Embed Size (px)
Citation preview

The Journal of Emergency Medicine, Vol. 44, No. 6, pp. 1101–1107, 2013Copyright � 2013 Elsevier Inc.
Printed in the USA. All rights reserved0736-4679/$ - see front matter
http://dx.doi.org/10.1016/j.jemermed.2012.12.018
The results offormat at the Nor2011, Washington
RECEIVED: 8 FebACCEPTED: 18 D
Selected Topics:Toxicology
HEMODIALYSIS AND EXTRACORPOREAL REMOVAL AFTER PEDIATRIC ANDADOLESCENT POISONING REPORTED TO A STATE POISON CENTER
Michael A. Darracq, MD, MPH*† and F. Lee Cantrell, PHARMD†‡§
*Department of Emergency Medicine, Division of Medical Toxicology, University of California, San Diego, San Diego, California, †CaliforniaPoison Control System, San Diego, California, ‡University of California, San Francisco, San Francisco, California, and §University of California,
San Diego, San Diego, California
Reprint Address:Michael A. Darracq, MD, MPH, Department of EmergencyMedicine, Division ofMedical Toxicology, University of California, SanDiego, 200 West Arbor Drive, San Diego, CA 92103
, Abstract—Background: There is currently limited liter-ature regarding the use of hemodialysis after acute pediatricand adolescent poisoning. Objective: We sought to charac-terize the use of hemodialysis (HD) and other extracorporealremoval techniques (ECR) in the treatment of acutely poi-soned children and adolescents reported to a state poisoncontrol system over a 10-year period. Methods: After insti-tutional review board approval, a state poison control sys-tem database was queried for all cases coded forhemodialysis and other ECR after pediatric and adolescent(0–19 years old) poisoning. We also analyzed National Poi-son System Data to determine national trends. Results:Ninety patients were reviewed after exclusions for errorsin coding or incomplete documentation. HD was the princi-ple method of ECR employed. One case of hemoperfusionand hemofiltration was reported. HD was used, on average,nine times per year. ECR was used predominantly in adoles-cent patients (age$ to 12 years) (84 patients, 93%) for inten-tional ingestions (82 patients, 91%). Fifteen different toxinswere encountered, with salicylates (29 patients) and ethyleneglycol (23 patients) most commonly encountered. Ethyleneglycol and methanol blood levels were not available beforeinitiation of hemodialysis in all but one case. Conclusions:All salicylate-poisoned patients who underwent HD demon-strated clinical findings indicative of toxicity even in theabsence of elevated levels advocated by some as indication
this study were previously presented in posterth American Clinical Congress of Toxicology,, DC.
ruary 2012; FINAL SUBMISSION RECEIVED: 5 Deceecember 2012
1101
for HD. HD and other ECR are rarely used in the manage-ment of pediatric and adolescent poisoning. � 2013Elsevier Inc.
, Keywords—poisoning; pediatric; adolescent; extracor-poreal removal technique; hemodialysis
INTRODUCTION
The kidney has the capacity to rapidly eliminate many ex-ogenous toxins from the human body. Unfortunately, thekidney is also susceptible to direct toxicity from thesesubstances as well as indirect toxicity arising from theirclinical effects. Both parent compounds and their metab-olites may impair elimination of exogenous and endoge-nous toxins with the potential for life-threatening toxicity.Extracorporeal removal techniques (ECR) such as hemo-dialysis (HD), charcoal hemoperfusion (HP), continuousveno-venous hemofiltration (HF), and hemodiafiltration(HDF), offer alternative mechanisms for removal oftoxins.
