Embed Size (px)
Citation preview

REVIEW
Hereditary medullary thyroid carcinoma: the managementdilemma
Ping Zhou • Jian Liu • Shao-Wen Cheng •
Bing Wang • Rong Yang • Ling Peng
Published online: 20 December 2011
� Springer Science+Business Media B.V. 2011
Abstract Hereditary medullary thyroid carcinoma (hered-
itary MTC) is a rare malignancy, accounting for 25–30% of
all MTC. It occurs as part of multiple endocrine neoplasia
type 2 (MEN 2). Autosomal dominant gain-of-function
mutations in the RET proto-oncogene is the cause of the
disease, in which the common mutations are codons 609,
611, 618, 620, 630, 634 and 918. In recent years, the spec-
trum of RET gene mutations has changed. The classical
mutations reduced, whereas the less aggressive mutations
increased. Hereditary MTC is a time-dependent disease.
Stages of the disorder at diagnosis can significantly influence
survival rates. Based on the genotype–phenotype, RET
mutations have been classified into four risk levels by
American Thyroid Association (ATA) at 2009. The classi-
fication system guides the hereditary MTC management,
including risk assessment, biochemical screenings and
surgical intervention. Though the application of genetic
testing and codon-specific phenotypes in hereditary MTC
diagnosis is effective with high accuracy, there are some
difficulties in implementing RET gene testing as a routine for
MTC diagnosis. And most of carriers with RET mutations
did not undergo thyroidectomy at the age recommended by
the ATA guidelines. The aim of the study is to review the
hereditary MTC and discuss the management dilemma.
Keywords Hereditary medullary thyroid carcinoma �RET proto-oncogene � Mutation � Management �Prophylactic thyroidectomy
Abbreviations
RET Rearranged during transfection
Hereditary MTC Hereditary medullary thyroid
carcinoma
MEN 2 Multiple endocrine neoplasia type 2
ATA American Thyroid Association
MTC Medullary thyroid carcinoma
CCH C-cell hyperplasia
Pheo Pheochromocytoma
HPT Hyperparathyroidism
FMTC Familial MTC
VUS Variant of unknown significance
HSCR Hirschsprung disease
Introduction
Medullary thyroid carcinoma (MTC) is a rare form of
thyroid cancer which originates from calcitonin-producing
parafollicular C cells, accounting for 3–8% of all thyroid
cancer [1]. In 1959, Hazard first distinguished MTC from
other poor differentiated or anaplastic forms of thyroid
Ping Zhou and Jian Liu contributed equally to this work.
P. Zhou � B. Wang � R. Yang
Department of Surgical Oncology, The First Affiliated Hospital,
School of Medicine, Zhejiang University, 79 Qingchun Road,
Hangzhou 310003, Zhejiang Province, China
J. Liu (&)
Department of Surgical Oncology, Hangzhou Hospital of
Traditional Chinese Medicine, 453 Stadium Road, Hangzhou
310007, Zhejiang Province, China
e-mail: [email protected]
S.-W. Cheng
Trauma Center, The Affiliated Hospital of Hainan Medical
College, 31 Long Hua Road, Haikou 571100, China
L. Peng
Department of Medical Oncology, The First Affiliated Hospital,
School of Medicine, Zhejiang University, 79 Qingchun Road,
Hangzhou 310003, Zhejiang Province, China
123
Familial Cancer (2012) 11:157–165
DOI 10.1007/s10689-011-9501-7

carcinoma. And C-cell hyperplasia (CCH) is the preneo-
plastic lesion [2, 3]. MTC can be divided into sporadic
(75%) and hereditary (25%) types [4]. Hereditary MTC is a
core feature of multiple endocrine neoplasia type 2 (MEN
2), an autosomal dominant inherited cancer syndrome.
Three distinct clinical subtypes of MEN 2 have been
characterized: (i) MEN 2A, by MTC ([90%) in combina-
tion with pheochromocytoma (Pheo) (10–50%) and
hyperparathyroidism (HPT) (10–25%), (ii) MEN 2B, by
MTC associated with Pheo, multiple mucosal neuromas
and marfanoid habitus, (iii) familial MTC (FMTC), by
MTC with a very low incidence of other endocrinopathies.
Because mutations (codons 768 and 804) of FMTC partly
overlap with MEN 2A, FMTC is now considered to be a
clinical variant of MEN 2A rather than a distinct entity [5].
RET genetic screening
RET gene mutations
RET proto-oncogene change or mutation is the cause of
hereditary MTC. In 1993 and 1994, three intense investi-
gations proved the association of RET gene mutations with
hereditary MTC [6–8]. The RET gene is localized to
10q11.2 encoding a tyrosine kinase receptor that influences
cell proliferation, differentiation, migration and apoptosis.
The receptor is mainly expressed in neural crest-derived
tissues, such as C-cells of the thyroid, adrenal medullary
cells, colonic ganglia cells and parathyroid cells.
RET mutations are heterozygous and missense sequence
changes in exons 5, 8, 10, 11 and 13–16. The web of ARUP
Scientific Resource for Research and Education offers full
RET proto-oncogene sequence analysis and sets up the
publicly available and searchable MEN2 RET database.
The database records all RET sequence variants related
with MEN2 syndromes and concerned clinical information.
In the database, RET sequence changes are divided into
four classifications: ‘‘Pathogenic’’ mutation, ‘‘Benign’’
polymorphism, VUS (variant of unknown significance) and
HSCR (Hirschsprung disease) variant. The ‘‘Pathogenic’’
mutation, a deleterious germline RET sequence change,
can cause MEN2 and segregate with the MEN2 disease
symptoms within a family (Table 1) [9].
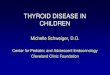
Studies have shown that more than 98% of MEN 2A,
95% of MEN 2B and 85% of FMTC have RET mutations
(Fig. 1). And codons 609, 611, 618, 620, 630 and 634 are
the common mutations of MEN 2A and FMTC, in which
the most common mutation is the codon 634, accounting
for 80–85% of MEN2A and 25–35% of FMTC [5]. In
addition, codon 533 mutation in exon 8 has also been
related to MEN2A and FMTC, but is rare [10, 11]. 95% of
MEN2B have codon 918 mutation, and the remaining 5%
of patients carry codon 883 mutation or two-hit mutations
of 804 with 805, 806 or 904 [12–15].
