Embed Size (px)
Citation preview

HEPATITIS C: AN OVERVIEW FOR THE PRIMARY CARE PROVIDERELAINE ACCOMANDO PA-CNORTH COUNTRY HEALTHCARE
(WITH CONTRIBUTION FROM ANN MOORE, FNPAND DR. RICHARD MANCH MD/HEPATOLOGIST)
www.hcvguidelines.org, AASLD, IDSA

OVERVIEW
• Definition
• Prevalence & Demographics
• Screening
• Transmission
• Treatment

DEFINITION
• Hepatitis C: RNA positive virus causing acute and chronic hepatitis
• Family Flaviviridae, Genus Hepacivirus
• Related genus Flavivirus- Dengue, Yellow Fever
• In vivo replication: liver and lymphocytes

HCV PREVALENCE
200 million Chronic Infections Worldwide2% of worlds population75% of people unaware of status
~5 millions Americans infected with HCV- 45-85% are unaware they are infected

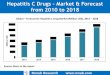
HEPATITIS C VIRUS GENOTYPES IN THE USA
All others1%
Type 310%
Type 217%
Type 172%
McHutchinson JG, et al. N Engl J Med. 1998;339:1485-1492.

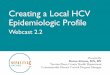
HCV PREVALENCE IN HIGH-RISK US POPULATIONS
•Weinbaum C, et al. MMWR Recomm Rep. 2003;52(RR-1):1-36. Edlin BR. Hepatology. 2002;36(5 suppl 1):210-219. National Survey on Drug Use & Health (NSDUH). NSDUH Report. 2003. Khalili MA, et al. Clin Inf Dis. 2000;31:154-161. LaBreque DR, et al. In: Hepatitic C Choices. 2002. Alter MJ, et al. N Engl J Med. 1999;341(8):556-562. Nyamathi AM, et al. J Gen Intern Med. 2002;17(2):134-143. Bräu N, et al. Am J Gastroenterol. 2002;97(8):2071-2078. Jonas MM. Hepatology. 2002;36(5 suppl 1):S173-S178.
•Homeless•~175,000 (22%)
•Alcoholics•~250,000 (11%-36%)
•IDUs•~300,000 (80%-90%)
•Incarcerated•~310,000 (15%)
•HIV Infected•~300,000 (30%)
•Veterans•~280,000 (8%)

HCV SCREENING AND TESTING RECOMMENDATIONS(CDC AND AASLD/IDSA)
• HCV testing is recommended at least once for persons born between 1945 and 1965
• Other persons should be screened for risk factors for HCV infection
• 1-time testing should be performed for all persons with behaviors, exposures, and conditions associated with an increased risk of HCV infection
• Annual HCV testing is recommended
• Persons who inject drugs
• HIV-positive MSMs who have unprotected sex
• Periodic testing should be offered to other persons with ongoing risk factors for exposure to HCV
Centers for Disease Control and Prevention. MMWR. 2012;61(RR-4):1-33.AASLD and IDSA. http://www.hcvguidelines.org/full-report-view. Version December 19, 2014.

TRANSMISSION• Percutaneous exposure with infected blood
• Contaminated devices shared for IV drug use
• Sexual transmission rare except in HIV infected anal unprotected MSM
• Recipients of blood products before 1992
• Vertical transmission from mother to baby rare ~1-2%
• Long-term hemodialysis
• Needle-stick injuries
• Unprofessional tattoos

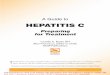
CHRONIC HCV INFECTION:DISEASE PROGRESSION
Poynard T, et al. Lancet. 1997;349:825-832.
Of every 100 persons infected with HCV, approximately• 15-25% of people infected with Hepatitis C virus will
naturally clear the virus and resolve the infection• 75% to 85% will develop chronic infection• 60% to 70% will develop chronic liver disease• 5% to 20% will develop cirrhosis in 20 to 30 years• 1% to 5% will die from the consequences of chronic
infection (liver cancer or cirrhosis)

COMORBIDITIES/EXTRAHEPATIC MANIFESTATIONS OF CHRONIC HCV INFECTION
• Arthralgia• Arthritis• Behcet’s disease• Canities• Cerebral vasculitis• Cryoglobulinemia• Diabetes• Fatigue• Fibromyalgia• Hypertrophic cardiomyopathy• Immune thrombocytopenic purpura• Insulin resistance• Lichen myxoedematosus and planus• Lung abnormalities• Membranoproliferative glomerulonephritis• Membrane nephropathy• Mooren corneal ulceration
• Multiple myeloma
• Neutropenia
• Non-Hodgkin’s lymphoma
• Paresthesia
• Porphyria cutanea tarda
• Pruritus
• Raynaud’s syndrome
• Sialadenitis
• Sjogren’s syndrome
• Spider nevi
• Systemic lupus erthematosus
• Thrombocytopenia
• Thyroid disease
• Vasculitis
• Vitiligo
• Waldenstrom macroglobulinemia

RISK FACTORS FORPROGRESSIVE FIBROSIS AND CIRRHOSIS
• Persistently elevated ALT levels
• Longer duration of infection
• Alcohol excess (>50 g/day)
• Age >40 years at time of infection
• HIV or HBV coinfection
• High BMI
• Male gender
Poynard T, et al. Lancet. 1997;349:825-832.Kim WR, et al. Gastroenterology. 2004;127:749-755.

