Embed Size (px)
Citation preview

Original Articles
Hemodynamic Abnormalities in Fetuses with Congenital Heart Disease
W.A. Lutin, M.R. Brumund, C. Jones, C.E. Tharpe, M. Montegomery, F.M. McCaffreyDepartment of Pediatrics, Section of Pediatric Cardiology, the Medical College of Georgia, 1120 15th Street,Augusta, GA 30912, USA
Abstract. The purpose of this investigation was to assessleft and right ventricular function, volume ejection frac-tion, combined stroke volume, and combined ventricularoutput in the human fetus with congenital heart diseasecompared to the normal healthy fetus. Seventy-two fe-tuses with a variety ofin utero diagnosed congenitalcardiac defects were compared with a control group offetuses with structurally normal hearts matched for race,maternal age, and gestational age. We demonstrated sig-nificant hemodynamic changes in the fetus with congen-ital heart disease. There was a significant (p < 0.0001)decrease in the volume ejection fractions, biventricularstroke volume, and cardiac output in the congenital heartdisease group compared to matched controls. Our find-ings suggest that hemodynamic abnormalities in the fetuswith congenital heart disease are present before birth andwe speculate that myocardial reserve may not be ad-equate to respond to hemodynamic stressors such as birthor heart surgery.
Key words: Fetus — Echocardiography — Heart de-fects — Congenital — Ventricular function
The human infant with congenital heart disease (CHD)has a high postnatal mortality. Despite its relative lowincidence (8 per 1000 live births), CHD is a leadingcause of nonaccident-related death in infancy and earlychildhood. Before birth, CHD has been thought to causefew clinical symptoms because of intact fetal circulatorypathways including the patent foramen ovale and ductusarteriosus. However, several studies have demonstratedthat in uteroCHD significantly alters the normal growthand development of the fetus and may contribute to ahigher incidence ofin utero fetal demise and perinataldeath [3, 8, 12–15, 19].
The neural crest ablated chick embryo as developedby Kirby and others is an excellent model of the patho-
genesis of congenital heart disease in the human fetus[1]. Investigators have demonstrated that ablation ofthese neural crest cells results in truncus arteriosus, asevere form of congenital heart disease with 100%in ovomortality in the avian embryo [1, 9]. This lesion is as-sociated with high morbidity and mortality in humaninfants.
Additional studies of the neural crest ablated chickembryo have shown that avian hearts with persistenttruncus arteriosus display physiologic signs similar toadult heart disease. These hearts have been shown to beenlarged with respect to body weight, to have reducedcontractility, and to result in edema of the embryo [2, 6,7]. Hemodynamic abnormalities appear early in chickembryos destined to develop persistent truncus arteriosus[5, 10]. Other studies found that left and right ventricularejection fraction, stroke volume, and cardiac output inembryos with persistent truncus arteriosus are signifi-cantly decreased compared to control, providing evi-dence that ventricular dysfunction may contribute to thenear 100%in ovomortality in chick embryos with partialtruncus arteriosus [18]. Based on this evidence, we hy-pothesized that human fetuses with congenital heart dis-ease have decreased left and right ventricular stroke vol-ume and cardiac output when compared to normal fe-tuses.
Methods
Patients
The study population consisted of 72 fetuses with a variety of congen-ital cardiac defects diagnosed by fetal echocardiography between No-vember 1, 1990 and November 31, 1996. The echocardiograms weretaken from a library of approximately 800 fetal echocardiograms of 680pregnancies from the Medical College of Georgia and the University ofKentucky, Lexington. The Institutional Review Board of the partici-pating institutions approved the study.
Subjects from these recordings were divided into two groups:those fetuses with structurally normal hearts and those fetuses withinutero diagnosed CHD. Fetuses with other noncardiac defects wereCorrespondence to:W.A. Lutin
Pediatr Cardiol 20:390–395, 1999
PediatricCardiology© Springer-Verlag New York Inc. 1999

excluded. The control group was composed of 72 fetuses with normalcardiac anatomy matched for race, maternal age, and gestational age.No fetus in the control population had maternal or familial risk factorsfor CHD and all had normal obstetrical ultrasounds prior to entry. Allmothers in the control group were healthy and nondiabetic. Gestationalages were determined from fetal morphometrics and last menstrualperiod. All in uterofetal cardiac diagnoses were confirmed postnatally.Fetuses of both groups were followed prospectively with mean follow-up time of 11 ± 8 months.
