Embed Size (px)
Citation preview
HEMANGIOPERICYTOMA# P A U L O’BKIEN, M.D., AND RICHARD D. BRASFIELD, M.D.
HE HEMANGIOPERICYTOMA FlKST WAS DE- T scribed in I942 by Stout and Murray as “vascular tumors featured by a prolifera- tion of capillaries; surrounding these were massed spindle shaped or rounded cells some- what in the fashion of the vessels and cells of the glomus tumors, but without the highly organized architecture and encapsulation of that spectacular neoplasm or the remarkable number of nerves and the paroxysmal attacks of pain associated with it.”g They also showed in tissue culture that the spindle shaped or rounded cells come from Zimmerman’s peri- cyte.7 The location of these spindle shaped or rounded cells in relation to the lumen of the associated blood vessels can be demon- strated nicely with silver connective tissue stain. This shows the cells to be extraluminal and avoids confusion with hemangioendo- thelioma, in which the cells are located intra- luminally. The clinical data of this tumor, particularly in the area of long-term follow- up, are sparse.R,IO The anatomical problems presented by this tumor are protean as hemangiopericytoma may occur wherever capillaries are found. (Fig. 1)
This report reviews the experience of Me- morial Hospital with hemangiopericytoma u p to 1959. All of the cases were diagnosed by the Pathology Department at Memorial Hospital. There were 24 cases reviewed, 23 of which had adequate follow up.
AGE AND SEX
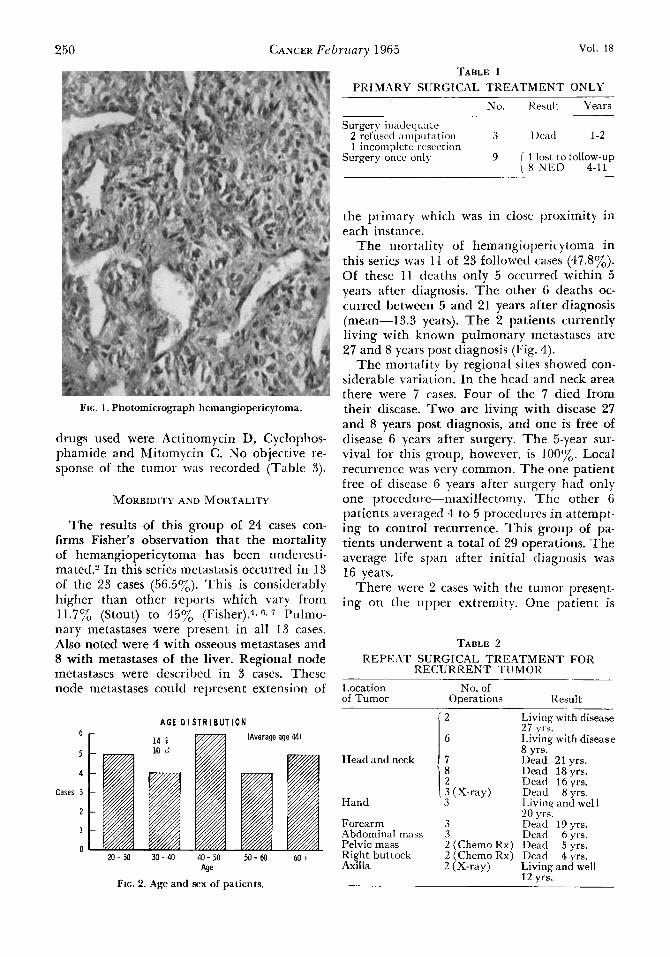
In this group were 14 females and 10 males. T h e preponderance of females is not statis- tically significant. The age at the time of diag- nosis varied from 20 years to 68 years. The tumor appeared most commonly in the fourth decade. Five cases, however, presented in the second decade and 5 cases in the sixth. (Fig. 2). No cases were found in children.4
From the Mixed Tumor Service, Memorial Hospital
+ Presented at the Symposium of the James Ewing
Received for publication July 2, 1964.
and James Ewing Hospital, New York.
Society, 1964.
