Embed Size (px)
Citation preview

I 86 BRIT. J. SURG., 1964, Vol. 51, No. 3, MARCH
The ends of these sutures are threaded through a metal ring with a handle at right angles (Fi,y. 4), and, by opening up the end of the Roux loop., applying traction to the stay sutures, and pressing back the folds of jejunal mucosa with the metal ring, the end of the bile-duct presenting within the jejunal incision is drawn into view.
Anastomosis in one layer is to be constructed with a series of transverse mattress sutures of fine catgut, each inserted as shown in Fig. 5.
The number of sutures depends upon the size of the bile-duct and will usually be between six and ten (Fig. 6).
With the intrajejunal anastomosis completed, the open end of the Roux loop is closed and the loop itself suspended from the peritoneum or the capsule of the liver so that there is no tension on the anasto- mosis (Fig. 7).
The abdomen is now closed, with drainage.
RESULTS Four patients have been operated upon in this way
for stricture of the common hepatic duct. In a number of others the method proved technically impossible on account of obesity or shortness of the hepatic duct available, and anastomosis working outside the jejunum was employed. The postoperative course in the 4 patients with an intrajejunal anastomosis was
exceptionally smooth. In all cases discharge of bile was nil and the patients left hospital on the tenth, tenth, twelfth, and fourteenth postoperative day respectively. So far the patients remain well, 25, 23, 18, and g months after operation.
It must be stressed that the method described is merely one way of making sure that the important principles of biliary-intestinal anastomosis are ob- served. Other surgeons may well achieve the same result using a totally different technique. I t is the principles that matter and these are worth restating: the widest possible stoma; duct lining to mucosa all round; no tension.
SUMMARY The complications of hepaticojejunostomy or
choledochojejunostomy usually result from a stenosed anastomosis. The principles of technique which minimize the chances of stenosis are described. If the bile-duct available for anastomosis is long enough, intrajejunal anastomosis is one method of ensuring that these principles are observed. The technique is described and reference made to a short follow-up of 4 cases.
Acknowledgement.-It is a pleasure to thank Mr. R. N. Lane, medical artist, for the preparation of the illustrations.
HEPATICOJEJUNOSTOMY WITH TRANSHEPATIC INTUBATION A TECHNIQUE FOR VERY HIGHISTRICTURES OF THE HEPATIC DUCTS
BY RODNEY SMITH ST. GEORGE’S HOSPITAL
INTRODUCTION injury is best treated by hepaticojejunostomy. As A STRICTURE of the common, right, or left hepatic duct suggested elsewhere (Smith, 1964) the essentials for presents a particularly difficult technical. surgical success are : (a) The largest possible stoma; (b) Accurate problem. The underlying pathology may be neo- apposition of the hepatic duct lining to the jejunal plastic, inflammatory, or traumatic, and of these, mucosa without any gaps; (c) No tension. regrettably, the traumatic is the most common. the The trouble is. of course. that cases are encountered trauma b&ng accidental damage during the operation of cholecystectomy. A patient with an injury to a hepatic duct really high up in the porta hepatis has, from the start, a lesion which is very difficult to repair and which will in the end kill him if it is not: repaired.
Repair is imperative, and yet whatever routine technique is selected the failure-rate is high. A failed repair leads to more fibrosis and a little less of the hepatic duct to use for the anastomosis ai. the next attempted repair; therefore a higher fail rate at the second attempt, and so on.
Before proceeding further, it will be very obvious that any surgeon would do well to keep before him these two guiding principles :-
I. These injuries are so difficult to treat that they simply must not be allowed to occur.
2. If, unfortunately, a duct is damaged, every con- ceivable effort must be made when repairing it to get it right first time.
Although end-to-end duct anastomosis has its advocates in some circumstances, a very high duct
where these essentials are herally quite impossible to observe. It is not too uncommon for a patient to be referred who, having sustained a high duct injury, has narrowly survived a stormy series of complications with bile leakage and subphrenic sepsis leading to massive scarring in the porta hepatis, and has then undergone several unsuccessful attempts at repair of the resulting high stricture, each time with failure due to re-stenosis. Consider for a moment what can be done for a patient of this kind, becoming jaundiced again, with chronic cholangitis and acute exacerbations and early biliary cirrhosis. If yet another operation is undertaken, dissection in the porta hepatis reveals massive fibrosis in which the surgeon may search for a long time before finding any trace of a bile-passage. When eventually a trickle of bile leads him in the right direction he may easily arrive at a point where all that can be demonstrated with certainty is what appears to be a rigid scarred orifice into the liver (Fig. I). The opening can be enlarged with dilators and the usual mixture of biliary mud and small

stones evacuated with scoops and by washing out. The object now must be to core out of the liver enough of the duct to construct a successful anasto- mosis; but this may well be not only difficult and hazardous, on account of danger to the blood-vessels in the porta hepatis, but even quite impossible. For when what appears to be a few millimetres of rigid ‘duct’ has been dug out, this may in fact be a short cylinder of scar tissue without a true epithelial lining, and if this is used for anastomosis re-stenosis is certain.