Holubek et al. (2008) analyzed a total of 21,341 casesfrom the American Association of Poison Control Cen-ters (AAPCC) National Poison Data System (NPDS) inwhich hemodialysis or other ECR techniques were em-ployed between 1985 and 2005 (1). Lithium and ethyleneglycol were the most common toxins encountered.Salicylates, methanol, theophylline, valproic acid, and
mber 2012;
1102 M. A. Darracq and F. L. Cantrell
acetaminophen were also commonly encountered (1).Unfortunately, this study did not delineate patients byage, and there is a general paucity of published literatureregarding the use of ECR in the treatment of acutely poi-soned children or adolescents. Therefore, we sought tocharacterize the use of hemodialysis and other ECR tech-niques in the treatment of acutely poisoned children andadolescents reported to a state poison control system overa 10-year period. Additionally, we reviewed NPDS in anattempt to determine national trends in the use of ECR forpoisoned children and adolescents.
MATERIALS AND METHODS
After Institutional Review Board review and approval,case records in a state poison control system database (Vi-sual Dotlab [VDL], Madera, CA) were queried for all in-stances in which hemodialysis or other ECR technique(HP, HF, HDF) were coded in pediatric (0–11 years old)and adolescent (12–19 years old) poisoning cases be-tween January 2000 and January 2010. Age, gender, cir-cumstances surrounding exposure, toxin involved,available toxin blood concentrations, rationale or indica-tion for hemodialysis, complications related to hemodial-ysis, and rates of hospital transfer for ECRwere recorded.Available VDL free-text notes were reviewed to corrobo-rate all data.
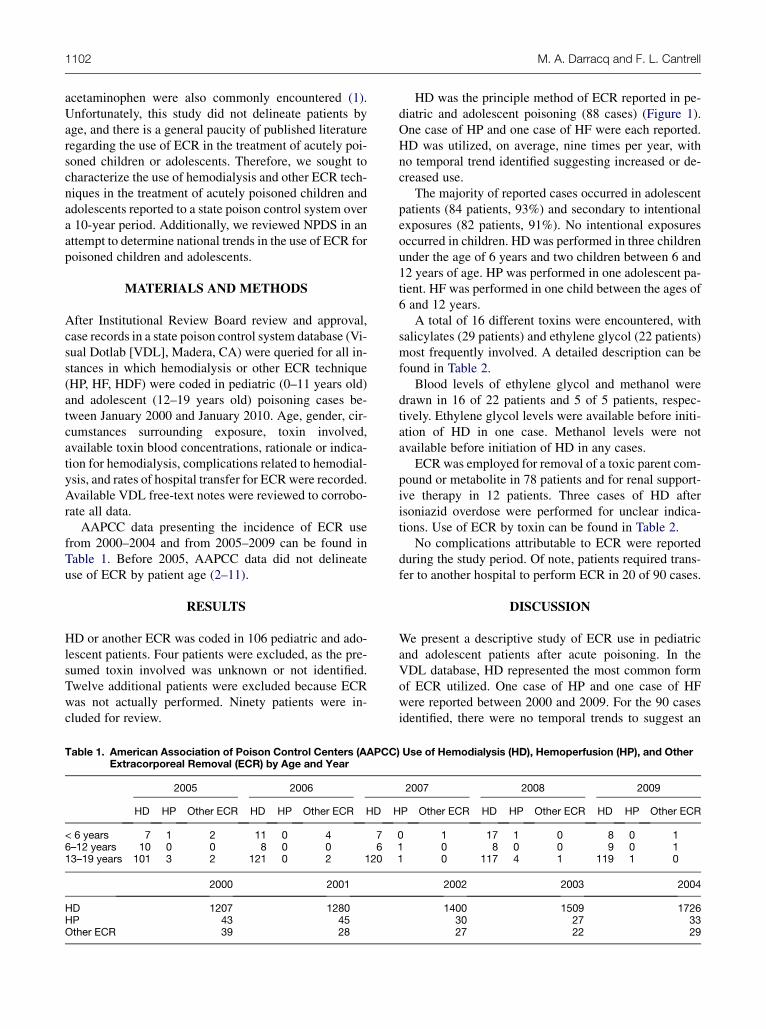
AAPCC data presenting the incidence of ECR usefrom 2000–2004 and from 2005–2009 can be found inTable 1. Before 2005, AAPCC data did not delineateuse of ECR by patient age (2–11).
