Embed Size (px)
Citation preview

HEDIS® Hybrid Measure Abstraction: COAPrepared for: 9th Annual HEDIS® Training WebinarDecember 9, 2019
1HEDIS® is a registered trademark of the National Committee for Quality Assurance (NCQA).
COA

© 2019 Confidential. All rights reserved. 2
Care for Older AdultsCOA
HEDIS® 2020 Tech Specs Changes/UpdatesSection: B. Effectiveness of Care - Preventive Page 120
Changes in this measure from 2019: Added examples of standardized functional status assessment tools in the third
bullet of the numerator of the hybrid specification for the functional status assessment indicator.
Added the Rules for Allowable Adjustments of HEDIS® section.

© 2019 Confidential. All rights reserved. 3
Care for Older AdultsCOA
Measure DescriptionThe percentage of adults 66 years and older who had each of the following during the measurement year (2019):
Advance care planning
Medication review
Functional status assessment
Pain assessment

© 2019 Confidential. All rights reserved. 4
Care for Older AdultsCOA
Medical RecordAdvance care planning is a discussion/plan in place regarding the patient's preferences for resuscitation, life-sustaining treatment, and end-of-life care. Evidence of advance care planning must include one of the following:
The presence of an advance care plan in the medical record on or before December 31st of the measurement year.
Documentation of an advance care planning discussion with the provider and the date when it was discussed. There must be evidence that the discussion occurred during the measurement year.
Notation that the member previously executed an advance care plan. The notation must be dated on or before December 31st of the measurement year.
Evidence of an advance care plan can be captured anytime in the patient’s history as long as there is no evidence that the care plan has been revoked or expired.

© 2019 Confidential. All rights reserved. 5
Care for Older AdultsCOA
Examples of Advance Care Planning
Advance Directive: Directive about treatment preferences and the designation of a surrogate who can make medical decisions for a patient who is unable to make them (e.g., living will, healthcare power of attorney, healthcare proxy).
Actionable Medical Orders: Written instructions regarding initiating, continuing, withholding, or withdrawing specific forms of life-sustaining treatment (e.g., full code, do not resuscitate [DNR], five wishes).
Living Will: Legal document denoting preferences for life-sustaining treatment and end-of-life care.
Surrogate Decision Maker: A written document designating someone other than the member to make medical treatment choices (not just future medical choices).

© 2019 Confidential. All rights reserved. 6
Care for Older AdultsCOA
Additional Notations of Advance Directives
Five Wishes/Open Door
• Combines a living will and healthcare power of attorney
My Directives
Personal Directives
Advanced Decision
Physician Orders for Life-Sustaining Treatment (POLST)
Medical Orders for Life-Sustaining Treatment (MOLST)
Medical Orders for Scope of Treatment (MOST)
Note: May be abstracted from an inpatient settingContinued on next slide.

© 2019 Confidential. All rights reserved. 7
Care for Older AdultsCOA
Additional Notations - Continued
Notation in the medical record of a discussion with a provider or initiation of a discussion by a provider during the measurement year (2019).
• Documentation that a member declined to discuss advance care planning is considered evidence that the provider initiated a discussion and meets criteria.
• Documentation that a provider asked the member if an advance care plan was in place and the member indicated a plan was not in place is not considered a discussion or initiation of a discussion.
Oral statements: Conversations with relatives or friends about life-sustaining treatment and end-of-life care, documented in the medical record. Patient designation of an individual who can make decisions on behalf of the patient. Evidence of oral statements must be noted in the medical record during the measurement year (2019).

© 2019 Confidential. All rights reserved.
Care for Older AdultsCOAAdvance Care Plan
Valid Examples Invalid Examples
Advance care discussion not done in measurement year
Documentation that a provider asked the member if an advance care plan was in place and the member indicated a plan was not in place
Advance care discussion in measurement year
Actionable medical order any time before 12/31/2019
Advance care plan any time before 12/31/2019
Conversations with relatives or friends about life-sustaining treatment and end-of-life care
Documentation that a member declined to discuss advance care planning

© 2019 Confidential. All rights reserved. 9
Care for Older AdultsCOA
Can “full code status” be captured as an advance directive plan?
Yes. Capture as actionable medical orders.

© 2019 Confidential. All rights reserved. 10
Care for Older AdultsCOA
Is there evidence of advance care planning?
Yes. The POLST form can be captured as actionable medical orders.