The situation of a patient of this kind can be a truly desperate one. There is no alternative to re-operation, for without it increasing cholangitis, deepening jaundice, and finally an irreversible biliary cirrhosis will lead to the death of the patient. On the other hand, the surgeon may very well say to himself, ‘How can I advise another operation when all I can do is to repeat the procedure which has already failed, this time with more pathology, less duct, and thus an even smaller chance of success ?’
Various techniques have been described in the past for coping with the type of pathology described. First, the surgeon may give up all attempts to con- struct a hepaticojejunal anastornosis with apposition of duct lining to jejunal mucosa and, instead, sew the open end of the jejunal Roux loop to the capsule of the liver around the scarred orifice into the duct system. The failure-rate of this operation is IOO per cent.
Secondly, the best anastomosis that is technically possible can be constructed and splinted by an
indwelling tube of latex rubber or polythene. The lower end is brought out through a small incision in the Roux loop some 6 in. distal to the anastomosis. The upper extends into the right or left hepatic duct or into both (Y-tube) (Fig. 2). Alternatively a
SMITH: HEPATICOJEJUNOSTOMY 187
FIG. 2.-High division of hepatic duct can be treated by hepaticojejunostomy over an indwelling Y-tube. A, The divided duct; 6, The technique employed.
FIG. I.-Very high division of common hepatic duct. Opera- tion reveals what appears to be merely a rigid scarred orifice into the liver.
A 6

I88 BRIT. J. SURG., 1964, Vol. 51, No. 3, MARCH
FIG. 3.-Hepaticojejunostomy splinted by a long T-tube.
FIG. ~.-Longmire’s operation. Anastomosis of the distal cut end of the left hepatic duct to a jejunal Roux loop.
FIG. 4.-End-to-end anastomosis of divided duct will join without a stricture if splinted with a T-tube for long enough.
T-tube may be used (Fig. 3). This is better, for Cattell and Braasch (1958a, b) and Maingot (1959) have shown that an end-to-end duct anastomosis, if pro- tected from contraction of scar tissue by an indwelling T-tube (Fig. 4), will remain patent after the tube has been removed. The tube must be left in, however, for a minimum of 3-6 months, and 12 months is often better. If the hepaticojejunal anastomosis is similarly splinted and protected, contraction can probably be prevented. Unfortunately the Roux loop will not usually allow the tube to stay in long enough. Even if a long-limbed Y-tube is employed (Fig. 2), it is ‘milked’ out of the ducts by peristalsis and, although the patient remains well while the tube is in place, a sudden return of symptoms, often 3 or 4 months after operation, leads to radiography which shows the tube to be lying free in the Roux loop.
Thirdly, the surgeon may give up all hope of employing any of the main hepatic ducts for anastomo- sis and, avoiding the porta hepatis, amputate part of the left lobe of the liver and try to construct an anastomosis between the distal cut end of the left hepatic duct and the jejunum (Longmire’s operation) (Fig. 5 ) . In practice, although a few patients have done well for a while after this procedure, re-stenosis is the rule and the failure-rate is very high indeed.
Basis of the Technique to be Described.- Anastomosis of the scarred, fibrotic, common hepatic duct to a Roux loop of jejunum is technically possible, but without the accurate apposition of duct-lining to jejunal mucosa which is essential for success. Part

SMITH : HEPATICOJEJUNOSTOMY
of the anastomosis has no true lining, and as the is dilated up and dissected out of the liver as effectively scar tissue at this point contracts stenosis will occur. as possible. The intrahepatic ducts are cleared of This must be prevented by an indwelling tube and small stones and biliary mud and bile taken for the tube must be inserted in such a way that it cannot culture. The duct system is washed out. be milked out of the duct system by the peristalsis of the jejunal Roux loop. A solution is to employ a transhepatic tube, splinting the anastomosis and extending up into the common hepatic duct, the left hepatic duct and, via a main subdivision of this,
FIG. 6.-An_eled gall-stone forceps used for inserting trans- hepatic tube.
