Embed Size (px)
Citation preview
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 1
Hematopoietic Stem Cell Transplantation Course
Study Module
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 2
Table of Contents COURSE PURPOSE .......................................................................................................................... 5 COURSE DESCRIPTION................................................................................................................... 5 TARGET AUDIENCE........................................................................................................................ 5 LEARNING ASSUMED TO BE IN PLACE .......................................................................................... 5 LEARNER OVERALL OUTCOMES................................................................................................... 5 COURSE CONTENT ......................................................................................................................... 6
HEMATOPOIESIS AND IMMUNOLOGY............................................................................... 7
OVERVIEW...................................................................................................................................... 7 CD34+ CELLS................................................................................................................................. 7 RED BLOOD CELLS ........................................................................................................................ 8 PLATELETS ..................................................................................................................................... 8 WHITE BLOOD CELLS.................................................................................................................... 9 THE IMMUNE SYSTEM ................................................................................................................... 9 LYMPHOCYTES .............................................................................................................................. 10 B AND T LYMPHOCYTES................................................................................................................ 10 IMMUNOGLOBULINS ...................................................................................................................... 11 CYTOKINES .................................................................................................................................... 11 THE HUMAN LEUKOCYTE ANTIGEN SYSTEM ............................................................................ 11 HUMAN LEUKOCYTE ANTIGEN MATCHING .................................................................................. 12
HEMATOPOIETIC STEM CELL TRANSPLANTATION................................................... 14
OVERVIEW.................................................................................................................................... 14 STEM CELLS SOURCES................................................................................................................. 15 ABO MISMATCH .......................................................................................................................... 15 PATIENT EVALUATION................................................................................................................. 16 PREPARATIVE REGIMENS............................................................................................................ 16 INDICATIONS FOR TOTAL BODY IRRADIATION.......................................................................... 17 PROPHYLAXIS AND TREATMENT OF GRAFT VERSUS HOST DISEASE ....................................... 17 IMMUNOSUPPRESSION ................................................................................................................... 17 T-CELL DEPLETION........................................................................................................................ 17 GRAFT VERSUS LEUKEMIA EFFECT............................................................................................ 17 MOBILIZATION OF STEM CELLS ................................................................................................. 17 COLLECTION OF STEM CELLS .................................................................................................... 18 PERIPHERAL BLOOD STEM CELL COLLECTION ............................................................................. 18 BONE MARROW HARVEST............................................................................................................. 18 CORD BLOOD COLLECTION ........................................................................................................... 19 INFUSION OF HEMATOPOIETIC STEM CELLS............................................................................. 19 CRYOPRESERVED STEM CELL INFUSION ....................................................................................... 19 FRESH HEMATOPOIETIC STEM CELL INFUSION............................................................................. 20 NURSING MANAGEMENT............................................................................................................... 20 POST STEM CELL INFUSION........................................................................................................... 20 ENGRAFTMENT............................................................................................................................. 21 COMPLICATIONS .......................................................................................................................... 21
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 3
GRAFT-VERSUS-HOST DISEASE .................................................................................................... 21 INFECTIONS.................................................................................................................................... 23 GRAFT FAILURE............................................................................................................................. 25 HEMORRHAGIC CYSTITIS .............................................................................................................. 25 VENO-OCCLUSIVE DISEASE (VOD) .............................................................................................. 25 REFERENCES ................................................................................................................................ 26
ADULT HSCT PROGRAM AT KFSH & RC.......................................................................... 28
BMT COORDINATION AND PRE-TRANSPLANT WORK-UP ........................................................ 29 PATIENT REFERRAL AND INCLUSION IN THE TRANSPLANT PROGRAM ................................... 29 PATIENTS ARE USUALLY ENROLLED IN THE TRANSPLANTATION PROGRAM THROUGH TWO DISTINCT CHANNELS:................................................................................................................... 29 RESULTS OF HLA TYPING ............................................................................................................. 29 PLANNING FOR DATE OF TRANSPLANT ......................................................................................... 30 PREPARATION FOR DISCHARGE..................................................................................................... 31 POST-TRANSPLANT FOLLOW-UP AT THE BMT CLINIC ................................................................. 31 RECIPIENT PRE-TRANSPLANT WORK-UP....................................................................................... 32 INDICATIONS FOR ALLOGENEIC HSC TRANSPLANTATION ...................................................... 33 ALLOGENEIC BONE MARROW AND PERIPHERAL STEM CELL ................................................. 34 TRANSPLANTATION PROGRAMS ................................................................................................. 34 ELIGIBILITY AND EXCLUSION CRITERIA ....................................................................................... 34 SOURCE OF STEM CELLS FOR ALLOGENEIC TRANSPLANTATION............................................ 35 INDICATIONS FOR AUTOLOGOUS HSC TRANSPLANTATION ..................................................... 36 AUTOLOGOUS STEM CELL TRANSPLANTATION PROGRAM...................................................... 37 ELIGIBILITY AND EXCLUSION CRITERIA ....................................................................................... 37 NON-MYELOABLATIVE ALLOGENEIC HEMATOPOIETIC STEM CELL TRANSPLANT PROGRAM....................................................................................................................................................... 38
RATIONALE............................................................................................................................... 38
NST TREATMENT PLAN................................................................................................................. 39 IMMUNOTHERAPY ........................................................................................................................ 43 INCLUSION CRITERIA .................................................................................................................. 43 EXCLUSION CRITERIA ................................................................................................................. 43 DIETARY GUIDELINES ................................................................................................................. 44
FOOD RESTRICTIONS ............................................................................................................ 44
FOOD PREPARATION TIPS .............................................................................................................. 45 TREATMENT GUIDELINES FOR PATIENTS WITH FEVER AND NEUTROPENIA ... 46 I. ANTIBACTERIAL PROPHYLAXIS IN AFEBRILE NEUTROPENIC PATIENTS.................................... 46 II. EMPIRICAL ANTIBACTERIAL THERAPY..................................................................................... 46 ACUTE GVHD .............................................................................................................................. 49 ACUTE GVHD PROPHYLAXIS REGIMEN ....................................................................................... 49
2. METHOTREXATE DOSE ADMINISTRATION AND REDUCTION GUIDELINES49
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 4
CHRONIC GVHD.......................................................................................................................... 56 OUTPATIENT VISIT SCHEDULE ................................................................................................... 57
FOLLOW UP OF CHRONIC-GVHD....................................................................................... 57
ANTIMICROBIAL PROPHYLAXIS POST SCT* • • • • • • .................................................................... 58
TREATMENT OF HZV INFECTIONS ................................................................................... 58
GONADAL DYSFUNCTION • •................................................................................................ 60
ACTIVITIES OF DAILY LIVING ........................................................................................... 61
IMMUNIZATION POST ALLOGENEIC BMT ..................................................................... 61
DIAGNOSIS/STAGE........................................................................................................................ 63
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 5
Course Purpose This course is designed to provide the nurse with in-depth knowledge base, skills and attitude to respond to both the present and future needs of patient/family undergoing hematopoietic stem cell transplant (HSCT) in a holistic manner.
Course Description This course is a 2-day program that prepares the nurse to work with an adult/child undergoing HSCT. The course focuses on the holistic approach of patient care through integration of the core knowledge, essential nursing skills, and supportive care in HSCT. The course utilizes the Oncology Nursing Society’s Standards of Oncology Nursing Practice as a framework for learner outcomes.
Target Audience The HSCT Course is designed for registered nurses who are novice to the care of patients undergoing HSCT. It can also be a valuable review for the experienced HSCT nurse.
Learning Assumed to be in Place Two years experience as a registered nurse with preferably one year experience in oncology nursing.
Learner Overall Outcomes • Discuss the rationale for treating certain cancers with bone marrow and
HSCT.
• Identify the various types of bone marrow and HSCT that are used to treat the patient with cancer.
• Discuss the role of cell immunology in HSCT
• Formulate a plan of care for patients undergoing HSCT
• Identify the complications of this treatment for the patient with cancer.
• Identify the nursing implications of HSCT therapy.
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 6
Course Content • Review of Hematopoiesis and Immunology
• HSCT: Types, Sources and Indications
• Pre-Transplant Phase: Donor Selection and Patient/ Family
Preparation.
• Pre-Transplant Phase: Stem Cell Collection, Mobilization, and Harvest.
• Transplant Phase: Nursing Implications
• Nursing Implications of acute and Chronic GVHD
• Acute and Late Complications of HSCT: Nursing Approach
• Psychosocial, and Ethical Considerations
• Quality of Life Post HSCT
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 7
Hematopoiesis and Immunology
Overview
Hematopoiesis is the process of growth, division, and differentiation of blood cells. From one originating stem cell, the bone marrow is capable of producing distinct cells that function in the body defense, oxygen carrying capacity, and clotting. These end products are white blood cells (WBCs), red blood cells (RBCs), and platelets respectively. In infancy all the bone marrow is hematopoietic but during childhood there is a progressive fatty replacement of marrow throughout the long bones so that in adulthood hematopoietic marrow is confined to the central skeleton and proximal end of humeri and femurs. Even In these areas, approximately 50% of the marrow consists of fat. However, if the bone marrow is injured at any age, hematopoiesis can resume in the liver and spleen. This is referred to as extramedullary hematopoiesis.
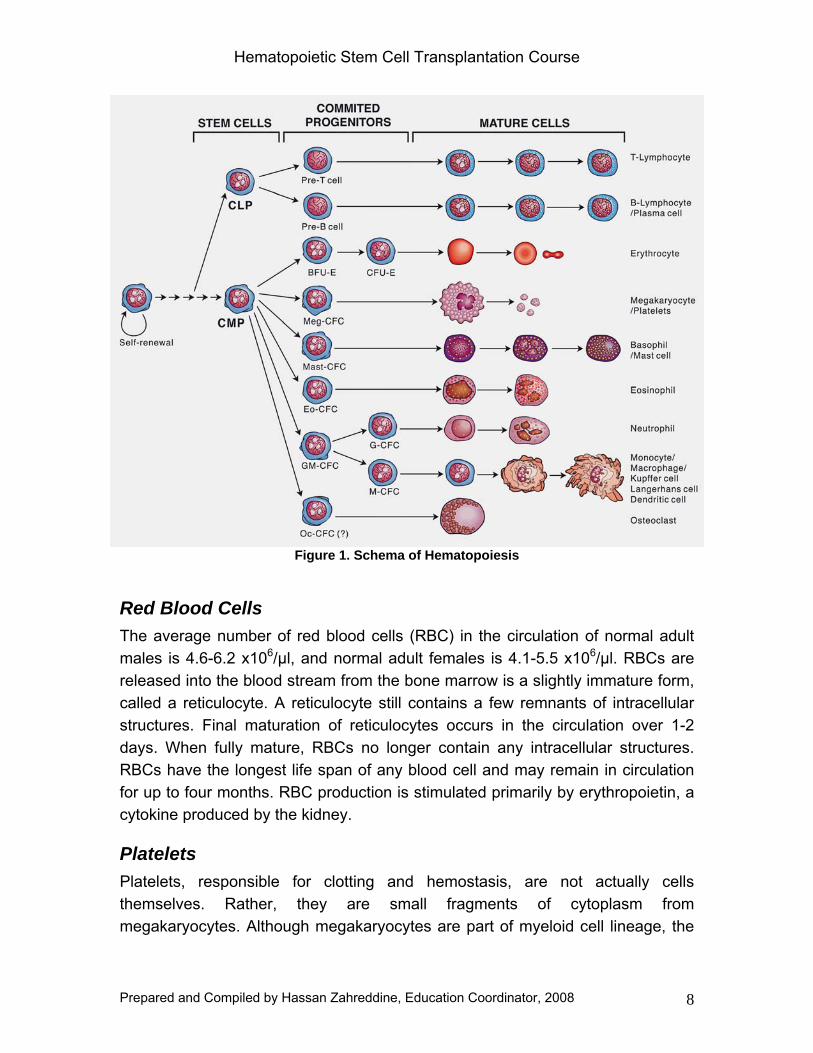
Hematopoiesis starts with a pluripotent hematopoietic stem cell (PHSC). These stem cells represent a self-renewing population of cells so that marrow cellularity remains constant in a normal healthy state. They have the potential to differentiate and to become committed to a particular blood cell lineage. Initial differentiation of PHSCs will be along one of two major pathways, lymphoid or myeloid. Lymphoid progenitor pathway for T cell and B cell progenitors and myeloid progenitor pathway for erythrocytes, neutrophils, eosinophils, basophils, monocytes, mast cells, and platelets (figure 1). As cells differentiate, their capacity to replicate and self-renew declines. They lose the ability to replicate when they are fully mature and are said to be terminally differentiated. The precursor cells, however, capable of responding to hematopoietic growth factors with increased production of one or other cell line when the need arises.
CD34+ Cells PHSC is identified by CD34, a characteristic protein produced on the surface of these cells. CD is an abbreviation for cluster differentiation. CD is a nomenclature developed to identify proteins or protein complexes on the surface of the cells. Each identifiable protein or protein complexes is given a designation CD followed by a unique number.
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 8
Figure 1. Schema of Hematopoiesis
Red Blood Cells The average number of red blood cells (RBC) in the circulation of normal adult males is 4.6-6.2 x106/µl, and normal adult females is 4.1-5.5 x106/µl. RBCs are released into the blood stream from the bone marrow is a slightly immature form, called a reticulocyte. A reticulocyte still contains a few remnants of intracellular structures. Final maturation of reticulocytes occurs in the circulation over 1-2 days. When fully mature, RBCs no longer contain any intracellular structures. RBCs have the longest life span of any blood cell and may remain in circulation for up to four months. RBC production is stimulated primarily by erythropoietin, a cytokine produced by the kidney.
Platelets Platelets, responsible for clotting and hemostasis, are not actually cells themselves. Rather, they are small fragments of cytoplasm from megakaryocytes. Although megakaryocytes are part of myeloid cell lineage, the
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 9
do not circulate in the blood stream. Rather they remain the in bone marrow and release platelets. The average number of platelets circulating in a normal adult is 150,000-350, 000/µl. Platelets remain in the circulation for four to seven days.
White Blood Cells Two lineages of hematopoietic cells produce different kinds of white blood cells WBCs. The primary function of all WBCs is to protect the body from foreign invaders. Mature WBCs from the myeloid lineages (see handout 21-1) include neutrophils, eosinophils, basophils, monocytes, dendritic cells, and mast cells. Neutrophils are the most common type of myeloid WBCs. The remaining circulating WBCs come from the lymphoid lineage. They include T lymphocytes, B lymphocytes, and NK cells.
WBCs production is primarily stimulated by inflammation and infection. The cytokines IL-3 and GM-CSF provide stimulus for the myeloid WBC production throughout the entire proliferation and differentiation process, whereas G-CSF plays an important role in the later stages of neutrophil maturation. Macrophage colony-stimulating factor, IL-4, and IL-5 stimulate later maturation of monocytes, basophils, and eosinpphils, respectively. Lymphoid WBC production is stimulated in the B cell lineage primarily by Il-1, IL-2, IL-4, IL-5, and IL-6. In the T cell lineage, lymphoid WBC production is stimulated primarily by IL-2, and IL-4.
The Immune System The immune system is a body wide network of cells, tissues, and organs that has evolved to defend against “foreign" invasions. The proper targets of the immune system are infectious organisms-bacteria, fungi, parasites, and viruses.
At the heart of the immune response is the ability to distinguish between "self" and "non-self." Every cell in the body carries the same set of distinctive surface proteins that distinguish it as "self." Normally the immune cells do not attack its own body tissues, which all carry the same pattern of self-markers; rather, the immune system coexists peaceably with other body cells in a state known as self-tolerance.
This set of unique markers on human cells is called the major histocompatibility complex (MHC). There are two classes: MHC Class I proteins, which are on all cells, and MHC Class II proteins, which are only on certain specialized cells.

Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 10
Lymphocytes In post natal life, the bone marrow and thymus are the primary lymphoid organs in which lymphocytes develop. The secondary lymphoid organs in which specific immune responses are generated are the lymph nodes, spleen and lymphoid tissues at the alimentary and respiratory tracts. An adult has about 1 x 1012 lymphocytes.
B and T Lymphocytes The immune response depends upon two types of lymphocytes, B and T cells. B cells mature in the bone marrow and circulate in the peripheral blood until they undergo recognition of antigen. The B cell receptor is membrane bound immunoglobulin and after activation this is secreted as free soluble immunoglobulin. At this point they mature into B cells or plasma cells. B cells have two primary functions, to present antigens to T cells and to produce antibodies. When B cell is stimulated to produce its antibody, it may develop into a plasma cell, which is a large cell that produces large amounts of a specific antibody.
T cells develop from cells that have migrated to the thymus where they differentiate into mature T cells during passage from cortex to medulla. They are responsible for cell-mediated immunity. There are three main types of T cells: regulatory, cytotoxic, and NK cells. Regulatory T cells are vital to the proper function of the immune system. There are two types of regulatory T cells: helper/inducer cells and suppressor cells. Helper/inducer T cells also are called T4 cells and carry the CD4 antigen on the surface of their cell membranes. T4 cells can initiate an immune response by activating b cells, other T cells, NK cells, and macrophages. T suppressor T cells can stop an immune response when it is no longer needed. Suppressor T cells are called T8 cells and carry the CD8 antigen on their cell surface. These cells produce cytokines that signal activated immune system to become inactive to stop responding to activation signal.
Cytotoxic T cells also have the CD8 antigen on their cell surfaces. They are programmed to recognize specific antigen. These antigens may identify cells that have been infected with a virus, malignant cells, or cells from foreign tissues and organs. When a cytotoxic T cell recognizes an antigen on a cell, it kills the cell on contact.
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 11
Unlike cytotoxic T cells, NK cells do not need to come in contact with a specific antigen before acting. Once stimulated in act, they will directly destroy any foreign cell, including tumor cells and microorganisms. NK cells also secrete large amounts of cytokines that regulate the immune system function.
Immunoglobulins These are group of proteins produced by plasma cells and B Lymphocytes that bind to antigen. There are five known classes of immunoglobulins: IgG, IgA, IgE, and IgD. The primary actions of the classes of antibodies are:
IgG: Coat invaders to speed uptake by other immune cells in the blood
IgA: Concentrate in body fluids to protect guard entrances to body
IgM: Link together in blood stream to kill invaders
IgE: Participate in allergic reactions
IgD: Regulate cell activation on B cell membrane
Cytokines Cytokines are polypeptides secreted by immune and other cells when the cell interacts with a specific antigen, endotoxin, or other cytokines. Major categories include IFNs (IFN-α, IFN-β, IFN-γ), TNFs (TNF-α, TNF-β), ILs, TGFs, and hematopoietic colony-stimulating factors (CSFs). Although lymphocyte interaction with a specific antigen triggers cytokine secretion, cytokines themselves are not antigen-specific; thus, they bridge innate and acquired immunity and generally influence the magnitude of inflammatory or immune responses. They act sequentially, synergistically, or antagonistically.
