Embed Size (px)
Citation preview
Hepatitis C:The State of Medicaid Access
2017 NATIONAL SUMMARY REPORTOctober 23, 2017

TABLE OF CONTENTSIntroduction..........................................................................................................................1Methods..............................................................................................................................2Findings..............................................................................................................................3Discussion........................................................................................................................16Conclusion............................................................................................................................19

Page 1
INTRODUCTION
Theadventin2013ofdirect-actingantivirals(DAAs)tocombatHepatitisC(HCV)wasamajordevelopment in curing the deadliest infectious disease in the United States. Unfortunately,despitetheimportantindividualandpublichealthpotentialofthesemedicationsmanypublicandprivatepayerschoosetolimitaccesstoDAAsduetotheircostaswellasotherconcerns.These limitations, generally expressed in prior authorization restrictions, form a significantbarriertocareformillionsofAmericansenrolledinMedicaid,despiteclearguidancefromtheCenters forMedicare andMedicaid Services that such restrictions often violate federal law.1Additionally, these restrictionsare indirectopposition to the“Recommendations forTesting,Managing,andTreatingHepatitisC”aspublishedbytheAmericanAssociationfortheStudyofLiverDiseases(AASLD)andtheInfectiousDiseasesSocietyofAmerica(IDSA).2
In2015,theCenterforHealthLawandPolicyInnovationofHarvardLawSchool(CHLPI),alongwithacademicresearchersatBrownUniversityandtheMiriamHospital,UniversityofNewSouthWales,andtheTreatmentActionGroup,publishedintheAnnalsofInternalMedicineasurveyofaccessrestrictionstoDAAsinstateMedicaidprogramsasofDecember2014.3SinceDecember2014,access toDAAs in stateMedicaidprogramshasbeen incrementallyexpanded,often inresponsetoadvocacyandimpactlitigation.
In the2017 “Hepatitis C: The StateofMedicaidAccess” report, CHLPI and theNationalViralHepatitisRoundtable(NVHR)updateandexpandupontheinitialsurveytodocumentthecurrentstateofaccessforMedicaidenrolleesacrosstheUnitedStates.The2017reportprovidesanin-depth evaluation of DAA access in each state’sMedicaid program, highlighting successes inaccess expansion as well as ongoing challenges. Alongside this report, CHLPI and NVHR arereleasingstate-specific“reportcards”thatreflectoverallHCVtreatmentaccessineachstate.Aspoliciescontinuetochangeonanongoingbasis,thedatapresentedinthisNationalSummaryReportaswellasthereportcardsiscurrentasofthefirsthalfof2017.
The2017reportfocusesonthreeofthemostsignificantrestrictivecriteriaMedicaidprogramsuse as methods of rationing access to the HCV cure: 1) fibrosis (liver damage or diseaseprogressionrequiredpriortotreatment);2)sobriety(periodsofabstinencefromalcoholand/orsubstanceuserequired);and3)prescriber(prescribingeligibilitylimitedtocertaincategoriesofspecialistpractitioners).
Overall,our2017analysisofthedatarevealsthatsince2014,transparencyofstateMedicaidprogramaccessrestrictionshasincreased.TheoverwhelmingmajorityofstatesnowhavetheirHCV treatment restriction criteria publicly available. In a few cases, however, states’ HCV
1CentersforMedicareandMedicaidServices,AssuringMedicaidBeneficiariesAccesstoHepatitisC(HCV)Drugs(ReleaseNo.172),Nov.5,2015,availableathttps://www.medicaid.gov/medicaid/prescription-drugs/hcv/index.html.2TheAmericanAssociationfortheStudyofLiverDiseasesandtheInfectiousDiseasesSocietyofAmerica,HCVGuidance:RecommendationsforTesting,Managing,andTreatingHepatitisC,Sep.21,2017,availableathttps://www.hcvguidelines.org/.3BaruaS.,Greenwald,R.,Grebely,J.,Dore,G.,Swan,T.,andTaylor,L.RestrictionsforMedicaidReimbursementofSofosbuvirfortheTreatmentofHepatitisCVirusInfectionsintheUnitedStates,163ANNINTERNMED.215(2015).

Page 2
treatmentrequirementsremainonlyavailablethroughdirectcommunicationwithofficials; inevenfewercasestheyremainunknowndespiterepeatedeffortstoidentifyrestrictions.Duringthis same time period, access to HCV treatment has improved. Among the progressmade,several states have completely eliminated fibrosis restrictions, while a significant number ofotherstateshavereducedtheirrestrictions.Toalesserextent,restrictionsaroundsobrietyandprescriberlimitationshavealsoimproved.
AsMedicaidprogramsincreasinglyfunnelenrolleesintomanagedcareorganizations(MCOs),the2017reportprovidesuswithacomprehensivenationalassessmentofMCOcoverageofHCVtreatment. In general, the findings indicate that although some MCOs have low levels ofrestrictions, many follow their states’ fee-for-service (FFS) Medicaid restrictions. While,consistentwithfederalMedicaidlaw,MCOsmustattheveryleastoffersimilarorlessrestrictivecoverageastheirrespectivestate’sFFSprogram,someMCOsimposemoreonerousrestrictions.4
AsrequiredbyfederalMedicaidlawandnationaltreatmentguidelines,stateMedicaidprogramsshouldeliminatetheremainingrestrictionsaroundfibrosis,sobriety,andprescriberlimitationsidentified in the 2017 report. Increased scrutiny must also focus onMCOs because of theincreasingnumberofMedicaidenrolleesfunneledintomanagedcare.AswithMedicaidFFS,noMCOshouldrequirerestrictivecoveragecriteriatoaccessHCVtreatment.
METHODS
WeevaluatedMedicaidreimbursementcriteriaforavailableDAAsforall50states,theDistrictofColumbia,andPuertoRico.Theinformationfor2014wasgleanedfromthesurveypublishedin theAnnalsof InternalMedicine. ThatsurveydrewuponstateMedicaidwebsitematerialspostedbetweenJune23andDecember7,2014.Datafor2014wasextractedbytwoco-authorsin duplicate and entered into a spreadsheet, with two different co-authors evaluating theextracteddata.Anydifferenceswereresolvedbyconsensus.
Forthe2017survey,wefirstsentaformsurveytoeachstate’sMedicaidofficialsrequestingtheirFFS coverage criteria for DAAs. Where states were unresponsive, we again searched stateMedicaidwebsitesforpubliclyavailablereimbursementcriteria. Allofthedatafor2017wascrosscheckedbyCHLPIandNVHR. Wheresurvey responsesconflictedwithpubliclyavailablecriteria,differenceswereresolvedeitherbydirectcommunicationwithMedicaidofficialsorbyconsensus. For each state, in both 2014 and 2017, data was extracted from Medicaidreimbursementcriteria, includingwhetherDAAswerecovered(paidforbyMedicaid)andthecriteriaforcoverage.Thepreferreddruglistswerealsorecordedandenteredintoeachstate’sreportcard.
Coveragecriteriawasfurtherbrokendownbyrestrictiontype.Forcriteriaaboutliverdiseasestaging,datawascollectedontheleveloffibrosis(liverscarring)requiredpriortoauthorizationoftreatment.CriteriarangedfromMeta-AnalysisofHistologicalDatainViralHepatitis(METAVIR)
442CFR§438.210.

