Embed Size (px)
Citation preview

Hemimegalencephaly: Evaluation with Positron Emission Tomography
Pertti J. Rintahaka, MD*t~, Harry T. Chugani, MD*t~, Cristina Messa, MD§, and Michael E. Phelps, PhD§
We performed positron emission tomographic (PET) studies with 2-deoxy-2[lSF]fluoro-D-glucose in 8 chil- dren with hemimegalencephaly (HME). HME is a developmental brain malformation associated with epilepsy, hemianopsia, and varying degrees of develop- mental delay. We hypothesized that the relatively poor overall developmental outcome of surgically hemi- spherectomized HME patients as a group, compared to children undergoing hemispherectomy for Sturge- Weber syndrome or chronic focal encephalitis, is re- lated to dysfunction of the structurally "normal" non- lIME side and that PET would be helpful in the pre- surgical evaluation of HME patients with intractable epilepsy. Visual analysis of the non-HME side on PET clearly revealed evidence of cortical hypometabolism in 4 patients compared to controls. Seven children un- derwent epilepsy surgery. One child had a glucose metabolic pattern suggesting a cortical lamination defect in the non-HME hemisphere, bilateral inde- pendent seizure onset, and was not considered to be a surgical candidate. We found a general correlation be- tween the pattern of glucose utilization in the less af- fected hemisphere and prognosis. Although the follow- up periods are short, it is recommended that HME children with intractable epilepsy undergo hemispher- ectomy in the first year of life in order to allow maxi- mal brain plasticity to occur; however, preoperative evaluation should also include an assessment of the integrity of the non-HME hemisphere.
Rintahaka P J, Chugani HT, Messa C, Phelps ME. Hemi- megalencephaly: Evaluation with positron emission to-
mography. Pediatr Neurol 1993;9:21-8.
Introduction
Hemimegalencephaly (HME) is a rare developmental
brain malformation characterized by congenital hyper- trophy of one cerebral hemisphere and ipsilateral ventric- ulomegaly [1-5]. Patients with HME are categorized into two groups: those with normal body symmetry and those
with body hemihypertrophy or other unilateral congenital somatic abnormalities [6]. The extracranial manifestation may be confined to the facial region [7].
HME is associated with epilepsy, hemianopsia, and
varying degrees of developmental delay [3-5,7,8]. Epilep- sy in these children is often refractory to all antiepileptic
medications, in which case cerebral hemispherectomy is
recommended [9]. Despite seizure control postoperatively, HME patients
as a group have a worse developmental outcome when
compared to other children undergoing hemispherectomy for intractable epilepsy, such as those with chronic focal
encephalitis of Rasmussen [10] or Sturge-Weber syn- drome [ 11 ].
The worse outcome in cognitive function of HME
patients is suspected to be related to a contralateral hemi-
sphere that is not entirely normal and, therefore, is in- capable of optimum reorganization of function prior to
and following hemispherectomy. In our study, we address the issue of functional integ-
rity - defined in this study as a normal pattern of glucose uptake - of the less affected hemisphere in HME patients using positron emission tomography (PET) of cerebral glucose utilization. The findings of PET are related to clinical features in 8 patients.
Methods
Patient Population. HME in this study was defined as all or most of one hemisphere being larger than the other, and the contralateral side appearing relatively normal structurally on computed tomography (CT), magnetic resonance imaging (MRI), or both. There were 7 boys and 1 girl in our series of HME patients. Clinical findings are presented in Table 1. Not all patients had increased head circumferences (Table 1). All had been admitted to UCLA Medical Center because of intractable epilepsy. The mean age of children at PET was 16 months (range: 2-41 months; Table 2).
The diagnosis of HME was made with CT, MRI, or both. The HME side was on the right in 3 patients (Table 2). Hemianopsia was present in 6 children, but difficult to verify in the remaining 2 (Patients 4,5) be- cause of their young ages. Hemiparesis, present in all 8 patients, was mild in the 2 youngest. None of the patients had somatic hemihyper- trophy. No family history of brain malformation existed. Seizures began before 6 months of life and were focal in all 8 children.
From the Departments of *Neurology, *Pediatrics, *Brain Research Institute; and §Division of Nuclear Medicine and Biophysics and Laboratory of Nuclear Medicine; UCLA School of Medicine; Los Angeles, California; 1Department of Neuropediatrics; Aurora Hospital; Helsinki, Finland.
Communications should be addressed to: Dr. Chugani; Division of Pediatric Neurology; Room MDCC 22-464; UCLA School of Medicine; Los Angeles, CA 90024. Received May 18, 1992; accepted September 10, 1992.
Rintahaka et al: PET in Hemimegalencephaly 21
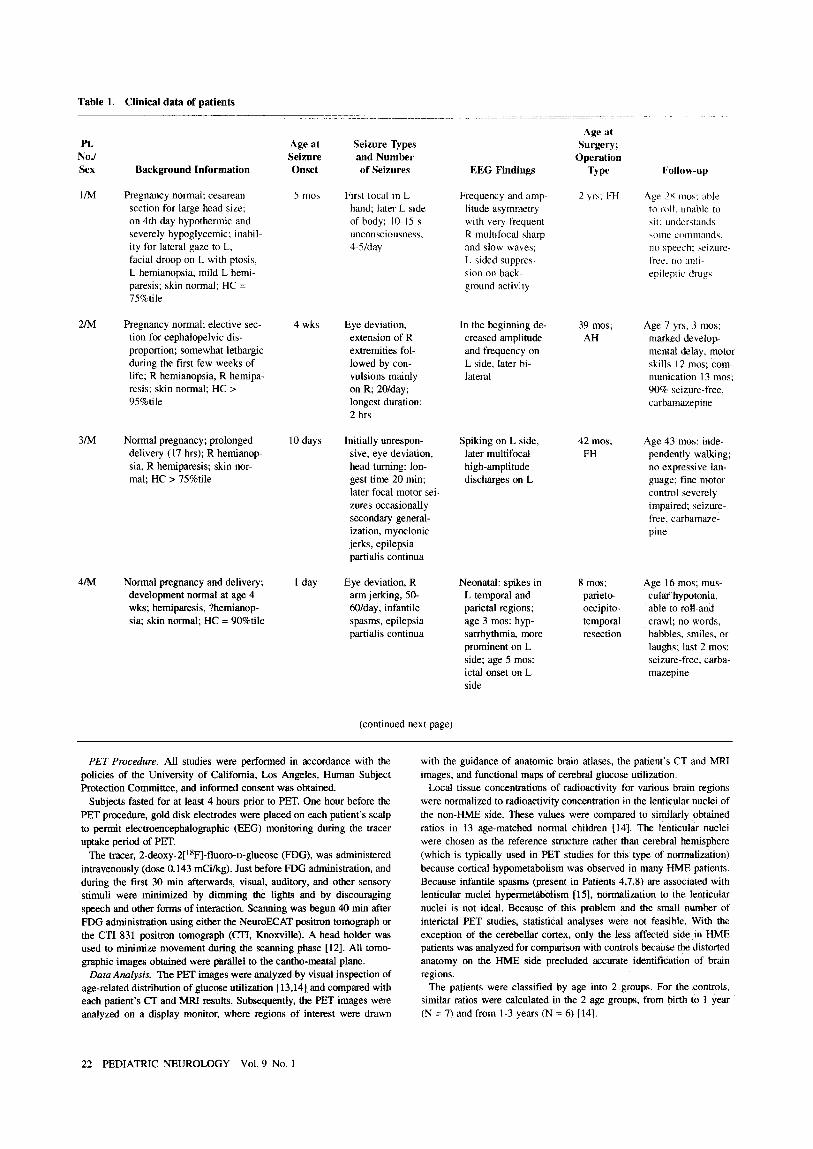
Table I. Clinical data of patients
Age at Pt. Age at Seizure Types Surgery;
No./ Seizure and Number Operation Sex Background Information Onset of Seizures EEG Findings Type I:ollow-up
IIM Pregnancy normal; cesarean 5 mos First tbcal in L Frequency and amp- 2 yrs; FH section for large head size; hand; later L side litude asymmetry on 4th day hypothermic and of body; 10-15 s with very frequent severely hypoglycemic; inabil- unconsciousness, R multifocal sharp ity for lateral gaze to L, 4-5/day and slow waves; facial droop on L with ptosis, L-sided suppres- L hemianopsia, mild L hemi- sion on back- paresis; skin normal; HC = ground activity 75%tile
Age 28 mos: able to roll. unable to sit: understands '-;Ollle coin lnl.nlds.
