Embed Size (px)
Citation preview
Heartbeat – May 2002
Triumph of the trials
Triumph of the trials: ACC 2002
Valentin Fuster MDDirector, Cardiovascular InstituteMount Sinai Medical CenterNew York, New York
Christopher Cannon MDCardiologistBrigham and Women's HospitalBoston, Massachusetts
Christopher M O'Connor MDAssociate Professor of CardiologyDuke University Medical CenterDurham, NC
Michael Weber MDProfessor of MedicineSUNY Downstate College of MedicineBrooklyn, New York
Heartbeat – May 2002
Triumph of the trials
DANAMI-2Transferring patients for PCI
LIFELosartan for hypertension
WIZARDAntibiotics for coronary
disease
Subjects
Heartbeat – May 2002
Triumph of the trials
DANAMI-2
DANish multicenter Trial in Acute Myocardial Infarction 2
1572 patients randomized to fibrinolysis (100 mg front loaded tPA)or PCI + stent
Referral hospitals: tPA or ambulance transfer to center for PCI
PCI centers: tPA or PCI
Primary endpoint: Death, reinfarction, or disabling stroke in 30 days
Heartbeat – May 2002
Triumph of the trials
ST-elevation 4 mm
Symptoms 12 hrs at randomization
Transfer 3 hrs from referral hospital to cath-lab
Maximum transport distance 95 miles
Mean transport distance 35 miles
DANAMI-2: Inclusion criteria
Heartbeat – May 2002
Triumph of the trials
DANAMI-2: New PCI centers
"In fact, one of the most interesting aspects of this study was that the Danish institutions didn't have PCI a few years ago, so they had to be trained."
5 PCI centers24 referral hospitals(62% of Danish population)
Fuster
Heartbeat – May 2002
Triumph of the trials
DANAMI-2: Strategies of care
O'Connor
"I think this is an extremely important trial because it not only addresses an important scientific question but it also looks at strategies of care."
Heartbeat – May 2002
Triumph of the trials
"They raised the bar in doing this study [in that] they geared up a system to try and extend the reach of primary angioplasty so that it would be possible to offer this for people as far away as 30 or 50 miles."
Cannon
DANAMI-2: Raising the bar
Heartbeat – May 2002
Triumph of the trials
"What people forget is that even here in the United States we don't all have an interventional lab next door or around the corner. In California you might find an interventional lab in every cardiologist's backyard or garage but here in New York we don't have that at all."
Weber
DANAMI-2: Important to US
Heartbeat – May 2002
Triumph of the trials
ACC 2002
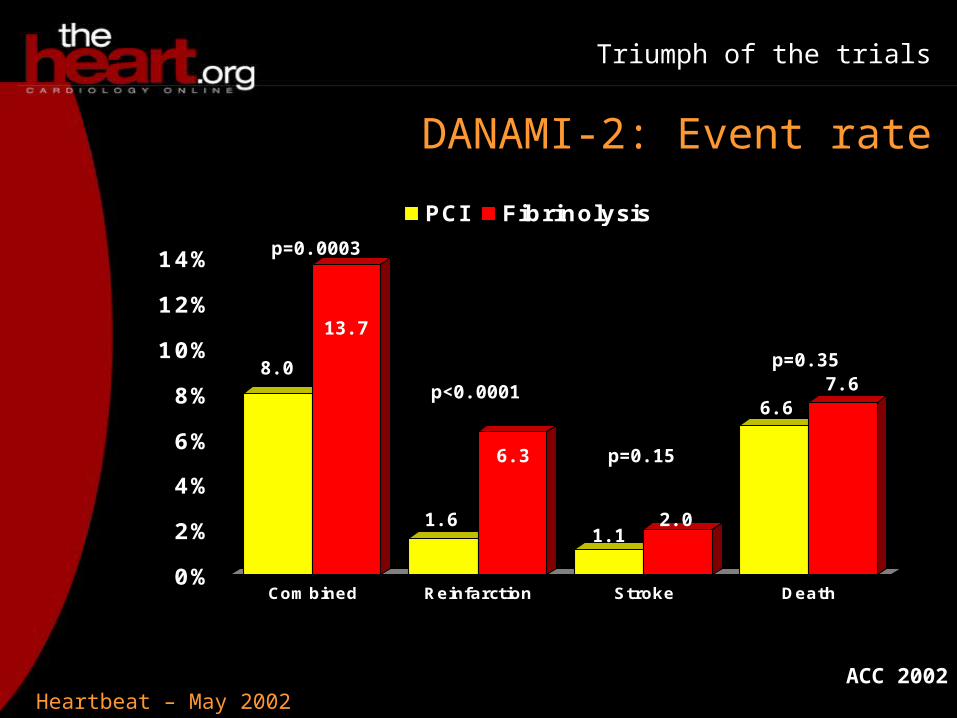
DANAMI-2: Event rate
0%
2%
4%
6%
8%
10%
12%
14%
Combined Reinfarction Stroke Death
PCI Fibrinolysis
p=0.0003
p<0.0001
p=0.15
p=0.358.0
13.7
1.6
6.3
1.12.0
6.67.6
Heartbeat – May 2002
Triumph of the trials
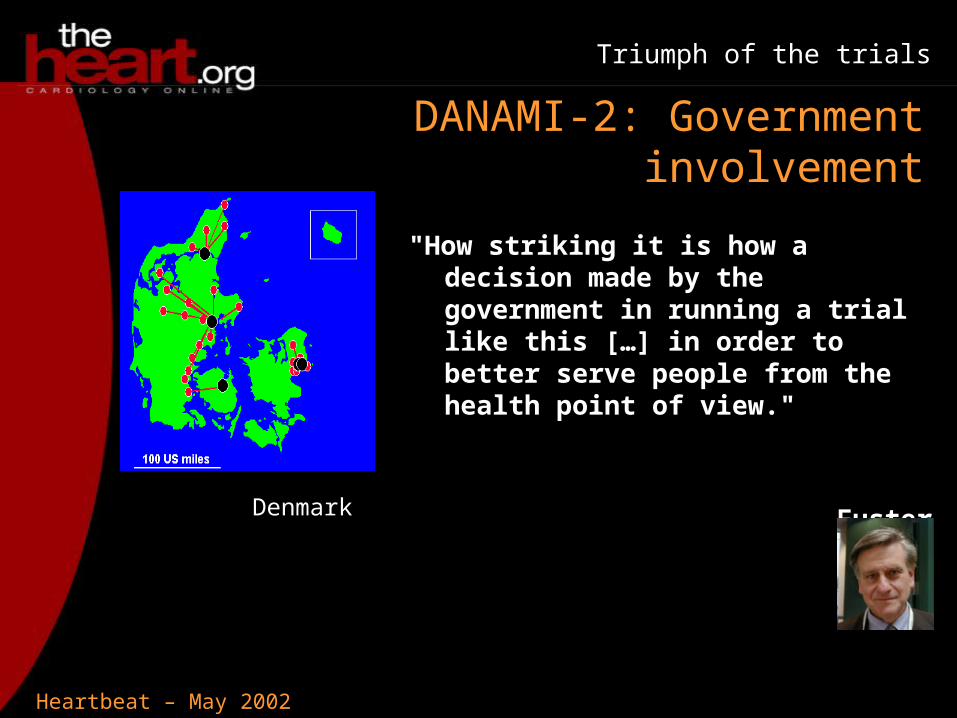
DANAMI-2: Government involvement
"How striking it is how a decision made by the government in running a trial like this […] in order to better serve people from the health point of view."