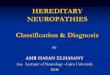
However, the spectrum of RET gene mutations has
changed in recent years. Compared with previous RET
mutation spectrum, Frank-Raue et al. [16–18] reported the
number of classical mutation at codon 634 (level 2, higher
risk of aggressive MTC) reduced, whereas the less aggres-
sive mutations and exons 13–15 mutations (level 1, high risk
of aggressive MTC) increased, especially at codons 790, 791
and 804 (Fig. 2). A study of Frank-Raue showed level 1
mutations were diagnosed in 38.9% of families, and level 2
and 3 mutations were screened in 54.4 and 5.6% of families
[19]. At the same time, some rare (codon 631) and de novo
mutations (codons 292 and 881) have emerged [20, 21].
Kalliopi et al. [22] reported two de novo mutations (the
2458C[T mutation and the transition from I590 to G608)
associated with MEN2. Perhaps, the change can be explained
by the extension (5, 8, and 13–16 exons) of RET sequence
analysis for the gene testing and the missed diagnosis of less
aggressive cases before [23]. In addition, the difference of
ethnical origins and different mutation sites studied in vari-
ous studies also influence the mutation spectrum.
Nevertheless, it has been unclear the prevalence of
specific RET mutations in distinct regions. And no com-
prehensive data has been obtained to clarify the familial
prevalence and RET mutations distribution on a national or
international level. The study of German RET mutations
families revealed the most frequent RET amino acid sub-
stitution was Cys634Arg (21%), followed by Met918Thr
(15%) and Cys634Tyr (9%) [23]. Collecting the data of
356 RET mutations families from Germany, France, Italy,
Poland and Czech Republic, Machens et al. [24] reported
the germline mutations in continental Europe mainly
involved codon 634 (41.0%), followed by codons 804
(11.8%) and 918 (9.6%). However, compared with Euro-
pean researches, the study of Italy showed the most fre-
quent RET amino acid substitution was Val804Met
(19.6%), followed by Cys634Arg (13.6%). And a higher
prevalence of Val804Met and Ser891Ala mutations, a
lower prevalence of Leu790Phe and Tyr791Phe mutations,
and an unexpected higher prevalence of FMTC (57.6%)
with respect to other MEN 2 syndromes (34% of MEN 2A
and 6.8% of MEN 2B) also were observed [25].
The significance and dilemma of RET genetic analysis
RET genetic analysis is a safe and accurate measure of
hereditary MTC diagnosis. Before RET genetic analysis,
the first-degree relatives of hereditary MTC patients who
have a 50% chance of inheriting the predisposing genes
had to undergo repeated biochemical screenings in order to
preclude the disorder. But because of the ambiguous results
of biochemical screenings, the disorder used to be missed,
158 P. Zhou et al.
123

or misdiagnosed, or diagnosed at an advanced stage. After
the application of genetic screening, the disease can be
diagnosed at the early stage and the result of genetic
analysis is more reliable than biochemical screenings.
Genetic testing permits identification of at-risk individuals,
more effective and timely screenings and early surgical
intervention. Meanwhile, Gene testing may make muta-
tion-negative family members avoid the unpleasant and
costly biochemical examinations.
The 2009 ATA guidelines recommended the first-degree
relatives of MEN2A and FMTC to perform genetic analysis
before 5 years old, while as soon as possible and within the
first year of life for the first-degree relatives of MEN 2B
[26]. Otherwise, it has to be discussed that germline
mutations were screened in 4–10% of apparently sporadic
MTC, which emphasized the significance of molecular
testing in order to characterize the MTC as sporadic or
hereditary [27–29].
Though DNA-based predictive testing is 100% accurate
and is considered to be the standard diagnosis for all
first-degree pre-symptomatic relatives, there are some
difficulties in implementing RET gene testing in the whole
family. From the patients’ perspective, there is a loss of
privacy and a feeling of discrimination, which prevent the
proband from informing their relatives about the hereditary
disease.
ATA genotype–phenotype classification
Particular mutations correlate with special phenotypes.
