Embed Size (px)
Citation preview

527I Med Genet 1992; 29: 527-530
ORIGINAL ARTICLES
Hereditary haemorrhagic telangiectasia: a clinicalanalysis
M E M Porteous, J Burn, S J Proctor
AbstractData from 98 patients with hereditaryhaemorrhagic telangiectasia (HHT) are
presented. All were symptomatic by 40years of age and 62% by 16 years. Nosebleeding was the first symptom of diseasein 90% of cases with mucocutaneoustelangiectases appearing 5 to 20 yearslater. Complications of HHT are dis-cussed and an age of onset curve given.
Department ofHuman Genetics,University ofNewcastle upon Tyne.M E M PorteousJ Burn
Department ofHaematology,University ofNewcastle upon Tyne.S J Proctor
Correspondence to DrPorteous, Regional GeneticsAdvisory Service, 19Claremont Place, Newcastleupon Tyne NE2 4AA.
Received 3 October 1991.Revised version accepted4 February 1992.
Hereditary haemorrhagic telangiectasia(HHT) is an autosomal dominant disorder ofvascular proliferation characterised by muco-
cutaneous telangiectases and epistaxes. Theterm HHT was suggested in 1909 by Hanes,'although the disease had previously been de-scribed by Sutton,2 Rendu,3 Osler,4 andWeber.5 HHT has been well documented inmost ethnic groups.67 With careful clinicalexamination of subjects at risk, non-pene-trance is rare.89 The homozygous state appearsto be lethal,'0 although there are few suchpublished cases.The usual presenting feature is epistaxis
from telangiectases over the nasal septum andinferior turbinate beginning around puberty."The characteristic cutaneous telangiectases ap-
pear much later and their absence does notpreclude the diagnosis. Most authors suggestthat a diagnosis of HHT can be made withconfidence if two of the following features are
present; a positive family history, mucocuta-neous telangiectases, and epistaxes.
Larger vessel involvement is common. Pul-monary arteriovenous malformations (PAVM)are found in approximately 15 to 20% ofpatients'2 and can lead to embolic complicationsor high output cardiac failure. AVMs also occurin the cerebral and hepatic vessels although lessfrequently. Though well recognised as a source
of clinical subjects for student medical exam-
inations, HHT families have attracted relativelylittle interest from the genetic viewpoint or
from the perspective of long term morbidityand mortality. We present clinical data from a
series of 98 patients with HHT from 35 familiesascertained throughout Britain.
Materials and methodsEthical approval for the clinical study was
given by the Newcastle District Ethical Com-
mittee and the help of the National Self Helpgroup for HHT sufferers solicited. The mem-bers of the self help group were sent an invi-tation to participate in research aimed at deli-neating the clinical spectrum ofHHT further.One of the authors (MP) visited families intheir own home to document features of HHTand take blood samples for DNA analysis. Inall cases, family members were subjected tolimited medical examination.An attempt at more complete ascertainment
in the Northern Region involved circulating allthe general practitioners, ENT surgeons, andhaematologists with a request for patients'names. The patients were then invited to takepart in the study. A total of 35 families wasascertained nationwide and 98 affected sub-jects assessed.
ResultsPREVALENCEAll general practitioners, ENT surgeons, andhaematologists in the Northern Region of Eng-land (population 3 1 million) were circulatedwith a request for details of patients over the ageof 16 years with HHT under their care on 1March 1990. A total of 316/1060 GPs, 7/22ENT surgeons, and 12/18 haematologistsreturned the questionnaire. Seventy-ninepatients were identified giving a minimumpoint prevalence on 1 March 1990 of 1 in39 216.
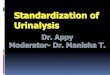
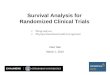
AGE OF ONSETPatients were asked to describe the presentingfeature of their disease; 88/98 reported epis-taxes, five visible telangiectases, and two gas-trointestinal bleeding. Two patients werediagnosed when routine chest radiographsshowed PAVMs (fig 1). One subject presentedwith an epileptic fit at the age of 6 years andwas shown to have a cerebral arteriovenousmalformation on cranial CT scan (fig 2).The age at which the patient first became
symptomatic is plotted as a cumulative fre-quency in fig 3. Where an approximate age ofonset was given, the latest age of onset wasplotted. There were 62% who were symptoma-tic by the age of 16, 83% by 26 years, and 97%by 35 years. All the patients in our seriesshowed evidence of the disease by the age of 40.In one family, an affected grandfather andgrandson were separated by an apparently nor-
on October 23, 2021 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.29.8.527 on 1 August 1992. D
ownloaded from

Porteous, Burn, Proctor
001)
0z
100
90
80
70
60
50
40
30
20
1inL
0 10 5 10 15 20 25 30
Age in years35 40 45
i.
