Embed Size (px)
Citation preview

Heart Replacement in the Age of Stem Cell Therapy and Biosensors Technology.
What we Know and What we can Expect
6th International Symposium on Stem Cell Therapy& Cardiovascular Innovations
Madrid, April 23-24, 2009
Treatment of Severe Heart Failure
Possible Strategies
To replace key dysfunctional pathways
To replace diseased segments of the left ventricle
To replace the whole left ventricle
To replace the whole heart by a transplant
To replace the whole heart by an artificial device
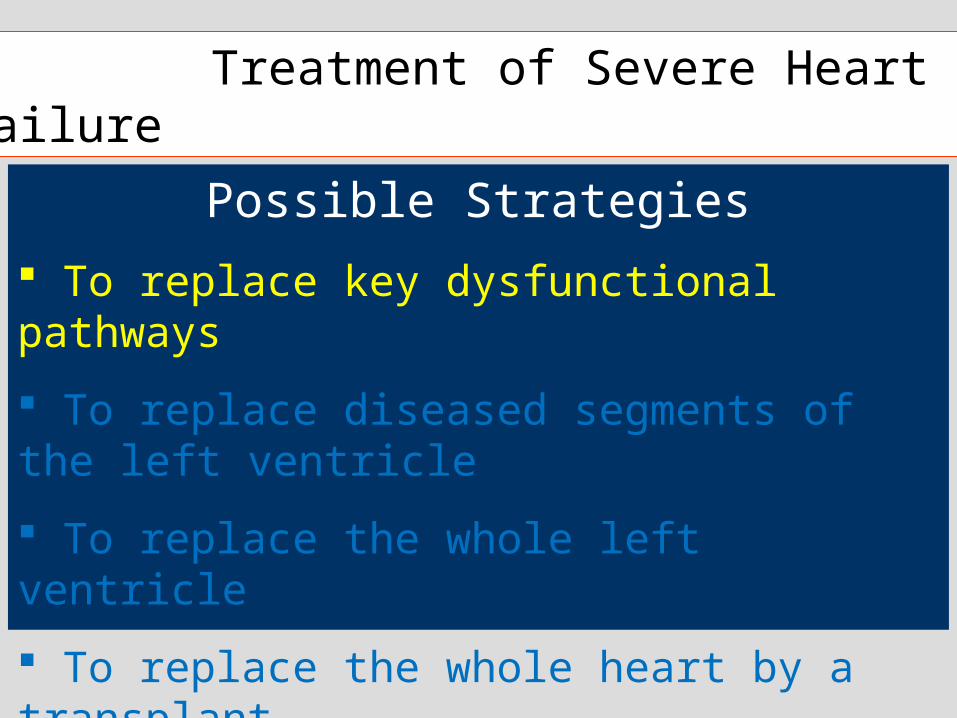
MacLennan Nature Reviews Molecular Cell Biology 2008;4:566-77.
Interactions Between Cardiac Signalling Pathways
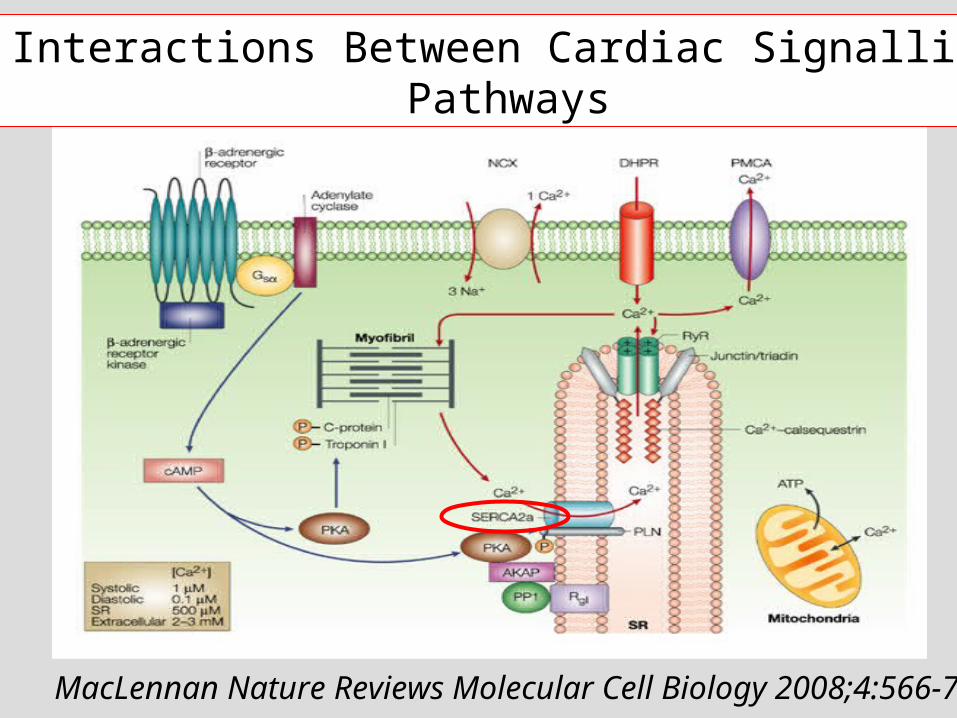
del Monte et al. Circulation 1999;100:2308-11.
Beneficial Effects of SERCA-2 Overexpression in Human Failing Cardiomyocytes
The CUPID Trial
Intracoronary infusion of AAV1/SERCA2a 9 pts with advanced HF (NYHA Class
III/IV; EF ≤30%; VO2 max 16mL/kg/min)
3 dose-escalating cohorts (3pts/cohort) Good safety profile 6- to 12-month FU : Encouraging hints of
efficacy (symptoms, LV function and remodeling, biomarkers)
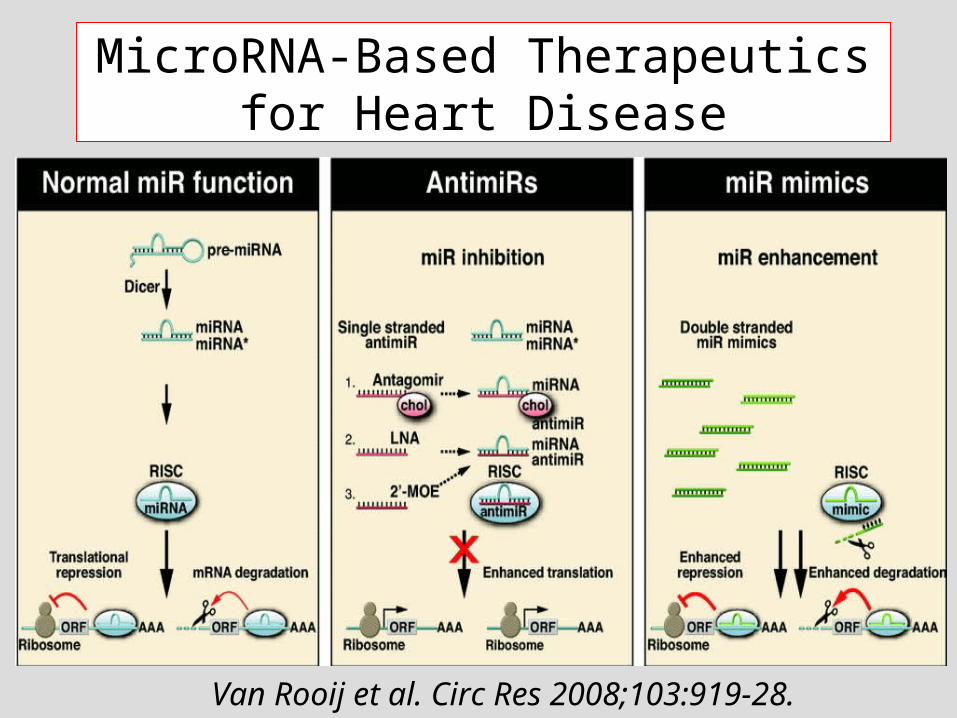
MicroRNA-Based Therapeutics for Heart Disease
Van Rooij et al. Circ Res 2008;103:919-28.
Treatment of Severe Heart Failure
Possible Strategies
To replace key dysfunctional pathways
To replace diseased segments of the left ventricle
To replace the whole left ventricle
To replace the whole heart by a transplant
To replace the whole heart by an artificial device