Page 3
fibrosisstageF0(nofibrosis)throughF4(cirrhosis).Forsobrietycriteria,datawascollectedonwhether drug or alcohol screening and counseling was required and whether a period ofabstinence (1, 3, 6, or 12 months) was required prior to authorizing HCV treatment. Forprescribertype,datawascollectedonwhetheranyprovidermayprescribetreatment,whetherprimarycarephysiciansmustconsultaspecialist,orwhethertheprescriberhadtobeaspecialist,usuallypracticingingastroenterology,hepatology,infectiousdiseases,orlivertransportation.
Our2017surveyexpandedinscopefromthe2014examinationofHCVtreatmentaccesscriteriafor both Medicaid fee-for-service (FFS) programs and MCOs. Because multiple MCOs mayoperateinastateandtheirrestrictionsmayvary,MCOcoveragemaybeexpressedinarange.Forexample,insomestatesoneMCOmayofferaccesstoDAAsforeveryonewhotestsatF2orhigherwhereasacompetitormaynotimposeaminimumfibrosisscore.Forthepurposesofthe2017 survey, we have categorized states with confirmed variation between their MCOsseparately. AnotherchallengetocategorizeaccesstoHCVtreatmentinmanagedcareisthatsomeMCOsrefusetoclarifytheiraccessrestrictions.IfwewereunabletoconfirmanyMCO’streatmentcriteria,weclassifiedthatstateas“RestrictionsUnknown.”However,ifwewereabletoconfirmatleastoneMCO’scriteriawheremultipleMCOsoperate,wecategorizedthatstateaccordingly.
FINDINGS
Findings:LiverDamageRestrictions
Liverdamage(fibrosis)restrictionsareoneoftheforemostandcommonbarrierstoaccessingDAAsinstateMedicaidprograms.TheserestrictionsrequirepatientstowaituntilHCVdamagestheirlivertoacertainlevel,asmeasuredbytheMETAVIRfibrosisscale.AMETAVIRscoreofF0indicates no fibrosis, whereas F4 indicates damage to the liver that is so severe as to beconsideredcirrhosis.
Since2014,progresshasbeenmadeineasingtheserestrictions,buttoomanystatescontinuetolimitaccesstoonlythoseindividualswhoseHCVhasprogressedtoatleastmoderate(F2)oradvanced(F3)fibrosis.ByrequiringpatientstodemonstrateaminimumlevelofliverdamagebeforetheyqualifyfortreatmentwithDAAs,MedicaidprogramsareforcingindividualstowaituntiltheirhealthworsensinordertoaccessthecureforHCV.
Comparing2014and2017MedicaidFee-for-ServiceLiverDamageRestrictions
Overall, transparency in liver damage restrictions has improved dramatically since the 2014survey,withasignificantnumberofstatesclarifyingtheirfibrosisrequirementsfortreatmentwithDAAs.In2017,allstates’fee-for-serviceprogramshaveknowncriteria(includingtheDistrictofColumbia’sandPuertoRico’sprograms).Thisisopposedtoonly34states(67%)in2014.Mostimportantly,manystateshaveeasedtheirliverdamagerestrictionssince2014.In2017,18states(35%)donot requirepatients todemonstrateaminimumlevelof liverdamagetoqualify fortreatmentwithDAAs. In2014,nostatemetthiscriterion. In2017,4states (8%)requirean

Page 4
individualtodemonstratemildfibrosis(F1)asopposedtoonestate(3%)in2014.In2017,18states(35%)requireanindividualtodemonstrateatleastmoderatefibrosis(F2)ascomparedtotwostates(6%)in2014.
WhilemanystatescontinuetorequirepatientstodemonstrateseriousliverdamagebeforetheycanaccessthecuretoHCV,the2017findingsdemonstrateadramaticimprovementover2014.In2014,ofthe34stateswithknowncriteria,31states(91%)limitedaccesstoDAAstoonlythosepatientsthatcoulddemonstrateadvancedfibrosisorcirrhosis,with27states (79%)requiringadvancedfibrosis(F3),and4states(12%)requiringcirrhosisoftheliver(F4).Incomparison,in2017,12states (23%) requireat leastadvanced fibrosis (F3) toqualify for treatment,andnostatescontinuetorequirecirrhosisofthelivertoqualify.

Page 5
Chart1:Comparing2014and2017MedicaidFFSLiverDiseaseRestrictions
Category 2014NumberofStateswithFFSLiverDamageRestriction
2014States 2017NumberofStateswithFFSLiverDamageRestriction
2017States
NoRestrictions
0(0%)56 None 18(35%)7 Alaska,Connecticut,Florida,Georgia,Maine,Massachusetts,Minnesota,Mississippi,Nevada,NewHampshire,NewYork,NorthDakota,PuertoRico,SouthCarolina,Virginia,Washington,Wisconsin,Wyoming
F1 1(3%) Maine 4(8%) Hawaii,NewMexico*,Pennsylvania,Utah
F2 2(6%) Maryland,Oklahoma 18(35%) Alabama,Arizona,California,Colorado,Delaware,DistrictofColumbia,Idaho,Indiana,Kentucky,Maryland,Michigan,NewJersey,NorthCarolina*,Ohio*,Oklahoma,Tennessee,Vermont,WestVirginia
F3 27(79%) Alaska,Arizona,Arkansas,California,Colorado,DistrictofColumbia,Florida,Idaho,Indiana,Iowa,Kentucky,Louisiana,Missouri,Montana,Nebraska,NewHampshire,NewYork,Ohio,Pennsylvania,RhodeIsland,SouthDakota,Tennessee,Vermont,Virginia,Washington,WestVirginia,Wisconsin
12(23%) Arkansas,Illinois,Iowa,Kansas,Louisiana,Missouri*,Montana,Nebraska,Oregon,RhodeIsland,SouthDakota,Texas
F4 4(12%) Connecticut,Delaware,Illinois,Oregon
0(0%) None
RestrictionsUnknown
18 Alabama,Georgia,Hawaii,Kansas,Massachusetts,Michigan,Minnesota,Mississippi,NewJersey,NewMexico,Nevada,NorthCarolina,NorthDakota,PuertoRico,SouthCarolina,Texas,Utah,Wyoming
0 None
5Percentagesarecalculatedbasedonthenumberofstatesthathadknownrestrictionsinagivenyear.For2014FFSMedicaidprograms,34stateshadknownfibrosisrestrictions.6Duetorounding,percentagesineachchartmaynotaddupto100%.7Percentagesarecalculatedbasedonthenumberofstatesthathadknownrestrictionsinagivenyear.For2017FFSMedicaidprograms,all52jurisdictionssurveyedhadknownfibrosisrestrictions.*Missouri,NewMexico,NorthCarolina,andOhioareallintheprocessofcompletelyeliminatingtheirfibrosisrestrictions,buthavenotdonesoyetatthetimeofthisreport.

