Embed Size (px)
Citation preview

Page 1Global Scientific Research Journal of Surgery
Hepatic Endometriosis: Systematic Review of Literature AND A Case Report
Hepatic Endometriosis: Systematic Review of Literature AND A Case Report
Laura Mastrangelo1*, Michele Masetti1, Maria Grazia De Blasiis1, Paolo Emilio Orlandi2, Angela Salerno3, Dario de Biase4, Sirio Fiorino5 and Elio Jovine1
1Department of Surgery, Maggiore Hospital, Bologna, Italy.2Department of Radiology, Maggiore Hospital, Bologna, Italy.
3Department of Anatomic Pathology, Maggiore Hospital, Bologna, Italy.4Department of Pharmacy and Biotechnology (FaBit), University of Bologna, Bologna, Italy.
5Department of Medicine, Maggiore Hospital, Bologna, Italy.
AbstractIntroduction: Endometriosis represents a very frequent condition in human pathology, in its predominant pelvic localization, however unusual sites may be affected, including liver. Hepatic Endometriosis (HE) is a diagnostic challenge, depending on the absence of specific clinical-, laboratoristic-and radiological patterns. These reasons make it difficult to diagnose this disorder preoperatively. Since a case of liver endometriosis was taken to our attention, we had the aim to review the available literature, to synthesize current knowledge on this topic and the case history of patients, described up to now.
Methods: A systematic computer-based search of published articles, according to the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) Statement was performed, and the following MESH (Medical Subject Headings) terms and keywords were used: ‘hepatic and liver endometriosis’, ‘hepatic and liver endometrioma’.
Review: We carried out a systematic search. We found 800 citations and 766 were excluded after a preliminary review of the titles and/or abstracts. Therefore, we examined the remaining 34 articles and reviewed the patients’ characteristics, described in these papers. Forty-one patients with HE (age ranging from 21 to 73 years) were included. Some of these subjects had a lesion with a diameter of more than 10 centimeters (cm). Five women presented areas of malignant transformation, arising in HE. We also described an illustrative case report.
Conclusion: HE should be included in the differential diagnosis for a woman of any age presenting with hepatic cystic or solid lesions of unknown cause, with or without a history of pelvic endometriosis.
Keywords: Endometriosis, Liver, Diagnosis, review
www.gsrjournals.com
Research Article Open Access
SurgeryVolume 1 - Issue 1 - 13 pages
IntroductionInitially described by von Rokitansky in 1860, en-dometriosis is defined as the presence of endome-trial glands and stroma outside the uterine cavity [1]. These ectopic endometrial implants are most com-monly found in the pelvis, including the ovaries, pelvic peritoneum, uterosacral ligaments, anterior and poste-
rior cul-de-sac, uterus, and fallopian tubes [2, 3]. How-ever, endometriosis can be found nearly anywhere in the body. Less common sites of involvement include the cervix, bladder, bowel, and pleural and pericardial cavities [4-10].
This case report describes a patient who initially un-derwent work up for a suspected spontaneous bleed-

Page 2Global Scientific Research Journal of Surgery
Hepatic Endometriosis: Systematic Review of Literature AND A Case Report
ing or rupture of liver hemangiomas which was discov-ered to be hepatic endometriosis by frozen section. In addition, a review of current literature was performed, summarizing radiographic and clinical findings asso-ciated with liver endometriosis [6, 9-11] and on the pathogenesis of this pathological condition [12-14].
Literature ReviewA systematic computer-based search of published articles, according to the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) Statement, issued in 2009 [15], was conducted through Ovid interface, in order to identify relevant studies on the hepatic endometriosis. The literature review was performed in March 2018. The following electronic da-tabases were used: MEDLINE (1950 to March 2018) and the Cochrane Library (until the fourth quarter of 2017) for all relevant articles. The search strategy and the search terms were developed with the sup-port of a professional research librarian. The search text words were identified by means of a controlled vocabulary, such as the National Library of Medicine’s MESH (Medical Subject Headings) and Keywords. The used MESH terms and keywords were: ‘hepatic and liver endometriosis’, ‘hepatic and liver endome-trioma’. The inclusion criteria for our search were: 1) study designs by considering data from all published
case series, case-control-, or case reports, as well as cohort-studies; 2) articles which were reported in Eng-lish, as peer-reviewed, full-text publications. Papers published in a language other than English were ex-cluded. The PubMed ‘related articles’ features and the reference lists of retrieved articles were also searched to find additional pertinent studies. Two authors (A.S. and S.F.), independently and in parallel, performed the literature search and screened relevant articles, based on title or abstract. The accuracy of data col-lection was checked by a third reviewer P.O. and disa-greements concerning the results were settled by con-sensus between all authors. If a study was considered potentially eligible by either of the two reviewers, the full-text of this study was further evaluated. Full-text assessment was performed according to eligibility cri-teria developed to systematically include studies into this review. Our search identified 800 citations and 763 were excluded after a preliminary review of the titles and/or abstracts. Further three reports were not considered, since they were published in a language other than English. The full-text of the remaining 34 articles was retrieved for a more detailed assessment.