Based on the genetype–phenotype, RET mutations have
been stratified into four risk levels (level A, B, C and D) by
American Thyroid Association (ATA) at 2009 [26]
(Table 1). Level D mutations, the typical MEN2B char-
acterized by the youngest onset age of MTC and the
highest risk of MTC metastasis and mortality, include
codon 883 mutations in exon 15 and codon 918 mutations
in exon 16. And dual mutations, codons 804/805, 804/806
and 804/904 mutations are also ascribed to the level. Level
C mutations, the classical MEN2A characterized by the
higher risk of aggressive MTC, involve codon 634
Table 1 Genotype–phenotype correlations and the MTC and ATA risk levels for hereditary MTC
Exon Mutation ATA
risk level
MTC
risk level
MEN2 phenotype Youngest age at first diagnosis References
MTC Pheo HPT
5 V292 M – – MEN2A 44 – – [21]
8 C515S A – Unclassified 35 – – [47]
8 532 duplication A – FMTC 19 – – [35]
8 G533C A 1 MEN2A/FMTC 21 34 – [9, 48]
10 C609R/G/Y/S/F B 2 MEN2A/FMTC/Unclassified 5? 19 38 [9, 16]
10 C611S/R/G/Y/F/W B 2 MEN2A/FMTC/Unclassified 6 30 40 [9, 49]
10 C618S/R/G/Y/F/W B 2 MEN2A/FMTC/Unclassified 7 19 41 [7, 9]
10 C620S/R/G/Y/F/W B 2 MEN2A/FMTC/Unclassified 5 19 – [7, 9]
11 C630R/Y/F B 2 MEN2A/FMTC/Unclassified 1 – 32 [9, 38]
11 D631Y B – MEN2A 22 – – [20]
11 C634S/R/G/Y/F/L/W C 2 MEN2A/FMTC/Unclassified 1.1 5 10 [9]
11 635insertion ELCR;T636P A – MEN2A – – – [9]
11 637 duplication – – MEN2A 56 – – [50]
11 K666E A 1 MEN2A/Unclassified 12 35 – [9, 51]
13 E768D A 1 MEN2A/FMTC/Unclassified 9 59 – [9]
13 Q781R – – Unclassified 71 – – [51]
13 L790F A 1 MEN2A/FMTC 9 28 – [9, 52]
13 Y791F A 1 MEN2A/FMTC 5 38 38 [9, 53]
14 V804 M/L A 1 MEN2A/FMTC/Unclassified 6? 28 9 [9, 54]
15 A883T/F D 3 MEN2B/Unclassified 10? – – [55]
15 S891A A 1 MEN2A/FMTC 13 46 17 [9, 56]
16 R912P A 2 Unclassified 14 – – [57]
16 M918T D – MEN2B 0.17 12 – [9, 43]
ATA American thyroid association, Risk from aggressive MTC: level D is highest risk
Risk from aggressive MTC from the Seventh International Workshop on MEN (2): Level 1, high risk; level 2, higher risk; level 3, highest risk
Hereditary medullary thyroid carcinoma 159
123

mutation in exon 11. Level B mutations, mostly MEN 2A
and minority FMTC, are at intermediate risk of aggressive
MTC and mainly include codons 609, 611, 618 and 620
mutations in exons 10. Level A mutations, predominately
FMTC and minority MEN2A, have the lowest risk of
aggressive MTC and mainly involve codons 768, 790 and
791 mutations in exon 13, codon 804 mutations in exon 14
and codon 891 mutations in exon 15 [26]. Studies have
shown patients of level B or A mutations have CCH rather
than MTC before the second decade of life and present
MTC with a less aggressive process [30].
Risk-factors influencing prognosis
The main factors influencing survival rates are disease stages
of the disorder (primary tumor size, regional lymph nodes
metastasis and distant metastasis) and age at diagnosis.
Disease staging
Disease stages significantly influence survival rates of the
disorder. An epidemiological and population-based study of
1252 MTC patients showed that patients with tumors confined
to the thyroid gland had a 10-year survival rate of 95.6%, those
with lymph nodes metastasis had an overall survival rate of
75.5% and with distant metastasis only 40% [31].
The presence of palpable thyroid nodules influences the
prognosis and is associated with persistent or recurrent
disease after surgical procedure. On the contrary, the dis-
ease without palpable thyroid nodules has a better prog-
nosis. Lau et al. [32] analyzed 22 patients who had codon
634 mutation and underwent prophylactic total thyroidec-
tomy, and the result showed five of six patients had normal
postoperative ultrasound and no patient presented recur-
rence of hereditary MTC after a median follow-up of
49 months (range, 13–128 months). Another study on 41
individuals younger than 25 years old from 17 independent
MEN2A kindred showed all of asymptomatic patients (20
individuals) were all disease-free after a follow-up of
4.4 ± 1.4 years, whereas 47.6% of symptomatic patients
(21 individuals) had persistent disease (follow-up of
12.0 ± 5.9 years) [33]. Similarly, children identified as
RET mutations carriers by DNA analysis had no evidence
of persistent or recurrent MTC in five or more years after
total thyroidectomy [33–35]. Otherwise, the histological
Fig. 2 Changes in the RET mutational spectrum through years.
a 1996, b 2003, c 2010, Un. Unknown
Fig. 1 The common codons mutations of the RET gene associated
with hereditary MTC (FMTC, MEN2A, MEN2B)
160 P. Zhou et al.
123

differences between the symptomatic and asymptomatic
patients were also obvious. In the asymptomatic group, the
histology was either isolated CCH or CCH associated with
MTC. In the symptomatic group, multifocal MTC without
CCH was detected. Then, palpable thyroid nodule is an
independent predictor of recurrent or persistent hereditary
MTC, patients with small foci may have a greater chance
of surgical cure than the large one. And if thyroidectomy is
performed at asymptomatic age, the disease can be curable
[36–38].
Lymph node metastasis is a poor prognostic factor of
hereditary MTC, which greatly influence the prognosis.
Though lymph node metastasis was uncommon in young
children with MEN2A, the youngest patient with lymph
node metastasis was 5 years old [33, 36]. Data analysis
showed patients with lymph node metastasis at diagnosis
were incurable by surgical intervention. And lymph node
metastasis was also associated with decreased 10-year
overall survival [39].
Age
Hereditary MTC is an age-related disease [3]. The age at
diagnosis greatly influences survival rates. Patients
younger than 40 years at diagnosis have a 5- and 10-years
disease-specific survival rate of 95 and 75%, respectively,
compared with 65 and 50% for those older than 40 years
[1]. The risk of tumor-related death increases by 5.2% for
each additional year of age. And the prognosis is especially
poor in patients older than 65 years [31].
Clinical symptoms and histological progression from
CCH to MTC are age-dependent. The mean age of CCH and
node-negative MTC at diagnosis are 8.3 years and 10.2
years among patients with extracellular-domain mutations
(exons 10 and 11), and 11.2 years and 16.6 years among
patients with intracellular-domain mutations (exons 13, 14
and 15) [3]. And the age from primary tumor of MTC to
lymph node metastasis is 10 years in exons 13, 14 and 15,
21 years in exon 10, 5 years in exons 11 and 2.7 years in
MEN2B. And the age from primary tumor to distant
metastasis is 56 years in exons 13, 14 and 15, 22 years in
exon 10, 15 years in exon 11 and 5 years in MEN2B [40].
Penetrance of RET mutations is also age-dependent.
Penetrance in exon 10 is 4% by age 10 years, 25% by age
25 years and 80% by age 50 years [41]. And penetrance of
both exons 10 and 11 mutations reach 80% by age 50 years
and almost 100% by age 70 years [42].
