-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
Department of Gastroenterology, Hepatology and
Endocrinology
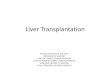
(1) Obermayer-Straub et al. Gastroenterology 2001; 121:668.
Hepatic Autoantigens in APECED associated AIH
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
Alcoholic Cirrhosis
Hepatitis in APS1
Dihydralazine Hepatitis
Tienilic Acid Hepatitis
Halothane Hepatitis
Autoimmune Hepatitis
Chronic Hepatitis C
Chronic Hepatitis D
Gonadal Failure in APS1
Adrenal Failure in APS1
Addison Disease
CYP2C9
rCYP3A1 rCYP2C11
CYP2E1 CYP2D6
UGT1
CYP11 CYP17
P450s & UGTs
CYP21
Anticonvulsant Hepatitis
? in APS1
CYP2A6 CYP1A2
CYPs and UGTs : Targets for Immune Reactions
Manns and Obermayer, Hepatology, 2002
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
0
20
40
60
80
100
Pati
en
ts [
%]
Hepatitis
in APS1 AIH PBC PSC
Vogel et al., Hepatology 2001 Djilali-Saiah et al., Journal of
Hepatology 2004
Frequency of Mutations in the AIRE Gene in Patients with AIH,
PBS and PSC
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
AIRE Mutations May Account for a More Severe Clinical Course in
Children with Autoimmune Liver Diseases
Patient 1 Patient 2 Patient 3 Patient 4 Patient 5
Autoantibodies Anti LKM-1 Anti CYP450 SCC Anti CYP450 C17
Anti-LC-1
Anti LKM-1 Anti CYP-450 SCC Anti CYP450 C17
Anti LKM-1
Anti LC-1
Extrahepatic manifestation
Hypopara-thyroidism Addison‘s disease
Gastric atrophy
(after ALF)
Autoimmune Enteropathy
(after OLT)
Autoimmune Enteropathy Autoimmune Nephropathy
(before ALF)
None
None
AIRE analysis Homozygous Deletion
P398fsX448, Exon 10
Homozygous Finnish major
mutation R257X, Exon 6
Heterozygous Polymorphism
R441C, Exon 12
None None
Clinical course ALF- 3 y, Azathioprin + Steroids
Remission
ALF- 6 m, OLT, azathioprin,
Steroids, Tacrolimus AIH recurrence
Exitus letalis at 3.5 y
ALF- 2 y, Azathioprin, Steroids,
Cyclosporin A Remission
ALF- 8 m, OLT, Chronic rejection
OLT n° 2 hepatic artery
thrombosis Exitus letalis 3.5 y
ALF- 1 y Azathioprin,
Steroids, Cyclosporin A
Remission
Lankisch, Jaquemin et al., Journal of Pediatrics 2005
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
Challenges in the diagnosis of AIH
• Diagnostic criteria
• Scoring systems
• Role of Autoantibodies
• Histology
• Differential Diagnosis: DILI, Viral Hepatitis, APECED, etc
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
10
AASLD CPG: First Line Treatment of AIH (adults)
Monotherapy Combination Therapy
Prednisone Prednisone Azathioprine
(mg/ day) (mg/ day) USA (mg/ day) EU (mg/ kg/ day)
Week 1 60 30 50 1 - 2
Week 2 40 20 50 1 - 2
Week 3 30 15 50 1 – 2
Week 4 30 15 50 1 – 2
Maintenance-Therapy 20 and less 10 50 1 - 2
Reasons for Choice of Therapy
Cytopenia Thiopurinmethyl-transferase-Deficiency Pregnancy
Tumors Therapy
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
Management of AIH in adults
Mieli-Vergani, G. et al. (2018) Autoimmune hepatitis
Nat. Rev. Dis. Primers doi:10.1038/nrdp.2018.17
Adapted with permission from European Association for the Study
of the Liver. EASL Clinical Practice Guidelines: Autoimmune
hepatitis. J. Hepatol. 63, 971–1004 (2015), Elsevier.