A flow-chart of the study search and selection pro-cess, evaluating publications on liver endometriosis available in literature, is reported in Table 1.
Table 1: Flow-Chart of the Study Search and Selection Process, Evaluating Publications on Liver Endo-metriosis Available in Literature
Hepatic endometrioma: n= 99
Hepatic endometriosis: n= 97
Liver endometrioma: n= 303
Liver endometriosis: n= 301
Articles considered, n = 34
Articles excluded, n = 766
Hepatic endometrioma: n= 99Hepatic endometriosis: n= 97Liver endometrioma: n= 303Liver endometriosis: n= 301
Articles excluded: n= 766
Articles considered: n= 34

Page 3Global Scientific Research Journal of Surgery
Hepatic Endometriosis: Systematic Review of Literature AND A Case Report
Table 2: Features of Reported Cases of Hepatic Endometriosis
Author/Year Refer-ence
Hystory of Endome-
triosis
Coexisting pelvic endome-
triosis
Previous Pelvic operation Pathology Treatment
Finkel 1986 [11] No Not available Fallopian tube cyst removal
Hepatic endome-trioma
Cyst enucleation by laparotomy
Grabb/1986 [23] No No Fallopian tube cyst removal
Hepatic endome-trioma
Danazol + deroof-ing therapy
Rovati/1990 [38] No Yes No Hepatic endome-trioma
Left lateral seg-mentectomy by
laparotomy
Verbeke/1996 [43] No No No Hepatic endome-trioma
Hemihepatectomy by laparotomy
(2 patients included) No No No Hepatic endome-trioma
Segmental liver resection by lapa-
rotomy
Cravello/1996 [21] Yes No No Hepatic endome-triosis
Tumorectomy by laparotomy
Chung/1998 [20] Yes YesLeft ovarian
cystectomy due to endometriosis
Hepatic endome-trioma
Cyst enucleation by laparotomy
Weinfeld/1998 [44] Yes No
Total abdominal hysterectomy,
bilateral salpingo-oophorectomy
Adenosquamous carcinoma arising
in hepatic endome-triosis
Segmental liver resection by lapa-
rotomy
Inal/2000 [29] Yes Yes Treatment of pelvic endometriosis
Hepatic endome-triosis Danazol therapy
N’Senda/2000 [34] Yes No
Total abdominal hysterectomy,
bilateral salpingo-oophorectomy
Adenosarcoma arising in hepatic
endometriosis
Segmental liver resection by lapa-
rotomy
Bohra/2001 [17] Yes Not available
Total abdominal hysterectomy,
bilateral salpingo-oophorectomy
Hepatic endome-trioma
Segmental liver resection by lapa-
rotomy
Jeanes/2002 [30] Yes Not available
Total abdominal hysterectomy,
bilateral salpingo-oophorectomy
Hepatic endome-trioma
Removal of cyst by laparotomy
Huang/2002 [28] Yes Not available
Total abdominal hysterectomy,
bilateral salpingo-oophorectomy
Hepatic endome-trioma
Left hepatic lobectomy by lapa-
rotomy
Khan/2002 [32] Yes Not available
Total abdominal hysterectomy,
bilateral salpingo-oophorectomy
Hepatic endome-triosis
En bloc removal of right lobe mass, left lobe mass left
by laparotomy

Page 4Global Scientific Research Journal of Surgery
Hepatic Endometriosis: Systematic Review of Literature AND A Case Report
Table 2 (Cont.)