The Human Leukocyte Antigen System The human leukocyte antigen (HLA) system, the major histocompatibility complex (MHC) in humans, is located on chromosome 6. It encodes cell surface molecules specialized to present antigenic peptides to the T-cell receptor (TCR) on T cells. MHC molecules which present antigens are divided into 2 major classes.
Every cell in the body is covered with these MHC self-marker proteins, and individuals carry different sets except for identical twins. MHC marker proteins
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 12
are as distinct as blood types and come in two categories, MHC Class I and MHC Class II. The immune cells recognize major histocompatibility complex proteins when they distinguish between self and non-self. An MHC protein serves as a recognizable scaffold that presents pieces (peptides) of a foreign protein (antigenic) to immune cells.
Prior to establishment of donor hematopoiesis, recognition of donor stem cells by immunocompetent host T cells can cause failed, delayed, or inadequate engraftment of donor hematopoietic stem cells (HSCs). Eradication of the host immune system and immunologic similarity between the patient and donor is important to ensure strong donor engraftment.
Class I HLA molecules are present on the surface of all nucleated cells and platelets. There are three major class I HLA genes identified as HLA-A, -B, or –C, which can be found at the A, B, and C loci in the MHC. Lymphocytes reactive to class I molecules express CD8 molecules often associated with effector cytotoxic function.
Class II MHC molecules are present on Antigen-presenting cells (APCs: such as B cells, macrophages, dendritic cells, and Langerhans' cells), thymic epithelium, and activated T cells. There are three major class II HLA genes, identified as HLA-DP, -DQ, and -DR which can be found at the DP, DQ, and DR loci in the MHC region of chromosome 6. Lymphocytes reactive to class II molecules express CD4 and are often helper T cells.
Individual alleles of each locus of the HLA system are given standard designations (eg, HLA-A1, -B5, -Cw1, -DR1). Alleles defined by DNA sequencing are named to identify the gene and to give each allele a unique number composed of the HLA locus, an asterisk, 2 numbers representing the serologic equivalent of the antigen, and 2 numbers representing the specific allele (eg, A*0201, DRB1*0103, DQA1*0102). Sometimes another number is added to identify a different subtype. Determination of HLA alleles of an individual is called HLA typing.
Human Leukocyte Antigen Matching Prior to establishment of donor hematopoiesis, recognition if donor stem cells by immunocompetent host T cells can cause failed, delayed, or inadequate engraftment. Eradication of the host immune system and immunologic similarity between the patient and donor is important to ensure strong engraftment.
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 13
Once the donor HSCs engraftment has occurred, immunocompetent T cells may recognize host cells as foreign and may attempt to destroy them. It is important that the patient and donor be as immunologically similar as possible to prevent this potentially fatal complication, referred to as GVHD.
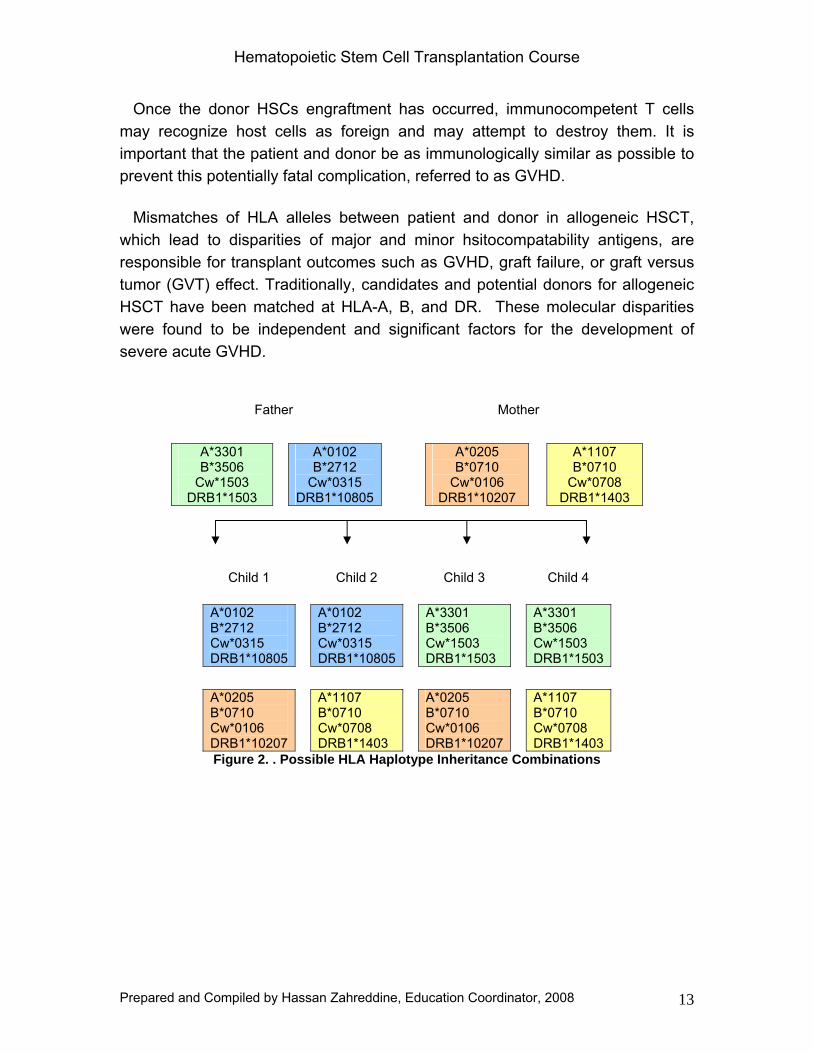
Mismatches of HLA alleles between patient and donor in allogeneic HSCT, which lead to disparities of major and minor hsitocompatability antigens, are responsible for transplant outcomes such as GVHD, graft failure, or graft versus tumor (GVT) effect. Traditionally, candidates and potential donors for allogeneic HSCT have been matched at HLA-A, B, and DR. These molecular disparities were found to be independent and significant factors for the development of severe acute GVHD.
Father Mother
A*3301 B*3506
Cw*1503 DRB1*1503
A*0102 B*2712
Cw*0315 DRB1*10805
A*0205 B*0710
Cw*0106 DRB1*10207
A*1107 B*0710
Cw*0708 DRB1*1403
Child 1 Child 2 Child 3 Child 4
A*0102 B*2712 Cw*0315 DRB1*10805
A*0102 B*2712 Cw*0315 DRB1*10805
A*3301 B*3506 Cw*1503 DRB1*1503
A*3301 B*3506 Cw*1503 DRB1*1503
A*0205 B*0710 Cw*0106 DRB1*10207
A*1107 B*0710 Cw*0708 DRB1*1403
A*0205 B*0710 Cw*0106 DRB1*10207
A*1107 B*0710 Cw*0708 DRB1*1403
Figure 2. . Possible HLA Haplotype Inheritance Combinations
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 14
Hematopoietic Stem Cell Transplantation
Overview Hematopoietic stem cell transplantation involves eliminating a patient’s hematopoietic and immune system by chemotherapy and/ or radiotherapy and replacing it with stem cells either from another individual or with previously harvested portion of the patient’s own hematopoietic stem cells. The term encompasses both bone marrow transplantation (BMT), in which stem cells are collected from the bone marrow, and peripheral blood stem cell (PBSC) transplantation in which stem cells are collected from peripheral blood. It was first attempted in 1939 when human bone marrow cells were injected intravenously to treat a patient with aplastic anemia. Since that time, despite uneven progress and problems with entities such as GVHD, the procedure has become an accepted treatment for various hematologic deficiencies and malignant conditions (see Table 1.)
The concept of rescuing an individual from the toxic effects of radiation and/or chemotherapy has evolved over the past 60 years. Early experiments in animals demonstrated that the spleen and marrow cells from a donor animal could support hematopoietic recovery after lethal doses of radiation or chemotherapy.
Table 1. Diseases Commonly Treated with HSCT
• Allogeneic o Acute Myeloid Leukemia o Acute Lymphobalstic Leukemia o Chronic Myeloid Leukemia o Myelodysplastic Syndrome o Non-Hodgkin’s Lymphoma o Hodgkin’s Disease o Severe Aplastic Anemia o Fanconi’s Anemia o Blackfan-Diamond Anemia o Thalassemia Major o Sickle Cell Anemia o Severe Combined Immunodeficiency o Wiskott-Aldrich Syndrome
• Autologous
o Multiple Myeloma o Non-Hodgkin’s
Lymphoma o Hodgkin’s Disease o Acute Myeloid
Leukemia o Neuroblastoma o Amyloidosis
HSCT can be performed with cells from a family member or an unrelated donor (allogeneic transplantation) or with stem cells previously collected from the patient (autologous transplantation). The choice between the more risky allogeneic transplant and an autologous procedure depends on patient age, the
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 15
underlying disease, donor availability and institutional preference. The drawbacks of an autologous transplant are possible contamination of the graft with malignant cells and the lack of a graft-versus-tumor effect. Allogeneic transplantation requires donor and recipient matching for major HLA antigens. The best donor is an HLA-identical sibling. Transplants with only partial matching for HLA antigens are associated with a higher risk of post-transplant complications.
Stem Cells Sources Stem cells may be collected through different methods or sources. Bone marrow is obtained through repeated aspirations of the posterior iliac crests while the donor is under general or epidural anesthesia in an operating room. Bone marrow was traditionally the most commonly used source for HSC collection. After harvesting, the cells are mixed with an anticoagulant and then are filtered to remove clots, bone particles, and fat cells.
Peripheral blood is another source of HSCs and has replaced marrow for autologous and most allogeneic transplantations. Peripheral blood stem cells (PBSC) produce more rapid hematopoietic reconstitution compared to marrow. Stem cells are mobilized out of the bone marrow into the peripheral blood with the use of granulocyte-colony stimulating factor (G-CSF). Stem cells are then collected from the peripheral blood through apheresis. Once the stem cells are obtained, they then are mixed with an anticoagulant and either preserved and frozen (cryopreserved) or infused fresh into the transplant recipient. One of the most important advantages of PBSC is early engraftment compared to bone marrow.
Umbilical cord blood (UCB) stem cells are collected from the umbilical cord and placenta immediately following birth. UCB is then tested for HLA, cryopreserved and stored in cord blood banks. One of the important advantages of UCB stem cells is the lower risk of GVHD.
ABO Mismatch Occasionally, a recipient may receive stem cells from a donor who possesses a different ABO blood type. Effective removal of red blood cells from the stem cell product has enabled successful transplantation in this case. After transplantation, the recipient will have the donor ABO blood type.
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 16
Patient Evaluation The patient is evaluated as a candidate for HSCT to determine which transplant type is most appropriate. The disease, stage of disease, performance status, availability of appropriate protocol, and donor availability are considered. The clinical evaluation is performed to determine if any organ dysfunction is present. Psychosocial evaluation begins with education of the patient and family about the rationale, risks, and benefits of HSCT. Discussion should include acute and long term effects. Sources of support and available resources are identified. Patient and family education begins with the initial period of evaluation and continuing throughout the process of HSCT. It is useful to provide oral and written information and allow sufficient time for patients and family to synthesize information and ask questions.
Preparative Regimens Selections of preparative regimens are based on two major goals: eradication of the disease and prevention of host immune rejection of the graft. An important principle in transplantation is to understand the difference between myelosuppression and myeloablation. A myeloablative regimen is lethal without hematopoietic rescue. When considering solid tumors, the primary goal of the preparative regimen is an antitumor effect, whereas the primary goal in the treatment of malignant marrow disorder is myeloablation.
The second goal in the planning of the preparative regimen is immunosuppression to prevent graft rejection during transplant. This is not a concern during autologous transplant. Examples of immunosuppressive agents include cyclophosphamide, total body irradiation (TBI), and antithymocyte globulin (ATG). These agents can be incorporated in the preparative regimen to facilitate allogeneic blood and marrow engraftment through host immunosuppression.
There are many combinations of preparative regimens consisting of chemotherapy, immunotherapy, and/or radiation therapy given pretransplant. The agents used vary depending on the type of transplant, disease, and desired effects. The types of drugs, doses, and schedules are not standardized and they vary from institution to institution. There may be scheduled days of rest that allow chemotherapy to be eliminated from the body. The scheduled days of the preparative regimen are counted as minus days (e.g. D -1, D-2, etc...), with transplant day as day zero (D zero).
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 17
Indications for Total Body Irradiation TBI is more widely used in allogeneic HSCT than autologous HSCT. It is mostly used in diseases that are sensitive to radiation, such as leukemias and lymphomas. It provides tumor eradication effect as well as immunosuppression to prevent rejection of donor cells.
Prophylaxis and Treatment of Graft versus Host Disease Methods used to decrease the risk of GVHD include prophylaxis, immunosuppression, and T-cell depletion of the donor stem cell product.
Immunosuppression Immunosuppressant medications like cyclosporine, mehtotrexate and steroids are commonly used to prevent or treat GVHD. These medications blunt the reaction of donor immune cells and keep them from identifying the host or patient as foreign.
T-cell Depletion Under normal immunologic conditions, T cells play a major role of recognition of self from non-self proteins. In allogeneic HSCT, active donor T cells within the stem cell product have the same capability. As a result, donor T cells may recognize the recipient tissue as foreign, initiating GVHD. Several methods are now available to deplete the stem cell product from T cells.
Graft versus Leukemia Effect The donor stem cells can also exert a beneficial effect against the malignancy. The immunocompetent donor cells can recognize the patient’s malignant cells as foreign and eliminate them. This effect was originally identified in leukemia patients. It was observed that relapse in patients with GVHD was much less than patients who did not have GVHD. Furthermore, syngeneic and autologous transplants lacking GVHD were noted to have higher relapse rates.
Mobilization of Stem Cells The number of circulating stem cells in the blood is low as compared with the number of stem cells in bone marrow. Mobilization of stem cells refers to the methods of stimulating the stem cell that originates in the bone marrow to move into the peripheral blood. Two methods have been used to increase the number of circulating stem cells. These include chemotherapy and growth factors. Following chemotherapy, there is a transient increase in the number of circulating
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 18
stem cells and they may be harvested during this phase. Hematopoietic growth factors is another more common method that is used to mobilize stem cells. Many mobilization protocols include chemotherapy and hematopoietic growth factors. The growth factors not only help to reduce Cytopenia following chemotherapy but also dramatically increase the number of circulating progenitor cell.
Collection of Stem Cells
Peripheral Blood Stem Cell Collection After mobilization, an apheresis machine collects the cells. This process involves using an automated cell separator that can isolate specific components from whole blood continuously. Any component can be targeted for relatively specific removal, including plasma, red blood cells, platelets, or white blood cells. Antecubital veins may be used to harvest PBSC. Most institutions use a large lumen catheter (10-18.5 French) apheresis or hemodialysis catheter. Pediatric patients may require smaller catheter size. Apheresis catheters are usually inserted into the subclavian vein and may be tunneled to provide long term access (e.g. Permacath).
Assessing the CD34+ cells in the peripheral blood, may indicate the best time to collect the stem cells. The collection usually starts 4-5 days following the start of growth factors. The stem cells are then collected using an apheresis machine. As blood is drawn from the central venous catheter and into the machine, an anti-coagulant, citrate dextrose solution (ACD-A), is added to prevent clotting. The machine transfers the stem cells into a collection bag, and returns the remaining blood to the patient. If the target CD34+ cell count is not achieved with one apheresis session, then it another session will be repeated until achieving the required count. The goal is to collect > 4x108 CD34+ cells/kg for allogeneic transplantation and > 5x108 CD34+ cells/kg for autologous transplantation. After collection the stem cells undergo further processing and are sometimes frozen (autologous transplantation). When frozen, a cryoprotectant (DMSO) is added to prevent cell damage during either freezing or thawing.
Bone Marrow Harvest Bone marrow is harvested from the posterior iliac crests through multiple needle aspiration. The procedure is usually performed in the operating room (OR) under general or spinal anesthesia. To improve the harvest yield, no less than four different well-spaced iliac crest puncture sites are carried out on each side with
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 19
multiple aspirations to be obtained by directing the needle to different areas of the marrow cavity. Puncture sites must be different for each aspiration (10 to 15 ml per aspiration). The total fluid volume collected is usually 500-1000 ml. In order to prevent clotting, which might considerably reduce the yield of the harvest, heparinized normal saline is added to the collection bag. Each syringe used for aspiration of bone marrow, is rinsed in the heparinized normal saline solution and1 ml of this solution is added to each syringe. The aspirated marrow is passed into a multiple filters to remove fat and bone particles and transferred into a collection bag. The number of nucleated cell attempted to be harvested is at least 2x108 nucleated cells/kg (10-15 ml/kg), and more in cases of ABO incompatible transplants and bone marrow failure syndromes. The cell count is obtained during the procedure (mid count) and when collection is completed.
Cord Blood Collection UCB and placental blood are collected immediately after delivery. Using sterile technique, a 16-gauge needle is inserted in the umbilical cord and the blood is then drained by gravity into a blood bag or withdrawn into a 60 ml syringe containing anticoagulant. The product is then processed and cryopreserved.
Infusion of Hematopoietic Stem Cells The infusion of HSC occurs on Day zero (Day 0). Autologous cells may be infused in one to two days depending on the volume and to minimize the side effects of dimethyl sulfoxide (DMSO) used to preserve the stem cells in the frozen state. The HSC may be infused without delay after TBI but are usually infused 24-48 hours after the last dose of chemotherapy. This is to ensure that no residual cytotoxic therapy that could harm the cells is still circulating.
Cryopreserved Stem Cell Infusion The cryopreserved product is thawed rapidly in a sterile saline or sterile water bath, heated to 37-45 oC, at the bedside and infused immediately. The thawing process of the second bag should not be initiated until the infusion of the prior bag is completed, because prolonged exposure of stem cell to DMSO has been shown to decrease colony formation of cryopreserved HSCs. The infusion might be accompanied by minor adverse effects, most resolve within 24-48 hours. Most adverse effects are caused by DMSO, red cell contamination and breakdown, and the total volume of cells infused. Other adverse effects include nausea, vomiting, abdominal cramping, diarrhea, facial flushing, hypertension, hypotension, dyspnea, fever, chills, and garlic-like taste in the mouth and unusual
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 20
breath odor. The garlic –like taste is caused by DMSO and should only last 24-28 hours. The family and staff will notice garlic –like odor on the patient’s breath and urine.