FusterDenmark
Heartbeat – May 2002
Triumph of the trials
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
8.0%
Death
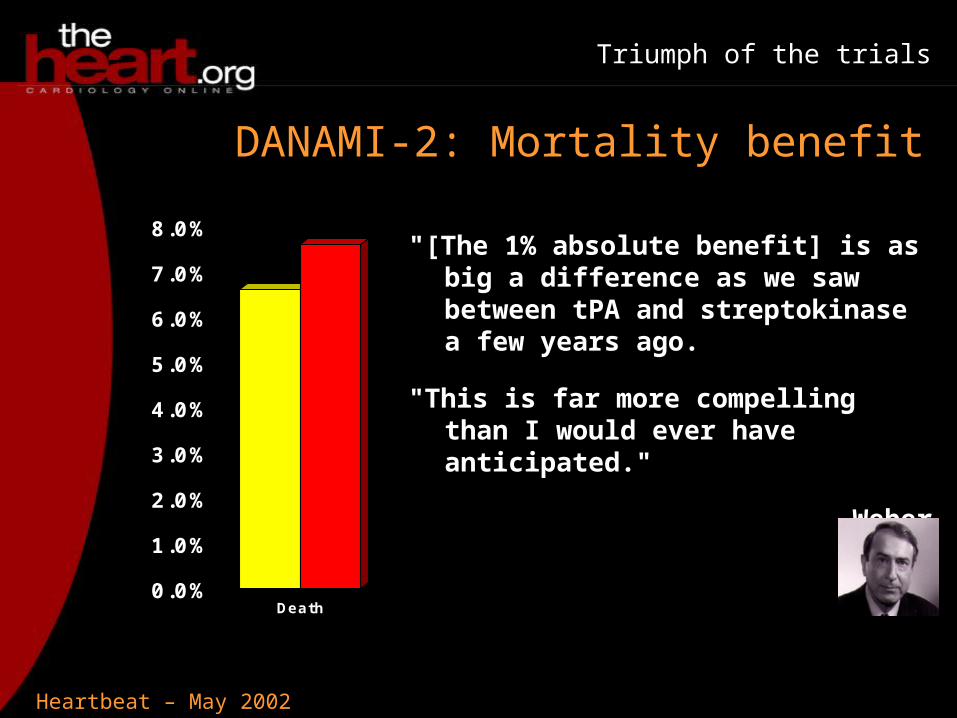
DANAMI-2: Mortality benefit
"[The 1% absolute benefit] is as big a difference as we saw between tPA and streptokinase a few years ago.
"This is far more compelling than I would ever have anticipated."
Weber
Heartbeat – May 2002
Triumph of the trials
"This isn't casual angioplasty versus thrombolysis but in order to offer or expect the benefits of this strategy you really have to gear things up and do rapid angioplasty."
"Making a real commitment to the strategy will be the key to its success."
Cannon
DANAMI-2: Treatment strategy
Heartbeat – May 2002
Triumph of the trials
DANAMI-2: Logistical problems
The great transfer success is because of an integrated system
Could the US adopt a system where a single phone call starts the system up at another hospital?
Fuster
Heartbeat – May 2002
Triumph of the trials
DANAMI-2: Committing to a system
O'Connor
"If we're going to make this effective therapy […], we have to have protocols in place just like we have a protocol to do a clinical trial, we have to follow the protocol and people have to think of the care they are delivering like a clinical trial."
