesh-tissue integration. Lysostaphin holds real promise inpreventing Staph related surgical infections.
O-121The MR-visible-Mesh as IPOM in rabbits: First in-vivoimaging of mesh ingrowth and delineation to itssurrounding structuresJ. Otto1, N. Kühnert1, N. Krämer1, H. Donker1, C. Kuhl1, I. Slabu2,M. Baumann2, U. Klinge11 University clinic rwth, Surgery, Aachen, Germany; 2 Rwth Aachen,Applied Medical Engineering, Aachen, Germany
Introduction: Implantation of textile meshes can cause severe complications like migration, erossion, shrinkage, deformation and fis-tula formation. In some of these cases the indication for surgical correc-tion is beyond despute, but often ‘only” funtional problems or unspecificdiscomfort is presented. In these cases the required procedere is not clear. Until now the conventional diagnostic was limited because X-ray,ultrasound, CT and MRI usually failed to visualize the implabtedmesh. Only in exceptional cases, if the mesh is surrounded by flu-ids or fat, the structure of the mesh can be delineated. After we could establish a possibility to produce and to visualize aMR-visible mesh with common MRI sequences, we could now pres-ent the first trial of imaging the mesh ingrowth and its delineationto surrounding structures.
Project and first Results: Therefore we implanted the MR visibleMesh (7x4 cm) in IPOM-position in 10 rabbits laparoscopically. Allmeshes were explanted after 12 weeks. MR investigations were done1 day, 4 weeks and 12 weeks after operation. The histological analy-sis and the macroscopic results of adhesion and deformation werecompared to the findings of MR investigations, which were donethree times during the whole period of examination. Conclusion: In the underlaying study in living animals we couldevaluate mesh ingrowth in terms of position, deformation and delin-eation to its surrounding structures with non-invasive MRI imagingin individual objects for the first time. The use of such a visible mesh wil be helpful for decision-makingwhether a revison operation of the mesh is necessary (explantation,refixation, implantation of a bigger mesh [3DOTS]) or not (in caseof not mesh-related current complaints). Furthermore the visiblemesh then could be useful to plan a revision. Acknowledgement: This work is supported by the German FederalMininstry of Education and Research (BMBF 01EZ 0849).
O-122Deformation behavior of lightweight surgical meshes inexperimental hernia repairM.V. Anurov1, S. Titkova2, A. Oettinger21 Russian State Medical University, Experimental Surgery, Moscow,Russian Federation; 2 Russian Federation
Background: Growth of recurrence rate after hernia repair with useof light meshes is recently noted. In most cases light elastic meshesare implanted haphazard without consideration of their anisotropicproperties and directions of physiological loads. We suppose that bio-mechanical discordance results in mesh deformation, which can leadto onset of margin hernia. This study aims to investigate deformations of light meshes with dif-ferent anisotropic properties in relation to theirs orientation inabdominal wall repair. Methods: Two lightweight large-porous surgical meshes ParieteneLight (PL) and Dyna Light (DL) underwent uniaxial tension andloop bending testing in longitudinal and transverse axes. In 24 rats(4 groups) middle hernia defect 28x18 mm was created and thenrepaired by sublay technique using either mesh, 40x30 mm in size.Each mesh was oriented in two perpendicular axes. In 6 monthsdeformations of meshes and related complications were investigated. Results: PL demonstrated weak anisotropy in tension and greatreduction of bending stiffness and springiness in longitudinal axis.DL exhibited 8-fold differences between perpendicular axes only intension with higher elasticity in transverse axis. In 6 months after implantation all animals in group with longitudi-nal orientation of PL had transverse folds on the mesh. As a resultmesh length decreased by 14.6% and hernia defect under caudal bor-der of mesh was detected in 3 animals (Fig. 1A). In DL group withlongitudinal orientation meshes both increased in width and reduced
Fig. 1: Longitudinal orientation of meshes.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S27

S28 Hernia (2011) 15 (Suppl 2): S1-S35
in length by 12.5%, which led to margin fascial defect formation in2 rats (Fig. 1B). Deformations and complications in groups withtransverse orientation of PL and DL were not detected, becauseanisotropic properties of meshes close conformed to asymmetry ofphysiological loads. Conclusion: Orientation of anisotropic light surgical meshes accord-ing to biomechanics of abdominal wall should allow avoiding her-nia recurrence due to the mesh deformation.
O-123Choice of Mesh for Laparoscopic Ventral HerniaRepair (LVHR); a comparison of two intraperitonealcomposite meshes in a rat caecal abrasion modelF. Abuzaina, D. Guyader, J. Thomas, A.R. HadbaCovidien, R&D, North Haven, Ct, United States of America
Background: The in-vivo performance of Covidien’s Parietex™Composite mesh (PCO) and Ethicon’s Physiomesh™* was evaluatedin a rat caecal abrasion model. The purpose of the study was to eval-uate local tissue tolerance including tissue integration as well as theadhesion-barrier performance of both meshes at one, two, and fourweeks post implantation. Methods: In 44 rats, an abrasion was created on the surface of thecaecum, one surgical defect was created on the peritoneal surface ofthe abdominal wall of each rat and covered with either the test arti-cles: Physiomesh™* (n=20) and PCO (n=20) or the nude controlarticles: Parietex™ (n=4). The local tissue tolerance was macroscop-ically and histologically evaluated after one, two, and four weeks.Incidence of caecal adhesions and adhesions’ surface area were eval-uated macroscopically at one and four weeks. Scanning ElectronMicroscopy (SEM) of in-vitro incubated samples was also performedto evaluate the barrier-film breakdown over time. Results: Incidence of adhesions and adhesions’ area appeared numer-ically greater with the Physiomesh™* samples than with the PCOsamples. The Physiomesh™* samples had 0% tissue integration compared to 100% for PCO at week one. The Physiomesh™* sam-ples continued to have less macroscopic integration and slowerremodelling than the PCO samples at weeks two and four. Imagesof Physiomesh™* samples showed that the Monocryl™* barrierswere fully intact for up to nine days post in-vitro incubation. Minimaland random cracking appeared at 14 days. Such delay in film break-down may delay tissue ingrowth, which might lead to mesh migra-tion and recurrence.
Conclusion: An ideal LVHR mesh should have a continuous adhesionbarrier on the visceral side to minimize the potential for post-surgicaladhesions and an open-pore structure on the parietal side to allow forimmediate tissue ingrowth. The results shown here indicate differencesthat merit further study with statistically significant samples.
O-124Evaluation of the tissue repair efficacy of biologicalmeshes in a full thickness abdominal wall (FTAW)defect model in ratsN. Bryan1, H. Ashwin2, N. Smart2, Y. Bayon2, J.A. Hunt21 University of Liverpool, Clinical Engineering, Liverpool, UnitedKingdom
Introduction: Biological meshes are manufactured from decellu-larised tissues from varying anatomical origins, typically porcine. Thesuccess of a biological mesh relies on mechanical stability and incor-poration into adjacent tissues. Mesh failure resulting in recurrence isoften a consequence of early degradation of the mesh or its encap-sulation. In this study, the tissue repair efficacy of commercial bio-logical meshes was characterized in a full thickness abdominal wall(FTAW) defect model in healthy rats and in clean conditions. Methods: 2.0x3.0 cm FTAW defect was created in 6 week old malewistar rats (n=4/material/time point). Biological meshes (2.5x3.5 cm)were inserted into the defect, underlying the peritoneum, and fixed usingresorbable interrupted sutures. Tissue repair was evaluated at 1, 3,6 months post-operatively. Processing of explanted tissues was carriedout after resin infiltration observing histopathology (H&E, VanGieson).All materials used were porcine origin and prepared from crosslinkedor non crosslinked dermis or small intestinal submucosa (SIS). Results: After 1 month all meshes demonstrated different levels ofcellular infiltration from surrounding tissue. All meshes retained theirintegrity with exception of the SIS mesh which exhibited significantearly delamination. After 6 months, the latter mesh was difficult torecover, and histologically demonstrated the presence of abundantamounts of granuloma tissue and foreign body giant cells, signs ofa persistent inflammatory reaction. Dermal meshes retained collagenstructure throughout 6 months with cross-linked and non cross-linkedproducts behaving similarly in their biodegradation profiles. Even ifdermal meshes were poorly cell colonized, they were all incorpo-rated into adjacent tissues, thereby mechanically supporting theFTAW defect. There was neither hernia recurrence nor mesh encap-sulation observed for any group.
Table 1: Macroscopic observations at termination.
1 week
Article Number Percentage Mean Percentage Mean Type of Breaking Incidence Incidenceof sites of tissue surface of of adherent maximal adhesion strength (N) (%)
integration adhesion mesh (%) length (grade)(edges of (mm2) (mm)the mesh)
Physiomesh™* 8 0 ± 0 25 + 52 7 ± 14 4 ± 7 1 ± 1 0.45 ± 1.09 2/8 25
Parietex™8 100 ± 1 7 ± 20 2 ± 5 2 ± 4 0 ± 1 0.00 ± 0.00 1/8 13
Composite PCO
Parietex™ 2 100 ± 0 253 ± 112 67 ± 33 23 ± 6 2 ± 0 3.62 ± 1.12 2/2 100
Article 4 weeks
Physiomesh™* 9 68 ± 29 114 ± 135 30 ± 36 11 ± 11 1 ± 1 2.25 ± 2.33 5/9 56
Parietex™8 91 ± 25 40 ± 70 11 ± 19 6 ± 10 0 ± 0 1.01 ± 1.77 2/8 25
Composite PCO
Parietex™ 2 100 ± 0 339 ± 53 90 ± 14 29 ± 1 2 ± 1 4.03 ± 0.00 2/2 100
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S28

Hernia (2011) 15 (Suppl 2): S1-S35 S29
Conclusions: The SIS mesh induced significantly more inflamma-tory reaction and degradation than the other tested dermal meshes.No significant biodegradation differences were observed betweenporcine dermis meshes after 6 months post-operatively.
O-125Adhesion formation to intraperitoneally implantedmeshesM. DitzelErasmus MC, Surgery, Rotterdam, Netherlands
Background: During laparoscopic incisional hernia repair a mesh ispositioned intraperitoneally. This provides a possibility to inspect theabdominal wall for additional hernias, doesn’t necessitate a large dis-section and facilitates good cosmetic results. However, direct contactbetween the mesh and the abdominal viscera is inevitable and may leadto adhesion formation. Composite meshes and biosynthetic meshes mayreduce intra-abdominal adhesion formation, when compared with syn-thetic meshes. The aim of this study was to compare commonly usedsynthetic, composite and biological meshes on adhesion formation,shrinkage and ingrowth after one month. Material and methods: Seventy Wistar rats, divided in 7 groups of10, underwent midline laparotomy and implantation of an intraperi-toneal mesh of 2,5 by 3,5 cm, which was fixated with six non-absorbable sutures to the abdominal wall. The implanted meshes wereProlene® (polypropylene), Optilene large pores® (polypropylene),Optilene® small pores (polypropylene), Parietex Composite® (collagencoated polyester), Dualmesh (ePTFE), Surgisis® (crosslinked colla-gen), Strattice® (non-crosslinked collagen). After one month the ani-mals were sacrificed and the meshes evaluated for adhesion formation(percentage and Zühlke score), shrinkage and ingrowth. Results: Mean adhesion formation on Parietex Composite® (9%) wassignificant lower than the other meshes (40-68%). The adhesion for-mation on Strattice® was significant lower than Optilene® small pores(60%), Prolene® (63%) and Dualmesh® (68%). The mean tenacity ofadhesions was significant lower on Parietex Composite® than Optilenelarge pores®. The mean ingrowth of the Parietex Composite® (68%)and Optilene® small pores (69%) was significant better than the othermeshes (35-52%). Surgisis® (46%) and Dualmesh® (70%) showed sig-nificant more shrinkage than the other meshes (9-17%). Conclusion: Intraperitoneally implanted Parietex Composite® mani-fests the least amount and lowest tenacity of adhesions after onemonth.
O-126Complete versus partial midline reinforcement inincisional hernia repair: A randomized controlled trial(nct 00498810) F. Berrevoet, E. Reynvoet, A. Vanlander, X. Rogiers, R. TroisiUniversity Hospital Ghent, General and Hepatobiliary surgery,Ghent, Belgium
Background: Scar tissue has a significantly lesser loading capacitythan the intact ventral abdominal wall and therefore poses a perma-nent risk for herniation. It remains a matter of debate whether itmight be useful to completely restore the integrity of the abdominalwall over the complete length of the former incision. Methods: In this prospective randomized trial patients were ran-domly allocated to complete (group I) or partial repair (group II),with a 5 cm mesh overlap mesh in sublay position. Sample size was
calculated hypothesizing a 1year reduction rate in recurrence from15 to 5% (n=80). All patients needed informed consent and approvalwas obtained by the Ethical Committee of the Ghent University.Primary endpoint was the recurrence rate at 1 year. Multiple defectsrequiring complete reinforcement were considered protocol viola-tions. Patients were analyzed according to “as-treated analysis”. Results: One hundred patients were randomized. Exploration of theabdominal wall showed multiple defects in 82 patients, while 10patients had one defect but were allocated to complete reinforcement.Only 8 out of 49 patients allocated to group 2 got their randomiza-tion treatment (16.3%). This was the only reason to stop the trialprematurely. The operation time was longer in group I than in group II (126 minversus 75 min; p<.001), while wound morbidity was slightly elevatedin group I. The mean VAS pain score was similar in both groupsand after 1 year 3 patients showed a recurrence in group II (37.5%),while only 1 recurrence was observed in group I (1.1%, p<0.001). Conclusion: In midline incisional hernias complete reinforcement ofthe former incision line is the treatment of choice in all patients. Thismight lead to good results after longer-time FU. Both morbidity andchronic pain after 1 year do not increase with more extensive surgi-cal dissection.
O-127Incisional hernia prophilaxisK.M. Mylytsya, M.M. Mylytsya, N.S. LutsenkoZaporizhzhya Medical Academy of Postdiploma Education, Surgery,Zaporizhzhya, Ukraine
Background: Frequency of incisional hernias after laparotomymakes 20-30%. Methods: Connective tissue was examined on 580 surgical patients(consisting of 53,360 anthopometrical, 1,580 morphological, 948immunohistochemical tests). The result has shown presence of vari-ous forms (easy, moderated, heavy) of connective tissue dysplasia(CTD) at 59.1%. Patients were divided into two groups: 1st withCTD, and 2nd without it. It emerged that incisional hernias in the1st group (with CTD) met 6 times more often, and recurrent hernias7 times more often than in 2nd group. Thus, patients with CTD (espe-cially with the moderate and heavy degree) are group of high riskin development of a incisional hernia. The noninvasive technique ofdefinition of CTD and method of definition of incisional hernia riskare developed. For patients with high risk of incisional hernia a newtechnique has been offered (patent’ - 43,924) which consists in pre-ventive prosthetic implantation during primary laparorrhaphy.Prosthetic mesh strip, width 3-4 cm, fixed over or under aponeuro-sis, stimulates proliferation of collagen-producing cells (fibroblasts),leading to aponeurosis regeneration (Fig. 1). 80 patients with high
Fig. 1: incisional hernia prophilaxis.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S29

S30 Hernia (2011) 15 (Suppl 2): S1-S35
risk of incisional hernia (more than 75%) have been divided into twogroups. 1st - 40 patients which was operate by preventive technicwith use of prosthetic mesh strip during laparorrhaphy. 2nd - another40 patients whose abdominal wall was sutured by traditional meth-ods. In both groups patients used a bandage during 3 months afteroperation. Results: In a year hernia isn’t diagnosed for any patient in thefirst group. At the second group incisional hernia was diagnosed at6 patients (15%). Occurrence of the first hernia is fixed on 5 monthsafter operation. Conclusion: patients with CTD have high risk of incisional hernia.Method of preventive implantation of a prosthetic mesh strip duringprimary laparorrhaphy is very good in incisional hernia prophylaxis.
O-128Significant differences in laparoscopic repair ofprimary versus incisional ventral herniasE.J.P. Schoenmaeckers1, V. Stirler2, J.F.T.J. Raymakers2, S. Rakic21 UMC Utrecht, Surgery, Utrecht, Netherlands; 2 ZGT Almelo,Surgery, Netherlands
Background: To analyze the differences in the characteristics of pri-mary ventral (PVH) and incisional hernias (IH) and the outcomes oftheir laparoscopic repair (LR). Methods: Medical records of all 825 patients who underwent LRof PVH or IH were reviewed for baseline characteristics, operativefindings, conversions, and postoperative complications Claviengrade ≥ 3. Patients were divided into two main groups: IH groupand PVH group. Results: There were 343 patients with IH and 482 with PVH. MeanASA classification was higher in IH group (1.9 vs. 1.7, P<0.05). Atotal of 81% of IH patients required adhesiolysis as compared withonly 1% in PVH group (P<0.001). Conversion rate was higher inIH group (6.7% vs. 0.4%, P<0.001). IH group required longer sur-gery time (79 vs. 47 minutes; P=0.001) and a longer hospital stay(4.8 vs. 2.6 days, P=0.001). Mean surface of hernia opening wasgreater in IH group (32 vs. 3 cm2, P=0.001) as well as the surfaceof the applied mesh (344 vs. 154 cm2; P=0.001). Follow up was sim-ilar for both groups (49 vs. 46 months). Recurrence rate was higherin IH group (6.3% vs. 0.6%; P=0.001). Mesh infection occurred onlyin IH group (3.1%; P=0.001). Bowel lesions diagnosed postopera-tively occurred only in IH group (1.6%; P<0.05). Total complicationrate was higher in IH group (19.4% vs. 3.2%; P=0.001). RecurrentIHs showed a higher conversion rate (11.6% vs. 6% p<0.05) but nota significantly higher total complications rate as compared with pri-mary IHs. Conclusions: IHs are significantly more complex than PVHs andtheir LR results in longer operative time, higher conversion rate,longer hospital stay, and higher recurrence and complication rate. Itdoes not seem justified to continue pooling data on LR of IHstogether with PVHs, as is common practise in current literature.
O-129Comparison of ultrasonography and physicalexamination in the diagnosis of incisional hernia in aprospective studyA. Bloemen, P. Van Dooren, B.F. Huizinga, A.G.M. HoofwijkOrbis Medical Centre, Surgery, Sittard-Geleen, Netherlands
Background: Incisional hernia is a frequently occurring complica-tion after abdominal surgery with different reported incidences(2-20%). The incidence of incisional hernia is defined by the diag-
nostic tools and diagnostic criteria used. Discussion about how todiagnose and define an incisional hernia still exists. Diagnosis byphysical examination is sometimes difficult, especially in small inci-sional hernias or in obese patients. The additional diagnostic valueof standardized ultrasonography was evaluated in this prospectivestudy. Methods: A total of 456 patients participating in a randomized trialcomparing two suture materials for closure of the abdominal fasciaunderwent physical examination and ultrasonography at six monthintervals. Wound complaints and treatment of incisional hernia werealso noted. Statistical analysis was performed using SPSS, Chi-squared and Fisher’s exact test. Intertest variability analysis was per-formed. Results: During a median follow up of 31 months, 103 incisionalhernias were found. A total of 82 incisional hernias were foundby physical examination. Ultrasonography found an additional21 hernias (table 1). Of these additional hernias, six were sympto-matic. Only one of the newly found hernias received operative treatment (mesh repair). Intertest variability was low with a Kappaof 0.697 (P<0.001), indicating a good correlation between the methods. Discussion and Conclusion: When strict diagnostic criteria areapplied and combined diagnostic methods are used, the incidence ofincisional hernia is even higher than previously estimated. Becauseof the standardized follow-up, most hernias were found in an earlystage of development and were not symptomatic. There are no clear diagnostic criteria for incisional hernia availablein the literature. Standardized ultrasonography during follow-upyields a significant number of, mostly asymptomatic, hernias whichwould not be found using physical examination alone. This is espe-cially relevant in research settings.
Physical examination Physical examination Totalpositive for hernia positive for hernia
Ultrasonography62 21 83
positive for hernia
Ultrasonography20 353 373
negative for hernia
Total 82 374 456
Fig. 1: Diagnosis of incisional hernia.
O-130Endoscopic transhernial total extraperitoneal sublayventral hernia repair in single port techniqueW.M.J. ReinpoldGross Sand Hospital Hamburg, Surgery, Hamburg, Germany
Background: Laparoscopic IPOM repair and open sublay repair areboth established techniques for the cure of ventral and incisional her-nias. The IPOM-technique is nowadays performed with expensivemeshes whose bowel facing side is covered with adhesion prevent-ing material. IPOM meshes have to be fixated thoroughly with trans-mural sutures, staples or clips which carry the risk of adhesions andpain. Methods: We developed an endoscopic total extraperitoneal singleport technique for the sublay repair of ventral hernias: Via a 3 to4cm incision the hernia sac and midline defect are dissected. Theextraperitoneal space around the defect is carefully enlarged by seper-
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S30

Hernia (2011) 15 (Suppl 2): S1-S35 S31
ation of the peritoneum from the abdominal wall. A single portwith three 5-mm trokars (Covidien) is inserted into the defect.Capnopreperitoneum of 10 mmHG is applied and the whole circum-ference of the defect is dissected endoscopically. A standardpolypropylene mesh is inserted in the sublay position and fixatedwith sutures or clips at the lateral border. Alternatively a self fixat-ing mesh can be used. The hernia sac is removed and the midlinedefect is closed via the port incision. Results: We report 21 cases of small and medium size ventral andincisional hernias with an average dect size of 18 cm2, an averagemesh size of 191 cm2, and a minimum overlap of 5 cm. The largestmesh was 30x20 cm. In 7 cases the abdominal cavity was not opened.There was one retromuscular hematoma that did not need surgicalintervention. Pain medication was stopped after a maximum of 4 daysin all patients. The average Follow up of 18 patients is 7 months (2to 12 months). Up to now there is no recurrence. Conclusion: This technique combines the advantages of minimalaccess surgery and open sublay repair: The technique has to be eval-uated in studies.
O-131Risk factors for incisional hernia after J-shapedsubcostal incision after liver transplantation:a prospective studyB. De Goede, H.H. Eker, P.J. Klitsie, H.W. Tilanus, R.A. De Man,H.J. Metselaar, J.F. Lange, G. KazemierErasmus Medical Center, Surgery, Rotterdam, Netherlands
Background: A J-shaped incision is increasingly used for liver trans-plantations instead of a Chevron incision in an attempt to reducewound complications and incisional hernia. However, no prospectivedata are available. In this prospective study we aim to determine riskfactors and incisional hernia rates in liver transplantation patientsafter a J-shaped incision. Methods: Between January 2004 and March 2010, we performed aprospective single-center study investigating risk factors and inci-sional hernia rates in patients with a J-shaped incision after livertransplantation. All patients with minimum follow up of three monthswere seen at the outpatient clinic to determine the presence of inci-sional hernia. Preoperatively, Model for End Stage Liver Disease(MELD score), Child-Turcotte-Pugh score, underlying liver disease,cardiovascular and pulmonary comorbidities, diabetes, preoperativeBody Mass Index (BMI), hernia in medical history, wound compli-cations, length of hospital and ICU admission were prospectively col-lected. The chi-square test and Mann-Whitney U-test were used forcategorical and continuous variables, respectively. Results: During the inclusion period, 201 patients were transplanted.Median MELD-score at transplantation was 16. Mean preoperativeBMI was 25. During follow up 40 patients died. None of the patientsdied as a result of complications of the J-shaped incision. At a meanfollow-up period of 33 months 140 patients were physically exam-ined at the outpatient clinic. The incisional hernia incidence was33%. BMI>30, protracted ICU admission, diabetes, surgical siteinfection (SSI) and abdominal wall hernia in medical history werefound to be predictive for incisional hernia. Conclusions: The incidence of incisional hernia after a J-shaped inci-sion for liver transplantation is high. Preoperative BMI>30, DM, SSIand abdominal wall hernia are independent risk factors. Use of pri-mary mesh during liver transplantation can be considered to preventincisional hernia in these high risk patients.
O-132The role of ultrasound scan in the diagnosis of occultinguinal herniasD. Light, K. Ratnasingham, A. Banerjee, R. Cadwallader,M.M. Uzzaman, B. GopinathNorth Tees and Hartlepool NHS Trust, General Surgery, Stockton onTees, United Kingdom
Aims: The aim of this study is to examine the role of ultrasound inconjunction with clinical judgment in diagnosing occult hernias inpatients with groin pain.Methods: The study involved a retrospective analysis of 297 patientswho presented over an 18 month period from January 2007 to August2008. All the patients presented to out-patient clinic with groin painbut a normal or equivocal clinical examination. Data was obtainedfrom hospital records, radiology system and operation notes.Results: 167 examinations (56%) were positive for a hernia, as aresult of which 116 patients underwent surgery. At surgery, a herniawas found in 85 cases and no hernia was found in 31 cases. 130examinations (44%) were negative for hernia. Six patients proceededto surgery despite a negative ultrasound due to ongoing pain and ahernia was found in 5 cases. Overall, correlation with surgical find-ings showed ultrasound to have a sensitivity of 94%. Ultrasound usedwith clinical judgment has a positive predictive value of 73%.Conclusions: The accuracy of ultrasound alone in diagnosing groinhernias is questionable when correlated with operative findings.However in conjunction with clinical judgment it is a useful tool indiagnosing occult groin hernias and aiding in further management.
O-134Groin hernia repair in young males: Mesh or suturedrepair?T. Bisgaard, M. Bay-Nielsen, H. KehletDepartment of Surgery, Køge Sygehus, Køge, Denmark
Background: Large-scale data for the optimal inguinal hernia repairin younger men with an indirect hernia is not available. We analysednationwide data for risk of reoperation in younger men after a pri-mary repair using a Lichtenstein operation or a conventional non-mesh hernia repair.Methods: Prospective recording of all inguinal hernia repairs from1 January 1998 to 31 December 2005 in the national Danish HerniaDatabase, using reoperation rate as a proxy for recurrence. Weincluded only men between the age of 18 and 30 years with a pri-mary repair of a primary indirect inguinal hernia.Results:A primary sutured repair was performed in 1,120 men (medianage 23 years, range 18-30) and a Lichtenstein mesh repair in 2,061young men (24 years, range 18-30) (total 3,181 patients). The obser-vation time after conventional hernia repair was median 62 months(range 0-96) and 41 months (range 0-96) after a Lichtenstein repair.The cumulative incidence of reoperation at 5 years was 1.6%(Lichtenstein) versus 3.9% (sutured repair), while overall reoperationrates were almost three-fold as high after a sutured repair (39 reoper-ations, overall reoperation rate = 3.5%) compared to a Lichtensteinrepair (24 reoperations, overall reoperation rate = 1.2%; P=0.0003).Conclusions: Lichtenstein repair for an indirect inguinal herniareduces the risk of recurrence in young men between the age of 18and 30 years compared with a sutured repair. The use of aLichtenstein mesh repair in young males must be balanced againstthe risk of chronic pain.Reference:Hernia. 2010 Oct; 14(5): 467-9. Epub 2010 May 9.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S31

S32 Hernia (2011) 15 (Suppl 2): S1-S35
O-137Effects of prophylactic ilioinguinal nerve excision inmesh groin hernia repair: Short- and long-termfollow-up of a randomized clinical trialN. Crea, G. PataDepartment of Medical & Surgical Sciences, 1st Division of GeneralSurgery, University of Brescia, Brescia, Italy
We performed a randomized clinical trial on the impact of prophy-lactic ilioinguinal nerve excision (INE) on neuralgia, hypoesthesia,and analgesia requirement following open herniorrhaphy as well ason sustainability of a selective approach. Ninety-seven consecutivepatients undergoing a Lichtenstein procedure were treated with INE(n = 45) or preservation (NP) (n = 52). Impact of patients’ age, gen-der, type of anesthesia, and hernia on outcomes was also evaluatedby logistic regression analysis (LRA). Patients receiving INEreported less pain on postoperative days (POD) 1 and 7 and at1 month and required less analgesia on POD 1. Overall youngerpatients (40 years old or younger) had more postoperative discom-fort at LRA. Pain intensity was similar at 6 and 12 months after INEor NP: moderate to severe pain in 4.4 versus 11.5 per cent (P=0.279)and 4.4 versus 9.6 per cent (P=0.445), respectively. Hypoesthesiawas more frequent after INE on POD 1 and 7: 68.9 and 53.3 percent versus 13.5 and 9.6 per cent, respectively (P<0.0001), but nolonger at 1 month: 11.1 versus 3.8 per cent (P=0.244) as well as at6 and 12 months (0% in both study groups). No further correlationwas found by LRA. INE prevents inguinodynia up to 1 month fol-low-up regardless of patient variables. Moreover, the increase ofhypoesthesia proved to be a short-term complication.
O-142Risk factors for incisional hernia developmentU. Klinge RWTH Aachen & Universitätsklinikum Aachen, Aachen, Germany
Incisional hernia is a hernia following a surgical trauma. Whereasusually approximation of tissue by sutures result in a close linkageby scar, even stronger than the surrounding tissues, in some patientsthis fibrosis healing does not work properly. The consecutive devel-opment of a an incisional hernia. may be indicated by a wideningof the linea alba closely after laparotomy closure. In principle three different reasons may be accused: • Defective genes due to polymorphisms of the nucleotide sequence,either tackling crucial components of the innate immunity system,a proper function of the fibroblasts or the adequate deposition ofECM.
• An environment that hinders the appropriate transcription of intactgenes via attenuating activity of the corresponding promotors.
• A poor surgical technique with insufficient overlap, which doesnot reinforce the entire scar (as potentially permanent weakness),or which favours development of infections or local tissue necro-sis and impairs wound healing.
There are some few subgroups at risk with suspected geneticBackground: e.g. polycystic kidney disease, AAA, Ehlers-Danlos.However, there are more patients with incisional hernias withouta monogenetic disease, and from these patients we know severalclinical constellations marking an increased risk: e.g. old age,high BMI, smoking, recurrent incision, enterostomy, severe co-morbid-ity etc. Generally, all these components reflect an environmentthat may result in an altered activation of gene promotors, maybeby pathological methylation or by simple misbalance of transcriptionfactors, ending up in an appropriate transcription of differentgenes. Correspondingly, in soft tissue of patients with incisional
hernia several disorders in the extracellular matrix have beendetected. Whereas any traumatic surgery is related with an impaired woundhealing and thereby may favour the development of infection and/orincisional hernia, surgery directly influences recurrence rate if pro-viding insufficient overlap. As scarring in these patients is supposedto be inadequate and consecutively the fibrous fixation of a mesh tosurrounding tissues, an extended overlap underneath healthy tissueis crucial for permanent prevention of a recurrence. However, theextent of overlap depends on the anatomy and the procedure chosen,and therefore a good surgeon’s choice may avoid a recurrent herniafor the whole life of the patient.
O-143TEP inguinal hernia repair compared withLichtenstein; quality of life (the LEVEL- trial)P.J. Klitsie1, H.H. Eker1, H.R. Langeveld1, E.W. Steyerberg1,H.J. Bonjer2, J.J. Jeekel1, J.F. Lange11 Erasmus Medical Center, Surgery, Rotterdam, Netherlands; 2 VUMedical Center, Surgery, Amsterdam, Netherlands
Background: The debate on the preferred approach for inguinal her-nia repair is still continuing. Postoperative pain and recurrence rateshave been the main endpoints for the majority of the current litera-ture. Quality of Life, however, is the main motivation to performinguinal hernia repair. Therefore quality of life is important in thechoice of surgical technique. Methods: In this multicenter trial 660 patients were randomizedbetween Lichtenstein and TEP. The primary endpoint was postoper-ative pain. Postoperative Quality of Life was a secondary endpoint.All patient were invited to fill out a SF-36 questionnaire preopera-tively and 1 week, 4 weeks, 5 years postoperatively. Results: 326 patients were randomised to TEP and 324 to Lichtensteinrepair. Six weeks postoperatively TEP was associated with less post-operative pain (p=0.01). The SF-36 questionnaire showed favourableoutcomes for TEP 1 week after surgery on physical functioning(p<0.001), role physical (p=0.022), bodily pain (p<0.001) and socialfunctioning (p=0.004). After 4 weeks physical functioning (p=0.003),role physical (p=0.008) and bodily pain (p=0.001) were still betterafter the TEP procedure. After 5 years follow-up, the significant dif-ference in Quality of Life was disappeared. Conclusion: The TEP procedure was associated with significantlylower postoperative pain. The TEP procedure was superior to theLichtenstein technique on multiple aspects of postoperative Qualityof Life at 1 week and at 4 weeks after surgery.
O-144Development an Validation of a screening instrumentfor the prediction of chronic postoperative painK.H. Moser1, A. Althaus1, R. Lefering1, E. Neugebauer1,A. Hinrichs-Rocker21 Universität Witten Herdecke, Krankenhaus Köln Merheim, Köln,Germany
Studies suggest an incidence of chronic postsurgical pain (CPSP) in10% to 50% of patients undergoing various common operations.Identification of patients at risk of developing chronic pain, and themanagement and prevention of CPSP remains inadequate. Our goalwas to develop and validate an easily applicable screening instru-ment for the detection of high risk patients that takes into accountthe multifactorial etiology of CPSP.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S32