RESULTS
HD or another ECR was coded in 106 pediatric and ado-lescent patients. Four patients were excluded, as the pre-sumed toxin involved was unknown or not identified.Twelve additional patients were excluded because ECRwas not actually performed. Ninety patients were in-cluded for review.
Table 1. American Association of Poison Control Centers (AAPCCExtracorporeal Removal (ECR) by Age and Year
2005 2006
HD HP Other ECR HD HP Other ECR HD H
< 6 years 7 1 2 11 0 4 76–12 years 10 0 0 8 0 0 613–19 years 101 3 2 121 0 2 120
2000 2001
HD 1207 1280HP 43 45Other ECR 39 28
HD was the principle method of ECR reported in pe-diatric and adolescent poisoning (88 cases) (Figure 1).One case of HP and one case of HF were each reported.HD was utilized, on average, nine times per year, withno temporal trend identified suggesting increased or de-creased use.
The majority of reported cases occurred in adolescentpatients (84 patients, 93%) and secondary to intentionalexposures (82 patients, 91%). No intentional exposuresoccurred in children. HD was performed in three childrenunder the age of 6 years and two children between 6 and12 years of age. HP was performed in one adolescent pa-tient. HF was performed in one child between the ages of6 and 12 years.
A total of 16 different toxins were encountered, withsalicylates (29 patients) and ethylene glycol (22 patients)most frequently involved. A detailed description can befound in Table 2.
Blood levels of ethylene glycol and methanol weredrawn in 16 of 22 patients and 5 of 5 patients, respec-tively. Ethylene glycol levels were available before initi-ation of HD in one case. Methanol levels were notavailable before initiation of HD in any cases.
ECR was employed for removal of a toxic parent com-pound or metabolite in 78 patients and for renal support-ive therapy in 12 patients. Three cases of HD afterisoniazid overdose were performed for unclear indica-tions. Use of ECR by toxin can be found in Table 2.
No complications attributable to ECR were reportedduring the study period. Of note, patients required trans-fer to another hospital to perform ECR in 20 of 90 cases.
DISCUSSION
We present a descriptive study of ECR use in pediatricand adolescent patients after acute poisoning. In theVDL database, HD represented the most common formof ECR utilized. One case of HP and one case of HFwere reported between 2000 and 2009. For the 90 casesidentified, there were no temporal trends to suggest an
) Use of Hemodialysis (HD), Hemoperfusion (HP), and Other
2007 2008 2009
P Other ECR HD HP Other ECR HD HP Other ECR
