Embed Size (px)
Citation preview

Hemosta(cOp(onsforHeavyMenstrualBleeding
Vision:Allwomenandgirlswithblooddisordersarecorrectlydiagnosedandoptimallytreatedandmanagedateverylifestage
Peter A. Kouides M.D. Medical and Research Director, Mary M. Gooley Hemophilia Center
Clinical Professor of Medicine, University of Rochester School of Medicine
Attending Hematologist, Rochester General Hospital

OBJECTIVES• Reviewthehemostasisofmenstura1on
• Iden1fytherapeu1ctargets
• Therapue1cop1onsforheavymensesingeneral
• Therapeu1cop1onsforinheritedbleedingdisorders
• Focusontherapeu1csinvonWillebranddisease
2


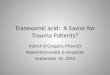
Overview of Hemostasis

Reminder…we do not bleed in a vacuum…

Endothelium
SubendothelialCollagen
VonWillebrandFactor
GPIIb/IIIa
Fibrinogen
SubendothelialCollagen
VonWillebrandFactor
Endothelium
IntrinsicPathway
ExtrinsicPathway
Thrombin

SubendothelialCollagen
VonWillebrandFactor
Endothelium
Plasmin
ExcessiveFibrinolysisAKAHeavyMenses

Hemostasis in menstrua7on
• vWFmediatedplateletaggrega(on
• Fibrinforma(on• Vasoconstric(on• Tissueregenera(on
• PGinducedplateletinhibi(on
• Fibrinolysis• Vasodilata(on
Endothelial cells
Collagen Subendothelium
platelets platelets
platelets
Platelet adhesion Platelet aggregation
GP 1b
GP
11b/
111a
Increasedmenstrualbloodflow>80cc=
MENORRHAGIA(HMB)
INDUCTION: COMPENSATION:INADEQUATE and/or OVER-
PossibleHemosta1cDefectsinMenorrhagia(HMB)
VWF

FIBRIN CLOT FORMATION FACILITATED BY PLATELET AGGREGATION via VWF
endothelial cells VWF FIBRIN STRANDS
Where/why a 22 y/o may present with heavy menses (HMB)
Decreased platelet
number and/or function
Decreased or dysfunctional von Willebrand factor
1.Decreased fibrin generation from the initiation of tissue factor that combines with VIIa→activates X →Xa activates prothrombin → thrombin then generates fibrin clot through cleavage of fibrinogen 2. Decreased fibrin propogation via FXI, FIX and FVIII 3. Decreased fibrin cross-linking d/t FXIII deficiency
Increased plasmin generation due to decreased anti-plasmin
or PAI
In ED with heavy period & blood blisters
in mouth
Dx- ITP
Heavy menses past 2 periods with severe cramps on Motrin 800 qid
Dx- Drug-induced platelet dysfunction
HMB since menarche and freq. epistaxis & bruising; mother same sx
Dx - Inherited Platelet Function Disorder (e.g., dense granule deficiency)
HMB since menarche, epistaxis and easy bruising;
mother same sx
Dx - Von Willebrands,
Type 1
HMB since menarche, history of bleeding at time of umbilical cord separation, easy bruising and epistaxis, history of knee hemearthroses when she fell off skateboard age 11 , mother asymptomatic
Dx - Severe FVII deficiency or could also be any severe rare bleeding disorder like Fibrinogen (FI) deficiency or Prothrombin (FII) deficiency or Factor V deficiency or Factor VII deficiency or FVIII or FIX carrier who is lyonized or Factor XI deficiency or FXIII deficiency
HMB since menarche with easy brusing; mother asymptomatic Dx- Inherited anti-plasmin or
plasminogen activator inhibitor HMB progressively worse past 4-6 cycles, no epistaxis or easy
bruising or family history
Dx - idiopathic HMB- in up to
50% of cases of HMB!

