Embed Size (px)
Citation preview

1726 JACC Vol. 25, No. 7 June 1995:1726-35
REVIEW ARTICLE
Heart Rate Adjustment of ST Segment Depression and Performance of the Exercise Electrocardiogram: A Critical Evaluation
P E T E R M. OKIN, MD, FACC, P A U L K L I G F I E L D , MD, F A C C
New York, New York
Analysis of the rate-related change in exercise-induced ST segment depression using the exercise ST segment/heart rate slope and ST segment/heart rate index can improve the accuracy of the exercise electrocardiogram (ECG) for the identification of patients with coronary artery disease, recognition of patients with anatomically or functionally severe coronary obstruction and detection of patients at increased risk for future coronary events. These methods provide a more physiologic approach to analysis of the ST segment response to exercise by adjusting the apparent severity of ischemia for the corresponding increase in myocardial oxygen demand, which in turn can be linearly related to increasing heart rate. Solid-angle theory provides a model for the linear relation of ST segment depression to heart rate during exercise and a framework for understanding the relation of the ST
segment/heart rate slope to the presence and extent of coronary artery disease. False positive and false negative test results of the heart rate-adjusted methods are well known in selected popula- tions and require further clarification. Application of these meth- ods is also highly dependent on the type of exercise protocol, number of ECG leads examined, timing of ST segment measure- ment relative to the J point and accuracy and precision of ST segment measurement. These methodologic details have been an important limitation to test application when traditional proto- cols and measurement procedures are required. When applied with attention to required details, the heart rate-adjusted meth- ods can improve the usefulness of the exercise ECG in a range of clinically relevant populations.
(J Am Coll Cardiol 1995;25:1726-35)
Poor sensitivity and poor predictive value of standard ST segment depression criteria have limited the usefulness of the exercise electrocardiogram (ECG) (or exercise tolerance test) for the detection and evaluation of coronary artery disease (1-9). In response to these well recognized limitations, new test algorithms based on heart rate adjustment of the magni- tude of ST segment depression during exercise have been developed over the past 15 years (10-52). Within defined conditions, these methods improve the accuracy of the exercise ECG, either for the detection of coronary obstruction (10- 12,19-23,25,26,29,30,37,42,46) or for assessment of the ana- tomic, functional and prognostic severity of coronary disease (10,11,19-21,24,27,34,37,44,48) in a range of clinically relevant populations. Application of heart rate-adjusted methods has been shown to be strongly dependent on population selection, exercise protocol, number of ECG leads and precision and accuracy of ST segment measurement (29-33,36-38,40- 43,46-61). This review examines the value and limitations of the heart rate-adjusted indexes of ST segment depression in a theoretic and experimental context (62-75) that focuses on the
From the Division of Cardiology, Department of Medicine, The New York Hospitat-Cornell Medical Center, New York, New York. This study was sup- ported by grants from the Elizabeth and Robert Rosenman Charitable Founda- tion and the David and Hope G. Solinger Foundation, Inc., New York, New York.
Manuscript received October 7, 1994; revised manuscript received January 26, 1995, accepted February 2, 1995.
Address for corresnondence: Dr. Peter M. Okin, The New York Hospital- Cornell Medical Center, 525 East 68th Street, New York, New York 10021.
methodologic and population conditions that govern perfor- mance of these new measures.
M e t h o d s o f H e a r t R a t e A d j u s t m e n t o f S T
S e g m e n t D e p r e s s i o n
Heart rate adjustment is a rational, physiologic approach to interpretation of the exercise tolerance test. ST segment depression recorded on the surface ECG during exercise- induced ischemia results primarily from the separate interac- tive influences of the extent of coronary obstruction and the magnitude of excess myocardial oxygen demand (51,62-75). In patients with demand-mediated myocardial ischemia due to obstructive coronary artery disease, ST depression will be proportional to exercise work load for any degree of obstruc- tion. Thus, a patient with 1.0 mm (100/xV) of ST depression during exercise might reach 1.5 or 2.0 mm of ST depression with further effort, whereas less effort might provoke only 0.5 mm of ST depression. Because the underlying extent of coronary obstruction is the same in each of these conditions, the ischemia apparent in ST depression alone cannot be directly related to the presence or extent of disease without adjustment for the corresponding myocardial work load.
Physiologic insights result when exercise-induced ST seg- ment depression is plotted against heart rate rather than against time. At higher exercise work loads, myocardial oxygen demand is directly proportional to heart rate (70,71,73,75), and clinical observations suggest that the relation between ST
©1995 by the American College of Cardiology 0735-1097/95/$9.50 0735-1097(95)00085-I

