Embed Size (px)
Citation preview

HENATOLYMPHOIDSYSTEM
THIRDYEARMEDICALSTUDENTS-UNIVERSITYOFJORDAN
AHMADT.MANSOUR,MD
NONNEOPLASTICDISEASESOFTHEWHITEBLOODCELLS
• TherearefivemajortypesofWBCsintheblood:neutrophils,lymphocytes,eosinophils,basophilsandmonocytes.
• Thenormalfunctionofthewhitebloodcellsdependsonatightregulationoftheircountandtheirfunction.Therefore,diseasedevelopsifthereisaderangementofthecellscountorfunction,ittakesoneofthefollowingforms:
o Cytosis:increaseinthenumberofcirculatingcellsabovereferencerange.(Note:leukocytosismeansanincreaseintheWBCcount,neutrophiliameansincreaseintheneutrophiliccount,lymphocytosismeansincreaseinthelymphocyticcount,monocytosismeansincreaseinthemonocyticcount,basophiliameansincreaseinthebasophiliccountandeosinophiliameansincreaseintheeosinophiliccount).
o Cytopenia:decreaseinthenumberofcirculatingcellsbelowreferencerange.(Note:neutropeniameansdecreasedneutrophils,lymphocytopenia,orsimplylymphopenia,meansdecreaseinlymphocytes,monocytopeniameansdecreaseinmonocytes,eosinopeniameansdecreaseineosinophils,andbasopeniameansdecreaseinbasophils).
o Abnormalorabsentfunction
• Cytosis:o Neutrophilia:definedasanincreaseintheneutrophiliccountinthe
peripheralbloodabovereferencerangeforage.o Causes:bacterialinfectionisthemostcommonandmostimportant
etiology.Tissuenecrosisincasesofburnsortraumaandmedicationssuchasepinephrineandcorticosteroidsarealsoadditionalcausesforneutrophilia.
§ Somephysiologicconditionscanleadtoneutrophiliasuchasstress,smokingandpregnancy.
o Pathophysiology:neutrophilsarepresentinthebloodintwopopulations:circulatingandmarginal(meaningneutrophilsstuckto

thevesselwall).ThenormalneutrophilcountreflectsonlythecirculatingpopulationandNOTthemarginalone.
§ Normally,thereisabalancebetweenneutrophilsproducedinthebonemarrowandtheonesremovedfromtheblood;therefore,thecountisnormallykeptinanormalrange.
§ Ifthisbalanceisbroken;duetoinfection,necrosis…etc.,therewillbeanincreaseinthenumberintheperipheralblood.Therearetwomechanismsforthisincrease:
• Demarginalization:thecellsmovefromthevesselwalltothecirculationwithoutanactualincreaseinthebonemarrowproduction:thisisseeninthesettingofstress,exerciseandepinephrineinjection.Alltheseconditionshaveincommonanincreaseinepinephrineinthebody,whichincreasestheproductionofcAMPthat,inturn,mobilizesthecellsfromthevesselwalltothecirculation.Thisconditionistermedpseudoneutrohiliaasthereisnoactualincreaseinbonemarrowproduction.
• Anincreaseinthebonemarrowproduction:thisisseenintissuenecrosis,bacterialinfectionandsteroidadministration.Severalmediators(interleukinsandcytokines)affectthebonemarrowdirectlyandincreasetheproliferationandreleaseofneutrophilsintotheblood.

Morphology:• Thereisanincreaseinthenumberofneutrophilsintheperipheralblood• Thereisa“leftshift”,whichmeansinincreaseinthenumberofmore
immaturegranulocyticcellssuchasbandsandmetamyelocytes.• Toxicchanges:thisismostnotablewithseverebacterialsepsisandis
composedofo Coarsecytoplasmicgranuleswhichareabnormalprimarygranuleso Döhlebodies:sky-bluepatchesofexpandedendoplasmicreticulumo Cytoplasmicvacuoles

