Embed Size (px)
Citation preview

6/23/14
1
Hemostasis and thrombosis in the ICU Robert Goggs Lecturer, Emergency & Critical Care Cornell University, College of Veterinary Medicine
IMTP • Immune-mediated process results in
premature destruction of thrombocytes
• IgG autoantibodies – Platelets or megakaryocytes – GpIIb/IIIa
• Extravascular removal – Mononuclear phagocytic system – FcR or complement mediated phagocytosis
• Antibody-mediated thrombocytopathy
A model of canine IMTP • LeVine DN et al. JVIM
• Repeated injection of 2F9 – Murine IgG2a monoclonal antibody to GPIIb
• All dogs developed thrombocytopenia within 2h – Median dose 63µg/kg (range 50.0-166.6µg/kg) – Plt counts 11-28 x103/µL – Platelet count remained <40 x103/µL for 24h – All dogs developed clinical bleeding
• No systemic inflammation generated

6/23/14
2
• 58 dogs with thrombocytopenia
• Dogs with <20x103/µL
• 36/55 diagnostic BM aspirates had <20x103/µL
• No definitive diagnosis made via BM evaluation
• BM evaluation unlikely to provide specific diagnostic or prognostic information in severe thrombocytopenia
• <24h post-admission, d1 after plt >40, then d4, d7, d14
• All dogs had hypocoagulable TEG tracings on admission
• All dogs developed hypercoagulable TEG tracings
• 24 dogs with primary IMTP
• All Tx with prednisone 1.5-2mg/kg
• 12 dogs treated with vincristine 0.02mg/kg
• Vinc Tx dogs had sig. faster plt recovery times – 4.9d ± 1.1 Vs 6.8d ± 4.5
• Vinc Tx sig. reduced duration of hospitalisation – 5.4d ± 0.3 Vs 7.3d ± 0.5
• No adverse effects noted

6/23/14
3
• Prospective RCT of 18 client-owned dogs with IMTP
• Median platelet count recovery time (p=0.018) – hIVIG group 3.5d (2-7) – Placebo group 7.5d (3-12)
• Median hospitalisation (p=0.027) – hIVIG group 4d (2-8) – Placebo group 8d (4-12)
• No significant difference in costs between groups
• No immediate or delayed adverse reactions identified
• 20 dogs with IMTP, Plt <16x103/µL, all Tx with steroids
• Randomized to: – hIVIG 0.5 g/kg OR – Vincristine 0.02 mg/kg
• No sig. difference between groups at discharge, 6m or 1y
• No adverse effects reported
Platelet products • Platelet rich plasma
• Platelet concentrate
• DMSO frozen platelets
• (Lyophilized platelets)
1580 AJVR, Vol 69, No. 12, December 2008
Platelets are anucleate, discoid-shaped, cytoplasmic fragments that play an essential role in primary hemo-
stasis, the initiation of a platelet plug, and the preservation of vascular integrity. Alterations in platelet number as well as platelet function have profound implications for the maintenance of hemostasis and vascular health. Throm-bocytopenia, a common finding in critically ill dogs,1,2 is often associated with spontaneous bleeding in dogs3 and in humans.4 Moreover, progressive development of throm-bocytopenia has been associated with a poorer outcome in human intensive care unit patients.5–7
In human medicine, platelet-rich products are available for the treatment of patients with thrombocy-topenia. The most commonly used product is a fresh PC stored at room temperature (20° to 24°C) with continu-ous, gentle agitation for up to 5 days. Fresh PC can be obtained from whole blood by serial centrifugation or by platelet apheresis. The minimum acceptable platelet count in a PC is 3.0 X 1011 platelets/300-mL bag, as de-fined by the American Association of Blood Banks.8
Assessment of a dimethyl sulfoxide–stabilized frozen canine platelet concentrate
Julien Guillaumin, Doct. Vet.; Karl E. Jandrey, DVM; Jeffrey W. Norris, PhD; Fern Tablin, VMD, PhD
Objective—To assess platelet count, mean platelet volume (MPV), metabolic characteris-tics, and platelet function in a dimethyl sulfoxide (DMSO)–stabilized canine frozen platelet concentrate (PC).Sample Population—11 units of a commercial frozen PC in 6% DMSO and fresh platelet-rich plasma from 6 healthy control dogs.Procedures—PCs were thawed, and the following data were collected: thaw time, platelet count, MPV, pH, PCO2, and PO2 and HCO3
–, glucose, and lactate content. Phosphatidylserine translocation was determined by use of flow cytometry. Fresh platelet-rich plasma from healthy dogs served as a source of control platelets for flow cytometric analysis.Results—At thaw, the platelet count in the frozen PC ranged from 243,000 to 742,000 platelets/ L. Median platelet count of paired samples was 680,000 platelets/ L and de-creased significantly to 509,000 platelets/ L at 2 hours after thaw. Median MPV at thaw was 11.15 femtoliters and was stable after 2 hours. Compared with fresh platelets, frozen PC had increased amounts of phosphatidylserine in the outer leaflet of the platelet mem-brane in the resting (ie, not treated with thrombin) state (19% vs 99%, respectively) and alterations in cellular morphology, all of which were consistent with platelet activation.Conclusions and Clinical Relevance—Results of this in vitro study indicated that there was a decrease in platelet quantity and function as well as an increase in platelet activation during the freeze-and-thaw process in DMSO-stabilized canine frozen PC. In vivo effects on PC remain to be determined. (Am J Vet Res 2008;69:1580–1586)
Cryopreservation, most commonly by use of DMSO as a cryopreservative, has also been used for the storage of human PCs.9 These DMSO-stabilized frozen PCs have a longer shelf life and are easier to ship, compared with stored fresh PC.9,10 Platelets in 6% DMSO have been stored at –80°C for up to 2 years.11,12 However, DMSO cryopreservation results in a substantial loss of platelets,13 altered platelet morphology, decreased response to agonists as evalu-ated by aggregation, and reduced clinical efficacy, compared with fresh platelets.10,14,15
In veterinary medicine, a frozen PC is commer-cially available for dogs,a which is prepared from a single donor by use of apheresis technologyb and cryopreserved with 6% DMSO. No published infor-mation exists regarding platelet function for this specific product. Limited information exists in the peer-reviewed veterinary literature regarding canine DMSO-stabilized frozen PC.16,17,c These studies did
Received December 22, 2007.Accepted March 21, 2008.From the Veterinary Medical Teaching Hospital (Guillaumin) and
the Departments of Surgical & Radiological Sciences (Jandrey) and Anatomy, Physiology & Cell Biology (Norris, Tablin), School of Vet-erinary Medicine, University of California, Davis, CA 95616.
This work was supported by the Center for Companion Animal Health, School of Veterinary Medicine, University of California, Davis.
The authors thank Dr. Michael Kent and Naomi Walker for technical assistance.
Address correspondence to Dr. Guillaumin.
ABBREVIATIONS
DMSO Dimethyl sulfoxideFITC Fluorescein isothiocyanateFTR Freeze-thaw recoveryMFI Mean fluorescence intensityMPV Mean platelet volumePC Platelet concentrateRFU Relative fluorescence unitsT0 Time zero
Original Study
Analysis of a commercial dimethyl-sulfoxide-stabilized frozen canine platelet concentrateby turbidimetric aggregometryJulien Guillaumin, Dr vet, DACVECC; Karl E. Jandrey, DVM, DACVECC; Jeffrey W. Norris, PhDand Fern Tablin, VMD, PhD
Abstract