Heartbeat – May 2002
Triumph of the trials
DANAMI-2 site
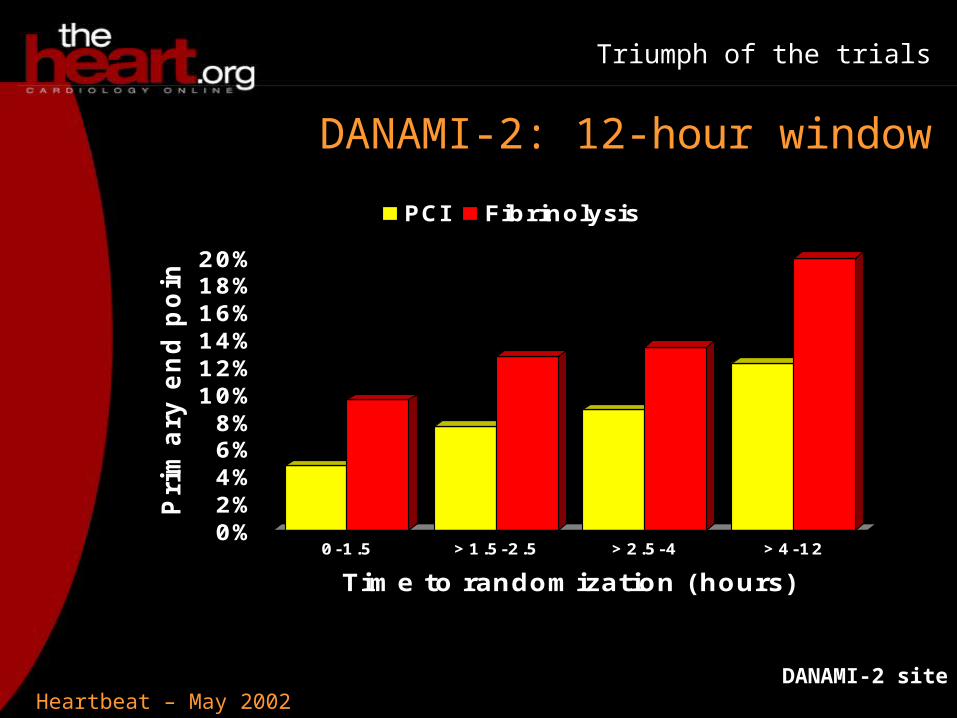
DANAMI-2: 12-hour window
0%2%4%6%8%
10%12%14%16%18%20%
Pri
mary
end p
oin
t
0-1.5 >1.5-2.5 >2.5-4 >4-12
Time to randomization (hours)
PCI Fibrinolysis
Heartbeat – May 2002
Triumph of the trials
DANAMI-2: Busy cath-labs
Weber
If we accept these results, won't there be a tendency for EMS and referring doctors to bypass any hospital without PCI?
It's very likely, but with only 10-15% of hospitals having cath-labs available, it will be very busy
At least we seem to have a 12-hour window for the PCI
Fuster
Heartbeat – May 2002
Triumph of the trials
DANAMI-2: Resistance
O'Connor
"In our health system, finances drive a lot of the way these patients are allocated to hospitals. And because the MI patient is a high-DRG diagnosis there is going to be some resistance, unfortunately, unless we can tie quality and outcomes to the care of these patients."
Heartbeat – May 2002
Triumph of the trials
"How expensive is it going to be to prepare institutions to be ready for these kinds of transfers?"
Fuster
"In figuring out the real costs we have to go beyond the acute event and see what happens over the next few days and the next few weeks."
Weber
DANAMI-2: Economics
Heartbeat – May 2002
Triumph of the trials
DANAMI-2: Summary
It is feasible to transfer patients in a reasonable window of time
It will require a community-wide commitment in order to make this happen
Is that commitment possible economically?
Fuster
Heartbeat – May 2002
Triumph of the trials
DANAMI-2: Costs
Costs are similar for thrombolysis and PCI since many thrombolysis patients go on to get PCI later
Receiving hospitals like more patients so there is not a burden
The fear is that the referral hospitals will lose not just the ST-elevation patients but all chest pain patients
Cannon
Heartbeat – May 2002
Triumph of the trials
DANAMI-2: Boston pilot study
We have to have the protocol of 12-lead ECG in field to target specifically the ST-elevation patients
We are changing the paradigm from going to the nearest acute hospital to going to the nearest primary angioplasty hospital
A 5- or 6-year process
Cannon
Heartbeat – May 2002