Differentiationbetweenreactiveandneoplasticgranulocytosisisusuallystraightforward,howeverconfusioncanariseinonesetting,theso-calledLEUKEMOIDREACTION.Leukemoidreactionisareactivegranulocyticproliferationsecondarytobacterialinfectionthatresultsinextremeelevationintheneutrophiliccountandextremeleftshift.Pleaseremember,intypicalbacterialinfectionstheWBCcountrisesupto15000-20000cell/microliter.However,inleukemoidreactiontherisemayreachupto40,000-100,000cell/microliter,whichoverlapswiththenumbersseeninthemoreominousneoplasmChronicMyeloidLeukemia(CML).Thepathogenesisofleukemoidreactioninvolvesoutpouringofhighquantitiesofinterleukinsandcytokines(suchasIL1andTNFa)thatinducesproliferationofgranulocytesinthebonemarrowandsubsequentlyintheperipheralblood.TherearedifferentmethodstodifferentiatebetweentheleukemoidreactionandCML:
1- HistoryofbacterialinfectionfavorsleukemoidreactionoverCML2- Leukocytealkalinephosphatase(theamountofalkalinephosphatasein
theWBCs)islowinCMLwhilenormalorhighinleukemoidreaction3- ThepresenceofBCR/ABLgenefusionisonlypresentinCMLandabsent
inleukemoidreaction4- Leukemoidreactionusuallysubsideswithtreatmentoftheunderlying
infection,whileCMLhaspersistentelevationintheWBCcounts.
o Lymphocytosis:anincreaseinthenumberoflymphocytesintheperipheralbloodabovethereferencerangeforage.
o Causes:viralinfection,chronicbacterialinfectionsuchastuberculosis,brucellosisand,inchildren,pertussis

o Pathophysiology:activationofcellularimmuneresponseinresponsetovirallyinfectedcellsandthesurgeinantibodiesthataccompanythatinfection.Inpertussis:changesinthesurfaceproteinsinthelymphocytesfavortheirmobilizationintothebloodandpreventingtheirgoingbacktothelymphoidtissue.
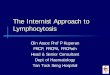
Morphology:Dependsontheetiology-Inlymphocytosiscausedbycertainvirusessuchascoxacki,adenovirusandechovirustherewillbelymphocytosisinwhichlymphocyteshavenormal,maturemorphology(similartonormallymphocytesbutincreasedinnumber)-InEBVinfectiousmononucleosis:reactivelymphocytesarenoted:thesearelymphocyteswithabundantcytoplasmthathavecytoplasmicextensionsthatwraparoundRBCs(pleaserememberthatEBVinfectsBlymphocytesbutthereactivelymphocytesareTcell)-Inpertussis:thelymphocyteshavecleavednucleisimilartotheonesyouseeincasesoffollicularlymphoma***Herearethemajordifferencesbetweenfollicularlymphomaandpertussis -Ageofpresentation:FLisadiseaseofpeopleabovetheageof50,pertussischieflyaffectschildren -Clinicalpresentation:WhoopingcoughinpertussisandlymphadenopathyinFL -ThecellsinFLaremonoclonal(expresseitherkappaorlambdalightchainsbutnotboth,cellsinpertussisarepolyclonal) -BCL2ispositiveinFLandnegativeinreactivefollicularhyperplasia

Figure:peripheralbloodfromapatientwithpertussis,noticelymphocyteswithcleavednuclei(similarfindingcanbeseeninfollicularlymphoma)
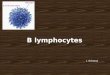
Figure:peripheralbloodfromapatientwithinfectiousmononucleosis(EBV),noticereactivelymphocyteswithabundantcytoplasmandcytoplasmicextensionswrappingaroundRBCs
o Eosinophilia:anincreaseinthenumberofeosinophilsintheperipheralbloodabovereferencerange
o Causes:o Allergicdisorders:asthma,hayfever,urticariao Parasiticinfections:trichinosis,filarial...etc.o Nonparasiticinfections:systemicfungalinfection,scarletfever,
chlamydiao Certainmedicationssuchaspilocarpine,physostigmine,digitalis,p-
aminosalicylicacid,sulfonamides,chlorpromazine,andphenytoin

o Pathophysiology:thecommonfeaturetoallconditionscausingeosinophiliaisthereleaseofIL-5,whichrecruitseosinophilsandincreasestheirproliferationandreleaseformbonemarrow.
o Morphology:normalmorphologybutincreaseinnumber
o Basophilia:anincreaseinthenumberofbasophilsintheperipheralbloodabovereferencerange
o Causes:o Rarelyasareactiveconditionincasesofallergy,postsplenectomyand
inflammatoryboweldiseaseo Associationwithunderlyinghematolymphoidmalignancy,most
commonlychronicmyeloidleukemia.o Morphology:normalinmorphology,justincreaseinnumber

o Monocytosis:anincreaseinthenumberofmonocytesintheperipheralbloodabovereferencerange
o Causes:o Infections:tuberculosis,protozoalinfections,subacutebacterial
endocarditis,syphiliso Recoveryfromneutropeniao Collagenvasculardisorderssuchasmyositis,temporalarteritis,and
polyarteritis.o Certainleukemias
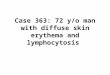
o Morphology:inreactiveconditions,monocyteshavenormalmorphologywithincreaseinnumbers,however,inmalignantconditionssuchasleukemia,thechromatinisfinewithprominentnucleoli.
**Thefirstimagerepresentsreactivemonocytosisandthesecondrepresentsacuteleukemiawithmonocyticdifferentiation(malignantmonocytes).Noteinthefirstimagethatthemonocyteshavenormalmorphologywithfoldednucleiandcoarsechromatinandinthesecondimagethenucleiareroundwithfinechromatinandprominentnucleoli.