© 2019 Confidential. All rights reserved. 11
Care for Older AdultsCOA
Is this example valid evidence of an advance directive discussion (assume that the date of the visit is in the measurement year)?
Yes. The example states discussed.
5/5/2019

© 2019 Confidential. All rights reserved. 12
Care for Older AdultsCOA
Does this count as an advance care plan or discussion?
Yes. The provider documented that the patient was counseled on advance directive issues/options in the measurement year.
5/5/2019

© 2019 Confidential. All rights reserved. 13
Step 1: Enter the DOS
Step 2: Select appropriate dropdown from
ACP type.
• Advance care plan
• Actionable medical orders
• Advance care discussion
Care for Older Adults: Tool ImageCOA

© 2019 Confidential. All rights reserved. 14
Care for Older AdultsCOA
Medication ReviewDuring the measurement year (2019), there must be at least one medication review conducted by a prescribing practitioner or clinical pharmacist, and the presence of a medication list in the medical record documentation must come from the same medical record and must include the following:
A medication list in the medical record and evidence of a medication review by a prescribing practitioner or clinical pharmacist and the date when it was performed
A medication list that is signed and dated by the appropriate provider type (prescribing practitioner or clinical pharmacist) meets the criteria for medication review
Note: May not be abstracted from an acute inpatient setting but can abstract from an ED visit
Continued on next slide.

© 2019 Confidential. All rights reserved. 15
Care for Older AdultsCOA
Medication Review - Continued
Notation that the member is not taking any medication and the date when it was noted.
A review of side effects for a single medication at the time of the prescription alone is not sufficient.
An outpatient visit is not required to meet criteria.

© 2019 Confidential. All rights reserved.
Care for Older AdultsCOAMedication Review
Valid Examples Invalid Examples
Medication reconciliation/review evidence without current medication list
Medication review performed by invalid provider type (e.g., RN, MA, LVN, LPN)
Review of medication allergies
Medication reconciliation performed in an acute inpatient setting
Current medication list with evidence of review:
• Changed dosages of medications
• Start/stop medications
Current medication list with signature of valid provider (even if medication review evidence not found additionally)
© 2019 Confidential. All rights reserved. 17
Care for Older AdultsCOA
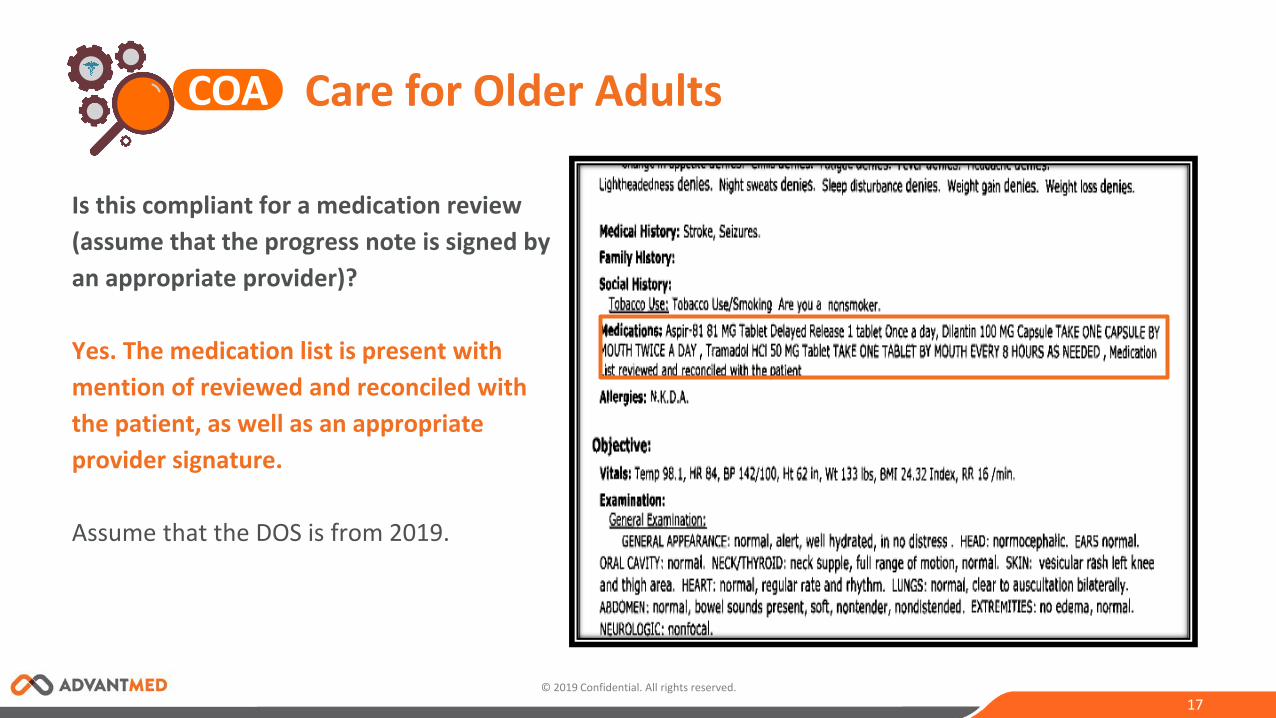
Is this compliant for a medication review (assume that the progress note is signed by an appropriate provider)?
Yes. The medication list is present with mention of reviewed and reconciled with the patient, as well as an appropriate provider signature.
Assume that the DOS is from 2019.