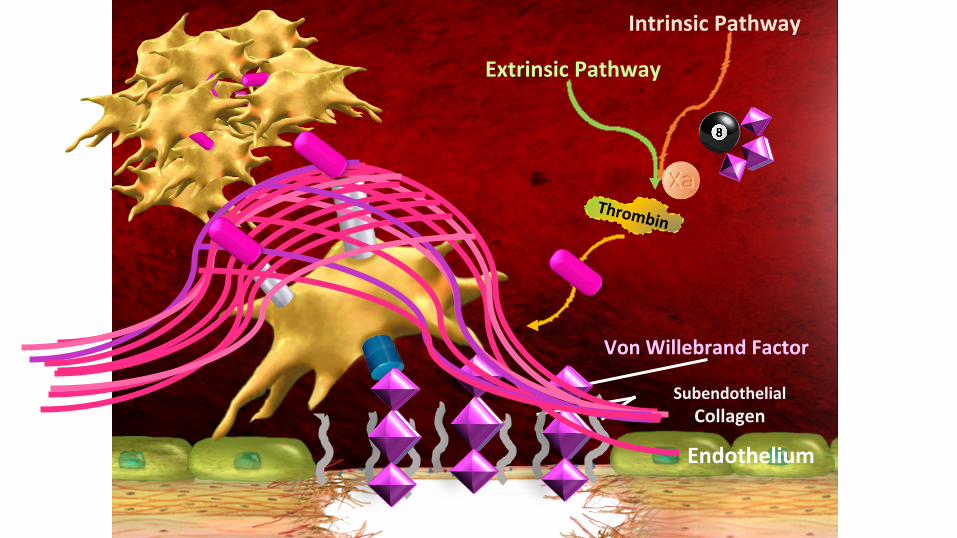
Best Therapy for Heavy Menstrual Bleeding?


Heavy Menstrual Bleeding as a Disorder of Increased fibrinolysis
• Reportsofincreasedsystemicandlocalizedintrauterinefibrinolysisinheavymenstrualbleedingandinpostpartumhemorrhage
• Catheterizedsamplesofincreasedfibrinoly1cac1vityinHMBpa1entscomparedtocontrols
WinklerUH.AnnNYAcadSci1992;667:289-90EdlundM,BlombackM,HeL..BloodCoagulFibrinolysis2003;14:593-8

• 12studiesinvolving690women-• thereduc1oninMBLrangedfrom34%to56%inthosetreatedwith>3mgtranexamicacidfor5days
• Superiorreduc1oninMBLoverthreecyclescomparedtomefanamicacid(54%versus10%,p<0.001)
• Overall,TAsignificantlyreducesMBLinwomenwithHMB.However,itdoesnotreducethedura1onofmensesorregulatethecycle
BitzerJ,etal.ObstetGynecolSurv.2015;70(2):115–30.MaXesonKA,etal.ObstetGynecol.2013;121(3):632–43.
Tranexamic Acid in HMB: Systema7c Review

ANewandImprovedTranexamicAcid?Lysteda–briefhistory
• Unique formulation that provides a higher per-tablet dose and increases drug absorption
• Designed to maintain efficacy of immediate release TA while minimizing gastrointestinal adverse effects
• Xanodyne Pharmaceuticals program (2003)
• FDA approval in November, 2009

FDA Licensure Trial for Lysteda
Lukes, et al. Obstet Gynecol. 2010; 116:865-75
Reduction of MBL*
TA (n=115) 69.6 mL (40.4%)
Placebo (n=67) 12.6 mL (8.2%) *(statistically significant difference, P<.001)

1.3 g tid dosing superior to 650 mg tid dosing
Freeman,etal.AmJObstetGynecol.2011;205:319.e1-7

Risk Profile of Lysteda • Nosta1s1callysignificantadverseeventscomparedtoplacebo
• Nothrombo1cevents
• Thrombosishasnotbeenobservedinmenorwomenreceivingtranexamicacidfor-
• bleeding2°tocardiacororalsurgery,acuteupperGIbleeding,oroculartrauma
• Useoftranexamicacidnotassociatedwithanincreasedriskorincidenceofthromboemboliceventscomparedwiththebackgroundrateofthrombo1ceventsinwomenofchildbearingage
Lukes, et al. Obstet Gynecol. 2010; 116:865-75

Outstanding Issues With Lysteda • Concurrentestrogen-containingcontracep1on
• Adolescents-aslicensurestudyexcludedage<18yearsage• However,apharmacokine1cstudyin20adolescentfemalesaged12-16yearsofage,nodoseadjustmentwasneeded
• Recentpilotstudy(n=17)showedoralTAappearedasefficaciousasOCinthemanagementofadolescentHMBbyreducingMBLandimprovingqualityoflife
SrivathsVL,etal.JPediatrAdolescGynecol.2015;28:254e257

