Embed Size (px)
Citation preview

Brief Clinical Report
Hemophagocytic Lymphohistiocytosis in a PatientWith Deletion of 22q11.2
Maurizio Arico,1 Alberto Bettinelli,2 Rita Maccario,1 Rita Clementi,1 Grazia Bossi,1 andCesare Danesino3*1Clinica Pediatrica, IRCCS Policlinico S. Matteo, Pavia, Italy2II Clinica Pediatrica, Istituti Clinici di Perfezionamento, Universita di Milano, Milan, Italy3Biologia Generale e Genetica Medica, Universita di Pavia, Pavia, Italy
We report on a new patient with deletion of22q11 associated with hemophagocytic lym-phohistiocytosis and a fatal outcome. Shehad minor facial anomalies and cardiac mal-formation corresponding to those describedin del (22q11) syndrome, normal T and B cellfunction and NK activity; bone marrow as-piration showed active erythrophagocyto-sis. Our case in addition to two other chil-dren reported previously suggest that sucha rare association between lymphocyte-macrophage activation and deletion of22q11 may be more frequent than previouslyrecognized. Am. J. Med. Genet. 87:329–330,1999. © 1999 Wiley-Liss, Inc.
KEY WORDS: histiocytosis; velo-cardio-facial syndrome
INTRODUCTION
Deletion of 22q11.2 is a relatively common chromo-some abnormality [Thomas and Graham, 1997]. Thespectrum of clinical manifestations is wide and in-cludes a number of immunological defects [Dallapiccolaet al., 1996; Ryan et al., 1997]. Hemophagocytic lym-phohistiocytosis (HLH) is a rare condition that may beobserved in childhood either as an autosomal recessivedisorder, usually with very early onset [Arico et al.,1996] or as an apparently sporadic condition, some-times associated with an infection. Common pathogenshave been reported in such patients, including the Ep-
stein-Barr virus (EBV) [Arico et al., 1996; Imashuku etal., 1999].
We report on a patient with HLH and a deletion of22q11.2. The possibility of this uncommon and severecomplication should be taken into account when caringfor del (22q) patients who are at risk for immune de-rangement.
CLINICAL REPORT
The patient was a girl born to nonconsanguineousIraqi parents; her birth weight was 2500 g at 38 weeks.Pregnancy was uneventful. Family history failed to dis-close any relevant medical problem; an older sister isreported to be healthy at the age of 18 years. A diag-nosis of tetralogy of Fallot with agenesis of the pulmo-nary valve was made at the age of 3 months and cor-rected surgically. The subsequent clinical course wasuneventful. At the age of 5 3/12 years she developedrecurrent episodes of mucosal bleeding (oral, nasal)and petechiae. On admission to our hospital she was asmall child (height, weight and cranial circumference<3rd centile) with hypertelorism, high nasal bridge,short philtrum, thin lips with down-turned mouth cor-ners; slender fingers; normal lung function; a heartmurmur with normal cardiac function; a slightly en-larged liver and grossly enlarged spleen, palpable atthe umbilical line. No bone abnormalities were evident;fundoscopy showed an embryotoxon. There were noneurological deficits. Psychological evaluation was in-complete because of her insufficient knowledge of theItalian language. Blood count showed moderate micro-cytic (65 fl) anemia (8.2 g/dL), ferritin 15.9 mg/dL, re-ticulocytes 150,000/mm3, with thrombocytopenia(52,000/mm3), leukocyte count 8500/mm3 with monocy-tosis (1955/mm3). Triglycerides were 113 mg/dL andfibrinogen 201 mg/dL. Moderate hypoparathyroidismwas noted (calcium 8.12 mg/dL, phosphoremia 4.79 mg/dL, parathyroid hormone 9 pg/mL, n.v. 10–71). Screen-ing for infectious disease showed the presence of cyto-megalovirus and EBV specific IgG antibodies. Bonemarrow aspiration showed normal cells and an in-
Contract grant sponsor: Telethon; Contract grant numbers:E755, C30; Contract grant sponsor: IRCCS Policlinico S. Matteo;Contract grant number: 390RCR9701.
*Correspondence to: Prof. Cesare Danesino, Biologia Generalee Genetica Medica, C.P. 217, 27100 Pavia, Italy.E-mail [email protected]
Received 22 April 1999; Accepted 27 August 1999
American Journal of Medical Genetics 87:329–330 (1999)
© 1999 Wiley-Liss, Inc.

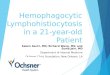
creased number of monocytes with active erythropha-gocytosis (Fig. 1). Immune function tests showed thefollowing: IgG 2280 mg/dL (n.v. 528–1959), IgA 211mg/dL (n.v. 37–257), IgM 1680 mg/dL (n.v. 25–493);lymphocyte subsets: CD3+ 89%, CD4+ 62% (1755/mm3), CD8+ 18%, CD56+ 8%. Bone age was 3 years atchronologic age 5.3 years. Brain CT scan showed anarachnoid cyst in the right frontotemporal lobe. Thepresence of minor anomalies, heart malformation, andmoderate hypoparathyroidism suggested a diagnosis ofvelo-cardio-facial syndrome and prompted a chromo-some analysis with fluorescence in situ hybridizationusing the DiGeorge region probe D22S75, whichshowed a deletion at band 22q11.2.