no speech: seizure- free. ao a l l [ i
epileptic drugs
2/M Pregnancy normal; elective sec- 4 wks Eye deviation, In the beginning de- 39 mos; tion for cephalopelvic dis- extension of R creased amplitude AH proportion; somewhat lethargic extremities fol- and frequency on during the first few weeks of lowed by con- L side, later bi- life; R hemianopsia, R hemipa- vulsions mainly lateral resis; skin normal; HC > on R; 20/day; 95%tile longest duration:
2 hrs
Age 7 yrs, 3 mos; marked develop- mental delay, motor skills 12 mos; com- munication 13 mos; 90% seizure-free, carbamazepine
3/M Normal pregnancy; prolonged 10 days Initially unrespon- Spiking on L side, 42 mos; delivery (17 hrs); R hemianop- sive, eye deviation, later multifocal FH sia, R hemiparesis; skin nor- head turning: Ion- high-amplitude mal; HC > 75%tile gest time 20 rain; discharges on L
later focal motor sei- zures occasionally secondary general- ization, myoclonic jerks, epilepsia partialis continua
Age 43 mos: inde- pendently walking; no expressive lan- guage; fine motor control severely impaired; seizure- tree, carbam~e- pine
4/M Normal pregnancy and delivery; 1 day development normal at age 4 wks; hemiparesis, ?hemianop- sia; skin normal; HC = 90%tile
Eye deviation, R Neonatal: spikes in 8 mos; arm jerking, 50- L temporal and parieto- 60/day, infantile parietal regions; occipito- spasms, epilepsia age 3 mos: hyp- temporal partialis continua sarrhythmia, more resection
prominent on L side; age 5 mos: ictal onset on L side
Age 16 mos; mus- cular hypotonia, able to mU and crawl; no words, babbles, smiles, or laughs; last 2 mos: seizure-free, carba- mazepinc
(continued next page)
PET Procedure. All studies were performed in accordance with the policies of the University of California, Los Angeles, Human Subject Protection Committee, and informed consent was obtained.
Subjects fasted for at least 4 hours prior to PET. One hour before the PET procedure, gold disk electrodes were placed on each patient's scalp to permit electroencephalographic (EEG) monitoring during the tracer uptake period of PET.
The tracer, 2-deoxy-2[18F]-fluoro-D-glucose (FDG), was administered intravenously (dose 0.143 mCi/kg). Just before FDG administration, and during the first 30 min afterwards, visual, auditory, and other sensory stimuli were minimized by dimming the lights and by discouraging speech and other forms of interaction. Scanning was begun 40 min after FDG administration using either the NeuroECAT positron tomograph or the CTI 831 positron tomograph (CTI, Knoxville). A head holder was used to minimize movement during the scanning phase [12]. All tomo- graphic images obtained were parallel to the cantho-meatal plane.
Data Analysis. The PET images were analyzed by visual inspection of age-related distribution of glucose utilization [13,14] and compared with each patient's CT and MRI results. Subsequently, the PET images were analyzed on a display monitor, where regions of interest were drawn
with the guidance of anatomic brain atlases, the patient's CT and MRI images, and functional maps of cerebral glucose utilization.
Local tissue concentrations of radioactivity for various brain regions were normalized to radioactivity concentration in the lenticular nuclei of the non-HME side. These values were compared to similarly obtained ratios in 13 age-matched normal children [14]. The lenticular nuclei were chosen as the reference structure rather than cerebral hemisphere (which is typically used in PET studies for this type of normalization because cortical hypometabolism was observed in many HME patients. Because infantile spasms (present in Patients 4,7,8) are associated with lenticular nuclei hypermetabolism [15], normalization to the lenticnlar nuclei is not ideal. Because of this problem and the small number of interictal PET studies, statistical analyses were not feasible. With the exception of the cerebellar cortex, only the less affected side in HME patients was analyzed for comparison with controls because the distorted anatomy on the HME side precluded accurate identification of brain regions.
The patients were classified by age into 2 groups For the controls. similar ratios were calculated in the 2 age groups, from birth to 1 year (N = 7) and from 1-3 years (N = 6) [14].