Figure I Plain chest radiograph showing largePAVM.
mal father. This subject was 22 years of age atthe time of examination and cannot be regardedas an example of non-penetrance at this age.
CLINICAL FEATURESEpistaxisOf the 40 patients in the study over 50 yearsold, 16 reported that the epistaxes hadincreased in frequency, duration, and severitywith age, 16 noticed no particular change, andeight noted an improvement. Neither nostrilwas preferentially involved. Cautery of nasallesions produced a temporary improvementbut this was only sustained in one case. Severalpatients felt that their condition deterioratedwithin six months of cauterisation.
Cutaneous telangiectasesMucocutaneous telangiectases tended to ap-pear between five and 20 years after the epis-taxes in the majority of patients. The common-est sites for the lesions were the palms andnailbeds (71%), the lips and tongue (66%, fig4), and the face (20%). The lesions tend tobecome more numerous with age.
Figure 3 Age of onset offirst symptoms ofHHTplotted against cumulative frequency.
Gastrointestinal bleedingGastrointestinal bleeding was present in 16patients. Lesions tended to be in the upper GItract and stomach although this may reflect thefact that predominantly upper GI tract imagingwas used to investigate these patients. Of thepatients with GI bleeding, eight required bloodtransfusions to maintain their haemoglobin level.
Pulmonary arteriovenous malformationsThirteen of the 56 patients in our series whohad been x rayed had a PAVM visible on chestradiograph. Of these, seven were symptomatic.Four patients developed embolic complica-tions, three cerebral abscess, and one stroke.One patient aged 17 when seen had beenshown to have a PAVM on chest radiograph atthe age of 5 years. As he was asymptomatic atthat time his parents decided against surgicalcorrection. Twelve years later he was cyanosedand clubbed with severely limited exercisetolerance. Cardiac catheterisation showed ashunt at the level of the PAVM of approxim-ately 50% of cardiac output (fig 5A). Surgicalresection of the apical segment of the rightlower lobe resulted in resolution of his symp-toms (fig 5B).
Cerebral involvementMuch of the neurological morbidity ofHHT isthe result of embolic complications of pulmon-
Z
4
Figure 2 Cranial CT scan and angiogram showing cerebral A VM.
528
Figure 4 Telangiectases of the lips and tongue.
on October 23, 2021 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.29.8.527 on 1 August 1992. D
ownloaded from

529Hereditary haemorrhagic telangiectasia: a clinical analysis
I
.*
.4
ary arteriovenous malformations.'3 Threepatients had symptomatic cerebral arterio-venous malformations; 46 3% of patients withno known CNS pathology described visualsymptoms suggestive of migrainous aura in theabsence of headache and nausea compared with5 7% of controls (manuscript in preparation).
DiscussionIn 1989, Plauchu et al9 reported a prevalenceof HHT in France of 1 in 8345, considerablyhigher than the previously accepted estimateof 1 in 100 000."4 In the 103 three generationpedigrees there were three cases of apparentnon-penetrance, suggesting a penetrance of97%. The present estimate of 1:39 216 is thefirst prevalence estimate in a British popula-tion and is, almost certainly, an underestimate.One weakness of the clinical study is that
frequently, on domiciliary visits, only a limitedexamination of the skin is possible. However,full body examination of a limited number ofcases indicates that cutaneous features are lar-gely confined to the face, hands, and oronasalmucous membranes.HHT is a very variable disorder which, al-
though no more than a minor inconvenience tosome patients, has devastating results in others.In common with other authors, we have foundthat most of the serious pathology associatedwith this condition is the result of pulmonaryinvolvement. The three patients with cerebralabscess secondary to septic emboli all hadasymptomatic pulmonary AVMs.