Hemosta7c Therapy Beyond Tranexamic Acid DDAVP induces Endothelial cell (EC) via cAMP mediated Weibel- Palade Body secretion increasing membrane- bound and circulating VWF as well as FVIII
DDAVP also induces platelet release and membrane presentation of P-selectin which Mediates platelet rolling on ECs under high shear conditions through PSGL-1/P-selectin Interaction
DDAVP increases EC adhesiveness for platelets and platelet adhesion to collagen probably via VWF P.J.SvenssonBloodReviews28(2014)95–102
DDAVP(1-deamino8-D-arginevasopressin)bindsprimarilytoan1diure1ctype2vasopressinreceptorscomparedtotype1receptors,soreducingundesirablevasoac1vesideeffectsandprolongsitshalf-lifewhencomparedtona1vevasopressin
Physiology of Vasopressin Exploited by DDAVP

Background, DDAVP responsiveness in VWD
• Type1-UsuallyifFVIII,VWFRCo>10%willhave2-6foldresponsewithimprovedplateletfunc1onbut-
• Whenbaselinelevels10-20%bewareofType1Cwithitsini1alexcellentresponsealbeitshort-lived
• Type2A-Variable
• Type2B-UsuallycontraindicatedCastamanG,etal.Blood.2008;111(7):3531–9.
DownsideofINDDAVPforVWD-relatedHMB:• Quarterofpa1entsexperiencemoderatetoseveresideeffects-
• Headache• Flushing• Nausea/Vomi1ng• Fa1gue• Weightgain• Leastcommonbutmostsevere-Hyponatremia>seizure
DunnA,etal.Haemophilia.2000;6:11-14.

CDC Female Data Collec7on pilot study (n=319): Treatments used for menorrhagia in Inherited Bleeding Disorders
Byams V, et al. Haemophilia. 2011; 17 (Suppl. 1): 6–13
Treatment
Oralcontracep(ve 55%
DDAVP 34%
An(-fibrinoly(cs 24%
Bloodorplasmaproducts 7%
Clo_ngfactorproducts 6%
Endometrialabla(on 4%
MIRENA 3%
Uterinearteryemboliza(on 2%
Platelettransfusion 1%
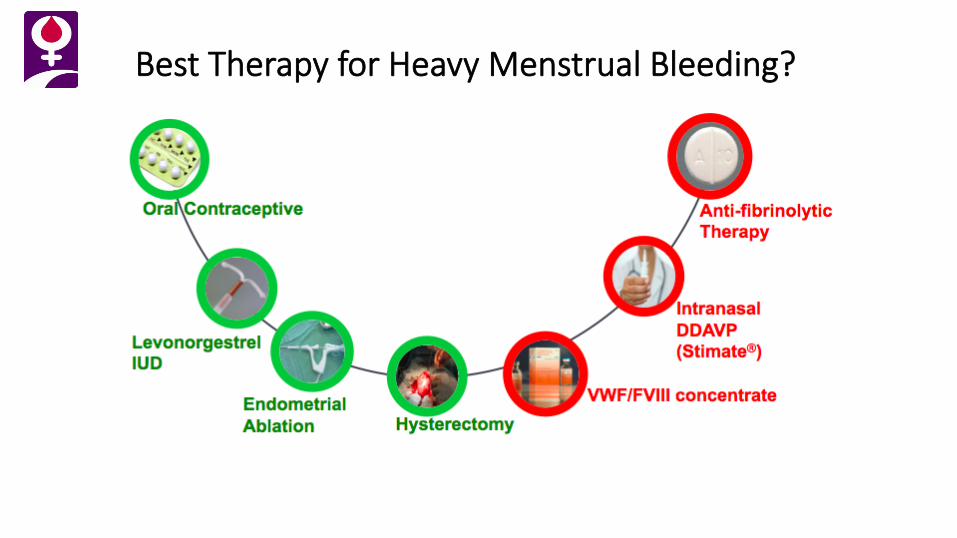
Bleeding Disorder Related Menorrhagia (HMB) Management: TA (Europe, Canada) or DDAVP (U.S.)
Desmopressin(DDAVP)• Posi1vecaseseriesexperiencebasedonsubjec1veassessment:Ø 80-90%goodtoexcellent
• Morerecentdata:ControlledstudiesusingPBACorspectrophotometry:Ø RoyalFreeLondon:
• IntranasalDDAVPwasnotbenerthanplacebo
Ø KarolinskaSweden:• IntranasalDDAVPincombina1onwithTAmosteffec1ve
Tranexamicacid(TA)• Innon-VWDmenorrhagia-randomizedstudyØ 54%reduc1oninMBLwithTAalone
• InVWDmenorrhagiaØ Smallstudies,
Ø Mohri:3g/dosein3pa1ents• Ong,etal:4g/d(1dose)in4pa1ents
• Onundarson:4g/d(1dose)in1pa1ent
• RoyalFreeLondon:15/37(40%)withPBAC<100
KadirR,etal.Haemophilia.2002;8:787-793;EdlundM,etal.BloodCoagFibrinolysis.2002;13:225-231.
MohriH.Thromb&hrombolysis.2002;14:255-257;OngYL,etal.Haemophilia.1998;4:63-65;OnundarsonPT.Haemophilia.1999;5:76.
BonnarJ,SheppardBL.BMJ.1996;313:579-582; RodegherioF,etal.T&H1996;76:692-696;LeissingerC,etal.Haemophilia.2001;7:258-266;