FIG. S.-GaIl-stone forceps passed via rhe lefr hepatic duct to the surface of the liver.
to the anterior surface of the liver, and through this and the abdominal parietes to the exterior. This tube is easily anchored and will stay in place until it is removed by the surgeon.
OPERATIVE TECHNQIUE Exploration of the abdomen and dissection in the
porta hepatis bring to light the high ductal injury under discussion. The scarred common hepatic duct
FIG. 7.-Branches of the left hepatic duct approach the surface of the liver at points A and B.
FIG. 9.-Larex tube grasped and drawn through the left hepatic duct down through the divided common hepatic ducr.
An angled gall-stone forceps (Fig. 6 ) is now intro- duced into the common hepatic duct and thence into the left hepatic duct. With a little manipulation the instrument can be easily introduced into one of two main subdivisions running close to the anterior surface of the liver. One of these ductal branches lies in the quadrate lobe (part of the left half of the liver), and if introduced into this the end of the forceps can be felt just to the right of the falciform ligament

I90 BRIT. J. SUIIG., 1964, Vol. 51, No. 3, MARCH
(Fig. 7, A).. The other anteriorly placed duct is in the lobus sinister proper, and if the forceps is intro- duced into this the end is felt to the left of the falci- form ligament (Fig. 7 , B). Blunt dissection down to
the duct and a small incision into the duct itself allow the end of the forceps to protrude from the liver (Fig. 8). The largest possible tube of latex or nylon is grasped and the forceps withdrawn, bringing
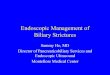
FIG. 10.-Photographs at operation of a transhepatic tube inserted.
FIG. i~.--Roux loop constructed and attached to the liver below the divided hepatic duct.
FIG. 12.-Hepaticojejunostomy over the transhepatic tube.
the end of the tube down through the duct system and out of the open common hepatic duct (Figs. 9,
A Roux loop some 8-10 in. in length is constructed and brought up to the porta hepatis. The end of the loop is closed and an opening in its anterior surface made the same size as the open end of the common hepatic duct (Fig. I I). Hepaticojejunal anastomosis is performed, using interrupted sutures of fine cat- gut on an eyeless needle. When half the anastomosis has been constructed the tube is inserted into the jejunal loop and the anastomosis is then completed (Figs. 12, 13). About 4in. of tube should project from the anastomosis into the jejunum. Above this
10).

SMITH: HEPATIC0 JEJUNOSTOMY 191
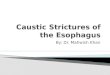
FIG. 13.--The completed anastomosis with tube in situ. FIG. 14.-Postoperative attachment of suction to the trans- hepatic tube is employed.
level there should be a number of lateral holes in the intrahepatic portion of the tube. The length of tube issuing from the anterior surface of the liver is fed through a separate stab incision in the anterior abdominal wall, and the abdomen is closed, with drainage of the subhepatic space.
Postoperative Management.-The transhepatic tube is connected to a low-tension electric pump and continuous suction applied. This diverts bile from the anastomosis and thus prevents leakage during the phase of healing. During the first 24-48 hours after operation, the bile draining is often very dirty and contains biliary mud and debris, even if the bile- passages have been thoroughly washed out at opera- tion. The subhepatic drain may be of corrugated rubber, or closed drainage with a rubber tube attached to a vacuum bottle may be used (Fig. 14).
Suction applied to the transhepatic tube is con- tinued for from 4 to 5 days and then stopped, and the tube allowed to drain into a bottle. If this results in bile appearing from the subhepatic drain, suction is restarted and continued for a further 2 days. If not, the tube is allowed to drain freely into a bottle until the tenth postoperative day. A check cholangiogram is now used to show that there is no leakage from the anastomosis, and assuming that the result is satis- factory the tube is spigoted off during the day, allowed to drain into a bottle during the night, and washed out with sterile water once daily. The patient is shown how to sterilize water by boiling and carry out the irrigation of the tube so that this is continued at home after discharge from hospital on about the fourteenth postoperative day.
FIG. 15.-If the duct injury is above the junction of right and left hepatic ducts two tubes can be employed, one through each main hepatic duct.