LOCATION
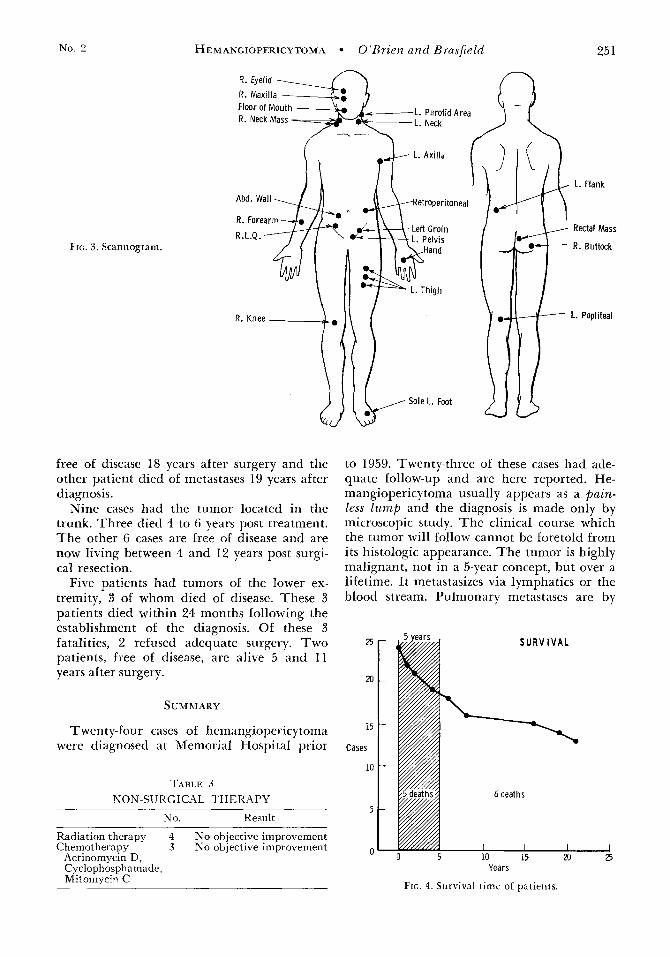
The site of the neoplasm varied greatly, the trunk in our series being the single most common site. There were 7 in the head and neck region, 2 in the upper extremities, 6 in the lower extremities, and 9 located in the trunk, chiefly in the lower-half of the abdo- men. N o thoracic hemangiopericytoma was found in our series, though it has been de- scribed’ (Fig. 3).
SYMPTOMS
In 22 of the 24 cases the presenting com- plaint was a painless mass. In 2 of the cases there were symptoms associated with mechani- cal infringement on adjacent structures. One patient with a lesion of the right buttock com- plained of a painful hip. The other patient with symptoms complained of constipation and passing flat stools. This patient had an hemangiopericytoma adjacent to the rectum. These 2 patients had symptoms for 2 and 3 years prior to definitive surgery. Both patients died of diffuse metastases within 2 years after surgery.
The duration of the painless l ump in the other patients prior to definitive treatment could not be determined accurately.
THERAPY
Of these 24 cases, 23 were treated with sur- gery, biopsy only being performed in one case. In three of the 23 cases adequate surgery was refused by the patient. A lesser surgical pro- cedure was performed. All 3 of these patients died within 2 years after their operation. (Table 1, 2).
Four patients were given X-ray therapy in conjunction with surgery. Two of the 4 are free of disease 4 years and 20 years post re- section. T h e other 2 patients died 8 years and 4 years post diagnosis. N o cases were treated only with X-ray. No marked diminu- tion in size of metastases or successful pallia- tion has been noted with X-ray therapy.3~ 5
T w o patients were treated with chemotherapy for an advanced stage of the disease. T h e
249
250 CANCEK Febrirnry 1965 V O l . 18
TABLE 1 PRIM.4RY SURGICAL TREATMENT ONLY
FIG. 1. Photomicrograph hemangiopericytoma.
drugs used were Actinomycin D, Cyclophos- phamide and Mitomycin C. No objective re- sponse of the tumor was recorded (Table 3).
MORBIDITY AND MOKTALlTY
The results of this group of 24 cases con- firms Fisher's observation that the mortality of hemangiopericytoma has been underesti- mated2 In this series metastasis occurred in 13 of the 23 cases (56.5%). This is considerably higher than other reports which vary from 11.7% (Stout) to 4576 (Fisher).', 6 , Pulmo- nary metastases were present in all 13 cases. Also noted were 4 with osseoiis metastases and 8 with metastases of the liver. Regional node metastases were described in 3 cases. These node metastases could represent extension of
A G E D I S T R I B U T I O N 6
5
4
Cases 3
2
1
0 XI- 30 30- 40 40- 50 50- 60 60 t
Age
FIG. 2. Age and sex of patients.