Bockeria et al. Eur J Cardio-thorac Surg 2006;29:S251-8S.
LV Reconstruction by Patch Plasty Jatene, Dor, Fontan
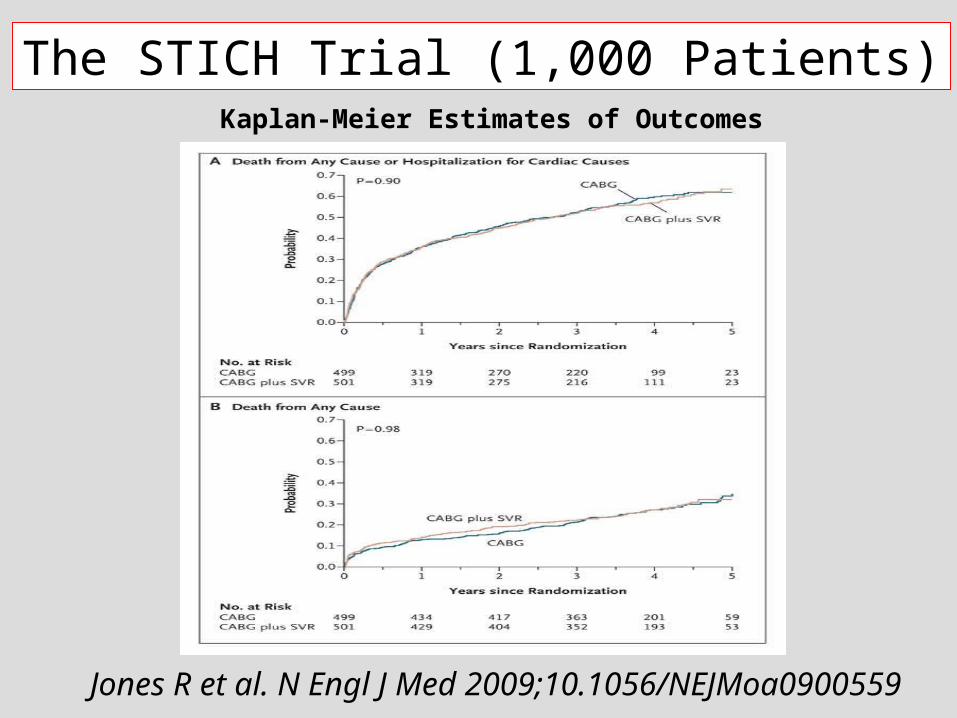
Kaplan-Meier Estimates of Outcomes
The STICH Trial (1,000 Patients)
Jones R et al. N Engl J Med 2009;10.1056/NEJMoa0900559