Triumph of the trials
LIFE: Inclusion Criteria
Losartan Intervention For Endpoint reduction in hypertension• 9193 patients
• Age 55-80 years
• Previously treated or untreated hypertension
• Systolic BP 160-200 mmHg or diastolic BP 95-115 mmHg
• ECG LVH
Cornell Voltage Duration Product >2440 mm*msec (6-mm gender adjustment in women)
Sokolow-Lyon >38 mm
Heartbeat – May 2002
Triumph of the trials
LIFE: Hypothesis
If two drugs lower the blood pressure equally but one causes LVH regression, is one superior in preventing CV events?
Primary composite endpoint of cardiovascular morbidity and mortality, defined as stroke, MI or cardiovascular death
Losartan vs atenolol
Heartbeat – May 2002
Triumph of the trials
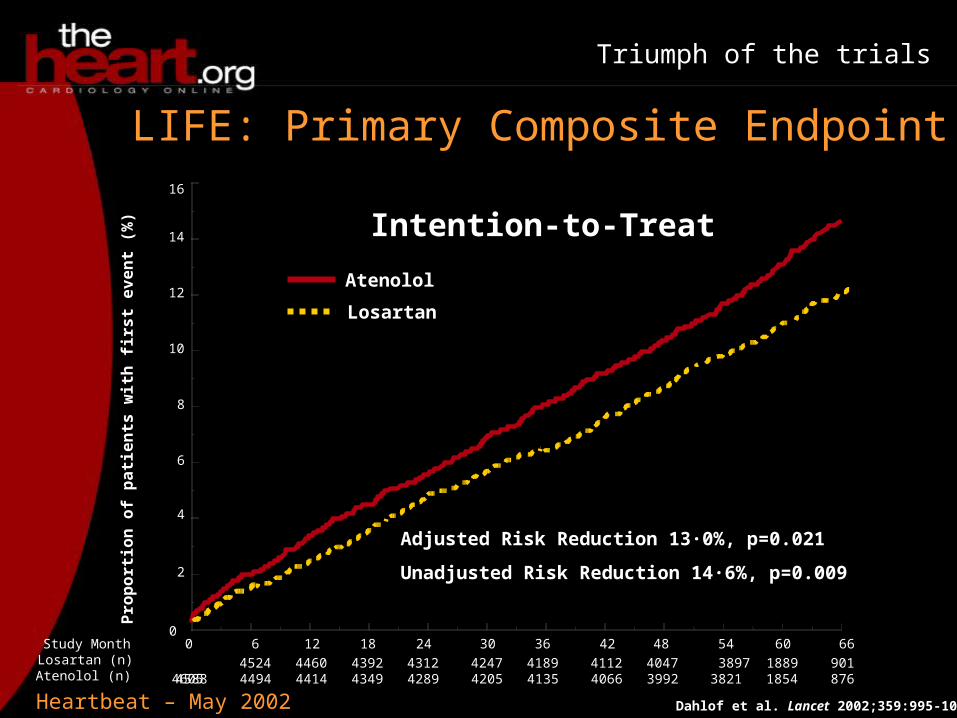
LIFE: Primary Composite Endpoint
6
Pro
port
ion
of
pati
en
ts w
ith
firs
t even
t (%
)
18 24 30 36 42 48 54
Losartan
Atenolol
Dahlof et al. Lancet 2002;359:995-1003
60 6600
2
4
6
8
10
12
14
16
Intention-to-Treat
12
Adjusted Risk Reduction 13·0%, p=0.021
Unadjusted Risk Reduction 14·6%, p=0.009
Study MonthLosartan (n)Atenolol (n)
4605 4524 4460 4392 4312 4247 4189 4112 4047 3897 1889 9014588 4494 4414 4349 4289 4205 4135 4066 3992 3821 1854 876
Heartbeat – May 2002
Triumph of the trials
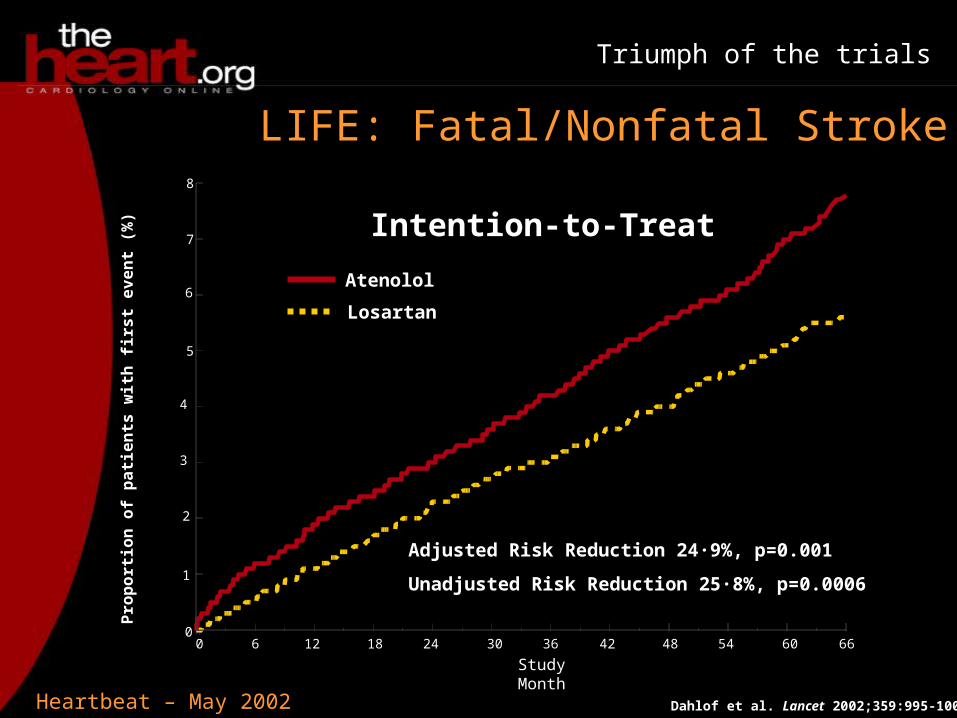
LIFE: Fatal/Nonfatal Stroke
6
Pro
port
ion
of
pati
en
ts w
ith
firs
t even
t (%
)
18 24 30 36 42 48 54
Losartan
Atenolol
Dahlof et al. Lancet 2002;359:995-1003
60 660
Intention-to-Treat
12
Adjusted Risk Reduction 24·9%, p=0.001
Unadjusted Risk Reduction 25·8%, p=0.0006
Study Month
8
7
6
5
4
3
2
1
0
Heartbeat – May 2002
Triumph of the trials
LIFE: Additional points
Blood pressure drop was the same in both groups
LVH regressed in roughly 1/3 of patients in losartan group
New onset of diabetes reduced by 25%
Heartbeat – May 2002
Triumph of the trials
"The first time that, head-to-head, one anti-hypertensive drug has beaten another anti-hypertensive drug in terms of important clinical endpoints."
"Since the blood pressure reductions with the two drugs were identical, then we have to believe that blocking the renin-angiotensin system […] is critical in providing protection for these vulnerable patients."