• Cytopenia:o Neutropenia:adecreaseinthenumberofneutrophilsinthe
peripheralbloodbelowreferencerange.o Causes
§ Decreaseproduction• Marrowhypoplasiainpatientswhoreceive
chemotherapyorradiationtherapy• Leukemiaorothertumorsreplacingthemarrow• Medications• Certaintypesofneoplasticlymphocyticproliferations
suchaslargegranularleukemia(LGL)§ Increasedperipheraluse
• Autoimmunedestruction• Overwhelmingbacterial,fungalorrickettsiainfection• Splenomegaly
o Labfindings:decreaseneutrophiliccountwithotherfindingsdependingontheunderlyingcause.
o Complications:increaseriskofinfection,especiallybacterialinfections.
o Lymphocytopenia,orsimply,lymphopenia,isadecreaseinthelymphocyticcountintheperipheralbloodbelowthereferencerange.
o Causes:§ ThemostimportantfactorisHIVinfection§ Mediationssuchassteroids,chemotherapyandmedications
forHIVinfection§ Debilitativeconditionssuchasadvancedcancer,renalfailure,
aplasticanemia,autoimmunedisordersandstarvation§ Infections:suchasTB,influenza,typhoidfever§ Abnormallymphaticcirculation:intestinallymphangectasia,
thoracicductobstructiono Labfindings:decreaselymphocyticcountwithotherfindings
dependingontheunderlyingcause.o Complications:increasedriskofinfectionbyawidevarietyof
organismsincludingcandida,virusesandbacteria.§ Opportunisticinfections:aninfectionthatiscausedbya
pathogenthatwouldnotcauseinfectioninnormalconditions,andtakestheopportunityofdisruptedimmunesystemtocausesevere,andsometimes,fataldisease.
o Monocytopenia:adecreaseinthemonocyticcountintheperipheralbloodbelowreferencerange.
o Rareasanisolatedfinding.

o Causes:§ Steroids,monocytesdropinthefirstfewhoursofreceiving
steroids.§ Hairycellleukemia:aformofBcellneoplasm.
o Basopeniaandeosinopeniaarenotacauseofclinicalconcernandwillnotbecoveredinthismanuscript.
• Functionaldisorders:o Neutrophilicfunctionaldisorders:fourdisorderswillbediscussed
§ Chédiak-Higashisyndrome§ Chronicgranulomatousdisease§ Myeloperoxidasedeficiency§ Leukocyteadhesiondeficiency
o Chédiak-Higashisyndrome:autosomalrecessiveaffectingtheLYSTgene(lysosomaltraffickingregulator).Thisgeneisinvolvedinregulationofvesicularsize,trafficking,andintracellularmovement,suchthatvesicularmigrationandreleaseareabnormal.
o Clinically:recurrentpyogenicinfection,albinism(affectsvesiclesthatcontainmelaninpigment,neurologicmanifestationsandphotophobia).Earlydeathduetoinfections.
o Morphology:largecytoplasmicgranulesintheneutrophils,monocytesandlymphocytes.

Noteinthisimagethelargebasophiliccytoplasmicgranulesintheneutrophil,similargranulescanbeseeninlymphocytesandmonocytes.
o Chronicgranulomatousdisease:autosomalrecessive(66%)orX-linked(33%)resultingingeneticdefectaffectingNADPHoxidase,thisenzymecatalyzestheproductionofoxygenradicalspeciesthatplaysavitalroleinkillingmicroorganisms.This,inturn,resultsininabilityofthecellstokillphagocytizedbacteria.
o Clinically:chronic,recurrentbacterialinfectionswithfrequentgranulomatouslesions
o Morphology:thereisnomorphologicchangeinthebloodcells(normalappearance).
o Myeloperoxidasedeficiency:autosomalrecessivedisorder,resultinginqualitativeorquantitativedeficiencyofMPO.
o Mostpeoplewiththisdeficiencyarecompletelyasymptomaticwithincreasedriskofinfection
o Inlessthan5%ofpatientsfungalinfectionsbycandidaspeciescandevelop.
o Theneutrophilslookabsolutelynormal.o Leukocyteadhesionmoleculesdeficiency(LAD):rare
disordercharacterizedbydefectiveexpressionoftheadhesionmoleculesontheneutrophils
o Clinically,thereisanincreaseriskofinfection,neutrophiliaanddelayedseparationoftheumbilicalcord.
o Therearenomorphologicchanges,theneutrophilslookabsolutelynormal.
***Functionaldiseasesofthelymphocyteswillbecoveredintheimmunologycourseandwon’tbediscussedinthismanuscript.
NONEOPLASTICLYMPHNODEDISEASES
Lymphoidtissue(lymphnodes,mucosaassociatedlymphoidtissue,Peyerpatches...etc.)aredynamicorgansthatundergochangesinresponsetoantigenicstimulation.Lymphadenopathyreferstoenlargementofthelymphnodes,readilynotableinthesuperficialgroupssuchascervical,axillaryandinguinallymphnodes.