No. Result Years
Surgery inadequate 2 rcfuscd amputation 3 UWd 1-2 1 incomdete resection
Surgery ohce only 9 j 1 lost to follow-up 1 8 N E D 4-11
the primary which was in close proximity in each instance.
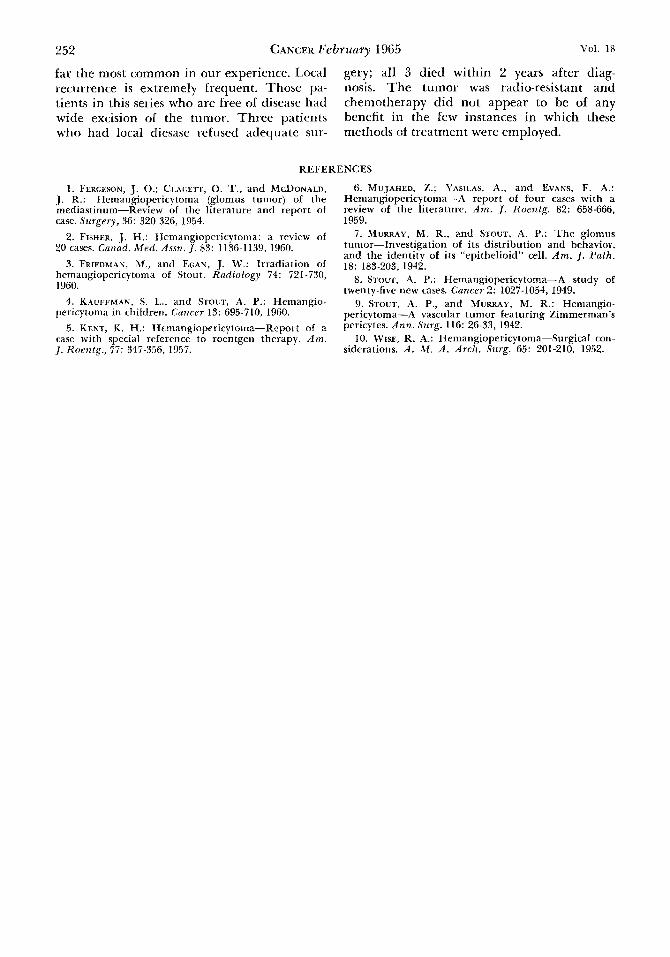
T h e inortali t y of hemangiopericytoma in this series was 11 of 23 followed cases (47.8'%). Of these 11 deaths only 5 occurred within 5 years after diagnosis. Tlic other 6 deaths oc- curred between 5 and 21 years alter diagnosis (mean--13.5 years). T h e 2 patients currently living with known pulmonary metastases are 27 and 8 years post diagnosis (Fig. 4).
T h e mortality by regional sites showed con- siderable variation. In the head and neck area there were 7 cases. Four of the 7 died lrom their disease. Two are living with disease 27 and 8 years post diagnosis, and one is free of disease 6 years after surgery. T h e 5-year sur- vival for this group, however, is 100%. Local recurrence was very common. T h e one patient free of disease 6 years after surgery had only one procedure-maxilleclorny. T h e other 6 paticnts averaged 4 to 5 procedures in attempt- ing to control recurrence. This group of pa- tients underwent a total of 29 operations. 'I'he average life span after initial tliagriosis was 16 years.
There were 2 cases with the tumor present- ing on the upper extremity. One patient is
TABLE 2 REPEAT SURGICAL T R E A T M E N T FOR
RECURRENT TUMOR
Location No. of of Tumor Operations Result
Head and neck
Hand
Forearm Abdominal mass Pelvic mass Right buttock Axilla
2
6
7 8 2 3 (X-ray) 3
3 3 2 (Chemo Rx) 2 (Chemo R x ) 2 (X-ray)
Living with disease 27 yrs. Living with disease 8 yrs. Dead 21 yrs. Dead 18yrs. r k d 16 yrs. Dead 8yrs . Living and well 20 yrs. Dead 19yrs. Dead 6yrs. Dead 5yrs . Dcad 4yrs. Living and well 12 vrs.
