-
7/30/2019 Hematologic Pathology p24-35
1/12
Eosinophils and basophils are rare in the blood.
LEUKEMIA:AcuteALL and AMLHi/Low WBC (unpredictable)Rapidly fatal
if untreated (matter of weeks); anemic andthrombocytopenic (almost
always. Patient is very sick.)Curable
`
ChronicCLL and CMLAlways high WBCSlowly progressive- patient
lives many yearsDifficult to cure
Above: SLL/CLL, lymph node. Leukemias start in the bonemarrow;
lymphomas start in lymph nodes. Small lymphocyticlymphoma = chronic
lymphocytic leukemia, but they have differentappearances. SLL goes
from the lymph nodes blood, and CLLgoes from the blood lymph
nodes.
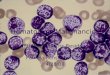
Acute leukemia. This is a40x microscope field. Should
~25 platelets, but see nonehere. This patient will have ahigh
WBC count and a lowplatelet count.
-
7/30/2019 Hematologic Pathology p24-35
2/12
Above: CML. Lots of blasts plus AML: All blasts, no
platelets.different forms of neutrophils.
Auer rod = precipitatedmyeloperoxidase
-
7/30/2019 Hematologic Pathology p24-35
3/12
M3 = treated w/retinoic acid. M4 = myelomonocytic. M5 =
monocytic.
M6 = red cells. M7 = megakaryocytic.
Rouleaux formation: RBCs stack on top of each other. Seen
inmultiple myeloma make amyloid. See halos due to
exaggeratedGolgi.
Lymphomas:
Hodgkin (CD15, CD30) Non-HodgkinRS Cells Low grade- slowly
progressive, rare cureOften curable High grade- rapidly
progressive; a minority are curableStage important Grade
importantFew malignant cells Mostly lymphoma< cell-mediated <
humoralLocalized radiation Systemic chemotherapy
-
7/30/2019 Hematologic Pathology p24-35
4/12
Above: Nodular Sclerosis Hodgkin Lymphoma, lymph node. Above:
Hodgkin Lymphoma. Eosinophils, lymphocytes,Fibrous bands
(sclerosis), nodules. Hodgkins cells.
Above: Hodgkin Lymphoma, spleen. Lymphocytes, Above: Follicular
hyperplasia, lymph node. Mantle zone,Reed-Sternberg cells
(identifies a sample as Hodgkins). light zone, dark zone, tingible
body macrophages (inside
macrophages are retractable bodies). See rim of blue cells.
Above: Follicular hyperplasia, lymph node. Mantle zone, Above:
Malignant follicular lymphoma, lymph node. Seelymphocytes, tingible
body macrophages. follicles.
Follicular lymphoma, lymph node. See follicles. Norim of blue
cells.
-
7/30/2019 Hematologic Pathology p24-35
5/12
Hematology Overview Mon. 10/18/10
Objectives: Overview of hematopoiesis (excluding
detailed discussion of immune system,addressed in previous
lectures)
Review of evaluation of hematologic patient Blood exam Bone
marrow exam Lymph node evaluation Spleen evaluation
Discussion of integrative approach tohematopathology diagnosis
Morphology Flow cytometry Cytogenetics/molecular studies
Components of hematopoietic system:
Hematopoiesis: the formation and developmentof blood cells.
Pictured here Sites are bone marrow, thymus, lymph
nodes,spleen.
Hematopoiesis: Myeloid Development:
Figure: Myeloid DevelopmentGoal: formation of mature
granulocytes andmonocytes for non-specific immune responses.Site:
bone marrow.
Stages are defined by specific markers:CD34, HLA-DR, CD117
immature markers define acute leukemic processes (involving
blasts).CD13, CD33 lineage-specific markers.
DONOT
MEMORIZE
-
7/30/2019 Hematologic Pathology p24-35
6/12
Erythroid development: Megakaryocyte development and platelet
formation:
Goal: formation of RBCs oxygen transport. Goal: formation of
platelets for hemostasisSite: bone marrow Site: bone marrow
B-cell development:
Goal: formation of diverse B-cell population for humoral
immunity.