Fresh Hematopoietic Stem Cell Infusion Allogeneic HSCs are usually infused fresh, immediately after apheresis or marrow harvest. Under some circumstances, they are cryopreserved and frozen. Placental and UCB stem cells must be cryopreserved and stored after collection. The product the goes to the lab for processing. If the donor and recipient are ABO incompatible, the product may then be red cell depleted and plasma reduced. Other processing may include T cell depletion to reduce the incidence of GVHD. The fresh HSCs are then delivered fresh and delivered at the bedside and infused via gravity into the patient’s central venous catheter. potential adverse effects are similar to those seen with blood product infusions and can include shortness of breath, hypotension, hypertension, tachycardia, fever, chills, chest patin ot tightness, flushing, nausea and vomiting, rash, hives, or anaphylaxis. Treatment may include administering medications such as hydrocortisone, diphenydramine, epinephrine, and administering oxygen.
Nursing Management • Aggressive IV hydration before the transplant to increase renal perfusion.
Mannitol and sodium bicarbonate may be added to promote osmotic diuresis.
• Premedications such as acetaminophen, diphenydramine, corticosteroids, diuretics, and antiemetics may be administered to diminish DMSO reaction and fluid volume excess.
• Preparation of the stem cell infusion and monitoring the patient for adverse effects.
• Oxygen and suction equipment should be available at the bedside. • Vital signs • The ABO compatible HSCs should be infused over two to four hours
depending on the volume.
Post Stem Cell Infusion The first day post HSC infusion is Day +1, second day id Day + 2, and so on. The first few weeks following the administration of HSC are the most critical. Patients

Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 21
may experience multiple toxicities from the preparative regimen and at the same time have little or no bone marrow function.
Engraftment Engraftment of HSCs refers to the state of acceptance of the infused HSCs as evidenced by a gradual but steady increase in blood counts. Following transplantation, newly infused stem cells give rise to a new hematopoietic and immune system. After a period of typically 1-3 weeks of severe pancytopenia, ther first signs of successful engraftment are monocytes and neutrophils in the blood with a subsequebt increase in platelet count. A reticulocytosis also begins and natural killer (NK) cells are among the earliest donor-derived lymphocytes to appear. G-CSF may be used to reduce period of neutropenia. Engraftment is usually quicker following PBSC transplantation compared with BMT. The marrow cellularity gradually returns to normal but the marrow reserve remains impaired for 1-2 years. There is profound immunodeficiency for 3-12 months with low level of CD4 helper cells and a raised CD8:CD4 ratio for 6 months or more. Immune recovery is quicker after autologous and syngeneic SCT than following allogeneic SCT. The patient’s blood group changes to that of the donor after approximately 60 days. Early evidence of engraftment is seen as the WBC cout rises and the population of cells shifts from lymphocytes to neutrophils. RBCs, platelets, and neutrophils are all capable of functioning effectively as soon as they are generated. However, T cells and B cells returns slowly and may never return to pretransplant levels.
Complications
Graft-Versus-Host Disease This is caused by donor-derived immune cells, particularly T lymphocytes, reacting against recipient tissues. Its incidence is increased with increasing age of donor and recipient and if there is any degree of HLA mismatch between them.
Acute GVHD
In acute GVHD, occurring in the first 100 days, the skin, gastrointestinal tract or liver are affected. The pathophysiology of acute GVHD involves a complex inflammatory response, regulated by the release of various cytokines. An initial development of an inflammatory environment results from host tissue damage from the preparative chemotherapy and radiotherapy regimen. The damaged

Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 22
tissues secrete inflammatory cytokines, interleukin-1, and tumor necrosis factor alpha. Donor and recipient APCs and additional inflammatory cytokines trigger the activation of donor-derived T cells. The activated donor T cells mediate the cytotoxic response against target host cells, which leads to the clinical manifestations of acute GVHD. Mortality associated with acute GVHD is directly related to the severity and extent of organ involvement.
Manifestations of acute GVHD are observed most often in the target organs of the skin, gastrointestinal tract, and liver. The most frequently involved site of acute GVHD is the skin, where observed symptoms include a sometimes painful, pruritic, and maculopapular rash. The rash initially affects the palms of the hands and soles of the feet, with progression to the trunk, chest, and upper back. Gastrointestinal symptoms of acute GVHD include diarrhea with or without anorexia, nausea, and emesis. Progression of those symptoms can lead to gastrointestinal bleeding and ileus formation. In addition, acute GVHD of the liver manifests as hyperbilirubinemia and an increase in alkaline phosphatase. Elevated transaminase levels also may be observed. Progressive acute GVHD of the liver can lead to hepatic failure
Chronic GVHD
Similar to acute GVHD, chronic GVHD also is characterized by time of onset. Generally, symptoms of chronic GVHD occur 100 days after allogeneic transplant. In addition, chronic GVHD is characterized by chronic immunodeficiency; therefore, it often is described as an autoimmune disorder. Symptom onset 100 days after transplant can create diagnostic difficulties. Patients may no longer be at a transplant center, often having returned to a community-based physician practice where familiarity with chronic GVHD may be limited. Frequent follow-up and diligent communication between practice environments are necessary to promote the best possible outcomes. As a multiorgan syndrome, chronic GVHD is the most frequent cause of poor long-term outcomes after allogeneic HSCT.
The incidence of chronic GVHD is widespread with risk factors similar to acute GVHD. The degree of HLA histoincompatibility, patient and donor age, source, and dose of hematopoietic stem cells (i.e., peripheral versus bone marrow) all are established chronic GVHD risk factors. However, a history of prior acute GVHD is the most important predictor of chronic GVHD incidence.
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 23
The pathophysiology of chronic GVHD largely is unclear and much less understood than acute GVHD. Donor-derived alloreactive T cells and thymic CD4+ T cells are believed to be involved in chronic GVHD at the cellular level. Thymus injury by previous history of acute GVHD, pretransplant conditioning regimen, or age-related atrophy impairs the normal ability of the thymus to delete autoreactive T cells. Most experts agree that chronic GVHD is a combination of autoimmune and alloreactive processes.
Clinical manifestations of chronic GVHD can be restricted to a single organ or may be expressed on an extensive scale. Classic symptoms of chronic GVHD are skin changes resembling scleroderma and the presence of sicca syndrome (i.e., extreme dryness of the skin, eyes, and mouth). Most organ systems can be affected by chronic GVHD.
Nursing Implications
A diagnosis of GVHD has numerous implications for oncology nurses. Timely and accurate assessment of presenting symptoms is crucial to GVHD treatment. Nursing management should focus on educating patients and family members or significant others about the signs and symptoms of GVHD. Close monitoring at an appropriate transplant center also is required.
The treatment of GVHD can be stressful and extremely debilitating. The psychological impact of GVHD treatment and quality of life currently is under investigation. Patients may be deconditioned physically or debilitated, as well as psychologically overwhelmed with their diagnosis and treatment. Strategies for managing fatigue, infection risk, and other survivorship issues (e.g., fertility, quality of life) are necessary. Patient and family education is essential for successful outcomes in allogeneic HSCT recipients.
Infections In the early post transplant period, bacterial or fungal infections are frequent. These may be reduced by laminar or positive pressure air flow and the use of skin and mouth antiseptics. Prophylactic therapy with acyclovir, antifungal agents and oral antibiotics is often added. If a fever or other evidence of infections occurs, broad spectrum antibiotics are commenced immediately after blood cultures and other appropriate micobiological specimens have been taken. Failure of response to antibacterial agents is usually an indication to commence systemic antifungal therapy with amphoterecin B, caspofungin or voriconazole.
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 24
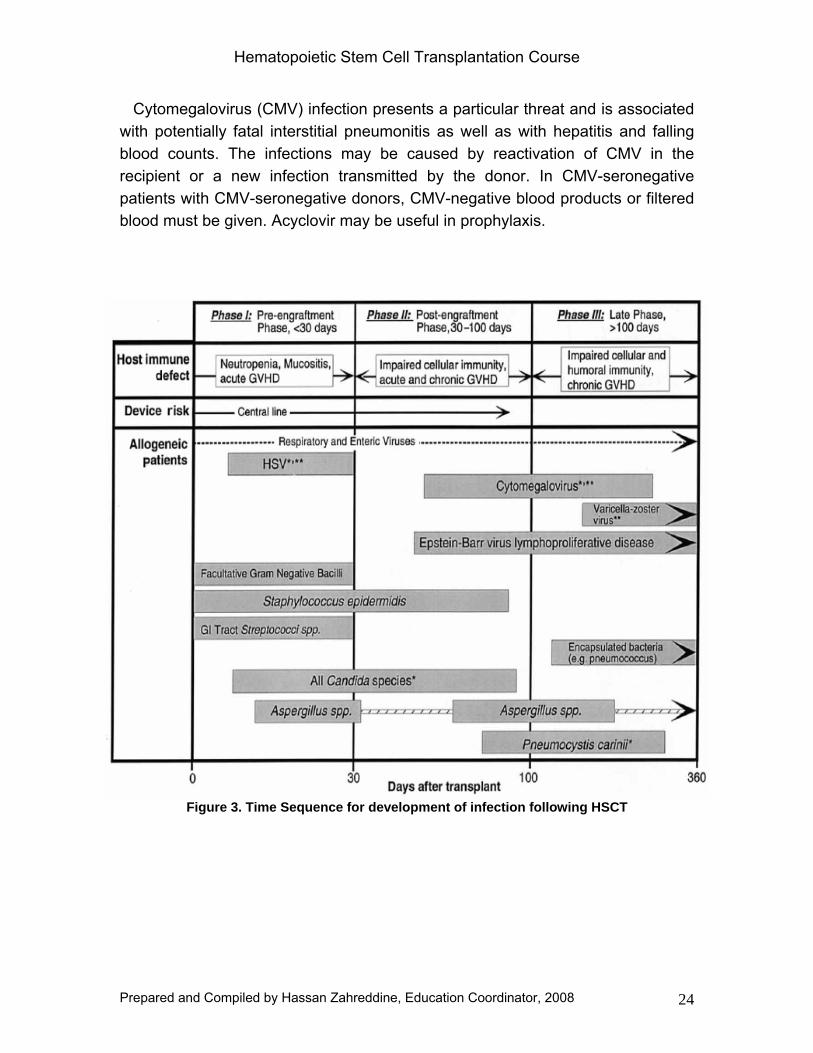
Cytomegalovirus (CMV) infection presents a particular threat and is associated with potentially fatal interstitial pneumonitis as well as with hepatitis and falling blood counts. The infections may be caused by reactivation of CMV in the recipient or a new infection transmitted by the donor. In CMV-seronegative patients with CMV-seronegative donors, CMV-negative blood products or filtered blood must be given. Acyclovir may be useful in prophylaxis.
Figure 3. Time Sequence for development of infection following HSCT
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 25
Graft Failure The risk of graft failure is increased if the patient has aplastic anemia or it T-cell depletion of donor marrow is used as GVHD prophylaxis. This suggests that donor T cells are needed to overcome host resistance to engraftment of stem cells.
Hemorrhagic Cystitis This is usually caused by the cyclophosphamide metabolite acrolein. Mesna is given in an attempt to prevent this. Certain viruses (e.g. adenovirus ot polyomvirus) may also cause this complication.
Veno Occlusive Disease (VOD) Veno Occlusive Disease, also known as sinusoidal obstruction syndrome, is a potentially fatal syndrome of tender hepatomegaly, direct hyperbilirubinemia, ascites, and weight gain. VOD is caused by damage to the sinusoidal endothelium, which results in sinusoidal obstruction. TBI and drugs, such as oral busulfan and cyclophosphamide, predispose patients to this complication. Preexisting liver disease and certain genetic mutations that alter drug metabolism may increase the risk of VOD. No standard effective therapy is currently available.
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 26
References
1. McCarthy, P., Williams, L., Holmes, M. (2005). Stem Cell Transplantation: Past, Present, and Future. In: Bucshel, P., Kapustay, P. Stem Cell Transplantation: A Clinical Textbook. 4th ed. United States of America: Oncology Nursing Society. 1.3-1.12.
2. Sutherland, C. (2005). The immunology of Peripheral Stem Cell Transplantation. In: Bucshel, P., Kapustay, P. Stem Cell Transplantation: A Clinical Textbook. 4th ed. United States of America: Oncology Nursing Society. 2.3-2.20.
3. Letheby, B., Jackson, J., Warkentin, P. (2005). Processing, cryopreservation, and Storage of Peripheral Blood Progenitor Cells. In: Bucshel, P., Kapustay, P. Stem Cell Transplantation: A Clinical Textbook. 4th ed. United States of America: Oncology Nursing Society. 4.3-4.14.
4. Kapustay, P., Buchsel, P. (2005). Process, Complications, and Management of Peripheral Stem Cell Transplantation. In: Bucshel, P., Kapustay, P. Stem Cell Transplantation: A Clinical Textbook. 4th ed. United States of America: Oncology Nursing Society. 5.10-5.25
5. Mills, S., Appel, B. (2005). Umbilical Cord Blood Transplantation. In: Bucshel, P., Kapustay, P. Stem Cell Transplantation: A Clinical Textbook. 4th ed. United States of America: Oncology Nursing Society. 10.3-10.7.
6. Hoffbrand, A.V., Moss, P.A.H, Pettit, J.E (2006). Essential Haematology. 5th ed. Blackwell Publishing: Blackwell Publishing Ltd. 249-262.
7. Williams, L. (2004). Comprehensive Review of Hematopoiesis and Immunology: Implications for Hematopoietic Stem Cell Transplant Recipients. In: Ezzone, S Hematopoietic Stem Cell Transplantation: A Manual for Nursing practice. Unites States of America: Oncology Nursing Society. 1-9.
8. Niess, D., Duffy, K.M., (2004). Basic Concepts of Transplantation. In: Ezzone, S Hematopoietic Stem Cell Transplantation: A Manual for Nursing practice. Unites States of America: Oncology Nursing Society. 13-17
9. Pokorny, K.S., (2004) Stem Cell Collection. In: Ezzone, S Hematopoietic Stem Cell Transplantation: A Manual for Nursing practice. Unites States of America: Oncology Nursing Society. 23-38.
10. McAdams, F.W., Burgunder, M.R. (2004) Transplant Course. In: Ezzone, S Hematopoietic Stem Cell Transplantation: A Manual for Nursing practice. Unites States of America: Oncology Nursing Society. 43-48.
11. Mitchell, S.A. (2004). Graft Versus Host Disease. In: Ezzone, S Hematopoietic Stem Cell Transplantation: A Manual for Nursing practice. Unites States of America: Oncology Nursing Society. 85-97
12. Weisdorf, D. (2007). GVHD-The Nuts and Bolts. Hematology. (1), 62-67. 13. Holler, E. (2007). Progress in Acute Graft Versus Host Disease. Current
Opinion in Hematology. (14), 625-631. 14. Tami, J. A. (1996). Biology and Collection of Hematopoietic Stem Cells.
Highlights on Antineoplastic Drugs. 13 (4), 54-61.
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 27
15. Buer, S.M. (2000). Immunology. In: Yarbo, C.H., Frogge, M.H., Goodman, M., Groenwald, S.L Cancer Nursing: Principles and Practice. 5th ed. United States of America: Jones and Bartlet. 36-46.
16. Whedon, M.B., Roach, M. (2000). In: Yarbo, C.H., Frogge, M.H., Goodman, M., Groenwald, S.L Cancer Nursing: Principles and Practice. 5th ed. United States of America: Jones and Bartlet. 488-503.
17. Mattson. M.R. (2007). Graft-Versus-Host Disease: Review and Nursing Implications. Clinical Journal of Oncology Nursing. 11 (3), 325-328.
18. Laffan, A., Biedrzycki, B. (2006). Immune Reconstitution: The Foundation for Safe Living After an Allogeneic Hematopoietic Stem Cell Transplantation. Clinical Journal of Oncology Nursing. 10 (6), 787-794.
19. Saria, M.G., Gosselin-Acomb,T.K. (2007). Hematopoietic Stem Cell Transplantation: Implications for Critical Care Nurses. Clinical Journal of Oncology Nursing. 11 (1), 53-63.
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 28
Appendix A
Adult HSCT Program at KFSH & RC
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 29
BMT Coordination and Pre-Transplant Work-Up
Patient Referral and Inclusion in the Transplant Program
Patients are usually enrolled in the transplantation program through two distinct channels: 1. New case referral at the outpatient clinic In this setting, the consultant sees the new case, and will discuss briefly with the patient and the family about the possibility of proceeding to BMT. At this specific point in time, the consultant will take the responsibility to:
Refer the patient with his/her family to the BMT coordinating team for HLA typing. The BMT coordinating team will not initiate any teaching on BMT issues until an HLA matched-donor has been identified.
Present in detail and submit for transplantation the new case in question to the Adult BMT team, at a regular Monday afternoon meeting. Once the case is approved for transplant, the BMT coordinator can register the new case on the waiting list as a potential candidate, until the result of the HLA typing.
Schedule a return to clinic within one month for results of the HLA typing.
2. New case referral from the in-patient service In this setting, a patient on the waiting list has been admitted for treatment on E1 or E3 (acute leukemia, aplastic anemia etc). The BMT coordinating team will follow the same logistics. The HLA typing is sometimes not possible in patients with acute leukemia at diagnosis in view of the paucity of lymphocytes. The typing must then be undertaken once the patient is in remission. This new patient must also be fully presented at the regular BMT meeting and be approved for transplant. However, if the team decides that this patient should be transplanted in case of relapse only, the HLA typing should be nonetheless undertaken to accelerate procedures in case of relapse.
Results of HLA Typing When, at a subsequent visit, there is confirmation of an HLA compatible donor, the patient, donor and family should be introduced briefly by the consultant to the
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 30
case manager or the BMT coordinator. At this point in time, the case manager and the BMT coordinating team are responsible for the following:
1. Initiate the recipient pre-transplant workup as per protocol 2. Initiate the donor workup as per protocol 3. Initiate intensive teaching about:
The nature of the patient’s disease and the reason for transplantation. The effects of chemotherapy, including sterility The nature and mechanics of the transplantation itself The major complications of transplantation The importance of reverse isolation The importance of following recommended treatment and guidelines
(urine collection, compliance to hygiene etc) The post-transplant follow-up (patients who live far from hospital have to
stay in Riyadh until Day +120, weekly visits at the BMT clinic, the issue of the mask, compliance to medication, hydration, etc.).
The consultant must be involved in elaborate teaching at the onset of BMT discussions with the patient and family. The role of the case manager and the coordination team is also extremely important at this specific stage. No patient should be hospitalized on the BMT ward for transplantation without being fully aware of all the transplant related issues. When needed, the case manager and the BMT coordinating team will be supported in this teaching process by the consultant responsible for the BMT clinic or for patient care on the ward. The case manager and BMT coordinating team will have to make regular visits on the ward to provide teaching to hospitalized patients, to their families and to make sure that all pre-transplant workup procedures are completed as per protocol. A social and psychological evaluation of the patient will have to be completed and discussed with the transplant team.