Author/Year Refer-ence
Hystory of Endome-
triosis
Coexisting pelvic endome-
triosis
Previous Pelvic operation
Pathology Treatment
(2 patients includ-ed) Yes No Removal of ruptured
cystEndometrial stro-
mal sarcomaRight hepatectomy
by laparotomy
Groves/2003 [24] Not available Not available
Total abdominal hys-terectomy, bilateral salpingo-oophorec-
tomy
Hepatic endome-trioma
Right hemiepa-tectomy by lapa-
rotomy
Tuech/2003 [42] No No No Hepatic endome-trioma
Removal of cyst by laparotomy
Reid/2003 [35] Yes Not available
Endometriosis surgery, subto-
tal hysterectomy, bilateral oopherec-
tomy, resection of an endometriotic bowel lesion, removal of
right lobe cyst
Hepatic endome-trioma showing
moderately atipica complex hyperpla-
sia
Right hemihepa-tectomy by lapa-
rotomy
Jelovsek/2004 [31] Yes Not availableHysterectomy with
bilateral salpingooo-phrectomy
Endometrioma with focal areas of mullerian adeno-
sarcoma
Resection of the liver mass
Nezhat/2005 [13] Yes Yes No Hepatic endome-triosis
Cyst enucleation by laparoscopi
(2 patients includ-ed) Yes Yes Treatment of pelvic
endometriosisHepatic edome-
triosisLaparoscopic exci-
sion
Sanchez-Per-ez/2006 [39] Yes Not available Ovarian cystectomy
Hepatic endome-trioma showing
moderately atipica complex hyper-
plasia with foci of carcinoma in situ
Right hepatectomy
Goldsmith/2009 [6] Yes Not available
Total abdominal hys-terectomy, bilateral salpingo-oophorec-
tomy
Hepatic endome-triosis
No anatomical resection
Asran/2010 [16] Yes Yes
Hysterectomy, right salpingo-oophorec-
tomy, bowel loop resection due to
obstruction
Hepatic endome-triosis, with involve-
ment of multiple liver segments
Not reported
Roesch-Di-etlen/2011 [37] No No No
Hepatic endometri-osis with right liver lobe involvement
Medical treatment (Danazol)
Schuld/2011 [40] No No No Hepatic endome-triosis
Atipical liver resec-tion of VIII segment

Page 5Global Scientific Research Journal of Surgery
Hepatic Endometriosis: Systematic Review of Literature AND A Case Report
Table 2 (Cont.)
Author/Year Refer-ence
Hystory of Endome-
triosis
Coexisting pelvic endome-
triosis
Previous Pelvic operation Pathology Treatment
Fluegen/2013 [22] No No No Hepatic endome-triosis
Ultrasonic pericis-tectomy (segments
IV-V and VIII)
Hertel/2013 [26] No No Partial Hysterecto-my, oophorectomy
Hepatic endome-triosis
Resection of a large cystic hepatic lesion involving the
segments V, VI, VII, and VIII of the
liver
Bouras/2013 [18] No No No Hepatic endome-triosis
Left lateral hepa-tectomy with partial right ventricle free wall resection and medial diaphragm
resection
Rivkine/2013 [36] No No Conservative hyster-ectomy
Hepatic endome-triosis
Left lobectomy with diaphragm resec-
tion for a large cystic tumor in liver segments II and III
Hsu/2014 [27]
NA Yes Hysterectomy Hepatic endome-triosis
Follow-up every 6 months
NA Yes None Hepatic endome-triosis
Left lobe hepatec-tomy, VIII
NA None Hysterectomy Hepatic endome-triosis
Left lobe hepatec-tomy
NA YesHysterectomy +
salpingo-oophorec-tomy
Hepatic endome-triosis
Left lobe hepatec-tomy
(5 patients includ-ed) NA Yes
Hysterectomy + salpingo-oophorec-
tomy
Hepatic endome-triosis
Lesion removal, segment VI
Cantos Pal-larés/2014 [19] No Yes No Hepatic endome-
triosis
Resection of lesion in liver segment V, adhered to the right
hemidiafragm
Zhao/2014 [45] No No No Hepatic endome-triosis
Resection of a cystic mass in seg-ment IV of the liver
Liu/2015 [33] No No No Hepatic endome-triosis
Pericistectomy of a large cystic tumor
occupying segment III of the liver

Page 6Global Scientific Research Journal of Surgery
Hepatic Endometriosis: Systematic Review of Literature AND A Case Report
Table 2 (Cont.)