Hemodynamic Measurements
This was a retrospective, blind case control study in which videotapesof normal and CHD fetuses were analyzed by three independent ob-servers who were blinded to thein uterocardiac diagnosis. All record-ings were done using a 4 mHz dual-frequency ultrasound transducerand a commercially available ultrasound machine (Hewlett-Packard orAccuson). The measurements were performed on previously recordedtapes using a Hewlett-Packard Sonos 2000 Ultrasound machine. Two-dimensional (2D) imaging and color-flow Doppler were used to iden-tify cardiac structures such as right and left ventricles, ascending aorta,main pulmonary artery, and descending aorta.
Left and right ventricular areas and lengths were measured viatracing 2D images, and volumes were calculated using Simpson’srule—a relatively geometry-independent method of assessing ventricu-lar volume [16]. Each ventricle was measured in five cardiac cyclesusing outline tracings of both diastole (maximal ventricular size) andsystole (minimal ventricular size) in two different planes—the apicalfour-chamber view and the parasternal long axis view. The medianmeasurement was selected for accuracy in each case. Averages couldonly be used for length measurements.
Using the resident software of the Sonos 2000, Simpson’s rulewas used to calculate end systolic volume (ESV) and end diastolicvolume (EDV) in single-plane and biplane modes. Area measurementswere used to calculate area ejection fractions. Based on quantitations ofESV and EDV, stroke volume (SV) and volume ejection fraction (VEF)were determined. Five measurements of heart rate from aortic andpulmonic Doppler tracings were averaged. Heart rate and stroke vol-umes were used to calculate left, right, and combined ventricular out-put.
Data Analysis
Normal and CHD fetal populations were compared with two-tailedpairedt-tests and unpairedt-tests using a commercial statistical pack-age (Statview II) on a Macintosh computer. For all comparisons,p <0.05 indicated statistical significance. Only differences found to besignificant in the unpaired tests were reported as significant. The effectsof gestational age were analyzed by two-way analysis of variance,partitioning the gestational age into four groups: 19–24, 25–29, 30–34,and 35–39 weeks’ gestation. For direct comparison to national normals,growth curves for cardiac output, SV, and ventricular volumes werecomputed by regression analysis using an expression of the formy 4
a × (gestational age)b, wherea andb are constants [17].
Results
Population Demographics
In our study, the normal and CHD fetal populations werematched for gestational age, maternal age, and race. Ges-
tational age for the CHD group was a mean of 29.2 ± 5.9weeks; in the normal group the gestational age was amean of 29.1 ± 5.9 weeks. The mean maternal age was28.4 ± 4.6 years for the normal population and 27.3 ± 6.6years in the CHD population. Fetal race in percentagenoncaucasian was 27% in the CHD population and 18%in the normal population (p 4 0.34). Table 1 lists theinuterodiagnosed and postnatally confirmed cardiac diag-noses of the CHD population.
Variability
Echocardiographically measured hemodynamic param-eters were valid and reproducible. Table 2 demonstratesthe low inter- and intraobserver variability for each car-diac measurement. Coefficient of variation was the samein normal and CHD groups.
Measurements
Heart rates were not significantly different between nor-mal and CHD fetuses. Figures 1A and 1B demonstrateleft and right ventricular end diastolic volumes (LVEDVand RVEDV) versus gestational ages in our normalpopulation and in healthy fetuses measured by Schmidtet al. [16] Our measurements of LVEDV and RVEDVare consistent with the results of Schmidt et al. and in-crease over gestational ages in a similar pattern.
After 30 weeks of gestation, we found no evidenceof diastolic volume overloading in the CHD populationwhen compared to the normal population. However,right and left ventricular end systolic volumes (RVESV
Table 1.CHD lesions in MCG patients
Diagnosis N
AV canal 9Aortic stenosis 3APVR 2Dextrocardia with VSD 2DORV 7Hypoplastic left heart 2Interrupted aortic arch 2Other 3PS/PA 4TOF 9Tricuspid atresia 4Truncus arteriosus 1VSD 24
Total 72
N, number of patients; APVR, anomalous pulmonary venous return;AV, atrioventricular; DORV, double-outlet right ventricle; Other, re-strictive patent foramen ovale; PS/PA, pulmonary stenosis/pulmonaryatresia; TOF, tetralogy of Fallot; VSD, ventricular septal defect.