22 PEDIATRIC NEUROLOGY Vol. 9 No. 1
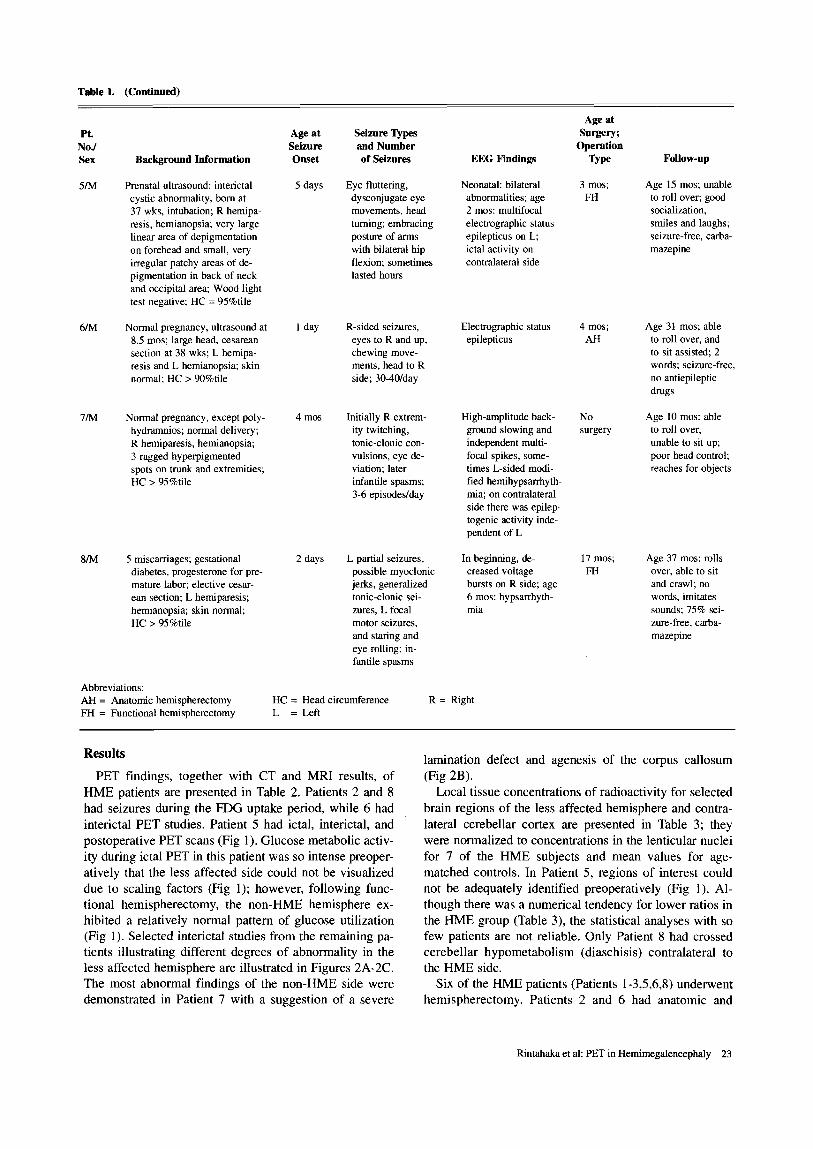
Table I. (Continued)
PL Age at Nod Seizure Sex Background Information Onset
5/M Prenatal ultrasound: interictal 5 days cystic abnormality, born at 37 wks, intubation; R hemipa- resis, hemianopsia; very large linear area of depigmentation on forehead and small, very irregular patchy areas of de- pigmentation in back of neck and occipital area; Wood light test negative; HC = 95%tile
6/M Normal pregnancy, ultrasound at 1 day 8.5 mos; large head, cesarean section at 38 wks; L hemipa- resis and L hemianopsia; skin normal; HC > 90%tile
7/M Normal pregnancy, except poly- 4 mos hydramnios; normal delivery; R hemiparesis, hemianopsia; 3 ragged hyperpigmented spots on trunk and extremities; HC > 95%tile
8/M 5 miscarriages; gestational 2 days diabetes, progesterone for pre- mature labor; elective cesar- ean section; L hemiparesis; hemianopsia; skin normal; HC > 95%tile
Abbreviations: Al l = Anatomic hemispherectomy FH = Functional hemispherectomy
Seizure Types and Number of Seizures
Eye fluttering, dysconjugate eye movements, head turning; embracing posture of arms with bilateral hip flexion; sometimes lasted hours
R-sided seizures, eyes to R and up, chewing move- ments, head to R side; 30-40/day
Initially R extrem- ity twitching, tonic-clonic con- vulsions, eye de- viation; later infantile spasms; 3-6 episodes/day
L partial seizures, possible myoclonic jerks, generalized tonic-clonic sei- zures, L focal motor seizures, and stating and eye rolling; in- fantile spasms
HC = Head circumference L = Left
EEG Findings
Neonatal: bilateral abnormalities; age 2 mos: multifocal electrographic status epilepticus on L; ictal activity on contralateral side
Electrographic status epilepticus
High-amplitude back- ground slowing and independent multi- focal spikes, some- times L-sided modi- fied hemihypsarrhyth- mia; on contralateral side there was epilep- togenic activity inde- pendent of L
In beginning, de- creased voltage bursts on R side; age 6 mos: hypsarrhyth- mia
R = Right
Age at Surgery;
Operation Type
3 mos; FH
4 mos; AH
No su~ery
17 mos; FH
Follow-up
Age 15 mos; unable to roll over; good socialization, smiles and laughs; seizure-free, carba- mazepine
Age 31 mos; able to roll over, and to sit assisted; 2 words; seizure-free, no antiepileptic drugs
Age 10 mos: able to roll over, unable to sit up; poor head control; reaches for objects
Age 37 mos: rolls over, able to sit and crawl; no words, imitates sounds; 75% sei- zure-free, carba- mazepine
Results
PET findings, together with CT and MRI results, of HME patients are presented in Table 2. Patients 2 and 8 had seizures during the FDG uptake period, while 6 had interictal PET studies. Patient 5 had ictal, interictal, and postoperative PET scans (Fig 1). Glucose metabolic activ- ity during ictal PET in this patient was so intense preoper- atively that the less affected side could not be visualized due to scaling factors (Fig 1); however, following func- tional hemispherectomy, the non-HME hemisphere ex- hibited a relatively normal pattern of glucose utilization (Fig 1). Selected interictal studies from the remaining pa- tients illustrating different degrees of abnormality in the less affected hemisphere are illustrated in Figures 2A-2C. The most abnormal findings of the non-HME side were demonstrated in Patient 7 with a suggestion of a severe
lamination defect and agenesis of the corpus callosum (Fig 2B).
Local tissue concentrations of radioactivity for selected brain regions of the less affected hemisphere and contra- lateral cerebellar cortex are presented in Table 3; they were normalized to concentrations in the lenticular nuclei for 7 of the HME subjects and mean values for age- matched controls. In Patient 5, regions of interest could not be adequately identified preoperatively (Fig 1). Al- though there was a numerical tendency for lower ratios in the HME group (Table 3), the statistical analyses with so few patients are not reliable. Only Patient 8 had crossed cerebellar hypometabolism (diaschisis) contralateral to the HME side.