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
12
Treatment of AIH: Endpoints
AASLD Clinical Practice Guidelines: Manns MP, et al. Hepatology.
2010 Jun;51(6):2193-213.
Endpoints Criteria Recommendations Remission Disappearance of
clinical symptoms,
Normalization of aminotransferases (ALT, AST), bilirubin und
-globulins Normal liver histology or inactive liver cirrhosis
Slow Reduction of steroids within 6 weeks Control of serum AST,
ALT, total-bilirubin, and -globulins in 3-week intervals during and
3 months after withdrawal, then every 6 months for 2 years, then
every year
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
13
Application of the 2010 AASLD criteria of remission to a cohort
of Italian patients with autoimmune hepatitis
Muratori L et al, Hepatology (correspondence), 2010 | Muratori P
et al, Journal of Hepatology, 2009
AIH
(n=163)
Remission n=119 (73%) [AASLD 2002]
Remission n=42 (26%) [AASLD 2010]
TREATMENT
Remission AIH (>60 months)
methyilprednisolone 2-4 mg/daily or every other day
N=89
65 (73%) ALT
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
Jones, Manns, Terracciano, Torbenson, Vierling, The Lancet GH,
May 2018
• Endpoint: Normal ALT, normal IgG, normal histology
• When: after 6 months
• However, patients with normal ALT and IgG may still develop
cirrhosis and have increased liver mortality (e.g. UK AIH
cohort)
• Therefore: Is normal ALT still normal enough ?
Unmet Needs and New Models for Future Trials in Autoimmune
Hepatitis
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
15
Second Line Therapy for AIH: Alternative Drugs
Safety (Intolerance) versus Efficacy
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
16
Frequency and Nature of Side Effects (Adults)
AASLD Clinical Practice Guidelines: Manns MP, et al. Hepatology.
2010 Jun;51(6):2193-213.
Prednisone-Related Side Effects Azathioprine-Related Side
Effects
Type Frequency Type Frequency
Cosmetic (usually mild) Facial rounding, Weight gain, Dorsal
hump striae, Hirsutism, Alopecia
Somatic (usually mild) Emotional Instability, Glucose
intolerance, Cataract
80% (after 2 years)
Hematologic (mild) Cytopenia
46% (especially with
cirrhosis)
Somatic (severe) Osteopenia, Vertebral compression, Diabetes
(brittle), Psychosis, Hypertension (labile)
13% (Treatment
ending)
Hematologic (severe) Leukopenia Thrombocytopenia
6% (Treatment
ending)
Inflammatory/Neoplastic Pancreatitis, Opportunistic infection,
Malignancy
Rare Somatic (mild) Nausea, Emesis, Rash, Fever, Arthralgias
5%
Neoplastic 3%
(after 10 years) Hematologic /enteric Bone marrow failure,
villous atrophy, Malabsorption
Rare
Teratogenic Rare (theoretical)
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
17
Decrease Of Steroid Specific Side Effects In Patients Switched
From Prednisone To Budesonide (n=87)
Manns MP, et al. Gastroenterology 2010;139:1198-1206
40.2% N=35
18.4% n=16
0
10
20
30
40
50
Month 6 Month 12
Perc
ent
P
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
18
European AIH-BUC Pediatric Subanalysis
Woynarowski et al. J. Pediatrics 2013 *Two sample t-test
(two-sided). # Paired t-test
Mean weight change at Months 6 and 12
46 pts in 5 Pediatric Centers
1.2 0.5
5.1
-2.8 -4
-2
0
2
4
6
Month 6 Month 12
Weig
ht change, kg
#P
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
19
Role of Budesonide
– Instead of Predniso(lo)ne to reduce side effects in
combination with Azathioprine
• Induction of remission in risk patients for steroid specific
side effects (SSSE)
• Long-term maintenance of remission
– Approved for AIH in 23 European and 13 Non-European
countries
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
Budesonide Versus Prednisone: Limitations
• Budesonide should not be given to cirrhotic patients due
to
– Portal hypertension and loss of „topical effects“ – Potential
safety issues (Hempfling et al, Hepatology, 2003)
• Long term benefits, i.e. on bone disease, are pending, long
term studies are
needed – Peiseler et al, EASL-AASLD MTC AIH, 2015, Clin
Gastroenterol Hepatol, 2018
• Limited if any benefit for patients not responding or
dependent to
predniso(lo)ne – Lalanne et al, EASL – AASLD AIH MTC, London,
2015
EDITORIAL: The right drug at the right time for the right
patient Manns, Jaeckel, Taubert, Clin Gastroenterol Hepatol,
2018
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
EFFICACY OF BUDESONIDE FOR THE LONG-TERM TREATMENT OF AUTOIMMUNE
HEPATITIS IN A SINGLE CENTRE EXPERIENCE
Peiseler et al, EASL - AASLD AIH MTC, London, 2015, abstract
book, p 70; Clin Gastro Hep 2018
0
20
40
60
80
100
6 months 24 months
% n
orm
aliz
ation
of
tra
nsam
inases
• Single Center Study (Hamburg/Germany)
• 83 Patients – 66 AIH, 17 AIH-Overlap
0
5
10
15
20
25
# o
f p
atien
ts
24 mths. budesonide
Worsened
Stable
Improved
10%
38%
35%
Initial Tx.