391Lutin et al.: Abnormal Fetal Hemodynamics

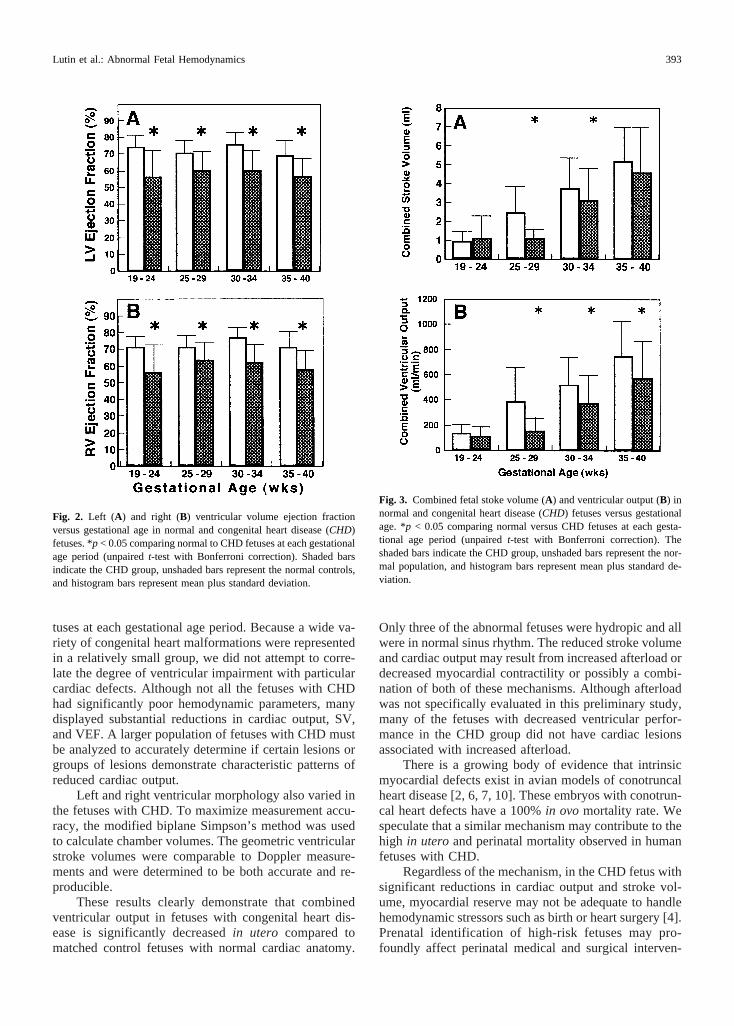
and LVESV) were significantly different between thetwo study groups. Left and right ventricular systolic vol-umes increased over gestation and were consistentlyhigher in the CHD group. After 30 weeks’ gestation, theend systolic volume in the LV was elevated [140.8% at30–34 weeks’ gestation and 136.4% at 35–39 weeks’gestation (p < 0.01)] and the RVESV was elevated[152.1% at 30–34 weeks’ gestation and 155.5% at 35–39weeks’ gestation (p < 0.02)] in the CHD population com-pared to the normal population. The higher end systolicvolumes resulted in a significant (p < 0.0001) decrease inthe measured area and volume ejection fractions in theCHD population when compared to the normal controls.Figures 2A and 2B show the volume ejection fractionsfor the two study groups. The volume ejection fractionsfor the RV and LV in the normal group were 73.0 ± 7%and 74.7 ± 8%, respectively. In the CHD population,volume ejection fractions for the RV were 50.5 ± 10%and for the LV were 51.6 ± 8%. Left and right ventricularejection fractions were constant throughout gestation.
Left and right ventricular stroke volume and ven-tricular output were significantly lower in the CHDgroup at the last three gestational ages tested. The LVstroke volume was 31% lower in the CHD populationcompared to the matched normals. There was a 28%decrease in RV stroke volume in the CHD group com-pared to the normal fetuses. This is consistent with thedecreased ejection fractions and increased end systolicvolumes measured in the CHD group. Since there is nodifference in heart rate between the study groups andstroke volume was significantly lower in the CHD popu-lation, combined ventricular output was also decreased.
This is demonstrated in Figs. 3A and 3B. Table 3 sum-marizes the hemodynamic abnormalities in the CHD fe-tuses over gestation.
Discussion
Accurate and reproducible values of cardiac output, enddiastolic volume, and stroke volume in the human fetuscan be measured and calculated using standard echocar-diographic instruments and technique. The validity ofour measurements is supported by the agreement of ourdata in the normal group with published normative data[17]. Insignificant differences of left and right ventricularEDV (LVEDV, p > 0.48; RVEDV,p > 0.38) between thetwo study populations suggest that volume loading doesnot occur to a significant degree in fetuses with CHD.However, ESV was significantly higher in the CHD fe-tuses compared to the normal controls after 30 weeks’gestation. Accordingly, calculated cardiac output andstroke volumes were lower in the fetuses with cardiacmalformations.