© 2019 Confidential. All rights reserved. 18
Care for Older AdultsCOA
Is this an acceptable example of medication review (assume that the progress note is signed)?
Yes. This would be considered valid as long as the provider that signs the progress note is the appropriate provider type.
6/6/2019

© 2019 Confidential. All rights reserved. 19
Step 1: Enter the DOS.
Step 2: Select appropriate dropdown for medication
reconciliation.
• Medication listed and review
• Not taking any medications
Step 3: Select appropriate provider type dropdown.
• Prescribing practitioner
• Clinical pharmacist
Care for Older Adults: Tool ImageCOA

© 2019 Confidential. All rights reserved. 20
Care for Older AdultsCOA
Functional Status AssessmentNotations for a complete functional status assessment must include one of the following:
Notation that Activities of Daily Living (ADL) were assessed or at least five of the six following ADLs were assessed:
bathing, dressing, eating, transferring, toileting, walking
Notation that Instrumental Activities of Daily Living (IADL) were assessed or at least four of the nine following IADLs were assessed:
shopping for groceries, driving or using public transportation, using the telephone, meal preparation, housework, home repair, laundry, taking medications, handling finances
Continued on next slide.

© 2019 Confidential. All rights reserved. 21
Care for Older AdultsCOA
Functional Status Assessment - Continued
Result of assessment using a standardized functional status assessment tool Page 123 of Tech Specs
Notation that at least three of the following four components were assessed:
cognitive status, ambulation status, sensory ability (includes hearing, vision, and speech), other functional independence (e.g., exercise, ability to perform job)
NOTE: An FSA limited to an acute or single condition, event, or body system does not meet the criteria for a comprehensive functional status assessment.

© 2019 Confidential. All rights reserved. 22
Care for Older AdultsCOA
Functional Status Assessment - ADL Assessment Criteria
Substituting for the other functional independences (assessment of bathing and dressing alone [need five]) is not compliant for the ADL component but can be used as other functional independence if two of the other components (ambulation, cognitive, sensory) are documented in the record.
Statements such as “independent with ADLs” meets the criteria.
Grooming does NOT qualify as an ADL or IADL.
Documentation of urinary "frequency," "retention," or "urgency" does NOT meet the criteria for the "using toilet" ADL.
Documentation of continence does NOT meet criteria.

© 2019 Confidential. All rights reserved. 23
Care for Older AdultsCOA
Functional Status Assessment - IADL Assessment Criteria
If less than four of the above IADLs are specified in the record, they may be used as the “other functional independence” component in three out of four functional status assessment criteria.
Example: Assessment of driving, meal prep, and housework alone are not compliant for the IADL component, but they can be used as other functional independence if two of the other components (ambulation, cognitive, sensory) are documented in the record.
Statements such as “independent with IADLs” meets the criteria.
© 2019 Confidential. All rights reserved. 24
Care for Older AdultsCOA
Standardized Functional Status Assessment ToolExamples of standardized functional status assessment tools include, but are not limited to, the following:
SF-36®
Assessment of Living Skills and Resources (ALSAR)
Barthel ADL Index Physical Self-Maintenance (ADLS) Scale
Bayer Activities of Daily Living (B-ADL) Scale
Barthel Index
Edmonton Frail Scale
Extended Activities of Daily Living (EADL) Scale
Groningen Frailty Index
Continued on next slide.
© 2019 Confidential. All rights reserved. 25
Care for Older AdultsCOA
Standardized Functional Status Assessment Tool - Continued
Independent Living Scale (ILS)
Katz Index of Independence in Activities of Daily Living
Kenny Self-Care Evaluation
Klein-Bell Activities of Daily Living Scale
Kohlman Evaluation of Living Skills (KELS)
Lawton & Brody’s IADL scales
ECOG
Karnofsky
Patient-Reported Outcome Measurement Information System (PROMIS) Global or Physical Function Scales

© 2019 Confidential. All rights reserved. 26
Care for Older AdultsCOA
Functional Status Assessment - Three Out of Four Components
Cognitive Assessment
• Cognitive refers to a person’s ability to process thoughts and primarily refers to things like memory, ability to learn new information, and reading comprehension.
• Statement of “alert and oriented” qualifies for cognitive assessment.
Sensory – Vision, Hearing, Speech
• Documentation MUST include all three of these components to be compliant.
• Notation that the member spoke with the provider during a visit (e.g., documentation that states the member “reports,” “denies,” “stated,” or “discussed”) does NOT meet the criteria for the speech (sensory ability) component. The intent is to find documentation that the provider performed a qualitative assessment of the member’s speech functioning.
Continued on next slide.

© 2019 Confidential. All rights reserved. 27
Care for Older AdultsCOA
Functional Status Assessment - Three Out of Four Components - Continued
Documentation of Speech Component: Documentation of Aphasia
Stuttering and cluttering
Other communication impairment
Speech is normal
Detail speech evaluation may include statements such as:
• Vocabulary
• Sentence production
• Conversation taking turns
• Natural speech and voicing
Continued on next slide.

