Embed Size (px)
Citation preview

magnetic flux far down the jets, as would be expected if the electromagnetic jetlaunching mechanism referred to above is at work. The authors’ results thus provide direct observational evidence that this is the case.
Theoretical simulations3,4 of accretion disks have shown that, under certain conditions, the magnetic flux in the vicinity of the black hole naturally reaches a maximum equilibrium value. When this happens, forces exerted by the magnetic field dominate in the inner part of the disk. Disks for which this is true are called magnetically arrested disks, or MADs3,4. Zamaninasab et al. find that the derived slope of the linear correlation between the accretiondisk luminosity and the jet magnetic flux is precisely the value predicted for such disks, strongly suggesting that this MAD scenario is operating in the hearts of AGN.
These results indicate that the jets of AGN are launched electromagnetically by magnetic fields twisted by the black hole’s spin, that these magnetic fields have a dominant role in determining the dynamics of the disk and jets in the vicinity of the central black hole, and that this may remain true at least out to VLBI scales, several parsecs from the black hole. It will therefore be important to consider the influence of the magnetic field, for example, when inferring the properties of the central black hole and accretion disk from highresolution studies made with millimetrewavelength, groundbased VLBI5–7, or with ‘space VLBI’, in which one or more antennas orbiting Earth are used with ground antennas8,9.
Zamaninasab and colleagues’ findings also radically change the way astronomers view the jets emanating from the centres of AGN. These jets are not just outflows of matter carrying tremendous amounts of energy, but are also intrinsically magnetic structures. Many of their properties are probably determined by the magnetic fields embedded in them and travelling outwards with them. The twisting of the central magnetic fields that launches the jets should give rise to helical jet magnetic fields, which may be manifest in the jets’ magneticfield structure and morphology10,11. Because a fundamental relationship exists between magnetic fields and electrical currents, jet outflows should be regarded as systems of magnetic fields and currents. This is essential if we are to understand these enormous structures: how they propagate, why they remain so narrow as they traverse enormous distances, and how they interact with the mater ial through which they are moving.
As the jets travel beyond their host galaxy and into intergalactic space, effects other than magnetic forces will probably also come into play, making the jets and the surrounding gas more turbulent and reducing the magnetic field’s effects. Further detailed studies of the jets of AGN and their magnetic fields, from VLBI scales out to the ends of the jets many
thousands of parsecs from the central black hole, should help to determine whether such a transition occurs, and where. ■
Denise Gabuzda is in the Department of Physics, University College Cork, Cork, Ireland.e-mail: [email protected]
1. Zamaninasab, M., Clausen-Brown, E., Savolainen, T. & Tschekhovskoy, A. Nature 510, 126–128 (2014).
2. Blandford, R. D. & Znajek, R. L. Mon. Not. R. Astron. Soc. 179, 433–456 (1977).
3. Tchekhovskoy, A., Narayan, R. & McKinney, J. C.
H E PAT I T I S C
Treatment triumphsA stampede of recent clinical studies suggests that we are on the cusp of developing well-tolerated, orally delivered drugs that can effectively eradicate hepatitis C virus from most, if not all, infected individuals.
C H A R L E S M . R I C E & M O H S A N S A E E D
The story of hepatitis C began in the 1970s, when it was recognized that something other than hepatitis A or
hepatitis B infections was causing liver inflammation following blood transfusions1,2. In 1989, the troublemaker was identified as a small RNA virus, named hepatitis C (HCV)3. Although there are now effective diagnostic procedures that allow a safe blood supply in most developed countries, intravenous drug abuse continues to lead to new infections. An estimated 185 million people are chronically infected with HCV and are at risk of developing lifethreatening liver diseases, including cirrhosis and cancer4. But a recent series of clinical trials, reported in the New England Journal of Medicine5–11, demonstrate drastic increases in the effectiveness of antiHCV drugs.
Historically, HCVinfected patients have
been treated by intravenous injections with type I interferons — secreted cellular proteins that elicit potent antiviral responses12. The success rates for interferonbased regimens improved from single digits in the 1970s to around 50% by 2002, accomplished by increasing dose, lengthening treatment, chemically stabilizing the interferon (by PEGylation) and adding ribavirin, an RNAnucleoside analogue. Ribavirin has poor antiHCV activity when used alone but significantly increased treatment success when combined with interferon (by mechanisms that are still unsettled). However, this treatment required a 24 or 48week course and was plagued by awful side effects, including nausea, depression and anaemia. Hence, the goal remained to develop highly effective, orally administered and welltolerated regimens that work for all patient groups.