Objectives – To assess platelet function of a commercial dimethyl-sulfoxide (DMSO)-stabilized frozen plateletconcentrate (PC) using turbidimetric aggregometry.Design – In vitro analysis.Setting – Research laboratory in a school of veterinary medicine.Animals – Five units of frozen PC in 6% DMSO were studied. Fresh platelet-rich plasma (PRP), with andwithout 6% DMSO, from 6 healthy dogs were used as controls.Interventions – Turbidimetric platelet aggregation was measured after initiation of platelet aggregation byaddition of adenosine diphosphate (ADP), collagen, or thrombin at concentrations of 30 mM, 20mg/mL, and0.5 U/mL, respectively. Measures were performed at thaw and repeated 2 hours after thaw for the frozen PC.Measurements and Main Results – Compared with PRP, the frozen PC showed decreased aggregation inresponse to thrombin (amplitude of 84% versus 25%, P 5 0.01), and collagen (amplitude of 13% versus 3%,P 5 0.05) but not ADP (6.5% versus 18%, P 5 0.2). Compared with frozen PC at thaw, the frozen PC at 2 hoursafter thaw showed decreased aggregation in response to thrombin, collagen, and ADP (Po0.05). There was nodifference in aggregation between PRP in 6% DMSO and frozen PC.Conclusions – These in vitro data suggest there is a decrease in platelet response to agonists associated withthe freeze-thaw process in the commercially available 6% DMSO canine frozen PC.
(J Vet Emerg Crit Care 2010; 20(6): 571–577) doi: 10.1111/j.1476-4431.2010.00580.x
Keywords: coagulation, critical care, fluid therapy, hemostasis, platelet function, transfusion medicine
Introduction
Hemostasis can be divided into 3 inter-related steps: (1)primary hemostasis, the initiation and formation of aplatelet plug, (2) secondary hemostasis, the propaga-tion of thrombin formation for ultimate clot stabiliza-
tion with cross-linked fibrin, and (3) fibrinolysis, thedissolution of the clot and the restoration of vascularintegrity.
Primary hemostasis can be affected by alterations inplatelet number as well as platelet function. Thrombo-cytopenia, a common finding in critically ill dogs,1,2 isoften associated with spontaneous bleeding in dogs3
and in humans.4 Moreover, progressive development ofthrombocytopenia has been associated with a pooreroutcome in critically ill human patients.5–7
Severe thrombocytopenia associated with life-threat-ening bleeding is usually treated with platelet products.The standard of care in human medicine is the trans-fusion of platelet concentrate (PC), which is stored forup to 5 days at room temperature (20–241C) with con-tinuous, gentle agitation. PC units can be obtained fromwhole blood by serial centrifugation or with pheresistechnology. The minimum acceptable platelet count in a
This work has been supported by the Center for Companion AnimalHealth, School of Veterinary Medicine, University of California, Davis.
Authors declare no conflict of interest.
Presented in part at the 14th International Veterinary Emergency and Crit-ical Care Symposium, Phoenix, Arizona, September 2008.
Address correspondence and reprint requests toDr. Guillaumin, Department of Veterinary Clinical Science, The Ohio StateUniversity College of Veterinary Medicine, Columbus, OH 43210, USA.Email: [email protected] April 16, 2009; Accepted August 23, 2010.
From the Departments of Surgical & Radiological Sciences (Guillaumin,Jandrey) and Anatomy, Physiology & Cell Biology (Norris, Fern), Univer-sity of California–Davis, Davis, CA 95616.
Journal of Veterinary Emergencyand Critical Care 20(6) 2010, pp 571–577doi:10.1111/j.1476-4431.2010.00580.x
& Veterinary Emergency and Critical Care Society 2010 571
Original Study Journal of Veterinary Emergency and Critical Care 22(1) 2012, pp 116–125doi: 10.1111/j.1476-4431.2011.00710.x
Use of fresh platelet concentrate orlyophilized platelets in thrombocytopenicdogs with clinical signs of hemorrhage: apreliminary trial in 37 dogsElizabeth B. Davidow, DVM, DACVECC; Benjamin Brainard, DVM, DACVA, DACVECC;Linda G. Martin, DVM, MS, DACVECC; Matthew W. Beal, DVM, DACVECC; Arthur Bode, PhD;Michael J. Ford, PhD; Noel Ramsey, BS, LVT, LATG; Alicia Fagella, DVM, DACVECCand Ari Jutkowitz, VMD, DACVECC
Abstract
Objective – To examine the safety and feasibility of using lyophilized platelets (LYO) and fresh platelet concen-trate (FRESH) in bleeding thrombocytopenic dogs.Design – Preliminary prospective randomized clinical trial.Setting – Two private referral centers and 3 university teaching hospitals.Animals – Thirty-seven dogs with a complaint of hemorrhage associated with thrombocytopenia (platelet count<70 × 109/L [70,000/!L], a hematocrit >15%, and that had received neither vincristine nor platelet-containingtransfusions within 72 h of enrollment were studied.Interventions – Animals were randomized to receive LYO or FRESH, dosed according to weight. Physical exam-ination, complete blood counts, and coagulation testing (prothrombin time and activated partial thromboplastintime) were performed at enrollment. Physical examinations were also performed immediately post transfusion,and at 1 and 24 h after transfusion. Complete blood counts were repeated immediately post transfusion and at24 h. Collected data included bleeding score (BLS), response to transfusion, adverse reactions, hospitalizationtime, need for additional transfusions, survival to discharge, and 28-d survival.Measurements and Main Results – Twenty-two dogs received LYO and 15 received FRESH. There was nodifference between groups in age, weight, BLS, platelet count, white blood cell count, hematocrit, or presenceof melena. There was no difference between groups in transfusion reaction rates, the need for additionaltransfusions, 24-h BLS, hospitalization time, survival to discharge, or 28-d survival.Conclusions – Transfusion of LYO was feasible and associated with a low transfusion reaction rate in thislimited study of thrombocytopenic canine patients presenting with mild-to-severe hemorrhage. LYO were easyto use and provided storage advantages over FRESH. Further study of this product, including examination ofefficacy and platelet life span, is warranted.
(J Vet Emerg Crit Care 2012; 22(1): 116–125) doi: 10.1111/j.1476-4431.2011.00710.x
Keywords: bleeding disorders, immune-mediated thrombocytopenia, platelet storage, primary hemostasis,transfusions
From the Animal Critical Care and Emergency Services, Seattle, WA 98125(Davidow, Ford); Section of Critical Care, College of Veterinary Medicine,University of Georgia, Athens, Georgia 30606 (Brainard); Departmentof Clinical Sciences, College of Veterinary Medicine, Auburn University,Auburn, AL 36849 (Martin); Michigan State University, East Lansing, MI48824 (Beal, Jutkowitz); Department of Pathology, East Carolina Univer-sity, Greenville, NC 27858 (Bode); Animal Blood Resources International,Stockbridge, MI 49285 (Ramsey); Dove Lewis Emergency Animal Hospital,Portland, OR 97209 (Fagella).
Fresh and Lyophilized Platelets products evaluated in the study were pro-vided by Animal Blood Resources International. Dr. Brainard is an Assistant
Abbreviations
aPTT activated partial thromboplastin timeBLS bleeding score
Editor for the journal, but did not participate in the peer-review process otherthan as an author. Presented in part at ACVIM Forum 2010 in Anaheim, CA.
Address correspondence and reprint requests toDr. Elizabeth Davidow, Animal Critical Care and Emergency Services, 11536Lake City Way NE, Seattle, WA 98125. USAEmail: [email protected] March 04, 2011; Accepted November 29, 2011.
116 C⃝ Veterinary Emergency and Critical Care Society 2012