LIFE: Head-to-head winner
Weber
Heartbeat – May 2002
Triumph of the trials
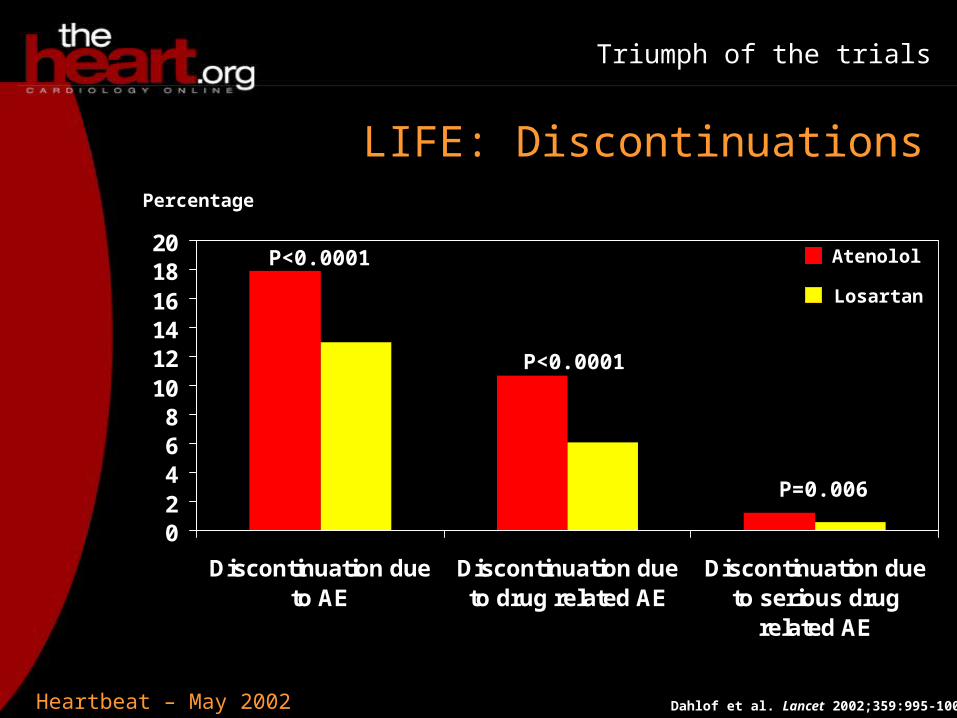
LIFE: Discontinuations
Dahlof et al. Lancet 2002;359:995-1003
02468
101214161820
Discontinuation dueto AE
Discontinuation dueto drug related AE
Discontinuation dueto serious drug
related AE
Percentage
P<0.0001
P<0.0001
P=0.006
Atenolol
Losartan
Heartbeat – May 2002
Triumph of the trials
ACC 2002
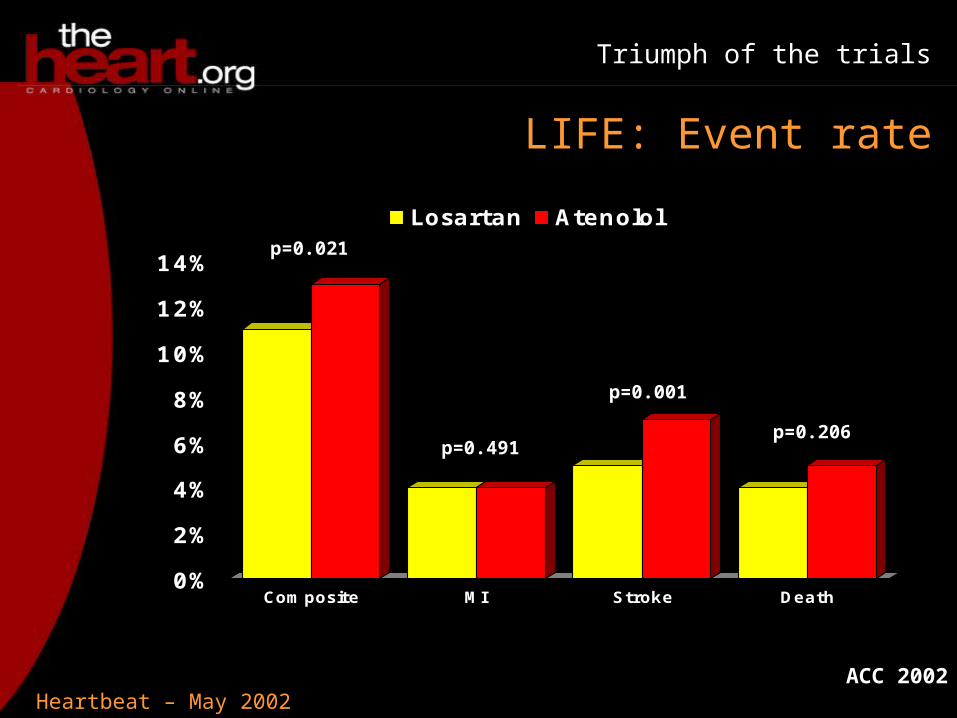
LIFE: Event rate
0%
2%
4%
6%
8%
10%
12%
14%
Composite MI Stroke Death
Losartan Atenololp=0.021
p=0.491
p=0.001
p=0.206
Heartbeat – May 2002
Triumph of the trials
"From a patient's point of view, these are all major cardiovascular events and so none of the three [death, MI, stroke] is any good to have."
It is hoped this will provide guidance for offering therapy a patient can comply with easily
"This could be a terrific way to offer appropriate blood pressure reduction."
LIFE: Patient's view
Cannon
Heartbeat – May 2002
Triumph of the trials
It is hoped this will point toward research into the effect of the renin-angiotensin system on stroke
A patient with a prior MI should be on a beta-blocker, and this suggests you should add angiotensin II inhibition as well
LIFE: Combination therapy
Cannon
Heartbeat – May 2002
Triumph of the trials
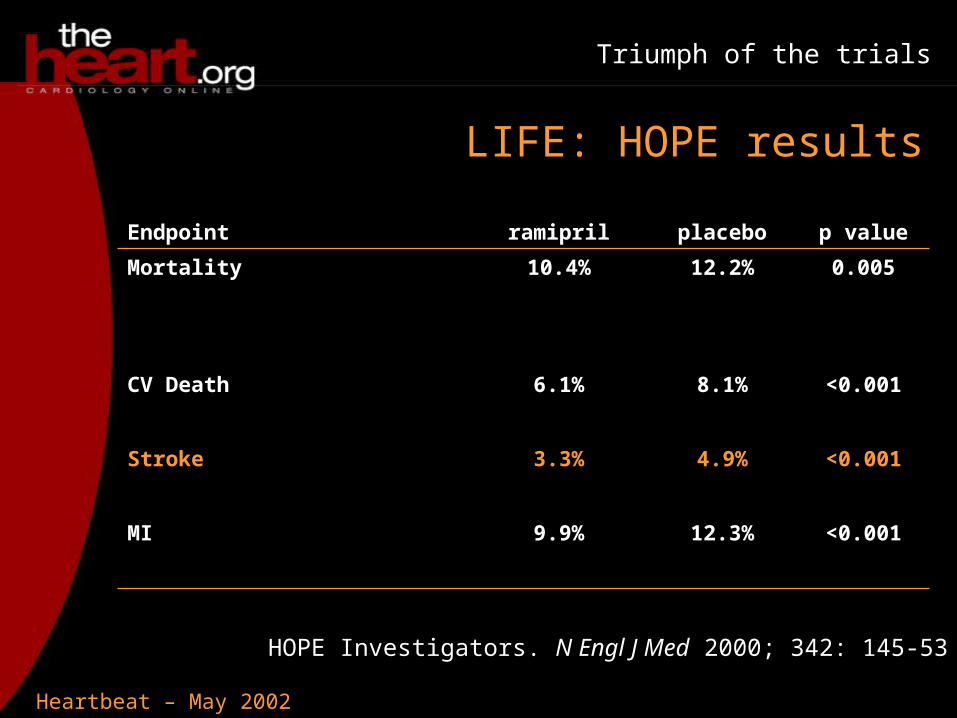
LIFE: HOPE results
Endpoint ramipril placebo p value
Mortality 10.4% 12.2% 0.005
CV Death 6.1% 8.1% <0.001
Stroke 3.3% 4.9% <0.001
MI 9.9% 12.3% <0.001
HOPE Investigators. N Engl J Med 2000; 342: 145-53
Heartbeat – May 2002
Triumph of the trials
HOPE compared ACE-inhibitor vs placebo
"The HOPE study was bedeviled by the fact that there were blood-pressure changes. Some people are even arguing that much of the benefit of the ACE inhibitor in HOPE could be explained by the fact that it lowered blood pressure pretty effectively."