Thefollowingwillbediscussed1. Acutelymphadenitis2. Follicularandparafollicularhyperplasia.3. Sarcoidosis.
Acutenonspecificlymphadenitis:Occursinthesettingofinfectioninthevicinityofthelymphnodes.Forexample,infectionofthetonsilsorteethabscesscanresultincervicalacutelymphadenitis.Infectionofthebreastcanresultinaxillarylymphadenitis,andinfectionoftheskinofthelowerextremitycausesinguinallymphnodeenlargement.Somebacterialorviralinfectionscanresultingeneralizedlymphadenopathy.Acutemesentericlymphadenitiscanresultasacomplicationtocertainviralinfections,andcanmimicacuteappendicitisclinically.Morphology:
o Enlarged,sometimestender,lymphnodes.o Large,variablysizedfollicleswithnecroticgerminalcentersandneutrophilic
infiltration.
o

Noteintheimagethatthecentercontainsalargenecroticfocusfilledwithdeadtissueandneutrophilicinfiltration.FollicularandparafollicularhyperplasiaRememberthatthelymphnodecontainsareasforB-lymphocytescalledthefolliclesorthecortexandareasforT-lymphocytestypicallyresidebetweenthefolliclesintheparafollicularorparacorticalarea.Thelocationoftheofthehyperplasia(corticalorparacortical)dependsthenatureofthestimulatingantigen,rememberthatBlymphocytesareinvolvedinhumoral(antibodyproducing)immuneresponsewhileTlymphocytesareactivatedbystimulithatneedT-cellmediatedimmuneresponse.FollicularhyperplasiaisdefinedasanincreaseinthenumberandsizeoffolliclessecondarytostimulithatneedBcellresponse
o Causeso Bacterialinfectiono Rheumatoidarthritiso Lupuso EarlystagesofHIVinfectiono Sometimesnoknowncauseisfound
o Morphologyo Numerous,variablysizedsecondaryfollicles(follicleswithgerminal
centers)o Abundanttangible-bodymacrophagesinthegerminalcenterso Frequentmitosiso Smallmantlezones
o

Noteintheimagesthepresenceoffollicleswithdifferentsized.Inthesecondimagenotethepresenceoftigible-bodymacrophagesthatcontaindebrisofapoptoticcells.
o Differentialdiagnosis:themostimportantdifferentialdiagnosisisfollicularlymphoma
o Incontrasttofollicularlymphoma,follicularhyperplasiaischaracterizedby
§ Tingible-bodymacrophages(FLdoesnothavemacrophagesasitiscomposedonlyofneoplasticBcells)
§ Ageofpresentation,follicularhyperplasiatypicallyaffectsyoungpatientswhileFLisaisadiseaseofthepeopleolderthat50yearsofage
§ BCL2(anantiapoptoticprotein)istypicallynegativeinhyperplasiawhilepositiveinFL(seelaterdiscussionoffollicularlymphoma)
ParacorticalhyperplasiaisdefinedasanexpansionoftheparacorticalareasbyTlymphocytesinvariousstagesofstimulationandmaturation.
o Causedusuallybyviralinfection,medicationsandaftervaccinationso Morphology:
o Expansionoftheparacorticalareaswithresultingatrophyofthefollicles
o Theparacorticalareasshowthepresenceofimmunoblasts(activatedTlymphocytesthatarethreetimeslargerthanthenormalTlymphocyteswithfinechromatinandprominentnucleoli.

o

Noteinthefirstimagethepresenceofatrophicfollicleintheupperhalfandanexpandedparacortexinthelowerhalf.Inthesecondimage,notethepresenceoflargecells(immunoblasts,thickarrow),comparethemtothematurelymphocyte(thinarrow).Sarcoidosis:Sarcoidosisisasystemicgranulomatousdiseaseofunknowncausethatmayinvolvemanydifferenttissuesandorgans.Inthevastmajorityofcasesthelungandhilarlymphnodesareinvolved.
o Morphology:thelymphnodesareeffacedbyalargenumberofnonnecrotizinggranulomas

o
Noteinthefirstimagethepresenceofnumerousgranulomas.Inthesecondimage,noticethatthesegranulomasdonotcontainnecrosisandarecomposedofepithelioidhistiocyteswitharimoflymphocytes.