6/23/14
4
Any other options?
• Ralph A et al. JVECC 2013; 23(S1):S16
• 10 non-coagulopathic anemic, bleeding IMTP dogs
• 10-30mg/kg/hr ACA / NaCl placebo until Plt >30x103/µL
• No sig. difference in median pRBCs or Tx time
TAC / ACOT-S
Severe trauma
ACOT-S
SAC
No coagulopathy
Death
Recovery
Death
Death
Recovery
Recovery

6/23/14
5
Noel P et al. Semin Hematol
2013; 50:259-269
ACOT-S in dogs?
Original Study Journal of Veterinary Emergency and Critical Care 23(4) 2013, pp 395–401doi: 10.1111/vec.12073
Hypoperfusion and acute traumaticcoagulopathy in severely traumatizedcanine patientsAmanda L. Abelson, DVM, DACVECC; Therese E. O’Toole, DVM, DACVIM, DACVECC; AndreaJohnston, DVM; Meghan Respess, DVM and Armelle M. de Laforcade, DVM, DACVECC
Abstract
Objective – To determine the incidence of acute traumatic coagulopathy in dogs suffering severe trauma andto investigate the association of markers of hypoperfusion with coagulation abnormalities.Design – A prospective observational study performed June, 2009 to February, 2011.Setting – A university teaching hospital.Animals – Thirty client-owned dogs weighing >5 kilograms that were presented to the Tuft’s CummingsSchool of Veterinary Medicine following severe trauma as defined by an animal trauma triage score (ATT) ≥5and having received no resuscitation with IV fluids or blood products prior to blood sampling.Interventions – None.Measurements and Main Results – Prior to resuscitation, data obtained at the time of admission to the emer-gency service included HCT, platelet count, lactate concentration, pH, base excess, thromboelastrogram (TEG),prothrombin time, activated partial thromboplastin time, fibrinogen level, and protein C activity. Rectal tem-perature and ATT were recorded for all dogs. Neither HCT nor platelet count was significantly decreased in anyof the dogs. Based on G values as measured by TEG, 10/30 dogs (33%) showed evidence of hypercoagulability.Hypocoagulability as determined by prothrombin time, activated partial thromboplastin time, or TEG was notshown in any of the 30 dogs.Conclusion – Dogs with severe trauma may experience hypercoagulability that is unrelated to fluid resuscitationor transfusion therapy. Future studies are warranted to better characterize coagulation changes in dogs withsevere trauma, particularly in relationship to fluid therapies and/or hemorrhage.
(J Vet Emerg Crit Care 2013; 23(4): 395–401) doi: 10.1111/vec.12073
Keywords: clotting times, hemostasis, thromboelastography, trauma
Introduction
Coagulopathyandhemorrhage occur commonly in hu-man traumapatients. Coagulationabnormalities havehistorically been attributed to coagulation factor con-sumption and simultaneoushemodilution from IV fluid
From the Department of Clinical Sciences, Cummings School of VeterinaryMedicine, Tufts University, North Grafton, MA 01536 (Abelson, Respess, deLaforcade, O’Toole); Department of Clinical Sciences, School of VeterinaryMedicine, Cornell University, Ithaca, NY 14850 (Johnston).
This work was conducted at the Cummings School of Veterinary Medicineat Tufts University.
This study was funded by a private grant.
The authors declare no conflict of interest.
Dr. Abelson’s current address is Department of Clinical Sciences, CummingsSchool of Veterinary Medicine, Tufts University, North Grafton, MA.
Address correspondence and reprint requests toDr. Amanda L. Abelson, Department of Clinical Sciences, Cummings Schoolof Veterinary Medicine, Tufts University, North Grafton, MA, USA.Email: [email protected] March 1, 2012; Accepted June 26, 2013.
Abbreviations
aPTT activated partial thromboplastin timeATC acute traumatic coagulopathyATT animal trauma triage scoreBE base excessCI coagulation indexED emergency departmentPT prothrombin timeTCSVM Tuft’s Cumming School of Veterinary
MedicineTEG thromboelastogram
and blood product administration. The etiology oftrauma-induced coagulopathy is likely multifactoral.Systemic acidosis and hypothermia are believed to con-tribute to coagulation derangements with mortality rates
C⃝ Veterinary Emergency and Critical Care Society 2013 395
TAC in dogs?
Original Study Journal of Veterinary Emergency and Critical Care 24(1) 2014, pp 93–104doi: 10.1111/vec.12141
Prospective multicenter evaluation ofcoagulation abnormalities in dogs followingsevere acute traumaMarie K. Holowaychuk, DVM, DACVECC; Rita M. Hanel, DVM, DACVIM, DACVECC; R. DarrenWood, DVM, DVSc, DACVP; Lindsey Rogers, DVM; Karen O’Keefe, DVM and Gabrielle Monteith,BSc (Hons)
Abstract
Objectives – To describe coagulation abnormalities in dogs following severe acute trauma and to evaluate therelationship between coagulation, clinical, and laboratory variables, and disease and injury severity, as well asthe ability of coagulation variables to predict the presence of body cavity hemorrhage (BCH), necessity of bloodproduct administration, and outcome.Design – Prospective, multicenter, observational study.Setting – Two university teaching hospitals.Animals – Forty client-owned dogs sustaining severe blunt or penetrating trauma.Interventions – Blood samples were collected within 12 hours of the traumatic incident for measurement ofblood gases, lactate concentration, platelet count, activated clotting time, prothrombin time, activated partialthromboplastin time (aPTT), fibrinogen concentration, antithrombin activity, D-dimer concentration, protein Cactivity, plasmin inhibition, plasminogen activity, and kaolin-activated thomboelastography.Results – Decreased platelet count was a risk factor for the presence of BCH (P = 0.006) and decreasedplatelet count (P < 0.001), protein C activity (P = 0.001), angle (!) (P = 0.001), maximum amplitude (MA)(P < 0.001), and clot strength (G) (P = 0.002) were risk factors for blood product administration. Nonsurvivingdogs were hypocoagulable with prolonged aPTT (P = 0.008), decreased plasmin inhibition (P = 0.033), decreased! (P = 0.021), and decreased MA (P = 0.038) compared to surviving dogs. Multivariate analysis accounting fordisease severity showed that prolonged aPTT (P = 0.004, OR = 1.74) was the strongest predictor of nonsurvival.Prolonged aPTT was positively correlated with APPLE-fast score (P < 0.001, r2 = 0.35), lactate concentration(P < 0.001, r2 = 0.35), and negative base excess (P = 0.001, r2 = 0.27). Acute traumatic coagulopathy, as definedby 2 or more abnormal coagulation tests, was diagnosed in 15% of dogs at hospital admission and was morecommon in dogs with increased disease severity (P = 0.002), decreased systolic blood pressure (P = 0.002), andincreased lactate concentration (P = 0.011).Conclusions – In dogs with severe traumatic injuries and hypoperfusion, measurement of thromboelastographyand aPTT should be considered to support clinical assessments in predicting the need for blood productadministration and nonsurvival.
(J Vet Emerg Crit Care 2014; 24(1): 93–104) doi: 10.1111/vec.12141
Keywords: hemostasis, hemorrhage, hypotension, lactate, perfusion, thromboelastography
From the Department of Clinical Studies, Ontario Veterinary College, Uni-versity of Guelph, Guelph, ON (Holowaychuk, Rogers, O’Keefe, Monteith);Department of Clinical Sciences, College of Veterinary Medicine, North Car-olina State University, Raleigh, NC (Hanel); and Department of Pathobiol-ogy, Ontario Veterinary College, University of Guelph, Guelph, ON (Wood).
The Ontario Veterinary College Pet Trust Fund provided funding for thisstudy.
This study was presented as an abstract at the 17th International VeterinaryEmergency and Critical Care Society Meeting in Nashville in September 2011.
The authors declare no conflict of interests.
Address correspondence and reprint requests toDr. Marie Holowaychuk, Department of Clinical Studies, Ontario Veterinary
Abbreviations
ACT activated clotting timeaPTT activated partial thromboplastin timeAT antithrombinATC acute traumatic coagulopathyBCH body cavity hemorrhage
College, University of Guelph, 50 Stone Road East, Guelph, ON N1G 2W1,Canada. Email: [email protected] June 18, 2012; Accepted November 14, 2013.
C⃝ Veterinary Emergency and Critical Care Society 2014 93