192 BRIT. J. SUF:G., 1964, Vol. 51, NO. 3, MARCH
Variations in Technique.- I. Occasionally the ductal injury is so high in the
porta hepatis that no common hepatic duct is left and
the right and left hepatic ducts have to be anastomosed individually to the jejunum. In the past, indwelling tubes brought out through the jejunum have been
A 0
FIG. 16.-A stenosed hepaticojejunal anastomosis does not necessarily have to be undone. An opening can be made into the jejunal loop as shown (A). Dilatation of a strictured hepatico- jejunal anastomosis can be carried out through the jejunal opening made (8). T h e hepatic tube can now be drawn down in the same way as before and the small opening in the jejunum closed with two or three fine catgut sutures (C).
used, but these will not usually stay in long enough to prevent stenosis. Bilateral transhepatic tubes can be employed (Fig. I 5).
2. In Oriental cholangiohepatitis, a disease common in South-East Asia, particularly in Hong Kong and on the Chinese mainland, gross suppuration and stone formation throughout the enormously dilated bile- passages pose a difficult problem. Washing out at operation and drainage of the common bile-duct after operation solve the problem temporarily, but the recurrence rate is high. It would appear that the technique of bilateral transheptic intubation might well allow prolonged drainage and irrigation to be used with improved results.
3. Considering again the patient with a high traumatic stricture, if there have been a number of repairs and the patient comes to surgery with a Roux loop already in the porta hepatis and a stenosed hepaticojejunal anastomosis, it does not follow that the anastomosis must be undone and refashioned. A small incision in the Roux loop itself, 1-2 cm. from the stenosed anastomosis (Fig. 16 A), allows Bakes dilators to be inserted and the stoma to be dilated up to a calibre of 6-7mm. (Fig. 16 B). Still working

SMITH : HEPATIC0 JE JUNOSTOMY I93
through the incision in the jejunum, the angled gall- stone forceps is introduced and a transhepatic tube drawn through the liver so that it lies as already described. T h e incision in the jejunum is now easily closed (Fig. 16 C).
Summary of Arguments in Favour of a Technique of this Kind.-
I . Without some such procedure, in this particular group of cases satisfactory bile drainage cannot be secured by operation; yet if drainage is not secured the patient will develop biliary cirrhosis and eventu- ally die of this.
2. Particularly i n those cases in which a small incision i n the jejunum allows the stenosed anasto- mosis to be dilated, the technique is swift, simple, and safe and does not compare in hazard with the alterna- tive of taking down the anastomosis, coring the duct out of the liver, and constructing a new anastomosis.
3. Postoperative suction allows leakage and pooling of infected bile around theanastomosis to be prevented.
4. T h e indwelling tube allows irrigation with sterile water to keep the bile-passages clear of debris, or with antibiotics if there has been severe cholangitis, the organism responsible being identified by culture of the bile withdrawn by suction.
5. Stenosis cannot occur while the tube is in situ. The length of time it should be left in is probably about the same as that for a T-tube splinting an end- to-end anastomosis, that is, a minimum of 3-6 months and in some cases u p to 12 months.
Possible Disadvantages.- I. It might prove difficult to introduce the trans-
hepatic tube. This has so far not proved to be the case.
2. T h e tube itself may become a route of infection into the bile-passages. This is clearly a theoretical risk, but it would seem a risk that should be accepted in preference to the certainty of cholangitis if lack of bile drainage continues.
3. Re-stenosis may occur after the tube is removed. Only a long-term trial can give the answer to this. In any event it cannot logically be argued that to allow biliary obstruction to continue is better than to relieve it by a method which may later be followed by recurrence. There seems no particular reason why intubation a second time should not be performed if re-stenosis should prove to be a hazard, and certainly patients with indwelling tubes appear to be physically so well, compared with their preoperative state, that it is justifiable to argue that a fit patient with a n indwelling tube for a n indefinite period is preferable to one with no tube but with chronic biliary obstruc- tion, cholangitis, and developing cirrhosis.
CASE REPORTS Case 1.-Mrs. G. Y., a Spanish lady of 45 years, had
been operated upon 2 years previously for a hydatid cyst of the liver adjacent to the porta hepatis. Surgery had proved difficult and there had been a good deal of con- tamination in the area of the common hepatic duct with blood, bile, hydatid cyst contents, and formalin. A stormy convalescence, complicated by bile leakage and local sepsis, had followed, but the patient eventually left hospital symptom-free. Within 2 months, however, attacks of cholangitis and a fluctuating obstructive jaundice had begun, and they eventually led to a diagnosii of stricture of !he common hepatic duct. The case was referred to the writer. After preparation with blood transfusion for a
I3
marked anaemia, antibiotics, and vitamin K, the abdomen was explored.