LIFE: Differences with HOPE
Weber
Heartbeat – May 2002
Triumph of the trials
"You can make an argument right now […] that for any reasonably high-risk hypertensive who came into your office that an angiotensin-receptor blocker might have to be your number-one preferred drug to start the treatment […] because it has gone out and beaten the drug that is currently recommended as the first step in treatment."
LIFE: New first-choice therapy
Weber
Heartbeat – May 2002
Triumph of the trials
LIFE: Future trials
Antihypertensive Lipid Lowering Heart Attack Trial – (ALLHAT)
doxazosin vs chlorthalidone
Valsartan Antihypertensive Long-term Use Evaluation - (VALUE)
valsartan vs amlodipine
Heartbeat – May 2002
Triumph of the trials
"All these hundreds of millions of dollars and years and years of effort will be wasted, or at least greatly diluted, if indeed we don't have equal blood pressure effects so we can really look at what goes beyond the blood pressure."
LIFE: Matching blood pressure
Weber
Heartbeat – May 2002
Triumph of the trials
WIZARD: C pneumoniae in MI
4-5 years ago we believed that infections are important in CVD
• C pneumoniae inside the arteries
• C pneumoniae inside the monocytes
• Small retrospective studies seemed to support this idea
Fuster
Heartbeat – May 2002
Triumph of the trials
WIZARD: ACADEMIC
Azithromycin in Coronary Artery Disease: Elimination of Myocardial Infection with Chlamydia
302 patients with CAD and positive serology for C pneumoniae randomized to receive either placebo or azithromycin
No significant difference in primary endpoint: CV death, non-fatal MI, or unplanned revascularization
Circulation 2000; 102(15):1755-60
Heartbeat – May 2002
Triumph of the trials
WIZARD: CLARIFY
Clarithromycin in Acute Coronary Syndrome Patients in Finland (CLARIFY)
148 patients randomized to placebo or clarithromycin for 3 months
Patients were followed for up to 3 years
51% relative risk reduction in CV events
Circulation 2002; 105(13): 1555-60
Heartbeat – May 2002
Triumph of the trials
WIZARD: Infectious burden
German study links the number of infections to severity of atherosclerosis
Circulation 2002; 105(1):15-21
"Where Framingham said risk factors are important, now we are going to say the number of infections are important but you have to accumulate a number of them to really have an impact."
Fuster
Heartbeat – May 2002
Triumph of the trials
WIZARD: Trial design
Weekly Intervention with Zithromax for Atherosclerosis and its Related Disorders
7747 patients with were randomized to 12 weeks of either azithromycin or placebo
Inclusion criteria> 6 weeks post-MI C pneumoniae 1:16
Heartbeat – May 2002
Triumph of the trials
WIZARD: Change in enrollment
O'Connor
WIZARD was originally powered to enroll 3000 patients and detect a 25% difference
Pfizer got feedback saying that a 15-20% event reduction would be acceptable, and so expanded and extended the trial
"It was very courageous of a sponsor because you don't see this often."
Heartbeat – May 2002
Triumph of the trials
WIZARD: Trial design
Primary composite endpoint:MortalityReinfarctionHospitalization for unstable anginaRevascularization
Trial concluded in Feb 2002 with >1000 adjudicated events
Heartbeat – May 2002
Triumph of the trials
0 6 12 18 24 30 36 42 48 540
5
10
15
20
25
30
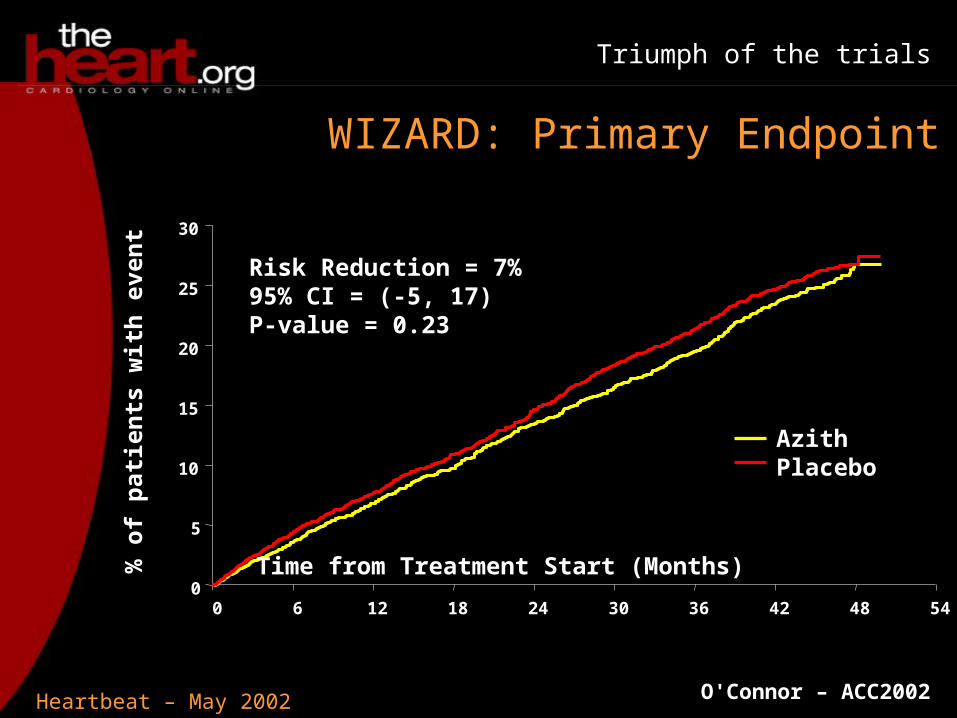
WIZARD: Primary Endpoint%
of
pat
ien
ts w
ith
eve
nt
Time from Treatment Start (Months)
Risk Reduction = 7%95% CI = (-5, 17)P-value = 0.23
AzithPlacebo
O'Connor – ACC2002
Heartbeat – May 2002
Triumph of the trials
WIZARD: Length of treatment
CLARIFY saw benefit appear after long treatment and long follow-up, do you think we will see the same with WIZARD?