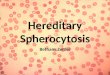
Prophylactic thyroidectomy
Given the penetrance of RET mutations is almost 100%, all
carriers should undergo prophylactic thyroidectomy. The
timing and extent of prophylactic thyroidectomy depend on
the ATA risk levels (Fig. 3). For the level D mutations,
MTC may be present in infancy and lymph nodal metas-
tasis may become apparent in childhood, and thus pro-
phylactic thyroidectomy with central node dissection
should be enforced as soon as possible and within the first
year of life. Among the level C mutations, the typical onset
age of MTC is the third or fourth year and then total thy-
roidectomy with or without central node dissection should
be enforced before the fifth year of life. Because subjects
with the level B or A mutations rarely advent MTC before
the second decade of life and tend to have a less aggressive
course of MTC, the recommended age of prophylactic
thyroidectomy is more controversial. Some practitioners
believed that the surgical intervention can be delayed
beyond age 5 years if basal and stimulated serum calcito-
nin and annual cervical ultrasound starting by 5 years of
age are normal [26, 30, 43]. Though there is enough evi-
dence to support prophylactic thyroidectomy before
5 years old in patients with codon 634 mutation, the
decision of prophylactic thyroidectomy in carriers with the
level A or B mutations still depends on personal experience
and the surgical intervention has to be individualized until
more data are available [26].
Taking into account risk-factors of hereditary MTC and
penetrance of RET mutations, RET gene carriers should
undergo timely prophylactic thyroidectomy before the
neoplastic transformation from CCH to MTC.
The dilemma of prophylactic thyroidectomy
The gold therapeutic standard of hereditary MTC is total
thyroidectomy. If found RET mutations, patients should
undergo total thyroidectomy before the neoplastic trans-
formation from CCH to MTC. But because of the surgical
complications (vocal cord paresis and hypocalcaemia) and
long-term drug compliance, few carriers accepted the
prophylactic intervention, especially young children
(Table 2). Lau et al. [32] reported 14% of hypocalcaemia
after total thyroidectomy in 22 carriers with codon 634
mutation. And Bergenfelz et al. [44] reported 3.9% and
4.4% of vocal cord paresis and hypocalcaemia, respec-
tively. In addition, owing to the influence of gene pene-
trance, some individuals with RET mutations had normal
glands in the adult or even later. For these reasons, some
RET mutations carriers are unwilling to undergo thyroid-
ectomy without clear evidence of MTC.
In order to lessen the surgical complications, many cli-
nicians think prophylactic thyroidectomy should be oper-
ated by specialists with a high level of thyroidectomy
experience. And specialist standards for prophylactic thy-
roidectomy should be defined and specified. Expertise of
approved centers should also be regulated and documented.
Hereditary medullary thyroid carcinoma 161
123

Hereditary MTC management
Management diagram
The application of RET proto-oncogene mutations, geno-
type–phenotype classification and prophylactic thyroidec-
tomy creates a new paradigm for hereditary MTC
management. And the present studies and follow-up data
support the application of ‘codon-directed’ guidelines for
hereditary MTC management [45]. Individuals with a per-
sonal history of MTC, a family history of MEN 2 and the
preneoplastic lesion CCH should accept the germline RET
gene testing. When a proband is found, the genetic coun-
seling, molecular diagnosis and risk assessment should be
provided to the proband. And all first-agree relatives of the
proband should undergo the genetic screening of the same
mutation. Testing negative members are at low risk of
developing hereditary MTC and can avoid the unpleasant
and costly biochemical screenings. Positive members are at
high risk of developing hereditary MTC (dependent on gene
involved) and should accept the genotype-informed sur-
veillance and prophylactic thyroidectomy.
Management dilemma
Unfortunately, despite of the emphasis on early diagnosis
and timely thyroidectomy, there has still no obvious
improvement toward earlier diagnosis and survival rates.
On the one hand, the timing of thyroidectomy in hereditary
MTC patients is relatively late because of the late
Fig. 3 Algorithm for the
diagnosis, follow up and
management of patients with
hereditary MTC
Table 2 The studies of prophylactic thyroidectomy for RET mutations carriers
Study (reference) RET mutations No. of carriers, age No. of carriers
not underwent PrThy
Management measures
Romei, 2011 [58] Not indicated 20, not indicated 20 Clinical and biochemical assessment yearly
Qi, 2011 [59] p.V292M/R67H/R982C 6, 19–70 years old 4 Two carriers await thyroidectomy
Two carriers are being followed up
Jung, 2010 [60] C618S 2, 12–37 years old 2 Refusing further biochemical investigation
Allen, 2009 [46] C618S 4, not indicated 4 Not indicated
Calva, 2009 [61] C609Y 14, not indicated 7 Not indicated
PrThy prophylactic thyroidectomy
Carriers, was defined as having no evidence or clinical suspicion of the disease at the time of the diagnosis
‘‘Management measures’’ are for carriers not underwent PrThy
162 P. Zhou et al.
123

diagnosis, the old age in work-up and time-consuming
decision-making. On the other hand, gene carriers are
reluctant to undergo prophylactic thyroidectomy owing to
the surgical complications and long-term drug compliance.
From the current literature, we conclude that there are
still some difficulties in hereditary MTC management [46].
First of all, some regions can not get RET gene mutations
testing. Secondly, inquiry and RET gene testing of the
apparently sporadic MTC kindred are not complete. And
clinicians are not fully aware of the signification of RET
mutations for hereditary MTC diagnosis and treatment.
Otherwise, most of carriers described in current studies did
not accept prophylactic thyroidectomy at the age recom-
mended by the ATA guidelines and the follow-up of pro-
phylactic surgery is not long enough.