Two enzymes encoded by HCV that are essential for viral replication — a serine
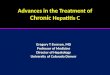
Figure 1 | HCV trajectory. In the 1980s, mysterious cases of liver inflammation following blood transfusions that were not explained by hepatitis A or hepatitis B viral infections were treated using type I interferon proteins, with a success rate of around 5%. The cause of these infections was identified in 1989 as RNA virus hepatitis C (HCV). The combination of PEGylated interferon (PEGIFN) and ribavirin, approved in 2002, improved cure rates to around 50%. By 2011, drug cocktails containing HCVspecific directacting antivirals (DAAs) were being used to treat patients, with around 75% cure rates, and recent clinical trials5–11 of alloral, interferonfree, DAAbased regimens have increased treatment success rates to more than 95%.
1980s
~5%cure
~50%cure
~75%cure
>95%cure
1989 20112002 2014
Mysteryvirus
HCV identi�ed,diagnostics developed
PEG-IFN +ribavirin
PEG-IFN +ribavirin + DAA
All-oralDAA
Mon. Not. R. Astron. Soc. 418, L79–L83 (2011).4. McKinney, J. C., Tchekhovskoy, A. & Blandford, R. D.
Mon. Not. R. Astron. Soc. 423, 3083–3117 (2012).5. Dexter, J. & Fragile, P. C. Mon. Not. R. Astron. Soc.
432, 2252–2272 (2013). 6. Doeleman, S. S. et al. Science 338, 355–358
(2012).7. Johannsen, T. et al. Astrophys. J. 758, 30 (2012).8. Kardashev, N. S. et al. Astron. Rep. 57, 153–194
(2013). 9. Takahashi, R. & Mineshige, S. Astrophys. J. 729, 86
(2011).10. Molina, S. N. et al. Astron. Astrophys. (in the press);
preprint at http://arXiv.org/abs/1404.5961 (2014). 11. Gabuzda, D. C., Cantwell, T. M. & Cawthorne, T. V.
Mon. Not. R. Astron. Soc. 438, L1–L5 (2014).
5 J U N E 2 0 1 4 | V O L 5 1 0 | N A T U R E | 4 3
NEWS & VIEWS RESEARCH
© 2014 Macmillan Publishers Limited. All rights reserved

protease (NS34A) and an RNA polymerase (NS5B) — are attractive drug targets. In the 2000s, inhibitors of these enzymes and of another nonenzymatic but essential HCV protein (NS5A), referred to as direct acting antivirals (DAAs), emerged as the lead targets for HCV drug development. In late 2011, two NS34A protease inhibitors were approved for human use in combination with PEGylated interferon and ribavirin, raising treatment success to more than 70% for patients with HCV genotype 1 (there are six highly divergent and variable genotypes of the virus).
However, euphoria over this advance was shortlived. Patients with advanced disease were treated but many others were not, owing to the additional, often severe, side effects of this drug combination and the emergence of viral resistance. In the meantime, and continuing into the present, dozens of new compounds were being tested in the clinic. In 2013, morepotent DAAs, in combination with PEGylated interferon and ribavirin, were approved, as was the first alloral regimen, consisting of a NS5Btargeting DAA combined with ribavirin alone.
The recent clinical studies5–11 present the next wave of interferonfree, alloral, DAAbased regimens, which are likely to be approved in the near future for HCV treatment. Without delving into details and trade names, several key points about these trials emerge. First, they include multiple alloral combinations that can achieve success rates of more than 95%. ‘Success’ for HCV treatment means no detectable virus 12 weeks after stopping treatment. Unlike drug treatments for hepatitis B and HIV, most HCV researchers believe that this endpoint represents a durable cure that lowers the risk of progressive liver disease. Second, these treatments are effective in patients who are in greatest need and are most difficult to treat — those with advanced fibrosis and cirrhosis, those who are coinfected with HIV, and even livertransplant candidates and recipients. Also noteworthy is that the new drug combinations promise shorter treatment times (12 weeks and possibly even less) and minimal side effects; as a result, fewer people are expected to discontinue their treatment.
So from a mystery virus and a 5% treatmentsuccess rate, we have come to an era of cure rates of more than 95% (Fig. 1). Game over, right? Not quite. What about viral resistance to the drugs? With nearly 200 million infected individuals, 6 diverse viral genotypes and around 1 trillion viral variants being generated per day per infected person, it is likely that HCV will have some tricks up its sleeve to develop resistance. However, some of the new DAAs, in particular sofosbuvir, which targets the active site of NS5B, have an extremely high barrier to resistance, and there have been only rare glimpses of resistant variants in clinical observations with multiple viral genotypes13. Combining potent DAAs, each with lower resistance barriers, can still be highly
effective at avoiding the buildup of resistance. Nonetheless, resistance will undoubtedly occur and should be taken into account to guide treatment decisions. The current drugs are also less effective against genotype 3 HCV, which is common in South Asia, although pangenotype drugs are in development.