Hernia (2011) 15 (Suppl 2): S1-S35 S33
245 patients having undergone different types of surgery wereprospectively included in the study. Follow-up data was collected sixmonths after baseline assessment (n = 199 patients). To validate thedeveloped screening instrument according to the criterion CPSP, dataof 150 patients were finally analyzed in logistic regression analyses. Six months after the operation, 43.3% of the patients suffered fromCPSP. Five predictors multivariately contributed to the prediction ofCPSP: Capacity overload, preoperative pain in the operating field,other chronic preoperative pain, post surgical acute pain, and co-mor-bid stress symptoms (Nagelkerke’s R2 = .33, ROC area = .77, 95%CI: .70-.84). The remaining five items, each assessed by yes-noresponses, constitute an ordinal scale ranging from 0 to 5 (amountof present risk factors). The amount of patients presenting CPSPincreases linearly with every additional risk factor, i.e. the screeneris sensitive across the whole range of the scale. The results of this study suggest that a patient’s risk of developingCPSP can be predicted by using a limited number of pre- and peri-operative patient characteristics that can easily be assessed. TheCPPS may help care givers to tailor individual analgesic manage-ment and to assist high-risk patients with pain coping.
O-145Prospective randomized clinical trial comparinglightweight PTFE mesh and heavyweightpolypropylene Preliminary results of short andmedium-term results mesh in TEP groin hernia repairS. Morales-Conde1, I. Alarcón1, J. Bellido2, M. Socas1, A. Barranco1,M.D. Casado1, V. Gomez1, J. Cañete1, I. Serrano1, H. Cadet1,J. Padillo11 Hospital Universitario Virgen del Rocio, General Surgery, Seville,Spain; 2 Hospital General Básico de Riotinto, General Surgery,Huelva, Spain
Background: New advances in the development of laparoscopicinguinal hernia must focus on patients outcome aspects such aschronic pain, comfort or foreign body reaction. The aim of this studywas to find out whether the lightweight PTFE mesh improves patientsoutcomes at these aspects. Methods: Double blind prospective randomized clinical trial with50 male patients with bilateral inguinal hernia, where TEP repairwould be performed with a randomized use of a polypropyleneHeavyweight mesh or a PTFE Lightweight mesh on each side.Postoperative data is collected in successive consults seven days, onemonth, three months, six months and one year after the surgery usinga visual analog scale (VAS). We present the first 3 months follow-up results of our study. Results: Up to now, 37 patients (74 hernias) have been included inthe study. Mean operating time: 37.3 minutes. PTFE mesh meaningplacing time was 3.5 minutes, and handling difficult of 4.2 in a0-10 score, while PPL mesh mean placing time was 2.9 with a dif-ficult of 3.1. No significant differences were found. Differences werefound at 7 days concerning groin pain at rest (9.9 vs 3.6; p=0,005),discomfort (17.5 vs 5.6; p=0,03) and testicular pain (18.4 vs 6.7;p=0,01) favoring PTFE mesh. At one month a no significant higherdiscomfort was observed in PPL group (7.5 vs 2.2). Small differ-ences were also found at pain at rest and at movement and testicu-lar pain. Results at three months showed no differences. There wereno differences concerning complications and no recurrence wasobserved. Conclusion: Lightweight mesh appear to have advantages in termsof lesser pain and discomfort at seven days days and one month post-operatively as is proven in our study. More patients are still neededto determinate the benefits of PTFE lightweight mesh in longer term.
O-146Does socioeconomic and ethnical background influencehow patients with groin hernia are treated?U. Fränneby1, J. Björstad2, U. Gunnarsson1, G. Sandblom11 Karolinska Institutet, Dept of Surgery, Södersjukhuset, Stockholm,Sweden; 2 Västerås Hospital, Dept of Surgery, Västerås, Sweden
Objectives: The socioeconomic background of the patient may havean impact on how health care is provided in patients with inguinalhernia. Methods All patients aged 15 years or older with a primary unilat-eral inguinal or femoral hernia repair recorded in the Swedish HerniaRegister (SHR) between November 1 and December 31, 2002 weresent a questionnaire inquiring about complications within the first30 postoperative days. Data on civic status, income, level of educa-tion and ethnic background were obtained from Statistics Sweden. Results: Of the 1,643 recorded patients, 1,448 (88.1%) responded:1,341 (92.6%) were men and 107 (7.4%) women; the mean age was59 years. There were 195 (11.9%) non-responders. Adverse eventswere reported in the questionnaire by 391 (23.8%) patients. Patientsborne within the country reported significantly higher incidence ofevents necessitating contact with health-care than patients of otherethnical backgrounds (p<0.05), whereas the incidence of postopera-tive complications recorded in the register was not associated withethnic background. There was no association between registered andself-reported outcome and civic status, income or level of education Conclusion: Ethnic background influence the way the patients appre-hend the postoperative course after hernia surgery but does not influ-ence health care delivered for inguinal hernia.
O-147Ultrasound-guided ilioinguinal/iliohypogastric nerveblocks for chronic pain after inguinal hernia repairS.W. Nienhuijs, I. Thomassen, H. Suijlekom vanCatharina Hospital Eindhoven, Surgery, Eindhoven, Netherlands
Background: Chronic pain affects approximately 10% of the patientsafter an inguinal hernia repair. Mostly with a neuropathic character,it is an invalidating complication. One proposed treatment option is(repeated) nerve blocks. The goal of this study was to determine out-come of patients who underwent these blocks ultrasound-guided. Methods: Since 2005, a total of 53 patients suffering chronicinguinal pain have received ultrasound-guided nerve blocks. Theirpatients’ and operative details were reviewed. All received a postalquestionnaire including the DN4 for neuropathic pain, VisualAnalogue Scale pain scores (VAS), the Hospital Anxiety andDepression Scale (HADS) and Pain Disability Index (PDI). Results: A total of 51 patients completed the questionnaire (96%).The inguinal hernia repair (n=49) or gynaecologic procedure (n=2)was performed a median 2 years (range 6 months - 18 years) aheadof the nerve blocks. A median of 2 treatments (range 1-7) wasperformed. Initial success was not reached in two patients (4%),who subsequently received a neurectomy. Median follow-up was24 months (range 5-60). Thirty-two patients (62%) no longer reportedneuropathic pain. Their VAS pain scores at rest and during activitiesand PDI-scores were significantly lower than their counterparts(p<.05). Anxiety and depression was reported more frequently bythose who suffered neuropathic pain. Conclusion: Ultrasound-guided ilioinguinal/iliohypogastric nerveblocks can be effective to treat chronic inguinal pain. Repeated treat-ments may be required. For one-third of the patients without prolongedinitial success, other options such as neurectomy should be considered.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S33

S34 Hernia (2011) 15 (Suppl 2): S1-S35
O-148Minimally symptomatic patients undergoing ventralhernia repair have improved quality of life:A prospective international reviewD.A. Klima1, V.T. Tsirline1, I. Belyansky1, L. McRoy2,C. Romanowski2, A.E. Lincourt1, S. Bringman3, B.T. Heniford11 Carolinas Medical Center, Carolinas Laparoscopic and AdvancedSurgery Program, Charlotte, United States of America; 2 UnitedStates of America; 3 Karolinska Institutet, Department of Surgery,Sodertalje, Sweden
Introduction: Ventral and incision hernia repair (VHR) with meshis one of the most common operations performed by GeneralSurgeons. The risk of morbidity or chronic pain after VHR oftendeters a primary care physician referral for surgery or a patient toaccept operative intervention when asymptomatic. We undertook thisstudy to better define post-operative QOL and complications inasymptomatic patients undergoing VHR as a means to better estab-lish expected outcomes. Methods: We identified asymptomatic ventral hernia patients in theInternational Hernia Mesh Registry (IMHR), a multi-national herniaregistry where patients record their own personal outcomes, betweenSeptember 2007 and 2010. A Carolinas Comfort Scale (CCS) painscore of <2, representing non-bothersome symptoms, was deemedasymptomatic. The CCS is a well-documented QOL scoring systemfor patients before and after having had a mesh hernia repair. Pre-operative CCS pain scores were used for comparison only in patientswith corresponding post-op scores. Results: N=226 asymptomatic patients that underwent ventral her-nia repair were identified. Average age was 58.3±14.1 yrs, BMI was30.4±6.44 and gender was 55.3% male. Average defect size was7.3±5.5 cm by 9.9±7.6 cm. Post operative complications included4 wound infections (1.7%), 2 seromas (0.9%) and no mortalities orhernia recurrences (0%). Paired CCS QOL scores at 1 month(N=207) (1.68±0.74 v. 1.40±0.40, p<.001) were worsened frompre-op but were significantly improved to 1.29±0.57 v 1.41±0.42(p=0.03) by 6 months (N=143). Patient’s pain also returned back tobaseline by 6 months. Conclusion: Repair of ventral hernias in minimally symptomatic orasymptomatic patients has very little morbidity. Paired CCS overallQOL scores were, as expected, worse in the early post-operativeperiod, had improved significantly from pre-op at 6 months withoutevidence of chronic pain. Delaying ventral hernia repair in asymp-tomatic patients for fear of complications or chronic discomfort maybe unwarranted.
O-149Adrianus van den Spiegel, the last famous anatomist ofthe school of PaduaP. Broos, I. FourneauKatholieke Universiteit Leuven, Leuven, Belgium
Adriaan van den Spiegel, van den Mirror or Spigelius was a Flemishanatomist and surgeon who continued the Vesalian tradition at theuniversity of Padua. His name still is associated with the linea semi-circularis at the lateral side of the rectus abdominis muscle and thehernia at that region. Adriaan van den Spiegel, Spigelius, was born in Brussels in 1578.He died in Padua on April 7, 1625.He was the son and grandson of surgeons. His father was inspectorgeneral of the military and naval surgeons of the Dutch Republic andsurgeon in ordinary to William of Orange and probably a protestant.He died in 1600. The Spigelius family was probably well off, how-
ever, and both Adriaan and his brother Gysbertus studied medicine. Adriaan attended the universities probably in Leuven but certainlyin Leiden where Gerardus Bontius (1536-1599) and Johannes vanHeurne were his teachers. Nevertheless he was especially influencedby Petrus Pauw (1564-1617) professor of botanic and anatomy. In1601 he moved to Padua, where he registered between a lot ofFlemish and Dutch students in the German Nation, the NatioGermanica. William Harvey (1578-1657) was one of his colleagues. At Padua, he studied under Hieronymus Fabricius ad Aquapendente(1537-1619) and Giulio Casserio from Piacenza (Julius CasseriusPiacentinus) (1561-1616) and probably graduated in 1604. From1606 he was physician to the students of the Natio Germanica.In this period Spigelius became the favoured pupil of Fabrici andassisted him at his botanical research and in his private practice. Heaccompanied the old man to Florence tot treat a Medici Prince andon another to Venice where Fabrici gave a consultation. During theseyears, Spigelius also travelled trough Italy studying botany. He wrotean introduction to this science, Isagoges in rem herbaria. Lliber duo(Padua 1606 and 1608), witch he dedicated to the students of theNatio Germanica. He proves to have learned a lot from an otherteacher in Leiden: Clusius. In 1607 he competed for the chair of practical medicine at Padua,left vacant by the death of Ercole Sassonia (1551-1607). The GermanNation, at Spiegelius’ request recommended him to the Riformatorifor the position, but Spigelius did not get the chair because he wasconsidered to be to young.In 1612 he left Italy for Flanders. He remained there briefly, how-ever he travelled trough Germany and finally settled in Moravia. Soonafter he became medicus primarius of Bohemia.After the death of Casserius, on December 22 1616, the VenetianSenate appointed Spigelius professor of anatomy and surgery. He hadbeen nominated to the position by the Venetian patrician, Giustiniani,Venetian ambassador to the emperor in Prague when Spigelius wasthere but also by his previous master Fabrici. Spigelius started hislectures on June 17, 1617.Because of his interesting colleges, Spigelius attracted many foreignstudents to his public performances in the famous theatre at Padua.On January 25, 1623, he was elected knight (“eques”) of Saint Marcusan received a golden necklace that he wearied on his portrait. In the mean time Spigelius married an Italian lady named Prudentia.Probabaly, because of her, he became catholic again.He died on April 7, 1625 after an illness of six weeks. There hasbeen some discussions concerning the causes of his death: an stupidaccident during the wedding of his unique daughter or a liver dis-ease resulting in a liver abscess. The solution could be fined in abook written by Benedetto Silvatico: Consiliorum et responsorummedicinalium centuria quatuor (Padua 1651). The clinical evolutionof Spigelius’s disease has been clearly described: “I have assistedhim at his sickbed during 65 days. He had cut himself with a knifeat his index finger. After a few days his whole arm was swollen, aplague spot developed in his axilla. He became sick and had highfever. The plague spot brake trough after 20 days with the evacua-tion of stinking liquid and blood. He felt a bit better but fever didnot disappear. He presented diarrhoea, evacuating the same kind ofliquid as the one observed from the plaque spot. He died on the63rd day.” On February 4, 1625, just 63 days before his death, hissole daughter Anzola (Angela) 18 years old, was married withLiberalis Cremona a medical doctor from Trevisa and Vice-Syndicusof the university! At autopsy finding an abscess was discovered underthe liver, originating from the posterior liver lobe. The destiny wantedthat this lobe was described by Spigelius as the “lobus caudatus” andnow well known as “lobus Spigelii”.Spigelius is considerd by the historians as the last great Paduananatomist. Although known primarily as an anatomist, Spigelius wasa busy and much sought clinician, a meritorious botanist and a goodhelmintholog. After a few years he suffered from “febris semi-ter-
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S34

Hernia (2011) 15 (Suppl 2): S1-S35 S35
tiana” (malaria!!) and rote some manuscript on the disease (De semi-tertiana libri quatuor 1624). In a letter to Johannes Faber (1547-1629), Spigelius asked if he knows something concerning this dis-ease who was already familiar to Galenus. Faber was born in Bamberand lived in Rome since 1570. He was a well known medical doc-tor in ordinary to pope Urbanus VIII and also the “professore pon-tifico de semplici” (the herb-doctor in ordinary to the pope). Faberwas a pupil of Andrea Cesalpino (1519-1603) and since 1611 withGalilei one of the most famous members of the Accademia de Lincei. Spigelius wrote also an interesting essay concerning the evolution ofthe foetus, partially based on observations of his master Fabrici.This essay was edited posthumous by Liberalis Crema his son-in-law: De formato foetu liber singularis, aenis figuris ornatus (Padua1626). In this book we find also nine embryological tables comingfrom Casserius’s Tabulae Anatomicae among them, drawings depict-ing a pregnant woman whose abdomen is open in a flower-like man-ner. Casserius’s illustrations were drawn by the Venetian painter andprintmaker Odoardo Fialetti (Edoardus Fialettus) who studied underTinoretto and the engravings were prepared by Francesco Valesio(Franciscus Vallesius). A tenth plate by Casserius illustrating theexternal genital organs of a female newborn was added tot the Deformato Foetu published in 1645 by Johannes Blaeu in Amsterdam.Spigelius however was also a good botanist. Albrecht von Haller(1708-1777) considered his “Isagoge” as “a booklet not unpleasantat all”. Carl von Linné (Linnaeus) (1707-1778) will honour him giving his name tot a South-African plant: Spigelia marilandica.Probably because this plant can be used against worms an Linnaeusknowed that Spigelius in 1608 wrote an essay concerning tapeworms(De lumbrico lato).However we know Spigilius at first as an anatomist. A few daysbefore dying he asked his pupil Jan Rindfleisch (Bucretius) (1600-1630) from Breslau to finish his work. Bucretius published in 1627De humani corporis Fabrica Liber decem. Spigelius’s text of a mere24 lectures was padded by Bucretius into a big volume consisting of10 Libri. Bucretius illustrated the books with Casserius’s tables(Tabulae Anatomicae) and added 20 new tables. But as noted by
Haller in 1774, not all the added tables were originals. Many of themwere repetitions of illustrations previously publisched by Vesalius oreven by Casserius himself. Al lot of variations, often erroneous wereunscrupulously made by Bucretius. This was the main source of mistakes, wrongly ascribed to both Casserius and Spigelius. In manycases, features present in the tables are not properly described in thelegends.In 1645, Johannes, Antonides van de Linden (1609-1664), professorof medicine at the Franeker university, an admirer of Spigelius, pub-lished his “Opera quae extant Omnia” (two volumes, three parts).The splendid volume contained also the second edition of his “DeSemertertiana libri quatuor” and Gasparo Aselli’s (1581-1626) “Delactibus sive lacteis venis” and the fifth edition of William Harveys’s“Exercitatio anatomica de motu cordis et sanguinis in anamalis”, aswell as a short biography and a portrait of Spigelius.The name Spigelius will always be associated with: the lobus caudatus Spigelii, of the liver, the linea semilunaris Spigelii, lateralborder of the rectus abdominis muscle, the fascia Spigelii, fascia ofthe transverse muscle of the abdomen, and the hernia Spigelii, her-nia trough this fascia. References:Hee R. van. Chirurgie tijdens de renaissance in Heelkunde inVlaanderen, 118-120, Martinus Nijhoff 1988Houtzager H.L. Adrian van den Spiegel en zijn briefwisseling metJohannes Faber, Tijdschrift voor Geneeskunde, 66, nr 6, 2010Lindeboom G.A. Adriann van den Spiegel (1578-1625) hoogleraarin de ontleed- en heelkunde te Padua. Rodopi, Amsterdam 1978Linden J.A. van der. Opera quae extant omnia, Johannes Blaeu,Amsterdam 1645Riva A. et al. Julius Casserius (1552-1616): The self-made Anatomistof Padua’s Golden Age; The Anaomical Record (new Anat) 265: 168-175, 2001Sondervorst F.A. Adriaan van den Spiegel, Geschiedenis van deGeneeskunde in België, 95-97, Elsevier Brussel 1981Thiery M. Adriaan van den Spiegel (1578-1625) en de lijn vanSpiegel, Tijdschr. Voor Geneeskunde 63, nr 14-15, 2007
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S35

HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S36

Hernia (2011) 15 (Suppl 1): S37-S66
ABSTRACTS
Poster
© Springer-Verlag 2011
P-001Lysostaphin-coated Human Acellular Dermis (HAD)improves survival while maintaining graft performancein an infected fieldI. Belyansky1, T.R. Martin1, P.N. Montero1, V.B. Tsirline1, J. Shipp1,A.E. Lincourt1, A. Vertegel2, B.T. Heniford11 Carolinas Medical Center, Carolinas Laparoscopic and AdvancedSurgery Program, Charlotte, United States of America; 2 ClemsonUniversity, Bioengineering, Clemson, South Carolina, United Statesof America
Background: Staphylococcus aureus (S. aureus) is the causative agentin up to 90% of mesh infections. Lysostaphin (LS), a naturally occur-ring anti-Staphylococcal protein, has been identified as a potentialantimicrobial for use with mesh. The goal of this study was to deter-mine if LS can protect HAD graft from infection and improve sur-vival in a rat model. Methods: HAD samples were implanted in the onlay fashion in rats(n=75). Rats were grouped according to the absence or presence ofLS bound to HAD (none or LS) and and the absence or presence ofa bacterial inoculum (sterile, 10^6 and 10^8 CFU S. aureus). Ratswere followed closely post-operatively, and the meshes wereexplanted at 60 days. Explanted samples were used to assess bacte-rial growth, evaluate histology and test tensile strength of the mesh-fascial interface. Results: All of LS treated groups with a bacterial inoculum clearedthe S. aureus. All infected controls not treated with LS died as aconsequence of infection. Tensile strength was compatible withinthe LS treated groups: 6.45±2.77 N (sterile) v 4.79±1.97 N (10^6)v 5.41±1.70 N (10^8) (no statistical difference in all). Grossly therewere no physical differences between controls and LS/inoculummeshes. No microscopic/histological differences were visualized byblinded evaluators between controls and LS groups (sterile and 10^6).Greater ingrowth of mesh into the native tissue was found in LS(10^8) group, p<0.05, when compared to all other groups. Conclusion: LS treated HAD completely cleared S. aureus with dra-matically improved survival, and maintenance of mesh integrity andtensile strength and as compared to untreated controls. These find-ings strongly suggest the clinical use of LS-treated biologic mesh incontaminated fields may translate into more durable hernia repair.We believe that LS-treated biologic mesh shows real promise inimproving outcomes in infected abdominal wounds.
P-002Evaluation of the in vivo inflammatory dynamics ofsynthetic and biological meshes proposed for use asabdominal wall repair biomaterials in a subcutaneousimplantation modelN. Bryan, H. Ashwin, N. Smart, Y. Bayon, J.A. HuntUniversity of Liverpool, Clinical Engineering, Liverpool, UnitedKingdom
Background: Hernia meshes are manufactured from a broad spec-trum of materials, synthetic or biological. Modifications in chemicalor biological composition result in changes in foreign body reaction.In this study inflammatory dynamics for both synthetic and biolog-ical meshes were investigated to determine responses in changingkey features: chemistry and knitting pattern (synthetics), and tissueorigin and cross linking (biologics). Methods: Materials (1 cm2) were implanted subcutaneously (SC) intothe backs of 6 week old male wistar rats (4 materials per animal,n=6/material/time point), for 2, 5, 7, 14 and 28 days. Tissue process-ing was carried out after resin infiltration observing histopathology(H&E, VanGieson, VonKossa) and quantitative immunohistochem-istry. Collagens I and III were identified to qualitate neotissuematrix. Materials included four synthetics (PP, PET, PGA) and fourcrosslinked or non-crosslinked biologics from dermis or small intes-tinal submucosa (SIS). Results: All meshes stimulated a foreign body reaction allowing pre-cise deduction of their inflammatory characteristics. Histopathologydemonstrated differences in the magnitude and kinetics of cellular infil-tration, neo-vascularisation and interface thickness. Immunohisto -chemistry allowed quantification of the immune cell profile of materi-
Fig. 1: Quantitative Immunohistochemical Analysis of CD68 (maturetissue macrophages) and wound maturation index Col I/III. All cellcounts are normalized to total cell number in the explanted graft.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S37

S38 Hernia (2011) 15 (Suppl 2): S37-S66
als throughout their implantation. The predominant cell types for allmaterials were of a myeloid rather than lymphoid origin demonstratedby staining using macrophage markers CD68 (Fig.1), CD163 andT-lymphocyte antigen CD5. Tissue repair index was evaluated to compare the quality of the neo-tissue from the ratio of collagenI:III (Fig.1). A greater acute inflammation reaction was observedwith synthetic vs. biological meshes with the exception of the SISmesh. Conclusion: By using inflammation and wound healing indicators,this study showed that synthetic meshes elicited the greatest coloniza-tion with myeloid cells with the largest amount of macrophagerecruited by the multifilament PET mesh, due to its greater surface contact. The SIS mesh also stimulated a similarly strong inflammatoryreaction.
P-003Short and long-term adhesion formation with regard tobiological meshesM. DitzelErasmus MC, Surgery, Rotterdam, Netherlands
Background: During incisional hernia repair a mesh is frequentlypositioned intraperitoneally. Direct contact between the mesh and theabdominal viscera is inevitable and may lead to adhesion formation.Biosynthetic meshes present a new generation in prostheses andmight be a promising development in adhesion prevention. The aimof this study was to compare commonly used synthetic meshes withnew biological meshes on short and long-term adhesion formation,shrinkage and ingrowth. Material and methods: Sixty-eight Wistar rats, divided in 4 groupsof 17, underwent midline laparotomy and implantation of anintraperitoneal mesh of 2,5 by 3,5 cm. The implanted meshes wereSurgisis® (crosslinked collagen), Strattice® (non-crosslinked colla-gen), Parietex Composite® (collagen coated polyester) an Prolene®
(polypropylene). Each mesh was intraperitoneally fixated with sixnon-absorbable sutures to the abdominal wall. In each group10 animals were sacrificed after 28 days and 7 animals after90 days. All meshes were histological evaluated and adhesion formation (percentage and Zühlke score), shrinkage and ingrowthwere measured. Results: After 28 days the mean percentage of the surface of themesh covered with adhesions was significant lower on ParietexComposite® (9%) than the other meshes (40-63%). After 90 daysParietex Composite® (5%) and Strattice® (9%) had significantless adhesion formation than Prolene® (44%). The mean tenacity ofthe adhesions on both collagen meshes was significant lower thanon Prolene® after 90 days. Surgisis® showed significant more shrink-age after 28 days (46%) and 90 days (59%) than the othermeshes. No siginificant differences between ingrowth were seen.Microscopically a new mesothelial layer was seen on ParietexComposite® and Strattice®. Parietex Composite® showed most fibrob-last formation. Conclusion: Parietex Composite® and biological Strattice® meshesmanifested least adhesion formation after 90 days. In case ofcontaminated abdomen biomeshes might be safely positionedintraperitoneally if sublay position is impossible.
P-004Comparison of tensile strength of the abdominal wallafter repairing muscle-aponeurotic defect withpolypropylene and polypropylene-polyglecaprone meshin ratsR.M. Melo1, L.S. Silva2, D.F. Rodrigues1, A.S. Silva1, N.M. Paulo11 Federal University of Goias, Surgery, Goiania, Brazil; 2 School ofVeterinary Medicine, Surgery, Goiania, Go, Brazil
Background: The tensile strength of abdominal wall muscles wasexamined after a defect produced in the abdominal wall, repairedwith different-weight polypropylene meshes and polypropylene meshassociated with polyglecaprone. Methods: A total of 54 Wistar rats were used and randomized intothree groups with 18 animals each. A 3.0 cm (longitudinally) x 1.0 cm(transversally) fragment of the muscle-aponeurotic layer was resectedin all animals. The defect was closed in one group with lightweightpolypropylene mesh, coated on one side with polyglecaprone (PLG).In the other two groups simple lightweight (PPL) and heavyweight(PPP) polypropylene meshes were implanted. The animals were eval-uated at 30, 90 and 180 days post-operatively, when a muscle-aponeu-rotic fragment encompassing the implanted mesh was withdrawn. Thissample was tested in a mechanical testing machine at constant forceapplied against the interface tissue-mesh-tissue. The maximum force inkilograms was registered at the rupture of the sample.Results: Thirty days after surgery there was a significant difference(p≤0.05) between mean forces in the PPP group (3.16 kg) andPPL (2.54 kg), but the values of the PLG and PPL groups were similar. There was no significant difference among the three groupsat 90 days. At 180 days, there was a significant difference betweengroups PPL (2.85 kg) and PLG (3.36 kg) (p≤0.05), but no differencein tensile strength when the last one was compared with simplepolypropylene mesh. Conclusion: Polypropylene-polyglecaprone coated mesh seems suit-able for abdominal wall repair in the late period.
P-005Lightweight polypropylene mesh coated withpolyglecaprone for preventing peritoneal adhesions inratsR.M. Melo1, L.S. Silva2, L.B. Menezes1, A.S. Silva1, N.M. Paulo11 Federal University of Goias, Surgery, Goiania, Brazil; 2 School ofVeterinary Medicine, Surgery, Goiania, Go, Brazil
Background: Synthetic materials are the leading choice for abdom-inal wall rapair, but adhesions formation is still a problem when pros-theses are in close contact with abdominal viscera, especially thepolypropylene ones. Aiming to prevent a direct contact of this mate-rial with peritoneal surfaces, we investigated the preventing effect ofperitoneal adhesion of polyglecaprone coating one side of a light-weight polypropylene mesh. Methods: An abdominal defect was produced in the rectus abdo-minis muscle of 54 Wistar female rats, which were divided into threegroups of 18 animals each. The defect was repaired with a mixedmesh consisting of lightweight polypropylene coated on one side withpolyglecaprone (PLg). In the other two groups heavyweightpolypropylene (PPp) and lightweight polypropylene (PPl) mesheswere implanted. The prostheses was implanted in intraperitonealposition and fixed with four cardinal sutures in all animals. The pres-ence of adhesions was evaluated macroscopically, after necropsy at30, 90 and 180 days. Quantitative and qualitative analysis of peri-toneal adhesions were performed.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S38