Six of the HME patients (Patients 1-3,5,6,8) underwent hemispherectomy. Patients 2 and 6 had anatomic and
Rintahaka et al: PET in Hemimegalencephaly 23
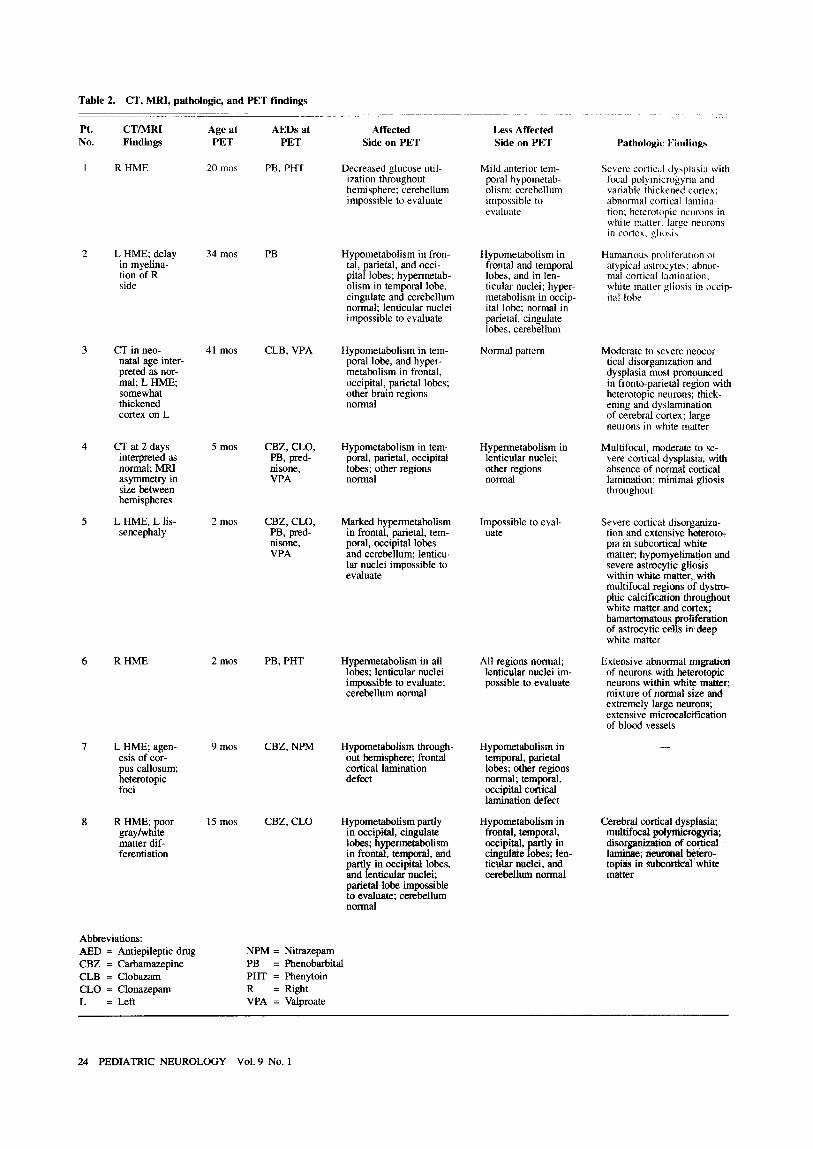
Table 2. CT, MRI, pathologic, and PET findings
Pt. CT/MRI Age at AEDs at No. Findings PET PET
Affected Less Affected Side on PET Side on PET Pathologic Findings
1 R HME 20 mos PB, PHT
2 L HME; delay 34 mos PB in myelina- tion of R side
3 CT in neo- 41 mos natal age inter- preted as nor- mal; L HME; somewhat thickened cortex on L
4 CT at 2 days 5 mos interpreted as normal; MRI asymmetry in size between hemispheres
5 L HME, L lis- 2 mos sencephaly
6 R HME 2 mos
7 L HME; agen- 9 mos esis of cor- pus callosum; heterotopic foci
8 R HME; poor 15 mos gray/white matter dif- ferentiation
CLB, VPA
CBZ, CLO, PB, pred- nisone, VPA
CBZ, CLO, PB, pred- nisone, VPA
PB, PHT
CBZ, NPM
CBZ, CLO
Decreased glucose util- ization throughout hemisphere; cerebellum impossible to evaluate
Hypometabolism in fron- tal, parietal, and occi- pital lobes; hypermetab- olism in temporal lobe, cingulate and cerebellum normal; lenticular nuclei impossible to evaluate
Hypometabolism in tem- poral lobe, and hyper- metabolism in frontal, occipital, parietal lobes; other brain regions normal
Hypometabolism in tem- poral, parietal, occipital lobes; other regions normal
Marked hypermetabolism in frontal, parietal, tem- poral, occipital lobes and cerebellum; lenticu- lar nuclei impossible to evaluate
Hypermetabolism in all lobes; lenticular nuclei impossible to evaluate; cerebellum normal
Hypometabolism through- out hemisphere; frontal cortical lamination defect
Hypometabolism partly in occipital, cingulate lobes; hypermetabolism in frontal, te.m{K~..., and partly in occipttal lobes, and lenticular nuclei; parietal lobe impossible to evaluate; cerebellum normal
Mild anterior tem- poral hypometab- olism; cerebellum impossible to evaluate
Hypometabolism in frontal and temporal lobes, and in len- ticular nuclei; hyper- metabolism in occip- ital lobe; normal in parietal, cingulate lobes, cerebellum
Normal pattern
Hypermetabolism in lenticular nuclei; other regions normal
Impossible to eval- uate
All regions normal; lenticular nuclei im- possible to evaluate
Hypometabolism in temporal, parietal lobes; other regions normal; temporal, occipital cortical lamination defect
Hypometabolism in frontal, temporal, occipital, partly in cingulate lobes; len- ticutar nuclei, and cerebellum normal
Severe cortical dysplasia with focal polymicrogyria and variable thickened cortex; abnormal cortical lamina- tion; heterotopic neurons in white matter: large neurons in cortex, gliosis
Hamartous proliteration ol atypical astrocytes; abnor- mal cortical lamination: white matter gliosis in occip- ital lobe
Moderate to severe ueocor- tical disorganization and dysplasia most pronounced in fronto-parietal region with heterotopic neurons; thick- ening and dyslamination of cerebral cortex; large neurons in white matter
Multifocal, moderate to se- vere cortical dysplasia, with absence of normal cortical lamination; minimal gliosis throughout
Severe conical disorganiza- tion and extensive heteroto- pia in subcorticat white matter; hypomyelination and severe astrocytic gliosis within white matter, with multifocal regions of dystro- phic calcification throughout white matter and cortex; hamartomatous proliferation of astrocytic cells in deep white matter
Extensive abnormal migration of neurons with heterotopic neurons within white matter; mixture of normal size and extremely large neurons; extensive microcalcification of blood vessels
Cerebral cortical dysplasia; multifocal polymicrogyria; disorganization of cortical 1 ~ ; n o n ~ a l betero- topias in subcortical white matter
Abbreviations: AED = Antiepileptic drug CBZ = Carbamazepine CLB = Clobazam CLO = Clonazepam L = Left
NPM = Nitrazepam PB = Phenobarbital PHT = Phenytoin R = Right VPA = Valproate
24 PEDIATRIC NEUROLOGY Vol. 9 No. 1
Figure 1. lctal, interictal, and postoperative interictal scans in Patient 5. lctal scan: because of the intense glucose utilization throughout the affected side the whole opposite hemisphere (arrow) is almost invisible due to scaling factors. Interictal scan: hyper- metabolism (associated with intense spike-and-wave activity on EEG) is observed inter- ictally throughout the HME hemisphere, but is not as marked as in the ictal study. Postoperative interictal scan: reveals a relatively normal glucose metabolic pattern in the cortical areas of the non-HME hemisphere; however, hypermetabolism in the frontal lobe of the affected side persists following functional hemispherectomy. Dotted lines are in the interhemispheric fissure.