When the study was planned, the issues around duration of therapy were toxicology issues
A decision was made to go ahead and not wait for the toxicology studies
O'Connor
Heartbeat – May 2002
Triumph of the trials
0 0.5 1 1.5
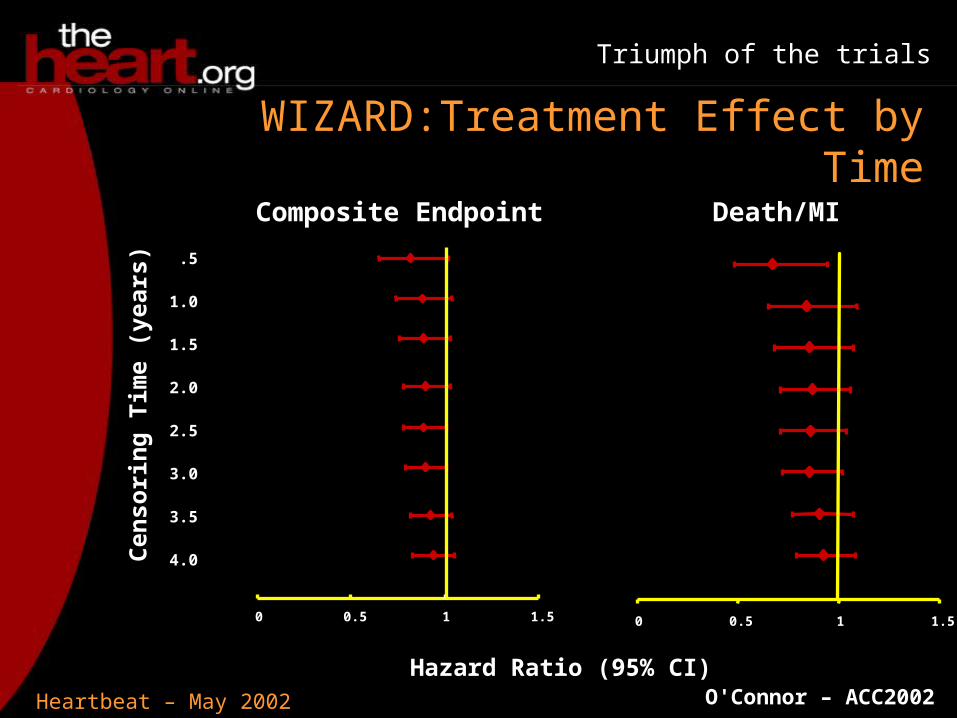
WIZARD:Treatment Effect by Time
0 0.5 1 1.5
Composite Endpoint Death/MI
Cen
sori
ng
Tim
e (y
ears
)
.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
Hazard Ratio (95% CI)O'Connor – ACC2002
Heartbeat – May 2002
Triumph of the trials
WIZARD: Duration is critical
O'Connor
"I think duration is critical, and therefore I think there is still hope."
"You just have to treat this longer."
Heartbeat – May 2002
Triumph of the trials
WIZARD: PROVE-IT
PROVE-IT: Pravastatin or Atorvastatin Evaluation and Infection Therapy
Patients will be randomized to pravastatin or atorvastatin and to gatifloxacin or placebo
Patients will receive gatifloxacin treatment throughout the trial (minimum 18 months, expected mean 24 months) for 10 days of every month
Heartbeat – May 2002
Triumph of the trials
"Until we do have some sort of toxicology data and some sort of sense of what we're doing to our whole flora, I really wouldn't know what to predict would be the effect of giving an antibiotic for that long and I would be very nervous about that."
Weber
WIZARD: Toxicology
Heartbeat – May 2002
Triumph of the trials
WIZARD: Multiple infections
Are we too focused on one microorganism?
It could be like giving a statin to a hypertensive patient or an anti-hypertensive to someone with high cholesterol
Maybe there are multiple microorganisms we need to target with different drugs
Fuster
Heartbeat – May 2002
Triumph of the trials
WIZARD: Multiple targets
We didn't make progress against Hodgkin's disease until we began using multiple agents
There is evidence for multiple organisms in CVD
"It's tricky when you're talking about duration of therapy."
O'Connor
Heartbeat – May 2002
Triumph of the trials
"A lot of it is driven by what agents we have. If we had an agent that could effectively treat CMV without a lot of toxicity that would certainly be worth testing, but we just have easy antibiotics that we used against chlamydia."