Hernia (2011) 15 (Suppl 2): S37-S66 S39
Results:All groups showed adhesions from the omentum to the pros-thesis in varying degrees. In PLg group, there were adhesions in 42%of the prosthesis area after 180 days, and in the PPl and PPp groupsadhesions were found in 61% and 84% of the implanted area, respec-tively. We observed 27% of intestinal adhesions and 5% of liver adhe-sions to the prostheses in PPl group. In PPp group there were 61%and 11% of intestinal and hepatic adhesions to the prostheses, respec-tively. There were no adhesions of viscera to the prostheses of PLggroup. Conclusion: The polypropylene mesh coated with polyglecapronecompletely prevented the formation of visceral adhesions whencompared to heavyweight or lightweight polypropylene meshes.
P-006Seroma formation in rat latissimus dorsi resectionmodel with porcine dermis xenograft implantation:Results with and without quilting fixationZ.M. Hurwitz, R. Ignotz, R.M. DunnUniversity of Massachusetts Medical School, Surgery, Worcester, Ma,United States of America
Background: The aim of this study is to examine seroma in a ratmodel with commonly used biologic meshes as well as the role ofmechanical fixation (quilting) in mitigating seroma development. Methods: Sprague-Dawley rats (n=96, 250-300 g) were assigned toeither “quilting” or “non-quilting” groups and further divided intoone of three porcine dermal implant groups (Permacol™, Strattice™,or XenMatrix™) or controls (n=12 per group). The latissimus dorsiwas resected bilaterally through a 5 cm midline back incision. Ratsassigned to porcine dermal implant groups had 5x5 cm implantssutured into the surgical bed. In rats assigned to the “quilting” group,sutures were spaced 2 cm apart between the skin and the implant ormuscle. At 28 or 90 days, rats were euthanized, seroma and implantswere examined grossly and under H&E light microscopy. Results: Without quilt fixation, 7% of controls developed clinicallyevident seromas compared with 25% of all implant groups. Onnecropsy, all of the rats with implants had subclinical seromas(presence of a bursa) while a majority of the controls had variableevidence of bursa. Of the rats that underwent quilting, none of thosewith implants developed clinically evident seromas while 13% ofthose without implants did. Most quilted animals had bursae uponnecropsy, although the locations where the quilting sutures wereplaced demonstrated healing at the fixation site. Further histologicanalysis is being completed and will be presented. Conclusions: This study has validated a new rat model of seromaformation, with the majority of rats forming overt or subclinicalseroma. There is a trend towards increased seroma formation in thepresence of biologic implants. Mechanical fixation may provide somemitigation of seroma formation when a biologic implant is used.There is no clear evidence of a difference in seroma formationbetween the biologic grafts examined.
P-007Beneficial effects of Mineralo- and GlucocorticoidReceptors on foreign body reaction C.J. Brandt1, U. Klinge2, A. Fiebeler3, D. Kammer21 Onze Lieve Vrouwen Gasthuis, Surgery, Amsterdam, Netherlands;2 RWTH, Surgery, Aachen, Germany, 3Charite, Internal Medicine,Berlin, Germany
Prosthetic reinforcements markedly reduce risk of hernia recurrence.However, the implantation of meshes is related to an inflammatory for-eign body reaction (FBR) with serious complications (i.e. persistentseroma, wound infection, mesh-migration, entrapment, chronic pain).Adrenal hormones profoundly modify inflammatory response,(but/however) their effects on FBR are ill defined. We studied FBR tomeshes of polyvinylidenfluoride mesh material coated with hydrocor-tisone, mifepristone, aldosterone or spironolactone (stimulate and blockthe glucocorticoid receptor or stimulate and block the mineralocorti-coid receptor, respectively; substance release from the meshes within24 hours). Seven, 21, and 90 days after implantation, specimen wereevaluated for collagen formation, granuloma size, inflammatory activ-ity, and angiogenesis. Hydrocortisone- and spironolactone coating pro-tected from inflammatory response, while aldosterone and mifepristoneshowed little difference to the control. The hydrocortisone and spirono-lactone-groups showed a smaller granuloma size at all time-pointsreduced number of inflammatory cells (p<0.001) at day 90, and colla-gen formation was decreased starting after 21 days (p<0.05). There wasa negative correlation for angiogenesis with inflammation around for-eign body structures. In summary, early and temporary stimulation ofthe glucocorticoid receptor or blockade of the mineralocorticoid recep-tor have beneficial effects on FBR in the long term. Next studies willelucidate underlying signaling pathways involved.
P-008Evaluation of intraperitoneal placement of the PTFEknitted mesh in a New Zealand white rabbit model J. Jerabek, T. Novotny, J. Cagas, J. BucekSt. Anne´s University Hospital Brno, 1st. Department of Surgery,Brno, Czech Republic
Background: One of the standard materials used for intraperitonealonlay mesh repair is ePTFE mesh. According to some authors itsfavourable intraperitoneal results are determined by its lamellar structure. The objective of the study was to evaluate the behaviourof the PTFE knitted mesh (a macroporous mesh) in the intraperi-toneal position. Methods: Fourteen New Zealand white rabbits were randomized intotwo groups. Through a 10 cm midline incision two 5x5 cm piecesof PTFE knitted mesh or light-weight polypropylene mesh wereimplanted on the intact peritoneum on both sides of the abdominalcavity. The shrinkage and adhesion formation was measured 90 daysafter implantation using computer-assisted planimetry and adhesionscoring system. Histological assessment of foreign body reaction toimplant was also performed. Results: We found a significantly higher shrinkage of the PTFE knitted mesh compared to the light-weight polypropylene mesh. ThePTFE knitted mesh showed a significantly lower adhesion rate anddensity of adhesions. Histological investigation revealed a good bio-compatibility of both implants. Conclusions: The PTFE knitted mesh shows good histological biocom-patibility as the light-weight polypropylene implant. In intraperitonealposition, it has a low adhesion formation potential and seems suitablefor intraperitoneal placement. The only disadvantage of the material isa higher shrinkage compared to the light-weight polypropylene meshand therefore a sufficient overlap during hernia repair is necessary.Fig. 1: Rat with voluminous seroma two weeks after surgery.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S39

S40 Hernia (2011) 15 (Suppl 2): S37-S66
P-009Shrinkage of the various pore size polypropylenemeshes in rabbit modelJ. Jerabek, T. Novotny, J. Cagas, I. CapovSt. Anne’s University Hospital Brno, 1st. Department of Surgery,Brno, Czech Republic
Background: Amongst other consequences of inflammatory reactionshrinkage of the mesh has been described as a reduction of theimplant surface after implantation. One of the properties of the meshwhich influences the shrinkage is the porosity. The aim of our studywas to assess shrinkage improvement of the mesh-tissue complexwith increased pore size to 3.0x2.8 mm. Materials and methods:We chose the small open animal model. NewZealand white rabbits weighing from 2.9 to 3.4 kg were used. Animalswere randomized into 3 groups each of size of 7 animals. Three meshtypes were implanted. Two of them were pure polypropylene light-weight meshes of pore size 1.0x0.8 mm (LW-PP) and 3.0x2.8 mm(ELP-PP). The standard heavy-weight polypropylene (HW-PP) mesh(Prolene, Ethicon, Inc., NJ, USA) served as a control group. Generalanesthesia was used. After midline incision standard sized 10x10 cmpolypropylene mesh was implanted in onlay position. After 3 monthsanimals were sacrificed and the complete abdominal wall with implantwithout skin was removed. The borders of the mesh were scanned foranalysis. The results are given as a percentage decrease of originalmesh surface. Results: Shrinkage was observed in all three groups. The biggestshrinkage was observed in HW-PP group (mean 49.5%). LW-PPmesh had shrunk at the same extent (mean 49.3%) as HW-PP mesh.In case of ELP-PP we observed significant shrinkage reduction (mean30.6%) compared to both other materials. Conclusions: Increased pore size of light-weight pure polypropylenemesh to approximately 3 mm is associated with significant reduc-tion of shrinkage of the hernia mesh in onlay position.
P-010An overview of interventions to treat chronic inguinalpain after inguinal hernia repairS.W. Nienhuijs, I. Thomassen, H. Suijlekom vanCatharina Hospital Eindhoven, Surgery, Eindhoven, Netherlands
Background: Chronic postoperative inguinal pain can impair dailylife activities which necessitates treatment. Several interventions havebeen described, however without a consensus in the literature for analgorithm or sequence when to use which treatment. The objectiveof this review is to evaluate recent literature for the different inter-ventions to treat chronic inguinal pain after inguinal hernia repairand their outcomes. Methods: A multi-database search was conducted to reveal relevantstudies since 2001 reporting an intervention and their outcome totreat chronic postoperative inguinal pain in adult patients. Results: A total of 29 studies was included, eleven of them wereprospective, the remaining retrospective. One study reported complete(n=1)/partial (n=1) relief in 2 patients with gabapentin. Two reportswere on peripheral nerve block with in total nine patients with a combined complete relief in 55%. A total of 12 patients discussed in3 articles were treated with radiofrequency. Reported was a complete(n=7), partial (n=4) and no relief (n=1). In a case report a success-ful removal of a tacker was described. Stimulation of the nervestreated the pain complete for 5 patients and partial for 2 patients(3 studies in total). Cryoanalgesic ablation relieved the pain complete(n=7), partial (n=2) or not at all (n=1) in one study. By far most
reported was the outcome of neurectomy. A total of 733 patients in15 reports. Complete success ranged from 28-100%, partial 0-100%or no success 0-38%. Conclusion: This collective review showed the broad spectrum ofinterventions to treat chronic postoperative inguinal pain. Althoughdue to a wide range of pain definitions and outcome measurement atrue comparison is difficult, out of the results of these recent stud-ies a treatment algorithm is proposed.
P-011Use of Human Fibrin Sealant (Tisseel_) in HerniaRepairR.H. FortelnyWilhelminenspital, Department of General, Oncological and VisceralSurgery, Vienna, Austria
Objective: A systematic review of clinical studies was performed toevaluate the efficacy and safety of Tisseel® for mesh fixation in her-nia repair. Methods: An NLM/PubMed title/abstract search was conductedusing the following terms: (fibrin glue OR fibrin sealant OR TisseelOR Tissucol) AND (hernia repair). Bibliographies of the publicationswere reviewed for additional references. Results: 25 studies involving 4412 patients were included for review.In 4 comparative studies (n=535) using open surgery for inguinal her-nias, mesh fixation with Tisseel® consistently reduced the incidenceof chronic pain and complications compared with no fibrin sealant.In 3 noncomparative study (n=612) using open surgery, surgeonsreported few complications and high patient satisfaction. In 10 com-parative studies assessing laparoscopic hernia surgeries (n=2,186),postoperative acute and chronic pain scores in Tisseel® groups weresimilar or lower than controls. Similarly, Tisseel® mesh fixationshowed comparable hernia recurrence compared to fixation with sta-ples or tacks. Results for operative times varied and partially demon-strated shorter operative time in Tisseel® than control. In 8 noncom-parative studies (n=1,079) using laparoscopic surgery, Tisseel® wasassociated with a low incidence of complications, pain (postoperativeand chronic), and recurrence. Patients were typically discharged fromhospital within 24 hours after surgery and reported improvements inquality-of-life measures. Data from 4 studies of 158 patients under-going incisional hernia repair reported lower postoperative morbidity,improved quality of life, and significantly shorter hospital stay inTisseel® than controls. Safety data indicated that complications (i.e.,hematomas, bleeding, and incisional hernias) were similar betweenTisseel® and controls. Adverse events reported in 1 study (N=316)suggested no significant differences in the overall or serious adverseevent rates between Tisseel® and controls (suture). Conclusions: This systematic review demonstrated the efficacy andsafety of Tisseel® in mesh fixation during groin and incisional her-nia repair by various open and laparoscopic techniques.
P-012Validation of a questionnaire for assessment of painafter ventral hernia repair (VHPQ)U. Fränneby, L. Clay, G. Sandblom, U. Gunnarsson, K. StrigårdKarolinska Institutet, Dept of Surgery, Södersjukhuset, Stockholm,Sweden
Background: The aim of this study is to evaluate the validity andreliability of a novel ventral hernia pain questionnaire (VHPQ).Methods: The questionnaire was constructed with focus groups andsingle patient interviews with new and repeated groups until agree-
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S40

Hernia (2011) 15 (Suppl 2): S37-S66 S41
ment on accuracy. Validity was tested in 71 patients who receivedthe VHPQ and Brief Pain Inventory (BPI) 1 and 4 weeks after theoperation (group 1). Reliability and internal consistency was testedin 100 patients having surgery 3 years earlier and received the VHPQand BPI on two occasions one month apart (group 2). The non- surgery related pain was examined with the VHPQ on one occasionin 100 patients not previously having an abdominal operation. Results: For both items of pain intensity, a significant decrease wasseen from one week to four weeks postoperatively (both p<0.05).The same was also seen for all items of pain interference with dailyactivities (all p<0.05) except sitting, walking in stairs and sport activ-ities. The intraclass correlations were significant between the painintensity items of the VHPQ and the corresponding BPI items testedone week postoperatively (pain right now and pain last day versuspain past week, both p<0.05). Kappa levels for the test-retest of theinterference with daily activities items were higher than 0.5 for allitems except driving car and sport activities. For all the pain inten-sity items, the intraclass correlation was significant (all p<0.05) inthe test-retest group. Three years after surgery, the operated groupstated more pain in the pain intensity items (all p<0.05) and moreinterference with all daily activities except driving car (all p<0.05)than a matched non-operated group from the general population. Conclusion: The validity and reliability are sufficient to make theVHPQ useful in assessing postoperative pain and patient satisfactionin patients having ventral hernia repair.
P-013Impact of number of tacs on postoperative pain inlaparoscopic repair of ventral herniasE.J.P. Schoenmaeckers1, R. De Haas2, V. Stirler2,J.F.T.J. Raymakers2, S. Rakic21 UMC Utrecht, Surgery, Utrecht, Netherlands; 2 ZGT Almelo,Netherlands
Background: We determined postoperative pain after laparoscopicrepair (LR) of primary umbilical hernia (PUH). The main goal ofthe study was to analyze whether there exists a relation between thenumber of tacks used and postoperative pain. Methods: To reduce the number of prognostic variables, onlypatients with PUH who underwent a standardized LR, with the sametype of mesh (Dualmesh, Gore), and with the same type of tacks(ProTack, TycoUSS), were enrolled in this study. The first group wascollected from a previous trial and consisted out of 40 patients whounderwent fixation with a double crown (DC) where no minimumamount of tacks was determined before hand (mean number of tacks45.4±9.6). The second group was a cohort of 40 new patients whounderwent DC fixation by using a minimal number of tackers considered to provide an adequate fixation of the mesh (mean number of tacks 20.4±1.4). To eliminate systematic and randomerrors, we analyzed only for postoperative pain. The severity of thepatients’ pain was assessed preoperatively and at 2, 6, and 12 weekspostoperatively by using a visual analogue scale (VAS). Results: There was a significant difference in the number of tack-ers used between the two groups (P=0.001). There were no signifi-cant differences between the two groups in VAS scores at any assess-ment time. There was no correlation between the number of tacksused and postoperative pain. Conclusions: Less tacks does not create less pain experienced bythe patient, nor do more tacks create more pain. This absence ofa correlation between the number of tacks used and postoperativepain may indicate that pain after LR of ventral hernias is generatedaccording to some “threshold” principle, rather than being due to acumulative effect created by more points of fixation.
P-014Use of the Carolina Comfort Scale (CCS) for evaluationquality of life after hernia surgery with meshA. Koch1, R. Lorenz2, M. Wiese3, H. Born41 Day Surgerey Center,Cottbus, Germany; 2 3 Chirurgen, Berlin,Germany; 3 Gesundheitszentrum Kelkheim, Kelkheim, Germany; Surgical Center Leipzig Lausen, Leipzig, Germany
Background: With the use of mesh shown to considerably reducerecurrence rates for hernia repair and the subsequent improvementin clinical outcomes, focus has now been placed on quality-of-lifeoutcomes in patients undergoing these repairs, specifically, as theyrelate to the mesh prosthesis. The SF-36 quality-of-life survey,although well studied and validated, may not be ideal for patientsundergoing hernia repairs. In 2007 Heniford et al. propose a newquality-of-life survey, the Carolinas Comfort Scale (CCS), pertain-ing specifically to patients undergoing hernia repair with mesh. Methods: 15 specialized ambulant hernia centers in Germany carryon a large multicenter study on hernia repair since 1st of October2009. There are enrolled more than 1,000 patients. The CCS ques-tionnaire was mailed to all patients 4 and 12 weeks after surgery. Aclinical examination by the surgeon was also made 4 and 12 weekspostoperatively. Future examinations and mailings of the CCS areplanned 52 weeks after surgery. Results: There were 75% of all questionnaires returned and used inthis study. The patient satisfaction rate was 98%. Conclusion: In conclusion, this study demonstrated that the CCS, ashort, disease-specific quality-of-life questionnaire, is a feasibleinstrument to evaluate the quality of life after hernia surgery as apart of a quality management system. It is easy to use and the accept-ance is high. The CCS should be the preferred quality-of-life surveyof patients undergoing hernia repair with mesh.
P-015Life quality of patients after hernia repairV.V. Parshikov1, V.V. Petrov2, V.A. Khodak2, A.B. Baburin2,A.A. Samsonov2, R.V. Romanov2, V.P. Gradusov2, A.I. Rotkov2,A.V. Samsonov21 Nizhny Novgorod State Medical Academy, Hospital Surgery, NizhnyNovgorod, Russian Federation; 2 Hospital 35, Surgical, NizhnyNovgorod, Russian Federation
Background: Abdominal wall tension-free plasty become the mainmethod of opera-tions in planned and urgent surgery of hernias[Gebrovsky V.V., 2005; Egiev V.N., 2009]. The problem of effect ofoperation’s method and implant’s material on the quality of life of thesepatients is important today. [Vnukov P.V., 2007; Liadov V.K., 2009].Methods: About 1300 operations on account of abdominal herniashave been performed in City Hospital '-35 of Nizhnii Novgorod dur-ing last 6 years. 262 of these patients were operated in urgent order.Since 2006 we apply reperene implants in surgery of hernias. Wequestioned 87 of all these patients with MOS SF-36. Research design.1st group includes patients with self-tissue ab-dominal wall plasty(N=11). 2nd group - patients after abdominal plasty with repereneim-plants (N=31). 3rd group - patients after plasty of abdominal wallwith polipropilene meshes (N=45). Results: It is established, that the quality of life of most of the patientswas high. The indices of the quality of life in groups of tension-freeplasty in comparison with group of self-tissue abdominal wall plastywas higher. Indicators of scales of role-physical functioning (p=0.012),bodily pain (p=0.045), general health (p=0.002), vitality (p=0.044),social func-tioning (p=0.0001) and mental health (p=0.041) were sig-nificantly higher after a plasty of the inguinal canal with reperenemeshes in comparison with 1st and 3rd groups (pic. 1).
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S41

S42 Hernia (2011) 15 (Suppl 2): S37-S66
Conclusion: Life quality indicators were higher by patients operatedwith implants and tension-free plasty. Life quality of patients afteringuinal hernia repair with reperene meshes was signifi-cantly higherin comparison to polypropylene. Chronic pain and foreign bodysensation in the polypropylene group had 33,3% of patients, inreperene group - 23%.
P-016Laparoendoscopic single site tep hernia repair –Comparison of two techniques: Initial experienceJ.F.C. Filipovic, I. Kirac, M. Bekavac Beslin, A. Mijic, T. KulisKB Sestre milosrdnice, Surgery, Zagreb, Croatia
Introduction: Single incision laparoscopic surgery (SILS) alsoknown as laparoendoscopic single site surgery (LESS) has recentlybeen implemented in many laparoscopic surgical procedures. Herein,initial experience with LESS total extraperitoneal (TEP) inguinal her-nia repair in comparison to standard laparoscopic TEP is reported. Methods: Between November 2008 and May 2010, 41 single-incisionlaparoscopic TEP repairs of inguinal hernia and 40 laparoscopic TEPrepairs of inguinal hernia were performed for 81 patients. Data regard-ing patient demographics, type of hernia, operating time, complications,postoperative hospital stay, and recurrence were prospectively collected. Results: All 81 patients were men, ranging in age from 17 to 84years. Of the 46 men, 6 had bilateral inguinal hernias in LESS TEPgroup and 12 in TEP group. The operating time for bilateral LESSTEP was 56.57 (40-70) and 51 (20-100) for unilateral LESS TEP,while for bilateral hernia TEP was 71.43 (40-100) and for unilateralTEP was 52.14 (40-80). There were no intraoperative complicationsand no deaths. There was one mesh displacement in early postoper-ative period in LESS TEP group. Discharge was within 72 hours formost patients in both groups.There was no evidence of early recur-rence during a median follow-up period of 312 days for LESS TEPand 293 days for TEP. Conclusion: In our experience LESS TEP inguinal hernia repair issafe and feasible in selected cases. There was no statistically signif-icant difference in operating times, hospital discharge or intraopera-tive complications between two groups. Further studies comparinglaparoendoscopic single site and conventional multiport laparoscopicTEP repairs with long-term follow-up evaluation are needed to confirm the initial experience.
P-017Laparoscopic totally extraperitoneal inguinal herniarepair: 27 serious complications after 4,408 consecutivecases.A. MeyerUniversity of São Paulo, Gastroenterology, São Paulo, Brazil
Background: Informed consent must be obtained for the laparo-scopic extraperitoneal inguinal hernia repair procedure, and the sur-geon must inform patients of the operative strategy and the possibil-ity of complications or conversion to an open surgery. The first aimof this study is to determine the rate of serious complications fol-lowing laparoscopic totally extraperitoneal (TEP) repair. The secondaim is to help the surgeon to avoid these complications. We will dis-cuss the technical changes to the operative technique that help reducethe rates of complication, and we will give our reasons for continu-ing to utilize the laparoscopic approach. Methods: We evaluated subjects for inclusion in a consecutive seriesof 4,408 laparoscopic hernia repairs for patients who had undergonethe TEP procedure between January 2001 and January 2009. Theinclusion criteria were diagnosis with symptomatic inguinal hernia,including recurrence after inguinal hernia repair and previous lowerabdomen and pelvic surgery. All patients were ≥ 18 years old. Patientswith urgent incarcerated hernia were excluded from the study. Results: A total of 4,408 hernia repairs were included in the study.The hernias were repaired by TEP technique. There were 27 seriouscomplications (0.6%): 12 hemorrhages (0.2%), 2 bladder injuries(0.04%), 5 occlusions (0.11%), 4 bowel perforations (0.09%),1 lesion of the iliac venous (0.02%), 1 lesion of the femoral nerve(0.02%), 2 lesions of the vas deferens (0.04%) and 2 deaths (0.02%)(pulmonary embolism, peritonitis). Conclusion: The rate of complications with TEP procedure is low.Laparoscopic hernia repair is a reproducible and reliable technique.In our experience, there are contraindications for the TEP procedure.The TEP technique must be meticulous to avoid intraoperative complications (bipolar diathermy). Complications can occur evenafter the surgeon has acquired substantial experience. The patientmust be told about the possible complications.
P-018Trans Abdominal Pre Peritoneal laparoscopic inguinalhernia repair: What's the best mechanism of prosthesisfixation?G. Cesana, S. Olmi, E. CrocePoliclinico San Marco, Surgery, Zingonia - Osio Sotto, Italy
Background: Laparosocpic inguinal hernia repair seems to have manyadvantages in postoperative outcome of the patient. Sutureless repairavoid chronic groin pain. In this study we compare laparoscopic inguinalhernia repair TAPP (Trans Abdominal Pre Peritoneal) using agrapphesas mechanism of fixation and sutureless technique using fibrin glue. Methods: Patients with inguinal hernia were enorolled in this retro-spective study. 604 patients underwent TAPP with agrapphes and 791patients underwent TAPP with fibrin glue. Results: With a complete follow up of 60 months we report onlyone conversion and one relapse in the agrapphes group. The inci-dence of seroma, of postoperative neuralgia, of persistent pain andinguinal hematoma was significatively lower in those patients whounderwent sutureless repair. Conclusions: Sutureless laparoscopic inguinal hernia repair is feasi-ble without big complications and seems to have some advantagesover the classic technique.
polypropylene reperene local tissue plastyPF – Physical Functioning (p=0.117) RP – Role-Physical Functioning (p=0.012)BP – Body pain (p=0.045) GH – General Health (p=0.002)VT - Vitality (p=0.044) SF – Social Functioning (p=0.0001)RE – Role-Emotional Functioning (p=0.278) MH – Mental Health (p=0.041)
PF RP BP GH VT SF RE MH
90%80%70%60%50%40%30%20%10%
0%
Fig. 1: 1. Life quality of patients after hernia repair.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S42

Hernia (2011) 15 (Suppl 2): S37-S66 S43
P-019Emergency groin hernia repair, our experienceH. Mesquita Fernandes, C. Santos CostaCentro Hospitalar do Alto Ave, General Surgey, Guimarães, Portugal
A surgery made in emergency context has worst outcome. Excessivewaiting time for elective hernia repair, delayed diagnosis or patientreluctance to surgery increases the risk of hernia strangulation, bowelresection, morbidity and mortality. The aim of this study is todescribe and characterize the population submitted to emergencygroin hernia repair in our hospital. It is a retrospective study carried out from January 2007-December2010. Epidemiologic, clinical and therapeutic aspects were studiedas well the associated morbidity and mortality. The data were ana-lyzed using SPSS Statistics 17.0® program. The study included 101 patients (59 Women/42 Men). Mean age 67.Concomitant diseases were present in 114 patients (hypertension36.6%, heart disease 22.8%, pulmonary disease 15.8%, dyslipidemia11.9%, warfarin-induced hypocoagulation 9.9%, diabetis mellitus9.9%). The majority of patients presented pain and swelling (76.2%);23.8% signs of occlusion. The hernia location: 57 cases femoral(84.7% women), 44 Inguinal (83.3% men). 40% of femoral herniashad previous inguinal hernioplasty. The femoral hernias were pre-dominantly repaired with “plug repair” technique (98.2%) with bowelresection in 15.7% and omentectomy in 5.26%. Inguinal hernias wererepaired with “tension free” technique (Lichtenstein 72.7%, Rutkow-Robbins 22.7%, Gillbert 4.5%). Bowel resection was performed in6.82% and omentectomy in 2.27%. One Amyand’s hernia wasrepaired with apendicectomy and Lichtenstein hernioplasty. The mostfrequent surgical complications were: wound site infection (2.0%),local hematoma (2%), scrotal hematoma (1%) and seroma (1%).30-day mortality rate was 4% (four cases).Between deads, all patientshad ≥ 77 years old and 75% an ASA score ≥ III. The mean hospi-talization time was 3.72 days. In this study, femoral hernias were more frequent, and the majorityof them occur in women. Inguinal hernia were more frequent inmen. The cases of strangulation were higher in femoral hernia(18.26% Vs 9.09%). The morbidity was 6%, and mortality 4%.No mortality was seen in patients with bowel resection. Higher age(≥77 years) and ASA score ≥ III were associated with increasedmortality.
P-020Clinical evaluation of the SWING-CONTACT® mesh,a new three-dimensional fixation free device withatraumatic grips on both sides, in the treatment ofgroin herniaE.M. Magne1, W. Bertolaso21 CliniqueTtivoli, Chirurgie Digestive Parietale, Bordeaux, France;2 Clinique du Pont de Chaume, Chirurgie Digestive, Montauban,France
The SWING-CONTACT® mesh (SWING-TECHNOLOGIES) ismade of polyester three-dimensional multifilaments with atraumaticgrips on both sides avoiding the use of a fixation system. A clinicaldata collection was set up in order to confirm the safety and per-formances of these new meshes used in hernioplasty.
It is a non-interventional scientific evaluation subjected and acceptedby the French authority according to the regulations in force. Thedata were collected by means of a pre-established follow-up form.The data include demographic and pre-operative data as well as theresults of a follow-up visit. We are reporting clinical data on a group of 52 patients operated foran inguinal or femoral hernia. Total extraperitoneal (TEP) meshrepair was performed for all patients. The mean surgery and hospi-talization length were respectively 33 minutes and 1.7 days. The her-nias sizes were comprised between 10 and 20 mn. A total of 74meshes were used in this group of patients. None of them was fixed. Peritoneal breach was reported during surgery in 3 patients (5.8%).A total of 20 complications were reported at the follow-up visit(mean of 24 days): 1 urinary retention (1.9%), 6 testicular syndromes(11.5%) and 13 seroma (25%). Only one testicular syndrome wasassociated with some pain evaluated at 6 on the visual analogue scale(VAS). The majority of seroma were painless and spontaneousresorption was achieved following few weeks. No recurrence wasrecorded. The time of return to a current activity for 46 patients wasbetween 2 and 21 days. In conclusion, no complication implicates the safety of the patientsor the benefit-risk ratio. All of them are classical complicationobserved in the treatment of groin hernia. The effectiveness of thegrips could be highlighted by the absence of recurrence and paindirectly related to the device or the presence of grips.
P-021Primary inguinal hernia and neuroma of theilio-inguinal nerveS. KumarThe Royal Infirmary, General Surgery, Edinburgh, United Kingdom
Background: A peripheral nerve subjected to local trauma or compression may develop a localised thickening or swelling calleda neuroma. Aim of this study was to examine the ilio-inguinal nerve for a neu-roma and determine its incidence in patients undergoing primaryinguinal hernia repair. Patients and methods: Ilio-inguinal nerve was examined for alocalised thickening or swelling, suggesting development of a neu-roma, in male patients undergoing primary inguinal hernia repairbetween Dec 2001 and May 2007. A neuroma bearing ilio-inguinalnerve was excised and subjected to microscopy for evidence of neu-roma such as fibrosis and axonal loss. The patients were counselledabout chronic pain and groin numbness after nerve excision, andreviewed in the outpatient clinic four weeks postoperatively.Subsequent follow up was on as required basis. Patients with previ-ous lower abdominal surgery were excluded from the study. Results: 102 male patients, median age 72 years (range 17-89) hadopen repair of primary inguinal hernia. 13 (12.7%) patients had clin-ical evidence of neuroma of the ilio-inguinal nerve, 11 (84.6%) ofwhom had histological evidence of a neuroma but no abnormalitywas seen in the other 2 (15.4%). Thus 11 (10.7%) patients had clin-ical and histological evidence of neuroma developing in the ilio-inguinal nerve. At follow up, all these 13 patients were free of groinpain but had some numbness in the groin. Conclusion: Neuroma of the ilio-inguinal nerve was evident in10.7% of patients undergoing primary inguinal hernia repair. Thismay influence the policy of nerve preservation at hernia repair.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S43