Page 6
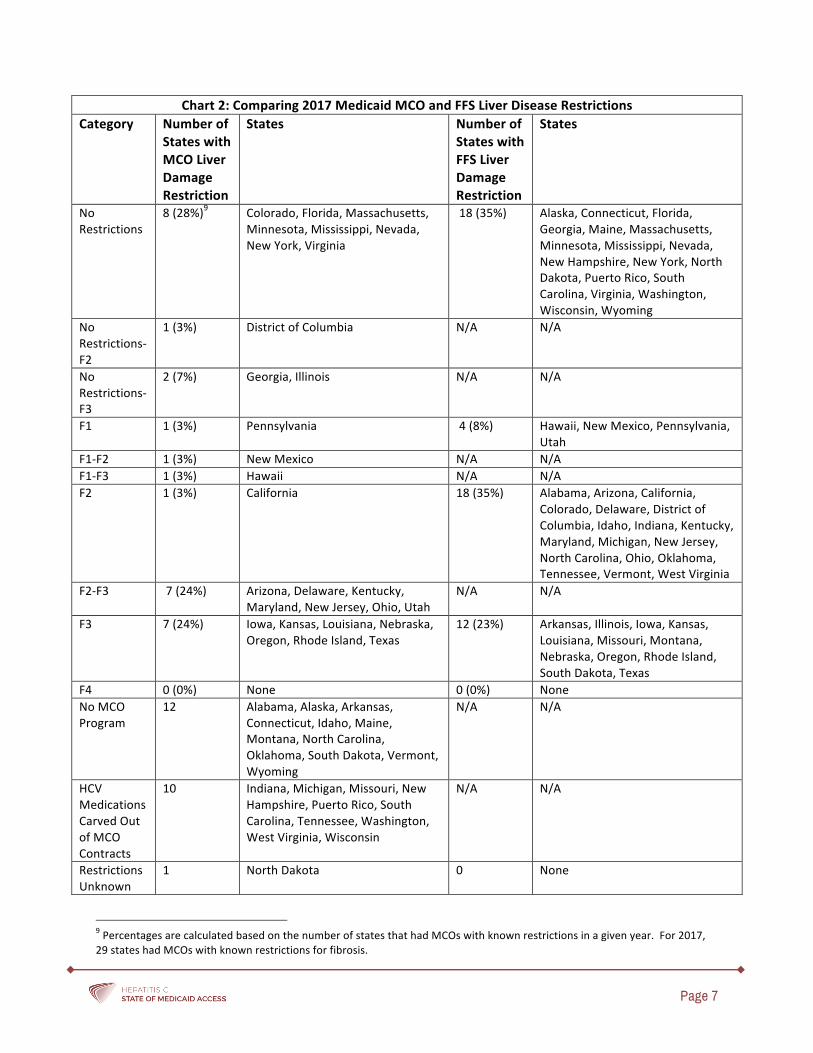
Comparing 2017 Medicaid Managed Care Organization and Fee-for-Service Liver DamageRestrictions
In2017,40states,includingtheDistrictofColumbiaandPuertoRico,haveMedicaidMCOs,as12statesdonothavecommercialMCOsintheirMedicaidprograms.Additionally,10stateshavecarved-outeitherDAAsorallprescriptiondrugsfromtheirMCOcontracts.Inthesestates,theFFSprogramsetsthecriteriaforDAAtreatment,evenforbeneficiariesenrolledinanMCO.Thus,30 states contract withMCOs to provide DAA treatment for theirMedicaid enrollees. As totransparency,29ofthesestateshaveatleastoneMCOwithpublishedliverdamagerestrictions.Ofthe29stateswithMCOswithavailableinformation,10states(34%)haveatleastoneMCOwithliverdamagerestrictionsthataremorerestrictivethantheircorrespondingFFSprogram.ThisisthecasedespitethefactthatMedicaidprogramsmust,bylaw,ensurethattheirMCOsoffersimilarorlessrestrictivecoveragetotheFFSprograminthestate.8
Eightstates(28%)withMCOsthatprovideDAAstoenrolleeshavenoliverdamagerestrictions.Eighteenstates’FFSprograms(35%)donot impose liverdamagerestrictions, includingsevenstatesthathavenorestrictionsineithertheirMCOsorFFSprograms,ninestatesthateitherdonothaveMCOsorhave carvedoutDAAs from theirMCOcontracts,one statewhoseMCO’srestrictions areunknown, andone state (Georgia) that has at least oneMCOwhich requirespatientstodemonstrateatleastadvancedfibrosis(F3)toqualifyfortreatmentwithDAAs.TheDistrict of Columbiahas at least oneMCO thatdoesnot impose liver damage requirements,althoughsomeMCOsrequireapatienttodemonstrateatleastmoderatefibrosis(F2)toqualify.Incontrast,thedistrict’sFFSprogramrequirespatientstoprogresstoF2priortotreatment.Twostates(7%),GeorgiaandIllinois,haveMCOsthatdonotimposeminimumfibrosisrequirements,althoughsomeMCOsinthesestatesrequirepatientstodemonstrateF3. Pennsylvania istheonlystatewhoseMCOsrequirepatientstodemonstratemildfibrosis(F1),whereas4states’FFSprograms(8%)sharethiscriterion. NewMexicoandHawaii’sMCOseachrequireat leastF1,although someMCOs require F2 and F3 respectively, despite the fact that both state’s FFSprogramsonly require patients to demonstrate F1. California is the only statewhoseMCOsrequirepatientstodemonstrateF2toqualify,whereas18states’FFSprograms(35%)sharethiscriterion, includingninestateswithMCOsthatprovideDAAstotheirenrollees. Sevenstates’(24%)MCOsvaryinthatwhilesomeonlyrequireF2,othersrequireatleastF3.Sevenstates’MCOsrequireatleastF3toqualifyfortreatment,whereas12states’FFSprograms(23%)sharethis criterion, including ten stateswithMCOs that processDAA treatments. Fortunately, nostate’sMCOsrequirepatientstodemonstratecirrhosis(F4)toqualifyfortreatment.
842CFR§438.210.
Page 7
Chart2:Comparing2017MedicaidMCOandFFSLiverDiseaseRestrictionsCategory Numberof
StateswithMCOLiverDamageRestriction
States NumberofStateswithFFSLiverDamageRestriction
States
NoRestrictions
8(28%)9 Colorado,Florida,Massachusetts,Minnesota,Mississippi,Nevada,NewYork,Virginia
18(35%) Alaska,Connecticut,Florida,Georgia,Maine,Massachusetts,Minnesota,Mississippi,Nevada,NewHampshire,NewYork,NorthDakota,PuertoRico,SouthCarolina,Virginia,Washington,Wisconsin,Wyoming
NoRestrictions-F2
1(3%) DistrictofColumbia N/A N/A
NoRestrictions-F3
2(7%) Georgia,Illinois N/A N/A
F1 1(3%) Pennsylvania 4(8%) Hawaii,NewMexico,Pennsylvania,Utah
F1-F2 1(3%) NewMexico N/A N/AF1-F3 1(3%) Hawaii N/A N/AF2 1(3%) California 18(35%) Alabama,Arizona,California,
Colorado,Delaware,DistrictofColumbia,Idaho,Indiana,Kentucky,Maryland,Michigan,NewJersey,NorthCarolina,Ohio,Oklahoma,Tennessee,Vermont,WestVirginia
F2-F3 7(24%) Arizona,Delaware,Kentucky,Maryland,NewJersey,Ohio,Utah
N/A N/A
F3 7(24%) Iowa,Kansas,Louisiana,Nebraska,Oregon,RhodeIsland,Texas
12(23%) Arkansas,Illinois,Iowa,Kansas,Louisiana,Missouri,Montana,Nebraska,Oregon,RhodeIsland,SouthDakota,Texas
F4 0(0%) None 0(0%) NoneNoMCOProgram
12 Alabama,Alaska,Arkansas,Connecticut,Idaho,Maine,Montana,NorthCarolina,Oklahoma,SouthDakota,Vermont,Wyoming
N/A N/A
HCVMedicationsCarvedOutofMCOContracts
10 Indiana,Michigan,Missouri,NewHampshire,PuertoRico,SouthCarolina,Tennessee,Washington,WestVirginia,Wisconsin
N/A N/A
RestrictionsUnknown
1 NorthDakota 0 None
9PercentagesarecalculatedbasedonthenumberofstatesthathadMCOswithknownrestrictionsinagivenyear.For2017,29stateshadMCOswithknownrestrictionsforfibrosis.