Author/Year Refer-ence
Hystory of Endome-
triosis
Coexisting pelvic endome-
triosis
Previous Pelvic operation Pathology Treatment
Sopha/2015 [41] No No Right salpingo-oo-phorectomy
Hepatic endome-triosis
Laparoscopic excisional biopsy
of VII segment. No treatment, patient
in follow-up
Sherif/2016 [46] Yes YesTotal abdominal hysterectomy for
endometrosis
Hepatic endome-trioma
Hepatic segmen-tectomy of VII
segment
De Riggi/2016 [47] No No No Cystic hepatic endometriosis
Atypical left hepa-tectomy tailored
on right margins of lesion
Mastrangelo/2018 present case No No No Hepatic endome-
triosis Right hepatectomy
The first case of intraparenchymal endometriosis of the liver was reported by Finkel et al. in 1986 in a 21 years old woman, who suffered from epigastric pain, nausea, and vomiting. She was found to have an en-dometrial cyst measuring 13 cm in diameter located in the left lobe of the liver [11]. Subsequently, 40 ad-ditional cases have been reported in 33 studies [6, 14, 16-47]. Four of these reports included more than one patient [14, 27, 32, 36]. The major clinical fea-tures of these previously described 41 patients, and the present one, are summarised in Table 2. They occurred in women with an age range from 21 to 73 years. They were cystic and located either in the left or the right lobe of the liver. In some cases [6, 11, 18, 22-24, 26, 30, 34, 35, 38, 42, 43, 47], the tumours had a diameter of more than 10 cm. They most often presented with abdominal pain, which was not asso-ciated with menses. Twelve patients [14, 16, 19, 20, 27, 29, 38, 46] had a coexisting and 18 had a past history of pelvic endometriosis [6, 14, 16, 17, 20, 21, 28-32, 34, 35, 39, 44, 46]. Twenty-six of them had previously undergone pelvic surgery [6, 11, 14, 16, 17, 20, 23, 24, 27-32, 34-36, 39, 41, 44, 46]. All pa-tients with hepatic endometriosis, but three [23, 29, 37] who were treated with Danazol, underwent sur-gery. In 5 women, areas of epithelial or stromal ma-lignant transformation, arising in hepatic endometrio-sis, were observed in the resected tissue specimens (one case of adenosquamous carcinoma, 2 cases of adenosarcoma, one case of endometrial stromal sar-
coma, one case including foci of carcinoma in situ in hepatic endometrioma with atypical complex hyper-plasia) [31, 32, 34, 39, 44]. The described subjects presented both intraparenchymal and extraparen-chymal hepatic endometriosis. Further three reports were not considered, since they were published in a language other than English (one in French, one in Spanish and one in Japanese) [39, 48, 49].
Case ReportThis is a 36 years old multiparous white Caucasian woman, who was referred to our Unit in September 2010, because of acute right upper quadrant pain. The patient’s past medical history was significant for hypertension and hyperlipidemia and she had no his-tory of endometriosis. Examination revealed slight right upper quadrant tenderness, but the patient large body habitus precluded any accurate assessment for an abdominal mass. Workup revealed a dropping of hemoglobin level and the alteration of the liver func-tion tests. A dedicated abdominal ultrasound dem-onstrated a right lobe non-homogeneous liver pa-renchyma. In light of this, a Computed Tomography (CT) scan of the abdomen and pelvis was performed confirming the liver lesion and showing an iperdense area with small arterial blushes on the VI segment, in the V segment a disomogeneous lesion (5 X 4 cm), with a hypodense margin, was found. These features suggested the existence of a possible adenoma with

Page 7Global Scientific Research Journal of Surgery
Hepatic Endometriosis: Systematic Review of Literature AND A Case Report
intralesional bleeding (Figure 1). Angiography did not reveal contrast enhancement blush compatible with active arterial bleeding. For an adequate clinical monitoring, the patient was transferred to the Inten-sive Care Unit, where, because of the decrease of the hemoglobin level, a blood transfusion with 4 units of red cells was carried out. In consideration of these findings prompted surgical consultation took place and the patients was transferred to our Surgical unit. Repeated CT scanning revealed 4 lesions ranging from 2-3 cm in the right hepatic lobe without signs of active bleeding and a diagnosis of adenomas or atypical multiple hemangiomas was made. The pa-tient was discharged from hospital 8 days later with no abnormality in hematological parameters and the liver function tests in the normal range. A Magnetic Resonance Imaging (MRI) (Figure 2) was performed in order to monitor the hepatic lesion and showed a significant reduction of subcapsular hematoma and confirmed the multiple lesions described above and confined to the right liver lobe. A right emihepatec-