0 1 17 1 0 8 0 11 0 8 0 0 9 0 11 0 117 4 1 119 1 0
2002 2003 2004
1400 1509 172630 27 3327 22 29
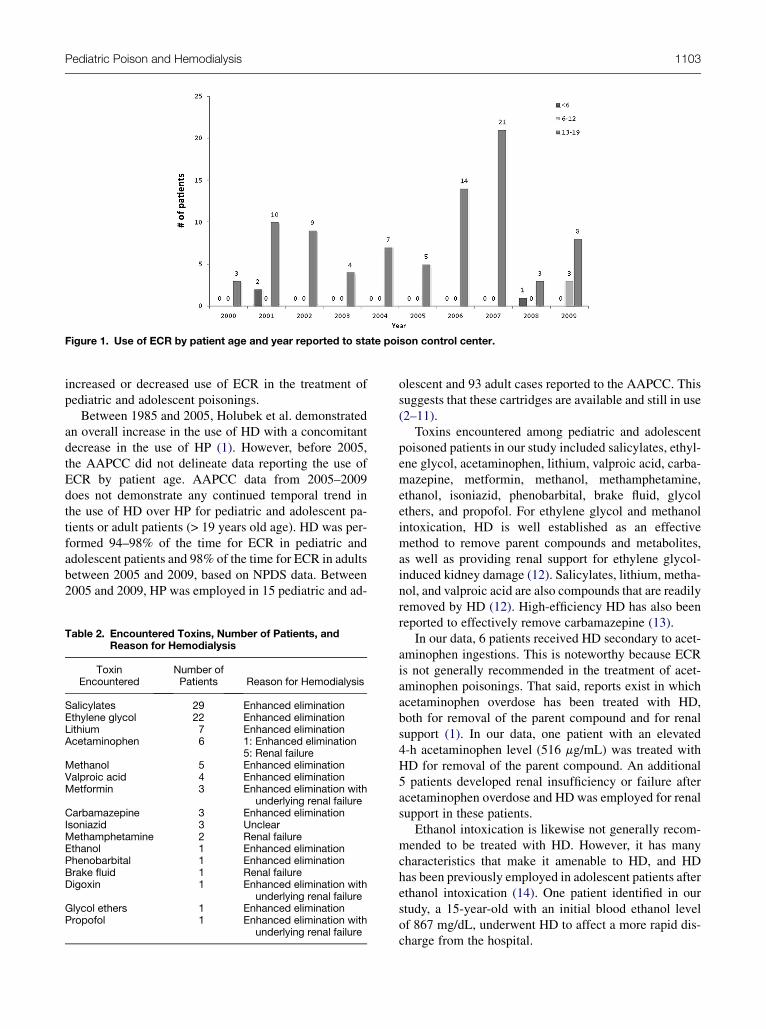
Figure 1. Use of ECR by patient age and year reported to state poison control center.
Pediatric Poison and Hemodialysis 1103
increased or decreased use of ECR in the treatment ofpediatric and adolescent poisonings.
Between 1985 and 2005, Holubek et al. demonstratedan overall increase in the use of HD with a concomitantdecrease in the use of HP (1). However, before 2005,the AAPCC did not delineate data reporting the use ofECR by patient age. AAPCC data from 2005–2009does not demonstrate any continued temporal trend inthe use of HD over HP for pediatric and adolescent pa-tients or adult patients (> 19 years old age). HD was per-formed 94–98% of the time for ECR in pediatric andadolescent patients and 98% of the time for ECR in adultsbetween 2005 and 2009, based on NPDS data. Between2005 and 2009, HP was employed in 15 pediatric and ad-
Table 2. Encountered Toxins, Number of Patients, andReason for Hemodialysis
ToxinEncountered
Number ofPatients Reason for Hemodialysis
Salicylates 29 Enhanced eliminationEthylene glycol 22 Enhanced eliminationLithium 7 Enhanced eliminationAcetaminophen 6 1: Enhanced elimination
5: Renal failureMethanol 5 Enhanced eliminationValproic acid 4 Enhanced eliminationMetformin 3 Enhanced elimination with
underlying renal failureCarbamazepine 3 Enhanced eliminationIsoniazid 3 UnclearMethamphetamine 2 Renal failureEthanol 1 Enhanced eliminationPhenobarbital 1 Enhanced eliminationBrake fluid 1 Renal failureDigoxin 1 Enhanced elimination with
underlying renal failureGlycol ethers 1 Enhanced eliminationPropofol 1 Enhanced elimination with
underlying renal failure
olescent and 93 adult cases reported to the AAPCC. Thissuggests that these cartridges are available and still in use(2–11).
Toxins encountered among pediatric and adolescentpoisoned patients in our study included salicylates, ethyl-ene glycol, acetaminophen, lithium, valproic acid, carba-mazepine, metformin, methanol, methamphetamine,ethanol, isoniazid, phenobarbital, brake fluid, glycolethers, and propofol. For ethylene glycol and methanolintoxication, HD is well established as an effectivemethod to remove parent compounds and metabolites,as well as providing renal support for ethylene glycol-induced kidney damage (12). Salicylates, lithium, metha-nol, and valproic acid are also compounds that are readilyremoved by HD (12). High-efficiency HD has also beenreported to effectively remove carbamazepine (13).