S44 Hernia (2011) 15 (Suppl 2): S37-S66
P-022TIP-technique for inguinal hernia after previousinguinal or preperitoneal surgery: A feasibility studyF. Berrevoet, C. Staelens, E. Snoeck, A. Vanlander, X. Rogiers,R. TroisiUniversity Hospital Ghent, General and Hepatobiliary surgery,Ghent, Belgium
Background: The preperitoneal space is considered the most phys-iological place for a mesh in inguinal hernia repair. However, previ-ous surgery in this surgical plane seems a contraindication for usinglaparoscopic techniques. The aim of this study was to evaluate thefeasibility of using the transinguinal preperitoneal (TIPP) techniqueusing a memory ring patch in this group of patients. Methods: We selected patients with former inguinal hernia repairand those with surgery in the preperitoneal space (group I, n=56)from our prospective database. We compared this cohort with a control group of consecutive patients treated with the TIPP techniquefor inguinal hernia repair in 2009 who never had inguinal or otherpreperitoneal surgery in the past (group II, n=58). Group I was fur-ther divided for subgroup analysis in a cohort with previous inguinalhernia repair (group Ia) and a cohort with former preperitoneal sur-gery or radiotherapy (group Ib). Approval by the Ethical Committeeof the Ghent University was obtained. Results: Preoperative characteristics were comparable. The meanoperative time was significantly shorter for group II versus group I(p=0.001). TIP Conversion Group Ia Lichtenstein n=6 6 0, Primary repair n=16 16 0,Stoppa n=3 1 2, TAPP n=4 1 3, TEPP n=2 2 0 Group Ib Prostatectomy n=9 5 4, Hysterectomy n=5 5 0,Radiotherapy n=10 8 2, Sacral trauma n=1 0 1 Group II No previous surgery 58 0 Mean hospital stay was comparable between the two groups, while4 patients of group I reported having chronic pain postoperatively,compared to none of the patients in group II. Conclusion: Previous preperitoneal surgery or inguinal hernia repairsare no strict contraindication to perform a TIP repair. However, dur-ing surgery the anatomical plane can’t be dissected in some patientsand an subaponeurotic repair is indicated.
P-023Laparoscopic transabdominal hernia repair forincarcerated groin hernias: Technique, pitfalls, results U. Steinhilper, E. Bielesch, D. LaquaKlinikum Muenchen-Pasing, Center of minimal invasive surgery,Munich, Germany
Introduction: Laparoscopic Hernia Repair for incarcerated herniasis rarely performed standardized and seldomly has been published instudies. We present our experiences in 54 emergency cases of TAPPoperation for acutely incarcerated hernias (Learning curve/acquiringa standardized technique/results), further on we will give a reviewof Literature. Method: Since 1995, beside 3600 scheduled Hernia procedures, weoperated laparoscopically on 54 patients with acutely incarceratedinguinal or femoral hernias in a standardized transabdominallaparoscopic procedure (TAPP) with application of a titaniumcoated mesh after Reduction of the Hernia Sac. Investigation wason to difficulties in laparoscopic hernia sac reduction, estimation ofthe vitality of the incarcerated tissue, i.o. complications and p.o.outcome.
Results: Acutely incarcerated Hernias: N= 54 (100%), Small bowelobstruction: 39 (72, 2%), Reduction Problems: 7 (13%), Conversiondue to Major-Complication (Small Bowel-Perforation): 1 (1, 85%),Simultaneous Operation of the contralateral side: 10 (18, 5%),Wound-, Mesh infection: 0. Further Results will be given.
Conclusions: Standardized laparoscopic Repair of incarcerated groinHernias is feasible and safe. Main Advantage is the meticulousassessment of the previously incarcerated organs with respect to theirvitality in combination with a minimal invasive one step Procedure.No infections occurred, however, there is a learning curve on tech-nical skills for Hernia sac Reduction at low Risk.
P-024Outcomes after emergency hernia repair, a four-yearstudyH. Mesquita Fernandes, C. Santos Costa, D. Teixeira, T. Neto SantosCentro Hospitalar do Alto Ave, General Surgey, Guimarães, Portugal
Emergency hernia repair has an increased risk of morbidity and mortality. The aim of this study is to describe the results of thepatients that were submitted to emergency hernia repair and find thefactors that can affect morbidity and mortality. It is a retrospective study carried out from January 2007-December2010. Epidemiologic, clinical and therapeutic aspects were studiedas well the associated morbidity and mortality. The data were ana-lyzed using SPSS Statistics 17.0® program. The study included 143 patients (88 Women/55 Men). Mean age65.45 (13-97 years). Concomitant diseases were present in 114 patients (hypertension 35%,heart disease 23.1%, pulmonary disease 15.4%, dyslipidemia 11.9%,and warfarin-induced hypocoagulation 11.2% the most frequent). The majority of patients presented pain and swelling (75.5%); 24.5%signs of occlusion. The hernia location: 52 cases femoral (36.4%), 49 Inguinal (34.3%),19 Umbilical (13.3%), 11 Epigastric (7.7%), 9 Incisional (6.3%),2 Spiegel (1.4%) and 1 Diaphragmatic (0.7%). 18.2% had strangu-lated hernia. The groin hernias were predominantly repaired with “tension-free”or “plug” techniques. Epigastric/Umbilical hernias were repaired asprimarily. The use of a mesh in incisional hernias with large defectwas the rule. The most frequent surgical complications were: wound site infection(3.5%), local hematoma (1.4%), scrotal hematoma (0.7%) andseroma (0.7%). Other complications: ileus (2.8%), kidney failure(1.4%), pulmonary infection (2.1%), digestive hemorrhage (1.4%)and peptic ulcer perforation (0.7%). 30-day mortality rate was 4,9%
Fig. 1: Small bowel after reduction of strangulated hernia.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S44

Hernia (2011) 15 (Suppl 2): S37-S66 S45
(seven cases). Between deads, all patients had ≥ 66 years old, 42.8%had bowel resection, 85.7% an ASA score ≥ III and one died in thefollow up period for bowel necrosis missed at the surgery. The meanhospitalization time was 4.41 days (1-39 days).The high morbidity (14%) and mortality (4.9%) is associated with age,coexisting diseases and ASA score, and strangulated hernia. In thisstudy, the rate of strangulated hernia and consequently the need of bowelresection was significant and affected the prognosis. Elective herniarepair should be done as soon as possible avoid emergency repair.
P-025Trabucco technique in the treatment of inguinal herniasin our centerV. Pejcic, M. Djordjevic, S. Jovanovic, T. Bojic, D. Bogdanovic,A. Pavlovic, B. JovanovicClinical Center Nis, Center For Minimally Invasive Surgery, Nis,Serbia
Objectives: Trabucco technique is suturless preshaped mesh hernio-plasty. The procedure has been successful ever since introduced. Theaim is to show results using this technique in the patients operatedfrom 2001-2010. Material and methods: Prospectively, we analyzed 1,297 patients(ASA I-III) with primary or recurrent unilateral or bilateral groinhernia (Nyhus III-IV) that underwent this repair. We analyzed choiceof anesthesia, operating time, postoperative complications, the needfor analgesics, hospitalization time and time before returning towork. Results: Median age was 59 (21-70). They were 1,172 male and125 female patients. Regional anesthesia was used in 363 (28.02%)and local in 934 (72.97%) cases. The average operating time was29 minutes (16-50 minutes). Postoperative complications were notedin 38 (3.06%) patients (28 seromas and 12 hematomas), all treated conservatively. Average hospitalization period was 10 (5-17) hours.261 (25.96%) patients needed analgesics postoperativly. Patientsreturned to work after 7 days (5-13 days). There was 10 recurrencein postoperative follow up after 6-120 months. Conclusions: Trabucco’s hernioplasty is safe and efficient method inthe treatment of inguinal hernias. Minimal operative trauma and tissue dissection, small size of prosthetic material used, reduction inpostoperative pain (sutureless method) and early return to workingactivities makes this method in our opinion a method of choice inthe treatment of inguinal hernias.
P-026Transinguinal preperitoneal (TIPP) repair with amemory ring mesh for bilateral inguinal hernias;feasibility and efficiencyS. Apostolidis1, A. Zatagias1, I. Andreadis2, O. Tsiripidis21 Euromedica Kyanous Stavros Hospital, Surgical Department,Thessaloniki, Greece; 2 Ptolemaida General Hospital, SurgicalDepartment, Ptolemaida, Greece
Background: Currently the preperitoneal space is believed to be theideal place for inguinal hernia mesh repairs. The transinguinal preperi-toneal technique is an already proven effective repair for unilateralinguinal hernias, with results comparable to the open anterior onlayand laparoscopic repairs. The feasibility and efficiency of the tech-nique is discussed regarding the simultaneous bilateral herniarepair.
Methods: between September 2007 and September 2010, 114 elec-tive bilateral hernia repairs were performed (228 procedures in total).Data concerning the operative time, intraoperative complications,postoperative pain score, hospital stay, postoperative complications,time to return to normal activities and work, chronic groin pain andrecurrences were analyzed. Results: in a follow-up period of 3 to 36 months, the recurrence raterecorded was 1.31% (3 recurrences out of 228 repairs). There wereno intraoperative complications and only minor postoperative compli-cations, such as a case of urine retention, 4 subcutaneous haematomasand one larger preperitoneal haematoma. The mean operative time was85 min for both procedures. The pain score was low (VAS was at 0.8at the first 3 months); there were no cases of chronic groin painrecorded during the follow up period. All patients had an early returnto their everyday activities and work. Conclusions: the transinguinal preperitoneal technique is an easilyfeasible and very efficient repair for the simultaneous treatment ofbilateral inguinal hernias. It combines the benefit of the open ante-rior approach with the preperitoneal placement of the mesh, andthus highly recommended for the treatment of bilateral inguinal hernias.
P-027Polysoft® patch and Modified Kugel® patch: Which isthe best inguinal herniorrhaphy of transinguinalpreperitoneal technique (TIPP)?F.M. Mihara, Y.M. EdamotoNational Center of Global Health and Medicice, Surgery, Tokyo,Japan
Background: Problems after inguinal herniorrhaphy are known asseroma, neuralgia, and chronic pain. Berrevoet mentioned that thetransinguinal preperitoneal technique (TIPP) using the patch withmemory ring is considered to be better than the conventional tech-nique. In Japan, Modified Kugel® patch repair (MK) has been famil-iar as TIPP like Polysoft® patch (PP). We reported the acceptableresults of MK methods in the congress of European Hernia societybefore. But nobody report which technique is better for patients. Weinvestigated the short-term results between Polysoft® patch andModified Kugel® patch as TIPP. Patients and method: 217 inguinal herniorrhaphies were performedin 186 consecutive patients from 2009/4/1 to 2010/11/30 in our hos-pital. Case of emergency, age ≤ 18, or bilateral hernias wereexcluded. We selected one hundred of 146 patients for a prospectiveanalysis. Ages, BMI, classification of hernias, operating time, post-operative complication, hernia recurrence, and days of pain-killerrequirement were recorded. Results: Of the 146 patients, 49 (33.6%) were underwent modifiedKugel® patch repair (Group MK), and 51 (34.9%) were underwentPolysoft® patch repair (Group PP). There was no significant differ-ence between the groups in terms of age, BMI or distribution of hernia classification. The median operating time did not differbetween the groups, in Group MK 27 min. (23-58), in Group PP33 min. (21-74). Seroma as only postoperative complication occurredin 3 (6.5%) patients in Group PP and one (2.2%) in Group MK.There was no significant difference statistically. The mean postoper-ative days of pain-killer requirement were 1.8 days in group PP(0-7) and 1.7 days in Group MK (0-10). No recurrence was foundin both groups during the study period. Conclusion: Polysoft® patch showed equal safety and efficacy tomodified Kugel® patch in terms of short-term results. Evaluation oflong-term outcomes including chronic pain and the quality of life isrequired.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S45

S46 Hernia (2011) 15 (Suppl 2): S37-S66
P-028PHS, UHS and 3DP devices in the inguinal herniarepair in ambulatory surgery conditionsD. Dabic, B. Maric, V. Perunicic, N. PijanovicDepartment of Surgery, General Hospital Cacak, General surgery,Cacak, Serbia
Background: Applications of diversity prosthetic material and meshof different construction are opening a new chapter in hernia surgery,while tension -free techniques are becoming a “golden standard” forsolving abdominal wall defects.The aim of this retrospective analysisis to present the results of using PHS, UHS and 3DP devices in theinguinal hernia repair in ambulatory surgery conditions. Methods: From May 2006 to September 2010, 220 patients wereoperated on because of inguinal hernia under local infiltrative anaes-thesia. We used above mentioned devices having taken acountRutkow-Robbins modification of the Glbert classification. 125 wereoperated on by using PHS, 73 with UHS and 22 of them got 3DPmesh. The mean follow up was 28 months. We analyzed preopera-tive settings with demographic data, type of anaesthetic, operatingtime, hernia aperture diameter, hospital stay and complications. Results: All the operation were performed by the same surgeon inambulatory surgery conditions. The mean diameter of hernia apertrurewas 2.8 cm (range 1-4). The mean operating time was 29 minutes(range 22-38). The mean hospital stay was 2.2 hours (range 2-3).The incidence of infection, chronic pain and recurrence was 0%.There were no reasons for urinary cateters. 7 patients had complica-tions: 4 seromas and 3 haemathomas. One patient required instrumen-tal evacuation of the haemathoma at the day surgery unit, while theothers were solved through spontaneus haemathoma resorption. Conclusion: Herniorraphy is a simple and effective method andfrom the author point of view PHS, UHS and 3DP devices inoutpatient surgery gave excellent results with short hospital stay,fast recovery, minor complications and fast return to work andnormal activity.
P-029Experience in inguinal hernia repair as Day Surgeryusing the Prolene Hernia System (PHS). Analysis of1,840 cases with 5 years follow-upF. Docobo Durántez, J.A. Navas Cuellar, J. Mena Robles,A.G. Jimenez Riera, J.M. Suarez Grau, F.J. Padillo RuizUniversity Hospital Virgen del Rocio, Day Surgery Unit, Seville, Spain
Background: To evaluate long-term feasibility and benefits ofinguinal hernia repair with Prolene Hernia System (PHS) using localanesthesia with sedation as a Day Surgery procedure. Methods: 2,138 patients with inguinal hernia were treated in the daysurgery unit (1997-2005), with 1,840 cases (86.06%) having a min-imum follow-up of 5 years. Distribution for sex: women 7.98% andmen 92.02%. Mean age: 56 years (18-82). According to Gilbert’sclassification: 15 (0.81%) type I, 49 (2.66%) type II, 736 (40%) typeIII, 939 (51.03%) type IV, and 101 (5.48%) type V. Primary hernias1692 (91.95%), and recurrent hernias 148 (8.05%). Local anesthesiawas a mixture of lidocaine and bupivacaine with adrenaline. Postoperative pain was assessed using analogical visual scale pain.Mild and moderate postoperative pain was managed with simpleanalgesics. Patients were discharged at 6 hours, and postoperativecontrols were at 30 days, 3 months and 5 years by phone call. Results: Anesthetic technique employed was local in 1793 (97.44%),regional in 45 (2.44%) and general in 2 (0.1%). Mean operation timewas 40 min (range, 30-80). Overall stay was 5-8 hours (mean6 hours). Operations were performed by staff in 838 cases (45.54%),by residents in 1,002 cases (54.45%). Postoperative pain: mild (2-4points) in 580 cases (31.52%), moderate (4-6 points) in 994 cases
(54.02%), severe (6-8 points) in 266 cases (14.45%). 10 (0.54%)patients return to the hospital: 7 (0.38%) patients due to surgicalwound hematoma, 3 (0.16%) to wound infection. 5 year-follow upresults revealed complete cure in 1,824 patients (99.13 %), cure withsequelae in 6 (0.32%) and hernia recidive in 10 (0.54%). Conclusion(s): Inguinal hernia repair with PHS performed underlocal anesthesia on a Day Surgery unit is a safe and feasible proce-dure with excellent long time results.
P-030Analysis of adult females who have undergone surgicalrepair of inguinal herniaY. Kurisu, S. Akagi, H. Sibamura, Y. Hayashidani, T. Tanaka,N. HayashidaniMazda Hospital, Department of Surgery, Hiroshima, Japan
Background: Inguinal hernia is less frequent among adult femalesthan in males, and its clinical features in adult females have not beencompletely clarified. Although mesh repair is a standard method forsurgical treatment of this disease in males, controversy exists overthe validity of this method in females. Non-mesh repair is oftenperformed in young patients with this disease. The aim of thisstudy was to analyze the clinical features of inguinal hernia inadult females, and to discuss the operative procedure for itstreatment. Method: In all, 619 adult patients (93 females and 526 males) withinguinal hernia who were surgically treated between January 2006and December 2010 were retrospectively analyzed with regard to age,hernia type, operative procedure for repair, postoperative complica-tions, and recurrence rate. Results: The slope of age distribution was gentler for adult femaleswith inguinal hernia than for males with the same disease. Indirecthernia and femoral hernia were predominant among females. In relatively young female patients with small inguinal hernia whohad undergone repair by internal inguinal ring suturing, recurrenceof the same type of hernia never occurred. In adult females,direct hernia was relatively rare, and mixed type hernia was morefrequent. The percentage of patients with complaints of discomfortwas low after repair with Polysoft hernia patch by preperitonealapproach. Conclusion: Internal inguinal ring suturing can be considered as astandard procedure for surgical repair of small indirect hernia.However, because some cases may develop femoral hernia, an oper-ative procedure that enables observation of the preperitoneal cavityand can reinforce the entire inguinal floor should be preferablyselected. Elderly thin females may complain of discomfort becausethe mesh-embedding scar plate is palpable. Repair with the Polysofthernia patch yielded favorable outcome when it was performed viathe preperitoneal approach.
P-031Pathological anatomy of hernia diseaseG. Amato1, G. Salamone1, G. Romano1, A. Agrusa1, V.A. Saladino1,G. Gulotta1, R. Bussani21 University of Palermo, General Surgery, Urgency, and OrganTransplantation, Palermo, Italy; 2 University of Trieste, Departmentof Pathological Anatomy and H, Trieste, Italy
The study of tissue specimens excised from 30 fresh male cadaverswith inguinal hernias demonstrated multiple histological changes:fibrohyaline degeneration of the myocytes, fatty dystrophy of themuscle fibers, inflammatory infiltration, venous congestion and veinfibrosis. The arterial structures showed sub-occlusion or even
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S46

Hernia (2011) 15 (Suppl 2): S37-S66 S47
complete obstruction due to medial hyperplasia. The nervous struc-tures demonstrated fibrotic degeneration, atrophy of the axons as wellas the thickening of the myelin sheath. The following consequences could be imagined regarding the possi-ble impact these damage have on the physiology and kinetics of thegroin: • Degenerative changes of motor nerves and thickened myelin sheathwhich have been seen, could be linked to the reduced motile activ-ity leading to muscle atrophy and, consequently, to a reduced contractile response (as a physiological barrier) to the visceralimpact when abdominal pressure arises.
• A decreased blood supply leading to ischemic degeneration of thegroin structures may represent the result of the artery sub occlu-sion or obstruction.
• Venous congestion, vein fibrosis and inflammatory infiltrate couldembody the outcome of a steady compressive effect exerted by theabdominal viscera to which follows tissue congestion and impairedmetabolism.
• Hyaline degeneration, fibrosis and fatty dystrophy of the musclefibers within the groin could be the result of the chronic, degen-erative changes to the vascular and nervous components seen inthat area. These multifactorial damages are probably amplified bythe effect of the visceral compression upon the lower abdominalwall.
All these findings could also explain the alterations of the collagenchains in the groin area evidenced by several scientists. In our opin-ion, the described results of the histological study in tissue border-ing the hernia opening could represent a further contribution inunderstanding the reasons of the multifactorial causes leading to theweakening of the inguinal area and to hernia protrusion.
P-032New methode of inguinal hernia repairV.V. Parshikov1, A.B. Baburin2, A.V. Samsonov2, V.A. Khodak2,V.V. Petrov2, A.A. Samsonov2, R.V. Romanov2, V.P. Gradusov21 Nizhny Novgorod State Medical Academy, Hospital Surgery, NizhnyNovgorod, Russian Federation; 2 Hospital 35, Nizhny Novgorod,Russian Federation
Background: The most reliable and modern variant of inguinal her-nia repair is Lichtenstein technique. However, becomes stronger onlya back wall of inguinal channel. But often forward wall inguinalchannel is presented only weak, destroyed aponeurosis an externalmuscle of abdomen, and inguinal ligament is flabby. Methods: With 2003 for 2010 was operated 860 patients withinguinal hernias. We developed and introduced in surgical practicethe new way of tension-free plastics on the basis of the Lichtensteinmethod, which comprises of itself the plastic of front and back wall
of the inguinal channel (2398527 RU patent). The comparative analy-sis of results of treatment of two groups of patients is carried out.In the basic group were included the patients, operated with appli-cation of named method. In the control group were included thepatients, operated by Lichtenstein technique. No significant differ-ences of a sex, age, indicators of clinical analyses, and sizes of hernial orifices were marked in both groups of patients. Dynamicsof the basic indicators of the postoperative period has been studiedby application of statistics methods. The life quality was studied withMOS SF-36. Results: Mortality was not. Suppurations were not observed. In control group 7.53% complications were noted, in the basic groupwere registered 2.22% complications. The life quality was very good.
Conclusion: Updating of Lichtenstein plastic, based on front andback wall of the inguinal channel strengthening with mesh, is ofinterest concerning increase of reliability of operation and prophy-laxis of relapses of hernias. Application of a new way does notincrease frequency of complications in near and last postoperativeperiod. The first experience has shown high efficiency plastics andnecessity of carrying out of the further researches.
P-033Evaluation of the introduction of laparoscopic inguinalhernia repair to a District General Hospital againstpredefined outcome measures and compare withpublished literatureR.M.S. Hammond, V. ChitreJames Paget University Hospital, General Surgery, Gorleston, UnitedKingdom
Aim: Evaluate the introduction of laparoscopic inguinal hernia repairto a District General Hospital against predefined outcome measuresand compare with published literature. Method:Medical records of patients undergoing a laparoscopic ingu-nial hernia repair between July 2005 and April 2008 were reviewedfor pre-defined outcome measures, including duration of surgery,operative complications, hospital stay, consent and thrombo-prophy-laxis. Results were compared with published literature. Results: There were 122 patients included. 95% were male, with anaverage age of 59.8 (17-83). All procedures were elective. 68 wereunilateral hernias and 34 were recurrent (32 unilateral). The average duration of surgery was 81.4 minutes (range 37-146).Duration varied between operators from an average of 62.7 minutes(n=24) to 116.5 minutes (n=6). A study of similar size had an aver-age duration of 77 minutes.
Fig. 1: Fibrotic degeneration of the myocytes - LGx190.
Fig. 1: 1-cut, 2-fat, 3-lig.inguin., 4-mesh, 5-funic., 6-musc.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S47

S48 Hernia (2011) 15 (Suppl 2): S37-S66
Seventy-one percent of patients were discharged on the same day.14.8% of patients had a complication, including groin pain (2.5%),haematoma (1.6%), infection (1.6%), port site hernia (1.5%), recur-rence (3.3%) and seroma (3.3%). There were no serious visceral orvascular injuries or mortalities. A Cochrane review found recurrencerates of 2.7% and six port site herniaes in the forty-one studiesreviewed. All patients had evidence of consent for the procedure. Twenty-three percent of patients had heparin prescribed and half ofthese had evidence of administration. Thirty-four percent had TEDstockings prescribed. The hospital standard is for all patients toreceive thrombo-prophylaxis unless contraindicated. Conclusion: This study demonstrates the successful introduction oflaparoscopic inguinal hernia repair to a District General Hospital.Results are comparable to published literature. A slightly higherrecurrence rate and port site hernia was noted. This study providesevidence that duration of surgery is operator dependent. All patients had evidence of consent. There were low rates of prescribing thromboprophylaxis for this pro-cedure.
P-034Complications of the inguinal hernia Surgery.Preventions and TreatmentsJ. Goderich Lalan1, E.J. Molina Fernandez21 Hospital Universitario Bruno Zayas, Cirugia, Santiago De Cuba,Cuba; 2 Hospital Universitario Fajardo, Cirugia, La Habana, Cuba
Background: Inguinal hernia is one of the most common conditionsthat need surgical treatment. Often local postoperative complicationsrelated to such surgical procedures arise.Objective: Characterize local postoperative complications of inguinalhernioplasties in several aspects and relation with the preventions.The extraordinary changes of this kind of surgery with the introduc-tion of a wide range of modern classifications and techniques ofmesh implants, make us plan new academic designs and think ofchanges in the policy of surgeons’ training. Methods: A descriptive study was carried out in order to character-ize local postoperative complications in 15,543 patients operated onbecause of inguinal hernia from 1994 to 2009 in the UniversityHospital “Dr. Juan Bruno Zayas Alfonso” of Santiago de Cubaand University Hospital “Comandante Fajardo” in Ciudad de laHabana. Results: 10.2% of the patients had local complications. Seromas(1.1%), oedema of the spermatic cord (1.0%) and infections (1.0%)were the more common early complications, but granuloma (3.3%)and recurrences (2.7%) were the more common late complications.Recurrences (2.0%) prevailed in procedures with bioprostheses,mainly in plug and patch techniques (6.3%) and Rives (4.3%). Themost common chronic complications of conventional techniques weregranulomas (5.2%) and recurrence (3.5%). The most common acutecomplications were seromas (1.6%), infections (1.4%) and theoedema of the spermatic cord (1.0%). Mc. Vay and Bassini tech-niques had more recurrences (9.2% and 7.6%). Most of the compli-cations took place in patients operated by expert surgeons, but thereis no doubt. Conclusions: Percentage of local complications was in a permissi-ble range. The most common local complications were recurrences,granuloma, seromas, oedema of the spermatic cord and infection ofthe surgical site. The surgical with less recurrences were: Lichtensteinand fascial overlapping. Most of the complications took place inpatients operated by expert surgeons.
P-035Five years results in modified plug-patch inguinalherniaJ. Massalis1, G. Efthymiou1, S. Stokidis1, P. Lambropoulos1,E. Pagoni2, J. Moysis1, P. Gkanas11 Surgery of Nafplion, Nafplion, Greece; 2 Anaesth. department ofNafplion, Greece
Aim: To evaluate the clinical results and complications of inguinalhernia with modified plug-patch repair in our hospital.Material and methods: 246 consecutive patients with inguinal her-nia were evaluated in five years period (2006-2011) retrospectivereview. All operations were done by three surgeons. A modified tech-nique using a plug and an onlay polypropylene patch was performedunder general anesthesia. One to three stiches was used to attach theplug to the tranverse fascia in order to prevent patch migration. Thenerves were routinely identified, registered and preserved. Patientswere evaluated for postoperative complications following observationin the outpatients clinic after 1, 4 and 24 weeks. Results: 218 patients operated electively and 28 operated as acutecases. The mean age of the patients was 63 years with male: femaleratio of 6.24:1 (212:34). Inguinal hernia was indirect in 143 (58.1%)patients, direct in 95 (38.6%) and “pantaloon hernia” in 8 patients(3.3%). Urinary retention was the commonest complication occurredin 6 (2.4%) patients. Wound hematoma observed in 5 (2.0%) casesall treated conservatively. 5 (2.0%) patients developed seroma mainlyrelated to the heavy polypropylene meshes utilized in the first yearof our study. 3 (1.2%) patients developed acute postoperative neu-ralgia and they reoperated within 48 h. We didn’t observe woundinfection observed. We didn’t diagnose any testicular atrophy and 10(4.0%) patients experienced hypaesthesia. All patients were dis-charged within 48 h after surgery. The average recovery time was12 days. No recurrences were recorded. Conclusion: The modified plug-patch technique is a safe and effec-tive procedure for inguinal hernia repair. The complications areacceptable in regard of the incidence of postoperative chronic pain.
P-036Moran - Combined soft tissue and prosthetic inguinalhernia repair. Operative tehnique and preliminaryresultsA. Gluhovic, R. Veljkovic, M. Protic, M. Korica, N. Beatovic,G. Pokusevski, D. Jovanovic, B. Rajkov, D. Bjelajac, D. PetrovicClinical centre Vojvodina, General surgery, Novi Sad, Serbia
Background: 3 years ago we introduced a new combined inguinalhernioplasty wich is based on anatomic reconstruction of posterioringuinal wall similar to Shouldice tehnique, with small prostheticpreperitoneal mesh (10x2,5 cm) reinforcement of transversalis fascia.Tehnique is autorised by Robert M. Moran from National Herniaambulatory surgery Insitute of Spain in 1999. In his series overall recu-rancy rate on 3,608 operated inguinal hernias, performed by 12 sur-geons, was only 0,39%. Method: The aim of this presentation is to show operative tehniquein “step by step” manner and our results. Results: In our institution, we operated 117 patients with this tehniquefor past 3 years. 81 patients were admitted in hospital and operatedin regional (41 pts) and general anesthesia (40 pts), and 36 patientswere operated in ambulatory surgery. 34 pts were admitted because ofincarceration, and operated in emergency surgery. The average oper-ation time was 37 min. All the admitted patients wented home at first
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S48

Hernia (2011) 15 (Suppl 2): S37-S66 S49
postoperative day, and reached full work recovery within 30 days. Onereccurency was noted only. Postoperative complications occured in justfew patients, and all of them were resolved conservatively. Conclusion: Our first experience with this operative tehnique is morethan excellent. The combination of anatomic reconstruction and pros-thetic preperitoneal mesh repair, in our opinion, seems to become awinning team in search for the ideal inguinal hernioplasty.
P-037Laparoscopic inguinal hernia repair IPOM: Feasibilityand advantagesG. Cesana, S. Olmi, E. CrocePoliclinico San Marco, Surgery, Zingonia - Osio Sotto, Italy
Background: Inguinal hernia repair by laparoscopic approach iscommonly performed by TEP or TAPP technique. The mesh is usu-ally placed in a retroperitoneal position and fixed by mechanicalclips. These procedures are quite long and complicated and manyauthors have shown that the training curve may be a serious issue.The IPOM (Intra Peritoneal Onlay Mesh) technique could be an inter-esting alternative, as this technique is much more easy and fast. Methods: From January 2003 to December 2010 we performed98 inguinal hernia repair procedures by laparoscopic approach(96 males, 2 female, mean age 60 years, mean weight 76 kgs), usingthe IPOM technique, using Parietex® Composite mesh (Sofradim -France) and fibrin glue (Tissucol - Baxter - USA and Quixil - Ethicon- USA) for mesh’s fixation. Results: Mean operative time was 10 minutes. Mean hernia diame-ter was 2.5 cm (±0.8 cm), 16 hernias were direct, 80 were indirectand 20 out of 96 were recurrent. We did not have to convert any ofthe laparoscopic procedures. The mean time of discharge was 1 day,the mean time of recovery for physical or working activities was5 days. With a mean follow-up of 36 months only 1.6% of thepatients showed hematoma at the trocar site; no additional compli-cation was reported, in particular no recurrence, no mesh migration,no occlusion no fistula was observed. Conclusion: IPOM is the easiest and fast hernia repair technique.This study shows that with the right material it is feasible withoutbig complications.
P-038Do Trans-inguino-preperitoneal repair reduce postoperative chronic pain and improve the QOL of thepatients?J.F. GillionHôpital Privé d'Antony, Antony, France
From June 2008 to December 2010, 525 patients (482 M, 43 F), aged59±15 (range 18-96) years old, BMI 25±3 (range 17-43) had TIPPrepair for treatment of 622 hernias, 605 primary hernias and 17 recur-rent hernias. The mesh (496 Polysoft medium and 126 large) wasinserted in the preperitoneal space, far from the three inguinal nerves,otherwise preserved thanks to the reduced premuscular dissection: Iliohypogastic n. was transected in only 9 cases. Genital branch was pre-served keeping it along the external spermatic vessels, intentionallynot mobilized. The ilio inguinal n., transected in 22 cases, was pre-
served in all others cases. The mean operative time was 37±11 mn(range 15-120). No patient dies. Post operative complications occurredin 27 groins (4%), minor in 24 cases and 3 leading to a redo: 2 meshesexplanted. Sixty percent of our patients were treated as day-case sur-gery, increasing to 70% in 2010. At D8, the mean VAS was 1/10 (0-8). At D30, VAS up to 2/10 was found in only 14 (2.5%) of the 549examined groins. All patients followed more than three months weresent a QOL questionnaire, similar to that they filled in the pre oper-ative period. The results of the entire series will be presented. At thismoment the results are known for the first 143 patients (170 hernias)of the cohort: No recurrence and no severe pain (need for a referralto a pain center) occurred. Two patients have pain, they assess asimportant, and 25 as a light pain. Only one of these patients consid-ers his impairment as more troublesome than the hernia he had before. Conclusion: TIPP repair seems to reduce post operative chronic painand improve the QOL of the patients. Randomized studies areneeded.
P-039Modified grid iron, (F. Ugahary), hernioplastie, using anew self expandable prosthesis. The really minimalinvasive preperitoneale approach: Review, resultsM. SolerClinique Saint Jean, Chirurgie, Cagnes Sur Mer, France
Background: After the first pionners, L. Nyhus achieved acceptanceof the preperitoneal approach in the sixties. R. Stoppa published thefist tension- free and sutureless hernia repair using a posteriorpreperitoneal approach. G. E. Wantz tried to develop in an ambula-tory setting, with local anesthésia, unilateral GPRVS for the treat-ment of complex hernias. F. Ugahary performed a unilateral preperitoneal technic to make pos-sible the G. Wantz and R Stoppa project and to treat complex anddifficult hernias with an open minimally invasive approach. Methods: The autor show the grid iron technique, and insist about: • The position of the small skin incision with anatomical landmarks-skin, the absence of nerves dissection or contact.
• The extend of the dissection in the pre peritoneal space, with asimple but specific divices.
• The procedure to treat the hernia sac, and to realise the parietal-ization of the cord.
• The structure of the new mesh used, with the rigid ring, that givethe self expandable effect to the prosthesis, that make easier theplacement of the mesh in the good position.
Results:One monocentric study, with 1,200 hernias, (1,068 patients). Anesthesia: Ilio-inguinal block: 55%, Spinal: 42%, General: 3% Hostitalisation: Day surgery: 70, 2%; Complications: Hematoma, n=30, (no intervention); Deep infection:n=1, (with the necessity to remove the mesh); severe pain before3 months: n=8 Recurrence rate: 1. 7%. No severe chronic pain after 3 months. Conclusion: This prepitoneal approach permits a minimal invasivetension free and sutureless procedure, with protection for the nerves.The use of the new self expandable prosthesis make easier the tech-nique and secure the good position of the mesh, specially for the bigmedial hernia. The reccurence rate is low. But the specific result of the study is the absence of severe chronicpain after 3 months.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S49