tomy procedure was planned for resection of liver lesions. In February 2011 surgical exploration re-vealed two diaphragmatic nodules less than 1 cm in diameter that were excised, and a fresh-frozen sec-tion histology was made. Histologic examination re-vealed endometrial glands and stroma within hepatic tissue, suggesting the presence of an endometriosis cyst. A thorough exploration of the abdominal cavity revealed no evidence of other endometrial implants. Hepatic ultrasound was performed and showed a non-homogeneous mass in the V-VIII segments of 5 X 4 cm in the context of a steatotic parenchyma. The patient was submitted to right emihepatectomy using Cavitron Ultrasonic Aspirator (CUSA System 200, Val-leylab, Boulder, CO, USA). A permanent histological examination of hepatic parenchyma was consistent with metahemorrhagic endometriosis cysts (Figure 3) as well the diaphragmatic nodules. Immunohis-tochemical characterization was made on selected samples with a marker for endometrial glands, and the cytoplasm of stromal cells were strongly positive
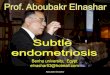
Figure 1: Computed Tomography (CT) Scan of the Abdomen and Pelvis, Showing an Hyperdense Area with Small Arterial Blushes in the VI Segment and a Disomogeneous Lesion, with a Hypodense Margin, in the V Segment

Page 8Global Scientific Research Journal of Surgery
Hepatic Endometriosis: Systematic Review of Literature AND A Case Report
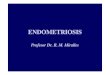
Figure 2: Magnetic Resonance (MR) of the Abdomen and Pelvis, Showing a Significant Reduction of Subcapsular Hematoma and Confirming the Multiple Lesions Described above and Confined to the Right Liver Lobe
Figure 3: Peri-Hepatic Haemorragic Cyst

Page 9Global Scientific Research Journal of Surgery
Hepatic Endometriosis: Systematic Review of Literature AND A Case Report
for Cluster of Differentiation (CD) 10 (Figure 4). Post-operative course was complicated by pulmonary embolism (although lower extremity echo-doppler showed no abnormality), treated with low-molecular-weight heparins and anticoagulant therapy thereafter up to 6 months. She was discharged ten days after surgery. One year after surgery the patient is asymp-tomatic. Surveillance Contrast Enhancement Ultra-sound (CEUS) demonstrated persisting multiple liver lesions (maximum diameter 2 cm) in the remnant he-patic left lobe. Transvaginal ultrasound demonstrated uterine endometriotic cysts. Hormone replacement therapy was contraindicated because of the high risk of thromboembolism; therefore, the patient has been treated with Gonadotropin-Releasing Hormone (GnRH) agonists.
DiscussionEndometriosis is an estrogen-dependent disorder that can result in substantial morbidity, including pelvic pain, multiple operations, and infertility which affects 6-10% of women in their reproductive years and af-fects up to 35-50% of women with pain or infertility [5].
Extra pelvic sites of endometriosis have been de-scribed varying from abdominal to thoracic organs. The only organ in the abdominal cavity that is appar-ently refractory to the disease is the spleen [7]. Hepat-ic endometriosis is an unusual phenomenon and sev-eral theories have been invoked to account for hepatic endometriosis, but the pathogenesis, especially in such rare cases, remains uncertain. The most widely accepted theory is based upon possible mechanisms
Figure 4: Peri-Hepatic Tissue with Hemorrhage, Hemosiderin Deposition, Macrophages and Endometrial-like Glands Surrounded by Spindled Endometrial Stroma (A, B, C) Strongly Positive for CD10 (D)

Page 10Global Scientific Research Journal of Surgery
Hepatic Endometriosis: Systematic Review of Literature AND A Case Report
which transport endometrial tissue to distant sites in fashion analogous to metastatic spread of neoplasm. The proposed theories of endometrioma formation are retrograde spread of endometrial cell collections during menstruation, blood, lymphatic or iatrogenic spread, celomatic metaplasia of the pelvic peritoneal cell, immune system dysfunction and autoantibody formation [9, 10].
It is likely that a combination of these theories may apply to each individual patient. Two phenotypic situ-ations should be distinguished: 1) patients in whom the only endometriotic lesion is an intraparenchymal hepatic endometrioma; and 2) patients in whom the in-traparenchymal liver endometrioma is associated with endometriosis elsewhere. Some Authors postulated that the theory of embryonic mullerian rests [13] of-fered the best explanation for the pathogenesis of iso-lated hepatic endometriomas as well as the absence of endometriosis in the spleen [14], that presents an environment hostile to survival of embryonic mullerian rest. Organogenesis of the liver, spleen and muller-ian ducts begins in that order between the 2nd and 6th month of fetal life, affording an opportunity for duplicat-ed mullerian tissue to become incorporated in the liver and the spleen [12]. However, since the liver initially is the primary organ of hematopoiesis, the optimal conditions for vasculogenesis not only ensure survival of intrahepatic mullerian rest but also maintenance of full functional potential during the long interval of hormonal deprivation between withdrawal of placen-tal hormones and onset of estrogen stimulation [12]. With regard to the second phenotypic presentation as intraparenchymal hepatic endometrioma associated with endometriosis elsewhere, the theory of embry-onic mullerian rests probably still holds because there is no direct communication between uterine and liver lymphatics. Furthermore, vascular spread also could provide a plausible explanation for the pathogenesis of the intraparenchymal endometriosis in the liver [42].