In our data, 6 patients received HD secondary to acet-aminophen ingestions. This is noteworthy because ECRis not generally recommended in the treatment of acet-aminophen poisonings. That said, reports exist in whichacetaminophen overdose has been treated with HD,both for removal of the parent compound and for renalsupport (1). In our data, one patient with an elevated4-h acetaminophen level (516 mg/mL) was treated withHD for removal of the parent compound. An additional5 patients developed renal insufficiency or failure afteracetaminophen overdose and HD was employed for renalsupport in these patients.
Ethanol intoxication is likewise not generally recom-mended to be treated with HD. However, it has manycharacteristics that make it amenable to HD, and HDhas been previously employed in adolescent patients afterethanol intoxication (14). One patient identified in ourstudy, a 15-year-old with an initial blood ethanol levelof 867 mg/dL, underwent HD to affect a more rapid dis-charge from the hospital.

1104 M. A. Darracq and F. L. Cantrell
Three cases of HD after isoniazid overdose were per-formed for unclear indications. These patients demon-strated no renal impairment, and isoniazid is notthought to be removed well by HD (15).
One case, a 14-year-old with intentional carbamaze-pine overdose and peak level of 48 mg/L, was treatedwith HP during the study period. Carbamazepine exhibitssignificant binding to plasma proteins, which may limitits clearance with hemodialysis (16). However, with theincreased availability of high-efficiency HD, treatmentwith either HD or HP is appropriate. Multi-dose-activated charcoal has previously been demonstrated toshow similar outcomes to HD or HP (17). In the identifiedcarbamazepine overdoses during the study period, 2 pa-tients underwent HD, and 1 patient underwent HP. All pa-tients left the hospital after 2 days with completeresolution of symptoms.
In metformin overdose with normal renal function,HD is generally not indicated as it is generally clearedquite well by the kidneys and prognosis is good withoutdialysis (12). However, in cases of metformin overdosewith associated renal insufficiency or failure, the smallmolecular weight of metformin and absence of significantprotein binding may allow for clearance of some of thedrug despite a large volume of distribution (18). Correc-tion of acidosis with HD and associated improvement inphysiological derangement is appropriate regardless ofthe degree to which metformin may be removed by HD.
HFwas performed in one child, a 10-year-old boy withknown seizure disorder who had received propofol for 16h after intractable seizures. He developed bradycardia,metabolic acidosis, and renal failure, and subsequentlyrequired tracheostomy and continued outpatient HD.
Propofol infusion syndrome (PRIS), a potentially life-threatening complication of prolonged propofol infu-sions, has been previously treated successfully with HF(19). The causative etiology for PRIS has not been iden-tified, but there is speculation that it may result from in-hibition of mitochondrial oxidative processes viaa potentially dialyzable propofol metabolite (19,20).The patient in our study is unique in that his totalduration of propofol infusion was well below thatpreviously reported by Wolf and others (19–21).
In the 23 acute salicylate-poisoned adolescent and pe-diatric patients who underwent HD during the study pe-riod, all demonstrated some clinical finding indicativeof toxicity, often with levels well below those advocatedby some as an indication for HD. The highest level re-corded among the patients was 95 mg/dL. EmergencyMedicine textbooks, review manuals, and nephrologypublications continue to list absolute salicylate levels asindications for hemodialysis after poisoning. Thesevalues range from > 80mg/dL to > 100mg/dL, dependingon the source (22–24). In addition to confusion regarding
the absolute number, treating physicians may forget orfail to appreciate that serum levels do not necessarilycorrespond to levels in the central nervous system(CNS), where toxicity primarily occurs, and thatindications for HD should follow clinical findingsrather than an absolute number (25). All salicylate-poisoned patients who underwent HD demonstratedclinical findings of deterioration or profound CNSimpairment, even in the absence of a markedly elevatedsalicylate level. These physiological derangements in-cluded alterations in mentation ranging from confusionand lethargy to seizures, development of an anion gap ac-idosis, or tachypnea. Indications for HD in salicylate-poisoned patients include renal failure, congestive heartfailure, acute lung injury, persistent neurological distur-bances, progressive deterioration in vital signs, severeacid-base or electrolyte imbalances despite appropriatetreatment, hepatic compromise with coagulopathy, andacute concentrations > 100 mg/dL only in the absenceof the above (25). Clinicians should make the decisionto utilize ECR in pediatric and adolescent patients basedon history and clinical findings rather than solely on toxinconcentrations in the blood.