Specialised centres now offer transcuta-neous balloon embolisation of pulmonaryAVMs and it is hoped that early treatment willprevent embolic complications.'5 Screening forpulmonary AVMs should be offered to all firstdegree relatives of patients with HHT. In ourcentre this consists of transcutaneous oxygen
saturation measurements erect and supine andbefore and after moderate exercise togetherwith a chest x ray. Any alteration in oxygensaturation merits further investigation of thepulmonary vasculature.The age of onset curve can be used in genetic
risk calculations. We have found that familymembers are usually correct in their assessmentof disease status in relatives. Where possible,nasal cautery should be avoided as its results areusually short term and may lead to furthermucosal damage. Initial results with the Nd-YAG laser are promising,'6 but this treatment isnot yet widely available in the UK.The clinical geneticist has an important role
to play in family tracing if adequate screeningof subjects at risk is to be offered. We foundtwo teenage patients with HHT and pulmon-ary AVMs who, despite being members offamilies well known to the local hospital, werenot under follow up. One has since had anopen resection while the other has beenreferred to a specialist cardiothoracic centre.The pathological basis for HHT is unknown
although it is likely to involve angiogenesis. Asyet, no candidate genes have emerged and atotal genomic search is under way for the locus.In addition to providing a means to identifypresymptomatic gene carriers, the product ofthis gene will be of interest to those interested inthe pathophysiology of new vessel growth.
1 Hanes FM. Multiple hereditary telangiectasis causinghemorrhage (hereditary hemorrhagic telangiectasia). BullJ7ohns Hopkins Hosp 1909;20:63-73.
2 Sutton HG. Epistaxis as an indication of impaired nutritionand of degeneration of the vascular system. Med Mirror1864;1 :769.
3 Rendu M. Epistaxis repetees chez un sujet porteur de petitsangiomes cutanes et muquex. Bull Mem Soc Med Hop1896;13:731.
4 Osler W. On a family form of recurring epistaxis associatedwith multiple telangiectases of the skin and mucousmembranes. Bull Johns Hopkins Hosp 1901;12:333-7.
5 Weber FP. Multiple hereditary developmental angiomata(telangiectases) of the skin and mucous membranes asso-ciated with recurring haemorrhages. Lancet 1907;ii:160-2.
AOA
on October 23, 2021 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.29.8.527 on 1 August 1992. D
ownloaded from

Porteous, Burn, Proctor
6 Posner DP, Sampliner RE. Hereditary hemorrhagic telan-giectasia in three black men. Am Gastroenterol1978;70:389-92.
7 Harding JA, Velchik MG. Pulmonary scintigraphy in apatient with multiple pulmonary arteriovenous malfor-mations and pulmonary embolism. Nucl Med1985;26: 151-4.
8 Bird RM, Hammarsten JF, Marshall RA, Robinson RR. Afamily reunion: a study of hereditary hemorrhagic telan-giectasia. N Engl Med 1957;257:105-9.
9 Plauchu H, de Chadarevian JP, Bideau A, Robert JM. Age-related clinical profile of hereditary hemorrhagic telan-giectasia in an epidemiologically recruited population.Am Med Genet 1989;32:291-7.
10 Snyder LH, Doan CA. Clinical and experimental studies inhuman inheritance: is the homozygous form of multipletelangiectasia lethal? Lab Clin Med 1944;29:1211-6.
11 Stecker RH, Lake CF. Hereditary hemorrhagic telangiecta-sia; review of 102 cases and presentation of an innovationto septodermoplasty. Arch Otolaryngol 1965;82:522-6.
12 Vase P, Holm M, Arendrup H. Pulmonary arteriovenousfistulas in hereditary hemorrhagic telangiectasia. ActaMed Scand 1985;218:105-9.
13 Hewes RC, Auster M, White RI. Cerebral embolism - firstmanifestation of pulmonary arteriovenous malformationin patients with hereditary hemorrhagic telangiectasia.Cardiovasc Intervent Radiol 1985;8: 151-5.
14 McKusick VA. Mendelian inheritance in man; catalogs ofautosomal dominant, autosomal recessive, and X-linkedphenotypes. Baltimore: Johns Hopkins University Press,1990:902-4.
15 White RI, Lynch-Nyhan A, Terry P, et al. Pulmonaryarteriovenous malformations: techniques and long-termoutcome of embolotherapy. Radiology 1988;169:663-9.
16 Mehta AC, Livingston DR, Levine HL. Fiberoptic bron-choscope and Nd-YAG laser treatment of severe epistaxisfrom nasal hereditary hemorrhagic telangiectasia andhemangioma. Chest 1990;91:791-2.
530
on October 23, 2021 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.29.8.527 on 1 August 1992. D
ownloaded from