The diagnosis of extrapelvic endometriosis may be challenging. Case reports described in literature dem-onstrated that medical history regarding pain may not be helpful in diagnosing hepatic endometriosis. This is also valid in our case where the upper abdominal pain associated with a bleeding lesion of the liver could be related to liver masses along with hepatocellular car-cinoma and adenoma both of which occur more com-monly. Since the lesion was bleeding, a percutaneous
liver biopsy was not performed. Although ultrasound, CT scan and MRI aid in the diagnosis, the final diag-nosis can be made only by pathologic evaluation, be-cause there are no radiological characteristics specific for the hepatic endometrioma. This is further compli-cated by the potentially fluctuating appearance of en-dometrial tissue under hormonal stimulation [6].
The laparoscopic approach may be recommended as an option for the diagnosis and the treatment of hepatic endometriosis in proper settings. One of the significant advantages of this minimally invasive pro-cedures is the thorough exploration of the abdominal cavity and pelvis, that could reveal endometriotic im-plants [14]. Frozen section histology at the time of sur-gery may help to avoid radical liver resection with no conversion to open surgery, when the size and the site of lesions could allow it [6].
In this context, it seems that no clues to hepatic endo-metriosis diagnosis can be gained from the history or examination and the imaging studies are not specific to this condition. For these reasons, early diagnosis may require a high degree of suspicion in women with liver mass.
In view of the present case report and the few ones described in the literature it is difficult to recommend a management strategy for this group of patients. In subjects with superficial lesions who are asympto-matic and are not treated, one should consider the possibility that these lesions may become infiltrative and symptomatic. When the patient is symptomatic, the need for treatment is clear. However, it remains undetermined whether asymptomatic patients should be treated to prevent the potentially severe and de-bilitating complications that can occur if the endometri-otic lesions deeply infiltrate the liver. Although rare, malignancy occurring within endometric foci has been well documented [25].
Hepatic endometriosis is a rare disorder character-ized by the presence of ectopic endometrium in the liver and its etiology and pathogenesis are unclear. The present case and the evidence in literature sug-gest that hepatic endometrioma should be included in the differential diagnosis for a woman of any age pre-senting with hepatic cystic or solid lesions of unknown cause, with or without a history of pelvic endometrio-sis. The lack of a clinical-radiological pattern makes it difficult to have a correct preoperative diagnosis, so

Page 11Global Scientific Research Journal of Surgery
Hepatic Endometriosis: Systematic Review of Literature AND A Case Report
that it is made by histological examination. Surgery plays an important role in the treatment of HE, is re-lated to the symptoms and the potential for malignant transformation of the lesion as well [32].
ConclusionOur paper underlines that hepatic endometriosis may represent a diagnostic dilemma. In fact, considering that liver involvement in patients suffering from this disease is a rare event, its presentation may be unu-sual and imaging techniques may be inconclusive, be-cause of lack of a specific radiological pattern. To date, only a limited number of cases have been described in literature. In our clinical practice, we observed a 36 years old white Caucasian woman with hepatic endometriosis. The diagnosis required the combined assessment of different elements: clinical history, im-aging techniques, surgical exploration and histological examination. Therefore, we performed a systematic review of literature to evaluate the impact of this dis-orders in clinical practice. This case report highlights that physicians should consider this pathological con-dition, even if infrequent, in the differential diagnosis for a woman of any age presenting with hepatic cystic or solid lesions of unknown cause (with or without a history of pelvic endometriosis). A correct preopera-tive diagnosis is very difficult, and the recognition of this condition mainly relies on a proper assessment of anamnestic, radiological and histological data.
References1. Benagiano G, Brosens I, History of adeno-
myosis. Best Pract Res Clin Obstet Gynaecol 2006;20:449-63.
2. Gustofson RL, Kim N, Liu S, Stratton P, Endome-triosis and the appendix: a case series and com-prehensive review of the literature. Fertil Steril 2006;86:298-303.
3. Jenkins S, Olive DL, Haney AF, Endometriosis: pathogenetic implications of the anatomic distri-bution. Obstet Gynecol 1986;67:335-8.
4. Comiter CV, Endometriosis of the urinary tract. Urol Clin North Am 2002;29:625-35.
5. Giudice LC, Kao LC, Endometriosis. Lancet 2004;364:1789-99.
6. Goldsmith PJ, Ahmad N, Dasgupta D, Campbell J, Guthrie JA, Lodge JP, Case hepatic endometrio-
sis: a continuing diagnostic dilemma. HPB Surg 2009;2009:407206.