The child was treated with dexamethasone and in-travenous immunonoglobulins with clinical improve-ment. One month after treatment started she againdeveloped fever, splenomegaly, anemia, and thrombo-cytopenia. Steroid dose was increased, and i.v. immu-noglobulins were given with moderate transient im-provement. During the following weeks the child hadpersistent fever and cytopenia. Three months later,during another acute phase of her disease, she under-went reevaluation, showing fever, cytopenia, hemo-phagocytosis, hypertriglyceridemia, and hypofibrino-genemia. Based on such findings a diagnosis of HLHwas made. Based on lack of familial occurrence and ofparental consanguinity, and normal natural killer lym-phocytotoxic activity, she was considered to have a sec-ondary form of HLH, likely associated with recent EBVinfection. The child was treated with etoposide anddexamethasone according to the HLH-94 treatmentprotocol [Henter et al., 1997]. Despite initial clinicalresponse the disease course was rapidly fatal and thechild died at age 6 2/12 years.
DISCUSSION
The diagnostic criteria for HLH diagnosis were es-tablished by the FHL study group of the HistiocyteSociety [Henter et al., 1991]. Clinical (fever and spleno-megaly), laboratory (cytopenia affecting at least two
lineages, hypertriglyceridemia and/or hypofibrinogen-emia) and histopathologic (hemophagocytosis in bonemarrow or spleen or lymph nodes without evidence ofmalignancy) criteria are required for the diagnosis ofHLH. Immune system derangement with T-cell andmonocyte hyperactivation, hypercytokinemia, and a se-lective deficiency of cellular cytotoxicity have been re-ported as potentially related to HLH pathogenesis[Arico et al., 1988; Burgio et al., 1990]. In addition tothe clinical picture of velo-cardio-facial syndrome, ourpatient also fits the diagnostic criteria for HLH.
The present case is the third one in which a 22q11deletion caused a clinical picture of histiocytic hyper-activation. Langerhans cell histiocytosis (LCH), an his-tiocytic disorder well distinguished from HLH, hasbeen reported with partial DiGeorge syndrome in anewborn infant [Levendoglu-Tugal et al., 1996]. Re-cently, in another patient with del (22q11) [Touraine etal., 1999] HLH was diagnosed, although active hemo-phagocytosis could not be documented. In our patienthistiocytic hyperactivation resulted in typical HLH. Wecannot exclude a random association of either form ofhistiocytosis with the deletion of 22q11. Yet, in view ofthe rarity of these conditions, estimated to occuraround 1:50,000 (for HLH) and 1:20,000 (for LCH), theprobability that this chromosomal aberration causes orpredisposes for histiocytic activation should be kept inmind and further cases with this association should bereported.
REFERENCES
Arico M, Janka G, Fischer A, Henter J-I, Blanche S, Elinder G, MartinettiM and Rusca MP for the FHL Study Group of the Histiocyte Society.1996. Hemophagocytic lymphohistiocytosis. Report of 122 childrenfrom the International Registry. Leukemia 10:197–203.
Arico M, Nespoli L, Maccario R, Montagna D, Bonetti F, Caselli D, BurgioGR. 1988. Natural cytotoxicity impairment in familial haemophago-cytic lymphohistiocytosis. Arch Dis Child 63:292–296.
Burgio GR, Arico M, Marconi M, Lanfranchi A, Caselli D, Ugazio AG. 1990.Spontaneous NBT reduction by monocytes as a marker of disease ac-tivity in children with histiocytosis. Brit J Haematol 74:146–150.
Dallapiccola B, Pizzuti A, Novelli G. 1996. How many breaks do we need toCATCH on 22q11? Am J Hum Genet 59:7–11.
Henter J-I, Arico M, Egeler M, Elinder G, Favara B, Filipovich A, GadnerH, Imashuku S, Janka-Schaub G, Komp D, Ladisch S, Webb D, HLHStudy Group of the Histiocyte Society. 1997. HLH-94 a treatment pro-tocol for hemophagocytic lymphohistiocytosis. Med Ped Oncol 28:342–347.
Henter J-I, Elinder G, Ost A, FHL Study Group of the Histiocyte Society.1991. Diagnostic guidelines for hemophagocytic lymphohistiocytosis.Semin Oncol 18:29–33.
Imashuku S, Hibi S, Ohara T, Iwai A, Sako M, Kato M, Arakawa H, So-tomatsu M, Kataoka S, Asami K, Hasegawa D, Kosaka Y, Sano K,Igarashi N, Maruhashi K, Ichimi R, Kawasaki H, Maeda N, TanizawaA, Arai K, Abe T, Hisakawa H, Miyashita H, Henter JI. 1999. Effectivecontrol of Epstein-Barr virus-related hemophagocytic lymphohistiocy-tosis with immunochemotherapy. Blood 93:1869–1874.
Levendoglu-Tugal O, Noto R, Juster F, Brudnicki A, Slim M, Beneck D,Jayabose S. 1996. Langerhans cell histiocytosis associated with partialDiGeorge syndrome in a newborn. J Pediatr Hematol Oncol 18:401–404.
Ryan AK, Goodship JA, Wilson DI, Philip N, Levy A, Seidel H, Schuffen-hauer S, Oechsler H, Belohradsky B, Prieur M, and others. 1997. Spec-trum of clinical features associated with interstitial chromosome 22q11deletions: a European collaborative study. J Med Genet 34:798–804.
Thomas JA, Graham JM. 1997. Chromosme 22q11 deletion syndrome: anupdate and review for the primary pediatrician. Clin Pediatr 36:253–266.
Touraine RL, Pondarre C, Till M, Bertrand Y. 1999. Hemophagocytic lym-phohistiocytosis and del22q11 [abstract]. Genet Counseling 10:114–115.
Fig.1. Bone marrow aspirate smear showing activated macrophagesengaged in phagocytosis of erythrocytes and leukocytes. May GrumwaldGiemsa.
330 Arico et al.