Embed Size (px)
Citation preview

Hemochromatosis
• Disorder of iron metabolism leading to progressive iron loading mainly involving the parenchymal cells of the liver, pancreas and heart.
• When the disease is fully developed, organ structure and function are impaired as a consequence of the toxic effect of the free iron component

Hemochromatosis Primary iron overload
Hereditary hemochromatosis (HH)– HFE-associated HH (C282Y) (AR)– Non HFE-associated HH
• TfR2 mutations (AR)• Ferroportin mutations (AD)• Other mutations...
– Juvenile H– Solomon Islands HH (AD)
African (Sub-Saharian) H– Heredity not yet characterised

Hemochromatosis
Secondary iron overload
– Chronic anemias– Thalassemia major– Sideroblastic anemia– Congenital atransferrinemia– Aceruloplasminemia– Porfiria cutanea tarda– Polymetabolic syndrome

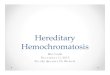
METABOLISMO DEL FERRO IN SOGGETTI NORMALI
Assorbimento ~ 1 mg/die
Perdite ~ 1 mg/die
Tessuti (mioglobina-enzimi)
140 mg - ~ 1 mg
Trasporto (transferrina)
3 mg
Serie eritroide (emoglobina)
2500 mg
Scorte (fegato, SRE)
(ferritina ed emosiderina) 100 / 400 mg - 1000mg
1,5-2 mg/die

EMOCROMATOSI GENETICA
• L’emocromatosi genetica, trasmessa con carattere autosomico recessivo, è caratterizzata da sovraccarico di ferro, a carico degli organi parenchimali.
• Il gene (HFE) responsabile è localizzato sul braccio corto del cromosoma 6, con due mutazioni importanti: - C282Y - H63D
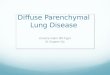
• La proteina HFE è situata a livello delle cripte intestinali in associazione con la beta-2 microglobulina ed il recettore della transferrina.

Fe3+ Fe2+
DCytB
Fe2+Ferritin
Fe2+
Fe2+
H+ DMT1
Fe2+ FerroportinFe3+
HephaestinFe-Tf
Intestinallumen
Vascular lumenTransferrin receptor (TfR)
HFE
Iron absorption

EMOCROMATOSI GENETICA
• La proteina mutata induce un aumento dell’assorbimento intestinale del ferro.
• Il quadro clinico si manifesta: nei soggetti omozigoti (C282Y+/+) (60-100%) nei soggetti con doppia eterozigosi (10%)
• Il 5% della popolazione normale presenta uno stato di eterozigosi per le due mutazioni C282Y eH63D

Genotype / PhenotypeGenotype Prevalence (%) Usual phenotype
G. Pop. HH
C282Y (+/+) 0.5 60-100 HH with variable grade of expression
C282Y (+/-) 13 3 Normal
H63D (+/+) 2 2 NormalRisk of iron overload < 0.2%
H63D (+/-) 25 2-3 Normal
C282Y/H63D 4 4 Normal:0.5-1.0% mild iron overload
Wild type 60-90 0-36 Normal Remember non-HFE associated HH !!
HFE - HH

Factors influencing phenotypic Factors influencing phenotypic expression of HH (liver damage)expression of HH (liver damage)
- Alcohol abuse- Anti HCV-positivity- HBsAg positivity- -thalassemia trait
- NASH

MECCANISMI PATOGENETICI DELLA TOSSICITA’ DA FERRO
Emocromatosi
Aumentato assorbimento di
ferro
Sovraccarico di ferro epatico
Effetto sul DNA epatico
Perossidazione lipidica delle membrane
Necrosi cellulare
Fibrosi Cirrosi
Epatocarcinoma
Aumentata sintesi di collagene nelle
cellule stellate

EMOCROMATOSI CLINICA
Il quadro clinico diventa evidente tra IV e V decade di vita ed è caratterizzato da :
epatomegalia 65%
iperpigmentazione cutanea 35%
diabete mellito 25%
cardiomiopatia dilatativa 20%
ipogonadismo ipogonadotropo 20%
poliartrite cronica 10-15%

-

-

DIAGNOSI• Il sospetto diagnostico di emocromatosi si basa sulla
storia familiare, le manifestazioni cliniche, l’aumento della percentuale di saturazione della transferrina (vn 40%) e della ferritina sierica (vn 200 ng/mL nelle femmine, 300 ng/mL nei maschi)
• Un’iperferritinemia può essere riscontrata anche in corso di processi infettivi, neoplastici o nell’abuso alcolico; è pertanto un insieme di dati che suggerisce la diagnosi di emocromatosi
• Biopsia epatica / RMN (Hepatic Iron Index): - età > 40 aa - transaminasi elevate - ferritina serica > 1.000 ng/ml

CLINICA
• L’accumulo di ferro a livello epatico porta allo sviluppo di cirrosi e delle sue complicanze
• La più frequente causa di morte è l’epatocarcinoma,
che si sviluppa su fegato cirrotico, specie a partire dai cosiddetti “foci ferro- privi”, che vanno considerati lesioni pre-neoplastiche

DIAGNOSI
• Il sospetto di emocromatosi trova definitiva conferma nella biopsia epatica, con valutazione del contenuto di ferro parenchimale
• Nelle fasi precoci della malattia: - siderosi è prevalente negli epatociti; - interessamento più tardivo delle cellule del sistema reticolo-endoteliale; - accumulo di ferro con distribuzione periportale