S50 Hernia (2011) 15 (Suppl 2): S37-S66
P-040Delayed and late mesh infections after inguinal herniarepairD. Galun, M. Milicevic, P. Bulajic, D. Basaric, I. Palibrk, M. ZuvelaFirst Surgical Clinic, Clinical center of Serbia, HPB and livertransplant unit, Beograd, Serbia
Background: The analysis of delayed or late mesh infections fol-lowing inguinal hernioplasty and methods for their solution. Methods: Between January 2004 - January 2011 fourteen patientswere operated on for delayed or late mesh infection followinginguinal hernioplasty - 11 deep incisional infections (9 followingLichtenstein and 2 PHS hernioplasty) and 3 organ/space infections(after PHS herniplasty). Eleven deep incisional infections and 1 of3 organ/space infections were preceded by an early mesh infection.Organ/space infections manifesting 6 and 7 years after the operationwere caused by: underlay PHS patch contact with appendix causingfistula in 2 patients, and with sygmoid colon in 1 patient. The reop-eration included: total mesh excision, McVay herniorrhaphy withdrainage, and additional procedures for intestine fistulas (appendec-tomy in 2 patients; the sygmoid colon fistula suturing and left hem-icastration followed by midline laparotomy and protective ileostomyin 1 patient). Operative difficulties occurred in 2 patients with PHSinfection: one due to close contact of femoral artery with underlayPHS patch and one due to bleeding caused by lesion of femoral veinduring underlay PHS patch excision. Results: Mean time between hernioplasty and reoperation was31.4 months (4-60) for patients with deep incisonal infection and77.7 months (72-84) for patients with organ/space infection. Twowound infections, 3 testicle complications (2 atrophy and 1 testicleremoval) and 1 hernia recurrence occurred during a mean follow-upof 28 months (1-84). Conclusion: Delayed or late mesh infection following inguinal hernio-plasty is deep incisional or organ/space infection. In our series, deepincisional infection was preceded by an early mesh infection causedby bacterial contamination during Lichtenstein and PHS hernioplasty.Organ/space infection occurring long after PHS hernioplasty andcaused by contact underlay patch and intestines is more challengingdue to closeness of underlay PHS patch and blood vessels.
P-041CONTACT mesh for Lichtenstein hernia repair:Quality of life and incorporation compared to Ultrapromesh – a matched pair analysisL.R. Ladurner, T.M. Mussack, U.L. LinsenmaierKlinikum der Universität München, Surgery Innenstadt, Munich,Germany
Background: The CONTACT mesh for inguinal hernia repair is apolyester multifilament mesh. The three-dimensional “honeycomb”knitted structure with “grips” allows mesh placement without additional mesh fixation. However, it is still unclear whetherthese properties might influence the mid-term clinical course aftersurgery. The objective of this prospective study was to compare theCONTACT mesh with a Ultrapro mesh for Lichtenstein inguinal hernia repair in terms of quality of life (QL) and morphologicalincorporation shown by functional magnetic resonance imaging(MRI). Methods: Up to now, 15 patients (14 male, 1 female; mean age,56 years [range 33-81]), who underwent day-case Lichtenstein repair,were enrolled. According to the EHS Groin Hernia classification,
hernias were rated as type L2 (n=7), L3 (n=4), M2 (n=3) and M3(n=1). The second group, who was matched for age, gender and typeof hernia, received polyglecaprone-polypropylene (PP) meshes(Ultrapro). QL was assessed by Visual Analogue Scale (VAS), dur-ing the first 14 days, and by SF-36 Health Survey at one and3 months after surgery. Groin morphology was evaluated by cine1.5T MRI, using transverse T2-weighted FISP sequences. Results: Operation time and hours until discharge were not differ-ent in both groups. The CONTACT group showed lower VAS scoresthan the PP group for the first 4 days. The SF-36 values were iden-tical, and reached the norm values for the age-stratified German normpopulation after 1 and 3 months. Cine MRI revealed a completeincorporation of both meshes over time. Conclusions: During the first 4 days after surgery, CONTACT meshfor Lichtenstein repair performed slightly superior to Ultrapro meshwith respect to postoperative pain. Concerning mid-term QL, it hasproven to be equal to PP mesh.
P-042Component separation technique with the use of tissueseparating mesh is sufficient to treat complex largeincisional hernias with loss of domainF. Berrevoet, A. Vanlander, B. De Smet, X. Rogiers, P. Smeets,R. TroisiUniversity Hospital Ghent, General and Hepatobiliary surgery,Ghent, Belgium
Background: Giant primary or recurrent incisional hernias stillremain an enormous challenge for adequate surgical repair. Recently,calculation of both hernia sac volume and abdominal cavity volumewas reported to evaluate the need for additional techniques as pro-gressive pneumoperitoneum to treat these hernias. Our aim was totest this hypothesis and see which volume reduction was still feasi-ble using component separation techniques (CST) and intra-abdom-inal mesh repair. Methods: All patients treated from January 2007 till July 2010 wereevaluated prior to this analysis. Patients which were treated withintra-abdominal mesh placement and CST were selected for review-ing and CT calculation of both hernia sac (HSV) and abdominal cav-ity volume (ACV). Volume reduction (VR) was calculated asHSV/ACV. All patients had pre- and postoperative CT evaluation.Postoperative morbidity as well as midterm recurrence rates wereevaluated. Approval of the Ethical Committee of the UniversityHospital Ghent was obtained. Results: During a 3.5 year period 28 patients were treated usingthis technique. The mean HSV was 1,166 cm3, the mean ACVwas 6,207 cm3, while the mean VR was 20%. In all patients meshaugmentation was possible, no patients had bridging of the defect.Morbidity mainly consisted of seroma (n=24; only 8 aspirated),superficial wound infections in 8 patients, while 3 patients hadto be admitted at the ICU for respiratory support after herniareduction. Mean hospital stay was 12 days (range 7 to 22 days). Themedian follow-up was 20 months with only 1 recurrence. Conclusion: Combination of an intraperitoneal composite meshrepair with adequate fascia elongation using CST, offers a solidsolution in repairing incisional hernias with loss of domain, upto 36% of volume reduction. Further studies need to estimate thecut-off value for using additional techniques in cases of loss ofdomain.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S50

Hernia (2011) 15 (Suppl 2): S37-S66 S51
P-043Non invasive measurement of advanced glycationendproducts: a new risk factor for incisional herniaformation? J.J. Harlaar1, K.A. Vakalopoulos1, H.H. Eker1, M. Castro Cabezas2,W. Hop1, A.C. Van der Ham2, J. Jeekel1, W.W. Vrijland2, J.F. Lange11 Erasmus University Medical Center, Surgery, Rotterdam,Netherlands; 2 Sint Franciscus Gasthuis, Internal medicine,Rotterdam, Netherlands
Background: Incisional hernia is a frequent complications of abdom-inal surgery, although an individual risk factor is lacking. The physiological formation of ‘advanced glycosylation endproducts’(AGEs) during aging is the result of non enzymatic synthesis of sugarwith free amino acids, lipids or nucliacids. These AGE’s also knownas non enzymatic collagen cross links are correlated with hyper-glycemia, hyperlipidemia and oxidative stress on connective tissueof the entire body. Studies have shown that there is a relation between AGE indirectlymeasured with auto fluorescence in the skin and the progression ofdiabetes, arteriosclerosis and end stage renal failure. Non invasive measurement of skin autofluorescence of AGEs in theskin with the AGE reader™ was an opportunity to investigate therelation between AGEs and incisional hernia. Methods: 18 patients with incisional hernia after midline incisionand 16 patients with no clinical diagnostically incisional hernia aftermidline incision were compared in a case-control study on autoflu-orescence in the skin of the underarm. Patients were matched forage. Data was analyzed with multiple regression. Results: There was a significant difference (p=0,020 t-test) inAGEs (measured in autofluoresence AF) between incisional herniapatients (mean 2,84 AF ± 0,12 [sem]) and normal healed patients(2,46 AF ± 0,10 [sem]). Corrected for AGE, sex and time betweenoperation and measurement the difference was 0.36 AF (95%CI: 0.05-0.67; p=0.024, multiple regression). There was no signifi-cant difference between ASA class, cardiovascular disease and dia-betes between both groups.
Conclusion: AGE accumulation measured in the skin, indirectlymeasured with autofluorescence, may be a risk factor for the devel-opment of incisional hernia. Prospective trials should confirm thisdata, to select high risk patients for tailor made clinical approach.
P-044Laparoscopic transperitoneal sublay repair of ventraland incisional hernias with large meshesW.M.J. Reinpold, M. SchröderGross Sand Hospital Hamburg, Surgery, Hamburg, Germany
Background: Laparoscopic IPOM repair and open sublay repair areboth established techniques for the cure of ventral and incisional her-nias. The advantages of minimal access surgery are evident. However,direct contact of standard alloplastic polypropylene and polyesterprosthesis with the bowel has to be avoided due to a high risk ofadhesions and fistula formation. The IPOM-technique is nowadaysperformed with meshes whose bowel facing side is covered with alayer of adhesion preventing material. Methods: We developed a laparoscopic transperitoneal sublay repair(LTSR) technique. In 102 small and medium size ventral hernias weused the laparoscopic sublay approach with standard polypropylenemesh. In 5 cases we used self fixating meshes. In 52 cases weimplanted large pieces of mesh (25x20 cm up to 30x20 cm) via aleft flank 3 port approach. The main steps are: 1) diagnosticlaparoscopy and adhesiolysis, 2) left lateral vertical incision of theperitoneum and posterior rectus sheath, 3) laparoscopic mobilisationof the hernia sac and peritoneum, 4) suture closure of the herniadefect, 5) retromuscular or preperitoneal mesh placement and suturefixation, 6) laparoscopic closure of the peritoneum. In all cases themesh was completely covered by peritoneum. Results: There was one early postoperative ileus which was treatedlaparoscopically and two hematomas that were treated conservatively.The medium follow-up of 81 patients (79%) is 23 months (2 to37 months). Up to now there is no recurrence. Seven patients reportminor discomfort or pain. Conclusion: Laparoscopic sublay repair combines the advantages ofthe laparoscopic IPOM technique and open sublay repair. In ourhands it is a technical demanding but save alternative procedure forthe repair of small and medium size ventral hernias.
P-045Usefulness of mesh reinforcement in Lázaro da Silvatechnique for abdominal wall reconstruction: the pilotof a prospective randomized trialR.M. Melo1, R.N. Tomas2, F.A.S. Penhavel1, C.E.S. Gontijo11 Federal University of Goias, Surgery, Goiania, Brazil; 2 Santa Casa deMisericordia de Goiania, Surgery - Abdominal Wall, Goiania, Go, Brazil
Background: Abdominal wall reconstruction in complex incisionalhernias remains a challenge for surgeons and for patients too. Tensionfree mesh repair has decreased recurrence rates, but the resulting fibro-sis is function-free as well. Indeed, the conventional or heavy-weightmesh related problems may be very difficult to deal. On the other hand,pure tissue repair are physiologically sound through muscle flaps(active or dynamic support), but it is associated with more recurrences.Coupling the advantages of two procedures, without the disadvantagesof each one, may be attractive with fewer side effects using a light-weight mesh. This is a pilot study to investigate if combined techniquefor complex midline incisional hernia repair using the Lázaro da Silvaprocedure, reinforced by mesh, can determine fewer recurrences. Methods: A prospective randomized trial will be conducted. Afterthe informed consent acceptance, all adult patients with large mid-line incisional hernia (10 cm width), irrespective of the time elapsedfrom the first/last operation will be elected for the trial. They willbe operated on by the same surgeon through Lázaro da Silva tech-nique with or without mesh reinforcement (fig. 1). The mesh shouldbe manufactured with polypropylene (PP) or polyvinylidene fluoride(PVDF) monofilament and must show a minimum effective porosity
Fig. 1: Autofluorescence of AGE’s versus age in years.
Age in years
Incisional herniaNon hernia
Autofluorescence of AGE’s versus age in years
AGEs
(AF)
4.0
3.5
3.0
2.5
2.0
1.5
1.050 60 70 80 90
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S51

S52 Hernia (2011) 15 (Suppl 2): S37-S66
of 20%. All patients will be evaluated after one month, to detect anylocal complications, and up to five years postoperatively by a sec-ond surgeon in search of recurrence. Results:We have operated on 10 patients in this pilot study and pre-liminary results shows only one case of surgical site infection whodeserved debridement with removing a central piece of the mesh, butno one had recurrence up to now. Conclusion: Combining both strategies (tissue + mesh repair) maybe suitable to restore the anatomy and the physiology of the abdom-inal wall, and to reinforce it simultaneously.
P-047Components separation technique, mass modificationvs rives sublay techique in the treatment of largeincisional midline herniasA. Antic, D. Galun, M. ZuvelaFirst Surgical Clinic, Clinical center of Serbia, HPB and livertransplant unit, Beograd, Serbia
Background: There is no “gold standard” for the surgical treatmentof large abdominal wall defects. Size, site, relative or absolute lackof viable tissue and degree of contamination are determinants for thechoice of surgical procedure. The aim of the study is to compare twodifferent operative techniques - Rives and Components SeparationTechnique (CST) in the treatment of large incisional midline hernias. Methods: A prospective study included 60 patients with large (diam-eter > 10 cm) incisional midline hernias without signs of local infec-tion, randomized in two groups, with 12 months follow up. Bothgroups “Rives” and “CST Mass modification” group consisted of30 pts. Operative wound infection was exclusion criteria in bothgroups. Demographic data, co-morbidities, body/mass index, datarelated to hernia, operative details and complications were analyzed. Results: No differences were found in demographic data, morbidityand size of the hernia defect. There was no intra-hospital mortality. In the “Rives” group seroma was in 2 and hematoma in 1 patient.Two patients had infection of prosthetic material and were re-oper-ated (total excision of mesh and CST in one patient and partial exci-sion of the mesh in other patient). One patient had chronic pain. In“CST” group seroma was in 2, hematoma in 1, wound infection in2, skin necrosis in 1 and recurrence in 2 patients. Recurrences werereported 6 months after the operation in the average, in upper partof operative incision, and were small in diameter (2-3 cm), withoutsignificant cosmetic effect, and were treated with simple suture. Conclusion: The prosthetic material repair is associated with lessrecurrence, but infection of the mesh may require re-operation.Despite of larger percentage of recurrences, CST remains feasibleprocedure with good functional and cosmetic results while majorityof recurrent hernias are asymptomatic and does not require furthertreatment.
P-048Ten years of experience in laparoscopic ventral herniarepair: Learned lessonsR. Fernandez Lobato, F.J. Angulo Morales, J. Garcia Septiem,F.J. Marin Lucas, M. Limones EstebanHospital U. Puerta de Hierro-Majadahonda, General Surgery,Madrid, Spain
Introduction: Ventral hernia laparoscopic repair is being consideredin last years as “gold standard” repair by good results in some cases. We present lessons learned by experience in ventral hernia repair bylaparoscopic approach along ten years. Patients and methods: We performed laparoscopic repair in 245patients (1999-2010) with incisional hernia (IH) and primary hernias(PH) bigger than 3 cm in obese patients or associated procedure.Abdominal cavity access was performed by Hasson trocar (10 c) inthe left side and 1 or 2, 5 mm working port. PTFEe Dual-Mesh with holes (Gore-Tex??-USA) is used and fixedwith helicoidally-stapled double-crown. No drains. Tight bandageused during 1 month. Results: 245 Patients: female (123)/male (122). 65% with BMI>30.Average age 55.6 years (range 15-84). Location of PH: 64 (27%),IH: 185 (73%) and recurrent 13%. Adhesiolysis was performed in78%. Conversion to open surgery: 7 (2.8%). Associated surgery: IH(13%) and PH (22.8%). Mean operative time: PH 56 min / IH 95 min. Size of the meshplaced during years of study are analyzed. Mean hospital stay: IH(2.5 days) and PH (1.4 days), and less than 48 hours in 59 and 79%respectively. Postoperative local morbidity: 4.8% (infection 1.6%) and generalmorbidity: 7%. Follow-up: Recurrences: 11 (4.5%) and site Hassonhernias (3 c). Learned lessons and modifications in the technique: 1. Use of optical port to avoiding trocar hernias 2. Bigger mesh size with 6 cm to overlap to avoiding recurrences 3. Use of 4 transabdominal sutures tied in subcutaneous tissue toimproved correct position and mesh fixation.
4. Fibrin glue applied into the sac, with reduction of appearance theseroma.
Conclusions:Abdominal hernia laparoscopic repair is safe and effec-tive, with good results. Lessons learned by expertise have improvedthe technique and results, avoiding seroma, reducing recurrences andtrocar hernias.
P-049New principal in incisional hernia repair: Thescaffolding sutureA. Doka, I. Smith, M. KassaiMonklands Hospital, General Surgery, Airdrie, United Kingdom
Background: One of the main reasons for failure in case of meshrepair of the incisional hernia is mesh migration. This may happenearly in the postoperative period due to poor fixation and/or bulging.Bulging occurs when increased intra-abdominal pressure is opposedby inadequate resistance around the hernial ring. This causes themesh to migrate into the existing hernial sac. This may dislodge thefixing tacks or stitches. Methods: We employ a technique of placing a #1 nylon suture in acriss-cross fashion across the defect to divide the space up to smallerareas. The aim is to create a net or scaffolding made out of thatsuture which supports the mesh, allowing it to withstand the intra-abdominal pressure without bulging. We maintain the tension-freeprincipal by tightening the suture only enough to support the meshwith no undue tension to the defect itself.
Fig. 1: Lazaro da Silva procedure.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S52

Hernia (2011) 15 (Suppl 2): S37-S66 S53
Results: 13 patients have undergone surgery since May 2009. Thetechnique was used in 5 open cases (3 in midline scars, 1 at a pre-vious ileostomy site and 1 during a redo parastomal hernia repair)and 8 laparoscopic cases (1 hernia at Pfannenstiel incision, 1 at aprevious ileostomy site, 1 in midline scars and 5 parastomal hernias).No significant intra or postoperative complication has been recorded.Average hospital stay was 2.2 days. Average BMI was 24.5. Follow-up ranged from 1 to 20 months (median: 7 months). No recurrencehas been identified. Conclusions: Our initial results suggest that a supportive “scaffold-ing suture” is safe and effective. At this stage, the minimum defect size where this reinforcement isadvisable is unknown. However, we believe that patients with largerdefects are most likely to benefit.
P-050The Abdoman®: A new model for research onabdominal wall suturing and mesh fixation techniquesJ.J. Harlaar1, E.B. Deerenberg1, R.H.M. Goossens2,E. Van Breemen2, P. Kandachar2, J. Jeekel1, G.J. Kleinrensink1,J.F. Lange11 Erasmus University Medical Center, Surgery, Rotterdam,Netherlands; 2 Technical University of Delft, Industrial design,Medisign, Delft, Netherlands
Introduction: The midline incision is the most frequently used approachto create an entrance in the abdomi¬nal cavity during abdominal sur-gery. The most common complication of abdominal surgery is the inci-sional hernia despite ongoing clinical and experimental research on lineaalba suturing. Even after mesh implantation recurrent hernias are fre-quent. A validated biomechanical model for the evaluation of differentsuture techniques of abdominal wall closure and mesh fixation has notyet been created. To gain better understanding of the biomechanics ofthe abdominal wall in relation to suture techniques and meshes, theAbdoman® project was developed. Methods: The aim of the Abdoman® project was to create a dynamicartificial abdominal wall that can simulate rises in intra-abdominalpressure, including coughing and post-operative ileus, to observe theeffects on suture techniques of the linea alba and mesh-fixation tech-
niques. A co-operation between the Technical University of Delft andthe Erasmus University Medical Center Rotterdam was establishedto develop this device. Results: In the Abdoman®, software is implemented to operate six inde-pendent pneumatic muscles that model the movements of the differentabdominal muscles. It can simulate different types of post-operative elevations of intra-abdominal pressure, for example repetitive coughingwith high peaks of intra-abdominal pressure or a continuous elevationcaused by an ileus. During the experiments video recording equipmentprovides visual feedback and quantitative data is collected bysensors and stored in a database. First experimental data will be pre-sented. Conclusion: The Abdoman® is an innovative model for research inabdominal wall surgery. It is a useful model that can be used toinvestigate different linea alba suture techniques and mesh fixationtechniques. In the future the Abdoman® can be used as a trainingtool for surgical residents.
P-051Cost analysis of wound complications after ventralhernia repairV.B. Tsirline, D.A. Klima, K.T. Dacey, I. Belyansky, S.B. Getz,A.E. Lincourt, B.T. HenifordCarolinas Medical Center, GI/MIS Surgery, Charlotte, United Statesof America
Background: Ventral hernia repair (VHR) is a common operationwith over 100,000 cases performed in US annually. Cellulitis, woundinfection, and breakdown occur in 20-50% of cases. Diagnosis, treat-ment, and prevention are extensively studied, but cost is rarelyreported. Methods: We reviewed all VHRs by our service from 2007 to 2010,including first year postoperative visits. Patients with documentedwound complications were compared to those without postoperativeproblems. Patients with other major non-wound related complicationswere excluded from both groups. Results: 679 cases met inclusion criteria, 140 (20.1%) had any form ofwound complication. Demographics were similar between groups.Patients with wound complications had longer hospital stay (average±SD8.0±5.8 vs 5.0±3.7 days), higher hospital charges ($56,000±$42,000 vs$36,000±$24,382), and median of 7 vs 2 postoperative visits (p<0.0001all comparisons). Average outpatient cost of wound complication was$9,900 compared to $289 without complications (p<0.0001, differenceCI95% $8,000-$11,300). Laparoscopic repairs had fewer wound complications 6.5% vs 24.2% open (p<0.0001), with annual outpatientcare cost of $3,300 vs $388 without complications (p=0.002). In multivariate analysis, wound complications had predominant effect onhospital and follow-up charges. There were no significant differences inhospital or outpatient costs between specific complications. Concomitantpanniculectomy performed by plastic surgeon was associated with41.5% wound complication rate compared to 16.2% in routine VHR.Average cost of panniculectomy wound complication was $16,700 vs$740 without complication (p=0.0002, difference CI95% $9,300-$22,500) in the first year. Conclusion: Postoperative cellulitis, wound breakdown and infectioncause patient morbidity but also represent substantial financial bur-den to society, raising follow-up costs 30-fold or more. Cost analy-sis should be included in risk-benefit assessment of treatment andprevention strategies of wound complications.Fig. 1: The Abdoman.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S53

S54 Hernia (2011) 15 (Suppl 2): S37-S66
P-053Local anaesthesia for open incisional hernia repair: Analternative choice?G. Brancato1, M. Donati2, E. Pulvirenti1, A. Donati11 University of Catania, Department pf Surgical Sciences, OrganTransplantation and Advanced Technologies, Catania, Italy; 2 CelleGeneral Hospital, General, Visceral and Thoracic Surgery, Celle,Germany
Background: Aim of this work was to give an accurate descriptionof a method of incisional hernia repair with an open technique, underlocal anaesthesia. Methods: Between January 1994 and December 2010, 148 patientshave been submitted to an open mesh surgical procedure for inci-sional hernia repair. From this cohort, a sub-population has beenselected as eligible for the present study, with the following inclu-sion criteria: Reducibility of the hernia sack, absence of bowelobstructive symptoms, hernia orifice smaller than 10 cm. Results: During the period of study 89 patients (60.13% of the pop-ulation) were considered eligible to the procedure. The median oper-ative time was 105 min. The intra-operative measurement of the her-nia defect showed that: in 26 patients (29.21%) it was within 3 cm,in 52 patients (58.42%) up to 10 cm. There were 2 conversions(2.24%) to general anaesthesia. Only 4 patients (4.49%) showed tran-sient intra-operative bradycardia. All the other 87 patients (97.75%)had immediate postoperative deambulation, feeding and were dis-charged within 24 h. During a 12-202 months of follow-up, only2 recurrences (1.35%) were detected. Conclusions: Local anaesthesia for incisional hernia repair with aopen preperitoneal mesh technique represents a safe, feasible andeffective approach with an associated low intraoperative risk; it iscost-effective with very good long-term results. References:1. M. Donati, G. Brancato, A. Donati. Open Incisional Hernia Repair.Acta Chir. Belg. 2010, 110: 45-50
2. M. Donati, L. Gandolfo, G. Brancato, A. Privitera, A. Donati. Dayhospital for incisional hernia, Acta Chir Belg 2008, 108: 198-202
3. L. Herszage, L. Dimasi, J.A. Abait, O.P.A. Damia, P. Giuseppucci,C.B. Mitru. Ambulatory surgery in abdominal wall pathology: 7years experience. Ambul Surg, 1999, 7: 13-15
4. G. Tzovaras, D. Zacharoulis, S. Geoorgopoulou, K. Pratsas,G. Stamatiou, C. Hatzithefilou. Laparoscopic ventral hernia repairunder spinal anaesthesia: a feasibility study. Am J Surg, 2008, 196:191-194
P-054A tailored approach for recurrent incisional herniarepair seems effective after mid-term follow-upF. Berrevoet, E. Reynvoet, A. Vanlander, X. Rogiers, R. TroisiUniversity Hospital Ghent, General and Hepatobiliary surgery,Ghent, Belgium
Background: The risk of developing a recurrent hernia increaseswith each additional operation. It was the aim of this retrospectiveanalysis to evaluate the outcome of recurrent incisional hernia repairsapplying a tailored surgical approach. Methods: From January 2000 until December 2010 a total of 862incisional hernias had been operated in 772 patients. Of this amount,185 operations were for recurrent hernias. Seventy-three patientsoperated by the same surgeonwere included for evaluation. If thepatients had not been examined in the outpatient clinic the last12 months, they were invited for a follow-up visit. Besides a clini-cal exam, the patients were questioned for postoperative pain and for
sensation of the implanted mesh by using respectively the VisualAnalogue Scale and the Carolina Comfort Scale. Approval wasreceived from the Ethical Committee. Results: The mean age of the patients was 54 years (±11.84), witha mean body mass index of 29.5 kg/m2 (±6.96). Forty-nine patients(67.1%) were operated for a first recurrence, 16 patients (21.9%) fora second, 7 patients (9.6%) for a third and one patient (1.4%) for afourth recurrence. In 15 patients the procedure was done laparoscop-ically, while 58 patients had an open repair. No matter the previousprocedure was performed open or laparoscopically, the open tech-nique was associated with a higher wound morbidity compared tolaparoscopy, and correlated with a higher recurrence rate (22.9% vs.6.6%). In total, 12 patients (16.4%) had a new recurrent hernia dur-ing a median follow-up period of 15.0 months (1-69). Chronic painand quality of life were acceptable with both techniques. Conclusion: Using a tailored approach, overall outcome after recur-rent incisional hernia repair seems worthwhile. However, wound mor-bidity contributed to new hernia recurrences, especially using an opentechnique.
P-056Open ventral hernia repair with concomitantpanniculectomy is safe and effective: An eleven yearexperience at a single institutionD.A. Klima, C.L. Carpenter, C.M. Hlavacek, A.E. Lincourt,S.B. Getz, B.T. HenifordCarolinas Medical Center, Carolinas Laparoscopic and AdvancedSurgery Program, Charlotte, United States of America
Introduction: The presence of a large pannus or a severely scarredabdomen can add significantly to the technical challenges of an openventral hernia repair (OVHR). Concomitant panniculectomy or broadskin and subcutaneous resection via a transverse incision during anOVHR (OVHR/PANN) could simplify access to the abdomen andfacilitate the technical aspects of mesh placement and fascial closureand improve the cosmetic result. This combined approach was eval-uated prospectively. Methods: Clinical outcomes, complications and demographics ofpatients undergoing OVHR/PANN until May 2010 were prospec-tively collected and analyzed. Standard statistical methods were usedwith significance defined as p<0.05. Results: N=148 patients underwent OVHR/PANN with 79% females(N=117). Mean age, BMI and defect size were: 54.0±12.7 years,37.0±8.9 kg/m2, and 255±240.8 cm2. Previous abdominal surgery hadbeen performed in 94.6% of patients (N=140), and 75% (N=111)had recurrent hernias (average 2.4±2.2 previous repairs). Meandrain duration was 18.5±12.1 days and average follow-up time was5.6 months (range 1-35). 66 patients (44.6%) developed post-opera-tive wound complications, although only 16 necessitated woundintervention (11.4%). There were 45 cases of cellulitis defined aserythema of the abdominal wall requiring antibiotics (30.4%).23 patients developed seromas (15.5%), of which 20 requireddrainage (13.5%). There were 20 cases of wound breakdown(13.5%), with 13 requiring surgical intervention (8.8%). Four patients(2.7%) had hernia recurrences and no post-operative deaths occurred(0%). Chronic Obstructive Pulmonary Disease (COPD) and smokingwere significant predictors for wound breakdown (p=0.004, p=0.03)and overall wound complications (p=0.002, p=0.02, respectively). Conclusion: OVHR/PANN is a safe and effective method of herniarepair for patients presenting with a large encumbering pannus. Woundcomplications were the most common post-operative complication, andpatients who smoke should be strongly encouraged to stop prior tosurgery. The combined OVHR/PANN approach demonstrated a lowrecurrence rate, low morbidity, no mortality, and improved cosmesis.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S54