Conclusion
Identification of RET gene mutations heralds the era of
evidence-based molecular diagnosis, gene-informed risk
assessment and preventative therapy. The application of
genetic testing and codon-specific phenotypes in hereditary
MTC diagnosis is safe and accurate, and provides the basis
for individualized risk evaluation and prophylactic thy-
roidectomy of carriers. The present studies and follow-up
data support the application of ‘codon-directed’ guidelines
for the hereditary MTC management. Therefore, the 2009
ATA guidelines of hereditary MTC management should be
strictly enforced in clinic. At the same time, concerted
efforts from the international collaboration are needed to
strengthen the signification of RET gene testing for
hereditary MTC diagnosis and treatment. And further
studies and more data are needed to observe the long-term
survival. Hopefully, the management paradigm of heredi-
tary MTC will be better carried out in clinic.
Acknowledgments We are deeply appreciative of our mentors and
friends for guide and help, including Zhi-Min Ma, Wen-He Zhao,
Wei-Bing Wang and Xin-Xing Duan. And we thank the following
institutions which provided valuable information: Department of
Surgical oncology and Pathology of the first affiliated hospital of
Zhejiang university school of medicine.
Conflict of interest There are no conflicts of interest.
References
1. Clark OH, Kebebew E, Ituarte PHG, Siperstein AE, Duh QY
(2000) Medullary thyroid carcinoma—clinical characteristics,
treatment, prognostic factors, and a comparison of staging sys-
tems. Cancer 88(5):1139–1148
2. Hazard JB, Hawk WA, Crile G Jr (1959) Medullary (solid) car-
cinoma of the thyroid; a clinicopathologic entity. J Clin Endo-
crinol Metab 19(1):152–161
3. Machens A, Niccoli-Sire P, Hoegel J, Frank-Raue K, van
Vroonhoven TJ, Roeher HD, Wahl RA, Lamesch P, Raue F,
Conte-Devolx B, Dralle H (2003) Early malignant progression of
hereditary medullary thyroid cancer. N Engl J Med 349(16):
1517–1525. doi:10.1056/NEJMoa012915
4. Jemal A, Tiwari RC, Murray T, Ghafoor A, Samuels A, Ward E,
Feuer EJ, Thun MJ (2004) Cancer statistics, 2004. CA Cancer J
Clin 54(1):8–29
5. Eng C, Clayton D, Schuffenecker I, Lenoir G, Cote G, Gagel RF,
van Amstel HK, Lips CJ, Nishisho I, Takai SI, Marsh DJ, Rob-
inson BG, Frank-Raue K, Raue F, Xue F, Noll WW, Romei C,
Pacini F, Fink M, Niederle B, Zedenius J, Nordenskjold M,
Komminoth P, Hendy GN, Mulligan LM et al (1996) The rela-
tionship between specific RET proto-oncogene mutations and
disease phenotype in multiple endocrine neoplasia type 2. Inter-
national RET mutation consortium analysis. JAMA 276(19):
1575–1579
6. Mulligan LM, Kwok JB, Healey CS, Elsdon MJ, Eng C, Gardner
E, Love DR, Mole SE, Moore JK, Papi L et al (1993) Germ-line
mutations of the RET proto-oncogene in multiple endocrine
neoplasia type 2A. Nature 363(6428):458–460. doi:10.1038/3634
58a0
7. Donis-Keller H, Dou S, Chi D, Carlson KM, Toshima K, Lair-
more TC, Howe JR, Moley JF, Goodfellow P, Wells SA Jr (1993)
Mutations in the RET proto-oncogene are associated with MEN
2A and FMTC. Hum Mol Genet 2(7):851–856
8. Eng C, Smith DP, Mulligan LM, Nagai MA, Healey CS, Ponder
MA, Gardner E, Scheumann GF, Jackson CE, Tunnacliffe A et al
(1994) Point mutation within the tyrosine kinase domain of the
RET proto-oncogene in multiple endocrine neoplasia type 2B and
related sporadic tumours. Hum Mol Genet 3(2):237–241
9. Margraf RL, Crockett DK, Krautscheid PM, Seamons R, Cald-
eron FR, Wittwer CT, Mao R (2009) Multiple endocrine neo-
plasia type 2 RET protooncogene database: repository of MEN2-
associated RET sequence variation and reference for genotype/
phenotype correlations. Hum Mutat 30(4):548–556. doi:10.1002/
humu.20928
10. Peppa M, Boutati E, Kamakari S, Pikounis V, Peros G, Pana-
yiotides IG, Economopoulos T, Raptis SA, Hadjidakis D (2008)
Multiple endocrine neoplasia type 2A in two families with the
familial medullary thyroid carcinoma associated G533C mutation
of the RET proto-oncogene. Eur J Endocrinol 159(6):767–771.
doi:10.1530/eje-08-0476
11. Kaldrymides P, Mytakidis N, Anagnostopoulos T, Vassiliou M,
Tertipi A, Zahariou M, Rampias T, Koutsodontis G, Konstanto-
poulou I, Ladopoulou A, Bei T, Yannoukakos D (2006) A rare
RET gene exon 8 mutation is found in two Greek kindreds with
familial medullary thyroid carcinoma: implications for screening.
Clin Endocrinol (Oxf) 64(5):561–566. doi:10.1111/j.1365-2265.
2006.02509.x
12. Gimm O, Marsh DJ, Andrew SD, Frilling A, Dahia PL, Mulligan
LM, Zajac JD, Robinson BG, Eng C (1997) Germline dinucleo-
tide mutation in codon 883 of the RET proto-oncogene in mul-
tiple endocrine neoplasia type 2B without codon 918 mutation.