The STICH Trial (1,000 Patients)
Jones R et al. N Engl J Med 2009;10.1056/NEJMoa0900559
Outcomes

Jones R et al. N Engl J Med 2009;10.1056/NEJMoa0900559
Angina and Heart-Failure Symptoms at Baseline and at the Last FU Visit
The STICH Trial (1,000 Patients)
Treatment of Severe Heart Failure
Possible Strategies
To replace key dysfunctional pathways
To replace diseased segments of the left ventricle
To replace the whole left ventricle
To replace the whole heart by a transplant
To replace the whole heart by an artificial device

Left Ventricular Assist Device

Lietz & Mille Semin Thorac Cardiovasc Surg 2008;20:225-33.
Survival Oucomes of Destination Therapy
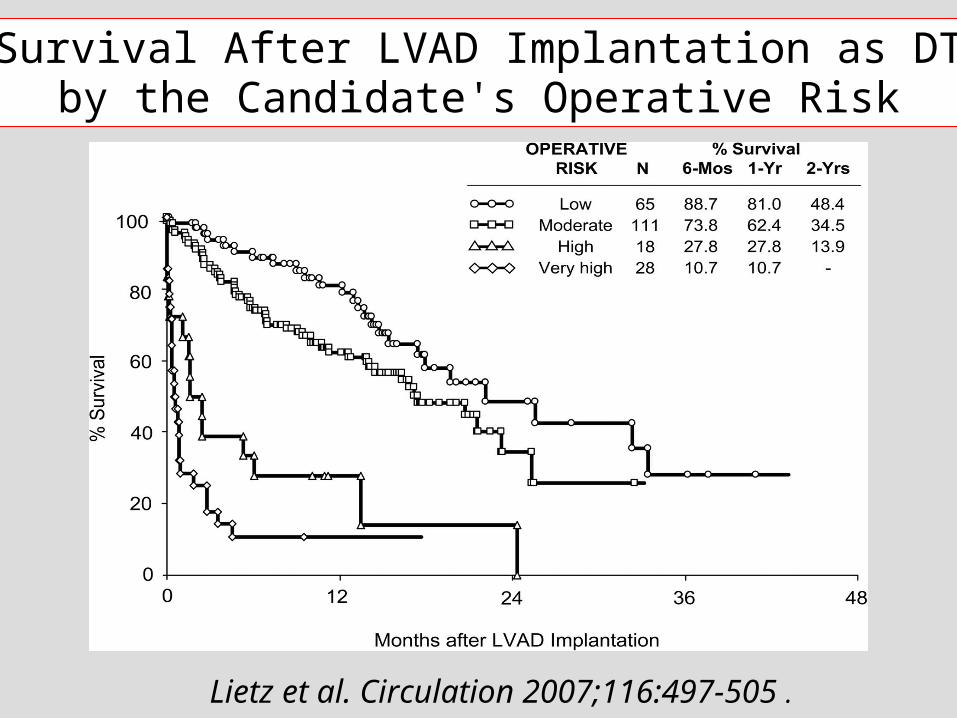
Survival After LVAD Implantation as DT by the Candidate's Operative Risk
Lietz et al. Circulation 2007;116:497-505 .