Site: bone marrow, lymph nodes.
These stages are not as discrete morphologically as monocytic
development. Developmentof immature B cells also occurs in bone
marrow, but all are quite similar morphologically (soit is not
helpful to define stages of maturation).
T-cell development:
DO NOT MEMORIZE!
Goal: formation of diverse T-cellpopulation for cellular
immunity.
Site: bone marrow, thymus.
Only very early T cells actuallyreside in the bone marrow.Can
stain for particular antigensto differentiate stages
ofmaturation.
DO NOT MEMORIZE
-
7/30/2019 Hematologic Pathology p24-35
7/12
Hematopoiesis: mature cells present in blood.
Diagnosis of hematologic disorders:- Morphology plays an
important role in the initial evaluation
- Due to the overlap in morphologic features, certain
hematologic disorders can only be distinguished by thepresence of
specific genetic lesions or the expression of specific proteins-
Treatment is strictly based on the pathologic diagnosis and
increasingly targeted at specific protein/gene
expression (e.g. Imatinib for CML and Ph+ ALL)
Integrated approach to the hematopathology diagnosis:
Integration of morphology withimmunophenotype and genetic
signature:
With the use of cytogenetics, could this be the end of the
morphology era?
In appropriate clinical and laboratory context - Morphology-
Flow cytometry, immunohistochemistry- Cytogenetic and molecular
studies
- Precise, clinically relevant classification- Diagnostic
support in morphologically challenging cases- Follow-up of the
disease
Precursor lymphoid neoplasms (acute lymphoblastic leukemias):- B
lymphoblastic leukaemia/lymphoma, NOS- B lymphoblastic
leukaemia/lymphoma with recurrent genetic abnormalities
- B lymphoblastic leukaemia/lymphoma with t(9:22)(q34;q11.2);
BCR-ABL1- B lymphoblastic leukaemia/lymphoma with t(v;11q23); MLL
rearranged- B lymphoblastic leukaemia/lymphoma with
t(12;21)(p13;q22); TEL-AML1 (ETV6-RUNX1)- B lymphoblastic
leukaemia/lymphoma with hyperidipoloidy- B lymphoblastic
leukaemia/lymphoma with hypodiploidy (Hypodiploid ALL)
- B lymphoblastic leukaemia/lymphoma with t(5;14)(q31;q32);
IL3-IGH- B lymphoblastic leukaemia/lymphoma with
t(1;19)(q23;p13.3); E2A-PBX1 (TCF3-PBX1)
- T lymphoblastic leukaemia/lymphoma
Very few entities are actually defined by morphology alone.
Evaluation of a patient with hematologic condition: Starting
point: complete blood count (CBC) and blood differential Additional
serum studies: iron, B12, folate, Coombs test etc + bone marrow
exam: morphology (biopsy, smear), flow cytometry, cytogenetics,
molecular studies + biopsy of lymph node or extranodal site:
morphology, immunophenotyping, molecular studies
Although there are multiple sites forhematopoiesis (bone marrow,
thymus, lymphnodes, spleen), the end effect is the same all the
different types of cells are in the blood.
-
7/30/2019 Hematologic Pathology p24-35
8/12
Evaluation of a patient with hematologic condition (contd):
Clinical pathologist:
CBC and peripheral blood differential Serum studies (iron, B12,
folate, Coombs test etc)
Hematopathologist bone marrow exam (biopsy, smear, flow
cytometry, cytogenetics, molecular studies) biopsy of lymph node or
extranodal site (including morphology, immunophenotyping, molecular
studies)
Complete Blood Count (CBC): Starting point of hematologic
evaluationPurpose:
- initial evaluation of the status of hematopoietic system-
Quantitative: increase or decrease in specific cell types-
Morphologic changes through review of blood smear- reflects both
production in bone marrow and modification by organs/factors
external to bone marrow (e.g.