J Clin Endocrinol Metab 82(11):3902–3904
13. Cranston AN, Carniti C, Oakhill K, Radzio-Andzelm E, Stone
EA, McCallion AS, Hodgson S, Clarke S, Mondellini P, Leyland
J, Pierotti MA, Whittaker J, Taylor SS, Bongarzone I, Ponder BA
(2006) RET is constitutively activated by novel tandem mutations
that alter the active site resulting in multiple endocrine neoplasia
type 2B. Cancer Res 66(20):10179–10187. doi:10.1158/0008-
5472.can-06-0884
14. Miyauchi A, Futami H, Hai N, Yokozawa T, Kuma K, Aoki N,
Kosugi S, Sugano K, Yamaguchi K (1999) Two germline mis-
sense mutations at codons 804 and 806 of the RET proto-onco-
gene in the same allele in a patient with multiple endocrine
Hereditary medullary thyroid carcinoma 163
123

neoplasia type 2B without codon 918 mutation. Jpn J Cancer Res
90(1):1–5
15. Iwashita T, Murakami H, Kurokawa K, Kawai K, Miyauchi A,
Futami H, Qiao S, Ichihara M, Takahashi M (2000) A two-hit
model for development of multiple endocrine neoplasia type 2B
by RET mutations. Biochem Biophys Res Commun 268(3):
804–808. doi:10.1006/bbrc.2000.2227
16. Frank-Raue K, Hoppner W, Frilling A, Kotzerke J, Dralle H,
Haase R, Mann K, Seif F, Kirchner R, Rendl J, Deckart HF, Ritter
MM, Hampel R, Klempa J, Scholz GH, Raue F (1996) Mutations
of the ret protooncogene in German multiple endocrine neoplasia
families: relation between genotype and phenotype. German
Medullary Thyroid Carcinoma Study Group. J Clin Endocrinol
Metab 81(5):1780–1783
17. Yip L, Cote GJ, Shapiro SE, Ayers GD, Herzog CE, Sellin RV,
Sherman SI, Gagel RF, Lee JE, Evans DB (2003) Multiple
endocrine neoplasia type 2: evaluation of the genotype-phenotype
relationship. Arch Surg 138(4):409–416. doi:10.1001/archsurg.
138.4.409 discussion 416
18. Frank-Raue K, Rondot S, Raue F (2010) Molecular genetics and
phenomics of RET mutations: impact on prognosis of MTC. Mol
Cell Endocrinol 322(1–2):2–7. doi:10.1016/j.mce.2010.01.012
19. Frank-Raue K, Rondot S, Schulze E, Raue F (2007) Change in
the spectrum of RET mutations diagnosed between 1994 and
2006. Clin Lab 53(5–6):273–282
20. Frank-Raue K, Dohring J, Scheumann G, Rondot S, Lorenz A,
Schulze E, Dralle H, Raue F, Leidig-Bruckner G (2010) New
mutations in the RET protooncogene-L881 V—associated with
medullary thyroid carcinoma and -R770Q—in a patient with
mixed medullar/follicular thyroid tumour. Exp Clin Endocrinol
Diabetes 118(8):550–553. doi:10.1055/s-0029-1241851
21. Castellone MD, Verrienti A, Magendra Rao D, Sponziello M,
Fabbro D, Muthu M, Durante C, Maranghi M, Damante G, Piz-
zolitto S, Costante G, Russo D, Santoro M, Filetti S (2010) A
novel de novo germ-line V292 M mutation in the extracellular
region of RET in a patient with phaeochromocytoma and med-
ullary thyroid carcinoma: functional characterization. Clin
Endocrinol (Oxf) 73(4):529–534. doi:10.1111/j.1365-2265.2009.
03757.x
22. Pazaitou-Panayiotou K, Giatzakis C, Koutsodontis G, Vratimos
A, Chrisoulidou A, Konstantinidis T, Kamakari S (2010) Iden-
tification of two novel mutations in the RET proto-oncogene in
the same family. Thyroid 20(4):401–406. doi:10.1089/thy.2009.
0262
23. Machens A, Dralle H (2008) Familial prevalence and age of RET
germline mutations: implications for screening. Clin Endocrinol
(Oxf) 69(1):81–87. doi:10.1111/j.1365-2265.2007.03153.x
24. Machens A, Lorenz K, Dralle H (2009) Constitutive RET tyro-
sine kinase activation in hereditary medullary thyroid cancer:
clinical opportunities. J Intern Med 266(1):114–125. doi:10.1111/
j.1365-2796.2009.02113.x
25. Romei C, Mariotti S, Fugazzola L, Taccaliti A, Pacini F, Opocher
G, Mian C, Castellano M, degli Uberti E, Ceccherini I, Cremonini
N, Seregni E, Orlandi F, Ferolla P, Puxeddu E, Giorgino F, Colao
A, Loli P, Bondi F, Cosci B, Bottici V, Cappai A, Pinna G,
Persani L, Verga U, Boscaro M, Castagna MG, Cappelli C, Za-
telli MC, Faggiano A, Francia G, Brandi ML, Falchetti A,
Pinchera A, Elisei R (2010) Multiple endocrine neoplasia type 2
syndromes (MEN 2): results from the ItaMEN network analysis
on the prevalence of different genotypes and phenotypes. Eur J
Endocrinol 163(2):301–308. doi:10.1530/eje-10-0333
26. Kloos RT, Eng C, Evans DB, Francis GL, Gagel RF, Gharib H,
Moley JF, Pacini F, Ringel MD, Schlumberger M, Wells SA Jr
(2009) Medullary thyroid cancer: management guidelines of the
American Thyroid Association. Thyroid 19(6):565–612. doi:
10.1089/thy.2008.0403
27. Bugalho MJ, Domingues R, Santos JR, Catarino AL, Sobrinho L
(2007) Mutation analysis of the RET proto-oncogene and early
thyroidectomy: results of a Portuguese cancer centre. Surgery
141(1):90–95. doi:10.1016/j.surg.2006.03.025
28. Wiench M, Wygoda Z, Gubala E, Wloch J, Lisowska K, Kras-
sowski J, Scieglinska D, Fiszer-Kierzkowska A, Lange D, Kula
D, Zeman M, Roskosz J, Kukulska A, Krawczyk Z, Jarzab B
(2001) Estimation of risk of inherited medullary thyroid carci-
noma in apparent sporadic patients. J Clin Oncol 19(5):
1374–1380
29. Elisei R, Romei C, Cosci B, Agate L, Bottici V, Molinaro E,
Sculli M, Miccoli P, Basolo F, Grasso L, Pacini F, Pinchera A
(2007) RET genetic screening in patients with medullary thyroid
cancer and their relatives: experience with 807 individuals at one
center. J Clin Endocr Metab 92(12):4725–4729. doi:10.1210/Jc.