Every patient should be provided with a self-explanatory and well-illustrated, detailed educational pamphlet, dealing will all aspects of bone marrow transplantation.
Planning for Date of Transplant The list of patients eligible for transplant is reviewed thoroughly at the weekly BMT meeting. Patients are prioritized according to diagnosis and risk of relapse. The date of admission for transplant and the initiation of the preparative regimen are determined by the coordinating team, as the schedules for bone marrow or peripheral blood stem cell harvest. PBHSC transplantation implies that the
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 31
coordinating team will make sure that the donor has a satisfactory venous access for harvest procedures. The donor must be evaluated by the apheresis team and decisions for the need of a catheter for apheresis must be taken well in advance. Teaching about mobilization procedures is the responsibility of the coordinating team.
Preparation for Discharge In order to facilitate the post-transplant follow-up at the BMT clinics, the coordinating team will have the responsibility to:
1. Make sure that the family and patient understand the importance of staying in the vicinity of the hospital until Day +120. 2. Explain the logistics of the BMT clinics 3. Initiate post-transplant teaching, such as the role and importance of adequate hydration, wearing of mask, low bacteria diet, etc. 4. Stress the importance of being compliant to the medication prescribed 5. Make sure that the patient discharge form is properly filled by the resident, fellow or consultant in order to insure adequate post-transplant follow-up at the BMT clinic.
Post-Transplant Follow-up at the BMT Clinic At discharge, patients will be referred to the corresponding consultant afternoon BMT Clinic. At presentation, the nursing team assigned to the BMT clinic will have the responsibility to:
Check the blood pressure, weight, and temperature Verify the patient’s compliance to the medication prescribed at the time
of discharge Obtain the appropriate blood work and chart results in the progress notes Assist the ward clerk with next appointment booking.
The BMT coordinator will be responsible for flagging the regular post-transplant workup, scheduled as per protocol at Day 120, 1 and 2 years post-transplant. Also, as per protocol, high-risk patients destined to receive post-transplant I.T. MTX at specific weeks post-transplant, need to be flagged by the BMT coordinator.
The BMT coordinator and case manager will be responsible for triage and will decide if a patient needs to be seen at the BMT drop in clinic or at one of the regular BMT clinics. If they need assistance in decision-making, they will refer to the consultant in charge of the clinic.
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 32
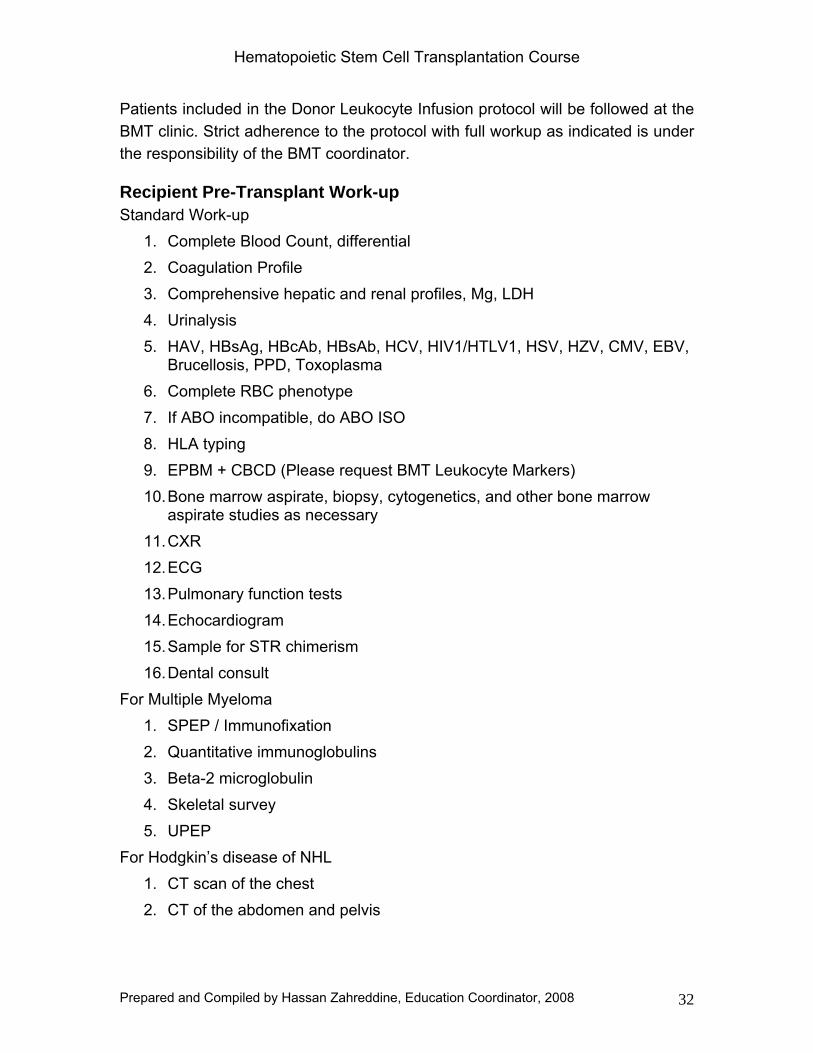
Patients included in the Donor Leukocyte Infusion protocol will be followed at the BMT clinic. Strict adherence to the protocol with full workup as indicated is under the responsibility of the BMT coordinator.
Recipient Pre-Transplant Work-up Standard Work-up
1. Complete Blood Count, differential 2. Coagulation Profile 3. Comprehensive hepatic and renal profiles, Mg, LDH 4. Urinalysis 5. HAV, HBsAg, HBcAb, HBsAb, HCV, HIV1/HTLV1, HSV, HZV, CMV, EBV,
Brucellosis, PPD, Toxoplasma 6. Complete RBC phenotype 7. If ABO incompatible, do ABO ISO 8. HLA typing 9. EPBM + CBCD (Please request BMT Leukocyte Markers) 10. Bone marrow aspirate, biopsy, cytogenetics, and other bone marrow
aspirate studies as necessary 11. CXR 12. ECG 13. Pulmonary function tests 14. Echocardiogram 15. Sample for STR chimerism 16. Dental consult
For Multiple Myeloma 1. SPEP / Immunofixation 2. Quantitative immunoglobulins 3. Beta-2 microglobulin 4. Skeletal survey 5. UPEP
For Hodgkin’s disease of NHL 1. CT scan of the chest 2. CT of the abdomen and pelvis
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 33
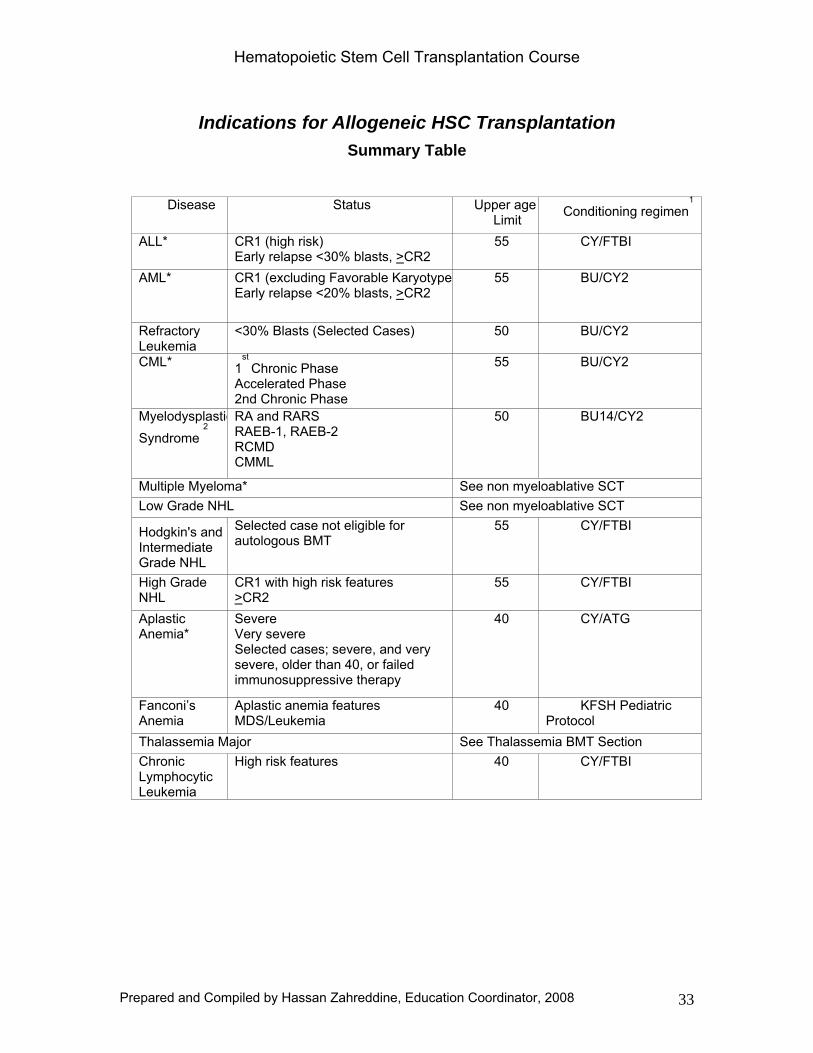
Indications for Allogeneic HSC Transplantation Summary Table
Disease Status Upper age
Limit Conditioning regimen1
ALL* CR1 (high risk) Early relapse <30% blasts, >CR2
55 CY/FTBI
AML* CR1 (excluding Favorable KaryotypeEarly relapse <20% blasts, >CR2
55 BU/CY2
Refractory Leukemia
<30% Blasts (Selected Cases) 50 BU/CY2
CML* 1st
Chronic Phase Accelerated Phase 2nd Chronic Phase
55 BU/CY2
MyelodysplasticSyndrome
2
RA and RARS RAEB-1, RAEB-2 RCMD CMML
50 BU14/CY2
Multiple Myeloma* See non myeloablative SCT Low Grade NHL See non myeloablative SCT
Hodgkin's and 3
Intermediate Grade NHL
Selected case not eligible for autologous BMT
55 CY/FTBI
High Grade NHL
CR1 with high risk features >CR2
55 CY/FTBI
Aplastic Anemia*
Severe Very severe Selected cases; severe, and very severe, older than 40, or failed immunosuppressive therapy
40 CY/ATG
Fanconi’s Anemia
Aplastic anemia features MDS/Leukemia
40 KFSH Pediatric Protocol
Thalassemia Major See Thalassemia BMT Section Chronic Lymphocytic Leukemia
High risk features 40 CY/FTBI
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 34
Allogeneic Bone Marrow and Peripheral Stem Cell
Transplantation Programs
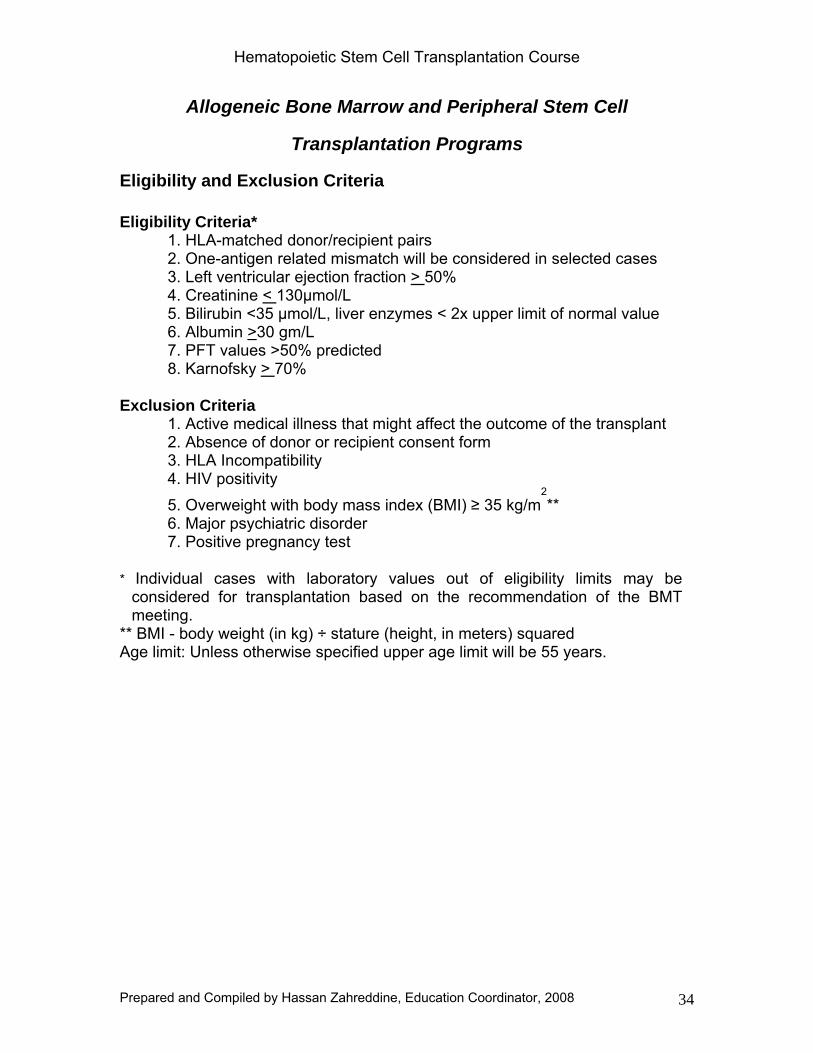
Eligibility and Exclusion Criteria
Eligibility Criteria* 1. HLA-matched donor/recipient pairs 2. One-antigen related mismatch will be considered in selected cases 3. Left ventricular ejection fraction > 50% 4. Creatinine < 130μmol/L 5. Bilirubin <35 μmol/L, liver enzymes < 2x upper limit of normal value 6. Albumin >30 gm/L 7. PFT values >50% predicted 8. Karnofsky > 70%
Exclusion Criteria
1. Active medical illness that might affect the outcome of the transplant 2. Absence of donor or recipient consent form 3. HLA Incompatibility 4. HIV positivity 5. Overweight with body mass index (BMI) ≥ 35 kg/m
2**
6. Major psychiatric disorder 7. Positive pregnancy test
* Individual cases with laboratory values out of eligibility limits may be
considered for transplantation based on the recommendation of the BMT meeting.
** BMI - body weight (in kg) ÷ stature (height, in meters) squared Age limit: Unless otherwise specified upper age limit will be 55 years.
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 35
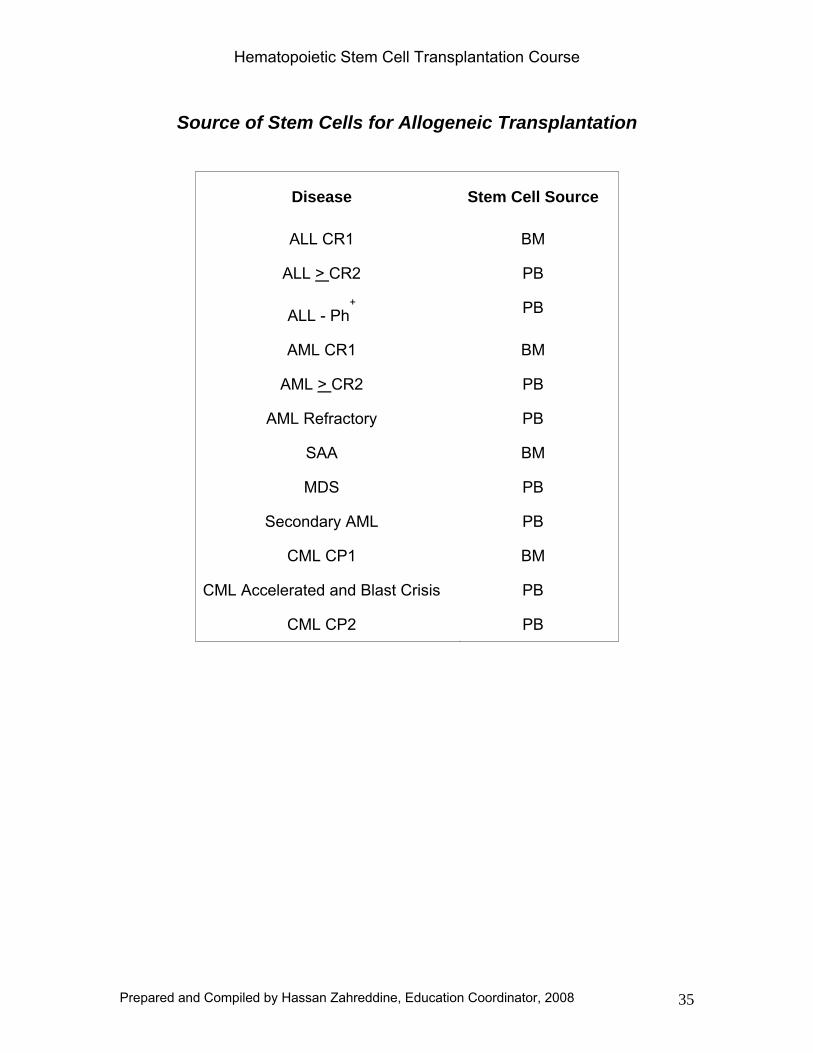
Source of Stem Cells for Allogeneic Transplantation
Disease Stem Cell Source
ALL CR1 BM
ALL > CR2 PB
ALL - Ph+ PB
AML CR1 BM
AML > CR2 PB
AML Refractory PB
SAA BM
MDS PB
Secondary AML PB
CML CP1 BM
CML Accelerated and Blast Crisis PB
CML CP2 PB
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 36
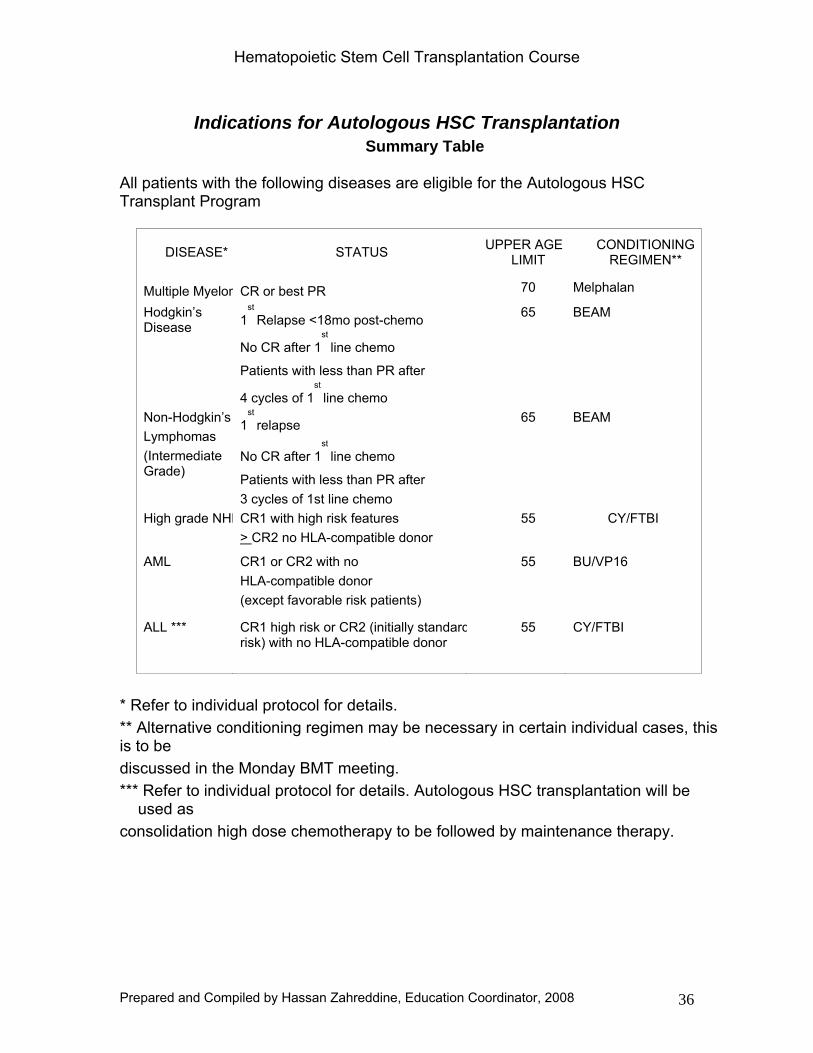
Indications for Autologous HSC Transplantation Summary Table
All patients with the following diseases are eligible for the Autologous HSC Transplant Program
DISEASE* STATUS UPPER AGELIMIT
CONDITIONING REGIMEN**
Multiple MyelomCR or best PR 70 Melphalan
Hodgkin’s Disease 1
st
Relapse <18mo post-chemo
No CR after 1st
line chemo
Patients with less than PR after
4 cycles of 1st
line chemo
65 BEAM
Non-Hodgkin’s Lymphomas (Intermediate Grade)
1st
relapse
No CR after 1st
line chemo
Patients with less than PR after 3 cycles of 1st line chemo
65 BEAM
High grade NHLCR1 with high risk features > CR2 no HLA-compatible donor
55 CY/FTBI
AML CR1 or CR2 with no HLA-compatible donor (except favorable risk patients)
55 BU/VP16
ALL *** CR1 high risk or CR2 (initially standardrisk) with no HLA-compatible donor
55 CY/FTBI
* Refer to individual protocol for details. ** Alternative conditioning regimen may be necessary in certain individual cases, this is to be discussed in the Monday BMT meeting. *** Refer to individual protocol for details. Autologous HSC transplantation will be
used as consolidation high dose chemotherapy to be followed by maintenance therapy.