7. Markham SM, Carpenter SE, Rock JA, Extrapel-vic endometriosis. Obstet Gynecol Clin North Am 1989;16:193-219.
8. Martin JD, Jr., Hauck AE, Endometriosis in the male. Am Surg 1985;51:426-30.
9. Sampson JA, Metastatic or Embolic Endometrio-sis, due to the Menstrual Dissemination of Endo-metrial Tissue into the Venous Circulation. Am J Pathol 1927;3:93-110 43.
10. Sampson JA, The development of the implanta-tion theory for the origin of peritoneal endometrio-sis. Am J Obst and Gynec 1940;40:549-557.
11. Finkel L, Marchevsky A, Cohen B, Endometrial cyst of the liver. Am J Gastroenterol 1986;81:576-8.
12. Batt RE, Lele SB, Mitwally MF, Yeh J, Isolated hepatic endometriosis: as rare as hens’ teeth, but sometimes you can learn a lot from a hen with teeth. Fertil Steril 2003;80:1284; author reply 1284-5.
13. Batt RE, Smith RA, Buck Louis GM, Martin DC, Chapron C, Koninckx PR, et al., Mullerianosis. Histol Histopathol 2007;22:1161-6.
14. Nezhat C, Kazerooni T, Berker B, Lashay N, Fer-nandez S, Marziali M, Laparoscopic management of hepatic endometriosis: report of two cases and review of the literature. J Minim Invasive Gynecol 2005;12:196-200.
15. Moher D, Liberati A, Tetzlaff J, Altman DG, Pre-ferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann In-tern Med 2009;151:264-9, W64.
16. Asran M, Rashid A, Szklaruk J, Hepatic endome-triosis mimicking metastatic disease: a case report and review of the literature. J Radiol Case Rep 2010;4:26-31.
17. Bohra AK, Diamond T, Endometrioma of the liver. Int J Clin Pract 2001;55:286-7.
18. Bouras AF, Vincentelli A, Boleslawski E, Truant S, Liddo G, Prat A, et al., Liver endometriosis pre-senting as a liver mass associated with high blood

Page 12Global Scientific Research Journal of Surgery
Hepatic Endometriosis: Systematic Review of Literature AND A Case Report
levels of tumoral biomarkers. Clin Res Hepatol Gastroenterol 2013;37:e85-8.
19. Cantos Pallares M, Lopez Andujar R, Montalva EM, Castillo Ferrer MC, Rayon Martın M, Endo-metrioma hepatico. Actualizacion y nuevos abor-dajes. Cir Esp 2014;92:212–214.
20. Chung CC, Liew CT, Hewitt PM, Leung KL, Lau WY, Endometriosis of the liver. Surgery 1998;123:106-8.
21. Cravello L, D’Ercole C, Le Treut YP, Blanc B, He-patic endometriosis: a case report. Fertil Steril 1996;66:657-9.
22. Fluegen G, Jankowiak F, Zacarias Foehrding L, Kroepil F, Knoefel WT, Topp SA, Intrahepatic endometriosis as differential diagnosis: case re-port and literature review. World J Gastroenterol 2013;19:4818-22.
23. Grabb A, Carr L, Goodman JD, Mendelson DS, Cohen B, Finkel L, Hepatic endometrioma. J Clin Ultrasound 1986;14:478-80.
24. Groves AM, Whitfield R, Lomas DJ, Gibbs P, Im-aging of a hepatic endometrioma in a patient with multiple haemangiomas. J Hepatol 2003;38:547.
25. Heaps JM, Nieberg RK, Berek JS, Malignant neo-plasms arising in endometriosis. Obstet Gynecol 1990;75:1023-8.
26. Hertel JD, Guimaraes M, Yang J, Hepatic endo-metriosis diagnosed by liquid-based cytology: a case report. Diagn Cytopathol 2014;42:441-4.
27. Hsu M, Terris B, Wu TT, Zen Y, Eng HL, Huang WT, et al., Endometrial cysts within the liver: a rare entity and its differential diagnosis with mu-cinous cystic neoplasms of the liver. Hum Pathol 2014;45:761-7.
28. Huang WT, Chen WJ, Chen CL, Cheng YF, Wang JH, Eng HL, Endometrial cyst of the liver: a case report and review of the literature. J Clin Pathol 2002;55:715-7.
29. Inal M, Bicakci K, Soyupak S, Oguz M, Ozer C, Demirbas O, et al., Hepatic endometrioma: a case report and review of the literature. Eur Radiol 2000;10:431-4.
30. Jeanes AC, Murray D, Davidson B, Hamilton M, Watkinson AF, Case report: hepatic and retro-per-
itoneal endometriosis presenting as obstructive jaundice with ascites: a case report and review of the literature. Clin Radiol 2002;57:226-9.