2007-1005
30. Allen SM, Bodenner D, Suen JY, Richter GT (2009) Diagnostic
and surgical dilemmas in hereditary medullary thyroid carci-
noma. Laryngoscope 119(7):1303–1311. doi:10.1002/lary.20299
31. Roman S, Lin R, Sosa JA (2006) Prognosis of medullary thyroid
carcinoma—demographic, clinical, and pathologic predictors of
survival in 1252 cases. Cancer 107(9):2134–2142. doi:10.1002/
Cncr.22244
32. Lau GS, Lang BH, Lo CY, Tso A, Garcia-Barcelo MM, Tam PK,
Lam KS (2009) Prophylactic thyroidectomy in ethnic Chinese
patients with multiple endocrine neoplasia type 2A syndrome
after the introduction of genetic testing. Hong Kong Med J 15(5):
326–331
33. Punales MK, da Rocha AP, Meotti C, Gross JL, Maia AL (2008)
Clinical and oncological features of children and young adults
with multiple endocrine neoplasia type 2A. Thyroid 18(12):
1261–1268. doi:10.1089/thy.2007.0414
34. Spinelli C, Di Giacomo M, Costanzo S, Elisei R, Miccoli P
(2010) Role of RET codonic mutations in the surgical manage-
ment of medullary thyroid carcinoma in pediatric age multiple
endocrine neoplasm type 2 syndromes. J Pediatr Surg
45(8):1610–1616. doi:10.1016/j.jpedsurg.2010.03.019
35. Frank-Raue K, Buhr H, Dralle H, Klar E, Senninger N, Weber T,
Rondot S, Hoppner W, Raue F (2006) Long-term outcome in 46
gene carriers of hereditary medullary thyroid carcinoma after
prophylactic thyroidectomy: impact of individual RET genotype.
Eur J Endocrinol 155(2):229–236. doi:10.1530/eje.1.0221636. Skinner MA, Moley JA, Dilley WG, Owzar K, Debenedetti MK,
Wells SA Jr (2005) Prophylactic thyroidectomy in multiple
endocrine neoplasia type 2A. N Engl J Med 353(11):1105–1113.
doi:10.1056/NEJMoa043999
37. Schellhaas E, Konig C, Frank-Raue K, Buhr HJ, Hotz HG (2009)
Long-term outcome of ‘‘prophylactic therapy’’ for familial
medullary thyroid cancer. Surgery 146(5):906–912. doi:10.1016/
j.surg.2009.06.007
38. Ukkat J, Gimm O, Brauckhoff M, Bilkenroth U, Dralle H (2004)
Single center experience in primary surgery for medullary thyroid
carcinoma. World J Surg 28(12):1271–1274. doi:10.1007/
s00268-004-7608-9
39. Raval MV, Sturgeon C, Bentrem DJ, Elaraj DM, Stewart AK,
Winchester DJ, Ko CY, Reynolds M (2010) Influence of lymph
node metastases on survival in pediatric medullary thyroid can-
cer. J Pediatr Surg 45(10):1947–1954. doi:10.1016/j.jpedsurg.
2010.06.013
40. Baumgartner-Parzer SM, Lang R, Wagner L, Heinze G, Niederle
B, Kaserer K, Waldhausl W, Vierhapper H (2005) Polymor-
phisms in exon 13 and intron 14 of the RET protooncogene:
genetic modifiers of medullary thyroid carcinoma? J Clin Endo-
crinol Metab 90(11):6232–6236. doi:10.1210/jc.2005-1278
41. Frank-Raue K, Rybicki LA, Erlic Z, Schweizer H, Winter A,
Milos I, Toledo SP, Toledo RA, Tavares MR, Alevizaki M, Mian
164 P. Zhou et al.
123

C, Siggelkow H, Hufner M, Wohllk N, Opocher G, Dvorakova S,
Bendlova B, Czetwertynska M, Skasko E, Barontini M, Sanso G,
Vorlander C, Maia AL, Patocs A, Links TP, de Groot JW, Ker-
stens MN, Valk GD, Miehle K, Musholt TJ, Biarnes J, Damja-
novic S, Muresan M, Wuster C, Fassnacht M, Peczkowska M,
Fauth C, Golcher H, Walter MA, Pichl J, Raue F, Eng C, Neu-
mann HP (2011) Risk profiles and penetrance estimations in
multiple endocrine neoplasia type 2A caused by germline RET
mutations located in exon 10. Hum Mutat 32(1):51–58. doi:
10.1002/humu.21385
42. Milos IN, Frank-Raue K, Wohllk N, Maia AL, Pusiol E, Patocs
A, Robledo M, Biarnes J, Barontini M, Links TP, de Groot JW,
Dvorakova S, Peczkowska M, Rybicki LA, Sullivan M, Raue F,
Zosin I, Eng C, Neumann HP (2008) Age-related neoplastic risk
profiles and penetrance estimations in multiple endocrine neo-
plasia type 2A caused by germ line RET Cys634Trp (TGC [TGG) mutation. Endocr Relat Cancer 15(4):1035–1041. doi:
10.1677/erc-08-0105
43. Raue F, Frank-Raue K (2010) Update multiple endocrine neo-
plasia type 2. Fam Cancer 9(3):449–457. doi:10.1007/s10689-
010-9320-2
44. Bergenfelz A, Jansson S, Kristoffersson A, Martensson H, Re-
ihner E, Wallin G, Lausen I (2008) Complications to thyroid
surgery: results as reported in a database from a multicenter audit
comprising 3,660 patients. Langenbecks Arch Surg 393(5):
667–673. doi:10.1007/s00423-008-0366-7
45. Grubbs EG, Waguespack SG, Rich TA, Xing Y, Ying AK, Evans
DB, Lee JE, Perrier ND (2010) Do the recent American Thyroid
Association (ATA) Guidelines accurately guide the timing of
prophylactic thyroidectomy in MEN2A? Surgery 148(6):
1302–1309. doi:10.1016/j.surg.2010.09.020 Discussion 1309–1310
46. Richter GT, Allen SM, Bodenner D, Suen JY (2009) Diagnostic
and surgical Dilemmas in hereditary medullary thyroid carci-
noma. Laryngoscope 119(7):1303–1311. doi:10.1002/Lary.20299
47. Fazioli F, Piccinini G, Appolloni G, Bacchiocchi R, Palmonella
G, Recchioni R, Pierpaoli E, Silvetti F, Scarpelli M, Bruglia M,
Melillo RM, Santoro M, Boscaro M, Taccaliti A (2008) A new
germline point mutation in Ret exon 8 (cys515ser) in a family
with medullary thyroid carcinoma. Thyroid 18(7):775–782. doi:
10.1089/thy.2007.0365
48. Da Silva AM, Maciel RM, Da Silva MR, Toledo SR, De Carv-
alho MB, Cerutti JM (2003) A novel germ-line point mutation in
RET exon 8 (Gly(533)Cys) in a large kindred with familial
medullary thyroid carcinoma. J Clin Endocrinol Metab
88(11):5438–5443
49. Mulligan LM, Eng C, Healey CS, Clayton D, Kwok JB, Gardner
E, Ponder MA, Frilling A, Jackson CE, Lehnert H et al (1994)
Specific mutations of the RET proto-oncogene are related to
disease phenotype in MEN 2A and FMTC. Nat Genet 6(1):70–74.