Long-term Outcomes and Costs of Ventricular Assist Devices Among Medicare Beneficiaries
Hernandez et al. JAMA 2008;300:2398–2406.
Mean 1-year Medicare payments for inpatient care for patients in the 2000–2005 cohorts were $178 714 (SD, $142 549) in the primary device group and $111 769
(SD, $95 413) in the postcardiotomy group

Ongoing Randomized Trials of DT
HeartMateII LVAD vs. HeartMateXVE LVAD
260 pts, estimated primary completion date : June, 2009
vs. Medical Tt (180 pts) or LVAD DT device (45 pts) estimated completion date : 2012
VentrAssist

Treatment of Severe Heart Failure
Possible Strategies
To replace key dysfunctional pathways
To replace diseased segments of the left ventricle
To replace the whole left ventricle
To replace the whole heart by a transplant
To replace the whole heart by an artificial device
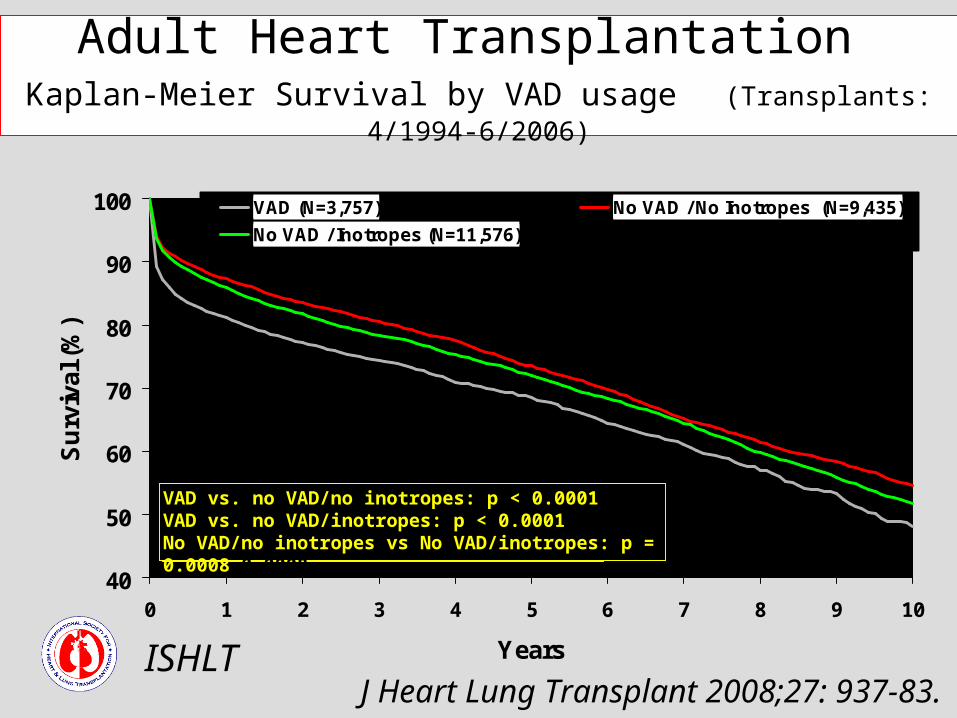
Adult Heart Transplantation Kaplan-Meier Survival by VAD usage (Transplants: 4/1994-6/2006)
40
50
60
70
80
90
100
0 1 2 3 4 5 6 7 8 9 10
Years
Su
rviv
al (
%)
VAD (N=3,757) No VAD / No Inotropes (N=9,435)
No VAD / Inotropes (N=11,576)
VAD vs. no VAD/no inotropes: p < 0.0001VAD vs. no VAD/inotropes: p < 0.0001No VAD/no inotropes vs No VAD/inotropes: p = 0.0008
ISHLT J Heart Lung Transplant 2008;27: 937-83.
VAD vs. no VAD/no inotropes: p < 0.0001VAD vs. no VAD/inotropes: p < 0.0001No VAD/no inotropes vs No VAD/inotropes: p = 0.0008 0.0008