Χεντερ φορ Δισεασε Χοντρολ - �ΥΣΑ Ωοµεν Ωιτη Βλεεδινγ Δισορδερ Μαναγεµεντ Στυδψ
0
10
20
30
40
50
60
70
80
90
No.
of S
ubje
cts
100-199
200-299
300-399
400-499
500-599
600-699
700-799
800-899
900-999
>1000
PBAC
Offered oral contraceptives, but can refuse for any reason and
stay in study
Women with menorrhagia (HMB)
Diagnostic workup
Randomized arm of: tranexamic acid versus intranasal DDAVP
STUDY OUTCOMES Quality of life
Menstrual flow
Coagulation parameters
Kouides, et al. British J Haem.
2009; 145 (2):212-220

PLOT OF MEAN PBAC OVER TIME BY SEQUENCE OF TREATMENT
100
120
140
160
180
200
220
240
260
280
300
0 1 2 3 4
PERIOD
MEA
N P
BA
C
STTS
IN-DDAVPx2cyclesthenTAx2cycle
TAx2cyclesthenIN-DDAVPx2cycles
Kouides, et al. British J Haem. 2009; 145(2):212-220

0
50
100
150
200
250
300
TA 1st DDAVP 2nd DDAVP 1st TA 2nd
PBAC Pre-tx
PBAC Post
The Center for Disease Control Women With Bleeding Disorder Management Study:
Reduction in PBAC - TA vs. DDAVP
PBA
C
Kouides, et al. British J Haem. 2009; 145 (2):212-220

The Center for Disease Control Women With Bleeding Disorder Management Study:
Improvement in QOL - TA vs. DDAVP
0
2
4
6
8
IN-DDAVP first TA first
Unhealthy days baseline
Unhealthy days after rx
n The number of unhealthy days by SF-36 QOL instrument:
Kouides, et al. British J Haem. 2009; 145 (2):212-220
The Center for Disease Control Women With Bleeding Disorder Management Study:
Improvement in QOL - TA vs. DDAVP, II
Kouides, et al. British J Haem. 2009; 145 (2):212-220
• TheCenterforEpidemiologicStudiesDepressionScale(CES-D)Ø summaryscoredecreasedfrombaseline,indica1ngfewerdepressivesymptomsinbotharms
• Rutamenorrhagiaques1onnaire-Ø ChangeinmeanscorefrombaselinetoaoerIN-DDAVP,pvalue=0.008
Ø ChangeinmeanscorefrombaselinetoaoerTA,pvalue=0.003

For DDAVP Failures?
• CombinedtherapywithTA-
EdlundM,etal.BloodCoagulabonandFibrinolysis.2002;13:225-231

VWF concentrates in DDAVP and/or TA refractory cases in VWD-related HMB
VWFformenorrhagia(HMB):Asurveyandliteraturereview• 83surveysdistributedtohemophiliatreatmentcenterMDs
§ 20(24.1%)providedsufficientdataforanalysis
• Of1321womenwithVWDseenduring2011–2014,816(61.8%)hadmenorrhagia(HMB)
• Combinedoralcontracep1ves,TAanddesmopressinwerethemostcommonfirst-linetherapies
• VWFreplacementwasathird-linetherapyreportedin13women(1.6%)
• Togetherwithdatafrom88womenfrom6publishedstudies,VWFreplacementtherapysafelyreducedmenorrhagiain101womenatadoseof33–100IU/kgondays1–6ofmenstrualcycle
Ragni,etal.Haemophilia.2016;22(3):397-402.

FDA Approved VWF products
SingalMandKouidesP:DrugsofToday.2016;52(12):653-666
Plasma-derivedVWFcontainingFVIIIconcentrates
Recombinant

Thankyou!
fwgbd.org