Cannon
WIZARD: Use the drugs we have
Heartbeat – May 2002
Triumph of the trials
WIZARD: Monitoring for superinfection
PROVE-IT is being monitored in a blinded fashion
•previous trials found fewer infections in the antibiotic groups
•multiple classes of agents allow us to evade resistance
Both ACES and PROVE-IT should be out in about 2 years
Cannon
Heartbeat – May 2002
Triumph of the trials
ICDs for post-MI patients with low EF
Economic factors are enormous
Should still do some kind of EPS study to risk-stratify
patients
Summary: MADIT II
Heartbeat – May 2002
Triumph of the trials
We didn't get the quality of life information we wanted
Mortality is not different between rate or rhythm control
Summary: Atrial fibrillation
Heartbeat – May 2002
Triumph of the trials
FIM study showed 0% restenosis
RAVEL also shows 0% restenosis in eluting-stent arm
Summary: Coated stents
Heartbeat – May 2002
Triumph of the trials
Maybe it is time for patients to be moved to PCI centers
Must have a system prepared to use this
The economic impact of this needs to be studied
Summary: DANAMI-2
Heartbeat – May 2002
Triumph of the trials
Similar drop in blood pressure with losartan but significant benefits over atenelol, especially in stroke
This may shift what we use as first-line therapy in
hypertension
Summary: LIFE
Heartbeat – May 2002
Triumph of the trials
We have much to learn about the microorganisms affecting the vascular system
WIZARD was disappointing, showing no significant effect of antibiotics
Summary: WIZARD
Heartbeat – May 2002
Triumph of the trials
It is exciting that we have the kinds of studies that can change practice
"I think in particular DANAMI-2 and LIFE will change the way I practice personally and the way we recommend practices to change in our healthcare system in North Carolina."
Conclusions: O'Connor
O'Connor
Heartbeat – May 2002
Triumph of the trials
Conclusions: Weber
Weber
DANAMI-2
"There seems to be a different time clock for the biology of what happens to a thrombus and what happens to the myocardium following an acute MI. Clearly, after 4-6 hours its too late to do anything about the thrombus, even so apparently the myocardium may still be very viable."
Heartbeat – May 2002
Triumph of the trials
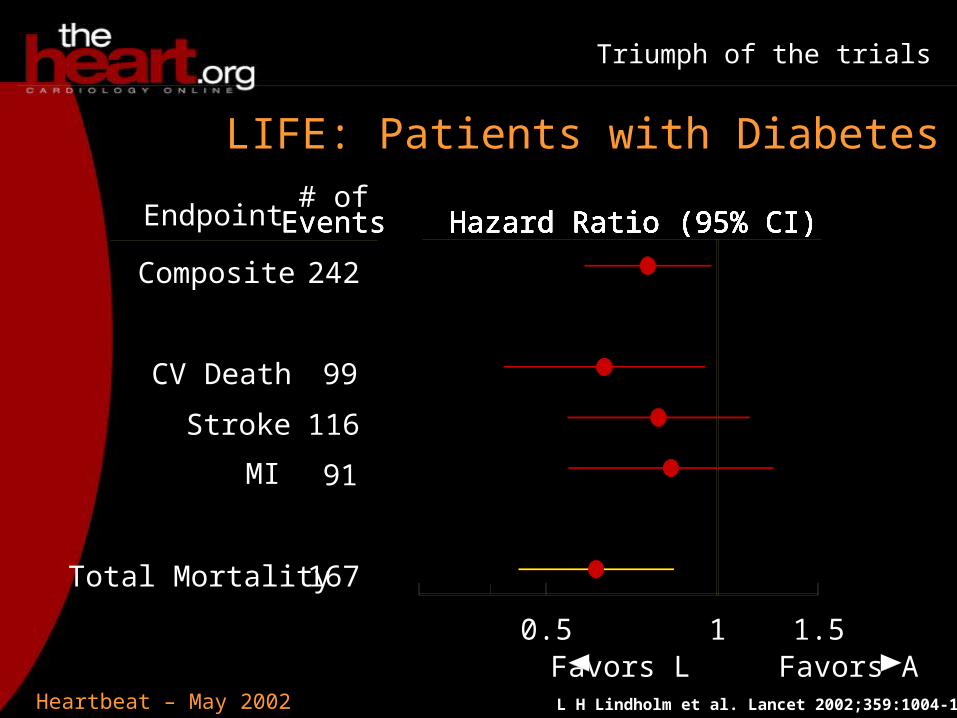
0.5 1 1.5Favors L Favors A
Hazard Ratio (95% CI)Hazard Ratio (95% CI)Hazard Ratio (95% CI)Hazard Ratio (95% CI)Hazard Ratio (95% CI)Hazard Ratio (95% CI)Hazard Ratio (95% CI)Hazard Ratio (95% CI)Hazard Ratio (95% CI)
Composite
CV Death
Stroke
MI
Total Mortality
Endpoint
242
99
116
91
167
# ofEventsEventsEvents
LIFE: Patients with Diabetes
L H Lindholm et al. Lancet 2002;359:1004-1010
Heartbeat – May 2002
Triumph of the trials
Conclusions: Weber
Weber
WIZARD
The presence of inflammatory markers does not necessarily indicate infection
Angiotensin and aldosterone can stimulate inflammatory reactions
Other mechanisms may be causing the rise of inflammatory markers
Heartbeat – May 2002
Triumph of the trials
Conclusions: Cannon
Cannon
To have so many good trials guiding therapy is good for cardiology
"We all have lots of things we can change so it keeps the field very fresh and good for patients."

Heartbeat – May 2002
Triumph of the trials
Triumph of the trials: ACC 2002
Valentin Fuster MDDirector, Cardiovascular InstituteMount Sinai Medical CenterNew York, New York
Christopher Cannon MDCardiologistBrigham and Women's HospitalBoston, Massachusetts
Christopher M O'Connor MDAssociate Professor of CardiologyDuke University Medical CenterDurham, NC
Michael Weber MDProfessor of MedicineSUNY Downstate College of MedicineBrooklyn, New York