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 37
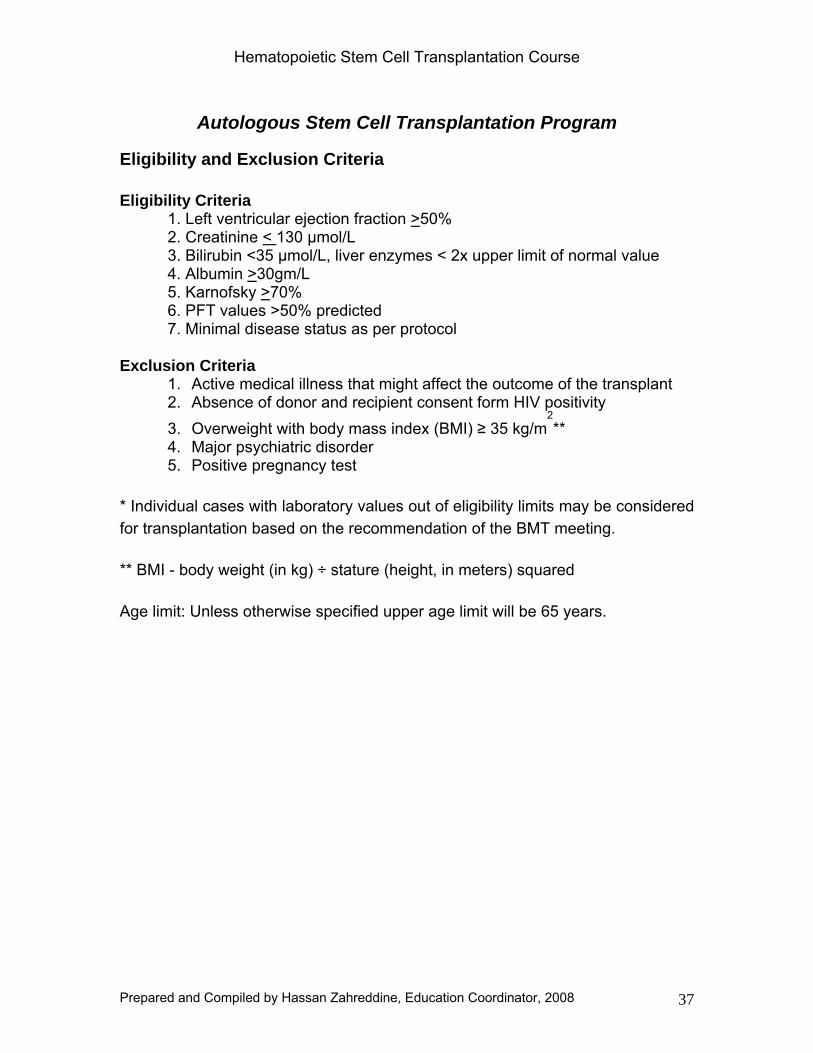
Autologous Stem Cell Transplantation Program
Eligibility and Exclusion Criteria
Eligibility Criteria 1. Left ventricular ejection fraction >50% 2. Creatinine < 130 μmol/L 3. Bilirubin <35 μmol/L, liver enzymes < 2x upper limit of normal value 4. Albumin >30gm/L 5. Karnofsky >70% 6. PFT values >50% predicted 7. Minimal disease status as per protocol
Exclusion Criteria
1. Active medical illness that might affect the outcome of the transplant 2. Absence of donor and recipient consent form HIV positivity 3. Overweight with body mass index (BMI) ≥ 35 kg/m
2**
4. Major psychiatric disorder 5. Positive pregnancy test
* Individual cases with laboratory values out of eligibility limits may be considered for transplantation based on the recommendation of the BMT meeting.
** BMI - body weight (in kg) ÷ stature (height, in meters) squared
Age limit: Unless otherwise specified upper age limit will be 65 years.
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 38
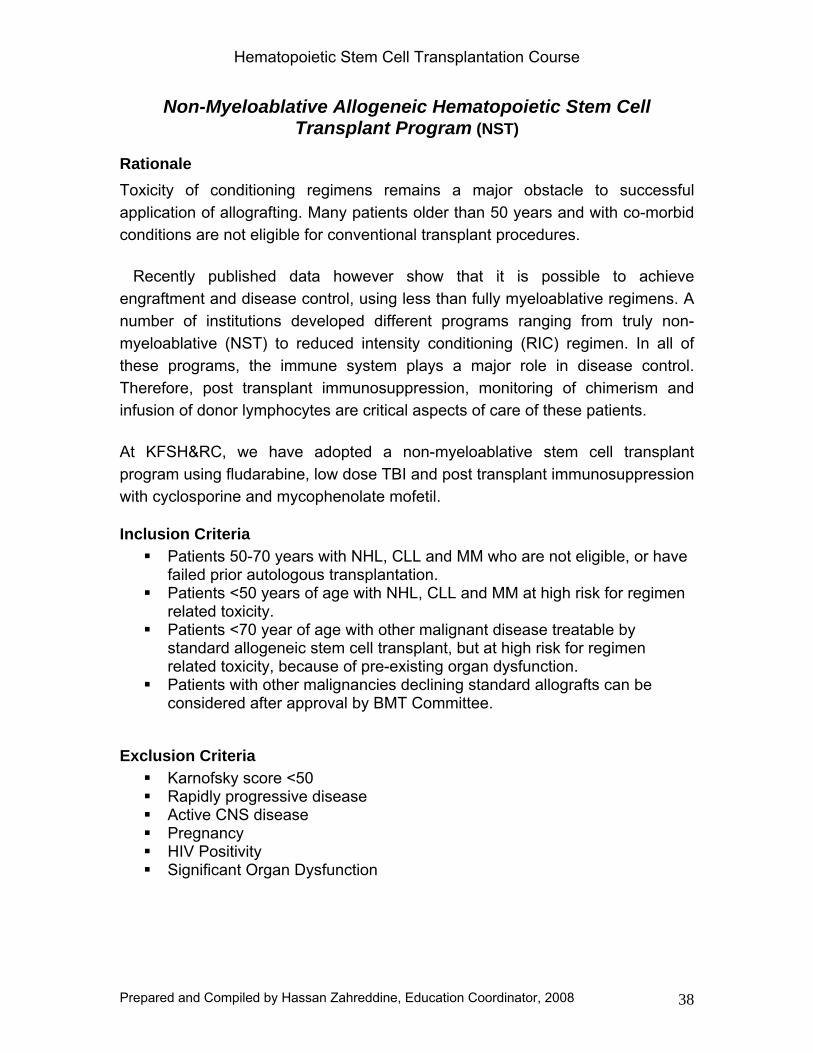
Non-Myeloablative Allogeneic Hematopoietic Stem Cell Transplant Program (NST)
Rationale Toxicity of conditioning regimens remains a major obstacle to successful application of allografting. Many patients older than 50 years and with co-morbid conditions are not eligible for conventional transplant procedures.
Recently published data however show that it is possible to achieve engraftment and disease control, using less than fully myeloablative regimens. A number of institutions developed different programs ranging from truly non-myeloablative (NST) to reduced intensity conditioning (RIC) regimen. In all of these programs, the immune system plays a major role in disease control. Therefore, post transplant immunosuppression, monitoring of chimerism and infusion of donor lymphocytes are critical aspects of care of these patients.
At KFSH&RC, we have adopted a non-myeloablative stem cell transplant program using fludarabine, low dose TBI and post transplant immunosuppression with cyclosporine and mycophenolate mofetil.
Inclusion Criteria Patients 50-70 years with NHL, CLL and MM who are not eligible, or have
failed prior autologous transplantation. Patients <50 years of age with NHL, CLL and MM at high risk for regimen
related toxicity. Patients <70 year of age with other malignant disease treatable by
standard allogeneic stem cell transplant, but at high risk for regimen related toxicity, because of pre-existing organ dysfunction.
Patients with other malignancies declining standard allografts can be considered after approval by BMT Committee.
Exclusion Criteria Karnofsky score <50 Rapidly progressive disease Active CNS disease Pregnancy HIV Positivity Significant Organ Dysfunction
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 39
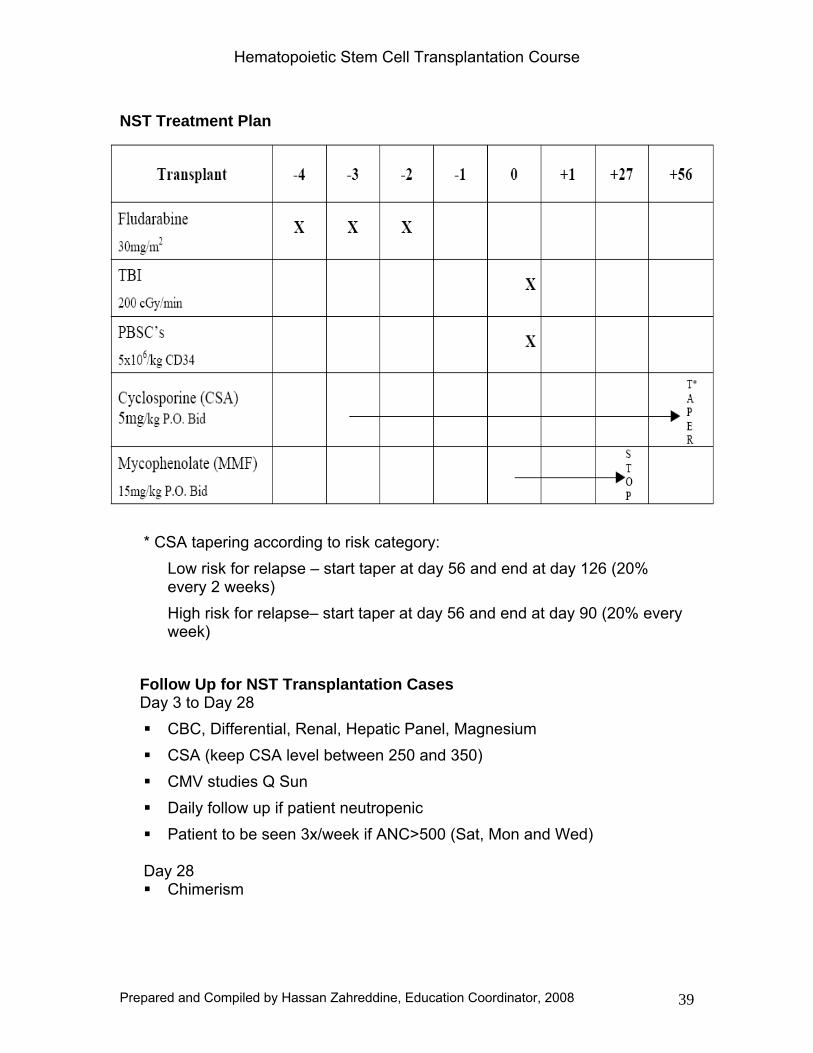
NST Treatment Plan
* CSA tapering according to risk category:
Low risk for relapse – start taper at day 56 and end at day 126 (20% every 2 weeks) High risk for relapse– start taper at day 56 and end at day 90 (20% every week)
Follow Up for NST Transplantation Cases Day 3 to Day 28
CBC, Differential, Renal, Hepatic Panel, Magnesium CSA (keep CSA level between 250 and 350) CMV studies Q Sun Daily follow up if patient neutropenic Patient to be seen 3x/week if ANC>500 (Sat, Mon and Wed)
Day 28 Chimerism
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 40
Day 28 to Day 56 CBC, Differential, Renal, Hepatic Panel, Magnesium CSA (keep CSA level between 250 and 350) CMV studies Q Sun Patient to be seen 2x/week
Day 56 Chimerism
Upon results of chimerism, inform the primary physician of the result and
follow guidelines for DLI as described in the attached table. Day 120 For all scenarios 120 days work up as per allogeneic post BMT protocol
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 41
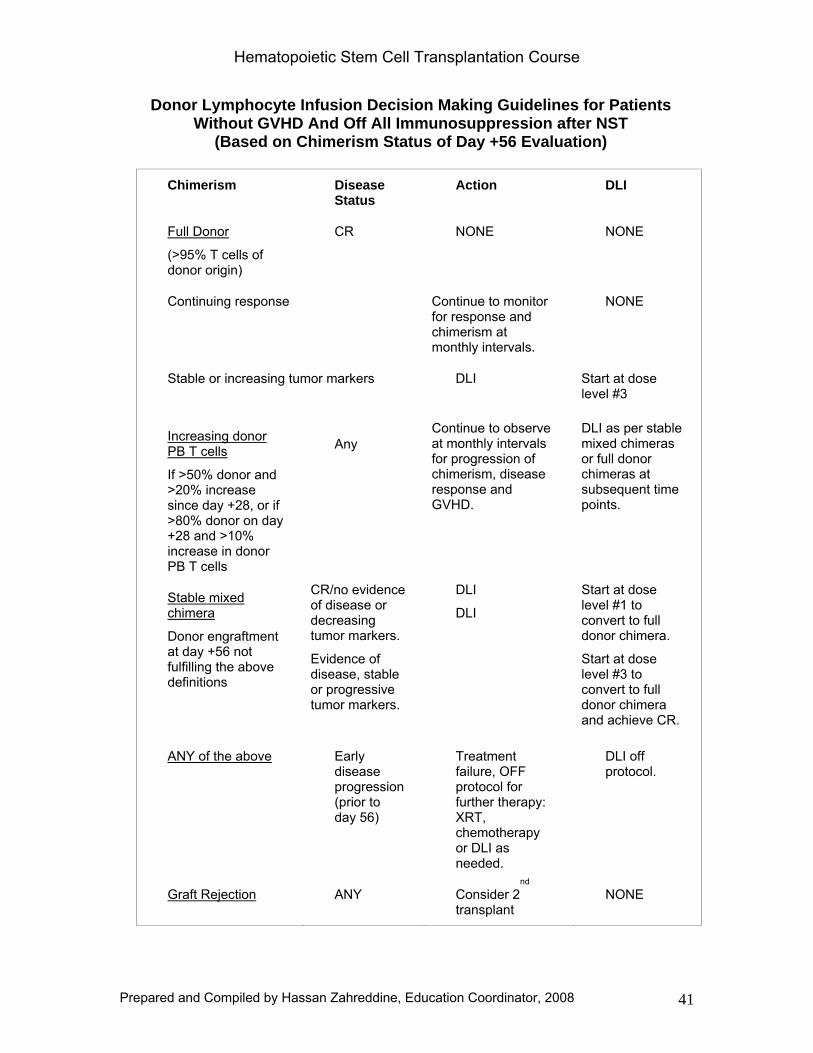
Donor Lymphocyte Infusion Decision Making Guidelines for Patients Without GVHD And Off All Immunosuppression after NST
(Based on Chimerism Status of Day +56 Evaluation)
Chimerism Disease Status
Action DLI
Full Donor
(>95% T cells of donor origin)
CR NONE NONE
Continuing response Continue to monitor for response and chimerism at monthly intervals.
NONE
Stable or increasing tumor markers DLI Start at dose level #3
Increasing donor PB T cells
If >50% donor and >20% increase since day +28, or if >80% donor on day +28 and >10% increase in donor PB T cells
Any Continue to observe at monthly intervals for progression of chimerism, disease response and GVHD.
DLI as per stable mixed chimeras or full donor chimeras at subsequent time points.
Stable mixed chimera
Donor engraftment at day +56 not fulfilling the above definitions
CR/no evidence of disease or decreasing tumor markers.
Evidence of disease, stable or progressive tumor markers.
DLI
DLI
Start at dose level #1 to convert to full donor chimera.
Start at dose level #3 to convert to full donor chimera and achieve CR.
ANY of the above Early disease progression (prior to day 56)
Treatment failure, OFF protocol for further therapy: XRT, chemotherapy or DLI as needed.
DLI off protocol.