© 2019 Confidential. All rights reserved. 28
Care for Older AdultsCOA
Functional Status Assessment - Three Out of Four Components - Continued
Sensory: Speech
Components can be captured from multiple visits.
Additional examples of valid evidence of speech evaluation include:
• Documentation of "Pt. denies difficulty speaking," "speech clear," "normal speech, documented in ROS," "negative speech disturbance," and "negative sluggish speaking" meet the criteria for the speech component.
• If the provider notes Cranial Nerve 12 (for Speech) in the physical exam, it is valid for the speech evaluation as long as there is documentation of an assessment with a result or finding.
Continued on next slide.

© 2019 Confidential. All rights reserved. 29
Care for Older AdultsCOA
Functional Status Assessment - Three Out of Four Components - ContinuedThe example below is NOT acceptable for speech evaluation.
Patient complaining is not acceptable for speech evaluation.
See page 124 of HEDIS® 2020 Tech Specs: The intent is to find documentation that the provider performed a qualitative assessment of the member’s speech functioning.
Continued on next slide.
ROS: Patient is complaining of swelling of the right knee.
Patient is complaining of right knee pain.

© 2019 Confidential. All rights reserved. 30
Care for Older AdultsCOA
Functional Status Assessment - Three Out of Four Components - Continued
Sensory: Vision and Hearing
Valid evidence of vision evaluation includes, but is not limited to:
• Blurred vision, no vision changes, vision normal, wears glasses, no issues with vision, result of vision 20/60 at the last eye exam.
• If the provider notes Cranial Nerve 2 (for vision) in the physical exam, it is valid for the vision evaluation as long as there is documentation of an assessment with a result or finding.
Valid evidence of hearing evaluation includes, but is not limited to :
• Wearing hearing aids, hearing loss, hearing normal, hearing impaired.
• If the provider notes Cranial Nerve 8 (for hearing) in the physical exam, it is valid for the hearing evaluation as long as there is documentation of an assessment with a result or finding.
Continued on next slide.

© 2019 Confidential. All rights reserved. 31
Care for Older AdultsCOA
Functional Status Assessment - Three Out of Four Components - Continued
Cranial Nerves II-XII assessed is not the same as intact.
Cranial Nerves II- XII were assessed meets criteria if the result or finding is also documented, because it is clear that cranial nerves II, VIII, and XII were assessed and the result/finding is present. Documentation of "Cranial Nerves II-XII assessed" alone does not meet criteria, because the result/finding is missing.
Continued on next slide.

© 2019 Confidential. All rights reserved. 32
Care for Older AdultsCOA
Functional Status Assessment - Three Out of Four Components - Continued
Ambulation
Look for the patient’s ability to ambulate, such as walk, run, jog, or walk the dog.
A notation of “falls” alone is not sufficient for ambulation.
Skilled nursing facilities may have ambulation documented on a Braden Scale.
NOTE: Provider recommendations for walking or other exercise does NOT meet this component.
Continued on next slide.

© 2019 Confidential. All rights reserved. 33
Care for Older AdultsCOA
Functional Status Assessment - Three Out of Four Components - Continued
Other Functional Independence
This includes the ability to exercise, perform a job, etc.
• Inability to work statements also count (e.g., disabled)
• Documentation of exercise tolerance, exercise regularity, and/or continue proper diet and exercise (under plan section)
• Documentation of living with another person or living independently
Remember: Documentation of less than five of the previously specified ADLs or less than four of the previously specified IADLs can be used for this component.
Components may be captured from multiple visits.

© 2019 Confidential. All rights reserved. 34
Care for Older AdultsCOA
FSA from Multiple Records NCQA PCS clarification #198949 8/7/2018 that the FSA components may be captured from multiple records as well as multiple dates of service. This has led to the NCQA PCS clarification #198949 8/7/2018 that the FSA components may be captured from multiple records as well as multiple dates of service. This has led to the update in Advantmed’s abstraction tool to collect any FSA component finding regardless of if it fully meets the measure. The data will then be exported to the client’s HEDIS® reporting tool to determine compliance.
Example:
Record A may only have ambulation and dressing.
Record B may have cognitive, vision, hearing, and speech.
Alone neither are compliant, but in the individual chases, the reviewer will abstract the information, allowing the software systems to determine.

© 2019 Confidential. All rights reserved. 35
Care for Older AdultsCOA
Functional Status Assessment Helpful Hints:
A functional status assessment limited to an acute or single condition, event, or body system (e.g., lower back, leg) does not meet the criteria for a comprehensive functional status assessment.
The components of the functional status assessment numerator may take place during separate visits within 2019.
NOTE: Functional status assessment may NOT be abstracted from an acute inpatient setting, but you can abstract from ED visits.
Reminder: Add page numbers for all components found in the same DOS or different DOS in the text box provided in the tool.