sequestration by spleen)
CBC Normal Values: Peripheral blood evaluation:
Peripheral blood smear
Indications for bone marrow examination:Abnormal CBC or blood
smear
- Unexplained cytopenias (low blood counts)- Unexplained
leukocytosis or abnormal WBCs on blood smear- Unexplained
thrombocytosis
Systemic disease- Unexplained lymphadenopathy, splenomegaly,
hepatomegaly- Tumor staging: solid tumors, lymphomas- Monitoring
response to chemotherapy- Fever of unknown origin
Bone marrow examination:- Site: posterior iliac crest, in
special circumstances sternum- Instrumentation: Jamshidi needle-
Local anesthesia- Most commonly both biopsy and aspirate are
obtained (aspirate
only when from sternum)
Purpose of bone marrow examination: Morphology. Assessment
ofcellularity: best performed on the biopsy (%
hematopoietic cells vs. adipose tissue) Cellularity is
usually50%
Test q:A 45F undergoes a bone marrow biopsy due to fever of
unknown origin. Thecellularity of the bone marrow is approximately
50%. This is considered to be: Normal.Test q:A 50M would be
expected to have a bone marrow cellularity of: 50%.
Test q:A 50F undergoes bone marrow biopsy to evaluate a
peripheral pancytopenia. Themarrow shows 50% adipose tissue and 50%
hematopoietic cells. The interpretation is:normal.
-
7/30/2019 Hematologic Pathology p24-35
9/12
Bone marrow aspirate smear: Morphology Evaluation of maturation
and composition of hematopoietic elements.
- Initial evaluation on the biopsy- Detailed evaluation using
bone marrow aspirate smear.
- Evaluation of iron stores: best seen on Prussian blue stain of
bone marrow aspirate smear- Other: detection of infections (bone
marrow can be cultured)
Above: Acute Leukemia.Heterogeneity is somewhat lost.
Purpose of bone marrow examination: Flow cytometry. Evaluation
of maturation Identification of specific cell types Specific
diagnosis Immunophenotypes suggestive of specific genetic lesion
(order additional
molecular studies)
Principle of flow cytometry:Stain cell surface markers different
colors. Use antigens/antibodies.
Figure:Cellularity innormal bone marrow,acute leukemia,
andaplastic anemia.
In acute leukemia,cellularity can increase toabove 90%. In
aplastic
anemia, cellularity can bedown to 10%.
Above: Normal bone marrow. Veryheterogeneous.
-
7/30/2019 Hematologic Pathology p24-35
10/12
Applications of flow cytometry:
Diagnosis and subclassification of leukemias and lymphomas
Detection of minimal residual disease before the overt relapse of
acute leukemia T-cell subset determination for diagnosis and
follow-up in HIV-positive patients Determination of deficient
cell-types in congenital immunodeficiencies Enumeration of
hematopoietic stem cells for bone marrow transplantation Diagnosis
of platelet disorders Detection of fetal hemoglobin in e.g.
feto-maternal hemorrhage
Purpose of bone marrow examination:Cytogenetics and molecular
studies Identification of cytogenetic/genetic abnormality
Cytogenetics conventional karyotype In situ hybridization
Polymerase chain reaction (PCR)
Summary: Purpose of bone marrow exam Morphology:
Assessment of cellularity Evaluation of maturation and
composition of hematopoietic elements Evaluation of iron stores
Other: detection of infections (bone marrow can be cultured)
Flow cytometry Evaluation of maturation Identification of
specific cell types Specific diagnosis Immunophenotypes suggestive
of specific genetic lesion (order additional molecular studies)
Cytogenetics and molecular studies Identification of
cytogenetic/genetic abnormality
Above: Flow cytometry. Inject cells into sheath fluid positions
cells into single file. Sends them in path of laserbeam. Antibodies
attach to fluorochromes tells you aboutpresence of antigens. SSC =
side scattered detector.
Above: Flow cytometry in hematology. Expansion of one cell
typewith same immunophenotype can lead to a specific diagnosis.