Decreased right and left ventricular stroke volume inthe fetuses with CHD resulted in significantly lower bi-ventricular area and VEFs compared to the control fe-
Table 2.Measurement variability of left and right ventricular geometicand hemodynamic measurementsa
Intraobservervariability (%)
Interobservervariability (%)
LVEDV 8.1 10.3LVESV 7.2 11.8RVEDV 6.9 9.0RVESV 9.6 13.1LVSV 10.8 15.3RVSV 11.2 13.7LVVEF 5.2 6.8RVVEF 7.1 8.9
LVEDV, left ventricular end diastolic volume; LVESV, left ventricularend systolic volume; RVEDV, right ventricular end diastolic volume;RVESV, right ventricular end systolic volume; LVSV, left ventricularstroke volume; RVSV, right ventricular stroke volume; LVVEF, leftventricular volume ejection fraction; RVVEF, right ventricular volumeejection fraction.a Intraobserver variability is reported as the coefficient of variation (%)for five measurements on all 144 patients. Interobserver variability isrecorded for 20 control and 20 CHD patients measured by three ob-servers. The average of three observers was used.
Fig. 1. Human fetal left (A) and right (B) ventricular end diastolicvolumes versus gestational age in our normal population compared topublished normals. The dashed line represents normative data. Thesolid line represents the normals from our study population.
392 Pediatric Cardiology Vol. 20, No. 6, 1999
tuses at each gestational age period. Because a wide va-riety of congenital heart malformations were representedin a relatively small group, we did not attempt to corre-late the degree of ventricular impairment with particularcardiac defects. Although not all the fetuses with CHDhad significantly poor hemodynamic parameters, manydisplayed substantial reductions in cardiac output, SV,and VEF. A larger population of fetuses with CHD mustbe analyzed to accurately determine if certain lesions orgroups of lesions demonstrate characteristic patterns ofreduced cardiac output.
Left and right ventricular morphology also varied inthe fetuses with CHD. To maximize measurement accu-racy, the modified biplane Simpson’s method was usedto calculate chamber volumes. The geometric ventricularstroke volumes were comparable to Doppler measure-ments and were determined to be both accurate and re-producible.
These results clearly demonstrate that combinedventricular output in fetuses with congenital heart dis-ease is significantly decreasedin utero compared tomatched control fetuses with normal cardiac anatomy.
Only three of the abnormal fetuses were hydropic and allwere in normal sinus rhythm. The reduced stroke volumeand cardiac output may result from increased afterload ordecreased myocardial contractility or possibly a combi-nation of both of these mechanisms. Although afterloadwas not specifically evaluated in this preliminary study,many of the fetuses with decreased ventricular perfor-mance in the CHD group did not have cardiac lesionsassociated with increased afterload.
There is a growing body of evidence that intrinsicmyocardial defects exist in avian models of conotruncalheart disease [2, 6, 7, 10]. These embryos with conotrun-cal heart defects have a 100%in ovo mortality rate. Wespeculate that a similar mechanism may contribute to thehigh in uteroand perinatal mortality observed in humanfetuses with CHD.
Regardless of the mechanism, in the CHD fetus withsignificant reductions in cardiac output and stroke vol-ume, myocardial reserve may not be adequate to handlehemodynamic stressors such as birth or heart surgery [4].Prenatal identification of high-risk fetuses may pro-foundly affect perinatal medical and surgical interven-
Fig. 2. Left (A) and right (B) ventricular volume ejection fractionversus gestational age in normal and congenital heart disease (CHD)fetuses. *p < 0.05 comparing normal to CHD fetuses at each gestationalage period (unpairedt-test with Bonferroni correction). Shaded barsindicate the CHD group, unshaded bars represent the normal controls,and histogram bars represent mean plus standard deviation.
Fig. 3. Combined fetal stoke volume (A) and ventricular output (B) innormal and congenital heart disease (CHD) fetuses versus gestationalage. *p < 0.05 comparing normal versus CHD fetuses at each gesta-tional age period (unpairedt-test with Bonferroni correction). Theshaded bars indicate the CHD group, unshaded bars represent the nor-mal population, and histogram bars represent mean plus standard de-viation.