OPERATION 1.-The porta hepatis was obscured by a mass of rigid scar tissue, and with much difficulty a dilated common hepatic duct was entered. Many small stones were scooped out and much debris and frankly purulent bile washed out. Bile was taken for culture. The general state of the patient, whose cholangitis was inadequately controlled by antibiotics, led to a decision not to proceed with a major reconstruction at this stage, and T-tube drainage was instituted as a first-stage procedure. Steady improvement followed and reoperation was undertaken.
OPERATION 2.-Dissection in the porta hepatis showed that scarring and fibrosis of the common hepatic duct extended as high as dissection could be carried. The duct was divided and a length of some 2-3mm. of common hepatic duct finally dissected free sufficiently to perform an anastomosis. This length of duct was, however, not only short but rigid and fibrotic, and lined with granulation tissue. A Roux loop of jejunum was constructed, brought up to the porta hepatis, and hepaticojejunosromy per- formed using a single layer of catgut sutures. The chances of stenosis were, however, considered to be high and the anastomosis was splinted with an indwelling Y-tube of latex rubber, the upper limbs being long and extending well into the right and left hepatic ducts, the lower limb being brought out through the side of the Roux loop and the parietes (Fig. 2 B).
After this operation the patient’s jaundice cleared and she remained well, without jaundice or evidence of cholangitis, for 4 months. She then complained, at follow- up, of renewed attacks of fever and malaise, and injection of hypaque through the Y-tube showed that this now lay free in the jejunum. Clinical and biochemical evidence soon suggested stenosis of the anastomosis and she was readmitted for transhepatic intubation.
OPERATION 3.-The hepaticojejunal anastomosis was found to be severely stenosed with, once more, biliary mud and debris in the hepatic ducts above. A new anasto- mosis was constructed, this time splinted with a trans- hepatic tube inserted in the manner described and emerging from the liver through a branch of the left hepatic duct to the left of the falciform ligament. Post- operative management has been described.
PROGRESS-The patient is in excellent health I year after operation. Improvement after transhepatic intubation was dramatic and she promptly got married, reporting from her honeymoon in Spain that the tube was no inconvenience and that she swam daily. The tube was removed after 8 months.
Case 2.-Mrs. S . , aged 29 years, developed a chronic enteritis due to Salmonella cholerae suis and for this had been treated by cholecystectomy. Damage to the common hepatic duct had occurred, and when admitted to hospital she was jaundiced and running a high fluctuating fever.
OPERATION I .-After intensive preparation with anti- biotics, laparotomy revealed an injury to the common hepatic duct high in the porta hepatis. In retrospect it would probably have been better to have drained the duct system at this stage as the f i s t of a two-stage procedure. However, a standard hepaticojejunostomy was performed, using a jejunal Roux loop. This was followed by gross subhepatic, subphrenic, and intrapleural sepsis, and many operations to drain local collections of pus. Bile leakage, however, did not recur and the patient remained free from jaundice through the early months of this stormy conva- lescence. Eventually she left hospital 8 months after her operation, by this time afebrile, not jaundiced, and free from symptoms. There was, however, even at this time, suspicion that all might not be well with the anastomosis, for there had been towards the end of her stay a transient jaundice lasting a few days on several occasions.
After discharge from hospital she was never really well; recurring mild jaundice and febrile episodes suggested stenosis of the anastomosis with cholangitis, and the liver

I94 BRIT. J. SUIIG., 1964, Vol. 51, No. 3, MARCH
became enlarged, firm, and tender. The spleen was palpable. She was admitted for reoperation and trans- hepatic intubation.
OPERATION L-AS expected, a mass of dense scar tissue concealed a stenosed anastomosis. This was refashioned after washing out the dilated hepatic ducts and a trans- hepatic tube inserted, the details being as already described. Liver biopsy was performed.
PROGRESS.-The smooth postoperative course and rapid improvement in health of this patient have been quite startling. Jaundice has cleared rapidly, she is afebrile, and feels well for the first time since her cholecystectomy. The tube is no worry to her and she washes this out herself once daily.