Graft Rejection ANY Consider 2nd
transplant NONE
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 42
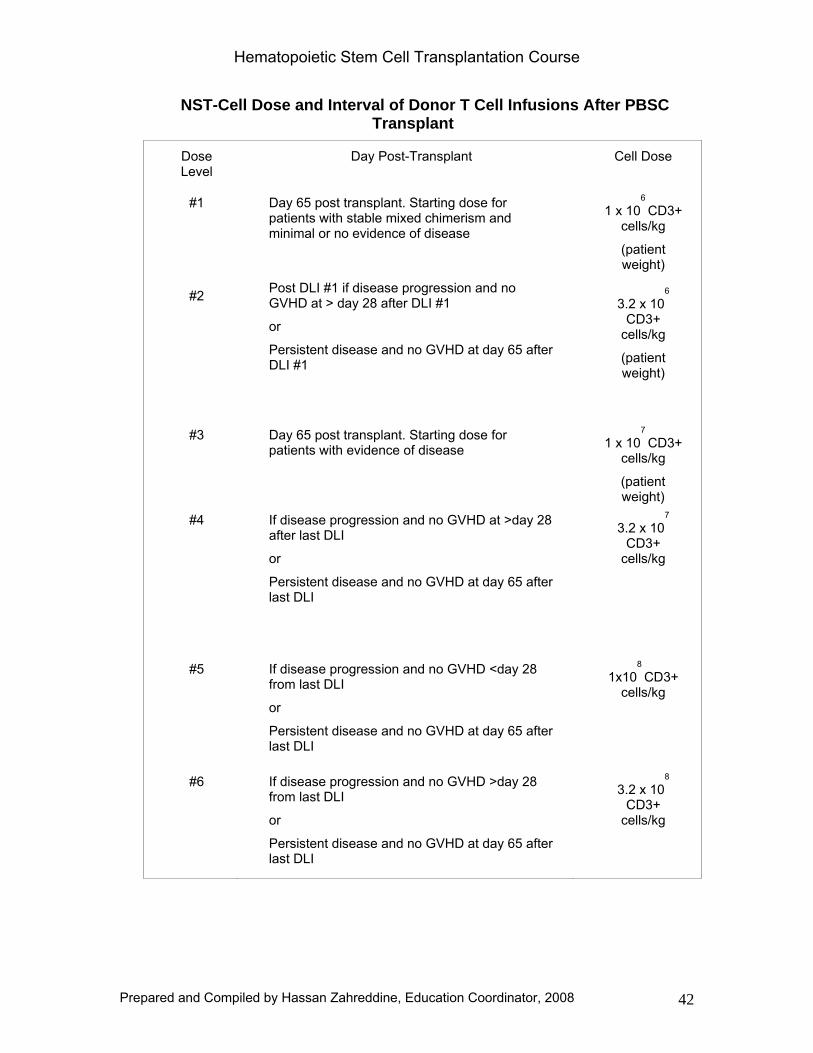
NST-Cell Dose and Interval of Donor T Cell Infusions After PBSC Transplant
Dose Level
Day Post-Transplant Cell Dose
#1 Day 65 post transplant. Starting dose for patients with stable mixed chimerism and minimal or no evidence of disease
1 x 106
CD3+ cells/kg
(patient weight)
#2 Post DLI #1 if disease progression and no GVHD at > day 28 after DLI #1
or
Persistent disease and no GVHD at day 65 after DLI #1
3.2 x 106
CD3+ cells/kg
(patient weight)
#3 Day 65 post transplant. Starting dose for patients with evidence of disease 1 x 10
7
CD3+ cells/kg
(patient weight)
#4 If disease progression and no GVHD at >day 28 after last DLI
or
Persistent disease and no GVHD at day 65 after last DLI
3.2 x 107
CD3+ cells/kg
#5 If disease progression and no GVHD <day 28 from last DLI
or
Persistent disease and no GVHD at day 65 after last DLI
1x108
CD3+ cells/kg
#6 If disease progression and no GVHD >day 28 from last DLI
or
Persistent disease and no GVHD at day 65 after last DLI
3.2 x 108
CD3+ cells/kg
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 43
Immunotherapy Since the original reports of treatment of patients with donor buffy coat infusions, donor lymphocyte infusions (DLI) have become widely accepted form of immunotherapy. DLIs are used primarily to treat patients with CML who relapse after allogeneic bone marrow transplantation and to induce the state of full donor chimerism after non-myeloablative stem cell transplants.
After diagnosis of relapse, chimerism status must be determined and immunosuppression stopped or quickly tapered. If no GVHD develops, DLI will be administered according to following guidelines.
Inclusion Criteria
1. Molecular (progressive increase in Q PCR value), cytogenetic or hematologic relapse of CML
2. Other malignancies (AML, ALL, MM, MDS, NHL, CML-BC, others) to be considered on individual case basis
3. Presence of residual donor T-cell chimerism
4. Karnofsky performance status >70
5. No significant organ dysfunction
Exclusion Criteria
1. Clinical GVHD
2. No donor T-cells present in blood or marrow
3. Rapidly progressive disease
4. Relapse less then 6 months after transplant (Except for CML)
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 44
Dietary Guidelines When patients become neutropenic they will select from a low-bacteria diet with the help of a dietitian and the food will be prepared by dietary services. The practice of bringing food from outside the hospital will be discouraged.
The only food that will be allowed from the outside is pre-packaged individual servings of cookies, crackers, pretzels, candy, and chips as well as pasteurized juices and drinks that can be consumed at one sitting. Any other exception to food from the outside requires a written order from the attending physician.
These guidelines are intended to minimize the introduction of pathogenic organism into the gastrointestinal tract by food while maximizing healthy food options for immunocompromised patients.
Basic safe food handling techniques should be practiced to decrease the risk of microbial contamination. Sanitary food practices can decrease the incidence of food-borne illnesses which can be life threatening to immune suppressed patients.
The guidelines consist of foods that have been shown by culture to be safe when properly prepared in the home and hospital kitchen. High-risk foods identified as potential sources of organisms known to cause infection in immunossupressed patients are restricted.
The diet guidelines meet the recommended dietary allowances of the National Research Council for all nutrients when carefully planned by patient and dietician and monitored for actual food intake. Multi-vitamin supplements (without iron when indicated) may be required if food intake is poor.
Food Restrictions 1. Raw vegetables and fruits 2. Raw or unpasteurized honey 3. Unpasteurized and raw milk products including cheese and yogurt 4. All moldy and out-dated food products 5. Well water, unless in large population, tested frequently and found safe 6. Herbal and non-traditional (health food store) nutrient supplements 7. Raw and under cooked meats, fish, shell fish, poultry, eggs 8. Cold smoke fish (salmon), pickled fish
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 45
9. Refrigerated cheese-based salad dressings (e.g. blue cheese), not shelf stable
10. Aged cheese, (e.g. brie, camembert, blue, Roquefort, sharp cheddar, stilton, etc)
Restaurants are not recommended, but if necessary, it is highly recommended that patients go at times when the restaurant is quiet. All food must be freshly prepared and hot, no salad bars or buffets at any time.
Food Preparation Tips wash hands before and after handling leftovers use clean utensils and food preparation surfaces divide leftovers into small units and store in shallow containers for quick
cooling refrigerate leftovers within 2 hours of cooking discard leftovers that were kept at room temperature for >2 hours reheat leftovers or heat partially cooked food throughout before serving bring leftover soups, sauces, and gravies to a rolling boil before serving follow published guidelines for cold storage of food
Discontinuation Autologous patient may discontinue guidelines three months post-transplant, unless directed by physician otherwise. Allogeneic patients may discontinue guidelines when off all immunosuppressive therapy unless directed by physician otherwise.
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 46
TREATMENT GUIDELINES FOR PATIENTS WITH FEVER AND NEUTROPENIA
These guidelines are intended to provide a unified recommendation for empirical antimicrobial therapy for adult patients with neutropenia and fever without a clear clinical source. Depending on the cause of neutropenia, other medical conditions, procedures or allergies, certain modifications may be required. These guidelines should not be a substitute to informed, sound medical judgment in individual cases. They were based on current available literature and resistance patterns of invasive microbial flora of medical units with high proportion of neutropenic patients. The role of simple but useful infection control policies and measures is very important in neutropenic patients. The importance of proper handwashing before examining any patient cannot be overemphasized.
Evaluation prior to initiating antimicrobial therapy should include physical examination, blood cultures from indwelling catheter and peripheral veins, urine analysis, and culture, CXR, other clinically indicated work-up (e.g. diarrheal stool, skin lesions).
Definitions Adult Patient: Age > 14 Years (Gregorian)
Fever: A single oral temperature of > 38.3oC, or > 38.0
oC over at least one
hour
Neutropenia: Absolute neutrophil count of < 500/mm3
Unstable patient: SBP<90 mmHg or drop of >20 mmHg points in systolic blood pressure from baseline
I. Antibacterial Prophylaxis in Afebrile Neutropenic Patients The use of antibacterial prophylaxis does not reduce febrile episodes in neutropenic patients. It enhances the chances for resistance in break through blood stream infection, eliminating useful therapeutic agents that were used as prophylaxis. It is not recommended to use antibacterial prophylaxis in neutropenic patients.
II. Empirical Antibacterial Therapy a. Clinically stable patients with first temperature spike with no identified source of fever:
i. First Choice: Cefepime (2 gm every 8 hours) and gentamicin (2mg/kg every 12 hours)
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 47
ii. Second Choice: Tazocin (4.5 gm every 8 hours) and gentamicin (2mg/kg every 12 hours)
b. Unstable patients with hypotension and impending shock: i. Imipenem (500mg every 6 hours) or Meropenem (1gm every 8 hours) and gentamicin (dosed as above)
c. Gentamicin can be discontinued after three days depending on clinical course and culture results. d. Order levels only if patients will be on gentamicin for more than 3 days. e. Adjust dosing according to renal function.
III. Use of Vancomycin in Febrile Neutropenic Patients Vancomycin is recommended as part of empirical therapy in the following situations:
a. Hemodynamically unstable patients b. Line related infection c. Severe mucositis d. Cutaneous infections
It can be discontinued based on clinical course and culture results. IV. Duration of Antimicrobial Therapy a. If the source of infection is identified, it should be treated accordingly. If fever subsides, antipseudomonal monotherapy should be continued until ANC is > 500/mm
3 for three days.
b. Persistent fever beyond three days with negative work-up should prompt reassessment rather than switching to meropenem if patients remains stable.
c. Antibiotics should be changed according to clinical findings or culture results (e.g. patient on Carbapenem and isolated organism sensitive to Tazocin, should be switched to Tazocin).
V. Antifungal Prophylaxis and Therapy
Antifungal prophylaxis is recommended for high risk groups of patients receiving cancer chemotherapy. Fluconazole is the only agent that has shown significant benefit in prospective randomized trials.
a. Leukemia patients who received chemotherapy with neutropenia expected to be less than 21 days: No antifungal prophylaxis.
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 48
b. Leukemia patients and auto SCT with neutropenia expected to be more than 21 days and all allogeneic HSCT: Oral fluconazole 200mg daily during the period of neutropenia. (I.V. substitute will be permitted for HSCT patient unable to take PO).
c. Patients with previous episode of candidemia should receive fluconazole 200 mg orally daily unless it is known to be resistant to fluconazole, then the choice is amphotericin B at 0.5 mg/kg/d. If the patient has previous aspergillosis, then he/she has to be on amphotericin B prophylaxis 0.7 to 1 mg/kg/d.
d. Empiric antifungal therapy for febrile neutropenics not responding to antibacterials: amphotericin 0.5 - 0.7 mg/kg/day, and if Aspergillus is suspected 1 mg/kg/day should be administered on day 6 after initiation of anti-gram negative coverage and in patients on no antifungal prophylaxis who are deteriorating rapidly with sepsis syndrome.
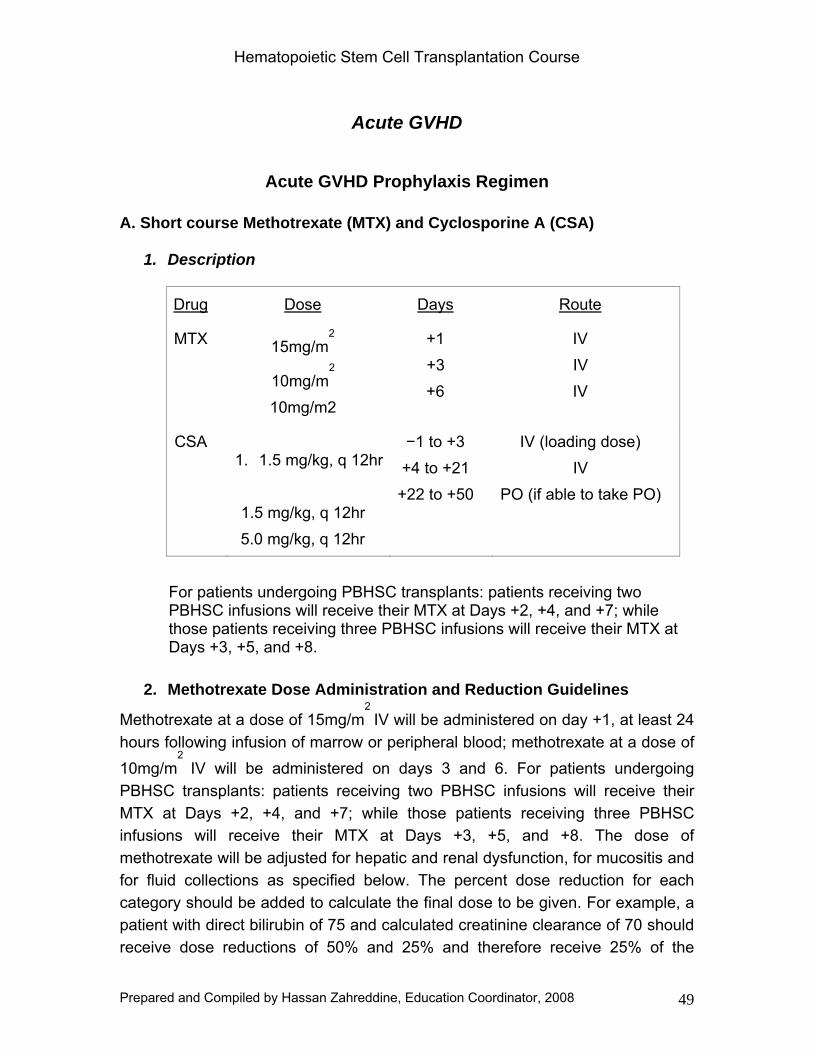
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 49
Acute GVHD
Acute GVHD Prophylaxis Regimen A. Short course Methotrexate (MTX) and Cyclosporine A (CSA)
1. Description
Drug Dose Days Route
MTX 15mg/m2
10mg/m2
10mg/m2
+1 +3 +6
IV IV IV
CSA 1. 1.5 mg/kg, q 12hr 1.5 mg/kg, q 12hr 5.0 mg/kg, q 12hr
−1 to +3 +4 to +21 +22 to +50
IV (loading dose) IV
PO (if able to take PO)
For patients undergoing PBHSC transplants: patients receiving two PBHSC infusions will receive their MTX at Days +2, +4, and +7; while those patients receiving three PBHSC infusions will receive their MTX at Days +3, +5, and +8.
2. Methotrexate Dose Administration and Reduction Guidelines
Methotrexate at a dose of 15mg/m2
IV will be administered on day +1, at least 24 hours following infusion of marrow or peripheral blood; methotrexate at a dose of 10mg/m
2 IV will be administered on days 3 and 6. For patients undergoing
PBHSC transplants: patients receiving two PBHSC infusions will receive their MTX at Days +2, +4, and +7; while those patients receiving three PBHSC infusions will receive their MTX at Days +3, +5, and +8. The dose of methotrexate will be adjusted for hepatic and renal dysfunction, for mucositis and for fluid collections as specified below. The percent dose reduction for each category should be added to calculate the final dose to be given. For example, a patient with direct bilirubin of 75 and calculated creatinine clearance of 70 should receive dose reductions of 50% and 25% and therefore receive 25% of the
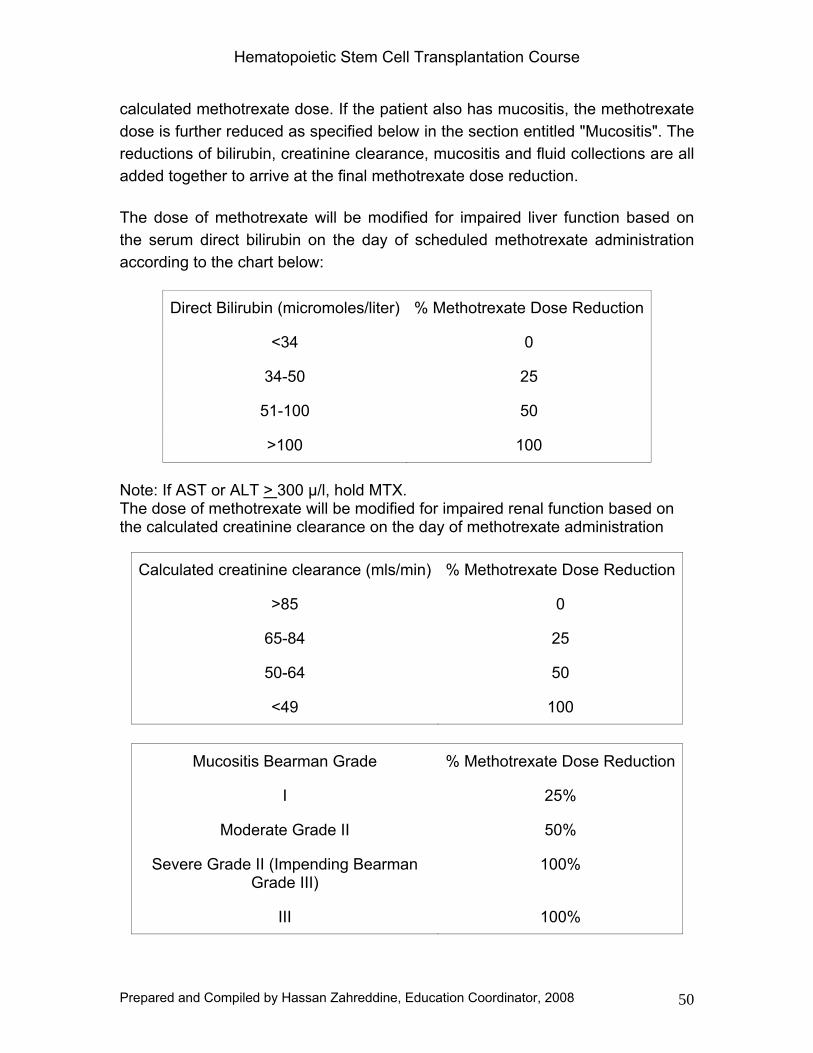
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 50
calculated methotrexate dose. If the patient also has mucositis, the methotrexate dose is further reduced as specified below in the section entitled "Mucositis". The reductions of bilirubin, creatinine clearance, mucositis and fluid collections are all added together to arrive at the final methotrexate dose reduction.