doi:10.1038/ng0194-70
50. Hoppner W, Dralle H, Brabant G (1998) Duplication of 9 base
pairs in the critical cysteine-rich domain of the RET proto-
oncogene causes multiple endocrine neoplasia type 2A. Hum
Mutat Suppl 1:S128–S130
51. Maschek W, Pichler R, Rieger R, Weinhausel A, Berg J (2002) A
new identified germline mutation of the RET proto-oncogene
responsible for familial medullary thyroid carcinoma in co-exis-
tence with a hyperfunctioning autonomous nodule. Clin Endo-
crinol (Oxf) 56(6):823
52. Jindrichova S, Vcelak J, Vlcek P, Neradilova M, Nemec J,
Bendlova B (2004) Screening of six risk exons of the RET proto-
oncogene in families with medullary thyroid carcinoma in the
Czech Republic. J Endocrinol 183(2):257–265. doi:10.1677/joe.
1.05838
53. Berndt I, Reuter M, Saller B, Frank-Raue K, Groth P, Grussen-
dorf M, Raue F, Ritter MM, Hoppner W (1998) A new hot spot
for mutations in the ret protooncogene causing familial medullary
thyroid carcinoma and multiple endocrine neoplasia type 2A.
J Clin Endocrinol Metab 83(3):770–774
54. Fink M, Weinhusel A, Niederle B, Haas OA (1996) Distinction
between sporadic and hereditary medullary thyroid carcinoma
(MTC) by mutation analysis of the RET proto-oncogene. Study
Group Multiple Endocrine Neoplasia Austria (SMENA). Int J
Cancer 69(4):312–316. doi:10.1002/(sici)1097-0215(19960822)
69:4\312:aid-ijc13[3.0.co;2-7
55. Smith DP, Houghton C, Ponder BA (1997) Germline mutation of
RET codon 883 in two cases of de novo MEN 2B. Oncogene
15(10):1213–1217. doi:10.1038/sj.onc.1201481
56. Hofstra RM, Fattoruso O, Quadro L, Wu Y, Libroia A, Verga U,
Colantuoni V, Buys CH (1997) A novel point mutation in the
intracellular domain of the ret protooncogene in a family with
medullary thyroid carcinoma. J Clin Endocrinol Metab 82(12):
4176–4178
57. Jimenez C, Dang GT, Schultz PN, El-Naggar A, Shapiro S,
Barnes EA, Evans DB, Vassilopoulou-Sellin R, Gagel RF, Cote
GJ, Hoff AO (2004) A novel point mutation of the RET proto-
oncogene involving the second intracellular tyrosine kinase
domain in a family with medullary thyroid carcinoma. J Clin
Endocrinol Metab 89(7):3521–3526. doi:10.1210/jc.2004-0073
58. Romei C, Cosci B, Renzini G, Bottici V, Molinaro E, Agate L,
Passannanti P, Viola D, Biagini A, Basolo F, Ugolini C, Mate-
razzi G, Pinchera A, Vitti P, Elisei R (2011) RET genetic
screening of sporadic medullary thyroid cancer (MTC) allows the
preclinical diagnosis of unsuspected gene carriers and the iden-
tification of a relevant percentage of hidden familial MTC
(FMTC). Clin Endocrinol (Oxf) 74(2):241–247. doi:10.1111/
j.1365-2265.2010.03900.x
59. Zhang XN, Qi XP, Ma JM, Du ZF, Ying RB, Fei J, Jin HY, Han
JS, Wang JQ, Chen XL, Chen CY, Liu WT, Lu JJ, Zhang JG
(2011) RET germline mutations identified by exome sequencing
in a Chinese multiple endocrine neoplasia type 2A/familial
medullary Thyroid carcinoma family. PLoS One 6(5). doi:
10.1371/journal.pone.0020353
60. Park H, Jung J, Uchino S, Lee Y (2010) A Korean family of
familial medullary thyroid cancer with Cys618Ser RET germline
mutation. J Korean Med Sci 25(2):226–229. doi:10.3346/jkms.
2010.25.2.226
61. Calva D, O’Dorisio TM, Sue O’Dorisio M, Lal G, Sugg S,
Weigel RJ, Howe JR (2009) When is prophylactic thyroidectomy
indicated for patients with the RET codon 609 mutation? Ann
Surg Oncol 16(8):2237–2244. doi:10.1245/s10434-009-0524-3
Hereditary medullary thyroid carcinoma 165
123