Patients 1, 3, 5, and 8 had functional hemispherectomy. One infant (Patient 4) had parieto-occipito-temporal resection. Surgery type and preliminary results of opera- tion are included in Table 1. The pathologic-anatomic findings are listed in Table 2.
The mean age of the patients when last evaluated was 3 years, 2 months (range: 16 months to 7 years). The mean follow-up time since operation was 16 months (range: 1 month to 4 years). All of the children who required sur- gery had fewer seizures after the procedure. Patients 1, 3, 5, and 6 were seizure-free (Table 1). The remaining 3 children who had surgery had 75-90% diminution in sei- zure frequency. Although developmental delay persisted in all of the surgically treated children, parents reported increased alertness and more cognitive interaction.
Discussion
We used PET to study cerebral glucose utilization in 8 patients with HME. All had intractable epilepsy which began earlier than in subjects reported from other studies [3-5,7,8,16]. Our patients did not have any distinct neuro- cutaneous syndrome which, in some patients with HME, is associated with milder neurologic symptoms [ 16].
In our patients, CT, MRI, and PET findings correlated well with the clinical findings of hemiparesis and hemian-
opsia. This relationship has also been observed in studies using single photon emission computed tomography (SPECT) [ 17].
Patient 7 had agenesis of the corpus callosum which, to our knowledge, has not been described in HME patients. Interestingly, Patient 7 also had a metabolic pattern sug- gesting a cortical lamination defect, which was not ob- vious on MRI. Therefore, PET may provide supplemen- tary information to MRI in evaluating HME patients.
P E T a n d H M E . PET is a noninvasive method used to study metabolism of the brain [ 18] and has proved to be useful in the understanding of many neuropediatfic syn- dromes and epilepsy [15,19-23]. Our study demonstrates that PET can provide unique information that is useful in the management of patients with HME. On the side of HME, there was a good correlation between CT/MRI and PET in delineating areas of abnormality; however, PET clearly revealed that many brain regions, particularly on the non-HME side, which appeared to be normal struc- turally were functionally abnormal. The typical focal ab- normality on PET was hypometabolism in the cortical regions; however, there was no consistent pattern in the distribution of hypometabolism among patients.
Glucose utilization was impossible to analyze reliably on the HME side due to malformed anatomy. In a SPECT
Rintahaka et al: PET in Hemimegalencephaly 25
A
B
-y¢
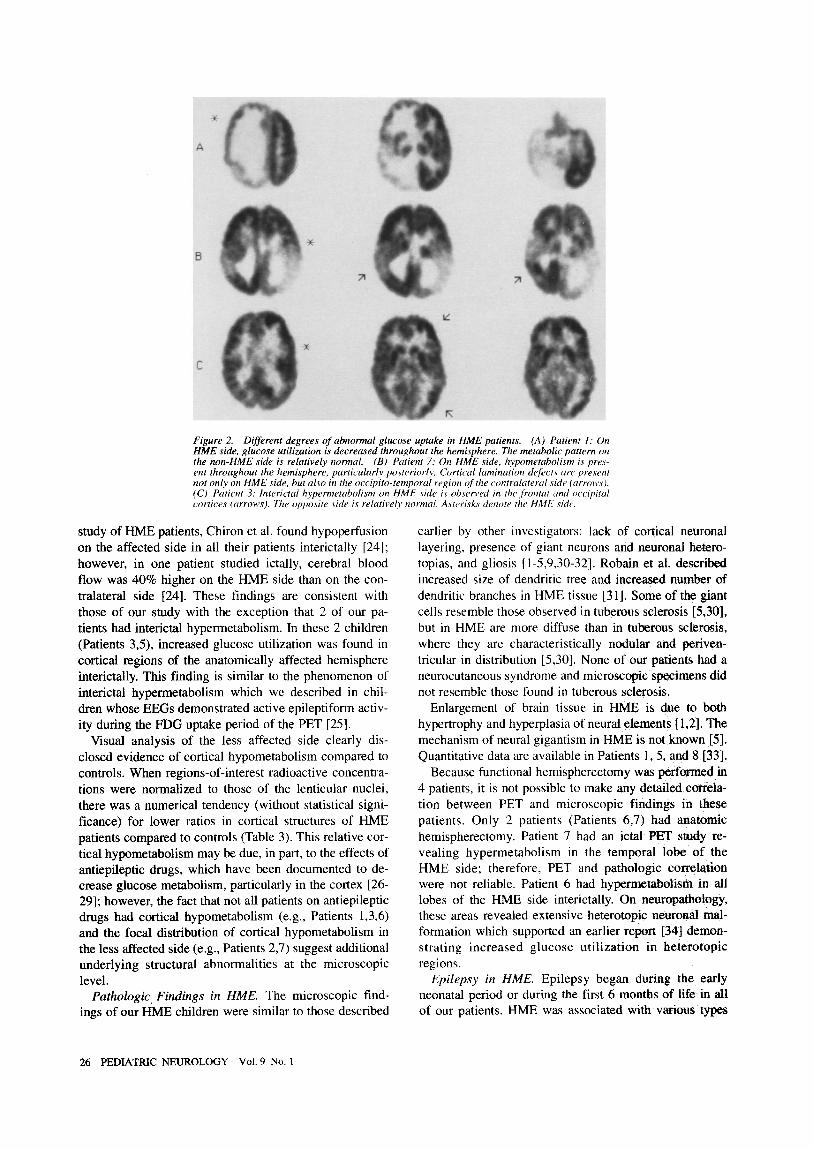
Figure 2. Different degrees o f abnormal glucose uptake in HME patients. (A) Patient 1: On HME side, glucose utilization is decreased throughout the hemisphere. The metabolic pattern on the non-HME side is relatively normal. (B) Patient 7: On HME side, hypometabolism is pres- ent throughout the hemisphere, particularly posterior(y. Cortical lamination defects are present not only, on HME side, but also in the occipito-temporal region of the contralateral side (arrows). (C) Patient 3: Interictal hypermetabolism on HME side is obsera,ed in the .t~'ontal and occipital cortices (arrows). The opposite side is relatively normal. Asterisks denote the HME side.