31. Jelovsek JE, Winans C, Brainard J, Falcone T, Endometriosis of the liver containing mullerian adenosarcoma: case report. Am J Obstet Gynecol 2004;191:1725-7.
32. Khan AW, Craig M, Jarmulowicz M, Davidson BR, Liver tumours due to endometriosis and endome-trial stromal sarcoma. HPB (Oxford) 2002;4:43-5.
33. Liu K, Zhang W, Liu S, Dong B, Liu Y, Hepatic en-dometriosis: a rare case and review of the litera-ture. Eur J Med Res 2015;20:48.
34. N’Senda P, Wendum D, Balladur P, Dahan H, Tubi-ana JM, Arrive L, Adenosarcoma arising in hepatic endometriosis. Eur Radiol 2000;10:1287-9.
35. Reid GD, Kowalski D, Cooper MJ, Kaloo P, He-patic endometriosis: a case report and review of the literature. Aust N Z J Obstet Gynaecol 2003;43:87-9.
36. Rivkine E, Jakubowicz D, Marciano L, Polliand C, Poncelet C, Ziol M, et al., Hepatic endometrioma: a case report and review of the literature: report of a case. Surg Today 2013;43:1188-93.
37. Roesch-Dietlen F, Jimenez-Garcia A, Perez-Mo-rales A, Grube-Pagola P, Ramirez-Cervantes KL, Remes-Troche JM, Hepatic endometriosis. Ann Hepatol 2011;10:347-8.
38. Rovati V, Faleschini E, Vercellini P, Nervetti G, Tagliabue G, Benzi G, Endometrioma of the liver. Am J Obstet Gynecol 1990;163:1490-2.
39. Sanchez-Perez B, Santoyo-Santoyo J, Suarez-Munoz MA, Fernandez-Aguilar JL, Aranda-Nar-vaez JM, Gonzalez-Sanchez A, et al., [Hepatic cystic endometriosis with malignant transforma-tion]. Cir Esp 2006;79:310-2.
40. Schuld J, Justinger C, Wagner M, Bohle RM, Koll-mar O, Schilling MK, et al., Bronchobiliary fistula: a rare complication of hepatic endometriosis. Fer-til Steril 2011;95:804 e15-8.
41. Sopha SC, Rosado FG, Smith JJ, Merchant NB, Shi C, Hepatic uterus-like mass misdiagnosed as hepatic abscess. Int J Surg Pathol 2015;23:134-9.

Page 13Global Scientific Research Journal of Surgery
Hepatic Endometriosis: Systematic Review of Literature AND A Case Report
42. Tuech JJ, Rousselet MC, Boyer J, Descamps P, Arnaud JP, Ronceray J, Endometrial cyst of the liver: case report and review. Fertil Steril 2003;79:1234-6.
43. Verbeke C, Harle M, Sturm J, Cystic endome-triosis of the upper abdominal organs. Report on three cases and review of the literature. Pathol Res Pract 1996;192:300-4; discussion 305.
44. Weinfeld RM, Johnson SC, Lucas CE, Saksouk FA, CT diagnosis of perihepatic endometriosis complicated by malignant transformation. Abdom Imaging 1998;23:183-4.
45. Zhao H, Li Y, Cao D, An uncommon cystic lesion of the liver. Gastroenterology 2014;146:e8-9.
46. Sherif AM, Musa ER, Kedar R, Fu L, Subcapsular hepatic endometriosis: case report and review of the literature. Radiol Case Rep 2016;11:303-308.
47. De Riggi MA, Fusco F, Marino G, Izzo A, Giant endometrial cyst of the liver: a case report and re-view of the literature. G Chir 2016;37:79-83.
48. Kouto Fichet G, Aube C, Lebigot J, Pessaux P, Rousselet MC, Caron C, [Endometriotic cyst of the liver: a case report]. J Radiol 2004;85:124-7.
49. Watari H, Shibahara N, Ebisawa S, Nogami T, Fu-jimoto M, Hikiami H, et al., [Case report; A case of hepatic endometriosis with periodic right up-per quadrant pain]. Nihon Naika Gakkai Zasshi 2012;101:3233-5.
Citation: Laura Mastrangelo, Michele Masetti, Maria Grazia De Blasiis, Paolo Emilio Orlandi, Angela Salerno, Dario de Biase, Sirio Fiorino and Elio Jovine, ”Hepatic Endometriosis: Systematic Review of Literature ANS A Case Report”, Global Scientific Research Journal of Surgery, 1(1), 2018, pp. 1-13.
Copyright © 2018 Laura Mastrangelo et al., This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.