393Lutin et al.: Abnormal Fetal Hemodynamics

tion. Afterload reduction or ionotropic support may benecessary to reduce morbidity and mortality in fetuseswith decreased cardiac output. Tables 4 and 5 summarizeour perinatal experience with fetuses diagnosedin uterowith CHD.
Future studies are needed to more clearly determinethe relative roles that afterload and myocardial contrac-tility play in the measured decreases in cardiac outputand stroke volume in CHD fetuses. Evaluating ventricu-lar wall size and comparing hemodynamic parameters inobstructive outflow tract anomalies with cardiac defectswith minimal afterload might help elucidate the relativeimpact that afterload has on cardiac output in fetuseswith CHD.
Despite traditional views that fetuses with heart mal-formations are relatively protectedin uteroby the uniquefetal circulation, we have offered convincing evidencethat the fetal circulation may not protect the fetus withCHD. Congenital heart disease remains an importanthealth problem for the unborn baby, and recent advancesin fetal echocardiography and improved screening tech-niques have resulted in a greater number ofin uteroCHDdiagnoses. Although the importance of detecting cardiacmalformations prenatally has been debated extensivelyin the literature, it has been well established that fetuseswith CHD have highin uteroand perinatal morbidity andmortality [8, 15, 16]. Our findings suggest that this maybe related to impaired fetal hemodynamics and thus pre-natal identification of heart malformations is importantand may improve the physician’s opportunity to alter thenatural course of CHD.
References
1. Allan LD, Sharland GK, Milburn A, et al (1994) Prospective di-agnosis of 1006 consecutive cases of congenital heart disease in thefetus.J Am Coll Cardiol 23:1452–1458
2. Bockman DE, Redmond S, Waldo K, Kirby ML (1987) Effect ofneural crest ablation of development of the heart and arch arteriesin the chick.Am J Anat 180:332–341
3. Clark E (1995) Epidemiology of cardiovascular malformations. In:Emmanouilides GC, Riemenschneider TA, et al (eds.)Heart Dis-ease in Infants, Children, and Adolescents: Including the Fetus andYoung Adult,5th ed. Williams & Wilkens, Baltimore, p 62
4. Cooper MJ, Enderlein MA, Dyson DC, Roge CL, Tarnoff H (1995)Fetal echocardiography: retrospective review of clinical experienceand an evaluation of indications.Obstet Gynecol 86:577–582
5. Creazzo T (1990) Reduced L-type calcium current in the embry-onic chick heart with persistent truncus arteriosus.Circ Res 66:1491–1498
6. Creazzo T, Burch J, Redmond S, Kuminski D (1994) Myocardialenlargement in the defective heart development.Anat Rec 239:170–176
7. Fogaca RTH, Warren KS, Tin JJ-C, Nosek TM, Godt RE (1993)Contractile alteration during myocardial development in the chicksubsequent to ablation of cardiac neural crest.J Cell BiochemSuppl 17D:211
8. Gough JD, Keeling JW, Castle B, Iliff PJ (1986) The obstetricmanagement of non-immunologic hydrops.Br J Obstet Gynaecol93:226–234
9. Kirby ML, Gale TF, Stewart DE (1983) Neural crest cells contrib-ute to normal aorticopulmonary septation.Science 220:1059–1061
10. Leatherbury L, Gauldin HE, Waldo KL, Kirby ML (1990) Micro-
Table 3.Hemodynamic abnormalities in the CHD population (% con-trol)
Variable Weeks
19–24 25–29 30–34 35–39
LVEDV 123.8 57.2 93.8 95.3LVESV 217.4* 75.6 140.8* 136.4*RVEDV 151.0 53.2 100.7 106.1RVESV 223.4* 68.4 152.1* 155.5*LVSV 100.4 44.5* 77.6* 79.2*RVSV 122.5 47.4 84.6* 85.2*LVVEF 75.3* 84.9* 79.2* 81.9*RVVEF 78.4* 89.7* 80.4* 80.9*CSV 114.2 46.0* 83.3* 88.4LVCO 73.9 40.0* 66.2* 68.0*RVCO 85.8 41.8* 75.4* 72.6*
LVEDV, left ventricular end diastolic volume; LVESV, left ventricularend systolic volume; RVEDV, right ventricular end diastolic volume;RVESV, right ventricular end systolic volume; LVSV, left ventricularstroke volume; RVSV, right ventricular stroke volume; LVVEF, leftventricular volume ejection fraction; RVVEF, right ventricular volumeejection fraction; CSV, combined stroke volume; LVCO, left ventricu-lar cardiac output; RVCO, right ventricular cardiac output.* p < 0.05.