6/23/14
6
Platelet dysfunction in trauma
• Lynch A et al. JVECC 2013; 23(S1):S8-9
• 5 dogs bled to 80% and 60% normal blood volume
• Sig. changes in PCV/TS, PT, aPTT, Fg, TEG R & MA
• Plt count did not sig. alter
• Sig. decrease in AA- and ADP-induced WB aggregometry AUC
Hyperfibrinolysis in trauma
CRITICAL CARE
Prevalence and impact of abnormal ROTEMw assays in severeblunt trauma: results of the ‘Diagnosis and Treatmentof Trauma-Induced Coagulopathy (DIA-TRE-TIC) study’H. Tauber 1, P. Innerhofer 1*, R. Breitkopf 1, I. Westermann 1, R. Beer 2, R. El Attal 3, A. Strasak 4
and M. Mittermayr 1
1 Clinic of Anaesthesiology and Intensive Care Medicine, 2 Clinic of Neurology, 3 Clinic of Trauma Surgery and Sports Medicine and4 Department of Medical Statistics, Informatics and Health Economics, Innsbruck Medical University, Anichstrasse 35, 6020 Innsbruck,Austria
* Corresponding author. E-mail: [email protected]
Editor’s key points
† In a cohort study of blunttrauma, impact ofabnormal ROTEMw assayswas evaluated.
† At defined thresholds forROTEMw, significantdifferences in mortalitywere seen.
† Maintaining fibrinpolymerization andtreating hyperfibrinolysismay improve outcome intrauma patients.
† This study adds to theevidence that ROTEMw
assays are useful inmanaging traumapatients.
Background. ROTEMw/TEGw (rotational thromboelastometry) assays appear to be useful forthe treatment of bleeding trauma patients. However, data on the prevalence and impact ofabnormal ROTEMw assays are scarce.
Methods. This is a prospective cohort study of blunt trauma patients (Injury Severity Score≥15 or Glasgow Coma Score ≤14) admitted to Innsbruck Medical University Hospitalbetween July 2005 and July 2008. Standard coagulation tests, antithrombin (AT),prothrombin fragments (F1+2), thrombin–antithrombin complex (TAT), and ROTEMw
assays were measured after admission. Data on 334 patients remained for final analysis.
Results. ROTEMw parameters correlated with standard coagulation tests (all Spearman r.0.5),and significant differences in mortality were detected for defined ROTEMw thresholds [FIBTEM7 mm (21% vs 9%, P¼0.006), EXTEM MCF (maximum clot firmness) 45 mm (25.4% vs 9.4%,P¼0.001)]. EXTEM MCF was independently associated with early mortality [odds ratio (OR)0.94, 95% confidence interval (CI) 0.9–0.99] and MCF FIBTEM with need for red blood celltransfusion (OR 0.92, 95% CI 0.87–0.98). In polytrauma patients with or without head injury(n¼274), the prevalence of low fibrinogen concentrations, impaired fibrin polymerization,and reduced clot firmness was 26%, 30%, and 22%, respectively, and thus higher than theprolonged international normalized ratio (14%). Hyperfibrinolysis increased fatality rates andoccurred as frequently in isolated brain injury (n¼60) as in polytrauma (n¼274) (5%, 95% CI1.04–13.92 vs 7.3%, 95% CI 4.52–11.05). All patients showed elevated F1+2 and TAT andlow AT levels, indicating increased thrombin formation.
Conclusions. Our data enlarge the body of evidence showing that ROTEMw assays are useful intrauma patients. Treatment concepts should focus on maintaining fibrin polymerization andtreating hyperfibrinolysis.
Keywords: blood, coagulation; measurement technique, thrombelastograph,thrombelastometry, trauma
Accepted for publication: 26 April 2011
Guidelines for managing trauma-induced coagulopathy (TIC)recommend administration of fresh-frozen plasma (FFP)according to measurements of prothrombin time (PT) andactivated partial thrombin time, although these tests havenever been validated for estimating bleeding tendency ortreatment of haemorrhage-induced coagulopathy andcannot reflect quality of clot formation.1 – 3 Because strategiesfor treating the main underlying pathologies of acquired coa-gulopathy, namely thrombin deficiency, poor clot firmness,and hyperfibrinolysis, are different, knowledge of primary
deficiencies is of clinical importance. While thrombin for-mation has been shown to be sustained in the early phaseof severe trauma,4 5 fibrinogen and platelets are consumedby the clot formation process itself. Furthermore, blood loss,dilution, acidosis, and hypothermia, commonly present ininjured patients, additionally decrease concentrations of fibri-nogen and numbers of platelets.6 Therefore, we hypothesizethat on admission, severely injured patients more frequentlyexhibit low clot firmness and poor fibrin polymerization thanimpaired thrombin formation.
British Journal of Anaesthesia 107 (3): 378–87 (2011)Advance Access publication 23 June 2011 . doi:10.1093/bja/aer158
& The Author [2011]. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved.For Permissions, please email: [email protected]
by guest on June 3, 2014http://bja.oxfordjournals.org/
Dow
nloaded from
• 20,211 trauma patients
• TXA or placebo within 8h
• All-‐cause mortality: – 14·∙5% Vs 16·∙0% – RR 0·∙91 (0·∙85-‐0·∙97; p=0·∙004)
• Death due to bleeding: – 4·∙9% Vs 5·∙7% – RR 0·∙85 (0·∙76–0·∙96; p=0·∙008)
acid binds with high affinity (dissociation constant[Kd]= 1.1mmol/L) to one lysine binding site on plas-minogen and with low affinity (Kd= 750mmol/L) tothe four or five other sites.[4] Tranexamic acidalmost completely blocks the binding of plasmi-nogen or the heavy chain of plasmin to fibrin, pri-marily through binding to the high-affinity lysinebinding site of plasminogen. Although plasmi-nogen may still be converted to plasmin in thepresence of a plasminogen activator, such as tis-sue plasminogen activator, after binding to tra-nexamic acid, it can no longer interact with anddigest fibrin (figure 2).[9] Tranexamic acid alsoblocks the binding of a2-antiplasmin to plasminand its inactivation of plasmin.
The binding potency of tranexamic acid toplasminogen is 6- to 10-fold higher than thatof the other antifibrinolytic synthetic lysine deri-
vative e-aminocaproic acid in fibrinolytic testsystems.[9] The lysine binding sites in plasmino-gen reside in separate kringle domains, which areareas of the protein chain characterized by tripleloop structures stabilized by three disulfide lin-kages. Both tranexamic acid and e-aminocaproicacid appear to interact with the low-affinity lysinebinding site of the kringle 5 domain. The kringle5 binding site may mediate the initial associationof plasminogen with fibrin. The high-affinity kringle1 lysine binding site appears to require C-terminallysine residues that are present on fibrin onlyafter partial digestion of fibrin.[10] In addition toinhibiting plasmin, tranexamic acid also compe-titively inhibits the activation of trypsinogen byenterokinase, noncompetitively inhibits trypsinandweakly inhibits thrombin.[9] In contrast, tranex-amic acid was shown to dose-dependently increase
Plasminogen
Lysine binding site
t-PA
Plasmint-PA
Fibrin degradationproducts
Fibrin degradationproducts
Activation of fibrinolysis Inhibition of fibrinolysis
Fibrin
Plasminogen
t-PA
Fibrin
Tranexamic acid
Plasmint-PA
Fibrin
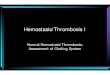
Fig. 2. Antifibrinolytic action of tranexamic acid. Plasminogen normally binds to lysine residues on fibrin and is converted to plasmin in thepresence of tissue plasminogen activator; plasmin then digests fibrin. Tranexamic acid reversibly binds to plasminogen at the lysine bindingsite, preventing the binding of plasmin(ogen) to fibrin and the subsequent degradation of fibrin [reproduced from Dunn and Goa. Tranexamicacid: a review of its use in surgery and other indications. Drugs 1999 Jun; 57 (6): 1005-32 with permission from Adis (ª Adis Data InformationBV 1991. All rights reserved)]. t-PA = tissue plasminogen activator.
588 McCormack
ª 2012 Adis Data Information BV. All rights reserved. Drugs 2012; 72 (5)

6/23/14
7
Tranexamic acid in dogs • Blackstock K et al. JVECC 2011; 21(S1):S10
• Plasma samples spiked with: – EACA to 80-500µg/mL – TXA to 0.25-15µg/mL
• Hyperfibrinolysis simulated with tPA in Kaolin-TEG
• Therapeutic serum concentrations estimated – Minimum required for 0% lysis at 30min
• Minimum serum concentrations: – EACA 450 µg/mL – TEA 12.5 µg/mL
• Dogs may require higher doses of EACA and TXA cf people
Tranexamic acid in dogs • Kelmer E et al. JVECC 2011; 21(S1):S7
• Retrospective of dogs receiving IV TXA for bleeding – 68 study dogs and 62 controls (equivalent baselines) – Median Tx 2d (1-21), mean dose 8.0 ± 2.2 mg/kg
• No difference in total product usage or volume – 1.9 Vs 2.2 units/dog p=0.952 – 27.2 Vs 29.6 mL/kg p=0.34
• Kelmer E et al. JVECC 2013; 23(S1):S8 – 2 dogs administered TA 15-20 mg/kg slow IV bolus vomited – 9 dogs administered TA 10 mg/kg slow IV bolus then 10 mg/kg/hr CRI
• TXA sig. decreased PT, Hct, R-time, alpha angle
• TXA sig. increased TEG LY30 (unexpected)
Hemorrhagic shock resuscitation • Current human medical practice suggests:
• Damage control resuscitation
• Early delivery of blood products
• 1:1:1:1 ratios?
• +/- TXA, rFVIIa, Fg concentrates
• Point of care coagulation testing (TEG / ROTEM)
• Massive transfusion protocols