Ethylene glycol and methanol blood levels rarelyinfluenced the use of HD in the present study. In onlyone case of ethylene glycol was a level available beforeinitiation of HD. This patient and all others had otherlaboratory and clinical evidence to suggest a significantingestion, including the presence of alteration in menta-tion, acidosis, or an osmolar gap. In no cases of methanolpoisoning were levels available before initiation of HD.Given the limited availability of ethylene glycol andmethanol levels in many treatment settings, cliniciansshould make decisions about the use of HD for toxic al-cohol poisoning based on history and clinical findingsrather than on blood level alone (26–29).
Although therewere no reported complications relatedto HD, this may reflect an absence of the appropriatequestions being asked rather than a true lack of complica-tions. Nevertheless, complications were not sufficient towarrant responding providers to mention them to poisoncontrol center (PCC) staff during follow-up calls or forthe responding PCC to document them.
Twenty patients were transferred for HD between2000 and 2010. Salicylate poisoning represented 8 ofthese patients, ethylene glycol represented 5 patients,methanol represented 2 patients, and acetaminophen, car-bamazepine, digoxin, valproic acid, and ethanol each rep-resented one case. Whereas the majority of these casesrepresented appropriate transfers for definitive care,ECR for acetaminophen, carbamazepine, and ethanolare not necessary or life-saving, as alternative therapiesare available. Transfer to another care facility has impor-tant financial and safety considerations. The average cost

Pediatric Poison and Hemodialysis 1105
for ambulance service in the state of California is $1468per transport (30). Transport may involve significant timedelays to definitive therapy with the potential for patientdeterioration and subsequent poor outcomes. Ground andaircraft transport have inherent safety risks. Fatalities andserious injury to patients, ambulance personnel, and pas-sengers in other involved vehicles occur due to ambu-lance crashes (31). Significant morbidity and mortalityis reported after Emergency Medical Services aircraft ac-cidents and crashes (32,33). Clinicians should approachthe decision to transfer a patient to another health carefacility with great caution when the poisoning can bemanaged with alternative therapies.
Limitations
This is a retrospective descriptive analysis limited to theinformation available in a poison control system data-base. Abstraction of data was performed by a single re-viewer and errors may have been made during dataabstraction or in data entry at the time of the initial callto the poison control center. There may be additionalcases where hemodialysis or other extracorporeal re-moval techniques were performed for toxin-related expo-sures that were not called into the poison control system.The results may not reflect these additional instances ofuse, which may distort the true frequency of toxins en-countered or other reported demographic characteristics.
CONCLUSION
The majority of pediatric and adolescent poisonings un-dergoing ECR are treated with HD; however, HP andHF are still being used. HD represents a therapeutic op-tion for the enhanced elimination of a number of potentialpoisons as well as supportive therapy after toxin-relatedrenal insufficiency in pediatric and adolescent poison-ings. The frequency with which ECR is employed inthis patient population seems to be static over the last10 years. Clinicians should make the decision to utilizeECR in pediatric and adolescent patients based on historyand clinical findings rather than solely on toxin concen-trations in the blood.
REFERENCES
1. Holubek WJ, Hoffman RS, Goldfarb DS, Nelson LS. Use of hemo-dialysis and hemoperfusion in the poisoned patient: a 21 year Amer-ican experience. Kidney Int 2008;74:1327–34.
2. Litovitz TL, Klein-Schwartz W, White S, et al. 2000 Annual re-port of the American Association of Poison Control Centers ToxicExposure Surveillance System. Am J Emerg Med 2001;19:337–95.