Page 8
Findings:SobrietyRestrictions
Another widespread restriction on DAA treatment access are restrictions related to alcoholand/orsubstanceuse. ManyMedicaidprogramsrequireindividualstoabstainfromuseforaspecifiedtimeframepriortostartingtreatment.Othersrequireindividualstosubmittoscreeningorattesttomaintainingabstinenceduringtreatment,orrequireproviderstocounselpatientsonsubstanceuseandinsomecases,referactiveusersfortreatment(acategorythisreportcalls“ScreeningandCounseling”).
ThesecommonrestrictionsoncareunderminetherecommendationsoftheAASLD/ISDAthatarewidelyrecognizedasthestandardofcare.Currentresearchshowsthatpeoplewhoinjectdrugsachievesimilarcurerates(sustainedvirologicresponse)ascomparedtopatientswhodonotusedrugs.10Additionally,injectiondruguseistheforemostdrivingfactorintheperpetuationoftheHCVepidemicwithintheUnitedStates.AstheAASLD/ISDAguidancenotes,“testingandlinkageto care combinedwith the treatment of HCV infectionwith potent interferon-free regimens[DAAs] has the potential to dramatically decrease HCV incidence and prevalence.”11 Thus,postponingaccesstocareforpeoplewhousesubstancesorotherwisedonotmaintainsobrietynotonlyallowsthehealthoftheseindividualstodeteriorate,butalsounderminespublichealtheffortstoendtheHCVepidemic.
Comparing2014and2017MedicaidFee-for-ServiceSobrietyRestrictions
In 2014 survey, 37 states (73%of those surveyed)had known sobriety requirements in theireligibilitycriteriaforreimbursement.Inthe2017survey,alljurisdictionsresearchedhadknownsobrietyrequirements,illustratingtheprogressmadeintermsofincreasingtransparency.
In 2017, 10 states (19%) do not impose abstinence periods or mandated screening as arequirementfortreatment.Nostatemetthiscriteriain2014.Thenumberandproportionofstates that required screening and counseling but did not impose abstinence requirementschangedfrom9states(24%) in2014to15states(29%) in2017. As in2014,twostates(4%)continuetorequireindividualstodemonstrateatleastonemonthofsobrietybeforereceivingtreatmentin2017.Fivestates(10%)in2017requireindividualstoabstainfromsubstanceusefor3monthsbeforereceivingtreatmentascomparedto6states(16%)in2014.Thenumberofstates requiring that individuals abstain from substance use for 6months prior to receivingtreatmentremainedconstantfrom2014to2017at18states,butdecreasedasapercentageofallstateswithknownsobrietyrestrictionsintheirFFSprogramsfrom49%in2014to35%in2017.Twostates (4%)continuetomandatea fullyearofsobrietyprior totreatment in2017. Twostatesalsoimposedthisrestrictionin2014.
10AspinallEJ,CorsonS,DoyleJS,etal.,TreatmentofhepatitisCvirusinfectionamongpeoplewhoareactivelyinjectingdrugs:asystematicreviewandmeta-analysis,57CLININFECTDIS.S80(2013).11TheAmericanAssociationfortheStudyofLiverDiseasesandtheInfectiousDiseasesSocietyofAmerica,HCVGuidance:RecommendationsforTesting,Managing,andTreatingHepatitisC,Sep.21,2017,availableathttps://www.hcvguidelines.org/.