Adult Heart RecipientsEmployment Status of Surviving Recipients
(Follow-ups: 1995 - June 2006)
ISHLT
Last updated based on data as of December 2006
J Heart Lung Transplant 2008;27:937-83.
Retired
Not working
Working part time Working full time
Retired

ISHLT
Last updated based on data as of December 2006
J Heart Lung Transplant 2008;27:937-83.
Cumulative Incidence of Leading Causes of Death After Heart Transplantation in Adults (January 1992-June 2005)

Transplantation for Severe Heart Failure
Areas of Improvement
Improved methods of organ preservation
Extension of the donor pool
Prevention of rejection

Transplantation for Severe Heart Failure
Improved Methods of Organ Preservation
Storage solutions
Manipulations of reperfusion conditions (adhesion molecules, postconditioning)
Continous organ perfusion
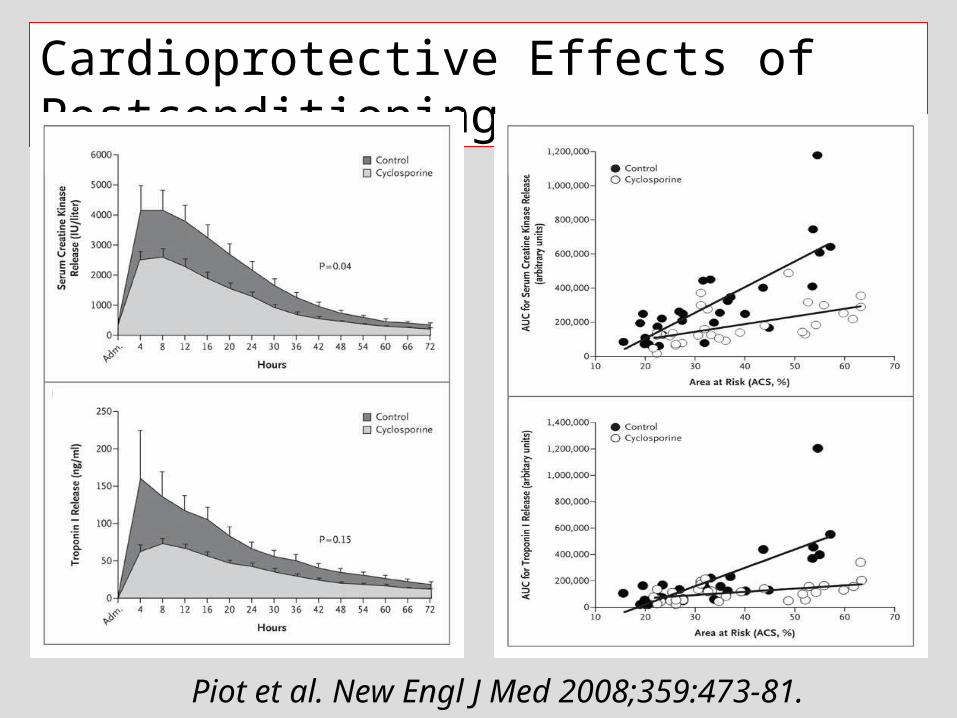
Cardioprotective Effects of Postconditioning
Piot et al. New Engl J Med 2008;359:473-81.
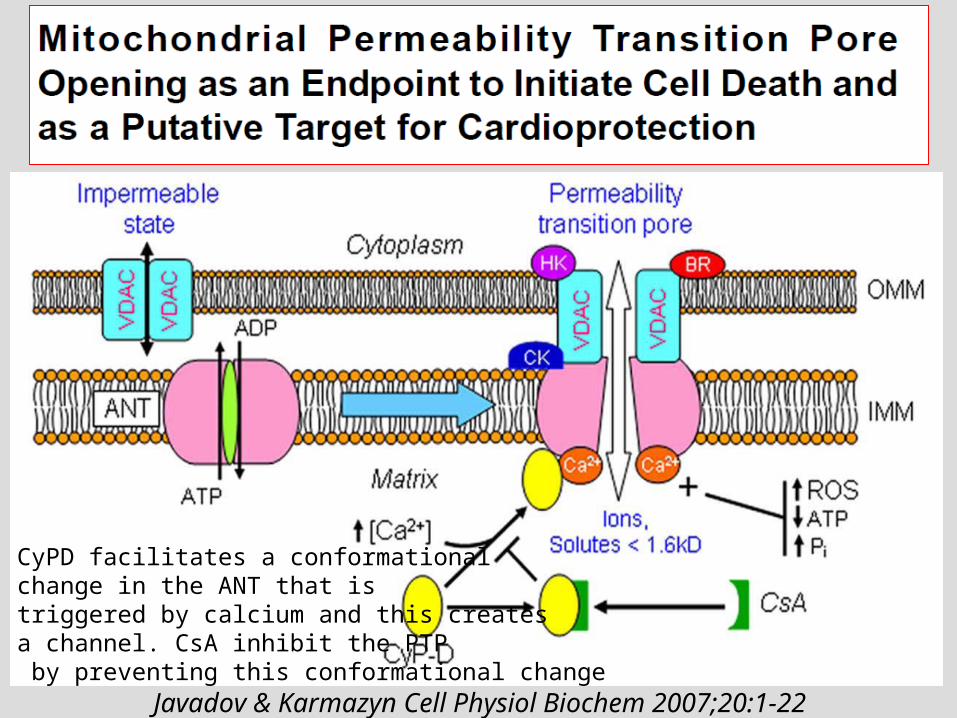
CyPD facilitates a conformational change in the ANT that istriggered by calcium and this creates a channel. CsA inhibit the PTP by preventing this conformational change
Javadov & Karmazyn Cell Physiol Biochem 2007;20:1-22
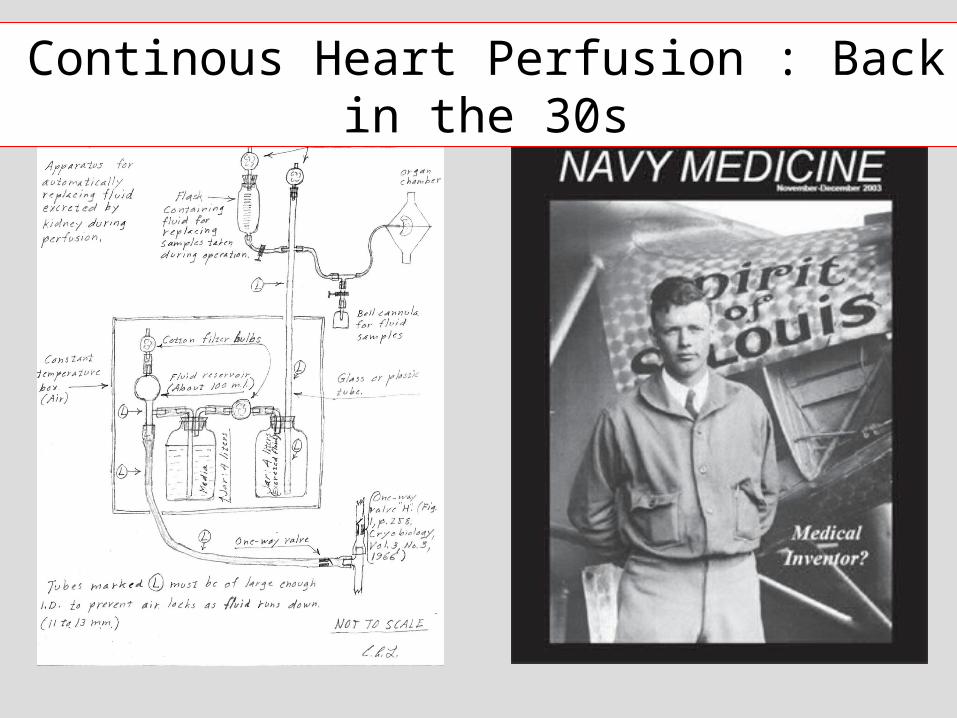
Continous Heart Perfusion : Back in the 30s
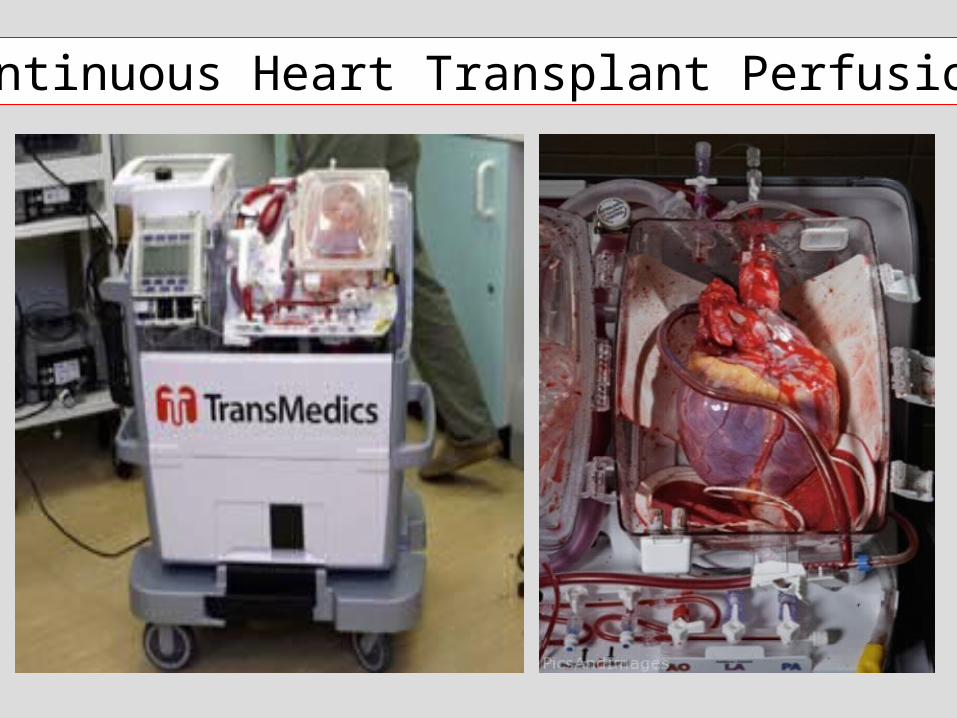
Continuous Heart Transplant Perfusion