DIAGNOSIS
• Screening for past or present HCV infection
• Hepatitis C antibody by enzyme immunoassay (EIA)
• Sensitive and inexpensive
• Confirmation of positive EIA
• PCR for HCV RNA quantitative
• Medical evaluation and management

HCV ASSAYS:WHAT THE RESULTS MEAN
AASLD and IDSA. http://www.hcvguidelines.org/full-report-view. Version December 19, 2014.
Anti-HCV
HCV RNA Interpretation
+ + Acute or chronic HCV depending on the clinical context
+ False positive HCV antibodyResolved infectionLow-level intermittent viremia
+ Early acute HCV infectionChronic HCV in setting of immunosuppressed stateFalse positive HCV RNA test
Absence of HCV infection

COUNSELING HCV-INFECTED PATIENTS:AVOIDING TRANSMITTING HCV TO OTHERS
• Items to avoid
• Sharing toothbrushes and dental or shaving equipment
• Using illicit drugs• Those who continue to inject drugs, avoid reusing or sharing syringes, needles, water, cotton
or other paraphernalia. Clean the injection site with a new alcohol swab and dispose of syringes and needles after one use in a safe, puncture-proof container
• Bandage bleeding wounds to prevent contact with others
• Do not donate blood, body organs, other tissue or semen
• Safe, sexual practices
• Encourage barrier protection for HIV-positive MSMs and those with multiple sexual partners or STIs
• For others with HCV infection, the risk of sexual transmission of HCV is low

INITIAL LABWORK AFTER CONFIRMATION OF HCV INFECTION

IMPORTANT POINTS ABOUT CURRENT HCV TREATMENT
• Most patients can be cured with 8-12 weeks of all oral therapy.
• >90% cure rates
• Cost of medications is high• Many restrictions by insurers on types of patients that can be
treated – but are improving!
• Most insurers require consultation with hepatologist, ID specialist, or GI
www.hcvguidelines.org

• Center for Disease Control (CDC) and Prevention Public Health Fund 2012, Viral Hepatitis, Early Identification and Linkage to Care for Chronic HCV (hepatitis C virus) Infections.
• The purpose of this initiative is to enhance linkage to care and treatment for people living with HCV.
• This initiative has enabled the University of Utah and St. Joseph’s Hospital in Arizona to work closely with the HCV Project ECHO team at UNMHSC to become regional hubs for training primary care clinicians in HCV treatment protocols, using the ECHO model™.
• This new and innovative program aligns directly with the CDC’s desire to work with academic and clinical partners, as well as other federal and state agencies, to replicate best practices and develop new models for HCV care.
• (North Country HealthCare participates in the Echo Program since 2012)

DIRECTLY ACTING ANTIVIRALS
• Combination medications
• Some with protease inhibitors
• Others with NS3-4-5 inhibitors
• Newer medications within the last 1-2 years treat all 6 genotypes – thus simplifying treatment regimens
• The sustained viral response (SVR) rates/cure rates are ~90-100%

CHILD-PUGH SCORE TO DETERMINE SEVERITY OF CIRRHOSIS (PRIOR TO TREATMENT)

TREATMENT: GENOTYPE 1A/1B WITHOUT CIRRHOSIS

TREATMENT: 1A WITH CIRRHOSIS

TREATMENT: 1B WITH CIRRHOSIS

TREATMENT: 2 WITHOUT CIRRHOSIS

TREATMENT: 2 WITH CIRRHOSIS

TREATMENT: 3 WITHOUT CIRRHOSIS

TREATMENT: 3 WITH CIRRHOSIS

TREATMENT: 4 WITH/WITHOUT CIRRHOSIS

DRUG TO DRUG INTERACTIONS (ABBREVIATED)

MONITORING DURING TREATMENT
• Once treatment approved, patients undergo compliance counseling – very important!
• Viral load PCR quantitative:• 2 weeks and 4 weeks into treatment
• End of treatment
• 1 month, 3 month, and 6 months after resolution
• GOAL: SVR = the continued absence of detectable HCV RNA for at least 12 weeks after completion of therapy

WHO WILL NEED SPECIALTY CARE?
• HIV/HCV Coinfection
• Decompensated Cirrhosis
• Organ Transplant patients
• Comorbidities like HBV, Autoimmune hepatitis, HIV/HBV/HCV
• Renal Failure Patients
• Hepatocellular Carcinoma
• Multiple Failures of HCV Therapy

CONCLUSIONS
• Treatment for hepatitis C has evolved rapidly in the past 3 years to simple, all oral regimens with high cure rates
• Increased screening and linkage to care is required as most patients with hepatitis C do not know they are infected
• Political and social activism is required to improve patient access to drugs
• Possibilities ahead for global eradication/elimination, with pilot projects being done

THE NORTH COUNTRY EXPERIENCE
• Personal experience treating Hep C since 2012
• One of the most rewarding parts of practice
• First 3 patients: 2 weeks after initial treatment, viral loads were all undetectable