Helen Gottfried –UnRuh Senior Manager, Canadian Mental Health Association – Ottawa Deanna Mercer...
43
Treating BPD in Ottawa Helen Gottfried –UnRuh Senior Manager, Canadian Mental Health Association – Ottawa Deanna Mercer MD FRCPC psychiatry Associate Staff, Department of Psychiatry, TOH Assistant Professor, Department of Psychiatry, University of Ottawa
Helen Gottfried –UnRuh Senior Manager, Canadian Mental Health Association – Ottawa Deanna Mercer MD FRCPC psychiatry Associate Staff, Department of Psychiatry,
Helen Gottfried UnRuh Senior Manager, Canadian Mental Health
Association Ottawa Deanna Mercer MD FRCPC psychiatry Associate
Staff, Department of Psychiatry, TOH Assistant Professor,
Department of Psychiatry, University of Ottawa
Slide 2
Slide 3
BPD symptoms A pervasive pattern of instability of
interpersonal relationships, self-image, and affects, and marked
impulsivity beginning by early adulthood and present in a variety
of contexts, as indicated by five (or more) of the following: 1.
frantic efforts to avoid real or imagined abandonment. Note: Do not
include suicidal or self-mutilating behavior covered in Criterion
5. 2. a pattern of unstable and intense interpersonal relationships
characterized by alternating between extremes of idealization and
devaluation. 3. identity disturbance: markedly and persistently
unstable self-image or sense of self. 4. impulsivity in at least
two areas that are potentially self-damaging (e.g., spending, sex,
substance abuse, reckless driving, binge eating). Note: Do not
include suicidal or self-mutilating behavior covered in Criterion
5. 5. recurrent suicidal behavior, gestures, or threats, or
self-mutilating behavior 6. affective instability due to a marked
reactivity of mood (e.g., intense episodic dysphoria, irritability,
or anxiety usually lasting a few hours and only rarely more than a
few days). 7. chronic feelings of emptiness (or boredom) 8.
inappropriate, intense anger or difficulty controlling anger (e.g.,
frequent displays of temper, constant anger, recurrent physical
fights) 9. transient, stress-related paranoid ideation or severe
dissociative symptoms
Slide 4
The pain of being borderline Newly admitted inpatients, 146
BPD, 34 Axis II controls 50 dysphoric feelings BPD > other Axis
II on all 50 dysphoric feelings % of time spent feeling:
Overwhelmed 61.7% Worthless 59.5% Very angry 52.6% Lonely 63.5%
Misunderstood 51.8% Abandoned 44.6% Betrayed 35.9% Rare in non-BPD
patients Evil 23.5% Out of control 33.5% Like a small child 39.1%
Like hurting or killing themselves 44% Zanarini et al 1998
Slide 5
Treatment Histories 2 year study of freshman with (169) and
without (192) BPD features BPD+ : more pharmacologic, psychological
and medical treatment, even after controlling for gender, Axis I,
II pathology Bagge et al 2005 MSAD: 290 BPD, 72 other axis II
consecutive inpatients at McLean hospital patients with BPD 2- 4.5
times more likely to have received each of 12 types of treatment
Zanarini et al 2001, CLPS study : treatment seeking patients 175
BPD, 426 other PD, 97 MDD only BPD > MDD OR 2.14 6.19
individual, group, family, day hospital, inpatient, all classes of
medication BPD > OPD for all treatments except family/couples
and self-help Bender 2001
Influence of BPD on Axis I disorders CLPS BPD + MDD : MDD
remission in 64% Other PD +MDD: MDD remission in 89% Gunderson et
al 2004 MSAD BPD remitted: significant decline in rates of axis I
disorders BPD never remitted: Rates of axis I disorders (mood,
anxiety, SUD, ED) remained stable despite intensive treatment
Zanarini et al 2004
Slide 9
Slide 10
Age as a predictor of symptomatology, co-occuring disorders,
and socioeconomic characteristics in BPD N. Kleindienst, M.
Limberger, J. Barth, M. Bohus Central Institute of Mental Health
Mannheim, Germany
Slide 11
Methods Sample of treatment-seeking BPD-patients (n=367)
University of Freiburg, CIMH (Mannheim) female BPD (DSM-IV) Age: 18
to 65 Census data from the general population comprising all women
from the catchment area (n=2,383,000) data from the general
population were matched by nationality and age Bench mark (e.g.,
marital status)
Slide 12
Distribution of Age (n=367 fem. BPD-Patients) Crucial for -
education - vocational training - employment - starting a
family
Slide 13
Education: Years of Schooling 2 =0.16, df=2 p=0.92 Patients are
on par with respect to schooling (qualifying for univ.
admission)
Slide 14
Completed Vocational Training 2 =7.59, df=2 p=0.02 Differences
were minor similar level with respect to vocational training
Slide 15
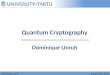
Employment Status Very large differences in employment status
Premature Pension: 7% (Re-)Education / Secon- dary Labor Market 21%
Homemaker: 7% other: 18% Employed Unemployed Other 2 =387.03, df=2,
p
Cochrane 2012 meta 4 outcomes DBT vs TAU Anger- large
Parasuicide, mental health status moderate Single studies estimates
of effect (DBT vs TAU) DBT>TAU BPD core pathology and associated
psychopathology
Slide 31
DBT vs TAU studies: summary 6 DBT (Linehan 1991, 2006, Turner
2000, Koons 2001, Verhuel 2003, Clarkin 2007) 2 DBT-S (Linehan
1999, 2002) With TAU 1-3 : DBTTAU retention 2/5 studies DBT
Slide 32
DBT vs Level 4 treatments Level 4 treatments Well defined
theoretical basis Weekly supervision, support Once or twice weekly
intervention Active therapists Here and now focus DBT=GPM
significant reductions in: suicide attempts*, self harm episodes,
ER visits, psych hospital days, # BPD symptoms, depression, anger,
interpersonal function McMain et al 2009 DBT vs TFP DBT= TFP
significant improvements SI/A, depression, anxiety, GAF, retention
in treatment DBT