The dose of methotrexate will be modified for impaired liver function based on the serum direct bilirubin on the day of scheduled methotrexate administration according to the chart below:
Direct Bilirubin (micromoles/liter) % Methotrexate Dose Reduction
<34 0
34-50 25
51-100 50
>100 100
Note: If AST or ALT > 300 μ/l, hold MTX. The dose of methotrexate will be modified for impaired renal function based on the calculated creatinine clearance on the day of methotrexate administration
Calculated creatinine clearance (mls/min) % Methotrexate Dose Reduction
>85 0
65-84 25
50-64 50
<49 100
Mucositis Bearman Grade % Methotrexate Dose Reduction
I 25%
Moderate Grade II 50%
Severe Grade II (Impending Bearman Grade III)
100%
III 100%
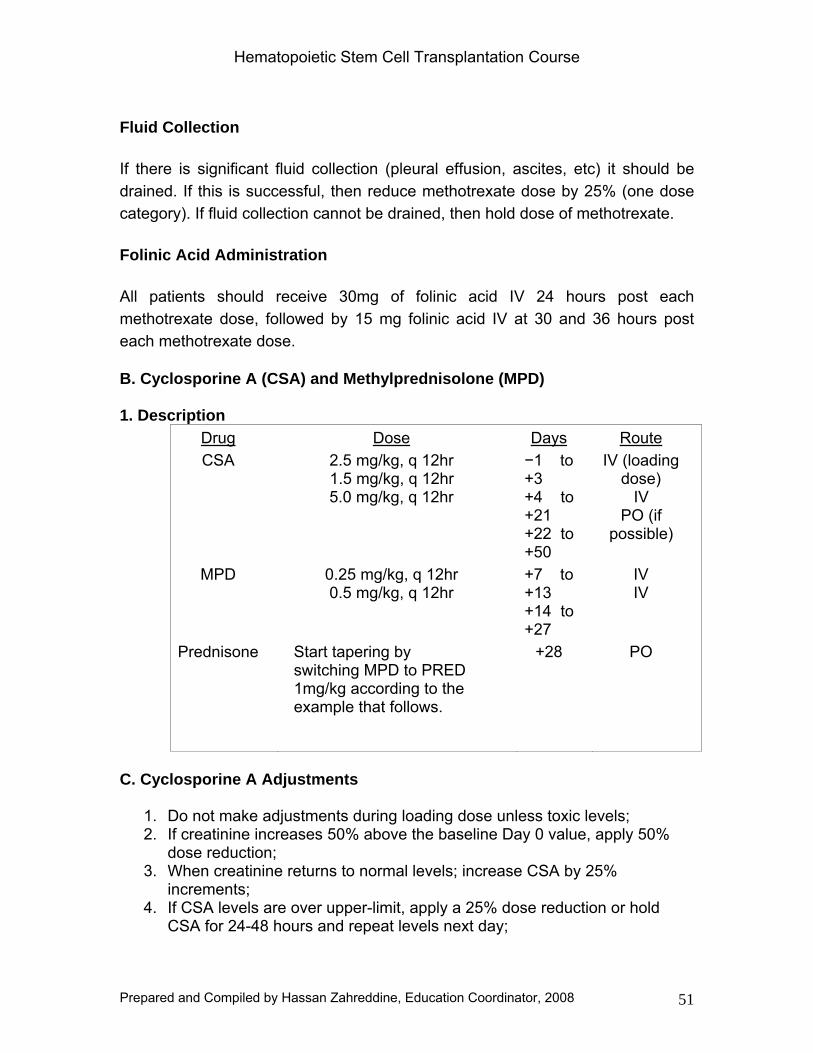
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 51
Fluid Collection
If there is significant fluid collection (pleural effusion, ascites, etc) it should be drained. If this is successful, then reduce methotrexate dose by 25% (one dose category). If fluid collection cannot be drained, then hold dose of methotrexate.
Folinic Acid Administration
All patients should receive 30mg of folinic acid IV 24 hours post each methotrexate dose, followed by 15 mg folinic acid IV at 30 and 36 hours post each methotrexate dose.
B. Cyclosporine A (CSA) and Methylprednisolone (MPD) 1. Description
Drug Dose Days Route CSA 2.5 mg/kg, q 12hr
1.5 mg/kg, q 12hr 5.0 mg/kg, q 12hr
−1 to +3 +4 to +21 +22 to +50
IV (loading dose)
IV PO (if
possible)
MPD 0.25 mg/kg, q 12hr 0.5 mg/kg, q 12hr
+7 to +13 +14 to +27
IV IV
Prednisone Start tapering by switching MPD to PRED 1mg/kg according to the example that follows.
+28 PO
C. Cyclosporine A Adjustments
1. Do not make adjustments during loading dose unless toxic levels; 2. If creatinine increases 50% above the baseline Day 0 value, apply 50%
dose reduction; 3. When creatinine returns to normal levels; increase CSA by 25%
increments; 4. If CSA levels are over upper-limit, apply a 25% dose reduction or hold
CSA for 24-48 hours and repeat levels next day;
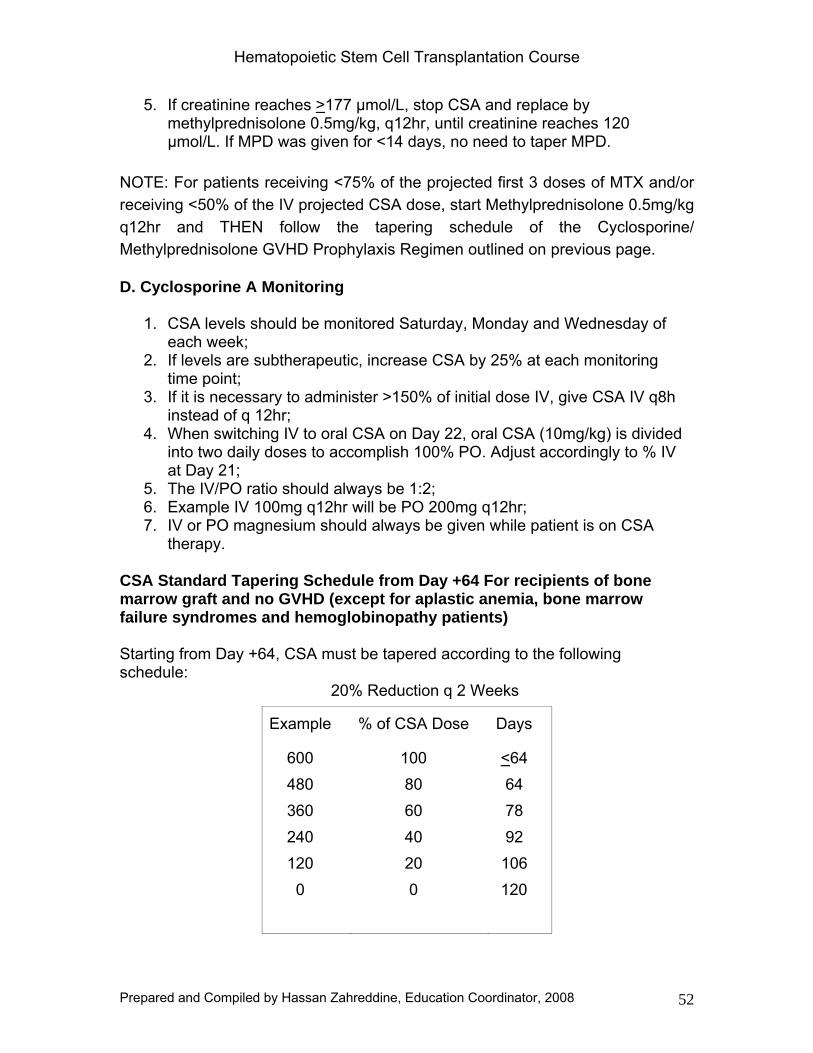
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 52
5. If creatinine reaches >177 μmol/L, stop CSA and replace by methylprednisolone 0.5mg/kg, q12hr, until creatinine reaches 120 μmol/L. If MPD was given for <14 days, no need to taper MPD.
NOTE: For patients receiving <75% of the projected first 3 doses of MTX and/or receiving <50% of the IV projected CSA dose, start Methylprednisolone 0.5mg/kg q12hr and THEN follow the tapering schedule of the Cyclosporine/ Methylprednisolone GVHD Prophylaxis Regimen outlined on previous page.
D. Cyclosporine A Monitoring
1. CSA levels should be monitored Saturday, Monday and Wednesday of each week;
2. If levels are subtherapeutic, increase CSA by 25% at each monitoring time point;
3. If it is necessary to administer >150% of initial dose IV, give CSA IV q8h instead of q 12hr;
4. When switching IV to oral CSA on Day 22, oral CSA (10mg/kg) is divided into two daily doses to accomplish 100% PO. Adjust accordingly to % IV at Day 21;
5. The IV/PO ratio should always be 1:2; 6. Example IV 100mg q12hr will be PO 200mg q12hr; 7. IV or PO magnesium should always be given while patient is on CSA
therapy. CSA Standard Tapering Schedule from Day +64 For recipients of bone marrow graft and no GVHD (except for aplastic anemia, bone marrow failure syndromes and hemoglobinopathy patients) Starting from Day +64, CSA must be tapered according to the following schedule:
20% Reduction q 2 Weeks
Example % of CSA Dose Days
600 480 360 240 120 0
100 80 60 40 20 0
<64 64 78 92
106 120
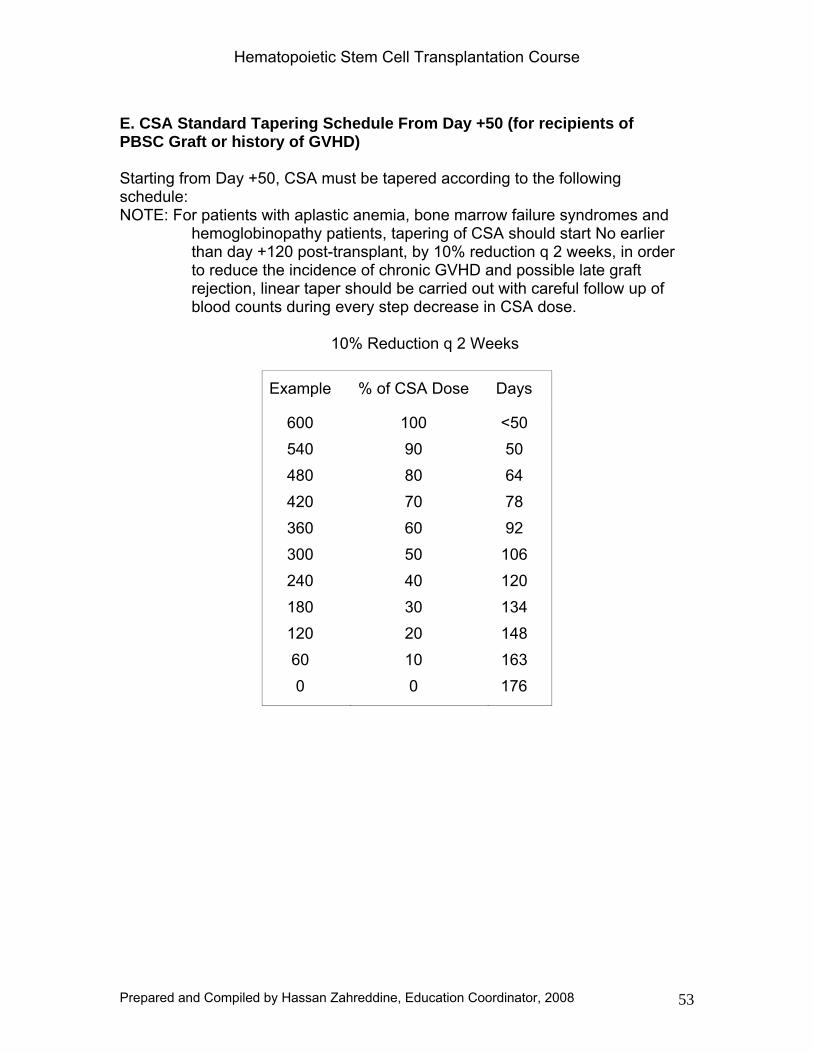
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 53
E. CSA Standard Tapering Schedule From Day +50 (for recipients of PBSC Graft or history of GVHD) Starting from Day +50, CSA must be tapered according to the following schedule: NOTE: For patients with aplastic anemia, bone marrow failure syndromes and
hemoglobinopathy patients, tapering of CSA should start No earlier than day +120 post-transplant, by 10% reduction q 2 weeks, in order to reduce the incidence of chronic GVHD and possible late graft rejection, linear taper should be carried out with careful follow up of blood counts during every step decrease in CSA dose.
10% Reduction q 2 Weeks
Example % of CSA Dose Days
600 540 480 420 360 300 240 180 120 60 0
100 90 80 70 60 50 40 30 20 10 0
<50 50 64 78 92
106 120 134 148 163 176
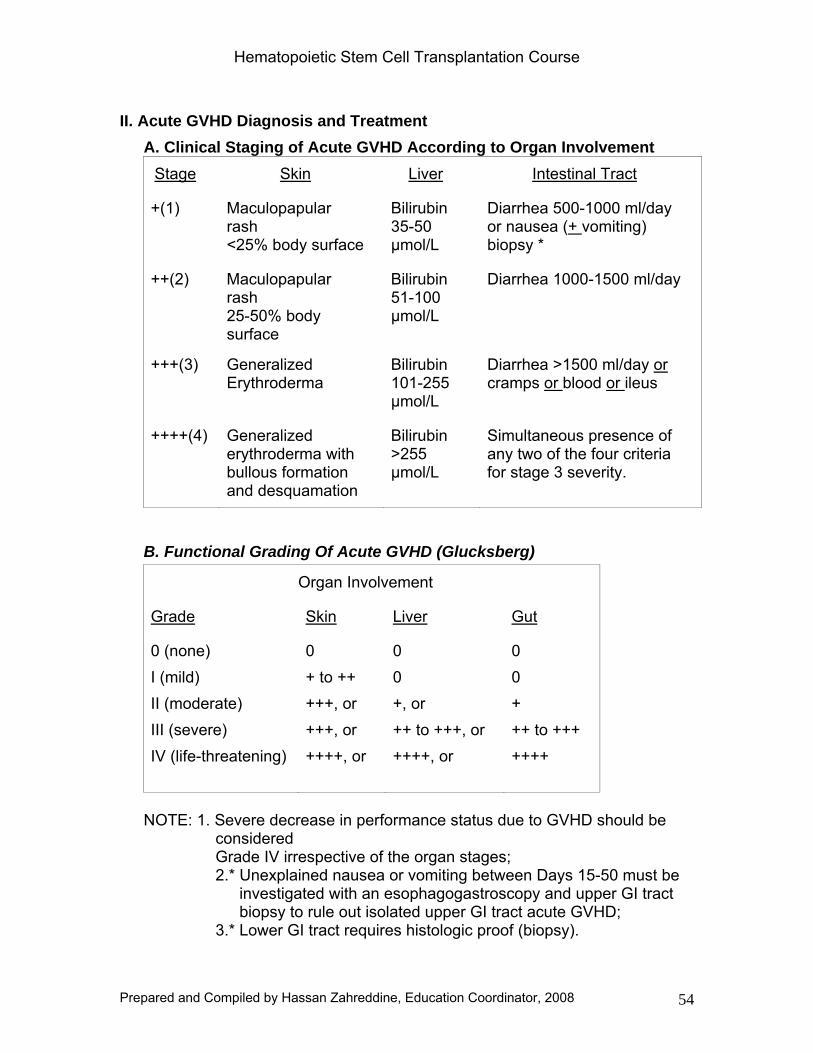
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 54
II. Acute GVHD Diagnosis and Treatment A. Clinical Staging of Acute GVHD According to Organ Involvement
Stage Skin Liver Intestinal Tract
+(1) Maculopapular rash <25% body surface
Bilirubin 35-50 μmol/L
Diarrhea 500-1000 ml/day or nausea (+ vomiting) biopsy *
++(2) Maculopapular rash 25-50% body surface
Bilirubin 51-100 μmol/L
Diarrhea 1000-1500 ml/day
+++(3) Generalized Erythroderma
Bilirubin 101-255 μmol/L
Diarrhea >1500 ml/day or cramps or blood or ileus
++++(4) Generalized erythroderma with bullous formation and desquamation
Bilirubin >255 μmol/L
Simultaneous presence of any two of the four criteria for stage 3 severity.
B. Functional Grading Of Acute GVHD (Glucksberg)
Organ Involvement
Grade Skin Liver Gut
0 (none) I (mild) II (moderate) III (severe) IV (life-threatening)
0 + to ++ +++, or +++, or ++++, or
0 0 +, or ++ to +++, or ++++, or
0 0 + ++ to +++ ++++
NOTE: 1. Severe decrease in performance status due to GVHD should be
considered Grade IV irrespective of the organ stages; 2.* Unexplained nausea or vomiting between Days 15-50 must be
investigated with an esophagogastroscopy and upper GI tract biopsy to rule out isolated upper GI tract acute GVHD;
3.* Lower GI tract requires histologic proof (biopsy).