Hernia (2011) 15 (Suppl 2): S37-S66 S55
P-057Developing new strategies in abdominal wall closureusing a virtual mechanical modelC. Justinger1, I. Shklyar2, P. Klein2, M.K. Schilling11 University of the Saarland, Department of General, Visceral,Vascular and Pediatric Surgery, Homburg/Saar, Germany;2 Frauenhofer, ITWM, Kaiserslautern, Germany
Background: Incisional hernia remains the most common long-termcomplication after midline incisions of the abdominal wall, its inci-dence varying between 9% and 20% in different studies due to vari-able definitions. Thousands of patients have been included in ran-domized trials and a number of meta-analyses have been performedto determine the optimal method of fascial closure. However, theideal method and material in closing the abdominal wall has not beenfound so far. As new strategies are needed to optimize the abdomi-nal wall closure after surgery our group developed a virtual mechan-ical model of the abdominal wall to demonstrate the optimizationpotential of the stitch pattern used after midline incision. Methods: Simulating the complex anatomical geometry of the abdom-inal wall the LaparOPT virtual mechanical model of the abdominalwall was developed. As the midline incision of all patients in our highvolume center is closed in a standardized way we analyzed the opti-mization potential of the stitch pattern in abdominal fascial closure. Results: The use of a virtual mechanical model of the abdominalwall works and helps to understand the abdominal wall closure.Analyzing the clinically used stitch pattern shows the optimizationpotential of surgical procedures in virtual models. New strategies toprevent incisional hernias including the development of new devicescan be simulated in virtual models. Conclusion: Using a virtual mechanical model to simulate thepatients’ abdominal wall may help to optimize the abdominal wallclosure and decrease the number of incisional hernia after abdomi-nal surgery.
P-058Influence of mesh features in intraperitoneal ventralhernia repair using a validated numerical modelG. Guerin, F. TurquierCovidien, R&D, TréVoux, France
Background: The outcomes of a Ventral Hernia Repair (VHR) donot only depend on the surgical technique but as well on the meshfeatures. A wide range of synthetic meshes is currently available onthe market with various mechanical properties that can be defined interms of stiffness and anisotropy. Our primary goal was to assess for intraperitoneal VHRs the influ-ence of the mesh features on the global abdominal wall behavior. Avalidated numerical model was used for this purpose. Methods: The model consisted of an abdominal wall defined asactive, with an elliptic and centered hernia defect. A particular effortwas made to model meshes. Both anisotropy and hyperelasticity weretaken into account. Mobility of the peritoneum on the wall was allowed and meshes werefixed either with tacks only or with tacks and transparietal sutures. Finally, the influence of both mesh mechanical properties (anisotropyratios) and overlap (2-5 cm) was investigated. Results: Numerical simulations showed that reducing the overlapresulted in higher stresses on meshes (up to +43%) and higher pull-out forces at fixation points (up to +220%). A higher compliance of the mesh with the abdominal wall in termsof anisotropy and stiffness helped to reduce this stress level.
Conclusions: Mesh features (stiffness, anisotropy and size) influ-enced significantly the early performance of intraperitoneal VHR.Highest stress concentration was observed for small overlap config-urations that potentially increased the risk of failure. Further para-metric studies should help to design better meshes.
P-060Self-gripping mesh in ventral hernia repair – one yearresultsS.B. HopsonBon Secours Hernia Center, Surgery, Newport News,Virgina, UnitedStates of America
Introduction: In a previous study, Progrip Self-Gripping Mesh wasfound to be safe and effective in open ventral hernia repair at6 months. In order to assess continued safety and efficacy, patientswere followed over a one year period. Methods: Patients underwent ventral hernia repair with a self-grip-ping, semi resorbable, lightweight mesh (Parietex Progrip™ mesh,Covidien). Demographic data, surgical procedure, comorbidities, hernia type, surgical procedure and postoperative course (pain assess-ment, recurrence rate, seroma, hematoma and infections) wererecorded at preoperative, perioperative, 1, 3, 6, and 12 month fol-low-up. In addition, VAS pain score was assessed at 12 months. Results: At one year post-op, results show that patients continue tohave a low rate of recurrence and complications and a favorable VASpain score. Conclusion: Self-gripping mesh can be used safely and effectivelyin open ventral hernia repair with acceptable results at one year.
P-061Seroma formation following incisional hernia repair –what factors are associated with their development?N.J. Smart1, D. Khan1, C. Pinckney2, I.R. Daniels11 Royal Devon & Exeter Hospital, Exeter Colorectal Unit, Exeter,United Kingdom; 2 Peninsula College of Medicine & Dentistry,Plymouth, United Kingdom
Background: Seroma is a common complication following incisionalhernia repair. The aim of this study was to assess the factors asso-ciated with seroma formation following incisional hernia repair in aconsecutive series. Methods: Retrospective review of 75 patients who underwent surgeryfor an incisional hernia between 2006 and 2010 under a single surgeon. Results: Data was available on 70/75 (33 males) patients. The30-day mortality was 1/70 with one patient dying in the follow-upperiod. Complications were assessed at discharge, six months andone year. The overall post-operative seroma rate was 28% (19/67)and the rate at one year was 18% (12/65). Factors associated withthe development of seroma following surgery were; female sex(26% v 10%) and smoking (31% v 15%) non-smokers. No differ-ence was noted in terms of BMI (<30 v >30), prior malignancy, pre-vious incisional hernia repair, material used (biologic v non-biologicimplant), and ASA. The presence of a seroma, however, was asso-ciated with the technique used, onlay 39% (95% CI 21%-57%) ver-sus sublay/sutured technique 3% (95% CI 0-9%). Conclusions: The on-lay technique for incisional hernia is statisti-cally significant for seroma formation. Female sex and smoking areassociated with seroma formation but not statistically significantly inthis series. BMI is not a risk factor.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S55

S56 Hernia (2011) 15 (Suppl 2): S37-S66
P-062Sutureless plastic in ventral hernia repairV.V. Parshikov1, V.A. Khodak2, V.V. Petrov2, A.V. Samsonov2,V.P. Gradusov2, A.A. Samsonov2, R.V. Romanov21 Nizhny Novgorod State Medical Academy, Hospital Surgery, NizhnyNovgorod, Russian Federation; 2 Hospital 35, Surgical, NizhnyNovgorod, Russian Federation
Backgrounds: Repair of primary and incisional hernias is a commonsurgical procedure. The various methods of hernia repair are onlay, inlay,sublay (retromuscular) and IPOM. Open IPOM is one of the easiest meth-ods after the onlay for the plenty of surgeons. The sutureless plastic isthe method, making IPOM hernia repair easier, faster, less tissue injury. Methods: In 2003-2010 393 patients underwent elective surgery onprimary and incisional ventral hernias. 85 patients operated by suture-less plastic. The principle of method is the use of specially formedmesh. The mesh has its central part, covering and overlapping thedefect. Peripheral parts of the mesh are several fixing straps. Themesh made with reperene (polymer) or polypropylene. The centralpart of mesh places in the wound. A troacar with a loop or Mikuliczclamp penetrates the abdominal wall, catches the straps. The strapsare led through the abdominal wall following the troacar or the clamptraction. The mesh stretches in the wound. Then the wound is sewing.No need to fix the straps to skin with sutures (photo 1).
Results: In the patient group with sutureless plastic there was1 hematoma, no suppuration. No mortality. The follow-up was2 years, no recurrence. Conclusions: Sutureless plastic is a fast, easy to learn, effective oper-ating technique. It shows good results in 2-year follow-up.
P-063No seroma formation with minimal invasive repairusing self expandable meshes for large ventral andincisional herniasS. Apostolidis, A. Zatagias, A. ZevgaridisEuromedica Kyanous Stavros Hospital, Surgical Department,Thessaloniki, Greece
Background: Seroma formation is a common postoperative compli-cation, concerning the repairs of large ventral and incisional hernias,where large fascial mobilization is performed. We present an openminimal invasive technique for a functional repair, without fascialdissection. The self expandable double layer mesh is inserted andfixed through the hernia defect.
Methods: From September 2007 to September 2010 a total of 68large (>7 cm) ventral and incisional hernia repairs were performed.The hernia sac was opened; the excess of the sac dissected andexcised without any further fascial dissection, the mesh was insertedthrough the defect and anchored in a sublay mode with transcuta-neous slowly absorbable sutures and absorbable tacks. The bordersof the abdominal wall were fixed on the upper side of the mesh.Vacuum drains were placed over the mesh. All patients underwentultrasound examination on discharge and a week after surgery. Theoperative time, seroma formation, wound infection and recurrencewere studied. Results: There were no seromas or wound infections recorded. After4 to 39 months of follow up there are no recurrences. Three of thesepatients (4,4%) suffered from a persistent pain in the abdomen for6 months, due to the transcutaneous anchoring sutures. Mean oper-ative time was 75 min, while the mean hospital stay was of 3 days.All patients returned to their everyday activities 8 days after surgeryand the employed ones to their work 16 days after surgery. Conclusion: An open minimal invasive technique without fascial dissection and intraperitoneal placement of the self expandable double layer mesh is an effective functional repair for large ventraland incisional hernias, with encouraging results concerning seromaformation.
P-064Use of bovine pericardium graft for abdominal wallreconstruction in contaminated fieldsL. D’AmbraS. Andrea Hospital, Surgery, La Spezia, Italy
Background: Incisional hernia is one of the most common compli-cation after laparotomy that can occurs in 3 to 20% of cases. Thehernia repair can be performed by simple primary closure, staged ordelayed reconstruction, surgical flaps or by prosthesis repair madein laparoscopic or open way. The use of prosthetic mesh significantlydecreases the hernia recurrence rate, but in can not be employedin particular conditions like septic contaminated or potentiallycontaminated surgical field, pre radiated tissues, and in case ofhernia recurrence on infected mesh. In these conditions is recom-mended to use an ideal material able to resist infection after itsimplantation. Methods: In our surgical department, from January 2006 to June2010, 48 patients underwent abdominal wall reconstruction usingacellular bovine pericardium; among them 34 patients had a contam-inated wound during diffuse peritonitis (complicated diverticolitis,bowel perforation, intestinal infarction, strangled hernia, etc) and14 patients had hernia relapse on infected synthetic mesh. Conclusion: Recurrence rate is quite similar to that occurring after pros-thetic mesh repair and the application of acellular bovine pericardium(Tutomesh®, Tutogen Medical Gmbh Germany) is moreover a safe andfeasible option that can be employed to manage complicated abdomi-nal wall defects when prosthetic mesh are scarcely tolerable.
P-065Results of ten-years single Institution series oflaparoscopic ventral hernia repairL.J. Sanchez, L. Bencini, M. Bernini, B. Boffi, M. Calistri, R. MorettiCareggi Hospital, General Surgery, Florence, Italy
Laparoscopic ventral hernia repair (LVHR) technique is feasible bothfor small primary or incisional defects and for very large parietaldefects, depending on the total abdominal surface. From January 2000 to December 2010 we treated, by the laparoscopicapproach, 198 patients suffering for ventral hernias at our Institution.
Photo 1.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S56

Hernia (2011) 15 (Suppl 2): S37-S66 S57
33 (17%) had a previous failed attempted repair. 7 (3.5%) required conversion to an open traditional technique. Of the remaining191 patients, 79 were males and 112 female (F/M=1.4). Mean age was63±11 years (range 32-89), with an ASA score of 1-2 /ASA3-4=166/25.Obesity (BMI>28) was present in 96 (50%). 44 (23%) had primitivedefects while 147 (77%) postincisional. Average of defect surface was58±55 cm2 (range 4-260). The mean operative time was 103±44 minutes (range 40-355) includ-ing 30 (16%) cases with an associated procedure. Mean postoperativestay was 4±3 SD days (range 1-30). We had 4 (2%) major surgicalcomplications: 3 intestinal injuries during adhesiolysis and treated byminilaparotomy, 1 reintervention from paralytic ileum; and 2 (1%)major medical complications: one stroke and one pulmonary embolism.We also report 27 (14%) minor complications: 12 (6%) seromas,10 urinary retentions, 2 deep venous leg thrombosis, 1 persistent post-operative pain, which resolved with medicines later on at home, and1 atrial fibrillation. We recorded 16 recurrences (8%), one being a tro-car site herniation, after a mean follow-up of 53 months (range 2-120). The results of this large single Institution series confirm that LVHR isa valid alternative over traditional intervention, due to better shortand medium-term results (few complications). However, the crucialproblem of recurrences is still present and tends to increase accordingto length of follow-up. Port-site recurrences or new fascial defectsoccurred far from the prosthesis should also be considered as technique’sfailure.
P-066Mesh repair of complex, incisional hernias utilising softtissue reconstruction and biological mesh insertion:A consecutive, single-team experienceJ.R.A. Skipworth1, L. Ovens2, C. Morkane3, C. Imber2, D. Floyd2,A. Shankar21 University College London, Surgery and Interventional Science,London, United Kingdom; 2 Royal Free Hospital, Department ofPlastic Surgery, London, United Kingdom: 3 University CollegeLondon Hospital, London, United Kingdom
Background: Mesh repair of complex, incisional hernias, with signif-icant loss of abdominal wall tissue resulting from wound/mesh infec-tions and intra-abdominal complications of gastrointestinal surgery,carries a significant risk of complications, including infection andrecurrence. A technique of soft tissue reconstruction and insertion ofintraperitoneal Strattice™ biological mesh (Porcine Collagen) wassubsequently developed as Strattice™ has been demonstrated to reducethe incidence of mesh infection when utilised in animal models. Methods: A retrospective case-notes review of all incisional herniapatients managed via soft tissue reconstruction and Strattice™ meshinsertion was performed. Standardised operative repair involved intra-peritoneal mesh insertion and soft tissue resection and reconstructionutilising a component separation technique. All cases were performedas a single-stage procedure by a General and Plastic Surgeon. Results: 35 patients underwent complex, incisional hernia repair fora combination of midline, transverse and lumbar hernias between Feb2009 and January 2011. Patient age ranged from 30-85 years, gen-der ratio was 52% M: 48% F and mean follow-up was ten months.Six (17%) patients had repair of recurrent incisional hernias, two(6%) patients had more than one mesh inserted for extremely largeand multiple defects, and three (9%) patients had been diagnosedwith previous infection of in-situ mesh. Post-operative complications included two (6%) MRSA mesh infec-tions, one (3%) seroma, one (3%) fat necrosis within the wound, one(3%) lower respiratory tract infection and one (3%) reoperation forwound debridement. However, there have been no hernia recurrencesto date and no requirements for mesh removal.
Conclusions: We present the indications, operative technique andoutcome from incisional hernia repair, utilising soft tissue reconstruc-tion, Strattice™ insertion and a combined General and PlasticSurgery approach. This technique allows for safe, reliable and defin-itive reconstruction of complex and recurrent incisional hernias, witha low incidence of post-operative mesh infections, no hernia recur-rences and minimal complications.
P-067Components separation technique augmented with abiologic underlay and a polypropylene onlay mesh L.M. Morris, K.A. LeBlancLouisiana State University Health Sciences Center, Surgery, BatonRouge, United States of America
Background: Reconstruction of large, complex abdominal wall her-nias is an ongoing challenge. Primary closure of such hernias is oftennot possible. The components separation technique (CST) is oneoption that has enabled primary closure of these hernias by a singleprocedure. Despite the CST’s utility, however, recurrence ratesremain as high as 32%. In an attempt to reduce recurrences, we addeda biologic underlay mesh and a lightweight polypropylene onlaymesh to the traditional CST. Methods: Patients with a large hernia defect with or without multi-ple recurrences were selected to undergo a CST augmented with anacellular porcine dermal collagen mesh underlay. Following midlineabdominal fascial closure, a lightweight, large-pore polypropyleneonlay mesh was fixed to the abdominal fascia. The skin and subcu-taneous layers were closed over two sump drains and two closed suc-tion drains. Data collection included patient demographicsand co-morbidities, procedure data, and outcomes including woundcomplications and recurrence rates. Results: Fifty-one patients underwent a mesh-reinforced CST fromMay 2006 to June 2010. The study population averaged 57.9±1.5years of age with 23 males and 27 females, BMI of 34.3±0.9 kg/m2,ASA score of 2.62±0.08, 29% were smokers, 29% were diabetic and69% had at least one previous abdominal wall hernia repair.Operative time averaged 196.5±7.2 minutes with a blood loss of318±24 mL, and hernia defect size of 301±31 cm2. Length of fol-low-up averaged 20.6±2.1 months, surgical site occurrences wereidentified in 39%, most commonly from skin necrosis and herniarecurrence was 5.9%. Conclusion: Repair of large, complex abdominal wall hernias byCST augmented with a biologic underlay mesh and a lightweightpolypropylene onlay mesh results in lower recurrence rates comparedto historical reports of CST alone.
P-068Tailoring incisional hernia treatment, how do we do it?A retrospective study with a 3 year clinical follow-upC.J. Brandt, M.P. SimonsOnze Lieve Vrouwen Gasthuis, Surgery, Amsterdam, Netherlands
Despite improvements over the past decades, incisional herniaremains a frequent complication after laparotomy with rates up to20%, and recurrence rates up to 54% after incisional hernia repair.Patient specific treatment and preoperative risk assessment mightaddress the problem of postoperative hernia recurrence and remaina major topic of discussion. We retrospectively studied a hernia population of 189 patients thatwere treated for incisional hernia between January 2006, andDecember 2007 at the OLVG: a large district teaching hospital withspecial interest in hernia surgery. A 3-year clinical follow-up wasperformed on 165 patients (87%), which were available for follow-up, in the outpatient clinic.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S57

S58 Hernia (2011) 15 (Suppl 2): S37-S66
Baseline characteristics, treatment specification and postoperativecomplications were put into a database. Outcome was computed withPASW Statistics 18. Major treatment procedures were: 1. Reeves-Stoppa; standard.2. Laparoscopic intraperitoneal mesh placement. 3 RamirezComponent seperation technique (CST) with, or without retromus-cular mesh placement, and 4. Primairy closure. After a mean follow-up of 35 months (24-47) recurrence rate was 21%. Conservativelytreated patients (28%) were significantly older than the operatedgroup, but showed no other differences at baseline. Reeves-Stoppais performed more often in case of recurrent incisional herniae orprevious laparotomies, and together with CST, is performed moreoften on larger defects than laparoscopic and primary closure(p<0.05). Emergency procedures were performed most often withCST. Furthermore, primary closure increased hernia recurrence to47%, and laparoscopic treatment decreased recurrence rates to 7%compared to 21% with standard open treatment (p<0.05). In summery, conservatively- and operatively treated patients showmoderate differences at baseline. Reeves-Stoppa and CST are per-formed more often in complicated surgical sites. Laparoscopic treat-ment seems to be a good option for uncomplicated hernia surgery. Further studies will have to elucidate the impact of risk factors onrecurrence after hernia repair.
P-069Workshops as training in incisional hernia laparoscopicrepairR. Fernandez Lobato1, F.J. Angulo Morales2, J. Garcia Septiem2,M. Arenillas2, J. Herrero21 Hospital U. Puerta de Hierro-Majadahonda, General Surgery,Madrid, Spain; 2 Spain
Introduction: Laparoscopic is elective approach in a lot of cases ofabdominal surgical procedures, but it is necessary a correct trainingof the surgeon to learns technique, improves surgical results andavoids iatrogenic lesions. Several systems to learn these procedures have been introduced inthe last years. We present the results in training laparoscopic ventralhernia repair courses performed in Hospital of Getafe (Madrid), withtheoretical part and practice part with the aim to improve the learn-ing curve of assistants. Methods: Work-shops have 1 day of duration and 2 parts: the firsta “live surgery” into OR. Laparoscopic repair are performed byexpert surgeon in the morning to 2-3 patients with different ventralhernia. The second pat, assistants are training in pig experimentalmodel in the evening (Vet control in all the procedure) and they prac-tise learned the correct technique. Assistants take part in the cases, asking doubts and viewing stepsconcerning the technique into OR and during the lunch. Results: 210 surgeons came from several countries (90 centres) to 55Work-shops performed in the last 7 years (3-4 assistants each one).Senior surgeons (185) and Training surgeons (25). 88% of then doesnot performed previously laparoscopic hernia repair. 95% were satis-fied for content learned and practised and 30% of them performedlaparoscopic repair in their hospitals during next year, with goodresults and non iatrogenic problems or complications of the technique. Advantages of the system are: • Learn laparoscopic repair with an expert and human cases.• The possibility of training in experimental model like humanwhere the problems and difficulty in the placing and fixing meshare the same.
Conclusions: Training courses contribute to improve the learningcurve in laparoscopic approach, with reduction of time to learn, bet-ter technical results in the patient and better efficiency of the healthsystem.
P-070Preliminary safety results of prophylactic mesh inelective and urgent abdominal surgeryJ. López-Monclús1, M.A. García-Ureña1, D.A. Melero1, A. Pueyo1,L.A. Blázquez1, P. López-Quindós1, A. Galvan1, E. Enrique1,N. Palencia2, R. Barriga2, A. Cruz1, A. Robin1, A. Aguilera11 Henares Hospital, General and Digestive Surgery, Coslada, Spain;2 Spain
Background: Incisional hernia is a frequent complication after mid-line incisions of the abdominal wall, with an estimated incidence of9%-20%. Patients suffer from pain, impaired quality of life, andpotentially life-threatening disorders, such as incarcerations or bowelstrangulation. Hospital readmission for surgical repair increases san-itary costs. The final endpoint of this study is to investigate whetherprophylactic polypropylene mesh could reduce the rate of postoper-ative incisional hernia; after the first 20 cases our objective is tostudy if this technique is safe without increasing the rate of compli-cations. Methods: Prospective study including patients operated through amidline laparotomy both in elective and urgent surgery. After mid-line closure with continuous suturing of long term absorbable loopmonofilament, 3 cm of prefascial space were dissected at eachside of the laparotomy. Two slices of 4,5x15 very low weightpolypropylene where placed in the prefascial space, being fixed withpolyglactine single stitches. An aspirative drain was placed for atleast 24 hours. Results: Twenty patients with a mean age of 69 (range 30-87) yearswere included, 11 (55%) of whom where women. Nine cases (45%)were urgent surgeries, with 13 clean-contaminated fields (65%),2 contaminated (10%) and 4 dirty fields (20%). Between the indica-tions, 12 (60%) were oncological colorectal surgery, 2 (10%) smallbowel obstructions, 1 (5%) perforated duodenal ulcer, and 3 (15%)miscellaneous indications. There were no perioperative deaths. Fourpatients (20%) developed local complications: 3 superficial woundinfections and one seroma. No mesh became infected neither in theshort or long term. Mean hospital stay was 9.7 days (range 4-20). Conclusion: Prophylactic polypropylene mesh placement in electiveand urgent abdominal surgery is a safe technique, without prolong-ing surgery or increasing wound complications. However, the finalstatement should await the outcomes of the long-term follow up ofthe studied cases.
P-071Peritoneal adhesions prevention withchitosan-polyethylene glycol coated polypropylenemesh in ratsR.M. Melo1, D.F. Rodrigues1, F.F. Mendes1, D.B. Silva1, A.S. Silva1,L.L.B. Guimaraes1, L.S. Silva2, A.M. Moraes3, N.M. Paulo11 Federal University of Goias, Surgery, Goiania, Brazil; 2 School ofVeterinary Medicine, Surgery, Goiania, Go, Brazil; 3 UniversidadeEstadual de Campinas, UNICAMP, School of Chemical Engineering,Campinas, Sp, Brazil
Background: Peritoneal adhesions are still a challenge in surgicalpractice as a potential source of serious sequelae, such as chronicabdominal pain, infertility and intestinal obstruction. Therefore pre-vention of adhesions became a target for surgeons. Due to its bio-compatibility, absorbable profile, tissue repair facilitation and antimi-crobial properties, chitosan is a biomaterial that has been studiedregarding the prevention of peritoneal adhesions. The objective ofthis study was to evaluate the effectiveness of polypropylene coatedwith chitosan-polyethylene glycol and uncoated polypropylene pros-theses to prevent peritoneal adhesions.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S58

Hernia (2011) 15 (Suppl 2): S37-S66 S59
Methods: Defects with approximately 1 cm2 involving the rectusabdominis and external oblique muscles were produced in the abdom-inal wall of Wistar rats, and repaired with a polypropylene meshcoated with chitosan-polyethylene glycol (QP-PP Group, n=12) oruncoated polypropylene mesh (PP group, n=12). Six animals fromeach group were euthanized at four and 45 days after implantation.The involved mesh area by the adhesion as well as the type of adhe-sion was evaluated. Results: One animal in PP group showed intestinal obstruction andwas discharged from the analysis before 45 days. All animals pre-sented adhesions, but QP-PP group showed less involvement of themesh in both periods. There was no significant difference of the typeof adhesion in four days. Regarding the type, severity of adhesionswas lower in QP-PP at 45 days. Conclusion: The polypropylene mesh coated with chitosan-polyeth-ylene implanted in the intraperitoneal space reduces the formation ofperitoneal adhesions in rats, but it does not prevent it completely.
P-072The evaluation and prediction of the acuteinflammatory characteristics of synthetic and biologicalmeshes using a sensitive quantitative in vitrochemiluminescent assayN. Bryan, N. Smart, Y. Bayon, N. Scarborough, J.A. HuntUniversity of Liverpool, Clinical Engineering, Liverpool, UnitedKingdom
Background: Clinical outcome of hernia meshes are decided early afterimplantation as leukocytes interrogate the material in the first day post-operatively. High degrees of leukocyte activation lead to chronic pain.Reactive oxygen species (ROS) are released by leukocytes when activated. This response can be used as a sensitive measurement ofleukocyte activation. The aim of this study was to compare the degreeof leukocyte activation of commercially available synthetic and biolog-ical hernia meshes. Methods: Chemiluminescence assay was performed using modificationsto a commercially available kit (Knight Scientific, UK). Whole bloodwas obtained from 5 different healthy human adults, combined withAdjuvantK, Pholasin and mesh, and incubated for 30 minutes with continuous chemiluminescent measurements. Leukocyte stimulantsfMLP and PMA were added as controls. Four different synthetic meshes
of varying chemistry (PP, PET, PGA) and knitting patterns and five dif-ferent dermis and small intestinal submucosa (SIS) biological mesheswere investigated. Statistics were performed using Waller-Duncan posthoc ranking into statistically homogenous subsets (see figure). Results: Chemiluminescence measurements of ROS demonstratedmaterial specific differences in leukocyte activation. Among syntheticmeshes, multifilament PGA mesh had significantly higher responsescompared to PP and PET meshes (p<0.05). Yarn conformation (ie.mono- vs multi-filament) made a greater difference to the leukocyteresponse than polymer composition. Waller-Duncan post hoc rank-ing allowed grouping of the materials into statistically similarly ROSstimulating groups. The biological meshes demonstrated significant differences in leukocyteactivation. The degree of leukocyte activation appears to be mainlyrelated to the tissue origin, the SIS mesh eliciting the greatest reaction. Conclusion: The most leukocyte activating synthetic and biologicalmeshes were the Multifilament PGA mesh and the SIS mesh, respec-tively, in in vitro conditions. In the case of synthetic meshes it wasconcluded that weave is a greater influence on leukocyte responsethan polymer chemistry.
P-073Evaluation of composite absorbable and permanentlaparoscopic mesh fixation devicesJ.F. Byrd, N. Agee, R.Z. Swan, K.N. Lau, J.J. Heath, I.H. McKillop,D. Sindram, J.B. Martinie, D.A. IannittiCarolinas Medical Center, General Surgery, Charlotte, United Statesof America
Background: Laparoscopic ventral hernia repair is commonly per-formed with mesh prostheses; however, there is no standard for fixation devices used to secure mesh to the abdominal wall. Thisstudy is a functional comparison of composite, screw-type absorbableand permanent fixation devices with a traditional titanium fixationdevice. Methods: Fifteen pigs each underwent laparoscopic placement oftwo 11 cm x 14 cm mesh prostheses and were randomized for meshfixation with either titanium spiral tacks (TS), absorbable screw-typefasteners (SF), or permanent screw-type fasteners, (PF) (N=10 meshprostheses for each fixation group). Adhesions were assessed laparo-scopically at 4 weeks with the Modified Diamond Scale for quan-tity and a tenacity scale to measure the density of adhesions. Thefixation devices were also embedded in porcine abdominal rectusmuscle for ex vivo mechanical testing along with partial thicknesspolypropylene suture (PR) as a control group (N=40 for each group).Maximum pull-off forces were measured. All statistical tests weretwo-tailed, and p<0.05 was considered significant. Results: Mean tenacity adhesion scores were 2.6±1.07 (TS),1.7±0.82 (SF), and 1.40±0.52 (PF). Adhesions in the PF group weresignificantly less tenacious compared with the TS group (p=0.01).Quantitative adhesion scores were not significantly different amonggroups. Maximum pull-off forces measured in Newtons were28.61±4.89 N (TS), 22.71±7.86 N (SF), 16.98±7.59 N (PF), and20.83±6.25 N (PR). The pull-off force in the TS group was higherthan all other groups (p<0.001). The SF group also had a higher pull-off force compared with the PF group (p<0.001). Conclusions: The ideal fixation device provides strong adherence ofmesh to the abdominal wall while minimizing intra-abdominal adhe-sion formation. The composite, screw-type fixation devices wereassociated with fewer adhesions as compared to the commonly usedtitanium spiral tack. The mechanical fixation strength of these deviceswas lower than titanium tacks, but comparable to polypropylenesuture.
Total RLU
Material
Multi PGAMulti PET LightMono PP LightMono PET LightCells Without Textile
700,000
600,000
500,000
400,000
300,000
200,000
100,000
0
!
&
@
@
#
Fig. 1: Comparison of total ROS production from donor whole bloodleukocytes in response to the panel of synthetic hernia repair tex-tiles. Symbols (!, &, @ and #) represent statistically homogeneousgroupings based on Walter-Duncan post hoc analysis. Error bars rep-resent one standard deviation from the mean, n=20, multi: multifil-ament yarn, mono: monofilament yarn, light: mesh density < 50 g/m2.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S59