6/23/14
8
TEG guided therapy in trauma
r-TEG
MA <55mm Platelets
Alpha angle <63o Cryo
TEGACT >110s FFP
• 51-year-old male, helmeted motorcycle crash victim
• FAST - massive abdo bleeding • Initial r-TEG shows prolonged
ACT with estimated 65% lysis
• ?Consumptive coagulopathy • Tx with large volume transfusion
TEG guided therapy in trauma • Patient continued to do poorly
• Estimated 72.7% lysis
• Products given inc: – 23 units PRBCs – 14 units FFP – 2 units cryoprecipitate – 2 units platelets
• Repeated r-TEGs provided confidence that the patient needed antifibrinolytics
• 5 g of Amicar (EACA) given
• Complete reversal of fibrinolysis
Options for veterinary patients?
1664 Scientific Reports: Retrospective Study JAVMA, Vol 220, No. 11, June 1, 2002
SMALLANIMALS/
EXOTIC
In recent years, blood transfusion of veterinarypatients has become commonplace. Transfusions
may consist of whole blood or blood components, suchas packed RBC (PRBC) or fresh-frozen plasma (FFP).Red blood cell transfusions are typically given to cor-rect anemia resulting from hemorrhage, RBC destruc-tion, or inadequate erythropoiesis. Plasma transfusionsare indicated to replace coagulation factors and occa-sionally to treat hypoproteinemia. Retrospectivereviews of transfusion practices in veterinary medicinehave been published,1-3 and in these reviews, the vol-ume of PRBC given to dogs receiving transfusions wastypically 10 to 19 ml/kg (4.5 to 8.6 ml/lb).2,3 Acuteblood loss, hemolysis, coagulopathy, and bone marrowfailure were the most common indications for transfu-sion. Survival rates of dogs undergoing transfusionranged from 47 to 61%,2,3 with most dogs dying of the
underlying disease process, rather than an inability tomeet blood transfusion requirements.
In human medicine, transfusion of very largeamounts of blood is occasionally warranted. Massivetransfusion, the term coined for this clinical situation,has been defined as transfusion of a volume of wholeblood or blood components that is greater than thepatient’s estimated blood volume within a 24-hour peri-od.4-6 Other definitions have included replacement ofhalf the patient’s estimated blood volume in 3 hours,6
administration of blood products at a rate of 1.5ml/kg/min over a period of 20 minutes, or the replace-ment of 150% of the patient’s blood volume irrespectiveof time.5 Given the severity of injuries and diseaseprocesses that cause near exsanguination, it should notbe surprising that individuals who receive massivetransfusion experience numerous complications and ahigh mortality rate. Some of the reported complicationsinclude electrolyte disturbances, coagulation defects,hypothermia, alterations in acid-base status, impairedwound healing, acute lung injury, various transfusionreactions, and transmission of infectious diseases.6-8
Massive transfusion imposes a substantial drain onblood banking resources, with a select few patientsconsuming a large percentage of a hospital’s blood sup-ply. To date, there have been no reports in the veteri-nary literature on massive transfusion, and survivalrate following this type of blood product expenditure isnot known. The purposes of the study reported herewere to determine clinical characteristics of dogs thatreceived massive transfusion and identify the underly-ing diseases, complications, and outcomes associatedwith massive transfusion in these dogs.
Criteria for Selection of CasesThe Tufts University hospital transfusion log for
January 1997 through June 2001 was reviewed, anddogs and cats receiving a substantial volume of bloodproducts relative to body size (approx 1 unit/5 kg [1unit/11 lb]) were identified. Medical records of theseanimals were subsequently evaluated to determinewhether they met the criteria for massive transfusion.For purposes of this study, massive transfusion wasdefined as transfusion of a volume of blood products inexcess of the patient’s estimated blood volume (90ml/kg [40 ml/lb] for dogs and 66 ml/kg [30 ml/lb] forcats9) in a 24-hour period or transfusion of a volume ofblood products in excess of half the patient’s estimatedblood volume in a 3-hour period. Blood products weredefined as whole blood, PRBC, or FFP. Blood productswere prepared from voluntary donors, stored, andtransfused according to standard techniques, asdescribed.10,11
Massive transfusion in dogs: 15 cases (1997–2001)
L. Ari Jutkowitz, VMD; Elizabeth A. Rozanski, DVM, DACVIM, DACVECC; Jennifer A. Moreau; John E. Rush, DVM, MS, DACVIM, DACVECC
Objective—To determine clinical characteristics ofdogs that received massive transfusion and identifythe underlying diseases, complications, and out-comes. Design—Retrospective study.Animals—15 dogs. Procedure—Medical records of dogs receiving amassive blood transfusion were evaluated for trans-fusion volume, underlying disease process or injury,benefits and complications of transfusion, and out-come. A massive transfusion was defined as transfu-sion of a volume of blood products in excess of thepatient’s estimated blood volume (90 ml/kg [40 ml/lb])in a 24-hour period or transfusion of a volume of bloodproducts in excess of half the patient’s estimatedblood volume in a 3-hour period.Results—Six dogs had intra-abdominal neoplasiaresulting in hemoabdomen, 3 had suffered a traumat-ic incident resulting in hemoabdomen, and 6 had non-traumatic, non-neoplastic blood loss. Mean volumesof packed RBC and fresh-frozen plasma administeredwere 66.5 ml/kg (30 ml/lb) and 22.2 ml/kg (10 ml/lb),respectively. All dogs evaluated developed low ion-ized calcium concentrations and thrombocytopenia.Transfusion reactions were recognized in 6 dogs.Four dogs survived to hospital discharge. Conclusions and Clinical Relevance—Results sug-gest that massive transfusion is possible and poten-tially successful in dogs. Predictable changes in elec-trolyte concentrations and platelet count develop. (JAm Vet Med Assoc 2002;220:1664–1669)
From the Department of Clinical Sciences, School of VeterinaryMedicine, Tufts University, North Grafton, MA 01536.
Address correspondence to Dr. Rozanski.
Brief Clinical Communication Journal of Veterinary Emergency and Critical Care 23(1) 2013, pp 82–86doi: 10.1111/vec.12017
Autologous canine red blood cell transfusionusing cell salvage devicesLindsay M. Kellett-Gregory, BSc (Hons), BVetMed (Hons), DACVECC, MRCVS; Mayank Seth, BSc(Hons), BVetMed (Hons), DACVIM, MRCVS; Sophie Adamantos, BVSc, DACVECC, MRCVS andDaniel L. Chan, DVM, DACVECC, DACVN, MRCVS
Abstract
Objective – To describe the use of automated blood salvage devices for autotransfusion in dogs.Technique – Blood salvage devices can be used to collect blood from the intraoperative surgical field orpostsurgical drainage sites. The salvage device washes cells in 0.9% saline, removing plasma proteins, othercellular components, and activators of coagulation and inflammation. Washed red blood cells may be safelyreturned to the patient, minimizing the need for allogeneic blood transfusions.Significance – Blood salvage has been safely used in human medicine for decades and is feasible in veterinarymedicine. Potential advantages include reduced reliance on banked blood for massive transfusions and min-imization of morbidities associated with the use of allogeneic and stored blood products. Concerns about thesafety of salvaged blood have been largely dispelled in human medicine but further investigation regarding thesafety of such procedures in veterinary patients is warranted.(J Vet Emerg Crit Care 2013; 23(1): 82–86) doi: 10.1111/vec.12017
Keywords: anemia, autotransfusion, autologous cell salvage, cell saver, dogs
Introduction
Transfusion of packed red blood cells (pRBCs) is anincreasingly common therapy in small animal veteri-nary medicine, but one frequently hampered by a lackof availability of blood products. The maintenance ofa large blood bank requires considerable monetary ex-penditure and expertise, and stored blood products mayonly be available to clinicians in limited quantities.1 Theavailability of fresh blood products may also be limited,as blood donors should be prescreened to assure goodhealth, ascertain their blood type, and to allow for ap-propriate infectious disease screening.2
The lack of availability of stored canine pRBCs fortransfusion may be partially mitigated by the use of an
From the Department of Veterinary Clinical Sciences, The Queen MotherHospital for Animals, The Royal Veterinary College, Hertfordshire, AL97TA, United Kingdom (Kellett-Gregory, Adamantos, Chan); and VRCC, 1Bramston Way, Southfield, Laindon, Essex SS15 6TP, United Kingdom (Seth).
Dr. Chan is Editor-in-Chief of the journal but did not participate in the peer-review process other than as an author. The authors declare no other conflictof interest.
Address correspondence and reprint requests toMrs. Lindsay Kellett-Gregory, Department of Veterinary Clinical Sciences,The Queen Mother Hospital for Animals, The Royal Veterinary College,Hertfordshire, AL9 7TA, United Kingdom.Email: [email protected] February 13, 2012; Accepted November 28, 2012.
autologous RBC salvage system or cell saver. Such sys-tems can be used to collect blood from a surgical fieldor incisional drain. Once collected, viable RBCs may beconcentrated and returned to the patient, minimizingthe need for stored pRBC transfusion when large vol-umes of hemorrhage have occurred or are anticipated.3
Cell salvage machines pump the collected blood from areservoir into a centrifugation bowl where dense RBCsare separated from plasma proteins and lighter cellularelements. The RBCs are then washed and resuspended in0.9% saline. This blood may then administered to the pa-tient immediately or stored for administration within 6 hof collection.4 Some newer salvage devices utilize a spiralcentrifugation system rather than processing batches ofblood in a bowl to allow continuous processing of bloodand immediate return of salvaged cells to the patient.5
Cell salvage systems are preferable to direct autotransfu-sion of blood from the surgical field as it removes othercontaminants from the collected fluid and allows concen-tration of pRBCs, minimizing the transfusion volume.
Autotransfusion has traditionally been consideredan option of last resort, yet it has potential benefitsover traditional allogenic blood transfusion. Autologousblood transfusions ensure RBC antigenic compatibil-ity, maximizing the longevity of transfused cells, min-imizing the contribution of a transfusion to inflamma-tion, and removing the costs and delays associated with
82 C⃝ Veterinary Emergency and Critical Care Society 2013