Page 9
Chart3:Comparing2014and2017MedicaidFFSSobrietyRestrictionsCategory 2014
NumberofStateswithFFSSobrietyRestriction
2014States 2017NumberofStateswithFFSSobrietyRestriction
2017States
NoRestrictions
0(0%)12 None 10(19%)13 California,Connecticut,Indiana,Massachusetts,Missouri,Nevada,NewJersey,Utah,Vermont,Washington
ScreeningandCounseling
9(24%) Arkansas,Maine,Massachusetts,NewHampshire,NewYork,NorthCarolina,Ohio,Vermont,Virginia
15(29%) Alaska,Colorado,Delaware,DistrictofColumbia,Georgia,Illinois,Maryland,NewHampshire,NewMexico,NewYork,NorthCarolina,Pennsylvania,RhodeIsland,SouthCarolina,Virginia
Abstainfor1month
2(5%) Florida,Wyoming 2(4%) Florida,Wyoming
Abstainfor3months
6(16%) Alaska,Delaware,DistrictofColumbia,Iowa,Missouri,Washington
5(10%) Arizona,Hawaii,Iowa,Texas,WestVirginia
Abstainfor6months
18(49%) Alabama,Arizona,California,Colorado,Idaho,Kentucky,Maryland,Mississippi,Montana,Nebraska,Oklahoma,Oregon,Pennsylvania,RhodeIsland,SouthDakota,Tennessee,WestVirginia,Wisconsin
18(35%) Alabama,Arkansas,Idaho,Kansas,Kentucky,Maine,Michigan,Minnesota,Mississippi,Montana,Nebraska,Ohio,Oklahoma,Oregon,PuertoRico,SouthDakota,Tennessee,Wisconsin
Abstainfor12months
2(5%) Illinois,Louisiana 2(4%) Louisiana,NorthDakota
RestrictionsUnknown
15 Connecticut,Indiana,Georgia,Hawaii,Kansas,Michigan,Minnesota,Nevada,NewJersey,NewMexico,NorthDakota,PuertoRico,SouthCarolina,Texas,Utah
0 None
Comparing 2017 Medicaid Managed Care Organization and Fee-for-Service SobrietyRestrictions
In 2017, 30 states, including theDistrict of Columbia, haveMedicaidMCOs that deliverDAAtreatmenttoenrollees,andallbutonestatehasatleastoneMCOwithpublishedcriteria.Ofthe29stateswithknownsobrietycriteria,8states(28%)contractwithatleastoneMCOthathas
12Percentagesarecalculatedbasedonthenumberofstatesthathadknownrestrictionsinagivenyear.For2014FFSMedicaidprograms,37stateshadknownrestrictionsforsobriety.13Percentagesarecalculatedbasedonthenumberofstatesthathadknownrestrictionsinagivenyear.For2017FFSMedicaidprograms,all52jurisdictionssurveyedhadknownsobrietyrestrictions.

Page 10
sobrietyrestrictionsthataremoreonerousthantheircorrespondingFFSprogram.ThesefurtherrestrictionspersisteventhoughMedicaidprogramsmust,bylaw,ensurethattheirMCOsoffersimilarorlessrestrictivecoveragetotheFFSprograminthestate.14
Four states (14%) of the 29 with MCOs with publicly available criteria do not impose anyrestrictions related to substance use, whereas 10 state FFS programs (19%) do not requiresobrietyorscreening.In4states(14%),MCOsrequirescreeningandcounselingasopposedto15stateFFSprograms(29%).Inonestate(3%),MCOsrequirepatientstoabstainforatleast1monthpriortotreatmentasopposedto2FFSprograms(4%).TheMCOsin2states(7%)requireenrollees to abstain for at least 3 months, whereas 5 state FFS programs (10%) share thiscriterion.In4states(14%),theMCOsuniformlyrequireindividualstoabstainfromsubstanceuseforatleast6monthspriortotreatment.Bycontrast,18stateFFSprograms(35%)havethesame requirements. Fortunately, no state contracts with MCOs that require a full year ofabstinenceprior to treatment,whereas twostateFFSprograms (4%)continueto imposethisbarrier.InapluralityofstateswithMCOswithknownrestrictions,14states(48%),includingtheDistrictofColumbia,haveMCOswhosesobrietyrestrictionsvarysignificantly,generallywithatleastoneMCOrequiringonlyscreeningandcounselingandatleastoneMCOrequiring3to6monthsofabstinencefortreatmenttobeauthorized.
1442CFR§438.210.

Page 11
Chart4:Comparing2017MedicaidMCOandFFSSobrietyRestrictionsCategory Numberof
StateswithManagedCareSobrietyRestriction
States NumberofStateswithFFSSobrietyRestriction
States
NoRestrictions
4(14%)15 California,Massachusetts,Nevada,RhodeIsland
10(19%) California,Connecticut,Indiana,Massachusetts,Missouri,Nevada,NewJersey,Utah,Vermont,Washington
ScreeningandCounseling
4(14%) Colorado,Georgia,NewMexico,Pennsylvania
15(29%) Alaska,Colorado,Delaware,DistrictofColumbia,Georgia,Illinois,Maryland,NewHampshire,NewMexico,NewYork,NorthCarolina,Pennsylvania,RhodeIsland,SouthCarolina,Virginia
Abstainfor1month
1(3%) Florida 2(4%) Florida,Wyoming
Abstainfor3months
2(7%) Iowa,Texas 5(10%) Arizona,Hawaii,Iowa,Texas,WestVirginia
Abstainfor6months
4(14%) Kansas,Mississippi,Nebraska,Oregon
18(35%) Alabama,Arkansas,Idaho,Kansas,Kentucky,Maine,Michigan,Minnesota,Mississippi,Montana,Nebraska,Ohio,Oklahoma,Oregon,PuertoRico,SouthDakota,Tennessee,Wisconsin
Abstainfor12months
0(0%) None 2(4%) Louisiana,NorthDakota
Varied 14(48%) Arizona,Delaware,DistrictofColumbia,Hawaii,Illinois,Kentucky,Louisiana,Maryland,Minnesota,NewJersey,NewYork,Ohio,Utah,Virginia
N/A N/A
NoManagedCareProgram
12 Alabama,Alaska,Arkansas,Connecticut,Idaho,Maine,Montana,NorthCarolina,Oklahoma,SouthDakota,Vermont,Wyoming
N/A N/A
HCVMedicationsCarvedOutofMCOContracts
10 Indiana,Michigan,Missouri,NewHampshire,PuertoRico,SouthCarolina,Tennessee,Washington,WestVirginia,Wisconsin
N/A N/A
RestrictionsUnknown
1 NorthDakota 0 None
15PercentagesarecalculatedbasedonthenumberofstatesthathadMCOswithknownrestrictionsinagivenyear.For2017,29stateshadMCOswithknownrestrictionsforsobriety.