study of HME patients, Chiron et al. found hypoperfusion on the affected side in all their patients interictally [241; however, in one patient studied ictally, cerebral blood flow was 40% higher on the HME side than on the con- tralateral side [24]. These findings are consistent with those of our study with the exception that 2 of our pa- tients had interictal hypermetabolism. In these 2 children (Patients 3,5), increased glucose utilization was found in cortical regions of the anatomically affected hemisphere interictally. This finding is similar to the phenomenon of interictal hypermetabolism which we described in chil- dren whose EEGs demonstrated active epileptiform activ- ity during the FDG uptake period of the PET [25].
Visual analysis of the less affected side clearly dis- closed evidence of cortical hypometabolism compared to controls. When regions-of-interest radioactive concentra- tions were normalized to those of the lenticular nuclei, there was a numerical tendency (without statistical signi- ficance) for lower ratios in cortical structures of HME patients compared to controls (Table 3). This relative cor- tical hypometabolism may be due, in part, to the effects of antiepileptic drugs, which have been documented to de- crease glucose metabolism, particularly in the cortex [26- 29]; however, the fact that not all patients on antiepileptic drugs had cortical hypometabolism (e.g., Patients 1,3,6) and the focal distribution of cortical hypometabolism in the less affected side (e.g., Patients 2,7) suggest additional underlying structural abnormalities at the microscopic level.
Pathologic Findings in HME. The microscopic find- ings of our HME children were similar to those described
earlier by other investigators: lack of cortical neuronal layering, presence of giant neurons and neuronal hetero- topias, and gliosis [1-5,9,30-32]. Robain et aL described increased size of dendritic tree and increased number of dendritic branches in HME tissue [31]. Some of the giant cells resemble those observed in tuberous sclerosis [5,30], but in HME are more diffuse than in tuberous sclerosis, where they are characteristically nodular and periven- tricular in distribution [5,30]. None of our patients had a neurocutaneous syndrome and microscopic specimens did not resemble those fbund in tuberous sclerosis.
Enlargement of brain tissue in HME is due to both hypertrophy and hyperplasia of neural elements [ 1,2]. The mechanism of neural gigantism in HME is not known [5]. Quantitative data are available in Patients 1,5, and 8 [33].
Because functional hemispherectomy was performed in 4 patients, it is not possible to make any detailed correla- tion between PET and microscopic findings in these patients. Only 2 patients (Patients 6,7) had anatomic hemispherectomy. Patient 7 had an ictal PET study re- vealing hypermetabolism in the temporal lobe of the HME side; therefore, PET and pathologic correlation were not reliable. Patient 6 had hypermetabolism in all lobes of the HME side interictally. On neuropathology, these areas revealed extensive heterotopic neuronal mal- formation which supported an earlier report [34] demon- strating increased glucose utilization in heterotopic regions.
Epilepsy in HME. Epilepsy began during the early neonatal period or during the first 6 months of life in all of our patients. HME was associated with various types
26 PEDIATRIC NEUROLOGY Vol. 9 No. 1
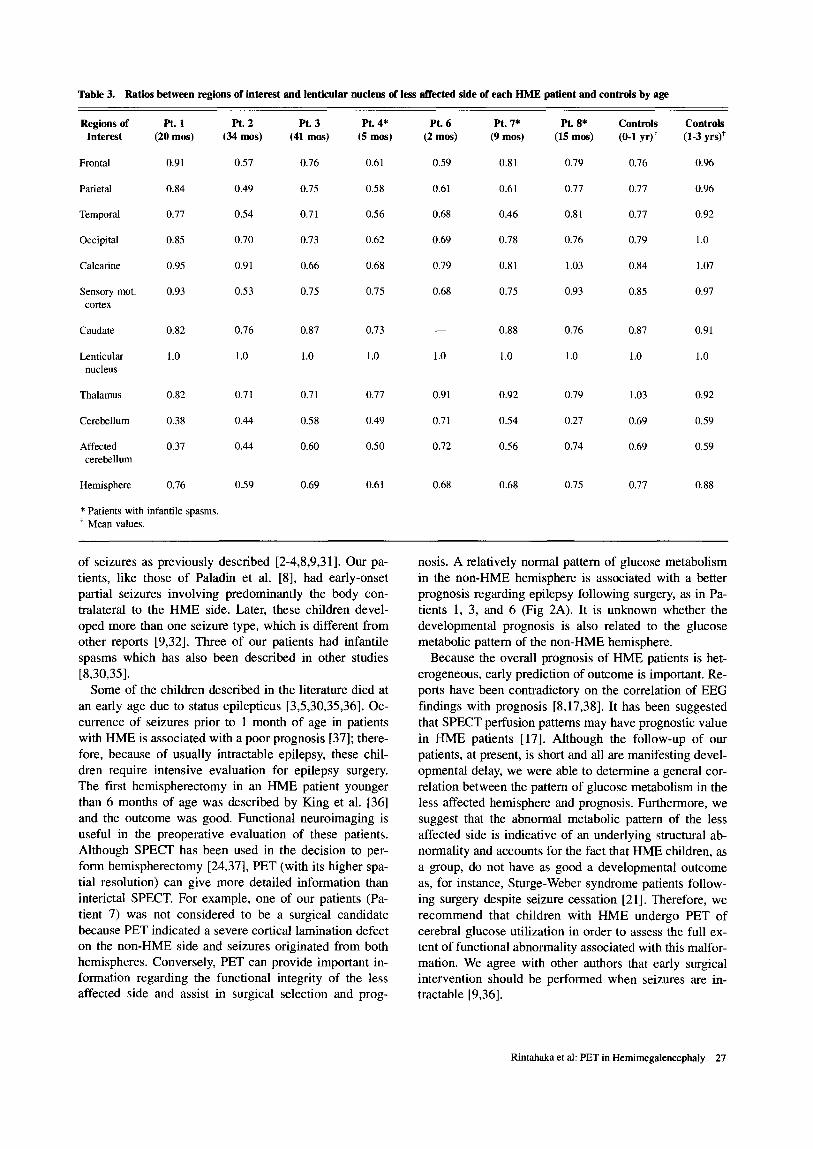
Table 3. Ratios between regions of interest and lenticular nucleus of less affected side of each HME patient and controls by age
Regions of Pt. 1 Pt. 2 Pt. 3 Pt. 4* Pt. 6 Pt. 7* Pt. 8* Controls Controls Interest (20 mos) (34 mos) (41 mos) (5 mos) (2 mos) (9 mos) (15 mos) (0-t yr)* (1-3 yrs)*
Frontal 0.91 0.57 0.76 0.61 0.59 0.81 0.79 0.76 0.96
Parietal 0.84 0.49 0.75 0.58 0.61 0.61 0.77 0.77 0.96
Temporal 0.77 0.54 0.71 0.56 0.68 0.46 0.81 0.77 0.92
Occipital 0.85 0.70 0.73 0.62 0.69 0.78 0.76 0.79 1.0
Calcarine 0.95 0.91 0.66 0.68 0.79 0.81 1.03 0.84 1.07
Sensory mot. 0.93 0.53 0.75 0.75 0.68 0.75 0.93 0.85 0.97 cortex
Caudate 0.82 0.76 0.87 0.73 - - 0.88 0.76 0.87 0.91
Lenticular 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 nucleus
Thalamus 0.82 0.71 0.71 0.77 0.91 0.92 0.79 1.03 0.92
Cerebellum 0.38 0.44 0.58 0.49 0.71 0.54 0.27 0.69 0.59
Affected 0.37 0.44 0.60 0.50 0.72 0.56 0.74 0.69 0.59 cerebellum
Hemisphere 0.76 0.59 0.69 0.61 0.68 0.68 0.75 0.77 0.88
* Patients with infantile spasms. t Mean values.