6/23/14
9
Liver failure
Hemostatic dysfunction liver disease
Hunt BJ. N Engl J Med 2014; 370:847-859
Factor deficiencies • Chronic hepatitis
– 1/3 dogs with CH have PT / aPTT prolongations – Decreased concentrations of FI, FV, FVII, FIX, FX, and FXI – Spontaneous bleeding rare except in advanced disease
• Acute liver disease – Prolonged clotting times – Decreased FVII, FVIII, FX and increased vWF – Synthetic failure complicated by DIC and thrombocytopenia
• Congenital portosystemic shunts – Mild prolongation of aPTT reported in some studies – Decreased thrombin, FV, FVII, and FX also documented – Bleeding rare (<2%)

6/23/14
10
Vitamin K deficiency – Decreased bile flow – Anorexia – Altered GI flora
• Canine biliary disease – Up to 50% have PT / aPTT prolongations – Perioperative bleeding tendencies uncommon
• Feline biliary disease – Alterations in coagulation profile in 50-75% – Most have Vitamin K dependent coagulopathy – Bleeding in ~20-50% cases depending on underlying disease – Cause largely unknown ?GI bleeding
Coagulation in hepatobiliary disease
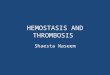
Figure 1: Guidelines for the management of patient with hepatobiliary disease and coagulation disturbances.PT, prothrombin time; aPTT, activated partial thromboplastin time; VK1, vitamin K1; FFP, fresh frozen plasma; PCV, packed cell volume;PLN, protein losing nephropathy; PLN, protein losing enteropathy; IMHA, immune-mediated hemolytic anemia; DIC, disseminatedintravascular coagulation; Tx, treatment.
heparin and in some reports these treatments have ledto resolution of the PVT.122 Even in people, treatmentrecommendations for PVT are controversial.127 A recentconsensus statement from the American Association forthe Study of Liver Diseases recommended that patientswith acute PVT (ie, PVT diagnosed in the setting of ab-dominal pain) receive treatment with anticoagulants (eg,warfarin or heparin) for at least 6 months.127 These rec-ommendations are based on the observation that 50%of patients will recanalize the portal vein if anticoagu-lant therapy is initiated promptly, while untreated pa-tients rarely spontaneously recanalize.186 The indicationfor treatment of chronic PVT with anticoagulants is lessclear, as studies show little benefit in thrombus reso-lution with treatment.186, 187 In addition, many humanpatients with hepatic disease that develop PVT are cir-rhotic with preexisting portal hypertension, and the useof anticoagulants may increase the risk for hemorrhagefrom gastroesophageal varices.22, 188 However, a recentretrospective evaluation of patients with chronic PVTshowed improved survival with the use of warfarin,with no increase in clinically significant gastrointesti-nal hemorrhage.188 Platelet inhibitors have not yet been
evaluated in veterinary patients with liver disease andstudies are needed in this area. Further studies are alsoneeded to determine with veterinary patients with hep-atobiliary disease are at the highest risk for thrombosisand which prophylactic interventions are appropriate.
As a clearer understanding of the role of parenchy-mal extinction in hepatic disease emerges in the comingyears, therapy aimed at hypercoagulability may becomea target for slowing the progression of liver disease.
Conclusion
Understanding and evaluating the coagulation status ofpatients with hepatobiliary disease is a challenge due tothe liver’s dual role in the synthesis and removal of pro-and anticoagulant factors. With hepatobiliary diseaseantagonistic alterations may occur in platelet numberand function, coagulation factors, fibrinolysis, and vas-cular endothelial function. Currently available coagula-tion tests have limitations in assessing coagulation sincethey fail to account for all the abnormalities occurring invivo. New diagnostic modalities, such as TEG, may helpto better elucidate the true risks of bleeding with invasive
C⃝ Veterinary Emergency and Critical Care Society 2011, doi: 10.1111/j.1476-4431.2011.00691.x 599
Kavanagh C et al. J Vet Emerg Crit Care 2011; 21(6): 589-604

6/23/14
11
Updates on plasma storage / stability
Arterial thromboembolism

6/23/14
12
• TAT complexes, D-dimers, FDPs, PT, aPTT, AT
• No sig. difference between groups for: – TAT complexes, D-dimers, FDPs
• AT activity sig. lower in HCM cats
• Hypercoagulability in 45% HCM cats
• Hypercoagulability defined as ≥2 of: – High Fg – High fVIII – High TAT complexes – High D-dimers – AT deficiency
• Endothelial injury assessed by vWF:Ag
• Hypercoagulability identified in: – Cats with spontaneous echocontrast – Cats with ATE
• ATE cats had higher vWF:Ag
• 42 clinically healthy cats and 30 cats with HCM
• Median CT of clinically healthy cats was 64 s (43–176)
• Median CT of cats with HCM was 74 s (48–197)
• No sig. difference between normal and HCM cats
• No sig. differences between mild - mod - severe HCM

6/23/14
13
“Despite the willingness of cardiologists to adopt treatment strategies for their feline HCM patients, we could find virtually no clinically relevant literature to support these decisions.”
GPIIb/IIIa inhibition
• Bright JM et al. Vet Ther 2003; 4:35-46
• Abciximab significantly reduced in vivo feline arterial thrombus formation
• Magee et al. AJVR 2014; 75:309-312
• Abciximab did not significantly inhibit ADP or TRAP induced feline platelet aggregation
Equipoise!
• Multi-‐centre, double-‐blinded, prospective study
• Cats that experienced a CATE event and survived 1–3
months were eligible for enrollment
• Aspirin (81 mg PO E3d) / Clopidogrel (18.75 mg PO SID)
• 1oy end-‐point
• Clinically evident embolic event
• 2oy end-‐points
• All-‐cause mortality, cardiac death, ADR