Another barrier is identifying those infected. Most people are unaware of their HCV infection14, and only a small minority has been treated15. Although some health agencies have recommended universal screening of highrisk groups, implementing such policies is challenging and timeconsuming. And once infected individuals are identified, how will society pay for their treatment? The current price tag for cuttingedge HCV treatment in the United States is more than US$80,000 for a 12week course. Competition among pharmaceutical companies may lower this price, but most people infected with HCV live in countries that cannot afford the new treatments. Fortunately, there is movement in the pharmaceutical industry to provide for lowcost drug production in certain countries, such as Egypt, where an estimated 10% of the population is infected. Finally, getting rid of the virus does not always erase the risk of future liverrelated problems — patients still need to be monitored routinely for liver function and cancer, particularly those whose infection had led to cirrhosis.
With the new drugs that are in hand or on the horizon, we have the means to eradicate this virus, possibly without needing a vaccine. However, the challenge now is to extend these
great medical advances on a national and global scale to those in need — something that has not been terribly effective in the past. We can hope that implementing these transformative HCV advances will help to create a model for success, for this and other widespread human diseases. ■
Charles M. Rice and Mohsan Saeed are in the Center for the Study of Hepatitis C, Laboratory of Virology and Infectious Disease, The Rockefeller University, New York, New York 10065, USA.e-mail: [email protected]
1. Prince, A. M. et al. Lancet 2, 241–246 (1974).2. Alter, H. J. et al. Lancet 2, 838–841 (1975).3. Choo, Q. L. et al. Science 244, 359–362 (1989).4. Mohd Hanafiah, K., Groeger, J., Flaxman, A. D. &
Wiersma, S. T. Hepatology 57, 1333–1342 (2013).5. Feld, J. J. et al. N. Engl. J. Med. 370, 1594–1603
(2014).6. Afdhal, N. et al. N. Engl. J. Med. 370, 1889–1898
(2014).7. Afdhal, N. et al. N. Engl. J. Med. 370, 1483–1493
(2014).8. Kowdley, K. V. et al. N. Engl. J. Med. 370, 222–232
(2014).9. Kowdley, K. V. et al. N. Engl. J. Med. 370, 1879–1888
(2014).10. Zeuzem, S. et al. N. Engl. J. Med. 370, 1604–1614
(2014).11. Sulkowski, M. S., Jacobson, I. M. & Nelson, D. R.
N. Engl. J. Med. 370, 1560–1561 (2014).12. Heim, M. H. Nature Rev. Immunol. 13, 535–542
(2013).13. Lawitz, E. et al. N. Engl. J. Med. 368, 1878–1887
(2013).14. Denniston, M. M., Klevens, R. M., McQuillan, G. M. &
Jiles, R. B. Hepatology 55, 1652–1661 (2012).15. Dore, G. J., Ward, J. & Thursz, M. J. Viral Hepat. 21
(suppl. 1) 1–4 (2014).
N E U R O L O G I C A L D I S O R D E R S
Quality-control pathway unlockedA modified ubiquitin protein has been identified by three independent studies as the missing link in a cellular quality-control pathway that is implicated in Parkinson’s disease. See Letter p.162
A S A A B E L I O V I C H
Parkinson’s disease, a progressive neurodegenerative disorder, has long been hypothesized to be caused by defects in
organelles called mitochondria, which power mammalian cells through the production of ATP molecules. An accumulation of dysfunctional mitochondria may lead not only to a cellular energy crisis, but also to excessive production of toxic byproducts. Two enzymes implicated in Parkinson’s disease, PINK1 and parkin1,2, are thought to be involved in the disposal of defective mitochondria, but how
the two proteins interact has been unclear. A trio of studies (by Kane et al.3, writing in the Journal of Cell Biology; by Kazlauskaite et al.4, in the Biochemical Journal; and by Koyano et al.5, on page 162 of this issue) now report that phosphorylated ubiquitin protein is the link between PINK1 and parkin, providing insights into a complex system of parkin regulation.
Kinase enzymes such as PINK1 alter the behaviour of target proteins through the addition of phosphate groups, a process called phosphorylation. PINK1 is imported to mitochondria and, in healthy cells, undergoes
4 4 | N A T U R E | V O L 5 1 0 | 5 J U N E 2 0 1 4
NEWS & VIEWSRESEARCH
© 2014 Macmillan Publishers Limited. All rights reserved