3. Litovitz TL, Klein-Schwartz W, Rodgers GC Jr, et al. 2001 Annualreport of the American Association of Poison Control Centers Toxic
Exposure Surveillance System. Am J Emerg Med 2002;20:391–452.
4. Watson WA, Litovitz TL, Rodgers GC Jr, et al. 2002 annual re-port of the American Association of Poison Control CentersToxic Exposure Surveillance System. Am J Emerg Med 2003;21:353–421.
5. Watson WA, Litovitz TL, Klein-Schwartz W, et al. 2003 annual re-port of the American Association of Poison Control Centers ToxicExposure Surveillance System. Am J Emerg Med 2004;22:335–404.
6. Watson WA, Litovitz TL, Rodgers GC Jr, et al. 2004 Annual reportof the American Association of Poison Control Centers Toxic Expo-sure Surveillance System. Am J Emerg Med 2005;23:589–666.
7. Lai MW, Klein-Schwartz W, Rodgers GC, et al. 2005 Annual Re-port of the American Association of Poison Control Centers’ na-tional poisoning and exposure database. Clin Toxicol (Phila)2006;44:803–932.
8. Bronstein AC, Spyker DA, Cantilena LR Jr, Green J, Rumack BH,Heard SE. 2006 Annual Report of the American Association of Poi-son Control Centers’ National Poison Data System (NPDS). ClinToxicol (Phila) 2007;45:815–917.
9. Bronstein AC, Spyker DA, Cantilena LR Jr, Green JL, Rumack BH,Heard SE. American Association of Poison Control Centers. 2007Annual Report of the American Association of Poison Control Cen-ters’ National Poison Data System (NPDS): 25th Annual Report.Clin Toxicol (Phila) 2008;46:927–1057.
10. Bronstein AC, Spyker DA, Cantilena LR Jr, Green JL,Rumack BH, Giffin SL. 2008 Annual Report of the American As-sociation of Poison Control Centers’ National Poison Data System(NPDS): 26th Annual Report. Clin Toxicol (Phila) 2009;47:911–1084.
11. Bronstein AC, Spyker DA, Cantilena LR Jr, Green JL,Rumack BH, Giffin SL. 2009 Annual Report of the American As-sociation of Poison Control Centers’ National Poison Data System(NPDS): 27th Annual Report. Clin Toxicol (Phila) 2010;48:979–1178.
12. Fertel BS, Nelson LS, Goldfarb DS. Extracorporeal removal tech-niques for the poisoned patient: a review for the intensivist. J Inten-sive Care Med 2010;25:139–48.
13. Schuerer DJ, Brophy PD, Maxvold NJ, Kudelka T, Bunchman TE.High-efficiency dialysis for carbamazepine overdose. J Toxicol ClinToxicol 2000;38:321–3.
14. Morgan DL, Durso MH, Rich BK, Kurt TL. Severe ethanol intoxi-cation in an adolescent. Am J Emerg Med 1995;13:416–8.
15. Malone RS, Fish DN, Spiegel DM, et al. The effect of hemodialysison isoniazid, rifampin, pyrazinamide, and ethambutol. Am J RespirCrit Care Med 1999;159:1580–4.
16. Pilapil M, Petersen J. Efficacy of hemodialysis and charcoal hemo-perfusion in carbamazepine overdose. Clin Toxicol (Phila) 2008;46:342–3.
17. Doyon S. Anticonvulsants. In: Nelson LS, Lewin NA,Howland MA, et al., eds. Goldfrank’s toxicologic emergencies.New York: McGraw Hill; 2011:698–702.
18. Lalau JD, AndrejakM, Moriniere P, et al. Hemodialysis in the treat-ment of lactic acidosis in diabetics treated by metformin: a study ofmetformin elimination. Int J Clin Pharmacol Ther Toxicol 1989;27:285–8.
19. Wolf A, Weir P, Segar P, Stone J, Shield J. Impaired fatty acid oxi-dation in propofol infusion syndrome. Lancet 2001;357:606–7.