© 2019 Confidential. All rights reserved.
Care for Older AdultsCOAFSA
Valid Examples Invalid Examples
Functional status assessment performed related to any condition
Cranial nerves assessment alone without result
Patient reports/denies/states does not meet the criteria for speech in sensory component
Functional status assessment performed in an inpatient setting
Patient denies ringing in ears does not qualify for hearing in sensory component
Standard function assessment tool
Memory-related evidence as cognitive component
Cranial nerves II to XII assessment with result is valid for sensory system components
Depression screening is valid for cognitive component
Alert, oriented for cognitive component

© 2019 Confidential. All rights reserved. 37
Care for Older AdultsCOA
Activity IndependentMin
assistMax assist Dependent
Bathing xDressing xCooking xFeed Self xAmbulation xToileting xClean Home xDriving xPay Bills xUses Phone xMedication Administration xPublic Transportation x
What ADLs are listed in this table?
Bathing Dressing Eating Ambulation Toileting
John Doe DOS: 6/1/19

© 2019 Confidential. All rights reserved. 38
Care for Older AdultsCOA
Would all three highlighted examples combine to a valid evidence of three out of four components?
No. Urinary frequency and continence are not valid.
Assume that screenshots are from 2019 chart note.

© 2019 Confidential. All rights reserved. 39
Care for Older AdultsCOA
These example show evidence of three out of four components from different progress notes.
Assume that screenshots are from 2019 chart note.

© 2019 Confidential. All rights reserved. 40
Care for Older AdultsCOA
Which dropdown would be selected for FSA in this example?
ADLs
7/22/2019
7/22/2019
7/22/2019

© 2019 Confidential. All rights reserved. 41
Care for Older AdultsCOA
Which components are present in this example?
CognitiveAmbulatorySensory
7/22/2019
7/22/2019

© 2019 Confidential. All rights reserved. 42
Care for Older AdultsCOA
Which dropdown would be selected for FSA in this example?
ADLs:Eating, Bathing, Dressing, Toileting, Transfers
7/22/2019

© 2019 Confidential. All rights reserved. 43
Care for Older AdultsCOA
Can we abstract functional assessment from this example?
Yes. See note for “can do ADLs.”
7/22/2019
9/28/2019
9/12/2019
© 2019 Confidential. All rights reserved. 44
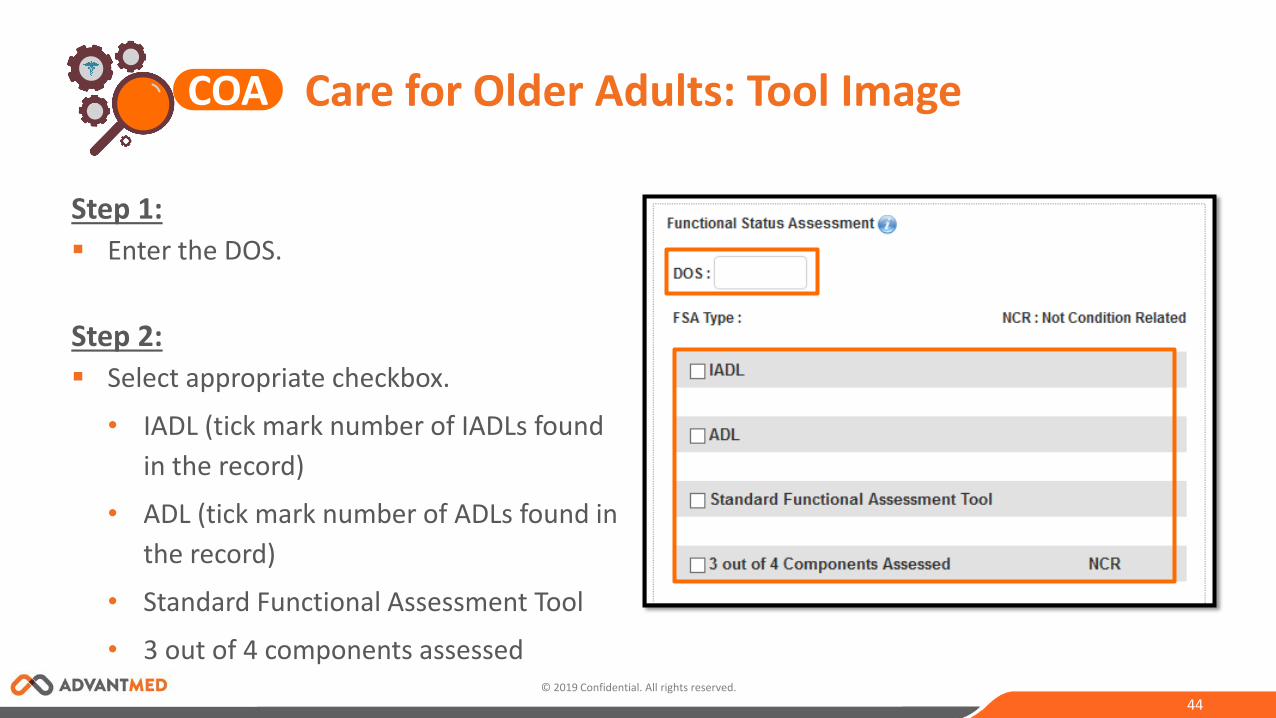
Step 1: Enter the DOS.
Step 2: Select appropriate checkbox.
• IADL (tick mark number of IADLs found in the record)
• ADL (tick mark number of ADLs found in the record)
• Standard Functional Assessment Tool
• 3 out of 4 components assessed
Care for Older Adults: Tool ImageCOA
© 2019 Confidential. All rights reserved. 45
Care for Older AdultsCOA
Pain AssessmentThere must be at least one pain assessment during the measurement year (2019). Documentation in the medical record must include evidence of a pain assessment and the date when it was performed. Notations for a pain assessment must include one of the following:
Documentation that the patient was assessed for pain (which may include positive or negative findings for pain)
Result of assessment using a standardized pain assessment tool (listed on next slide)
CANNOT be abstracted from an acute inpatient setting
Continued on next slide.
Visual Analogue Scale Brief Pain Inventory Chronic Pain Grade PROMIS Pain Intensity Scale Pain Assessment in Advanced Dementia
(PAINAD) Scale
Continued on next slide.
© 2019 Confidential. All rights reserved. 46
Care for Older AdultsCOA
Pain AssessmentExamples of pain assessment tools include, but are not limited to:
Numeric Rating Scales (verbal or written)
Face, Legs, Activity, Cry Consolability (FLACC)scale
Verbal Descriptor Scales (5–7 Word Scales,Present Pain Inventory)
Pain Thermometer
Pictorial Pain Scales (Faces Pain Scale, Wong-Baker Pain Scale)