-
7/30/2019 Hematologic Pathology p24-35
11/12
Components of lymph node examination: Morphology:
Assessment of overallarchitecture
Evaluation of expected lymphnode compartments
Other: detection of infections(lymph node can be cultured)
Flow cytometry Identification of specific cell types Specific
diagnosis Immunophenotypes suggestive of
specific genetic lesion (orderadditional molecular studies)
Cytogenetics and molecular studies Identification of
cytogenetic/genetic abnormality
Above: Architecture of normal lymph node. (both figures)
Benign lymph node enlargement (lymphadenopathy)
Most common pattern: Follicular Hyperplasia Infections
Autoimmune disorders Non-specific
Benign lymphadenopathy: Paracortical hyperplasia Viral
infections Skin disease Non-specific
Benign lymphadenopathy: Sinus histiocytosis LN draining limbs,
abdominal organs Inflammatory lesions Malignancies
Follicular Hyperplasia.Many follicles scattered Paracortical
Hyperplasia. Expanded area of Sinus histiocytosis.throughout entire
lymph node not just in cortical paracortex area containing T-cells.
Folliclesarea. See many empty spaces within. displaced to the
side.
DZ = dark zone Normal lymph nodes have a very orderly
organization.LZ = light zone Mantle zone is a small layer of
lymphocytes. DarkMZ = mantle zone zone (DZ) mostly centroblasts.
Can see polarization
DZ looks darker than LZ.
Test q:A 25F is evaluated for generalized
lymphadenopathy.Histologic exam reveals follicular hyperplasia. She
most likely
suffers from: bacterial infection.
Test q:A 36y/o rancher lacerated the skin of his upper arm
while
stringing barbed wire. Subsequent infection produced an area
ofsubcutaneous suppuration. He then developed an enlarged,tender
axillary lymph node. Microscopic exam of the lymph node
would most likely reveal histologic features of:
hyperplasia.
-
7/30/2019 Hematologic Pathology p24-35
12/12
SpleenSplenic Architecture
Function: Removal of damaged red cells, bacteria, cell debris
Immune response (follicles, periarteriolar T-cells zones) Temporary
storage of non-circulating blood elements such as
granulocytes, platelets, RBCs Site of hematopoiesis if bone
marrow compromised (ex: malignant
neoplasm)
Spleen can be very valuable source of info in not only myeloid
disorders butalso lymphomas. Spleen has identical
composition/architecture of germinalcenters as in the lymph
node.
Causes of splenomegaly (palpate LUQ!):
Integrative approach to diagnosing patient with hematologic
condition :
Whatever site inspected include: Morphology Immunophenotyping
Cytogenetics/molecular studies
Test q: For the past 6mo, a 35F has experienced an excessively
heavy menstrual flow each month. She also has noticed increasing
numbers ofpinpoint hemorrhages on her lower extremities in the past
month. Phys exam shows no organomegaly or lymphadenopathy. CBC
shows Hgb 14.2g/dL, hematocrit 42.5%, MCV of 91 m
3, platelet count of 19,000/mm
3, and WBC count of 6950/mm
3. On admission to the hospital, she has melena and
is given a transfusion of platelets, but her platelet count does
not increase. An emergency splenectomy is performed, and her
platelet count increases.
Which of the following describes the most likely basis for her
bleeding tendency? Destruction of antibody-coated platelets by the
spleen.
Robbins: This patients bleeding tendency is caused by a low
platelet count. She most likely has idiopathic
thrombocytopenic purpura (ITP) ,in which platelets are destroyed
in the spleen after being coated w/antibodies toplatelet membrane
glycoproteins IIb-IIIa or Ib-IX affecting both the patients
platelets and the transfused platelets.Because the spleen is the
source of the antibody and the site of destruction, splenectomy can
be beneficial.
Directly translates to choice oftreatment (including new
targetedapproaches) and patients prognosis
Test q: Causes of splenomegaly include all
the following except: Sickle cell anemia.(Other choices:
infections, congestive statesrelated to portal hypertension,
Hodgkin
lymphoma, and Non-Hodgkinlymphoma/lymphocytic leukemias)














![Introduction to Mathematica [p24]](https://img.pdfslide.us/doc/110x75/577cc0de1a28aba71191676b/introduction-to-mathematica-p24.jpg)