Prednisolone dependency
Steroid sp. side effects
0
20
40
60
80
100
Bud
eson
ide a
dhe
ren
ce
Last follow-up
Return to prednisolone
On budesonide
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
BUDESONIDE IN THE TREATMENT OF EXPERIENCED AUTOIMMUNE HEPATITIS
PATIENTS WHO RELAPSED WHILE ON PREDNISONE AND/OR AZATHIOPRINE: FROM
TRIALS TO EVERYDAY PRACTICE
© 2017 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
WWW.AASLD.ORG 22
Lalanne et al, EASL - AASLD AIH MTC, London, 2015 , abstract
book, p 71 - 72
• Retrospective Single Center Study (Bologna/Italy)
• AIH reactivation under Prednisolone +/- Azathioprine with side
effects contraindicated an increase of dose (19 out of 327
patients)
• Regimen:
• 14/19 patients: 9mg Budesonide + 50mg Azathioprine until
remission, then taper to 6mg
• 5/19 patients: Budesonide monotherapy due to Azathioprine
intolerance/side effects
Treatment response (Transaminases and IgG)
Remission 37%
Incomplete/non Response 63%
Nonresponders: Switched to Prednisolone within 7 month
(1-60)
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
23 Frequency and Nature of Side Effects (Adults)
AASLD Clinical Practice Guidelines: Manns MP, et al. Hepatology.
2010 Jun;51(6):2193-213.
Prednisone-Related Side Effects Azathioprine-Related Side
Effects
Type Frequency Type Frequency
Cosmetic (usually mild) Facial rounding, Weight gain, Dorsal
hump striae, Hirsutism, Alopecia
Somatic (usually mild) Emotional Instability, Glukose
intolerance, Cataract
80% (after 2 years)
Hematologic (mild) Cytopenia
46% (especially with
cirrhosis)
Somatic (severe) Osteopenia, Vertebral compression, Diabetes
(brittle), Psychosis, Hypertension (labile)
13% (Treatment
ending)
Hematologic (severe) Leukopenia Thrombocytopenia
6% (Treatment
ending)
Inflammatory/Neoplastic Pancreatitis, Opportunistic infection,
Malignancy
Rare Somatic (mild) Nausea, Emesis, Rash, Fever, Arthralgias
5%
Neoplastic 3%
(after 10 years) Hämatologic /enteric Bone marrow failure,
villous atrophy, Malabsorption
Rare
Teratogenic Rare (theoretical)
Routine assessment of thiopurine methyltransferase (IPMT) ?