Page 12
Findings:PrescriberRestrictions
MedicaidprogramssometimesrestrictaccesstoHCVtreatmentbylimitingwhichprovidersareeligible to prescribe DAAs, often only allowing specialists such as hepatologists,gastroenterologists,orinfectiousdiseasepractitionerstoprescribe,orbyrequiringthatpatientsatleastobtainaconsultationwithoneofthesespecialistspriortotreatment.Medicaidprogramsthat limit the ability to prescribe DAAs to certain specialists create a prescriber bottleneckbecausespecialistsoftenhavelimitedbandwidthtotreatthenumberofpeopleinneedofHCVtreatment and/or to consult with other providers. Additionally, prescriber limitations maypresent practical access barriers for beneficiaries that live in rural or otherwise sparselypopulatedareasthatmaynothaveaspecialistnearby.DAAshaverelativelyfewsideeffectsandarenotdifficulttomonitorduringtheshortcourseoftreatment.ProviderswhoareskilledandpossesstherequisiteknowledgefortreatingHCV,whetherornottheyareaspecialist,shouldbeallowedtoprescribeDAAsandtreatpeoplelivingwithHCV.
Comparing2014and2017MedicaidFee-for-ServicePrescriberRestrictions
In2017, transparencyregardingprescriberrestrictions increasedsignificantly. Onlyonestate(2%)in2017didnothaveknownprescriberrestrictionsforHCVtreatment,ascomparedto22states(42%)in2014.Oftheremaining51jurisdictionswithavailableinformation,14states(27%)donotrequireaspecialisttoprescribeorconsult,whereasnostatemetthiscriteria in2014.Twenty-eightstates (55%)withknownprescriberrestrictionsrequirethataspecialistmustatleastbeconsultedbeforeDAAtreatmentwillbeauthorized,asopposedtoonly15states(52%)in2014.Ninestates(18%)onlyapprovetreatmentwhenaspecialistprescribesDAAtherapy,ascomparedto14states(48%)in2014.

Page 13
Chart5:Comparing2014and2017MedicaidFFSPrescriberRestrictionsCategory 2014
NumberofStateswithFFSPrescriberRestriction
2014States 2017NumberofStateswithFFSPrescriberRestriction
2017States
Norestrictions 0(0%)16 None 14(27%)17 Alaska,Alabama,California,Connecticut,Delaware,Georgia,Massachusetts,Missouri,Nebraska,Nevada,NewMexico,NorthCarolina,Wisconsin,Wyoming
Byorinconsultationwithspecialist
15(52%) Arizona,California,Colorado,Connecticut,Idaho,Illinois,Kentucky,Louisiana,Mississippi,Oklahoma,Oregon,SouthDakota,Utah,Virginia,WestVirginia
28(55%) Arizona,Colorado,DistrictofColumbia,Florida,Hawaii,Idaho,Illinois,Indiana,Kansas,Kentucky,Maine,Maryland,Michigan,Minnesota,Mississippi,NewHampshire,NewYork,NorthDakota,Oklahoma,Oregon,PuertoRico,SouthCarolina,Texas,Utah,Vermont,Virginia,Washington,WestVirginia
Specialistmustprescribe
14(48%) Florida,Indiana,Iowa,Maine,Maryland,Montana,NewHampshire,NewYork,Ohio,Pennsylvania,RhodeIsland,Tennessee,Washington,Wisconsin
9(18%) Arkansas,Iowa,Louisiana,Montana,Ohio,Pennsylvania,RhodeIsland,SouthDakota,Tennessee
RestrictionsUnknown
23
Alabama,Alaska,Arkansas,Delaware,DistrictofColumbia,Georgia,Hawaii,Kansas,Massachusetts,Michigan,Minnesota,Missouri,Nebraska,Nevada,NewJersey,NewMexico,NorthCarolina,NorthDakota,PuertoRico,SouthCarolina,Texas,Vermont,Wyoming
1 NewJersey
16Percentagesarecalculatedbasedonthenumberofstatesthathadknownrestrictionsinagivenyear.For2014FFSMedicaidprograms,29stateshadknownrestrictionsforprescribingprivileges.17Percentagesarecalculatedbasedonthenumberofstatesthathadknownrestrictionsinagivenyear.For2017FFSMedicaidprograms,51stateshadknownrestrictionsforprescribingprivileges.

Page 14
Comparing 2017 Medicaid Managed Care Organization and Fee-for-Service PrescriberRestrictions
In 2017, 30 states, including theDistrict of Columbia, haveMedicaidMCOs that deliverDAAtreatmenttoenrollees,andallbutonestatehasat leastoneMCOwithpublishedcriteria.Ofthese29stateswithknownprescriberrestrictions,12statescontractwithatleastoneMCOthathas prescriber restrictions that are more burdensome than their state’s corresponding FFSprogram.ThisisthecasedespitethefactthatMedicaidprogramsmaynot,bylaw,allowtheirMCOstoprovidemorerestrictivecoveragethantheFFSprograminthestate.18
Six states’MCOs (21%) uniformly do not require a specialist to prescribe or consult prior totreatmentwithDAAs,asopposedto14state(27%)FFSprograms.Threestates(10%)haveatleastoneMCOthatdoesnot imposeprescriberrestrictions,aswellasat leastoneMCOthatrequires either a specialist to consult or prescribe themselves. Five states’MCOs (17%) onlyrequire thata specialist is consultedbefore treatment,whereas28stateFFSprograms (55%)sharethiscriterion.Tenstates(34%)haveatleastoneMCOthatonlyrequiresconsultation,aswellasatleastoneMCOthatrequiresaspecialisttoprescribe.Another5states’MCOs(17%)uniformlyrequireaspecialistprescribeDAAtherapy,asopposedto9stateFFSprograms(18%).
1842CFR§438.210.

Page 15
Chart6:Comparing2017MedicaidMCOandFFSPrescriberRestrictionsCategory NumberofStates
withManagedCarePrescriberRestriction
States NumberofStateswithFFSPrescriberRestriction
States
Norestrictions 6(21%)19 California,Georgia,Massachusetts,Nebraska,Nevada,NewMexico
14(27%) Alaska,Alabama,California,Connecticut,Delaware,Georgia,Massachusetts,Missouri,Nebraska,Nevada,NewMexico,NorthCarolina,Wisconsin,Wyoming
Norestrictions-Byorinconsultationwithspecialist
1(3%) NewYork N/A N/A
Norestrictions-Specialistmustprescribe
2(7%) Kentucky,Utah N/A N/A
Byorinconsultationwithspecialist
5(17%) Colorado,Florida,Kansas,Mississippi,Texas
28(55%) Arizona,Colorado,DistrictofColumbia,Florida,Hawaii,Idaho,Illinois,Indiana,Kansas,Kentucky,Maine,Maryland,Michigan,Minnesota,Mississippi,NewHampshire,NewYork,NorthDakota,Oklahoma,Oregon,PuertoRico,SouthCarolina,Texas,Utah,Vermont,Virginia,Washington,WestVirginia
Byorinconsultationwithspecialist-Specialistmustprescribe
10(34%) Arizona,DistrictofColumbia,Hawaii,Illinois,Maryland,Minnesota,Ohio,Oregon,Pennsylvania,Virginia
N/A N/A
Specialistmustprescribe
5(17%) Delaware,Iowa,Louisiana,NewJersey,RhodeIsland
9(18%) Arkansas,Iowa,Louisiana,Montana,Ohio,Pennsylvania,RhodeIsland,SouthDakota,Tennessee
NoManagedCareProgram
12 Alabama,Alaska,Arkansas,Connecticut,Idaho,Maine,Montana,NorthCarolina,Oklahoma,SouthDakota,Vermont,Wyoming
N/A N/A
HCVMedicationsCarvedOutofMCOContracts
10 Indiana,Michigan,Missouri,NewHampshire,PuertoRico,SouthCarolina,Tennessee,Washington,WestVirginia,Wisconsin
N/A N/A
RestrictionsUnknown
1 NorthDakota 1 NewJersey
19PercentagesarecalculatedbasedonthenumberofstatesthathadMCOswithknownrestrictionsinagivenyear.For2017,29stateshadMCOswithknownrestrictionsforprescribingprivileges.