of seizures as previously described [2-4,8,9,31]. Our pa- tients, like those of Paladin et al. [8], had early-onset partial seizures involving predominantly the body con- tralateral to the HME side. Later, these children devel- oped more than one seizure type, which is different from other reports [9,32]. Three of our patients had infantile spasms which has also been described in other studies [8,30,35].
Some of the children described in the literature died at an early age due to status epilepticus [3,5,30,35,36]. Oc- currence of seizures prior to 1 month of age in patients with HME is associated with a poor prognosis [37]; there- fore, because of usually intractable epilepsy, these chil- dren require intensive evaluation for epi lepsy surgery. The first hemispherectomy in an HME patient younger than 6 months of age was described by King et al. [36] and the outcome was good. Functional neuroimaging is useful in the preoperative evaluation of these patients. Although SPECT has been used in the decision to per- form hemispherectomy [24,37], PET (with its higher spa- tial resolution) can give more detailed information than interictal SPECT. For example, one of our patients (Pa- tient 7) was not considered to be a surgical candidate because PET indicated a severe cortical lamination defect on the non-HME side and seizures originated from both hemispheres. Conversely, PET can provide important in- formation regarding the functional integrity of the less affected side and assist in surgical selection and prog-
nosis. A relatively normal pattern of glucose metabolism in the non-HME hemisphere is associated with a better prognosis regarding epilepsy following surgery, as in Pa- tients 1, 3, and 6 (Fig 2A). It is unknown whether the developmental prognosis is also related to the glucose metabolic pattern of the non-HME hemisphere.
Because the overall prognosis of HME patients is het- erogeneous, early prediction of outcome is important. Re- ports have been contradictory on the correlation of EEG findings with prognosis [8,17,38]. It has been suggested that SPECT perfusion patterns may have prognostic value in HME patients [17]. Although the follow-up of our patients, at present, is short and all are manifesting devel- opmental delay, we were able to determine a general cor- relation between the pattern of glucose metabolism in the less affected hemisphere and prognosis. Furthermore, we suggest that the abnormal metabolic pattern of the less affected side is indicative of an underlying structural ab- normality and accounts for the fact that HME children, as a group, do not have as good a developmental outcome as, for instance, Sturge-Weber syndrome patients follow- ing surgery despite seizure cessation [21]. Therefore, we recommend that chi ldren with HME undergo PET of cerebral glucose utilization in order to assess the full ex- tent of functional abnormality associated with this malfor- mation. We agree with other authors that early surgical intervention should be performed when seizures are in- tractable [9,36].
Rintahaka et al: PET in Hemimegalencephaly 27
We thank Dr. Harry V. Vinters for pathologic-anatomic information. We are indebted to the cyclotron staff for radionuclide production, the chemistry staff for FDG synthesis, and Ron Sumida. Larry Pang, Francine Aguilar, and Gloria Stocks for technical assistance.
Dr. Messa thanks Associazione per la Promozione delle Ricerche Neurologiche (ARIN) for financial support.
References
[1] Laurence KM. A case of unilateral megalencephaly. Dev Med Child Neurol 1964;6:585-90.
[21 Bigmani A, Palladini G, Zappella M. Unilateral megalencephaly with nerve cell hypertrophy. An anatomical and quantitative histochemi- cal study. Brain Res 1968;9:103-14.
[3] Townsend JJ, Nielsen SL, Malamud N. Unilateral megalen- cephaly: Hamartoma or neoplasm? Neurology 1975;25:448-53.
[4] Manz HJ, Phillips TM, Rowden G, McCullough DC. Unilateral megalencephaly, cerebral cortical dysplasia, neuronal hypertrophy, and heterotopia: Cytomorphometric, fluorometric cytochemical, and bio- chemical analyses. Acta Neuropathol 1979;45:97-103.
[5] Robain O, Floquet CH, Heldt N, Rozenberg E Hemimegalen- cephaly: A clinicopathological study of four cases. Neuropathol Appl Neurobiol 1988;14:125-35.
[6] Dekaban AS, Sakuragawa N. Megalencephaly. In: Vinken PJ, Bruyn GW, eds. Handbook of clinical neurology. Amsterdam: North- Holland, 1977;30:647-60.
[7] Trounce JQ, Rutter N, Mellor DH. Hemimegalencephaly: Diag- nosis and treatment. Dev Med Child Neurol 1991 ;33:261-6.
[8] Paladin F, Chiron C, Dulac O, Plouin P, Ponsot G. Electroen- cephalographic aspects of hemimegalencephaly. Dev Med Child Neurol 1989;31:377-83.