© 2019 Confidential. All rights reserved. 47
Care for Older AdultsCOA
Pain Assessment
NOTE:
Documentation of sore throat is acceptable for pain assessment.
Documentation of pain assessment includes notations of positive or negative (absence of) findings for pain and counts towards pain assessment. Only one body system is required.
Notation of screening for chest pain alone or documentation of chest pain alone does NOT meet criteria.
Do NOT include pain assessments performed in an acute inpatient setting, but you can abstract from ED visits.
Notation of a pain management plan alone does NOT meet criteria.
Notation of a pain treatment plan alone does NOT meet criteria.
Continued on next slide.

© 2019 Confidential. All rights reserved.
Care for Older AdultsCOAPain Assessment
Valid Examples Invalid Examples
Chest pain alone
Pain management/treatment alone
Pain assessment performed in an acute inpatient setting
Pain scale
Pain assessment performed during the physical exam
Pain assessment performed in during the review of system
Condition-related pain assessment is also valid
© 2019 Confidential. All rights reserved. 49
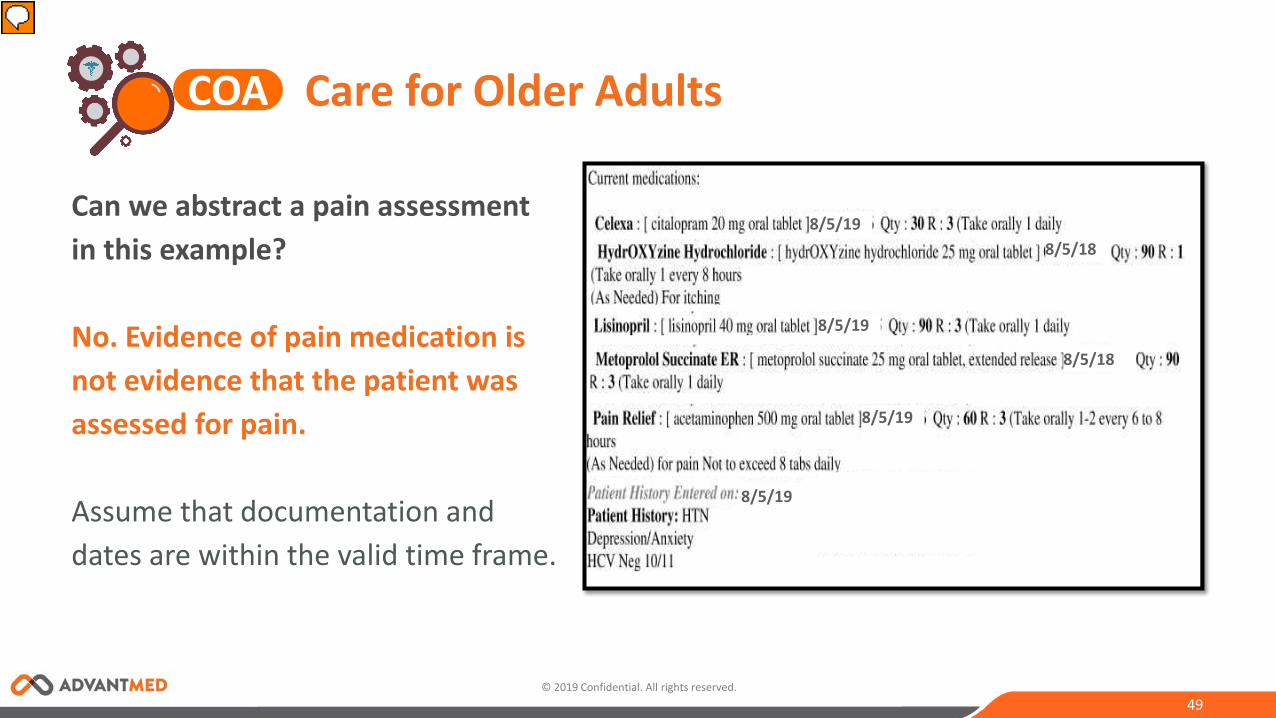
Can we abstract a pain assessment in this example?
No. Evidence of pain medication is not evidence that the patient was assessed for pain.
Assume that documentation and dates are within the valid time frame.
8/5/18
8/5/19
8/5/18
8/5/19
8/5/19
8/5/19
Care for Older AdultsCOA