Page 16
DISCUSSION
MovingTowardTransparency
The most striking difference between our 2014 and 2017 findings is the extent to whichjurisdictionsaretransparentaboutthecriteriathatMedicaidbeneficiariesmustmeettoqualifyforHCVtreatment.In2014,18jurisdictionsdidnotpublishordiscloseinformationaboutfibrosisrestrictions,15didnotpublishsobrietyrestrictions,and23didnotpublishprescriberrestrictions.In 2017, all jurisdictions disclosed their criteria, with one exception. In New Jersey, the FFSprogram’sprescriberrestrictionsremainunclear.
The willingness of states to communicate clearly about their restrictions is welcome andnecessary.ProvidersandpatientsdeservetoknowtheimpedimentsthatexistordonotexistinobtainingHCVtreatmentwithineachplanofferedintheirstate.Byclarifyingtheirrequirements,stateshavealleviatedsomeoftheconcernsanduncertaintyabouttreatmentintheHCV-affectedcommunity. Accurate, up-to-date information is vital to ensuring that individuals who needtreatmentreceiveitandthatthosewhoaredeniedtreatmentareclearastothereasonswhy.Plain and simple language, regularly updated on each state’s website, is also imperative toeducatethepublicandpolicymakersaboutwhereprogressisneededtoachieveuniversalHCVtreatment.
FewerRestrictionsBasedonDiseaseSeverity
Ourfindingsrevealthatmorestatesareeliminatingorreducingrestrictionsthatrationtreatmentaccordingtoseverityofillness.In2014,FFSprogramsin4states(Connecticut,Delaware,Illinois,andOregon)requiredpatientstodemonstratecirrhosis(F4)toqualifyfortreatment.In2017,thatnumberstandsatzero.Mostnotably,Connecticutopenedaccesstoallpatientsregardlessof disease stage. After Connecticut became the first state to open access on this basis, 17additionaljurisdictions(16statesandPuertoRico)havejoinedsuitandhaveremovedalldiseaseseverityrestrictionsfromtheirFFSprograms.
Thenumberofjurisdictionsrequiringindividualstodemonstrateadvancedfibrosis(F3)intheirFFSprogramshasalsodroppedfrom27(26statesandtheDistrictofColumbia)in2014to12states in 2017.Many of the jurisdictions that had required patients to demonstrate F3 nowrequirethemtodemonstrateF2.TheFFSprogramsof18jurisdictions(17statesandtheDistrictof Columbia) require individuals to demonstrate moderate fibrosis (F2) in order to obtaintreatment.Fourstates(Hawaii,NewMexico,Pennsylvania,andUtah)mandateprogressiontomildfibrosis(F1)fortreatment.
MCOprograms in10 stateshavemore restrictive fibrosis criteria than theirFFScounterpartsdespite the legal obligation thatMCO programsmust not offer less comprehensive ormorerestrictivetreatmentthantheirstate’sFFSprograms.20SevenofthosestatesoperateMCOsthat
2042CFR§438.210.
Page 17
demandprogressiontoF2-F3.Forexample,GeorgiahassomeMCOsthatrequireprogressiontoF3althoughtheFFSprogrammaintainsnofibrosisrestrictions.PatientswithHCVareentitledtotreatmentregardlessofwhethertheyareenrolledinanMCOorFFSprogram.StateMedicaidprogramsmustensurethateligibilitycriteriaremainconsistentandthatmanagedcaredoesnotequatetodenialofcare.
Withoverathirdofstatescurrentlyimposingnofibrosisrestrictionsonpatients,progresstowardfullcompliancewiththelawamongMedicaidprogramsisnowundeniable.However,amajorityofstatesstillwithholdtreatmentuntilpatientshaveprogressedtoF1orhigher.Amongthem,30statesrequireindividualstodemonstrateF2orF3.21
SobrietyRequirementsRemainPervasive
Unfortunately, many states have maintained discriminatory sobriety restrictions to HCVtreatment,evenwhentheyhaverelaxedrestrictionsbasedondiseaseseverityand/orprescribertype.
ThemostdrasticexampleisLouisiana,whichsince2014hasrequiredindividualstodemonstrate12monthsofsobrietybeforequalifyingfortreatment.NorthDakotaalsoimposesa12monthsobrietyrestriction.Illinois,whichrequired12monthsofsobrietyin2014,hassincemovedinamore positive direction and now only requires screening and counseling before access totreatment.
In 2014 and 2017, 18 jurisdictions require 6 months of sobriety before initiating treatment(although some of the jurisdictions have changed). Five states impose a 3 month sobrietyrestriction(largelyunchangedsince2014).FloridaandWyomingremain,astheydidin2014,theonlytwostatesthatimposea1monthsobrietyrequirement.Fifteenjurisdictions(14statesandtheDistrictofColumbia)imposetheslightlylesspunitive–butstillobstructive–requirementofscreeningandcounseling.
Twenty-fivestatesdonotrequireindividualsmeetsobrietycriteriabeforeobtainingtreatment,with15of thosestates requiringscreeningandcounseling.Thus,53%of jurisdictions imposemandatedsobrietyperiodsonMedicaidpatients.
Remarkably,somestateshaveclungtosobrietyrestrictionsevenastheyhaveloosenedfibrosisrestrictions.NorthDakotarequirespatientstoabstainfromdrugsandalcoholforafullyear,butdoesnotrequirethemtoadvancetoaspecificstageofliverdamage.Fourjurisdictions(Maine,Mississippi,PuertoRico,andWisconsin)imposenofibrosisrestrictionsbutmaintaina6monthsobrietyrequirement.NeitherFloridanorWyomingimposefibrosisrestrictions,yetbothpersistinrequiring1monthofsobriety.
21Atthetimeofpublication,fourjurisdictionshaveannouncedplanstodroportoconsiderdroppingfibrosisrestrictionsbuthavenotdonesoyet:Missouri,NewMexico,NorthCarolina,andOhio.