S60 Hernia (2011) 15 (Suppl 2): S37-S66
P-074New synthetic bioabsorbable mesh in open abdomenC. Doerhoff, P. TegetSurgiCare of Missouri, PC, Surgery, Jefferson City, United States ofAmerica
Background: The open abdomen (OA) strategy reduces the risk ofabdominal compartment syndrome, but many patients with OA havecontaminated wounds. Use of nonabsorbable synthetic mesh forabdominal wall closure after OA carries a high incidence of infec-tion and fistula. Employing biologic mesh may lower this risk; how-ever, biologic devices are costly, may require pre-use soaking,and may not be available in large sheets. A new synthetic bioab-sorbable mesh (GORE® BIO-A® Tissue Reinforcement) may providea similarly decreased risk at a lower cost and with more conven-ience. Methods: The bioabsorbable mesh was used in 2 male patients (aged45 and 54 years) with OA. In both patients, the mesh was placedintra-abdominally and fixed with transfascially placed absorbablesutures. The younger patient had a small-bowel (SB) obstruc-tion/perforation and numerous intra-abdominal abscesses. He under-went several irrigation procedures in a week, with temporary cover-age of OA obtained by using a Fish retractor. The mesh was thenimplanted, and the abdominal defect was progressively closed overa 2-week period with use of a second piece of mesh. The older patientinitially had an abscess and enterocutaneous fistula. The abscess wasdrained and the fistula was closed. During the subsequent 6 weeks,multiple SB leaks were repaired and several irrigation procedureswere performed. After SB leakage stopped, the bioabsorbable meshwas used to close the abdomen. Following closure, the patient hada recurrent fistula that sealed. Results: There were no mesh-related complications. The patientsare eating normally and are without recurrent ventral hernias 5 and7 months, respectively, after mesh implantation. Conclusion: The synthetic bioabsorbable mesh requires no prepara-tion, is available in large sheets (up to 20x30 cm), costs less thanbiologic meshes, and has been used safely in contaminated OA.
P-075Local tissue effects and performance evaluation of anew semi-resorbable Plug&Patch in pig groin herniarepair modelD.G. Guyader, G. Doucet, M. BuffinCovidien, RD, Trévoux, France
Introduction: Parietex™ Plug and Patch System (Parietex™ PP,Covidien) is composed of a lightweight onlay patch and a self-form-ing semi-resorbable plug. The patch is crafted from a flat-sheet poly-ester (PET) warp-knit, while the plug is made from PET and poly-lactic acid (PLA), all in monofilament form. Unique to theconstruction of the plug is a peripheral ring of resorbable hooks thatimparts self-forming and self-gripping properties. The study purposewas to evaluate and compare procedural ease-of-use and key per-formance attributes (migration, integration, inflammation) of the newParietex™ PP to the existing Bard™ Mesh PerFix™ Plug (Bard™Mesh PerFix™ P, Bard™) in a porcin model. Materials and methods: In each of 6 pigs (male), two incisionswere performed in both inguinal areas. Digital manipulation was usedto widen the internal ring to mimic a groin hernia. In each animal,one of each product type was implanted. Key performance attributeswere then macroscopically or histologically (qualitative and semi-quantitative evaluation) evaluated after 4 and 12 weeks.
Results and discussion: In preparation for and during surgery, theperipheral ring of hooks of the Parietex™ PP facilitated customizedshaping of the plug, easier suturing due to the grip of the hooks tosurrounding tissue, and good conformance to the defect after place-ment. Macroscopically, both products showed good tissue integrationwith no evidence of migration at each time period. Microscopically,the inflammatory reaction of the Parietex™ PP was of a lower gradecompared to the Bard™ Mesh PerFix™ P. Conclusion: Handling, macroscopical and histological observationsdemonstrate the excellent local tolerance and overall performance ofthe new semi-resorbable Parietex™ PP. Furthemore, compared to anon-resorbable plug & patch system, e.g. Bard™ Mesh PerFix™ P,the Parietex™ PP seems to decrease the inflammatory reaction, andpresumably reduce the extent of associated fibrosis.
P-076Laparoscopic hiatus hernia repair with Gore Bio-Amesh: A pilot studyParas Jethwa, K. Sriskandarajah, A. JamesSurrey & Sussex NHS Trust, Gastrointestinal disease, Redhill, UnitedKingdom
Background: Recurrence of hiatal defects is a frequent complication(up to 42%, Granderath 2006) after antireflux surgery. Revisional sur-gery is both technically challenging and has the potential for signifi-cant morbidity. While the use of prosthetic meshes is associated witha marked reduction in recurrence, the use of non-absorbable prostheticmaterial at the can lead potentially to catastrophic complications. Thepurpose of this pilot study was to evaluate the safety and efficacy ofa slowly absorbable mesh in the management of large and recurrenthiatal defects at the time of laparoscopic antireflux surgery (LARS). Methods: Six patients with large (>6 cm) and four patients withrecurrent hiatal defects underwent LARS with hiatal repair betweenJune 2009 and May 2010. At surgery hiatal defects were repaired byprimary cruraplasty, reinforced with a “U” shaped Gore Bio-A syn-thetic mesh. A buttress of Bio-A was used for anterior crural rein-forcement. All patients received an anterior 180 degree fundoplica-tion. Patients were evaluated postoperatively for functional outcomesand radiologically with contrast swallows at six months post surgery. Results: Mean follow up and age were 13 months (8-19 months)and 60.4 years (38-81 years) respectively. Postoperatively all patientswere able to tolerate a liquid diet with no patients requiring repeatintervention or dilatation at any point. The mean dysphagia score(Knyrim 1993) at six weeks was 0.6 and 0.3 at six months. Contrastswallows demonstrated no evidence of hernia recurrence. Despitesuccessful surgery one patient continued to have symptoms of gas-tro-oesophageal reflux but, repeat pH testing demonstrated aDeMeester score of <5. Conclusions: LARS of recurrent and large hiatal defects with Bio-A mesh is both safe & effective and, in this study, not associatedwith postoperative dysphagia or recurrence. Whilst longer term eval-uation is necessary, the use of this material appears to be well tol-erated and effective.
Fig. 1: Parietex PP - Bard Mesh Perfix P.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S60

Hernia (2011) 15 (Suppl 2): S37-S66 S61
P-078One-year results of first-in-man trial of a new syntheticlong-term resorbable mesh for inguinal hernia repairS.B. Stellan Björck1, F. Ruiz-Jasbon2, J. Norrby21 Sahlgrenska University Hospital, Department of Surgery,Gothenburg, Sweden; 2 Kungsbacka Hospital, Department of Surgery,Kungsbacka, Sweden
Background: Conventional meshes for hernia repair and abdominalwall reinforcement are usually made of polypropylene, polyester orother synthetic plastic materials known to promote foreign body reac-tions and a state of chronic inflammation that may lead to long-termcomplications. A novel approach is to use synthetic, long-termresorbable products such as the completely new TIGR MatrixSurgical Mesh. Pre-clinical studies have shown that this mesh main-tains mechanical integrity beyond the point in time where newlyformed tissue is capable of carrying the abdominal loads. Methods: This was a first-in-man, open, uncontrolled clinical studyperformed at two sites in Sweden. 40 patients with primary inguinalhernias were enrolled for Lichtenstein repair using TIGR Matrix. Theprimary endpoint was safety as assessed by monitoring the incidenceof Adverse Events and Serious Adverse Events related and unrelatedto the mesh and rehabilitation. Secondary endpoint was the perform-ance of the mesh with respect to pain and discomfort. Patients have been followed up at 0.5, 1, 3, 6 and 12 months. Long-term monitoring will be available through the Swedish hernia regis-ter. Pain assessment has been performed using a visual analogue scale(VAS 0-100) and a questionnaire in order to follow up other factorsaffecting the patients’ QOL. Results: All patients followed a normal postoperative course. After12 months, no serious adverse events were reported. Potential meshrelated complications at 12 months include one recurrence and one caseof groin muscular weakness. 3 patients experienced mild pain (VAS<10)after one year and only 4 patients could feel the presence of a meshin their groin. This compares favorably with previously publisheddata.Conclusion: Preliminary results show that the long-term resorbableTIGR Matrix Surgical Mesh is safe to use for inguinal hernia repair.Results in terms of reduced chronic pain are promising.
P-079Laparoscopic surgery of the ventral hernia: Analysis of207 casesI. Gil1, J. Deus1, J. Marin1, J. Quintana1, E. Bernal1, S. Casado1,D. Mira1, J.M. Martinez21 Universitary Hospital of Zaragoza, Surgery A, Zaragoza, Spain;2 Zaragoza University, Computer Systems and Engineering,Zaragoza, Spain
Background: The surgical treatment of ventral hernia is not alwaysaccompanied by good results, with 36% recurrence in classic sur-gery and 3-8% in laparoscopy. The use of the laparoscopic approachprovides good visualization of the hernia defect, as well as the pos-sibility to perform a tension-free reparation by placing an intraperi-toneal prosthesis. Material and methods: We present the patients diagnosed of ven-tral hernia which were operated by our surgical team betweenJanuary 2006 and December 2009. Inclusion criteria were: under fif-teen-cm diameter ventral hernias, separated more than 5 cm from the
xiphoid appendix or pubis, ASA 1 to 3. The technique used waslaparoscopic hernioplasty by means of 2 types of mesh fixation, withtackers or with fibrin. The mesh placed was always the same type(double-layer, polyethylene terephthalate, polyurethane type). Results: Two hundred and seven intraperitoneal hernioplasties wereperformed by laparoscopic approach: 175 fixed with metal tackers(GROUP A), and 32 with fibrin (14 autologous and 18 heterologous(GROUP B). Incisional hernias were 57% of the cases, whilst 43%were primary. Mean age was 54 years (range 37-79 years), mean BMI30.29 (range 24-35) and operation time 45-90 min (mean 62 min).One patient required reoperation due to subocclusion. Recurrence ratewas 2% after one-year follow up. No significant differences werefound between the 2 groups. Conclusions:1. The use of the laparoscopic approach for the treatment of ventralhernia is safe and has low complication rate.
2. Recurrence rate is similar to other published series. 3. Our results, like previous investigations, confirm the safety andeffectiveness of biological glues in mesh fixation.
P-080Reducing post-operative pain and costs in tapp procedureby using parietex progrip™. Preliminary results G. Piccinni1, G. Manca2, A. Angrisano2, A. Gurrado1, G. Lissidini1,I.F. Franco1, M. Testini11 University of Bari, Dept of Biomedical Sciences and ClinicalOncology, Bari, Italy; 2 Ospedale, A. Perrino U.O.C. ChirurgiaGenerale, Brindisi, Italy
Introduction: Laparoscopic groin hernia repair using the transab-dominal preperitoneal (TAPP) technique allows good results concern-ing post-operative pain and consequently faster full physical recov-ery to be obtained, when compared to open tension-free repairs.Some argue in favour of open repair because TAPP has increasedcosts due to trocars and fixation devices. What is more TAPPrequires a general anaesthesia. In this presentation we report our initial experience with self-gripping lightweight mesh (ParietexProGrip™- Covidien) that does not require fixation devices orglue. Materials and methods: In the period January - December 2010, 30male patients affected by both direct and indirect groin hernia were operated with a TAPP repair. 18 pts presented a bilateral hernia, 5 ptsout of 30 were affected by a recurrence and in 7 cases the repairwas primary. Patients with ASA III and IV, giant and femoral herniaswere excluded from the study. The mesh implanted was the ParietexProGrip™ mesh. No fixation devices or glues were used. We recordedoperating time, post-operative pain and full recovery of physicalactivity. Results: Mean operating time was 45 minutes (average 30-60 min).Antalgic post-operative therapy consisted of 2 administrations of30 mg i.v. of Ketorolac every 8 hours. Discharge of the patients wasalways after 24 hours in a one-day surgery regimen. We recorded3 complications in the bilateral group: 2 monolateral seroma and1 scrotal haematoma solved spontaneously. Conclusions: In our initial experience, the use of ProGrip™ meshallows us to successfully conclude the TAPP procedure in a shorteroperating time. Fixation devices or the application of glue is not nec-essary so the cost, post-operative and chronic pain are reduced. Thelight weight of the mesh is another factor that helps optimal patientcomfort to be achieved.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S61

S62 Hernia (2011) 15 (Suppl 2): S37-S66
P-081Augmented reality and 3d measurement for monocularlaparoscopic abdominal wall hernia repairI. Gil1, J. Deus1, J. Marin1, J. Quintana1, E. Bernal1, S. Casado1,D. Mira1, J.M. Martinez21 Universitary Hospital of Zaragoza, Surgery A, Zaragoza, Spain;2 Zaragoza University, Computer Systems and Engineering,Zaragoza, Spain
Background: Let be a hand-held monocular camera – or endoscope –observing an unknown rigid cavity. It is a classical result in computervision that, up to a scale factor, both a 3D cavity model (map) and thecamera location with respect to the map can be computed solely fromthe gathered image sequence. Only recently are there available algo-rithms to routinely perform this computation robustly and in real time.These algorithms collectively referred as SLAM (Simultaneous cameraLocation And Mapping). The research is focused in exploit monocularSLAM in hernia repair surgery. On one hand the defect size and hencemesh patch size is computed solely from the endoscope images. Onthe other hand augmented reality procedures to help the mesh align-ment with respect to the defect are researched. Material and methods: Translating endoscope observing the defectand a known size tool image sequence is gathered. 2 points over theknown size tools and 5 points over the hernia defect boundary areclicked. The defect is modelled as an ellipse defined by two axes.The computer estimates two axes modelling the defect and also thetwo axes defining the mesh patch. In an additional screen the endo-scope image sequence is augmented with a superimposed defect loca-tion and also the computed mesh so that the surgeon can anticipatethe region where the mesh will be located. The estimated defect sizeis compared with respect the classical measurement methods both interms of accuracy and surgical time. The utility of the augmentedreality is qualitatively assessed by the surgeons. Results: We have performed seven procedures which show the fea-sibility of the proposed method. Conclusions: SLAM makes the surgery easier, because it does pre-cise measurements, lets the surgeon check the wall defect and allowstreatment by covering it completely with the mesh.
P-082Systematic review of the use of fibrin sealant inabdominal wall repair surgeryS. Morales-Conde, M. Socas, A. Barranco, I. Alarcón, M.D. Casado,J. Cañete, I. Serrano, V. Gomez, H. Cadet, J. PadilloHospital Universitario Virgen del Rocio, General Surgery, Seville,Spain
Background: The objective was to analyse the advantages and incon-veniences associated with the use of fibrin sealant, compared to mechan-ical means, for mesh fixation following abdominal wall surgery. Data Sources: Literature search included in MedLine, EMBASE,Cochrane Library Plus databases. Articles included were randomisedclinical trials, non-randomised comparative studies, and case seriescontaining at least 10 patients. Conclusions: The fibrin sealant was shown to be biocompatible withthe surrounding tissue. In patients treated with fibrin sealant, lowerprevalence of acute and chronic post-operative pain was observed,and less haemorrhagic complications. There are no data on the influ-ence of fibrin sealant on seroma decrease. Efficiency in experimen-tal models was similar to that observed for mechanical methods offixation. Also, adhesions with fibrin sealant were less than that formechanical methods. Compared to mechanical methods, fibrinsealant is an efficacious alternative for the fixation of mesh post-sur-gery of the abdominal wall.
P-083Ex vivo mechanical response of an abdominal wall infull dayF.P. Podwojewski1, M. Ottenio1, P. Beillas1, G. Guérin2, F. Turquier2,D. Mitton11 Université de Lyon, Lyon, France; Ifsttar, UMR_T9406, LBMC;Université, France; 2 Covidien, France
Background: To improve the design of meshes for the treatment ofincisional hernias, the use of numerical models could be very helpful.However, these models need experimental data to be developedand then validated. So, an experimental protocol was developed(Podwojewski et al. EHS 2010). According to this protocol, an abdom-inal wall is subjected to different mechanical loadings, and a full dayis needed to test the specimen. Hence, the first aim of the presentstudy was to evaluate the influence of time and of the loading sequenceon the obtained mechanical response. Moreover, a hernia and a wallreparation using meshes are planned in the protocol. The second aimis to check the clinical reliability of the current protocol. Methods: Tests were performed on ex vivo porcine abdominal walls.Specimens were subjected to two loading cases: air pressure and contact loadings. The internal and the external sides of the abdomi-nal wall were simultaneously videoed to get the measurements of themaximum displacement and surface strains. An intact specimen was tested at t0 and four hours later, by switch-ing the different loadings. Other specimens were tested under threedifferent states: intact, incised, and repaired. Results: Concerning the first aim, the same mechanical response wasobtained whatever the time of the tests for the contact loading.Indeed, for a 35 mm displacement, the measured force was 300 Nat t0 and 280 N four hours later. Concerning the second aim, a hernia was well observed during airpressure loading for the incised wall, which was not the case any-more when a mesh was used. Conclusion: These experiments give us some confidence in the pro-tocol that will be used to get biomechanical data on porcine abdom-inal walls, and later on human ones.
P-085Treatment of abdominal hernias in day surgery.Training programF. Docobo Durántez, J.A. Navas Cuellar, A.G. Jimenez Riera,J.M. Suarez Grau, J. Mena Robles, F.J. Padillo RuizUniversity Hospital Virgen del Rocio, Day Surgery Unit, Seville,Spain
Background: To evaluate the surgical activity in abdominal wall her-nias in day surgery training programs in a type 2 day surgery unitof a university hospital. Methods: From January 2005 to December 2009, 10,500 patientswere operated, being 4,112 (39.30%) abdominal wall hernias whichwere anatomically located as groin (2,685), umbilical (929), epigas-tric (256), post-laparotomy (155), femoral (35), Spiegel (8) and pros-thetic rejection (15). The resident surgical program included 5 monthsin day surgery unit during their second year of training. Cure rates,morbidity, recurrence rates, return to the unit, reoperative index andsubstitution index were evaluated. Results: Postoperative follow-up period has been 1-5 years. 3,891(94.62%) consisted of hernioplasty with prosthetic material and 221(5.38%) were primary non-mesh anatomic operations. The most commonly performed anesthetic technique was local plus sedation
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S62

Hernia (2011) 15 (Suppl 2): S37-S66 S63
(3,943, 95.89%), with regional (164, 3.98%) or general (5, 0.12%)anesthesia employed in other cases. The rate of procedures performedby the resident as first surgeon relative to every location were as fol-lows: total 3,143/4,112 (76.43%); groin 1,934/2,685 (72.02%); umbil-ical 830/929 (89.34%); epigastric 240/256 (93.75%); post-laparotomy100/155 (64.51%); femoral 24/35 (68.57%); Spiegel 4/8 (50%); mesh-rejection 11/15 (73.3%). Cure index was 98.49% (4,050 patients).Global morbidity was 64 (1.55%), including pain (26), superficial sur-gical site infection (4) and bleeding (32). 19 patients returned to theunit (0.46%) and 22 (0.53%) were reoperated. The global outpatientindex was 99.69 %. When considered by groups, outpatient was99.72% for groin, 100% for umbilical, epigastric and rejection, 96.77%for post-laparotomy and 62.5% for Spiegel. The inpatient index was0.31% (13 /4112), due to pain in 6 cases (0.31%) and bleeding in7 cases (0.86%). Recurrence global rate has been 0.86% (43 patients). Conclusions: Surgical procedures in abdominal wall hernias as out-patient basis are feasible and safe in the second year training surgi-cal program.
P-086Incarcerated diaphragmatic hernia during pregnancy:A case report A. Cheragwandi1, N. Van De Winkel2, M. Vanhoeij2,K. De Vogelaere2, G. Delvaux21 UZ Brussel, Abdominal surgery, Brussels, Belgium
A 33-year-old woman was referred to the gynecology department dur-ing the 21st week of pregnancy for severe abdominal pain and exces-sive vomiting. The patient's past medical history included chronic self-inflicted vomiting, Helicobacter pylori gastritis and anterior lumbar corpectomy and fusion for an L1 burst fracture. During diagnostic work-up the patient collapsed with cardiopulmonary arrest. A successful resus-citation ensued. Despite all resuscitative measures the fetus did not sur-vive. A Total Body Computed Tomography (CT) revealed herniation ofthe stomach and small bowel in the left thoracic cavity with mediasti-nal shift to the right. A left subcostal incision was performed. A largediaphragmatic rupture was encountered with stomach, small bowel andspleen in the left thoracic cavity. Reintroduction of the organs into theabdomen revealed partial necrosis of the stomach. A partial gastrectomyand primary restoration of the diaphragmatic integrity was carried out.Postoperative course was complicated by pneumonia, empyema andAcute Respiratory Distress Syndrome (ARDS). We present this case toillustrate that even a hyperemesis gravidarum can turn out to be an indi-cation for diaphragmatic hernia repair.
P-087An unusual combination of internal hernias as a causeof intestinal obstruction: mesocolic and mesentericC. Frizis, N. Vasios, G. Komninos, R. FrizisHippokration General Hospital of Thessaloniki, 1st SurgicalDepartment, Thessaloniki, Greece
Background: Internal hernias are a rare cause of intestinal obstruc-tion with an incidence of 0.2-0.9%, which are frequently diagnosedin surgery. The most common type is paraduodenal. The less commontypes include mesocolic and transmesenteric, usually occurring after
abdominal surgery. This paper concerns a young patient with smallbowel obstruction (SBO) due to mesocolic and mesenteric hernias withnonspecific abdominal signs and no prior surgical procedures. Methods:A 27-year-old male patient with G-6-PD deficiency was admit-ted to the internal medicine department with moderate dehydration dueto vomiting for 5 days. He complained about mild epigastric distentionwith nonspecific abdominal signs from the clinical examination. Results: The diagnostic workup of the patient revealed elevated ureaand creatinine levels, rise of WBC and gastric distention (abdominalx-ray, U/S). A nasogastric tube was placed with an output of 5lt offecal content. An abdominal CT without i.v contrast or gastro-graphine due to renal failure didn’t show any signs of SBO. Afternormalization of his renal function, laparotomy was performed. Theprocedure revealed a small bowel loop through a mesocolic defect,while another loop was trapped in a second orifice with smooth bor-derlines (congenital?), at the mesenterium, causing torsion of thesmall intestine along the mesenteric axis. Both hernias were reducedand the defects were closed. The postoperative course was unevent-ful and the patient was discharged a week after surgery. Conclusions: Synchronous presence of mesocolic and transmesenterichernias causing intestinal obstruction is a very rare entity not yetdescribed in modern literature. It’s important to stress that the probabil-ity of dealing with a congenital mesenteric defect (due to its morphol-ogy-smooth borderlines) in a 27-year-old patient with no previous his-tory of abdominal complaints or surgery, increases the rarity of the case,as congenital hernias are more common in the pediatric population.
P-088Talc powderage as an effective treatment of persistentinguinal seroma J. López-Monclús, L.A. Blázquez, D.A. Melero, A. Pueyo,R. Barriga, A. Galvan, N. Palencia, A. Robin, E. Enrique,P. López-Quindós, A. Cruz, M.A. García-UreñaHenares Hospital, General and Digestive Surgery, Coslada, Spain
Background: We present a case of recurrent groin seroma after aninguinal reintervention secondary to a granuloma mesh-relatedhernioplasty treated successfully with talc powderagwe in the seromacavity. Methods:A 67 years old man with a suprapubic recurrent right groinhernia after Linchstenstein repair underwent one year ago apolypropylene mesh plug placement in the hernia defect. Chronicinguinal pain refractory to medical treatment developed as a late com-plication. The patient underwent an inguinal second look, evidenc-ing the presence of an inflammatory meshoma. Partial removing ofthe meshoma was carried out, and pubis infiltration with corticos-teroids was done before wound closure. Three days later the patientpresented a right groin fluctuant mass beneath the surgical woundwith no signs of infection, and was discharged after seroma aspira-tion. After 23 days of increasing drainage, the seroma cavity wasthoroughly dried with clean gauze swabs and 1 cc of sterilized drytalc powder was sprinkled into the seroma cavity with a 5 cc syringe.A compressive dressing was placed, and the patient was discharged. Results: One week after talc powderage, surgical wound was almostclose with a minimal oozing from the drainage incision. No adverseeffects were reported by the patient. Two weeks later, the wound wasfully healed Conclusions: Talc powderage seems to be an effective, quick, andsafe method for the treatment of inguinal seromas after inguinalhernioplasty refractory to conservative management.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S63

S64 Hernia (2011) 15 (Suppl 2): S37-S66
P-090Alloplasty of ventral wall defect when colostomy isliquidated in patients with paracolostomy herniaO.V. Chynba, V.G. Yatsentuyk, V.O. DubenetsCity Center for Hernia Surgery, Surgery, Kyiv, Ukraine
Background: Reliable and mechanically strong reinforcement of theventral wall supportive structures in the removed colostomy area inpatients with paracolostomy hernias while performing reparative-reconstructive operations on the colon. Methods: During the period of 2000 to 2010, 27 patients with para-colostomy hernias were operated on at Kyiv City Center for VentralHernia Surgery, while performing reparative-reconstructive opera-tions on the colon. There was approbated an original method for theventral wall defect closure on site of a colostomy removed with ause of polypropylene meshes in 13 patients with paracolostomy her-nias, and its efficacy was compared with 14 patients operated onusing autoplasty (the control group).Results: The use of autoplastic methods for the ventral wall defectclosure, while performing the colostomy removal in patients withparacolostomy hernias, resulted in hernial recurrences in about thirdof the patients operated on in such a way. The immediate and remote results of surgical treatment in patientswith paracolostomy hernias, which had had reparative-reconstructiveoperations on the colon, demonstrated high efficacy of the methodproposed for alloplastic closure of the ventral wall defect on site ofa colostomy removed. Complications on the wound side were onlyobserved in one (7.6%) patient in form of serous wound inflamma-tion; no case of hernial recurrence was revealed. Conclusions: The method proposed for allohernioplasty of the ven-tral wall colostomy defect allows for reliable reinforcement of theventral wall with a polypropylene mesh fixed to supportive structureswithin submuscular space, and reduces significantly the number ofboth hernial recurrences and postoperative complications on woundside.
P-091Results of a prospective, multicentric clinical studyevaluating the INTRA-SWING IS120 and IS210dual-side mesh for an intraperitoneal repair on34 patientsP. Bourdonnec, D. DelarueCHP Saint Grégoire, Digestive Department, Rennes, France
A prospective multicentric study was set up in order to evaluate until48 months post-surgery, the efficacy and the safety of the INTRA-SWING (Swing-Technologies) meshes in the treatment of umbilical,incisional or ventral hernia. The INTRA-SWING' meshes are madeof polyester coated on one side with a thin membrane of poly(etherurethane). We are reporting data of 34 patients treated between 2005 and 2008.The data include demographic, per-operative data as well as theresults of the follow-up visits. INTRA-SWING mesh was positioned intraperitoneally by laparoscopyor laparotomy. The mean age of the patients was 63.7 years old and58.8% of them were women. Half of the patients was on overweightor presented a moderate obesity. Thirty (30) patients were treated foran incisional or ventral hernia (88%) and for 10 patients, it was arecurrence.
Two patients were withdrawn of the study for surgical strategy mod-ification. The IS120 and IS 210 implants were respectively used in29 and 3 patients. All of them were fixed. The mean surgery lengthwas 73 minutes. Three recurrences (9.4%) were observed in the study. Among them,2 were associated with a second recurrence with one patient havinga BMI>50. A total of 12 complications were reported during the study. Amongthem, we observed: • 3 hematoma one of whom induced an infection leading to theimplant removal,
• 1 seroma associated with a patient discomfort, • 2 infections related with 2 recurrences. At 2 years of follow-up, the comfort is satisfactory with 7% of painat rest and 17% of pain during effort. The easiness to introduce themesh in a trocar was judged satisfactory. In conclusion, no complication implicates the safety of the patients orthe benefit-risk ratio. Indeed, the intraperitoneal technique is recom-mended for patient at risk. Obesity is generally a recurrence factor.
P-092Italian register of umbilical hernia treatment (RIEO)M.G. MuziPoliclinico Tor vergata, Chirurgia Generale, Rome, Italy
Background: In Italy about 11.000 surgical interventions are per-formed for treatment of umbilical hernia every year, about 5% of thehernia pathology variety. The direct suture procedure is performed especially for the treatmentof little size hernias (<3 cm) with an unacceptable incidence of recur-rences about 30-40%. Methods: In the last Winter EHS Meeting, M.G. Muzi championedan Italian Register of umbilical hernias (RIEO), in that register everyumbilical hernia, should be noted with its surgical technique andprosthetic materials. to verify the treatment of this patology. The mainend points will be represented by the recurrence rate, the pain andthe postoperative outcomes. All members of Italian Chapter of EHS were invited to participateto RIEO sending a mail ([email protected]) withthe request of participation, they will receive a questionnaire tofill in and a protocol of collection of retrospective and prospectivedata. Result: The repair of umbilical hernia can be performed with tradi-tional surgical approaches or laparoscopic techniques; with a directsuture or with the interposition of a prosthesis. A great variety ofprosthetic materials are available. The choice of a surgical interven-tion to perform is often suggested by circumstantial factors rather areal knowledge of all therapeutic possibilities and prosthetic materi-als. For this reason it’s very difficult to compare the different ther-apeutic procedures. Conclusion: The purpose of RIEO is monitoring the umbilical hernia treatment in Italian centres associated to EHS to reach a better knowledge of the disease both from quantitative and qualitativepoint of view being low the reported cases for every surgical unit.The results could allow randomized and perspective studies to iden-tify the most convenient surgical intervention for umbilical hernia treatment. At present 15 centers joined to RIEO providing preliminary data of2009 concerning 257 patients.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S64