CLINICA
• La malattia esordisce più frequentemente tra la IV e la V decade di vita, in relazione al lungo tempo necessario perché il ferro raggiunga concentrazioni tali da condizionare insufficienza funzionale degli organi colpiti. La malattia conclamata è prevalente nei maschi.
• Il quadro clinico è manifesto solo nei soggetti omozigoti, mentre negli eterozigoti è silente anche in presenza di cofattori (virus, alcol, ecc)

EMOCROMATOSI GENETICA
• La proteina mutata induce un aumento dell’assorbimento intestinale del ferro.
• Il quadro clinico si manifesta: nei soggetti omozigoti (C282Y+/+) (60-100%) nei soggetti con doppia eterozigosi (10%)
• Variabilità fenotipica: omozigoti C282Y+/+ senza fenotipo di HH omozigoti C282Y -/- con fenotipo di HH
• Il 5% della popolazione normale presenta uno stato di eterozigosi per le due mutazioni C282Y eH63D

EMOCROMATOSI GENETICA
• L’emocromatosi genetica, trasmessa con carattere autosomico recessivo, è caratterizzata da sovraccarico di ferro, a carico degli organi parenchimali.
• Il gene (HFE) responsabile è localizzato sul braccio corto del cromosoma 6, con due mutazioni importanti.
• Il gene è in stretta vicinanza con il complesso HLA; si ha una stretta associazione con l’antigene HLA-A3 (fino al 75%) e con minor frequenza con gli antigeni B7 e B14

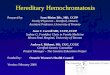
Iron MetabolismIron MetabolismCirculating erythrocytes
Erythroid Hepatocytes R E cells
bone marrow
Tf (plasma)
Other GI iron absorptioncells

HH- Approximate prevalence in HH- Approximate prevalence in comparison with other autosomal recessive comparison with other autosomal recessive
diseasesdiseasesDisease Homozygote (q2) Mutant gene(q)
Heterozygote (2pq)*
HH 1:400 1:20 1:10
1ATD 1:600 1:40 1:20
CF 1:2500 1:50 1:25
PKU 1:10.000 1:100 1:50
WD 1:100.000 1:300 1:150
*Hardy-Weimberg equilibrium

HH - Gene(s) and disease(s)HH - Gene(s) and disease(s)
HH Type 1 2A 2B 3 4
Chr. 6 1 19 7 2
Clin. HFE HJV Non-HFE Non-HFE Non-HFE
Mut. C282Y ND Hepc TfR 2 FPN 1

HH - FrequencyHH - Frequency
# / 1000 95% CI
Overall 4.5 (3.3-5.8)
Caucasians 5.4 (4.0-7.1)
Male / Female ratio 1.8 : 1

Type 1 HH ( HFE - HH )
Late onset
Prevalent in males
Low penetrance
AR
Intestinal iron absorption not maximal

HFE-HH HFE-HH
Cloned in 1996Located 4.5 Mb telomeric to the HLA-A locus on chromosome 6Encodes an HLA-class Ib proteinTwo missense mutations described:
Cys 282 Tyr ( C 282 Y ) 60-100% +/+ in clinical HH
His 63 Asp ( H 63 D )
5% of the general population: compound heterozygosityC282Y/H63D

Problems to be considered for C282Y mutation
C 282 Y + / + without phenotipic expressed
C 282 Y - / - with fully developed disease
Possible role of :- other mutation (s) on the same gene- other gene(s) - cofactor(s)

C282Y: Penetrance
It depends upon: age, sex and evaluated population ( 1-70% for males in different studies )
Genotype: it indicates the susceptibility to the disease
The concurrent role of genetic and environmental factors are mandatory

HH- Clinical findings (I)HH- Clinical findings (I)• “Classical” presentation with liver disease, diabetes and
pigmentation occurs now in less than 5% !
• Pre-symptomatic stage always more frequent due to:- General population screening- Incidental finding- Family screening- Screening of groups at higher risk for HH
• Symptomatic stage: significant relation between liver iron concentration and clinical findings

HH- Clinical findings (II)HH- Clinical findings (II)- Chronic parenchymal liver disease, including HCC
- Cardiomyopathy and/or arrhythmias
- Diabetes mellitus type I and II
- Impotence, loss of libido
- Amenorrhea / Infertility
- Anterior pituitary failure
- Arthritis and arthralgia (particularly in association with chondrocalcinosis)
- Inappropriately increased skin pigmentation
- Porphyria cutanea tarda

HH - Groups at higher riskHH - Groups at higher risk
• Siblings of HH probands
• Patients with:– Diffusely increased skin pigmentation– Dilative cardiomyopathy– Diabetes mellitus (especially NID)– Arthropathy of non obvious rheumatologic
etiology

HH - DiabetesHH - Diabetes
Diabetics (# 894) Controls (# 467)
M/F (#) 418 / 476 234 / 233
Age (yrs, mean+SD) 62+9 60+11
HH (#) 12 (NIDDM) 1
% (95% CI) 1.34 (0.7-2.3) 0.2 (0.01-1.1)
ODD RATIO HH / DIABETES 6.3 (95% C I 1.1-37.7)