6/23/14
14
• 72 cats enrolled (36 cats in each study group)
• Randomization adequate WRT: age, weight, gender, underlying cardiac disease, and ATE recovery time
Study period Endpoint Aspirin (d) Clopidogrel (d) p
First 12 months
ATE recurrence 192 >365 0.021
ATE or cardiac death 128 346 0.028
All cause mortality 116 248 0.051
Whole study
ATE recurrence 192 443 0.019
ATE or cardiac death 128 346 0.025
All cause mortality 116 248 0.046
• 61.2% cats (n=153) euthanized at presentation
• 27.2% cats (n=68) survived >24h
• 12.0% cats (n=30) survived >7d
• MST 94d (95% CI, 42–164) (if cat alive at d7)
• 2.4% cats (n=6) alive at 1y
Canine ATE
Aortic thrombosis in dogs: Presentation, therapy,and outcome in 26 cases*
Randolph L. Winter, DVM a, Cassidy D. Sedacca, DVM, MS b, Allison Adams,DVM c, E. Christopher Orton, DVM, PhD c,*
aDepartment of Clinical Sciences, Texas A&M University, College Station, TX, USAbUpstate Veterinary Specialists, 222 Troy Schenectady Rd, Latham, NY, USAcDepartment of Clinical Sciences, Colorado State University, Fort Collins, CO, USA
Received 23 July 2011; received in revised form 27 January 2012; accepted 18 February 2012
KEYWORDSDog;Aortic;Thromboembolism;Warfarin
Abstract Objectives: The pathogenesis and presentation of aortic thrombosis(AT) in dogs is not well characterized and an effective antithrombotic therapy forAT in dogs has not been identified. Our goal is to report the clinical presentationand results of therapies in dogs with AT.Animals: Twenty-six client-owned dogs.Methods: Retrospective review of medical records of dogs diagnosed with ATbetween 2003 and 2010.Results: Twenty-six dogs had an apparent primary mural aortic thrombus. None hadstructural heart disease at diagnosis. Twenty dogs were ambulatory with varyingdegrees of pelvic limb dysfunction. Duration of ambulatory dysfunction was 7.8weeks (range 1 daye52 weeks). A majority of dogs (58%) had no concurrent condi-tions at diagnosis.Fourteen dogs were treated with a standard warfarin protocol for a median
period of 22.9 months (range 0.5e53 months). Ambulatory function improved inall dogs treated with warfarin. Time until clinical improvement was 13.9 days(range 2e49 days). Dogs treated with warfarin did not become non-ambulatory,die or undergo euthanasia related to AT, or have a known serious hemorrhagicevent.Conclusions: The pathogenesis of AT in dogs is distinct from that of aortic thrombo-embolism (ATE) in cats. Aortic thrombosis in dogs is more likely to involve localthrombosis in the distal aorta with embolization to the arteries of the pelvic limb
* Previous presentation: This paper was presented in abstract form via oral presentation at the ACVIM Forum in Denver, CO on June16, 2011.* Corresponding author.E-mail addresses: [email protected], [email protected] (E.C. Orton).
1760-2734/$ - see front matter ª 2012 Elsevier B.V. All rights reserved.doi:10.1016/j.jvc.2012.02.008
Journal of Veterinary Cardiology (2012) 14, 333e342
www.elsevier.com/locate/jvc
910 Scientific Reports JAVMA, Vol 241, No. 7, October 1, 2012
SM
ALL
AN
IMA
LS
Aortic thromboembolism occurs commonly in cats and has been addressed extensively in the litera-
ture.1–6 Typical clinical signs in feline patients consist of acute-onset hind limb paresis, pain, absent femoral pulses, and nail bed cyanosis.2,3 Although idiopathic cases have been reported,7 most cats have underlying cardiac disease, with congestive heart failure reported in 40% to 66% of cats.2,3,7 Prognosis is typically poor, with a reported rate of survival to discharge of 0% to 50% and 6-month recurrence rate of 45% to 75%.2,8 Low rectal temperature, bradycardia, and multiple limb involvement have all been associated with decreased survival rate.3 Euthanasia is common, occurring in 24% to 35% of cases.3
Clinical information regarding aortic thrombosis in dogs is less thoroughly documented in the current liter-ature. In canine patients, aortic thrombosis has been as-sociated with multiple conditions, including hyperad-renocorticism, protein-losing glomerulonephropathy, infective endocarditis, and neoplasia.9–12 Both acute and chronic onset of disease has been reported,9 and clini-cal signs include exercise intolerance, hind limb pare-sis, absent femoral pulses, cold extremities, and signs of pain.9,11,13 Survival rate in dogs with aortic thrombosis
Aortic thrombosis in dogs: 31 cases (2000–2010)
Geri A. Lake-Bakaar, DVM; Eric G. Johnson, DVM, DACVR; Leigh G. Griffiths, VetMB, DACVIM, PhD
Objective—To describe clinical signs, treatment, and outcome of aortic thrombosis in dogs.Design—Retrospective case series.Animals—31 dogs with aortic thrombosis.Procedures—Records were retrospectively reviewed and data collected regarding signal-ment, historical signs, physical examination findings, laboratory testing, definitive diagno-sis, and presence of concurrent disease.Results—The records of 31 dogs with clinical or postmortem diagnosis of aortic thrombo-sis were reviewed. Onset of clinical signs was acute in 14 (45%) dogs, chronic in 15 (48%), and not documented in 2 (6%). Femoral pulses were subjectively weak in 6 (19%) dogs and absent in 17 (55%). Frequent laboratory abnormalities included high BUN concentration (n = 13), creatinine concentration (6), creatine kinase activity (10), and D-dimer concentration (10) and proteinuria with a urine protein–to–creatinine concentration ratio > 0.5 (12). Concur-rent conditions included neoplasia (n = 6), recent administration of corticosteroids (6), and renal (8) or cardiac (6) disease. Median survival time was significantly longer for dogs with chronic onset of disease (30 days; range, 0 to 959 days) than for those with acute onset of clinical signs (1.5 days; range, 0 to 120 days).Conclusions and Clinical Relevance—Results suggested that aortic thrombosis is a rare condition in dogs and accounted for only 0.0005% of hospital admissions during the study period. The clinical signs for dogs with aortic thrombosis differed from those seen in feline patients with aortic thromboembolism. Median survival time was significantly longer for dogs with chronic disease than for dogs with acute disease. Despite treatment, outcomes were typically poor, although protracted periods of survival were achieved in some dogs. (J Am Vet Med Assoc 2012;241:910–915)
has been reported to exceed that of cats with ATE; how-ever, the prognosis and rate of recurrence have not been fully addressed.9,13
In feline patients, the outcome of therapeutic inter-ventions, including thrombolytic treatment with strep-tokinase or t-PA or long-term anticoagulant treatment with acetylsalicylic acid, clopidogrel, warfarin, and heparin, has been reported.1,5,6,8,14 The literature con-cerning therapeutic intervention in dogs is sparse and conflicting.9 Two case reports14,15 of dogs reported strep-tokinase or t-PA administration to result in partial or complete thrombus resolution. However, another case report9 indicated that t-PA treatment was ineffective. To our knowledge, there are no reports of long-term man-agement of the disease.
The purpose of the study reported here was to de-scribe the clinical signs and diagnostic findings for dogs with aortic thrombosis and assess associations with survival data. We also aimed to describe short-term (thrombolytic drug treatment and rheolytic thrombec-tomy) and long-term (anticoagulant and antiplatelet treatment) therapeutic interventions. Clinical decision
From the Departments of Medicine and Epidemiology (Lake-Bakaar, Griffiths) and Surgical and Radiological Sciences (Johnson), School of Veterinary Medicine, University of California-Davis, Davis, CA 95616.
The authors thank Dr. Molly Church for pathology images and Den-nis Feser for compilation of hospital population data.
Address correspondence to Dr. Griffiths ([email protected]).
ABBREVIATIONS
ATIII Antithrombin IIIATE Aortic thromboembolismINR International normalized ratioPT Prothrombin timet-PA Tissue plasminogen activatorUPC Urine protein–to–creatinine concentration ratio

6/23/14
15
Rivaroxaban (Oral DTI)
Cats
• Dixon-Jimenez A et al. JVECC 2013; 23(S1):S12-3
• 0.7-1.3 mg/kg
• Samples at T=0, 3, 8 24h
• Dose dependent effect
• Peak effects vs PT, aPTT at 3h
• Anti-Xa persisted >24h
• No bleeding noted
Dogs
• Conversey B et al. J Vet Intern Med 2013;27:709
• 8 dogs: Placebo or 2 mg/kg rivaroxaban SID or BID
• Rivaroxaban significantly affected PT, aPTT, CAT, AXA and TEG
• Difference between SID Vs BID noted with PT and CAT
• Rivaroxaban BID maintains 24h anticoagulant efficacy
Pulmonary thromboembolism
Identifying risk factors
Quantifying consequences
Definitive thrombus imaging
Risk factors for PTE Disease process / Risk factor
Hypercoagulable state
Flow abnormalities
Endothelial dysfunction
DM !
DIC ! !
FIP ! !
Hypercortisolemia !
IMHA !
Indwelling catheters ! !
Neoplasia ! !
Pancreatitis ! !
PLE / PLN !
Sepsis ! !
Trauma ! !