Hernia (2011) 15 (Suppl 2): S37-S66 S65
P-093Laparoscopic ventral hernia repair, experience in ateaching hospitalD. Hussain, R. Hartung, Z. AbdelazizDubai Hospital, Surgery, Dubai, United Arab Emirates
Background/Objective: To determine the outcome of patients afterlaparoscopic ventral hernia repair. Patients and methods: All patients above 13 years of age, whounderwent laparoscopic ventral hernia repair, were included. The dataof these patients was collected retrospectively from January 2007 toDecember 2008. Results: There were 19 patients. Their mean age was 46 years. Therewere 15 female and 4 male patients. All patients presented withabdominal wall swelling, 13 patients had pain. The hernia was par-tially reducible in 9 patients, and completely reducible in 10 patients.Five patients had hypertension, 4 had ischemic heart disease, and3 had obesity as co morbid conditions. All patients underwent laparo-scopic hernia repair with proceed dual mesh. The mean defect sizeof the hernia was 4 cm, and mean duration of surgery was 99 min-utes. Early post operative complications included, seroma in2 patients, and haematoma in one patient. The mean follow up was12 months. Four patients have pain at the site of hernia. Conclusion: laparoscopic ventral hernia repair has less wound complications, and is an appropriate approach in many patients.
P-094Results in tep vent/inc.herB. Radovanovic, M. CudomirovicGeneral hospital, Surgery, Pozarevac, Serbia
Background: During last twenty years open Rives-Stoppa repairbecome standard for repair of incisional hernias. Endoscopic retro-muscular approach offers advantages of minimal invasive surgery. Material and method: Between April 2003 -September 2010 we per-formed 54 operations in selected cases. We operated patient with her-nia diameter les the 10 cm. Patients with symptoms of chronic andacute incarceration were excluded, but some of operated patients hadirreducible hernias. The age of patients was between 42 and78 years, BMI 38 kg/m2. We had twenty eight ventral and 26 incisionalhernias. We used lateral approach in all cases. Three ports et the levelof semi-lunar line, 0 mm for laparoscop, and two 5 mm for workinginstruments. The troacars are inserted under the rectus muscle andworking space is created by insuflation and blunt dissection. Dissection of hernia sack is sometimes difficult and peritoneum tearsespecially in cases of umbilical hernias. After opposite retro muscularspace is created we placed mesh of adequate size. With suture- passermesh is fixing transcutaneusly in all corners. We always put a drain.Results: 88% of patients were evaluated. Erly complication: Few hematomas in subcutaneous plan. One conversion (second case) with addition of small incision for correctplacement and fixation of mesh. One small bowel injury with second open operation. Two recurrensin incisional hernia group, both in first postoperative year. Remote results: No recurrence after first year. Very low postopera-tive pain and discomfort. In two cases late excision of skin for cos-metic reasons (umbilical hernias).Conclusion: Besides we are still in the learning curve, we can saythat this approach can be used in all cases of small and mediumsized hernias, specially in the middline. We can use broad spectrumof meshes, and fixations is easy and chip.
P-095A collective review on mesh-based repair of umbilicaland epigastric herniaS.W. Nienhuijs, J. PontenCatharina Hospital Eindhoven, Surgery, Eindhoven, Netherlands
Background: In accordance with the tension-free principles in otherhernia repair, umbilical and epigastric hernia should be repaired mesh-based. The number of randomized studies is increasing, most of themshowing significant less recurrences with the use of a mesh. Thereforedifferent devices are available, placed by different approaches. Theobjective of this review is to evaluate recent literature for the differentmeshes to treat the umbilical / epigastric hernia and their outcomes. Methods: A multi-database search was conducted to reveal relevantstudies since 2001 reporting a mesh-based umbilical/epigastric her-nia repair and their outcome in adult patients. Results: A total of 19 studies was included, fourteen of them solelyincluded umbilical hernias, whereas the remaining also included theepigastric or sometimes incisional hernias. A median of 103 (range25-384) patients were described per report. Three-quarters of them hada follow-up of at least 2 years. Five studies described the results oflaparoscopic approach. Used meshes were polypropylene, PTFE,Parietex polyester® and Goretex patch®. In one study a recurrence rateof 2.7% was found, the remaining studies reported no recurrences. Intwo comparative studies, lower incidences of complications and post-operative pain were reported than after open repair. Sixteen studiesreported results of open mesh-based repairs. Devices in this approachwere the Prolene Hernia System®, Ventralex®, plug, polypropylene orPTFE and Vypro® for retromuscular repair. In six studies no recurrencewere found after mesh repair. Other reported rates up to 3.1% recur-rences. For complications a wide range of 0 to 33% was reported. Conclusion: This collective review showed acceptable recurrencerates for mesh-based umbilical/epigastric hernia repair. The range inused devices was wide. There was a tendency for more complica-tions after open repair in comparison to laparoscopic repair.
P-096Tension-free open hernia repair using CA.B.S.’ AirEndoprosthesis: Clinical resultsB.Sh. GogiaA.V.Vishnevsky Institute of Surgery, Plastic Surgery, Moscow, RussianFederation
Background: In the last 10 years new generation of endoprostheseswith more biocompatibility, low price and simple handling has beenappeared. It led to their more often usage in surgical practice thus stim-ulating changes in methods of ventral hernia treatment. Such methodsallowed to perform ventral hernia plastics preserving normal anatomywithout tension leading to reduction of incisional complications afterconventional surgery. The aim of investigation was to estimate the results of ventral herniatreatment with CA.B.S.’Air (Cousin Biotech, France) endoprostheses. Methods: From 2004 till May 2010 we performed 24 surgical inter-ventions with application of CA.B.S.’Air endoprostheses in patients withumbilical hernias - 9, inguinal - 9, spigelial line - 2, small incisionalhernias - 2 and port-site hernias - 2. In common, patients were aged3¬7-83 (in average 63±2,4). Local anaesthesia was performed in 15cases, epidural anaesthesia - in 5 and general anaesthesia - in 4 cases. Results: Postoperative course was without complications. No casesof endoprostheses’ rejections. No recurrent cases in long-term obser-vations (from 6 months till 6 years). Conclusions: CA.B.S.’ Air endoprosthesing in small hernia gates isa safe, quickly performed method with excellent long-term results.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S65

S66 Hernia (2011) 15 (Suppl 2): S37-S66
P-097TiMesh in the treatment of ventral herniasV.P. Pejcic, T.B. BojicClinical Center Nis, Center For Minimally Invasive Surgery, Nis,Serbia
Background: “TiMesh is a monofilament, composite mesh combin-ing polypropylene with a covalent bonded titanized surface and it’sdemonstrates a high degree of biocompatibility. Optimal mesh fea-tures include those with a low potential for reactivity and inflamma-tory response”. The aim of this study is to present our experience inapplication of this type of mesh. Method: In period of 5 years (2005-2010 year), 85 patients withventral hernias were operated with using the TiMesh. All patientshad an antibiotic prophylaxis (Cefazolin 2.0g). There were 45 her-nias with supraumbilical localization (53%), 32 with umbilical local-ization (38%), and 8 (9%) combined epigastric and umbilical her-nias. Defect size was ranging from 5x5 to 20x10 cm. Mesh size wasranging from 15x15 cm to 30x30 cm. Rives-Stoppa technique wasused in 75 cases and Chevrel technique in 10 cases. We have ana-lyzed: operating time, postoperative complications, time beforereturning to work, and a number of recurrences. Results: Average operating time was 65 minutes (45-145 minutes).Median age was 55 year (from 32 to 70). All patients were ASA I, IIand in selected cases ASA III. In local anesthesia were operated42 patients and in OET 43 patients. There were no intraoperative complications. Follow up period was from 1 to 6 years. Postoperativelywe had 3 recurrences (3.5%), 3 hematomas and 3 seromas. Also,1 wound infection (1.2%) which was treated conservatively. Allpatients returned home after 7 days (1 to 12 days). All patients gotback to normal activities in 20 days (15-32 days). Only 45 patients(1.8%) needed postoperative analgesia. Conclusions: Operative treatment of abdominal wall hernias with usethe TiMesh is effective and safe method with low rate of recurrenceand postoperative complications. Recurrence and wound infection ratewas significantly lower than with other types of meshes.
P-099Surgical management of abdominal wall hernias inadults: our experienceP. Milosevic, M. KolinovicGeneral Hospital “Danilo I”, Cetinje, Montenegro
The goal of our study is to perform a detail epidemiological analy-sis of the surgical management of abdominal wall hernias in our hos-pital and present our experiences in this field as well as to comparethe obtained results with the actual data from the literature. This retrospective study included 964 patients who underwent surgicaltreatment for abdominal wall hernia during a 5-year period (from 2005to 2010) in a General Hospital “Danilo I” in Cetinje, Montenegro.Data (gender, age, localization and type of hernia and some othercharacteristics, operative technique, type of anesthesia) were obtainedfrom medical documentation and statistically analyzed.The study included 741 (76.87%) male and 223 (23.13%) femalepatients (M: F=3:1). Total number of surgicaly treated hernias was 1,101.There were 861 (78.20%) primary, 92 (8.36%) recurrent and 148(13.44%) postoperative hernias.Two hundred ninety nine (27.16%) hernias were incarcerated. There was statistically significant difference between frequencies ofdirect and indirect inguinal hernias in patients of both genders(p<0,05). Indirect hernias were more frequent. Umbilical herniaswere more common in men while infraumbilical hernias were morefrequent in female patients. Statistically significant difference wasfound between frequencies of primary and postoperative ventral hernias in patients of both genders (p<0.05). In the examined patients with inguinal hernias, appendix was foundinside hernial sac in 0.3% of patients. One patient had right-sidedinguinal hernia with urinary bladder in the hernial sac.Early postoperative complications occurred in 335 (34.75%) patients.The most common was seroma which was reported in 290 (30.08%)patients. Polypropylene mesh extirpation was performed predomi-nantly in patients with inguinal hernias.Lichtenstein and Rives/Stoppa techniques were most commonly per-formed. The major advantages of the tension-free mesh repair wereless pain, shorter postoperative recovery and rare hernia recurrence.Tension methods were associated with a lower frequency of seromaand infection.
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S66

Hernia (2011) 15 (Suppl 1): S67-S70
AUTHOR INDEX
Author Index
© Springer-Verlag 2011
Abdelaziz Z., P-093, S65Abuzaina F., O-123, S28Acosta S., O-076, S17Agee N., P-073, S59Agrusa A., O-094, S21, P-031, S46Aguilera A., P-070, S58Airo I., O-014, S4Akagi S., P-030, S46Alarcón I., O-031, S9, O-145, S33,P-082, S62Alonso P.A., O-045, S12Althaus A., O-144, S32Amato G., O-094, S21, P-031, S46Andreadis I., P-026, S45Andreoli F., O-091, S20Angrisano A., P-080, S61Angulo Morales F.J., P-048, S52,P-069, S58Antic A., P-047, S52Anurov M.V., O-122, S27Apostolidis S., P-026, S45,P-063, S56Arenillas M., P-069, S58Ashwin H., O-124, S28, P-002, S37Baburin A.B., P-015, S41,P-032, S47Banerjee A., O-132, S31Barranco A., O-031, S9,O-108, S24, O-145, S33,P-082, S62Barriga R., O-015, S4, O-112, S25,P-070, S58, P-088, S63Barthes T., O-010, S2, O-026, S7Basaric D., P-040, S50Baumann M., O-121, S27Bay-Nielsen M., O-134, S31Bayon Y., O-124, S28, P-002, S37,P-072, S59Beatovic N., P-036, S48
Beillas P., P-083, S62Bekavac Beslin M., P-016, S42Bellandi D., O-045, S12Bellido J., O-145, S33Bellido Luque A., O-107, S23Belyansky I., O-012, S3,O-120, S27, O-148, S34,P-001, S37, P-051, S53Bencini L., O-032, S9, P-065, S56Berger E., O-045, S12Bernal D., O-031, S9Bernal E., P-079, S61, P-081, S62Bernini M., O-032, S9, P-065, S56Berrevoet F., O-033, S9,O-051, S12, O-075, S17,O-078, S18, O-126, S29,P-022, S44, P-042, S50,P-054, S54Berselli M., O-106, S23Bertocchi V., O-087, S19Bertolaso W., P-020, S43Bertrand C., O-033, S9Berwouts L., O-033, S9Bianchi V., O-106, S23Bielesch E., P-023, S44Bisgaard T., O-134, S31Bjarnason T., O-076, S17Bjelajac D., P-036, S48Björck M., O-076, S17Björstad J., O-146, S33Blázquez L., O-015, S4, P-070, S58,P-088, S63Bloemen A., O-004, S1, O-129, S30Boffi B., O-032, S9, P-065, S56Bogdanovic D., P-025, S45Bojic T., P-025, S45, P-097, S66Bojovic P., O-025, S7Bonjer H.J., O-074, S17,O-143, S32
Bontinck J.S.B., O-048, S12Born H., P-014, S41Bourdonnec P., P-091, S64Brancato G., P-053, S54Brand J., O-068, S15Brandsma T., O-083, S19Brandt C.J., P-007, S39, P-068, S57Brankovic M., O-025, S7Brinck T., O-014, S4Bringman S., O-148, S34Broos P., O-149, S34Browet F., O-095, S21Bryan N., O-124, S28, P-002, S37,P-072, S59Bucek J., P-008, S39Buffin M., P-075, S60Bulajic P., P-040, S50Bussani R., P-031, S46Buunen M., O-074, S17Byrd J.F., P-073, S59Cabunac P., O-025, S7Cadet H., O-145, S33, P-082, S62Cadet J.M., O-031, S9, O-108, S24Cadwallader R.A., O-132, S31Cagas J., O-049, S12, P-008, S39,P-009, S40Calistri M., P-065, S56Campanelli G., O-087, S19Cañete J., O-031, S9, O-108, S24,O-145, S33, P-082, S62Canziani M., O-087, S19Capov I., O-049, S12, P-009, S40Carbonell A.M., O-117, S26Carpenter C.L., O-012, S3,P-056, S54Casado M.D., O-108, S24,O-145, S33, P-082, S62Casado S., P-079, S61, P-081, S62Casaer J., O-030, S9
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S67

S68 Hernia (2011) 15 (Suppl 2): S67-S70
Castro Cabezas M., P-043, S51Cavalli M., O-087, S19Ceriani F., O-087, S19Cesana G., O-077, S18, P-018, S42,P-037, S49Ceulemans R., O-043, S11Cheragwandi A., P-086, S63Chiapponi C., O-016, S4Chitre V., P-033, S47Chynba O.V., P-090, S64Ciangola C.I., O-091, S20Cijan V., O-025, S7Claeys D.A., O-048, S12Clay L., P-012, S40Cobb W., O-010, S2, O-026, S7Coco C., O-022, S6Cocozza E., O-106, S23Conze J., O-079, S18, O-114, S25Crea N., O-137, S32Croce E., O-077, S18, P-018, S42,P-037, S49Cruz A., O-015, S4, P-070, S58,P-088, S63Cudomirovic M., P-094, S65Dabic D., P-028, S46Dacey K.T., P-051, S53Dahlstrand U., O-024, S7D'Ambra L., P-064, S56Daniels I.R., P-061, S55De Backer T., O-033, S9De Goede B., O-131, S31De Gols J., O-033, S9De Haas R., P-013, S41De Keukelaere I., O-030, S9De Luca E., O-091, S20De Man R.A., O-131, S31De Smet B., P-042, S50De Vogelaere K., P-086, S63Deerenberg E.B., P-050, S53Deguines J.B., O-116, S25Delarue D., P-091, S64Delvaux G., P-086, S63Delvaux P., O-033, S9Deseyne P., O-078, S18Deus J., P-079, S61, P-081, S62Ditzel M., O-125, S29, P-003, S38Djavani K., O-076, S17Djordjevic M., P-025, S45Docobo Durántez F., P-029, S46,P-085, S62Doebler O., O-111, S24Doerhoff C., P-074, S60Doka A., O-057, S13, P-049, S52Donati A., P-053, S54Donati M., P-053, S54Donker H., O-121, S27Doucet G., P-075, S60Dubenets V.O., P-090, S64Dumanian G.A., O-042, S11,O-093, S21
Dunn R.M., O-013, S3, O-029, S8,P-006, S39Durán Ferreras I., O-107, S23Edamoto Y.M., P-027, S45Efthymiou G., P-035, S48Eker H.H., O-074, S17, O-131, S31,O-143, S32, P-043, S51Eklund A., O-023, S6Emanuelsson P.M., O-072, S16Enrique E., O-015, S4, P-070, S58,P-088, S63Farassino L., O-106, S23Farsi M., O-032, S9Fernandez Lobato R., P-048, S52,P-069, S58Fiebeler A., P-007, S39Filipovic J.F.C., P-016, S42Floyd D., P-066, S57Fortelny R.H., O-053, S13,O-068, S15, P-011, S40Fourneau I. , O-149, S34Franco I.F., P-080, S61Fränneby U., O-146, S33,P-012, S40Frizis C., P-087, S63Frizis R., P-087, S63Galun D., P-040, S50, P-047, S52Galvan A., O-015, S4, P-070, S58,P-088, S63García J., O-107, S23Garcia Septiem J., P-048, S52,P-069, S58García-Ureña M.A., O-015, S4,O-112, S25, P-070, S58,P-088, S63Getz S.B., O-012, S3, P-051, S53,P-056, S54Gil I., P-079, S61, P-081, S62Giles D., O-010, S2, O-026, S7Gillion J.F., P-038, S49Gingell-Littlejohn M., O-023, S6Gkanas P., P-035, S48Glaser K., O-068, S15Gluhovic A., P-036, S48Goderich Lalan J., P-034, S48Goetze T., O-094, S21Gogia B.Sh., P-096, S65Gomez V., O-145, S33, P-082, S62Gomez Menchero J., O-107, S23Gong D.Q., O-063, S14Gontijo C.E.S., P-045, S51Goossens R.H.M., P-050, S53Gopinath B., O-132, S31Gradusov V.P., P-015, S41,P-032, S47, P-062, S56Gruber-Blum S., O-068, S15Gu Y., O-063, S14Guerin G., P-058, S55, P-083, S62Guffanti E., O-106, S23Guimaraes L.L.B., P-071, S58
Guimarães L.M.V., O-045, S12Gulotta G., O-094, S21, P-031, S46Gunnarsson U, O-024, S7,O-058, S13, O-146, S33,P-012, S40Gurmu A., O-058, S13Gurrado A., P-080, S61Guyader D., O-123, S28, P-075, S60 Hadba A.R., O-123, S28Hammond R.M.S., P-033, S47Hansson B.M.E., O-074, S17,O-080, S19 Harlaar J.J., P-043, S51, P-050, S53 Hartung R., P-093, S65Hayashidani N., P-030, S46Hayashidani Y., P-030, S46Heath J.J., P-073, S59Heniford B.T., O-012, S3,O-120, S27, O-148, S34,P-001, S37, P-051, S53,P-056, S54Herrero J., P-069, S58Hinrichs-Rocker A., O-144, S32Hlavacek C.M., O-012, S3,P-056, S54 Hoofwijk A.G.M., O-004, S1,O-129, S30Hop W.C., O-074, S17, P-043, S51 Hopson S.B., P-060, S55Huizinga B.F., O-004, S1,O-129, S30Hunt J.A., O-124, S28, P-002, S37,P-072, S59Hurwitz Z.M., O-013, S3,O-029, S8, P-006, S39Hussain D., P-093, S65Iannitti D.A., P-073, S59Ignotz R., P-006, S39Imber C., P-066, S57Jacobs I., O-043, S11James A., P-076, S60Janssen I.M.C., O-074, S17Jeekel J., O-074, S17, O-143, S32,P-043, S51, P-050, S53Jerabek J., O-049, S12, P-008, S39,P-009, S40Jethwa P., P-076, S60Jimenez Riera A.G., P-029, S46,P-085, S62Johanet H., O-010, S2, O-026, S7Jovanovic B., P-025, S45Jovanovic D., P-036, S48Jovanovic S., P-025, S45 Jurado J.G., O-107, S23Justinger C., P-057, S55 Kammer D., P-007, S39 Kandachar P., P-050, S53 Kassai M., O-057, S13, P-049, S52Kazemier G., O-131, S31 Kehlet H., O-134, S31
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S68

Hernia (2011) 15 (Suppl 2): S67-S70 S69
Khan D., P-061, S55 Khodak V.A., P-015, S41,P-032, S47, P-062, S56Kingsnorth A.N., O-023, S6,O-034, S10Kirac I., P-016, S42Kitowski J., O-096, S22Kiudelis M., O-006, S1 Klein P., P-057, S55 Kleinrensink G.J., P-050, S53 Klima D.A., O-012, S3, O-148, S34,P-051, S53, P-056, S54Klinge U., O-021, S5, O-121, S27,O-142, S32, P-007, S39Klitsie P.J., O-074, S17, O-131, S31,O-143, S32Koch A., O-028, S8, O-069, S15,O-070, S15, P-014, S41Kolinovic M., P-099, S66 Komninos G., P-087, S63 Korica M., P-036, S48 Krämer N., O-121, S27 Kuhl C., O-121, S27 Kühnert N., O-121, S27 Kulis T., P-016, S42 Kullman E., O-023, S6 Kumar S., P-021, S43Kurisu Y., P-030, S46 Ladurner R., O-016, S4, P-041, S50Lafullarde T., O-033, S9 Lambropoulos P., P-035, S48 Lange J.F., O-074, S17, O-131, S31,O-143, S32, P-043, S51,P-050, S53Langeveld H.R., O-143, S32 Laqua D., P-023, S44 Latham L., O-106, S23 Lau K.N., P-073, S59 LeBlanc K.A., O-073, S16,P-067, S57 Lefering R., O-144, S32 Lepere M., O-010, S2, O-026, S7 Light D., O-132, S31 Limones Esteban M., P-048, S52 Lin L., O-075, S17 Lincourt A.E., O-120, S27,O-148, S34, P-001, S37,P-051, S53, P-056, S54Linsenmaier U.L., P-041, S50 Lissidini G., P-080, S61 Livraghi L., O-106, S23 Lomanto D., O-020, S5López-Monclús J., O-015, S4,O-112, S25, P-070, S58,P-088, S63López-Quindós P.J., O-015, S4,O-112, S25, P-070, S58,P-088, S63Lorenz R., O-028, S8, O-069, S15,O-070, S15, P-014, S41
Lundström K.J., O-027, S8Luque J.B., O-107, S23Lutsenko N.S., O-127, S29Magne E.M., P-020, S43Maleckas A., O-006, S1Manca G., P-080, S61Manno A.M., O-022, S6Maric B., P-028, S46Marin J., P-079, S61, P-081, S62Marin Lucas F.J., P-048, S52Martin T.R., O-120, S27, P-001, S37Martinez J.M., P-079, S61,P-081, S62Martinie J.B., P-073, S59Mascianà G., O-022, S6Massalis J., P-035, S48Matthews B., O-010, S2, O-026, S7McKillop I.H., P-073, S59McRoy L., O-075, S17, O-148, S34Meir E., O-033, S9Melero D.A., O-015, S4,O-112, S25, P-070, S58,P-088, S63Melo R.M., P-004, S38, P-005, S38,P-045, S51, P-071, S58Mena Robles J., P-029, S46,P-085, S62Mendes F.F., P-071, S58Menezes L.B., P-005, S38Mensah E., O-116, S25Mesquita Fernandes H., P-019, S43,P-024, S44Metselaar H.J., O-131, S31Meyer A., O-045, S12, P-017, S42Michiels M., O-043, S11Mihara F.M., P-027, S45Mijic A., P-016, S42Milicevic M., P-040, S50Milosevic P., P-099, S66Mira D., P-079, S61, P-081, S62Miserez M., O-023, S6, O-092, S20Mitchell J., O-075, S17Mitton D., P-083, S62Molina Fernandez E.J., P-034, S48Monteiro O., O-045, S12Montero P.N., P-001, S37Montgomery A., O-098, S23Moraes A.M., P-071, S58Morales-Conde S., O-031, S9,O-108, S24, O-145, S33,P-082, S62Moretti R., O-032, S9, P-065, S56Morkane C., P-066, S57Morris L.M., P-067, S57Moser K.H., O-144, S32Moysis J., P-035, S48Mussack T., O-016, S4, P-041, S50Muysoms F., O-033, S9,O-048, S12, O-118, S26Muzi M.G., O-091, S20, P-092, S64
Mylytsya K.M., O-067, S15,O-127, S29Mylytsya M.M., O-127, S29Narula V., O-010, S2, O-026, S7Nasvall P., O-058, S13Navas J.A., O-031, S9, O-108, S24Navas Cuellar J.A., P-029, S46,P-085, S62Navez B., O-033, S9Neto Santos T., P-024, S44Neugebauer E., O-144, S32 Nienhuijs S.W., O-008, S2,O-023, S6, O-071, S16,O-147, S33, P-010, S40,P-095, S65Nigro C., O-091, S20 Noceti A., O-044, S11, O-110, S24,O-109, S24Nordin P., O-027, S8 Norrby J., P-078, S61 Novitsky U., O-010, S2, O-026, S7 Novotny T., P-008, S39, P-009, S40 Nussbaumer P., O-037, S11 O’Brien J., O-013, S3, O-029, S8 Oettinger A., O-122, S27 Olmi S., O-077, S18, P-018, S42,P-037, S49Oppong F.C., O-034, S10 Ottenio M., P-083, S62 Otto J., O-121, S27 Ovens L., P-066, S57 Paajanen H., O-014, S4 Padillo F.J., O-031, S9, O-108, S24,O-145, S33, P-029, S46,P-082, S62, P-085, S62Pafundi D.P., O-022, S6 Pagoni E., P-035, S48 Palencia N., O-015, S4, O-112, S25,P-070, S58, P-088, S63Palibrk I., P-040, S50 Pålsson B., O-076, S17 Paolucci V., O-094, S21 Parshikov V.V., P-015, S41,P-032, S47, P-062, S56Pata G., O-137, S32 Pattyn P.R.L., O-030, S9 Paulo N.M., P-004, S38, P-005, S38,P-071, S58Pavlovic A., P-025, S45 Peeters E., O-092, S20 Pejcic V., P-025, S45, P-097, S66Penhavel F.A.S., P-045, S51Perata O., O-044, S11, O-109, S24,O-110, S24Perunicic V., P-028, S46Petersson U., O-076, S17,O-097, S22Petrov V.V., P-015, S41, P-032, S47,P-062, S56Petrovic D., P-036, S48
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S69

S70 Hernia (2011) 15 (Suppl 2): S69-S73
Petter-Puchner A.H., O-068, S15Piccardo A., O-044, S11,O-109, S24, O-110, S24Piccinni G., P-080, S61Pierik E.G.J.M., O-074, S17Pijanovic N., P-028, S46Pinckney C., P-061, S55Podwojewski F.P., P-083, S62Pokora W.J., O-096, S22Pokusevski G., P-036, S48Ponsky J., O-010, S2, O-026, S7 Ponten J., P-095, S65 Protic M., P-036, S48 Pudar Z., O-025, S7 Pueyo A., O-015, S4, O-112, S25,P-070, S58, P-088, S63Pulvirenti E., P-053, S54Qassemyar Q., O-095, S21 Quintana J., P-079, S61, P-081, S62 Radovanovic B., P-094, S65 Rajkov B., P-036, S48 Rakic S., O-128, S30, P-013, S41 Ranoya M.A.A., O-045, S12 Ratnasingham K., O-132, S31 Ratto E.L., O-044, S11, O-109, S24,O-110, S24Raymakers J.F.T.J., O-128, S30,P-013, S41 Redl H., O-068, S15 Régimbeau J.M., O-095, S21,O-116, S25 Reinpold W.M.J., O-130, S30,P-044, S51Reynvoet E., O-051, S12,O-126, S29, P-054, S54Rizzo G., O-022, S6Robbe M., O-095, S21Robin A., O-015, S4, O-112, S25,P-070, S58, P-088, S63Rodrigues D.F., P-004, S38,P-071, S58Rogiers X., O-078, S18,O-126, S29, P-022, S44,P-042, S50, P-054, S54Romano G., O-094, S21, P-031, S46Romanov R.V., P-015, S41,P-032, S47, P-062, S56Romanowski C., O-148, S34 Rosen M., O-010, S2, O-026, S7Rosman C., O-008, S2, O-071, S16Rotkov A.I., P-015, S41 Ruiz-Jasbon F., P-078, S61 Ruppert M., O-033, S9 Sabbagh Ch., O-116, S25 Saladino V.A., O-094, S21,P-031, S46Salamone G., O-094, S21,P-031, S46Samsonov A.A., P-015, S41,P-032, S47, P-062, S56
Samsonov A.V., P-015, S41,P-032, S47, P-062, S56Sanchez L.J., O-032, S9, P-065, S56Sandblom G., O-024, S7, O-027, S8,O-146, S33, P-012, S40Sanders D., O-036, S10Santos Costa C., P-019, S43,P-024, S44Scarborough N., P-072, S59v
Scepanovic M., O-025, S7Scheuerlein H., O-010, S2,O-026, S7Schilling M.K., P-057, S55Schoenmaeckers E.J.P., O-128, S30,P-013, S41Schröder M., P-044, S51Schülenberg E., O-023, S6Serrano I., O-031, S9, O-108, S24,O-145, S33, P-082, S62Shankar A., P-066, S57Shipp J., O-120, S27, P-001, S37Shklyar I., P-057, S55Sibamura H., P-030, S46Silva A.S., P-004, S38, P-005, S38,P-071, S58Silva D.B., P-071, S58Silva L.S., P-004, S38, P-005, S38,P-071, S58Simons M.P., P-068, S57Sindram D., P-073, S59Skipworth J.R.A., P-066, S57Slabu I., O-121, S27Smart N.J., O-124, S28, P-002, S37,P-061, S55, P-072, S59Smedberg S.G.G., O-027, S8,O-060, S14Smeds S., O-023, S6Smeets P., P-042, S50Smet B., O-030, S9Smietánski M., O-096, S22Smith I., O-057, S13, P-049, S52 Snoeck E., P-022, S44Socas M., O-031, S9, O-108, S24,O-145, S33, P-082, S62Soler M., O-046, S12, P-039, S49 Sommeling C., O-035, S10Souza J.M., O-093, S21Sriskandarajah K., P-076, S60Staal J.F., O-071, S16Staelens C., P-022, S44Stechemesser B., O-111, S24Steinhilper U., P-023, S44Stellan Björck S.B., P-078, S61Steyerberg E.W., O-143, S32Stirler V., O-128, S30, P-013, S41 Stocker U., O-016, S4Stokidis S., P-035, S48Strigård K., O-058, S13, P-012, S40 Strobbe L.J.A., O-071, S16
Suarez Grau J.M., O-107, S23,P-029, S46, P-085, S62Svensson M., O-076, S17Swan R.Z., P-073, S59Tanaka T., P-030, S46Tang R., O-063, S14Teget P., P-074, S60Teixeira D., P-024, S44Testini M., P-080, S61Thomas J., O-123, S28Thomassen I., O-147, S33,P-010, S40Tilanus H.W., O-131, S31Titkova S., O-122, S27Tollens T., O-033, S9Tomas R.N., P-045, S51Tovar D., O-107, S23Tran H.M., O-011, S3 Troisi R., O-078, S18, O-126, S29,P-022, S44, P-042, S50,P-054, S54Tsiripidis O., P-026, S45 Tsirline V.B., O-012, S3,O-120, S27, O-148, S34,P-001, S37, P-051, S53Tucci G., O-091, S20 Turquier F., P-058, S55, P-083, S62 Uzzaman M.M., O-132, S31 Vakalopoulos K.A., P-043, S51 Van Breemen E., P-050, S53 Van De Winkel N., P-086, S63 Van der Ham A.C., P-043, S51 Van Dooren P., O-004, S1,O-129, S30 Van Suijlekom H., O-147, S33 Vanhoeij M., P-086, S63 Vanlander A., O-078, S18,O-126, S29, P-022, S44,P-042, S50, P-054, S54Vasios N., P-087, S63Veljkovic R., P-036, S48Venclauskas L., O-006, S1Verbo A., O-022, S6Verhaeghe P., O-095, S21,O-116, S25Vertegel A., O-120, S27, P-001, S37Vrijland W.W., P-043, S51Vuylsteke P., O-030, S9Wałecka J., O-096, S22Wanhainen A., O-076, S17Wiese M., P-014, S41Wollert S., O-024, S7Yao Q., O-059, S14Yatsentuyk V.G., P-090, S64Zatagias A., P-026, S45, P-063, S56Zevgaridis A., P-063, S56Ziprin P., O-023, S6Zuvela M., P-040, S50, P-047, S52
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S70

HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S71

The bioabsorbable synthetic 3D matrixdesigned to facilitate tissue generation.
New Choice
W. L. Gore & Associates, Inc. • Flagstaff, AZ 86004 • goremedical.com
Products listed may not be available in all markets. GORE®, BIO-A®, PERFORMANCE THROUGH INNOVATION, and designs are trademarks of W. L. Gore & Associates. ©2010 W. L. Gore & Associates, Inc. AP3014-EU1 JULY 2010
for Complex Soft Tissue Reinforcement
P E R F O R M A N C E t h r o u g h i n n o v a t i o n
LargeSizesNow
Available
GORE® BIO-A® Tissue Reinforcement is a unique non-biologic that is gradually absorbed by the body, leaving no permanent material behind. The open, highly interconnected 3D pore structure facilitates cell infi ltration and growth, quickly forming vascularization within one to two weeks.
100% synthetic, bioabsorbable tissue matrix Rapid cell population and vascularization Versatile for numerous applications Now available in large sizes up to 20 cm x 30 cm
With a three-year shelf life that requires no special handling, storage or tracking, this versatile material is the easy-to-use, non-biologic alternative for surgeons, as well as hospitals.
Visit Gore’s Booth at EHS
HERNIA_SUPP 2011 - 2:- 14/04/11 16:07 Page S72