Table 4.Outcomes for fetuses with congenital heart disease
72 Total fetuses39 Survived to hospital discharge (54%)33 deaths (46%)
6 Pregnancy terminations13 In utero fetal demises14 Postnatal deaths
4 Elected no therapy for lethal lesions (10%)10 Died after treatment
Table 5.Neonatal interventions in fetuses within utero congenitalheart disease
Type of intervention% of fetuseswith CHD
Neonatologist at delivery 100Cardiologist at delivery 65Vasoactive or cardiotonic medication required in
the first 6 hours of life55
Prostoglandin E1 infusion required in the first 6hours of life
20
Cardiac catheterization 31Surgery 61Special feeding regimen in the first 24 hours of
life50
394 Pediatric Cardiology Vol. 20, No. 6, 1999

cinephotography of the developing heart in neural crest-ablatedchick embryos.Circulation 81:1047–1057
11. Lutin WL, Tharpe CE, McCaffrey FM (1997) Biventricular dys-function in fetuses with congenital heart disease.J Am Coll Car-diol 29:508A
12. Montana E, Khoury MJ, Cragan JD, et al (1996) Trends and out-comes after prenatal diagnosis of congenital cardiac malformationsby fetal echocardiography in a well defined birth population, At-lanta, Georgia, 1990–1994.J Am Coll Cardiol 28:1805–1809
13. Paladini D, Calabro R, Palmieri S, D’Andrea T (1993) Prenataldiagnosis of congenital heart disease and fetal karotyping.ObstetGynacol 81:679–682
14. Rosenthal GL, Vargo TA, Ferencz C (1997) Differences in fetalsomatic growth may be due to abnormal intrauterine hemodynam-ics. Pediatrics 100:435A
15. Samantek M, Goetzova J, Benesova D (1985) Distribution of con-
genital heart malformations in an autopsied child population.Int JCardiol 8:235–250
16. Schmidt, KG, Silverman NH, Hoffman JIE (1995) Determinationof ventricular volumes in human fetal hearts by two-dimensionalechocardiography.J Am Coll Cardiol 76:1313–1316
17. Schmidt KG, Silverman NH, VanHare GF, et al (1990) Two-dimensional echocardiographic determination of ventricular vol-umes in the fetal heart: validation studies in fetal lambs.Circula-tion 84:1289–1295
18. Tomita H, Connuck DM, Leatherbury L, Kirby ML (1991) Rela-tionship of early hemodynamic changes to and cardiac phenotypeafter neural crest ablation in chick embryos.Circulation 84:1289–1295
19. Vergani P, Mariani S, Ghidini A, et al (1992) Screening for con-genital heart disease with the four chamber view of the heart.AmJ Obstet Gynecol 167:1000–1003
Pediatric Critical Care: The EssentialsBy Joseph D. Tobias, M.D., Futura Publishing
This book is intended for pediatricians, residents, and medical students. It deals with the initial diagnostic andtherapeutic issues when a child first presents with a critical illness. This manual was not intended to be anauthoritative text written for pediatric intensivists. Instead, it deals with issues of critical illness in children as theyfirst present in an outpatient or emergency room setting.
The chapter dedicated to Cardiology (Chapter 7: Congenital Heart Diseases/Arrhythmias) is written by Dr.Marcus S. Schamberger of Riley Children’s Hospital in Indianapolis, Indiana. The author presents cardiac lesionswhich may manifest as an acute and critical condition; therefore, acyanotic congenital heart diseases are notincluded. Cyanotic and obstructive congenital heart diseases are nicely presented. The author narrows his focusto management in the acute setting, thus avoiding unnecessary and irrelevant information frequently seen in suchtexts. This is followed by a segment on cardiac arrhythmias and finally by a list of medications frequently neededin such emergencies.
Chapter 8, by Drs. Joseph D. Tobias and William R. Wilson, discusses postoperative cardiac care. Theirreview is brief, however, and difficult to follow by physicians not involved in postoperative care. This chapterwould have been more appropriate for a manual intended for pediatric cardiologists in training rather than medicalstudents, pediatric residents, or general pediatricians who would rarely be involved in postoperative cardiac care.
Dr. Schamberger’s chapter is well suited for medical students and pediatric residents. Furthermore, it wouldcertainly be a valuable addition to any general pediatrician’s library.
Ra-id Abdulla, M.D.Editor
395Lutin et al.: Abnormal Fetal Hemodynamics





























