Embed Size (px)
Citation preview

Hemovigilance in Hospital’s Blood Bank
Dr Azita Chegini

History of transfusionsHistory of transfusions
• The first blood transfusions were attempts toThe first blood transfusions were attempts to transfusion humans with animal blood
• The 18th century, it forbadeThe 18 century, it forbade• The 19th century, Henri Leacock and James Blundell pioneered inter human transfusionBlundell pioneered inter human transfusion as a life saving therapy
• After the discovery of the ABO blood groupsAfter the discovery of the ABO blood groups by Landsteiner, blood transfusion became less dangerous but certainly still not without risk


Introducing hemovigilanceIntroducing hemovigilance
• The word “hemovigilance” comes from theThe word hemovigilance comes from the French and is derived from Greek haemameaning blood and the latin vigilans meaningmeaning blood and the latin vigilans meaning watchful
• Pharmacovigilance (1970)• Pharmacovigilance (1970)• 1980‐1990s HIV• In France in1994 was the start of hemovigilance


IHNIHN
• IHN = International Hemovigilance NetworkIHN = International Hemovigilance Network• A set of surveillance procedures covering the whole transfusion chainwhole transfusion chain
• From the collection blood to the follow‐up of i irecipients
• Unexpected or Undesirable effects resulting from transfusion
• Prevent their occurrence or recurrence

Quality systemQuality system
• Biovigilance• Calibration• Control of change• Control of procedures• Documentation• Near missC l f• Control of process
• Competence

Blood safety/ Transfusion safetyBlood safety/ Transfusion safety
SAFE TRANSFUSION
PROCESSPROCESS
SAFE BLOODSAFE BLOOD COMPONENT

HemovigilanceHemovigilance
Total Health Care
Vigilance
Vigilance on medical devices
pharmacovigilance
Hemovigilance
Rene R.Pde veries, Jean claude faber.HemovigilanceTextbook 2012p:6Textbook 2012p:6

An Adverse Eventارتباط بين واکنش جانبی وحادثه
ق ال ق ث وحادثه قريب الوقوعا
Adverse reaction واکنش جانبی
)رخداد(حادثه IncidentIncident
خطاھا وانحراف از استاندارد روشھای
Near‐missحادثه قريب الوقوع
ر ی ھ رو
Rene R.Pde veries, Jean claude faber.Hemovigilance Textbook 2012p7-9

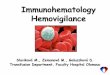
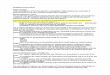
SHOTSHOT

Delayed17%
Acute10% Incorrect
component
Infections1%
p72%

Incorrect componentIncorrect component
Prescription, Sampling &O Sampling &
Request27%
Other2%
Blood Bank28%28%
Collection & Administration
43%43%


Modern Hemovigilance
Recipient Process Donor
AE ER NM ID AE
Recipients Processes / Products DonorsRecipients Processes / Products Donors
collection / analysis of data
continuous improvement of transfusion safety

The local transfusion safety and h i il ihemovigilance committee
Management, HO, prescribers, nurses, regional g p gcoordinator
organization of transfusion
transfusion procedures
organization of transfusioninformation
traceability
transfusion reactions
training
traceability
16

آيا حادثه بدليل کيفيت فرآورده نوع واکنش است؟
آيا حادثه بدليل اختلالی است؟ خون تزريق توسطدرروند پيشگيری قابل قابل پيشگيری توسطدرروند تزريق خون است؟است؟
ھموليزايمونولوژيک به دنبال ABOناسازگاری
-خيرخير
ھموليزايمونولوژيک به دنبال ديگر آلوآنتی باديھا
-بلهخير
ھموليز بدليل نگھداری ناصحيح
روند تزريق خون بلهخيرنظارت بر يخچال بانک خون وزنجيره سرما وحمل ونقل
عفونت ھای باکتریال قابل انتقال ازراه خون
احتمالا بدليل عدم ارزيابی بلهنکات فنی کيسه خون
وفرآورده قبل از تزريق است
ضدعفونی پوست اھداکننده-استفاده از کيسه جانبی -
عفونت ھای ويرال قابل انتقال ازراه خون
انتخاب اھداکننده سالم خيربلهآزمايشات خون اھداکننده
انتقال قابل انگل ھای سالخيربلهعفونت اھداکننده نتخاب عفونت ھای انگلی قابل انتقال...)مالاريا و(ازراه خون
نتخاب اھداکننده سالم خيربلهآزمايشات خون اھداکننده