6/23/14
16
• PME confirmed PTE in 29 dogs
• No pathognomonic clin-path or radiographic findings
• PTE suspected antemortem in 11/29 (38%) dogs
• PTE was only a differential in 11/17 dogs despite compatible clinical signs
• All had diseases previously associated with PTE
• Arterial blood gases measured in 15/29 (52%) dogs: 12/15 exhibited hypoxaemia 15/15 had increased A-a gradient
• Response to supplemental O2 was variable
• At PME: 86% dogs had grossly visible emboli 59% dogs had multiple disease processes 55% dogs had additional pulm. pathology
Identifying risk factors

6/23/14
17
Biomarkers of PTE
• A-a gradient
• PaO2:PaCO2
• PaCO2:ETCO2
• cTn
• BNP
• FDPs
• D-dimers
• TAT complexes
• P-selectin
• PLAs
• Protein C
• TFPI
Identifying consequences
Identifying consequences

6/23/14
18
Defini3ve diagnosis
Defini3ve diagnosis
Can it be done in real patients with respiratory distress?
PETSAVERS PAPER
190 Journal of Small Animal Practice • Vol 55 • April 2014 • © 2014 British Small Animal Veterinary Association
Journal of Small Animal Practice (2014) 55, 190–197DOI: 10.1111/jsap.12185
Accepted: 16 December 2013; Published online: 13 February 2014
Comparison of computed tomography pulmonary angiography and point-of-care tests for pulmonary thromboembolism diagnosis in dogsR. Goggs, D. L. Chan, L. Benigni, C. Hirst, L. Kellett-Gregory and V. L. Fuentes
Department of Clinical Science and Services, Royal Veterinary College, North Mymms, AL9 7TA
R. Goggs’s current address is Department of Clinical Sciences, College of Veterinary Medicine, Cornell University, Ithaca, NY, 14853, USA
C. Hirst’s current address is Fitzpatrick Referrals, Halfway Lane, Godalming, Surrey, GU7 2QQ
OBJECTIVES: To evaluate the feasibility of CT pulmonary angiography for identification of naturally occur-
ring pulmonary thromboembolism in dogs using predefined diagnostic criteria and to assess the ability
of echocardiography, cardiac troponins, D-dimers and kaolin-activated thromboelastography to predict
the presence of pulmonary thromboembolism in dogs.
METHODS: Twelve dogs with immune-mediated haemolytic anaemia and evidence of respiratory distress
were prospectively evaluated. Dogs were sedated immediately before CT pulmonary angiography using
intravenous butorphanol. Spiral CT pulmonary angiography was performed with a 16 detector-row
CT scanner using a pressure injector to infuse contrast media through peripheral intravenous cath-
eters. Pulmonary thromboembolism was diagnosed using predefined criteria. Contemporaneous tests
included echocardiography, arterial blood gas analysis, kaolin-activated thromboelastography, D-dimers
and cardiac troponins.
RESULTS: Based on predefined criteria, four dogs were classified as pulmonary thromboembolism posi-
tive, three dogs were suspected to have pulmonary thromboembolism and the remaining five dogs
had negative scans. The four dogs identified with pulmonary thromboembolism all had discrete filling
defects in main or lobar pulmonary arteries. None of the contemporaneous tests was discriminant for
pulmonary thromboembolism diagnosis, although the small sample size was limiting.
CLINICAL SIGNIFICANCE: CT pulmonary angiography can be successfully performed in dogs under seda-
tion, even in at-risk patients with respiratory distress and can both confirm and rule out pulmonary
thromboembolism in dogs.
INTRODUCTION
Pulmonary thromboembolism (PTE) is the obstruction of the pulmonary artery or its branches by thrombi and is a major cause of morbidity and mortality in dogs with immune- mediated haemolytic anaemia (IMHA) (Reimer et al. 1999, Scott-Moncrieff
et al. 2001). Dogs with IMHA are predisposed to PTE potentially because of an associated hypercoagulable state (Fenty et al. 2011, Goggs et al. 2012) that may result from increased intravascular tissue factor expression secondary to the marked inflammatory response that accompanies the disease (Piek et al. 2011, Kidd & Mackman 2013). There is also evidence of platelet activation in
http
://w
ww
.bsa
va
.co
m/

6/23/14
19
Sepsis, SIRS and DIC!
Sepsis associated thrombosis
Hunt BJ. N Engl J Med 2014; 370:847-859
PAPER
Journal of Small Animal Practice • Vol 54 • March 2013 • © 2013 British Small Animal Veterinary Association 129
Journal of Small Animal Practice (2013) 54, 129–136DOI: 10.1111/jsap.12037
Accepted: 17 December 2012
Characterisation of changes in the haemostasis system in dogs with thrombosisN. Bauer and A. Moritz
From the Department of Veterinary Clinical Sciences, Clinical Pathology and Clinical Pathophysiology, Justus-Liebig University Giessen, Giessen, Germany
OBJECTIVE: To prospectively assess (2008 to 2009) all phases of coagulation including thromboelastog-
raphy in dogs with thrombosis to determine if thrombosis is associated with hypercoagulable states.
METHODS: Coagulation reaction in dogs with thrombosis (n=7) diagnosed by diagnostic imaging or histo-
pathology was compared with 56 control dogs. Dogs pretreated with antiplatelet and anticoagulation
drugs were excluded. Thromboelastographic G-values >10·3 Kdyn/cm2 were used to define a hyperco-
agulable state.
RESULTS: Compared with the controls, there was a significantly higher mean platelet component
indicating lower platelet activation status (17·99 ±1·36 versus 20·48 ±2·04 g/dL, P=0·0004),
increased thromboelastographic G-value (6·4 ±1·6 versus 13·1 ±6·2 Kdyn/cm2, P=0·0029), activated
partial thromboplastin time, fibrinogen, D-dimers (all: P<0·0001) as well as decreased antithrombin
(P=0·0049), factor VIII (P<0·0001), protein C (P<0·0001), protein S (P=0·0373) and activated protein
C-ratio (P=0·0013). On the basis of thromboelastographic G-value, three of six thromboelastographic
tracings were classified as normocoagulable and three as hypercoagulable.
CLINICAL RELEVANCE: In dogs with thrombosis, both normo- and hypercoagulable states are present and
activated protein C resistance is common.
INTRODUCTION
Characteristics of thromboembolic disease are of growing inter-est in both human and veterinary medicine. Three factors – the so called Virchow’s triad – may be responsible for the develop-ment of thrombosis including venous stasis, injury of the vascu-lar endothelium and a hypercoagulable state (Favaloro & Lippi 2011). However, in dogs and humans a hypercoagulable state is difficult to detect during routine coagulation analysis. The rou-tinely measured coagulation variables (coagulation times, fibrin-ogen, D-dimers) have been evaluated previously in dogs with thrombosis (Nelson & Andreasen 2003, Rosser 2009). To our knowledge all phases of the coagulation process have not been assessed to date.
Increased platelet function and activation status may con-tribute to thrombophilia (i.e. a prothrombotic state), but the measurement of platelet function and platelet activation status is
more difficult to perform on a routine base. During each haema-tological examination, the ADVIA 120/2120 (Siemens Health-care Diagnostics) laser-based haematology analyser, provides a variety of unique platelet morphology indices. In dogs, ADVIA 120/2120 platelet morphology indices have been rarely evaluated (Bauer et al. 2012, Moritz et al. 2003a,b). Previous investiga-tions in dogs (Moritz et al. 2005) and humans (Chapman et al. 2003) demonstrated that one of these indices – the mean platelet component concentration (MPC) – can be used to assess platelet activation status because of its correlation with P-selectin.
The assessment of single coagulation variables has the dis-advantage that only one phase of the haemostasis process is determined and it is difficult to detect hypercoagulable states. In contrast, thromboelastography (TEG) reflects the whole coagulation process and was used previously to detect throm-bophilia in dogs with disseminated intravascular coagulation (DIC) (Wiinberg et al. 2009), neoplasia (Kristensen et al. 2008),
http
://w
ww
.bsa
va
.co
m/

6/23/14
20
Identifying thrombi
TEG identification of non-overt DIC
• CD UFH q6h to d7, then q8
• IAD based on anti-Xa activity
• IAD daily to d7, then weekly to d28
• 7 IAD dogs alive at 180d
• 1 CD dog alive at 180d
• TE in 5/7 CD dogs Vs 2/8 IAD dogs
• 15 dogs with primary IMHA
• Standardized IMHA therapy and CD UFH 150U/kg SC, n=7, or IAD UFH, n=8

6/23/14
21
Was IAD actually effective? +2h
+6h
PK / PD of LMWH (dalteparin)
• 150IU/kg q8h
• aPTT & TT not useful
• AT activity 102 → 91 • Plt count 317 → 281 • Hct 51 → 43
• Mischke R et al. Am J Vet Res 2001;62:595-598
Take home messages… • Consider vincristine / IVIG for IMTP
• Frozen platelets are a poor substitute for fresh platelets
• TAC definitely occurs in dogs, ACOT-S may too
• If TAC occurs, consider DCR, early transfusion and TXA
• Myriad hemostatic disorders accompany hepatobiliary disease
• Plasma products may be more stable than we thought
• No evidence-based acute therapy for FATE
• Current recommendation = clopidogrel +/- aspirin for FATE prevention
• ID at-risk patients to improve PTE detection
• CTPA is the future of PTE diagnosis
• TEG may aid DIC identification
• UFH more likely to be efficacious if dose is individualized