Case 3.-J. H., a naval officer aged 48 yeaxs, had been investigated and found to have gall-stones. He was advised not to have an operation on the grounds of his large size and the mild nature of his symptoms. As luck would have it, having accepted this advice, he was overtaken by an attack of cholecystitis while far from home and this was treated by cholecystectomy. Postoperatively profuse bile discharge and severe subphrenic suppuration led to a highly critical situation and his life was saved by Professor Arthur Mackey, in Glasgow, who drained several collections of pus and eventually performed a hepaticojejunostomy for a severed common hepatic duct. The odds were loaded against this operation, and stenosis 6 months later led to jaundice and increasing cholangitis.
OPERATION I .-Laparotomy revealed a grossly stenosed hepaticojejunal anastomosis. This was undone and many small stones and much biliary mud were recovered from the dilated hepatic ducts. A wide, good-looking re-anastomosis was secured and this was splinted by an indwelling tube brought out through the side of the jejunal loop. This slipped out after 4 weeks, but there had been no leakage of bile around the anastomosis, convalescence had been smooth and free from infection, and re-stenosis appeared to be unlikely. However, 4 months after leaving hospital minor febrile episodes began to occur, lasting for I day only. These began to occur more frequently and last longer. Eventually minimal jaundice appeared again and the liver was palpable and tender. A diagnosis of re-stenosis was made and the patient readmitted for transhepatic intubation.
OPERATION 2.-A stenosed hepaticojejunal anastomosis was found. This was undone, the hepatic ducts washed out, and a new anastomosis constructed over a transhepatic tube inserted as described.
PRocREss.-Convalescence was uneventful and the patient left hospital on the fourteenth postoperative day. He remains not jaundiced, afebrile, and without symptoms.
Case 4.-Mrs. P., aged 29 years, was reoperated upon after the following series of operations:-
I. Cholecystectomy-damaged common hepatic duct. 2. End-to-end ductal anastomosis over T-tube. 3. Drainage of subphrenic abscess. 4. Dilatation of strictured duct. Reinsertion of T-tube. 5. Division of duct at level of stricture. Hepatico-
6 . Refashioning of anastomosis with Roux loop. 7. Resection of stenosed anastomosis : new hepatico-
jejunostomy, end-to-side with entero-anastomosis.
jejunostomy constructed.
8. Re-stenosed anastomosis excised. Duct cored out of the liver. Hepaticojejunostomy performed over a long- limb Y-tube, extending well into hepatic ducts with lower limb emerging from the Roux loop.
The patient was well while this tube stayed in. After z months, however, it slipped into the jejunum and re- stenosis occurred.
OPERATION.-The jejunal Roux loop was opened I cm. from the anastomosis. Dilatation and washing out the ducts were easily performed. A transhepatic tube via the left lobe of the liver was introduced. The small jejunal incision was closed. Liver biopsy was performed. Apart from opening and closing the abdomen the whole procedure took 15 minutes.
I t is reasonable to emphasize that the procedure appears to be remarkably simple and free from hazard. The same cannot be said of any alternative operation when a recurrent stricture lies at this high level.
SUMMARY T h e very high hepatic duct stricture may present
an almost insoluble problem. Hepaticojejunostomy, using a jejunal Roux loop, is probably the best opera- tion, but the principles essential for success are often not attainable. Re-stenosis is thus common. Pro- longed splintage with an indwelling tube would probably prevent stenosis if the tube could be kept in long enough. Placed in from below, even a long- limb Y-tube is within a few months milked out of the hepatic ducts by jejunal peristalsis, and when this happens re-stenosis is likely to occur.
A method of transhepatic intubation is described. T h e tube, emerging from the anterior surface of the liver, will remain until the surgeon decides it is safe to remove it. T h e tube also allows diversion of bile from the anastomosis by suction in the immediate postoperative period, and daily washing out of the ducts while it is in place to keep it clear of biliary mud.
Since this paper was accepted for publication the writer has operated upon 6 other patients with high hepatic duct strictures employing this technique. In addition, Mr. Alan Hunt, of St. Bartholomew’s Hospital, has employed the technique on two occasions and Professor Louw, of Cape Town, on one.
Acknowledgements.-It is a pleasure to acknow- ledge the help given by Mr. R. N. Lane, medical artist, and Miss S. Fry, medical photographer, in the preparation of these illustrations.
REFERENCES CATTELL, R. B., and BRAASCH, J. W. (1958a), Surg. Clin.
_ _ _ - (1958b), Lahey Clin. Bull., 10, 94. MAINGOT, R. (I959), Ann. R. Coll. Surg. Engl., 24, 186. SMITH, RODNEY (1964), Brir. J . Surg., 51, 183.
N. Amer., 38, 645.