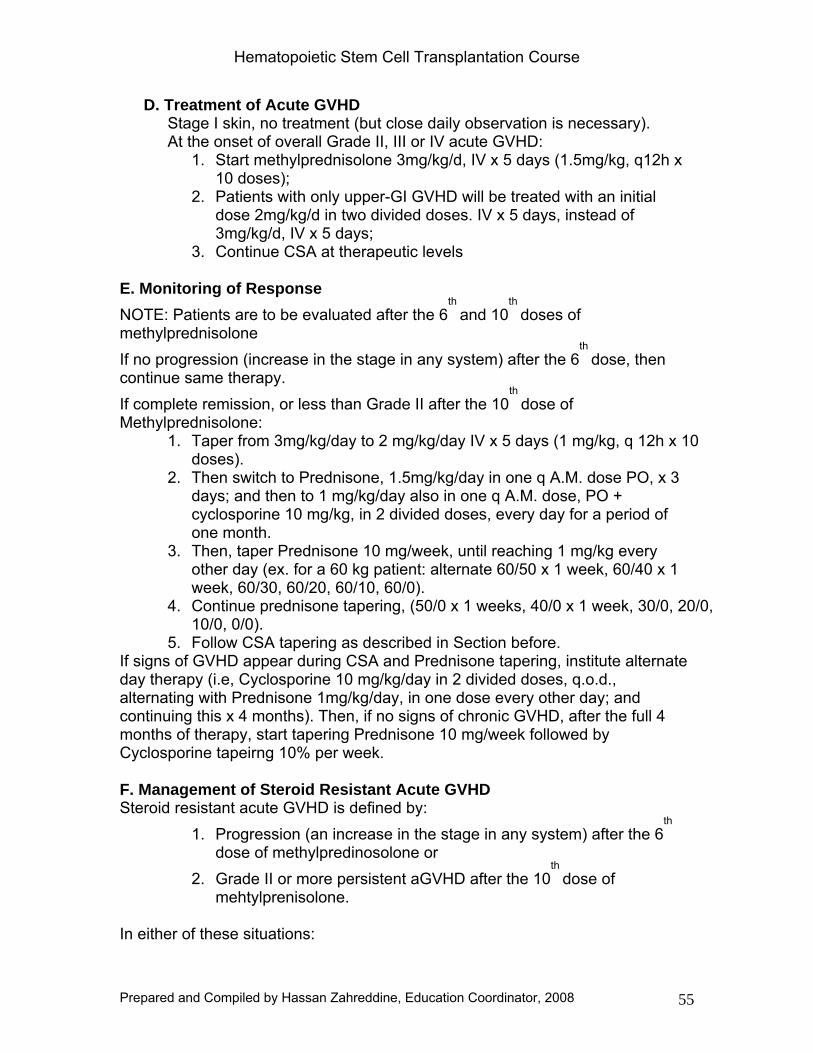
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 55
D. Treatment of Acute GVHD Stage I skin, no treatment (but close daily observation is necessary). At the onset of overall Grade II, III or IV acute GVHD:
1. Start methylprednisolone 3mg/kg/d, IV x 5 days (1.5mg/kg, q12h x 10 doses);
2. Patients with only upper-GI GVHD will be treated with an initial dose 2mg/kg/d in two divided doses. IV x 5 days, instead of 3mg/kg/d, IV x 5 days;
3. Continue CSA at therapeutic levels E. Monitoring of Response NOTE: Patients are to be evaluated after the 6
th and 10
th doses of
methylprednisolone If no progression (increase in the stage in any system) after the 6
th dose, then
continue same therapy. If complete remission, or less than Grade II after the 10
th dose of
Methylprednisolone: 1. Taper from 3mg/kg/day to 2 mg/kg/day IV x 5 days (1 mg/kg, q 12h x 10
doses). 2. Then switch to Prednisone, 1.5mg/kg/day in one q A.M. dose PO, x 3
days; and then to 1 mg/kg/day also in one q A.M. dose, PO + cyclosporine 10 mg/kg, in 2 divided doses, every day for a period of one month.
3. Then, taper Prednisone 10 mg/week, until reaching 1 mg/kg every other day (ex. for a 60 kg patient: alternate 60/50 x 1 week, 60/40 x 1 week, 60/30, 60/20, 60/10, 60/0).
4. Continue prednisone tapering, (50/0 x 1 weeks, 40/0 x 1 week, 30/0, 20/0, 10/0, 0/0).
5. Follow CSA tapering as described in Section before. If signs of GVHD appear during CSA and Prednisone tapering, institute alternate day therapy (i.e, Cyclosporine 10 mg/kg/day in 2 divided doses, q.o.d., alternating with Prednisone 1mg/kg/day, in one dose every other day; and continuing this x 4 months). Then, if no signs of chronic GVHD, after the full 4 months of therapy, start tapering Prednisone 10 mg/week followed by Cyclosporine tapeirng 10% per week. F. Management of Steroid Resistant Acute GVHD Steroid resistant acute GVHD is defined by:
1. Progression (an increase in the stage in any system) after the 6th
dose of methylpredinosolone or 2. Grade II or more persistent aGVHD after the 10
th dose of
mehtylprenisolone.
In either of these situations:
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 56
1. START ATG 20mg/kg for 8 days; 2. When ATG is started, STOP Cyclosporine; 3. Taper Methylprednisolone 0.5mg/kg/day, q5 days until reaching
1mg/kg/day.
NOTE: Patients treated for acute GVHD (aGVHD) with high dose of Methylprednisolone and/or ATG must be monitored for:
1. Bacterial and/or mycotic infection with q.o.d. blood cultures; and 2. CMV infection with weekly blood surveillance (pp65 antigenemia
or PCR or shell vial).
In case of response of ATG (CR or good PR):
1. Start Tacrolimus (FK 506) at 0.12mg/kg/d, in 2 divided doses, one week after cessation of ATG, x 6 months.
2. Maintain Prednisone 1mg/kg/d x 1 month; 3. Taper Prednisone 10mg/week until reacihng 1mg/kg q.o.d. x 6
months; 4. If no signs of chronic GVHD at 6 months, THEN taper Prednisone
10mg/week followed by FK506 tapering 10%/week; 5. Acute GVHD resistant to ATG: treatment to be discussed case-
by-case at BMT Meeting
Chronic GVHD A. Definition
1. Progressive: Chronic graft-versus-host disease following unresolved acute GVHD.
2. Quiescent: Chronic graft-versus-host disease occurring after a complete resolution of acute GVHD.
3. De novo: Chronic graft-versus-host disease appearing in a patient with no previous acute GVHD, usually occurring during or at the end of CSA tapering (around Day 160 to 180 post-transplant).
C. Treatment of Quiescent and de novo GVHD 1. Limited skin chronic graft-versus-host disease should not be treated; but if
indicated, topical steroids only should be used. 2. When limited liver GVHD and/or extensive disease is diagnosed: START prednisone 1 mg/kg/day x 4 weeks: If complete response: 1. Taper 10 mg, q.o.d. per week (ex. for 60kg: 60/50 x 1 week; 60/40 x 1 week; 60/30 x 1 week) until 1 mg/kg, q.o.d. x 3 months; 2. Then taper 10mg, q 2 weeks.
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 57
If no response after one month of prednisone therapy, or relapse during tapering of prednisone: Start cyclosporine 10mg/kg, q.o.d. x 6 months, alternating with Prednisone 1mg/kg, q.o.d. x 6 months. If complete resolution after 6 months: 1. First taper Prednisone 10mg/week; 2. Then Cyclosporine by 10% of initial dose per week. If evidence of resistant chronic GVHD or relapse during tapering, add Mycophenolate Mofitil (MMF) 1000mg PO Bid and consider using FK-506 as a substitute for cyclosporine. NOTE: All patients with chronic GVHD must receive antimicrobial prophylaxis as outlined in the antimicrobial prophylaxis guidelines.
Post Transplantation Outpatient Care
Outpatient Visit Schedule All recently discharged patients are to be seen once a week at the BMT Oupatient Center or more frequently if needed, during the first six weeks after discharge. If stable, patients can then be followed at 2-week intervals for 2 months; and thereafter at 3 - 4 week intervals, depending on their clinical status. Once discharged from the hospital, and until Day 120, patients will be advised to wear a mask at all times except when at home. They will avoid public places and until the Day 120 workup where each patient will be evaluated on a personal basis. Follow Up Routine Laboratory Workup At each visit, the following tests should be done:
CBCD, Renal and Hepatic Panel, Magnesium. Cyclosporine levels, only if < 70 days post-transplant or if the patient is in full dose CSA for treatment of acute GVHD
Shell-vial culture and pp65 antigenemia for CMV monitoring should be done weekly until Day 120 post-transplant (or later if the patient is still on immunosuppressive therapy)
As needed or appropriate, CXR, PFT
Follow Up of Chronic-GVHD Patients with progressive, quiescent and/or de novo chronic GVHD are to
be discussed at the weekly BMT meeting
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 58
Patients with signs of bronchiolitis obliterans should be followed with regular lung function tests, and receive monthly, IV IgG, and pulmonary follow up as necessary
Patients on extended steroid therapy are at high risk for avascular necrosis of bone. Vitamin D and Calcium supplements should be considered in these patients. Female patients should be on hormone replacement
Antimicrobial Prophylaxis Post SCT 1. Allogenic SCT patients No GVHD or Steroids
Bactrim DS tab PO BID every Saturday and Sunday 2. Allogenic SCT patients with history of GVHD or Steroids use
Bactrim DS tab PO BID every Saturday and Sunday Penicillin V 500mg PO QD** Acyclovir 200mg PO BID Monthly IV IgG***
3. Allogenic nonmyeloablative SCT As above + if ANC < 1000 with predicted fall Ciprofloxacin 500mg
PO QD 4. Autologous SCT Bactrim DS tab PO BID every Saturday and Sunday • Prophylaxis continues for 6 months after discontinuation of
immunosuppresive therapy.
Treatment of HZV Infections Nearly half of BMT patients will contract an HZV infection, in the late post-transplant course (after Day +50).
Antiviral IV therapy will be promptly instituted if HZV infection is within the first year after transplant (or longer if on chronic GVHD treatment). Acyclovir will be given intravenously at a dose of 500mg/m
2 per dose given as a 1 hr infusion q
8hr for 7 days. Acyclovir is poorly absorbed after oral administration, and although plasma levels achieved are adequate to treat Herpes simplex, they are not high enough to treat Herpes zoster.
Hematopoietic Stem Cell Transplantation Course
Prepared and Compiled by Hassan Zahreddine, Education Coordinator, 2008 59
Bone Marrow Studies Mandatory for follow up of CML patients; at D+120 bone marrow aspirate for cytogenetics and QPCR should be obtained, if all negative, follow up peripheral blood QPCR should be obtained Q 3 months for the first 3 years, and Q 6 months subsequently, if PCR positive, at anytime bone marrow aspirate cytogenetics should be obtained.
For disease where good molecular markers are available e.g. AML with t(15;17), t(8;21) etc. peripheral blood QPCR should be obtained at D+120, D+180, and Q 6 months subsequently for the first 3 years
For other diseases, bone marrow studies should be obtained as clinically indicated
Engraftment and Chimerism Should be submitted for all patients at D+120, D+180, and at 1 year, studies will be performed on separated T lymphocytes and myeloid cells:
• Test for Short Tandem Repeats (called STRs) will be the standard test for chimerism in sex-match and sex-mismatch transplantations. This test can be routinely obtained through Immunopathology Laboratory.
Specimen requirements:
• Pre-transplant • ACD yellow tubes containing 5-10 ml whole blood: • (Recipient and Donor) • Recommended number of cells: 25 million cells or more • Minimum: 2 million cells • EDTA (purple) tubes are accepted
Note: Routine bone marrow aspirate cytogenetics or Fluorescence In Situ Hybridization (FISH) in bone marrow or peripheral blood can be obtained to evaluate chimerism, in sex-mismatch cases, if STRs are not available. Red blood cell phenotype (only if informative differences, monitor for donor and recipient phenotype).
One Year Work Up For All Patients Immune Reconstitution BMT Leukocyte markers
• Lymphocyte functional assays • Quantitative Ig • Endocrine FSH, LH, TSH • Pulmonary Status Pulmonary Function Test • Autoimmune Status Anti –Nuclear Antibodies (ANAP) • Anti-Smooth Muscle Antibodies (ASMA) • Anti-Thyroid Antibodies (FTA) • Anti-Cardiolipin Antibodies (ACL) • Direct Coombs Test • Rheumatoid Factor (RF)
To be repeated once/year for recipients of radiation containing conditioning
• TSH
• Clinical evaluation for possible development of cataract
For Multiple Myeloma Patients • Serum and urine IFE, QIg Q 3 months for 2 years
• Q 6 months in the subsequent 2 years
• Once a year subsequently
• Skeletal survey Q 6 months in the 1st
4 years then once/year subsequently
For Hodgkin’s and Non-Hodgkin’s Lymphoma Patients • CT Scan or other imaging studies as clinically indicated
Gonadal Dysfunction All women treated with high dose chemotherapy and/or radiotherapy are likely to suffer from ovarian failure or gonadal dysfunction post-transplant and become symptomatic. Approximately 25%, will eventually recover gonadal function approximately 3 years post-transplant.
Combined hormone replacement (Progylton is used at KFSH&RC) should be administered for three years to all women who had normal gonadal function pre-transplant. This therapy can then be stopped to evaluate if ovarian recovery has occurred during this period of time and further therapeutic decisions should be taken depending on the results of the investigation. This therapy will be started at one year if there is no contraindications (e.g. LFT abnormality).
Hematopoietic Stem Cell Transplantation Course
61
Prevention of Potential Osteoporotic Consequences of Chronic Steroids Therapy
• All patients on steroid treatment for more than 6 months as a treatment of GVHD or other indications should be given daily calcium supplement (Caltrate tablet PO QD) and vitamin D (400 IU PO QD).
• If the patient is expected to be on steroids for more than one year, he/she should be placed on Alendronate (Fosamax 10mg PO QD) in addition to calcium and vitamin D as long as they are on steroids.
Return to Work or School Unless there is significant professional or financial hardship, patients should not return to work or school before 6-9 months post-transplant. Home tutors can be arranged, or perhaps the patient can work at home or at the office during off-hours. Moreover, most patients don’t feel capable of a full workload much before 6-9 months post-transplant.
Activities of Daily Living The patient should be encouraged to exercise. Appetite starts to improve as salivary function, smell and taste return after chemoradiotherapy. Anorexia may persist in those patients continuing on cyclosporine. Contact with household pets (but not feces) and gardening are safe. However, contact with barnyard animals, swimming in public or private pools, etc., should be discouraged for the first 9-12 months. Patients should avoid the use of pesticides, solvents, fertilizers, or other myelosuppressive agents. Sexual activity may be resumed.
Immunization Post Allogeneic BMT Months Post-Transplant Vaccines
1. 12 months 1st
dose o IPV; DT* o HB vaccine** o Hepatitis A vaccine o HIB vaccine*** o Pneumovax o Meningococcal vaccine o Influenza vaccine (every Fall)
2. 14 months 2nd
dose o Repeat all the above EXCEPT: o Pneumovax ; meningococcal; Hepatitis A vaccine
Hematopoietic Stem Cell Transplantation Course
62
3. 16 months 3rd
dose o Repeat all the above EXCEPT Pneumovax; meningococcal;
Hepatitis A vaccine 4. 18 months Hepatitis A vaccine 5. 24 months MMR*****
o Meningococcal vaccine (then yearly after that)
Note: 1. Immunizations are not given within first year post transplant due to the
inability to mount adequate antibody response. 2. Patients should avoid persons receiving live virus vaccines up to four
weeks during their first year post transplant. 3. Family member needing polio vaccine should use inactivated vaccine. 4. Patients with chronic GVHD should avoid persons with live virus
vaccinations for four to six weeks. 5. Patients with chronic GVHD or on immunosuppressive therapy should
not receive live vaccines. Live Immunizations MMR Plain Measles Oral Polio Varicella
Lumbar Puncture and IT Therapy Patients on protocols who do not receive TBI: 1 pre and 4 post transplant
doses of IT MTX (or Ara-C) Patients on protocols who receive > 12 Gy of TBI: 1 pre and 2 post
transplant doses of IT MTX (or Ara-C) All pre and post transplant IT MTX should be followed by Leucovorin 15
mg PO starting 6 hours after LP Q 6hrs x 6 doses
1st
post transplant IT therapy will start at +50 and repeated every 3 weeks
IT chemotherapy dose given through Ommaya reservoir should be 2/3rd
the dose given through LP Leucovorin rescue 15mg PO q 6hrs x 6 doses, starting 6 hrs after IT MTX
administration will be given to all patients
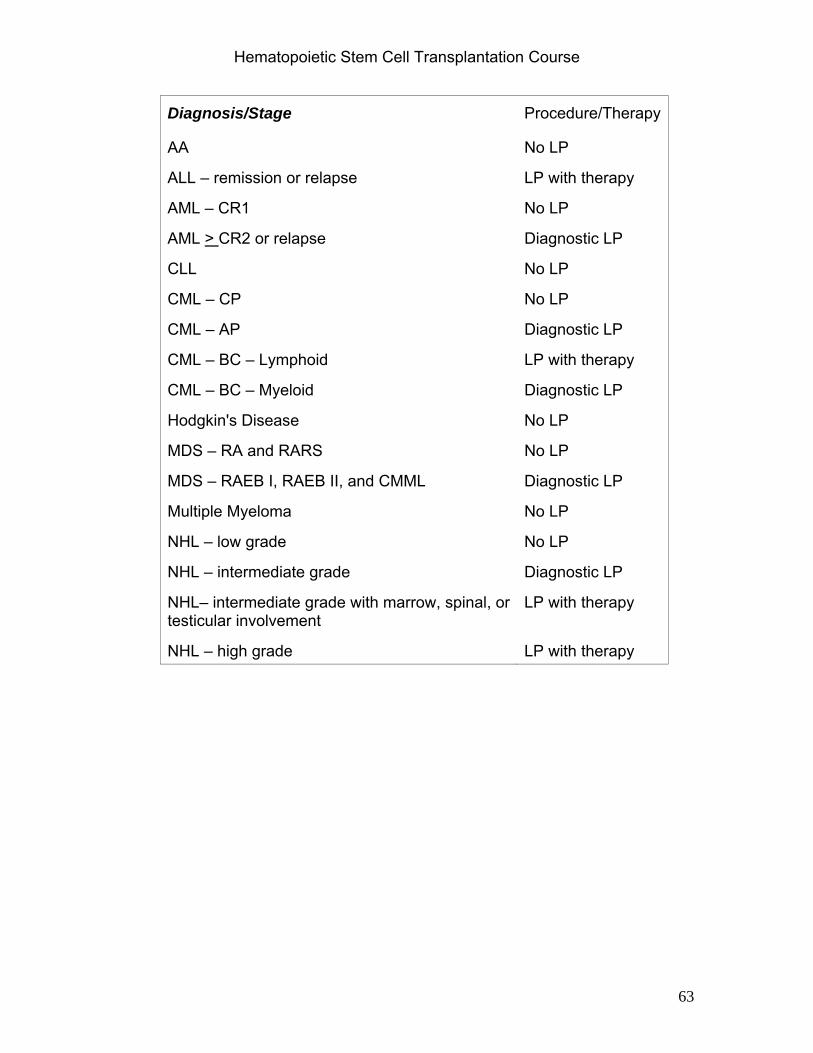
Hematopoietic Stem Cell Transplantation Course
63
Diagnosis/Stage Procedure/Therapy
AA No LP
ALL – remission or relapse LP with therapy
AML – CR1 No LP
AML > CR2 or relapse Diagnostic LP
CLL No LP
CML – CP No LP
CML – AP Diagnostic LP
CML – BC – Lymphoid LP with therapy
CML – BC – Myeloid Diagnostic LP
Hodgkin's Disease No LP
MDS – RA and RARS No LP
MDS – RAEB I, RAEB II, and CMML Diagnostic LP
Multiple Myeloma No LP
NHL – low grade No LP
NHL – intermediate grade Diagnostic LP
NHL– intermediate grade with marrow, spinal, or testicular involvement
LP with therapy
NHL – high grade LP with therapy





