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
24
Mycophenolate Mofetil (MMF) as Second Line Therapy –
Retrospective Analysis
• MMF in n = 36 patients – n = 27 due to AZA intolerance – n =
09 due to AZA insufficiency
• Remission : < 2x ULN • Total Remission to MMF: 14/36 (38 %)
• Remission in AZA intolerant pts: 12/28 (~ 43 %) • Remission in
AZA failure pts: 02/08 (~ 25 %)
• MMF should be considered in AZA intolerant patients
Hennes et al, Am J Gastro, 2008
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
25
Mycophenolate induction therapy treatment naïve patients (first
line)
Zachou et al, J Hepatol 2011;55 636–646
▪Gamma globuline
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
26 Second line in autoimmune hepatitis: 6-thioguanine
Van den Brand, de Boer, ….Drenth, Bouma, EASL 2017
6-TG was effective and clinically well tolerated as rescue
treatment in 25 pts with AIH, previously non-responsive or
intolerant to thiopurins (AZA, 6-MP)
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 13.01.2018
27
Second Line Therapy for AIH: Alternative Drugs
Safety (Intolerance) versus Efficacy
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
28
Second Line Therapy for Treatment Failures:
Alternative Drugs
Dose Side effects
Cyclosporine A 3-5 mg/kg kg/qd hypertension renal
insuffiency
Tacrolimus 3 mg bid (5 – 7 ng/ml)
hypertension renal insuffiency Diabetes, neuropathy
Mycophenolate Mofetil 750-1000 mg bid Diarrhea, leucopenia
6-thioguanine 20 mg/day
6-mercaptopurine 1.5 mg/kg/day
Methotrexate 10 mg per week
Cyclophosphamide 1-1.5 mg/kg/day Cystitits, leucopenia
Everolimus 0.75-1.5mg bid (3-6ng/ml)
Proteinuria, lipid disturbance, ulcera
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
29
Everolimus (mTOR Inhibitor) as Second Line Therapy Retrospective
Analysis
• N=7 / steroid refractory
• 3/7 complete biochemical
response (BR)
• 4/7 incomplete biochemical
response (IR)
Ytting and Larsen, Scand J Gastroenterol 2015
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
30
Management of failures to standard of care
– Biologicals
• Anti TNF
• Anti CD 20 (Rituximab)
• Anti B cell and anti BAFF-R (VAY736)
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
31
Treatment of refractory AIH with anti-TNF
Weiler-Norman et al. J Hepatol 2013
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
32
Treatment of refractory AIH with anti-TNF
Weiler-Norman et al. J Hepatol 2013
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
33
Anti-TNF alpha may cause AIH
• Induction of AIH following TNF alpha antagonists: – Harada K
et al. Clin Rheumatol 2008 AIH Exacerbation following Etanercept in
patients with
rheumatoid arthritis
– Ozorio G et al. Med J Aust 2007 AIH following infliximab
therapy of ankylosing spondylitis.
– Cravo M. BioDrugs 2010 AIH induced by Infliximab in a patient
with Crohn‘s disease, no relapse after switch to adalimumab
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
Rituximab Treatment of AIH
PLoS ONE 6(10): e26358
Chimeric monoclonal antibody against B cell marker CD20
Rituximab
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
35 Rituximab response: case report Successful Treatment of
Refractory Autoimmune Hepatitis with Rituximab
D'Agostino et al. Pediatrics 2013
-
Department of Gastroenterology, Hepatology and
Endocrinology
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
37
Rituximab in AIH Immunohistochemistry
Burak et al. Can J Gastroenterol. 2013; 27: 272 – 80.