© 2019 Confidential. All rights reserved. 50
Can we abstract a pain assessment in this example?
Yes. This is acceptable.
Assume that the screenshot is from 2019 chart note.
Care for Older AdultsCOA
© 2019 Confidential. All rights reserved. 51
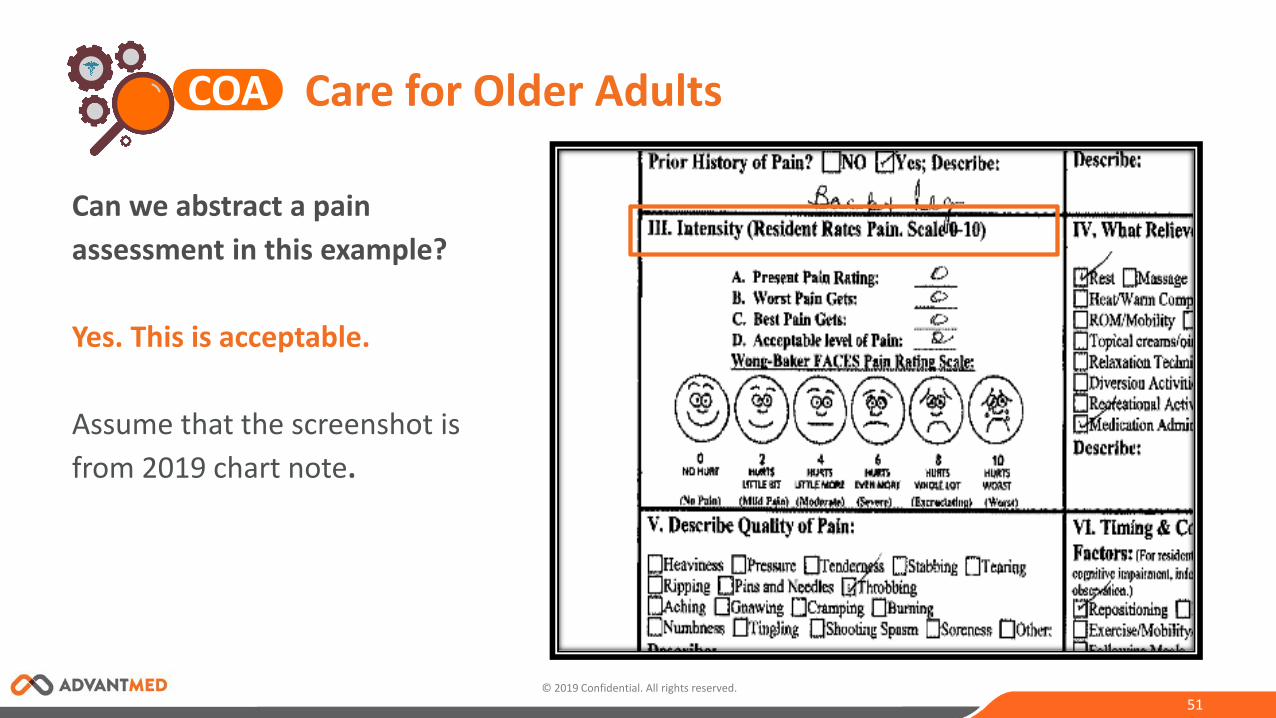
Can we abstract a pain assessment in this example?
Yes. This is acceptable.
Assume that the screenshot is from 2019 chart note.
Care for Older AdultsCOA
© 2019 Confidential. All rights reserved. 52
Helpful Hints
Documentation that a member declined to discuss advance care planning is considered evidence that the provider initiated a discussion and meets criteria.
Documentation that a provider asked the member if an advance care plan was in place and the member indicated a plan was not in place is NOT considered a discussion or initiation of a discussion.
A medication list signed and dated during the measurement year by the appropriate practitioner type (prescribing practitioner or clinical pharmacist) meets the criteria (the practitioner’s signature is considered evidence that the medications were reviewed).
A review of side effects for a single medication at the time of prescription alone is NOT sufficient.
Pain Management: Do not include pain management or treatment plan alone.
Care for Older AdultsCOA