Transplantation for Severe Heart Failure
Areas of Improvement
Improved methods of organ preservation
Extension of the donor pool
Prevention of rejection

Ali et al. Eur J Cardiothorac Surg 2007;31:929-33.
Tx Using Hearts From Non-Heart-Beating Donors
38 pts; mean duration of cardiac arrest : 15 min

Transplantation for Severe Heart Failure
Areas of Improvement
Improved methods of organ preservation
Extension of the donor pool
Prevention of rejection

Transplantation for Severe Heart Failure
Prevention of Rejection
New immunosuppressive drugs
Induction of tolerance
Pharmacogenomics

T Cell Activation Through Three Signals
Signal 1 : Recognition of HLA and peptide antigen by T lymphocyteSignal 2 : Co-stimulationSignal 3 : IL-2-triggered lymphocyte proliferation
Halloran PF New Engl J Med 2004;351:2715-29.

Vincenti & Dirk Am J Transplant 2008;1972-81.
Small molecules in clinical trials Biologics in clinical trials
Immunosuppressive Drugs : What’s Next in the Pipeline ?

Transplantation for Severe Heart Failure
Immunosuppressive Agents Under EvaluationExtension from Oncology and Autoimmunity
Monoclonal antibodies (anti-CD3, anti-CD52)
B cell-targeted drugs (anti-CD20 & anti-CD22 mAbs, blockers of the B lymphocyte Stimulator [BLyS] pathway)
Inhibitors of cytokine pathways

Transplantation for Severe Heart Failure
Prevention of Rejection
New immunosuppressive drugs
Induction of tolerance
Pharmacogenomics

Conditioning regimen : cyclophosphamide (D-5, D-4); CD2 (D-1, D0, D+1), ciclosporine, thymic irradiation (D-1)
New Engl J Med 2008;358:353-61.
Transplantation for Severe Heart Failure
Prevention of Rejection
New immunosuppressive drugs
Induction of tolerance
Pharmacogenomics

Anglicheau et al. Am J Transplant 2005;5:595-603.
Consequences of Genetic Polymorphisms For Sirolimus Requirements
Renal transplant in patients on primary sirolimus therapy

Treatment of Severe Heart Failure
Possible Strategies
To replace key dysfunctional pathways
To replace diseased segments of the left ventricle
To replace the whole left ventricle
To replace the whole heart by a transplant
To replace the whole heart by an artificial device