20. Coetzee JF, Coetzer M. Propofol in paediatric anaesthesia. CurrOpin Anaesthesiol 2003;16:285–90.
21. Diedrich DA, Brown DR. Analytic reviews: propofol infusion syn-drome in the ICU. J Intensive Care Med 2011;26:59.
22. Long H. Acetaminophen, aspirin and NSAIDS. In: Barton ED,Collings J, DeBlieux PMC, Gisondi MA, Nadel E, James G, eds.James J. Adams emergency medicine. New York: Saunders Elsev-ier; 2008;1519–22.
23. Buchanan JA, Mendoza CD, Rhyee SH, et al. Salicylates. In:Blok B, Cheung DS, Platts-Mills TF, eds. First aid for the emer-gency medicine boards, an insider’s guide. New York: McGraw-Hill Medical; 2009:370–2.

1106 M. A. Darracq and F. L. Cantrell
24. Bayliss G. Dialysis in the poisoned patient. Hemodial Int 2010;14:158–67.
25. Flomenbaum NE. Salicylates. In: Nelson LS, Lewin NA,Howland MA, et al., eds. Goldfrank’s toxicologic emergencies.New York: McGraw-Hill; 2011:508–17.
26. Patil N, Lai Becker M, Ganetsky M. Toxic alcohols: not alwaysa clear-cut diagnosis. Evid Based Emerg Med 2010;12:1–25.
27. Church AS, Witting MD. Laboratory testing in ethanol, methanol,ethylene glycol, and isopropanol toxicities. J Emerg Med 1997;15:687.
28. Fraser AD. Clinical toxicologic implications of ethylene glycol andglycolic acid poisoning. Ther Drug Monit 2002;24:232.
29. Wu AH, McKay C, Broussard LA, et al. National Academy of Clin-ical Biochemistry Laboratory Medicine. Practice guidelines: rec-ommendations for the use of laboratory tests to support poisoned
patients who present to the emergency department. Clin Chem2003;49:357–79.
30. Gustafson C. Rural metro ambulance service stays for now. UnionTribune, San Diego. 13 June 2011. Available at: http://www.utsandiego.com/news/2011/jun/13/ruralmetro-ambulance-service-stays-now/. Accessed December 22, 2011.
31. Centers for Disease Control ambulance crash related injuries amongEmergency Medical Service workers—United States 1991–2000.MMWR Morb Mortal Wkly Rep 2003;52:154–6.
32. Improving safety in Helicopter Emergency Medical Services(HEMS) operations. Alexandria, VA: Helicopter Association Inter-national; 2005.
33. Special investigation report on Emergency Medical Services opera-tions (2001-06, NTSB/SIR-06/01). Washington, DC: NationalTransportation Safety Board; 2006.

Pediatric Poison and Hemodialysis 1107
ARTICLE SUMMARY
1. Why is this topic important?There is a general paucity of data involving the use of
hemodialysis and other extracorporeal removal tech-niques in the treatment of pediatric and adolescent poison-ing. To our knowledge, this is the first descriptive study onthe use of these techniques after acute poisoning in thispopulation.2. What does this study attempt to show?
This study characterizes the demographics of pediatricand adolescent poisoning for which hemodialysis or otherextracorporeal removal techniques were employed, thetoxins encountered, reasons for hemodialysis, and the rel-ative contribution of blood toxin concentrations to the de-cision to institute hemodialysis or other extracorporealremoval technique.3. What are the key findings?
Hemodialysis is the primarymethod employed after pe-diatric and adolescent poisoning, however, hemoperfu-sion and hemofiltration are used. Indications for dialysisincluded removal of the toxic product or renal support.Ethylene glycol and methanol levels did not influencethe decision to institute hemodialysis. Patients with salic-ylate poisoning demonstrated considerable toxicity de-spite levels below those often proposed as indicationsfor dialysis.4. How is patient care impacted?
Physicians should make decisions about instituting he-modialysis or other extracorporeal removal techniquesbased on clinical findings rather than on blood toxin con-centrations alone.