© 2019 Confidential. All rights reserved. 53
Step 1: Enter the DOS.
Step 2: Select appropriate dropdown
pain assessment type.
• Assessed for pain
• Standardized pain assessment tool or scale
Care for Older Adults: Tool ImageCOA
© 2019 Confidential. All rights reserved. 54
Secondary Pursuit Notes:
Alternate Provider Identified
Any Admission Identified
Other
Care for Older AdultsCOA

© 2019 Confidential. All rights reserved. 55
Test Your Knowledge - FSA
NCQA #212647 (2018)
Question: Is “eating and sleeping okay” evidence of the eating ADL?
Care for Older AdultsCOA

© 2019 Confidential. All rights reserved. 56
Test Your Knowledge - FSA
NCQA #212647 (2018)
Answer: Yes. Documentation of “eating and sleeping okay" counts as evidence of the “eating" ADL. Please keep in mind that to meet the criteria in bullet 1 (in the Medical Record section on page 103 of HEDIS® 2019) the medical record must indicate that at least five ADL components were assessed in order to be compliant.
Care for Older AdultsCOA

© 2019 Confidential. All rights reserved. 57
Test Your Knowledge - FSA
NCQA #212648 (2018)
Question: Does documentation of “agitated" qualify for a cognitive evaluation for three out of four components for the functional status assessment?
Care for Older AdultsCOA

© 2019 Confidential. All rights reserved. 58
Test Your Knowledge - FSA
NCQA #212648 (2018)
Answer: No. Documentation of "agitated" alone would not count towards the cognitive component. This documentation alone is not considered evidence that a cognitive assessment took place.
Care for Older AdultsCOA
© 2019 Confidential. All rights reserved. 59
Test Your Knowledge - HEDIS® 2020 Tech Specs
Question: Can a medication review, functional status assessment, or pain assessment be abstracted from an acute inpatient record?
Care for Older AdultsCOA

© 2019 Confidential. All rights reserved. 60
Test Your Knowledge - HEDIS® 2020 Tech Specs
Answer: No (Tech Specs clarification).
Update: The medication review, functional status assessment, and pain assessment numerators exclude services provided in an acute inpatient setting (pages 123 and 124).
Care for Older AdultsCOA

© 2019 Confidential. All rights reserved. 61
Test Your Knowledge - Advanced Care Plan
NCQA PCS #211805 (2018)
Question: Can an advanced care plan be abstracted from an acute inpatient record? As per HEDIS® 2019 Specs, medication review, functional status assessment, and pain assessment numerators should exclude service provided in an acute inpatient setting. Is it applicable to an advance care plan as well?
Care for Older AdultsCOA
© 2019 Confidential. All rights reserved. 62
Test Your Knowledge - Advanced Care Plan
NCQA PCS #211805 (2018)
Answer: An advanced care plan abstracted from an acute inpatient record meets the numerator criteria for the advanced care planning numerator. Please note, the intent to exclude functional status assessments, pain assessments, and medication reviews provided in an acute inpatient setting are because these often rapidly change during an acute inpatient stay.
Care for Older AdultsCOA

© 2019 Confidential. All rights reserved. 63
Test Your Knowledge - Three Out of Four Components
PCS Case #00211810 (2018)
Question: If the documentation states "c/o tinnitus," does this evidence qualify as evidence of hearing for sensory in the three out of four components?
Care for Older AdultsCOA

© 2019 Confidential. All rights reserved. 64
Test Your Knowledge - Three Out of Four Components
PCS Case #00211810 (2018)
Answer: Yes. Documentation of "c/o tinnitus" is sufficient to meet the hearing component of the COA measure. Please note, documentation must contain evidence that all three sensory components (hearing, vision, and speech) were assessed to meet the criteria for the sensory component.
Care for Older AdultsCOA

© 2019 Confidential. All rights reserved. 65
Test Your Knowledge - Advanced Care Plan
PCS Case #00211062 (2018)
Question: For the advanced care plan sub-measure, if there is documentation in a progress note stating "Advanced Directive-reviewed 11.06.2018-None," is this acceptable to abstract as an advanced care plan discussion when the progress note is dated 11.06.2018?
Care for Older AdultsCOA
© 2019 Confidential. All rights reserved. 66
Test Your Knowledge - Advanced Care Plan
PCS Case #00211062 (2018)
Answer: Documentation of "Advanced Directive-reviewed 11.06.2018-None" does not meet the criteria for the advanced care planning numerator because there is no evidence of an advanced care plan in place or a discussion with a provider. For advanced care planning, a member is compliant if there is an advanced care plan in place or if there is evidence of a discussion with a provider about advanced care planning. Documentation that a provider initiated a discussion about advanced care planning (medical advanced directive was offered) but the patient did not want to move forward with putting an advanced care plan in place (refused) is considered evidence that a discussion occurred.
Care for Older AdultsCOA

Questions?
67

68
Thank you.





