No. 2 HEMANGIOPERICYTOMA O’Brien and Brasfield 25 1
FIG. 3. Scannogram.
L. Flank
Rectal Mass
R . Buttock
L. Popliteal
free of disease 18 years after surgery and the other patient died of metastases 19 years after diagnosis.
Nine cases had the tumor located in the trunk. Three died 4 to 6 years post treatment. The other 6 cases are free of disease and are now living between 4 and 12 years post surgi- cal resection.
Five patients had tumors of the lower ex- tremity, 3 of whom died of disease. These 3 patients died within 24 months following the establishment of the diagnosis. Of these 3 fatalities, 2 refused adequate surgery. Two patients, free of disease, are alive 5 and 11 years after surgery.
SUMMARY
Twen ty-four cases of hemangiopericy toma were diagnosed at Memorial Hospital prior
TABLE 3 NON-SIJRGICAL THERAPY
No. Result
Radiation therapy 4 No objective improvement Chemotherapy 3 No objective improvement
Actinomycin D, Cyclophosphamade, Mitoinycin C
to 1959. Twenty-three of these cases had ade- quate follow-up and are here reported. He- mangiopericytoma usually appears as a pain- less lump and the diagnosis is made only by microscopic study. The clinical course which the tumor will follow cannot be foretold from its histologic appearance. The tumor is highly malignant, not in a 5-year concept, but over a lifetime. I t metastasizes via lymphatics or the blood stream. Pulmonary metastases are by
S U R V I V A L
6 deaths
Years
Frc. 4. Survival timc of patients.
252 CANCER Febritury 1965 voi. 18
far the most common in our experience. Local gery; all 3 died within 2 years after diag- recurrence is extremely frequent. Those pa- nosis. The tumor was radio-resistant and tients in this series who are hee of disease had chemotherapy did not appear to be of any wide excision of the tumor. Three patients benefit in the few instances in which these who had local tliesase refused adequate sur- methods of treatment were employed.
REFERENCES
1. FERGESON, J . 0.; CLAGETT, 0. T., and MCDONALD, 1. R.: Hemangiopericytoma (glomus tumor) of the mediastinum-Review of the literature and report of case. Surgery, 36: 320-326, 1954.
2. FISHER, J. H.: Hemangiopericytoma: a review of 20 cases. Canad. M e d . Assri. J. 83: 1136-1139, 1960.
3. FRIEDMAN, M., and EGAN, J. W.: Irradiation of hemangiopericytoma of Stout. Radiology 74: 721-730, 1960.
4. KAUFFMAN, S . I,., and STOUT, A. P.: Hemangio- pericytoma in children. Cancer 13: 695-710, 1960.
5. KENT. K. H.: HemaneioDericvtoma-ReDort of a “ 1 ,
case with special reference to roentgen therapy. A m . J. Rorntg., 77: 347-356, 1957.
6. MUJAHED, Z.; YASILAS, A,, and EVANS, F. A,: Hemangiopcricytoma-A report of four cases with a review of the literaturc. A m . J. Xoentg. 82: 658-666, 1959.
7. MURRAY, M. R., and STOL~T, A. P.: T h e glomus tumor-Investigation of its distribution and behavior, and the identity of its “epithelioid” cell. Am. J. Path.
8. STOUT, A. P.: Hemangiopericytorna-A study of twenty-five new cases. Cancer 2: 1027-1054, 1949.
9. STOUT, A. P., and MURRAY, M. R.: Hemangio- pericytoma-A vascular tumor featuring Zimmerman’s pcricytes. Ann. Surg. 116: 26-33, 1942.
10. WISE, R. A,: Hemangiopericytoma-Surgical con- siderations. A . M . A . Arch. Surg. 65: 201-210, 1952.
18: 183-203, 1942.



![Metastatic Intracranial Hemangiopericytoma to the Spinal ... · 128 INTRODUCTION Intracranial hemangiopericytoma (HPC) is a rare tumor with malignant features [1], of which incidence](https://img.pdfslide.us/doc/110x75/5d4d5a7488c993a90e8bc971/metastatic-intracranial-hemangiopericytoma-to-the-spinal-128-introduction.jpg)

