A: anti CD 3 staining B: Fox P3 + staining at baseline C: Fox P3
+ staining 48 weeks after starting rituximab
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
Rituximab treatment experience in patients with complicated type
1 autoimmune hepatitis in Europe and North America
Than et al, EASL 2018, J Hepatol, 68, S217-8, 2018
• 22 patients, retrospective analysis, UK, Canada Germany •
Befere and 24 months after RTX • Reduction of Predniso(lo)ne and
freedom of flares • Improvement of ALT, AST and sustained for 24
months, (p < 0.0010)
• ALT 167 IU/L to 32 IU/L (p< 0.001) • AST 127 IU/L to 29
IU/L • IgG 18.9 g/l to 13.2 g/L (p< 0.001)
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
Than et al, EASL 2018, J Hepatol, 68, S217-8, 2018
Kaplan-Meier curve of freedom from flare-up following Rituximab
therapy
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
Than et al, EASL 2018, J Hepatol, 68, S217-8, 2018
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
42
Rituximab – Complications and Adverse Events
• Usually mild, infrequent:
– Infusion reactions, bacterial infections, neutropenia, anemia,
rash, fever, diarrhea, reactivation of viral infections
• But include:
– Late onset neutropenia, rheumatic disease, HBV reactivation,
activation of a latent polyoma virus (JC virus) with multifocal
leucoencephalopathy
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
Molecular pathogenesis of autoimmune hepatitis
Manns et al., Journal of Hepatology, 2015
VAY736
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
VAY736: Anti-BAFF-R antibody with dual action 1) ADCC mediated B
cell depletion; 2) Functional BAFF-R blockade
www.clinicaltrials.gov: NCT03217422
Rapid and profound B cell depletion | Prevention of BAFF-induced
hardening of autoimmunity
BAFF-R blockade
BAFF
B
B
B cell depletion NK cells Kupffer cells Granulocytes
B
BAFF-R
B
VAY736
Persistence of pathogenic B cells
Differentiation into long-lived PC
1 2
http://www.clinicaltrials.gov/
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
45
AIH: Future Therapies
• Can we increase therapeutic response by strengthening
immunoregulation ?
• Anti CD 3
• Low dose IL-2
• Adoptive transfer of Tregs ?
Treg
Teff
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
Molecular pathogenesis of autoimmune hepatitis
Manns et al., Journal of Hepatology, 2015
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
Intrahepatic accumulation of Tregs in AIH
© 2017 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
WWW.AASLD.ORG 47
PB LTx: protocol biopsy after liver Tx; ACR: acute cellular
rejection after liver Tx (steroid sensitive portal hepatitis)
Hamburg cohort
Peiseler et al. 2012
Hannover cohort
Taubert et al. 2014
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
Low IL-2 in patients with incomplete remission and under steroid
therapy (pAIH)
Diestelhorst … Manns … Jaeckel, Taubert; Plos One 2017
Diestelhorst … Manns … Jaeckel, Taubert; submitted
Serum IL-2
pAIH: pediatric AIH; pNAFLD: pediatric NAFLD; aAIH: adult AIH
BR: subsequent biochemical remission; IR: subsequent incomplete
response; LTX: subsequent need for liver transplantation
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
Therapies of AIH: The Reality (1)
• SOC: None of the drugs Pred +/- Aza underwent drug development
program
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
Therapies of AIH: The Reality (1)
• SOC: None of the drugs Pred +/- Aza underwent drug development
program
– SOC not optimal for all !
– „Complete response“ varies from 26 – 90 %
– Responders have increased liver related mortality
– Intensified therapy for normal ALT and IgG but histological
activit y ?
– Some patients overtreated ?
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
Jones, Manns, Terracciano, Torbenson, Vierling, The Lancet GH,
May 2018
Bottom Up versus Top Down Approach
• Identification of high risk patients pretreatment and starting
with disease
modifying biological agents
• Unmet needs: biomarkers – Proteomic based serum activity
markers – Transcriptomic based liver tissue markers – Non-invasive
fibrosis markers
Unmet Needs and New Models for Future Trials in Autoimmune
Hepatitis
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
Therapies of AIH: The Reality
• SOC: None of the drugs Pred +/- Aza underwent drug development
program
• Non-Responder Therapie
– None of the therapies are approved
– Clinical observation: improvement of concomittant AIH, e.g.
TNF, anti CD20, stem cell therapies
– Use of approved immunosuppressive agents from rheumatology or
transplantation medicine
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
14 Studies Found For Autoimmune Hepatitis (Recruiting)
https://clinicaltrials.gov accessed April 2018.
https://clinicaltrials.gov/
-
Prof. Dr. med. M.P. Manns Department of Gastroenterology,
Hepatology and Endocrinology 11.04.2018
54
Thank you for your attention
Hannover Medical School