آيا حادثه بدليل کيفيت فرآورده نوع واکنش است؟
آيا حادثه بدليل اختلالی درروند است؟ خون تزريق
قابل پيشگيری توسطتزريق خون است؟است؟
غيرقابل پيش بينی وغيرقابل خيرخيرآنافيلاکسی يا حساسيت شديداجتناباجتناب
پورپورای پس از ترانسفيوژنPPT
غيرقابل پيش بينی وغيرقابل خيرخيرباجتناب ج
صدمه حادريه بدنبال تزريق TRALIخون
از FFPممکن است با گرفتن خيربلهاھداکنندگان مردکاھش يابد
بيماری پيوندعليه ميزبانGVHD
بلهبلهبدليل انتخاب نامناسب محصول خونی ياعدم تشخيص بيماری
استفاده از محصولات اشعه ديده برای بيماران درمعرض خطر
افزايش بارقلبی بدنبال تزريق TACOخون
بلهخيربدليل عدم تشخيص بيماردرمعرض خطر
پرھيز ازتزريق حجم زيادخون
واکنش تب زای غيرھموليتيکFNHTR
شيوع آن ممکن است با فرآورده خيربلهکم لکوسيت کاھش يابد

EFSAFSSaPS
Medical &nursing team
R i lMedical &
i t RegionalcoordinatorTSHC Haemovigilance
officers (HO)
nursing team
officers (HO)
19

Pick up Blood and other products


Blood group serology‐compatibilityBlood group serology compatibility
• National guidelines for pre‐transfusion testingg p g• Protocols for ABO‐Rh• Ab‐screening• Group and sreen• Crossmatching• Sample validity• Selection of RBC and non_RBC productsE f i• Emergency transfusion
• Quality control

RecommendationsRecommendations
• PregnancyPregnancy• Selection of blood & products in neonatal and infantsinfants
• Autologous transfusion

Guidance on identificationGuidance on identification
• Standardization of patient identificationStandardization of patient identification• Standard Blood sampling• Sample collection• Sample collection• LabelingC tibilit t t• Compatibility tests
• Records• Ensure quality and safety in blood group serology and compatibility

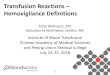
Patient IdentificationPatient Identification
• Must confirmMust confirm recipient’s ID from bracelet ON the patient– Full patient name and hospital numberN f h i i– Name of physician
http://www.usatoday.com/tech/news/techinnovations/2006‐07‐17‐chips‐everywhere_x.htm


Sample IdentificationSample Identification
• The sample should also phave the full patient name, hospital number, and physicianand physician
• Date and time of collection,collection, phlebotomist’s initials
• All of this should be on the request form and the sample

Specimen TubesSpecimen Tubes
Pink Top ‐ EDTA Red Top – no additives

samplingsampling


Aim of transfusion laboratoryAim of transfusion laboratory
• Right testRight test• Right sample
i h l• Right results

Quality assuranceQuality assurance
• PersonnelPersonnel• Records• Reagents• Equipment• Storage requirements• TransportTransport• Computer validation

Incorrect blood component transfusedIncorrect blood component transfused
• IBCTIBCT
l i f d b• Analysis of data by category• Transfused with reaction• Transfused without reaction• Component not transfused(near miss)Component not transfused(near miss)

Site of primary error
• Blood unit (wrong donor group label wrongBlood unit (wrong donor group label, wrong recipient identification on unit)
• Patient sample(wrong name of tube including• Patient sample(wrong name of tube, including wrong patient collected)T f i (ABO i ibl f i• Transfusion(ABO‐incompatible transfusion, wrong patient but ABO‐compatible, wrong
d l l l )product type plasma versus platelet)


Errors associated with blood group lserology
• Technical failure in testingTechnical failure in testing• Inadequate procedures
i id tifi ti f ti t d lmisidentification of patient or donor sampleTranscription errorsMisinterpretation of results
• Combination of factors with the original error being perpetuated or compounded by the lack of adequate checking procedures



• The first step in the process of obtaining the sample is the request f t tifor testing.
• The laboratory must make available a test request form that specifies all the information that will be needed for proper handling and reportingand reporting.
• Essential information for the test request form includes:• • patient identification;• • tests requested;• • tests requested;• • time and date of the sample collection;• • source of the sample, when appropriate;• • clinical data when indicated;• • clinical data, when indicated;• • contact information for the health care provider requesting the
test.