CardioWest TAH
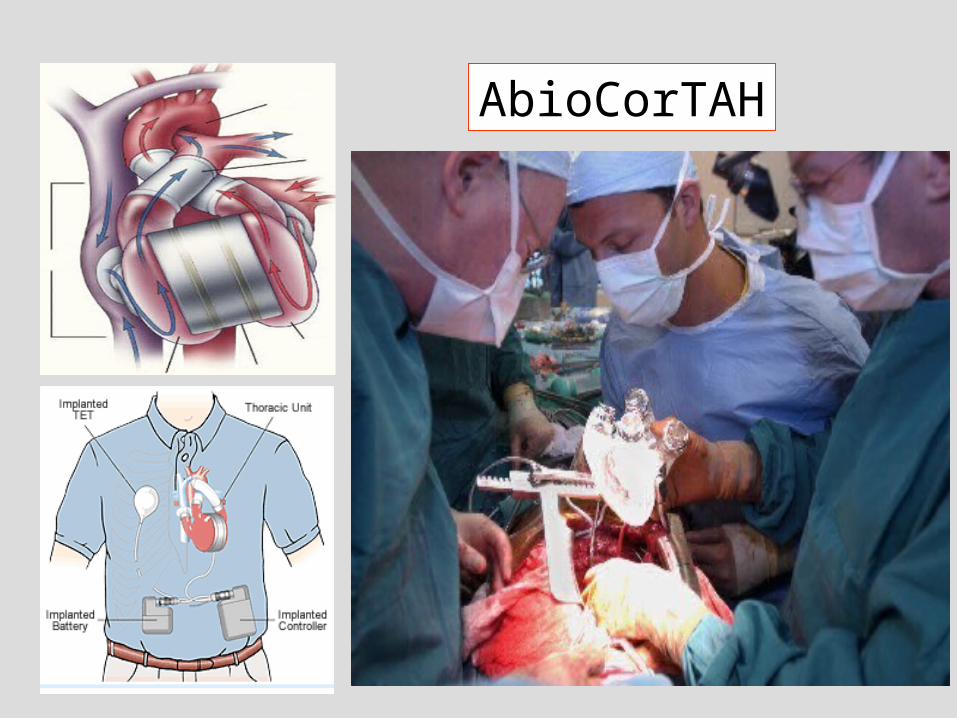
AbioCorTAH


Treatment of Severe HF by Mechanical Devices
Expectations Miniaturization of systems Better durability Easier mode of operation Totally implantable designs
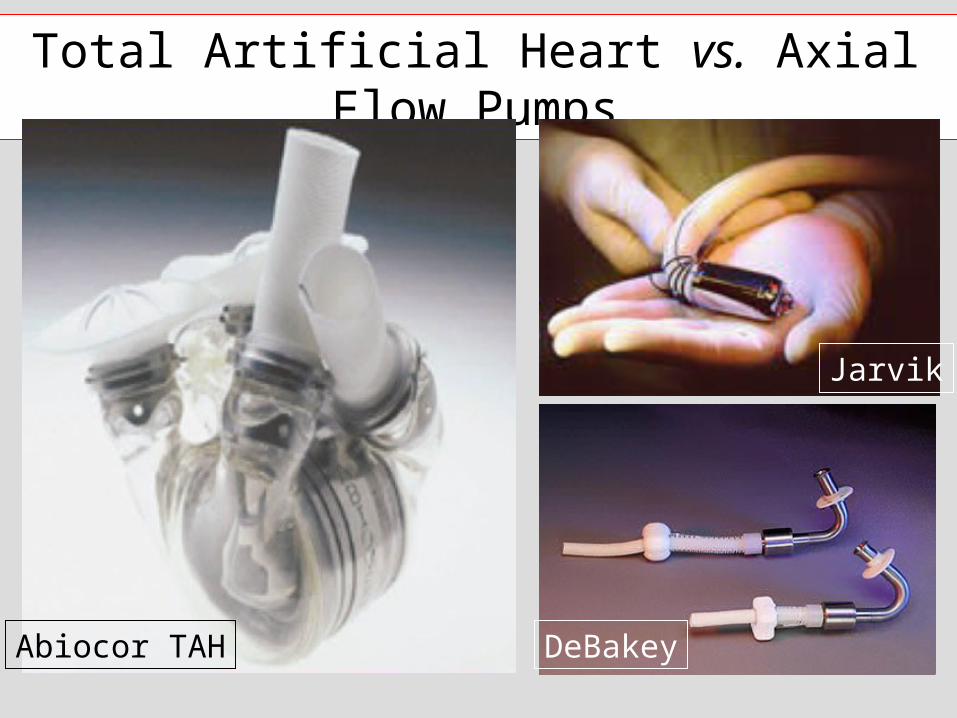
Total Artificial Heart vs. Axial Flow Pumps
Abiocor TAH
Jarvik
DeBakey

Treatment of Severe HF
Conclusions Patients with severe HF can now be offered awide variety of therapeutic interventions The place of stem cells will depend of how they compete with these treatments with regard to safety, efficacy, but also, practicality of implementation, approvability by regulatory authorities and cost