Page 18
DespiteevidencethatinjectiondruguseisnowthecauseofmostnewreportedHCVinfections,22somestateswith thehighest ratesofopioidoverdoseandHCVblockpatients fromreceivingtreatmentbyimposingsobrietyrestrictions.BothKentuckyandTennesseerequireindividualstodemonstrate6monthsofsobrietybeforeaccessingtreatment.WestVirginiaimposesa3monthsobrietyrequirement.Incontrast,Indiana,whichsufferedanotoriousoutbreakofHCVandHIVin2015,treatspatientswithoutimposinganysobrietyrequirements.
AmpleresearchdisprovesthedangerouscontentionthatDAAtherapyislesseffectiveinpeoplewhousedrugsoralcohol.Arecentreviewofseveralstudiesexaminingtreatmentresponseinpeoplewhoinjectdrugsrevealedadherence,completion,andcureratescomparabletothoseinpeople who do not use drugs.23 In another analysis involving 17,487 patients starting DAAtherapy, researchers found no significant differences in cure rates between people whoabstainedfromalcoholandpeoplewhodrankalcohol.24TheAASLD/IDSAtreatmentguidelinespointtothehighadherenceratesandlowreinfectionratesamongpeoplewhoinjectdrugsinarguing that sobriety restrictions must be removed to combat the HCV epidemic mosteffectively.25
Policymakersinalljurisdictionsmustacknowledgethelackofmedicalandscientificevidencetosupport sobriety requirements. These discriminatory restrictionsmerelymanifest the stigmasurroundingalcoholanddruguse,whichcanoftendiscouragepeoplewhousedrugsoralcoholfrom seeking HCV testing and treatment. When states impose sobriety-based barriers totreatment,theynotonlymissanopportunitytocurbthespreadofHCV,theyalsoinstitutionalizeandperpetuatestigma.
Finally,theunfortunatetrendofsomejurisdictionsallowingMCOstoimplementmorerestrictivecriteriathantheirrespectiveFFSprogramappliestosobrietyrestrictionsaswell.TheMCOsin8states impose more restrictive sobriety requirements than their FFS counterparts. Thegovernments of all jurisdictions must act to ensure that MCOs and FFS programs employconsistentcriteria,asrequiredbylaw,intheiradministrationoftreatmenttoHCVpatients.
ClarifyingPrescriberLimits
Thetrendtowardtransparencyhasdispelledsomeconfusionaboutwhetherpatientsincertainstatesmustfirstvisitorconsultaspecialistbeforereceivingtreatment.In2014,23jurisdictions(22statesandPuertoRico)didnotpublish informationaboutprescriber limitations. In2017,prescriberrestrictionsarenowunknowninonlyonestate:NewJersey.
22Campbell,Canary,Smith,etal.,StateHCVIncidenceandPoliciesRelatedtoHCVPreventiveandTreatmentServicesforPersonsWhoInjectDrugs—UnitedStates,2015–2016,66MMWR1(2017).23GrebelyJ.,HajarizadehB.,andDoreG.,Direct-actingantiviralagentsforHCVinfectionaffectingpeoplewhoinjectdrugs,106NATREVGASTROENTEROLHEPATOL1(2017).24TsuiJ,WilliamsE,GreenP,BerryK,SuF,andIoannouG.,AlcoholuseandhepatitisCvirustreatmentoutcomesamongpatientsreceivingdirectantiviralagents,169DRUGALCOHOLDEPEND101(2016).25TheAmericanAssociationfortheStudyofLiverDiseasesandtheInfectiousDiseasesSocietyofAmerica,HCVGuidance:RecommendationsforTesting,Managing,andTreatingHepatitisC,Sep.21,2017,availableathttps://www.hcvguidelines.org/.

Page 19
Encouragingly,fewerjurisdictionsnowrequirepatientstovisitaspecialisttoreceivetreatment.Fourteenstatesimposenoprescriberrestrictionsin2017,whereasnostatemetthiscriteriain2014.In2014,15statesrequiredprescriptionsbyaspecialistonly.In2017,9statesrequireaspecialist to prescribe. However, as more jurisdictions are transparent about prescriberrestrictions, their barriers to treatment have emerged. While 14 jurisdictions requiredprescriptionsbyorinconsultationwithaspecialistin2014,28jurisdictions(26states,theDistrictofColumbia,andPuertoRico)nowimposethisrequirement.
Finally, justassomeMCOs imposemorerestrictive fibrosisandsobrietycriteria than theFFSprogramintheirstates,someimposemorerestrictiveprescriber limits.ElevenstatesandtheDistrictofColumbiacontractwithatleastoneMCOwithharsherprescriberrestrictionsthantheFFSprograminthosejurisdictions.SevenofthesestatesoverlapwiththoseoperatingMCOsthatimposemorerestrictivefibrosiscriteria.
CONCLUSION
InevaluatingMedicaidHCVtreatmentcriteriafrom2014to2017,afewkeytrendsemerge.Manystates continue to violate their treatment obligations under the law despite strong, clearguidancefromtheCentersforMedicareandMedicaidServicesthatcurrentrestrictionsviolatefederallaw.Additionally,therestrictionsinplacedirectlycontradictthestandardofcareoutlinedin the treatment guidelines established by the American Association for the Study of LiverDiseasesandtheInfectiousDiseasesSocietyofAmerica.
Despitethepersistenceoftoomanyrestrictions,significantprogresshasbeenmade:
• ManymorestateshavepubliclyavailableinformationregardingaccessrestrictionstoHCVtreatmentthanstatesdidin2014;
• Accessrestrictions,particularlyforliverdamage,havedecreasedsince2014;and
• WenowhavebaselineinformationonMCOrestrictionsfromwhichtoevaluatefuturetrends.
Wemustbuildontheprogressthathasbeenmadeinlesseningliverdamagerestrictionsandeliminate these restrictions nationwide. Similarly, wemust work to ensure that restrictionsbasedonsobrietyandprescriberspecialtyfollowsuit.ToaccomplishthisgoalandworktowardseliminatingHCV,wemustholdfederalandstateregulatorsaccountableforensuringthatpeoplelivingwithHCVhaveaccesstotreatmentconsistentwithestablishedtreatmentguidelinesandrelevantfederalandstatelaws.Mostimportantly,wemustensurethattheCentersforMedicareandMedicaidServices,aswellasotherfederalandstateregulators,monitorandenforceparitybetweenMedicaidFFSandMCOprograms.Ataminimum,regulatorsmustensurethatMCOs

Page 20
donotimposemorerestrictivetreatmentaccesscriteriathantheircorrespondingFFSprogram,asrequiredbylaw.
With the availability of live-saving cures for HCV, policymakers and advocatesmust push toeliminateunnecessary,discriminatory,andillegalbarrierstocare,andhelpensureallMedicaidbeneficiariescanaccessthecureforthisdeadlydisease.

Copyright © 2017





