Sample collection requirementsSample collection requirements• Sample collection and preservation will vary, depending on the test and the type of sample to be
collected. The laboratory must carefully define a sample collection process for all tests it performs. The following should be considered when preparing instructions:The following should be considered when preparing instructions:
• • Patient preparation—Some tests require that the patient be fasting. There may also be special timing issues for tests such as blood glucose, drug levels, and hormone tests.
• • Patient identification—The person collecting the sample must accurately identify the patient. This might be done by questioning the patient, by questioning an accompanying family member, or by the use of an identifying wrist band or other deviceby the use of an identifying wrist band or other device.
• • Type of sample required—Blood tests might require serum, plasma, or whole blood. Other tests might require urine or saliva. Microbiology testing deals with a variety of sample types, so specific information as to what is required for the test is needed.
• • Type of container—The container for the sample is often very important, as it will affect volume d d d ddi i h i l d i If h i dand any needed additives such as anti‐coagulants and preservatives. If the container does not
control volume, for example as with Vacutainer® tubes, this will need to be clearly specified. Some microbiology samples will require specific transport media to preserve microorganisms.
• • Sample labeling—All requirements for labeling of the sample at the time of collection will need to be explained in detail in the instructions for collection.
• Special handling—Some samples may require special handling, such as immediate refrigeration, protection from light, or prompt delivery to the laboratory. Any important safety precautions should be explained.

Samplel b llabeling
• Each sample should be clearly labeled with:ac sa p e s ou d be c ea y abe ed t :• • the patient’s first and last name;• • a unique identification number – this might be a unique identification number this might be a hospital number or a
• number assigned by the laboratory;g y y;• Sample Management • • the test that has been requested;q ;• • the time and date of collection;• • the initials of the person collecting the sample. the initials of the person collecting the sample.


potential outcomes of collection potential outcomes of collection errors
• Proper sample collection is an important element for good laboratory practice.
• Improper collection of samples can lead to poor outcomes,Improper collection of samples can lead to poor outcomes, such as:
• • delays in reporting test results• • unnecessary re draws/re tests• • unnecessary re‐draws/re‐tests• • decreased customer satisfaction• • increased costs• • incorrect diagnosis / treatment• • injury• • death death.

• The laboratory should keep a register (log) ofThe laboratory should keep a register (log) of all incoming samples. A master register may be kept, or each specialty laboratory may keep its own sample register.
• Assign the sample a laboratory identification number – write the number on the sample and the requisition form. If computers are
d f h i f i iused for reports, enter the information into the computer.











Overview of Sample ManagementOverview of Sample Management
• Sample management is a part of process control, Sa p e a age e t s a pa t o p ocess co t o ,one of the essentials of a quality management system.
• The quality of the work a laboratory produces is only as good as the quality of the samples it uses f t tifor testing.
• The laboratory must be proactive in ensuring that the samples it receives meet all of thethe samples it receives meet all of the requirements needed to produce accurate test results.

Samplemanagementmanagementcomponents
• Written policies for sample management must beWritten policies for sample management must be established and reflected in the Laboratory Handbook. Components to be addressed include:
• • information needed on requisitions or forms• • handling urgent requestsg g q• • collection, labeling, preservation and transport• • safety practices (leaking or broken containers, y p ( g ,contaminated forms, other biohazards)
• • evaluating, processing, and tracking samplesg p g g p• • storage, retention, and disposal.

Getting the historyGetting the history
• Look at recipient’s records for any prior unexpected antibodiesp
• Previous transfusion reactions


Error managementError management
• Up to half of all serious transfusion reactionsUp to half of all serious transfusion reactions are preventable
• With appropriate measurements• With appropriate measurements• Electronic system( barcode)• Automated laboratory equipment• Process control• HTC

AUDIT IN TEHRAN’S HOSPITALAUDIT IN TEHRAN S HOSPITAL
Improvementblood bank
88 9%Refrigerator 88.9%Refrigerator
61%Freezer
50%Shaker incubator
61% Calibration

Audit in hospital blood banksAudit in hospital blood banks
13851394
Cross match 44.4%100%
Ab‐screening 5.5%22.2%

Percentage changeBlood grouping
44.4%Slide to tube test
11.1%Tube to slide test
27.8%Tube to tube (without change)
16.7%Slide to slide (without change) ( g )

Thank you for your attentionThank you for your attention