[9] Vigevano E Bertini E, Boldrini R, et al. Hemimegalencephaly and intractable epilepsy: Benefits of hemispherectomy. Epilepsia 1989; 30:833-4.
[10] Rasmussen T, Andermann F. Rasmussen's syndrome: Sympto- matology of the syndrome of chronic encephalitis and seizures. In: Luders H, ed. Epilepsy surgery. New York: Raven Press, 1991;173-82.
[11] Hoffman HJ, Hendrick EB, Dennis M, Armstrong D. Hemi- spherectomy for Sturge-Weber syndrome. Childs Brain 1979;5:233-48.
[12] Mazziotta JC, Phelps ME, Meadors AK, Ricci A, Winter J, Bentson JR. Anatomical localization schemes for use in positron com- puted tomography using a specially designed head holder. J Comput Assist Tomogr 1982;6:848-53.
[13] Chugani HT, Phelps ME. Maturational changes in cerebral function in infants determined by 18FDG positron emission tomography. Science 1986;231:840-3.
[14] Chugani HT, Phelps ME, Mazziotta JC. Positron emission to- mography study of human brain functional development. Ann Neurol 1987;22:487-97.
[15] Chugani HT, Shewmon DA, Sankar R, Chen BC, Phelps ME. Infantile spasms: II. Lenticular nuclei and brain stem activation on posi- tron emission tomography. Ann Neurol 1992;31:212-9.
[16] Cusmai R, Curatalo E Mangano S, Cheminal R, Echenne B. Hemimegalencephaly and neurofibromatosis. Neuropediatrics 1990;21: 179-82.
[17] Konkoi RJ, Maister BH, Wells RG, Sty JR. Hemimegalen- cephaly: Clinical, EEG, neuroimaging, and IMP-SPECT correlation. Pediatr Neurol 1990;6:414-8.
[18] Phelps ME, Mazziotta JC, Schelbert H. Positron emission tomography and autoradiography. In: Principles and application for the brain and heart. New York: Raven Press, 1986.
[19] Chugani HT, Mazziotta JC, Engel J Jr, Phelps ME. The Lennox-Gastaut syndrome: Metabolic subtypes determined by 2-deoxy- 2(lgF)tluoro-D-glucose positron emission tolnograph~ Ann Neurol 1987;21:4-13.
[20] Chugani HT, Shewmon DA, Peacock WV. Shields WI). M~ziotta JC, Phelps ME. Surgical treatment of retractable neonatal- onset seizures. The role of positron emission tomography. Neurology 1988;38:1178-88.
[21] Chugani HT, Phelps ME, Mazziotta JC. Stnrge-Weber syn- drome: A study of cerebral glucose utilization with positron emission tomography. J Pediatr 1989;114:244-53.
[22] Chugani HT, Shields WD, Shewmon DA, Olson DM, ['helps ME, Peacock WJ. Infantile spasms, 1. PET identifies focal cortical dys- genesis in cryptogenic cases for surgical treatment. Ann Neural 1990: 27:406-13.
[23] Kerrigan JF, Chugani HT, Phelps ME. Regional cerebral glu- cose metabolism in clinical subtypes of cerebral palsy. Pediatr Neurol 1991;7:415-25.
[24] Chiton C, Raynaud C, Dulac O, Tzourio N, Plouin P, Tran Dinh S. Study of the cerebral blood flow in partial epilepsy of childhood using the SPECT method. J Neuroradiol 1989; 16:317-24.
[25] Chugani HT, Shewmon DA, Khanna S, Phelps ME. lnterictal and postictal focal hypermetabolism on positron emission tomography. Pediatr Neurol 1993;9:10-5.
[26] Theodore WH, Brooks RD, Patronas N, Brooks RA, Di Chiro G. The effect of phenobarbital and phenytoin on cerebral glucose metab- olism measured by positron emission tomography. Neurolo~?y 1984;34 (Suppl):118.
[27] Theodore WH. Antiepileptic drugs and cerebral glucose metab- olism. Epilepsia 1988;29(Suppl 2):$48-55.
[28] Valmier J, Touchon J, Blayac JP, Baldy-Moulinier M. Initiation of carbamazepine therapy in partial epilepsy: A regional cerebral blood flow study. Epilepsy Res 1990;5:229-34.
[29] Leidenman DB, Balish M, Bromfield EB, Theodore WH. Ef- fect of valproate on human cerebral glucose metabolism. Epilepsia 1991 ;32:417-22.
[30] Tjiam AT, Stefando S, Schenk VWD, de Vlieger M. Infantile spasms associated with hemihypsarrhythmia and hemimegatencephaly, Dev Med Child Neurol 1978;20:779-89.
[311 Robain O, Chiron C, Dulac O. Electron microscopic and Golgi study in a case of hemimegalencephaly. Acta Neuropathol 1989;77: 664-66.
[32] Vigevano F, Di Rocco C. Effectiveness of hemispherectomy in hemimegalencephaly with intractable seizures. Neuropediatrics 1990;21: 222-3.
[33] De Rosa MJ, Secor DL, Barsom M, Fisher RS, Vinters HV. Neuropathologic findings in surgically treated hemimegalencephaly: Immunohistochemical, morphometric, and ultrastructural study. Acta Neuropathol 1992, in press.
[34] Bairamian D, Di Chiro G, Theodore WH, Holmes MD, Dorwart RH, Larson SM. MR imaging and positron emission tomog- raphy of cortical heterotopia. J Comput Assist Tomogr 1985 ;9:1137-9.
[35] Bignami A, Zappella M, Benedetti P. Infantile spasms with hypsarrhythmia. A pathological study. Helv Paediatr Acta 1964;4: 326-42.
[36] King M, Stephenson JBE Ziervogel M, Doyle D, Galbruith S. Hemimegalencephaly. A case for hemispherectomy? Neuropediatrics 1985; 16:46-55.
[37] Kalifa G, Chiton C, Sellier N, et al. Hemimegalencephaly: MR imaging in five children. Radiology 1987;165:29-33.
[381 Chiton C, Raynaud C, Jambaque I, Dulac O, Zitbovicius M, Syrota A. A serial study of regional cerebral blood flow before and after hemispherectomy in a child. Epilepsy Res 1991 ;8:232-40.
[39] Konkol R J, Maister BH. Relevance of EEG to prognosis in hemimegalencephaly. Dev Med Child Neurol 1989;31:827-8.
28 PEDIATRIC NEUROLOGY Vol. 9 No. 1






















![PET/ CT [Positron Emission Tomography]](https://img.pdfslide.us/doc/110x75/56d6bf451a28ab30169592f3/pet-ct-positron-emission-tomography.jpg)