JACC Vol. 25, No. 7 OKIN AND KLIGFIELD 1727 June 1995:1726-35 HEART RATE ADJUSTMENT OF ST SEGMENT DEPRESSION
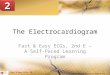
Figure 1. Calculation of the ST segment depression/heart rate (STAIR) slope. Pro- gressive ST segment depression in lead CM 5 (shown as a positive magnitude on the vertical axis) is plotted against exer- cise heart rate in a patient with three- vessel coronary artery disease. This case illustrates the linear relation "of ST seg- ment depression to heart rate as peak exercise is approached. As a result, the slope of the line relating the final three data points by linear regression is higher than the slope of lines incorporating ear- lier data points. When more than one linear correlation is statistically significant, the greatest value (in this case 10.0) is taken as the test result for that patient. Note that the value obtained by simply dividing the total change in ST segment depression by the total change in heart rate (the ST segment/heart rate index) markedly underestimates the true ST seg- ment/heart rate slope, bpm = beats/rain.
300
200
ST DEPRESSION
(uv) lOO
0
- 1 0 0 50
0 / 0 /
~ 0 . . . . . ST/HR slope= 10.0 (r= 1.000, p<O.05)
i - 0 . . . . . ST/HR slope=7.2 (r=0.967, p(O.05) O - - - - - - -ST /HR slope=5.65 (r=0.945, p(O.01)
II- ~ ST/HR index=5.65
7'0 9'0 HEART RATE
(bpm)
11o
segment depression and heart rate is generally linear near peak exercise in patients with coronary disease (10-16). The true linearity of this relation is strikingly evident on examination of exercise ECG data from which ST segment/heart rate slopes were calculated in our own laboratory (31,33). Analysis of findings from 100 consecutive patients with coronary artery disease reveals a mean correlation coefficient for the end- exercise linear relation between ST depression and heart rate of 0.97 + 0.04 (mean _+ SD), with a mean of only 4 +_ 1 data points required for statistically significant regression. As a consequence, heart rate changes during exercise, as a measure of changing oxygen demand, can be used to adjust evolving ST depression for variable exercise work load to provide a more accurate measure of the extent of underlying coronary obstruc- tion.
Two related but distinct methods of heart rate adjustment of the magnitude of ST segment depression occurring during exercise have evolved: the linear regression-based ST segment/ heart rate slope and the simpler ST segment/heart rate index. The ST segment/heart rate slope is calculated from the maxi- mal rate of change of ST depression relative to heart rate during the period of active ischemia that accompanies end- exercise. The ST segment/heart rate index represents the average change of ST depression relative to heart rate change over the entire course of exercise, which therefore underesti- mates the maximal ST segment/heart rate slope because it includes a large change in heart rate before any ischemia occurs. Both of these methods specifically do not consider any ST segment depression that occurs during the postexercise recovery period (10,11,31,37,39).
Regression-based ST segment/heart rate slope calculation. Accurate measurement of the ST segment/heart rate slope is determined by linear regression analysis to relate the measured amount of ST segment depression in each lead to the heart rate at the end of each stage of exercise and at peak exercise
(10-12,31-33,37,40). Because the maximal rather than the average rate of change is sought, linear regression analysis is performed from the end of exercise to progressively earlier intermediate stage data using heart rate as the independent variable and ST depression as the dependent variable. The highest ST segment/heart rate slope with a statistically signif- icant correlation coefficient is taken as the test finding for that lead (in/xV/beat per min), as illustrated in Figure 1. After calculation of the maximal ST segment/heart rate slope in each lead, the highest ST segment/heart rate slope with a statisti- cally significant correlation coefficient among all the leads (including bipolar CM 5 but excluding aVR, aVL and V1) is taken as the final test result (10-12,31-33,37,40).
Although a major goal of exercise electrocardiography is improved sensitivity for coronary disease, new tests must also perform with high specificity in general populations. Accord- ingly, an ST segment/heart rate slope partition of 2.4/zVfoeat per min with 95% specificity in clinically normal subjects correctly identified 90% of patients with nonanginal chest pain and a predictably lower 72% of patients with normal coronary arteries at catheterization (37). This criterion for identification of coronary disease was found to have a sensitivity of 95% in our first series of patients at catheterization and also 95% in patients with stable angina, compared with only 68% for standard criteria in these same subgroups (37).
For assessment of the severity of coronary obstruction, perhaps for evaluation of potentially high risk symptomatic patients for coronary angiography, high test sensitivity is a more critically important feature of test performance than is high specificity. An ST segment/heart rate slope partition of 6.0/xV/beat per min, observed in early studies (10-12,27) to be at the upper range of values in patients with two-vessel disease was found to identify 93% of patients with three-vessel or left main coronary artery disease, with a specificity of 57% (34),

1728 OKIN AND KLIGFIELD JACC Vol. 25, No. 7 HEART RATE ADJUSTMENT OF ST SEGMENT DEPRESSION June 1995:1726-35
thus providing a usefully sensitive, if imperfect, marker for extensive obstruction in this important subgroup.
SimpLe ST/HR index calculation. This simplification of the ST segment/heart rate slope method, which evolved from separate observations by Detrano et al. (20), is derived by dividing the maximal change in ST segment depression during exercise by the total change in heart rate from rest to peak effort (20,33,37,42). An ST segment/heart rate index partition of 1.6 ~V/beat per rain with 95% specificity in clinically normal subjects had a specificity of 88% in patients with nonanginal chest pain but a specificity of only 61% in patients with normal coronary arteries at catheterization (37). The 93% and 88% sensitivity of this partition for identification of coronary disease in our initial series of patients with catheter- ization-proved disease and patients with stable angina (37) was similar to the 95% sensitivity of the ST segment/heart rate slope and significantly greater than the 68% sensitivity of standard criteria in these groups. However, for identification of three-vessel or left main coronary artery disease, an ST segment/ heart rate index partition of 3.3 txV/beat per min, at a specificity of 57% matched to the ST segment/heart rate slope partition, identified anatomically severe disease with a sensi- tivity of only 77%, a value between the 66% sensitivity of a markedly positive standard test and the 93% sensitivity of the ST segment/heart rate slope for this purpose (34). Thus, the simple ST segment/heart rate index appeared to approach the performance of the ST segment/heart rate slope for identification of coronary disease only, not for assessment of its anatomic severity.
Theoretic and Experimental Background for Heart Rate Adjustment of ST
Segment Depression Experimental evidence (62-75) provides a theoretic frame-
work for a model that relates measured ST segment depression to heart rate during exercise (51). According to solid-angle theory (65), the magnitude of ST depression recorded at a surface electrode (AST) can be related to the product of spatial and nonspatial determinants as defined by the following rela- tion:
AST = (D./4~r)(AVm)K, [11
where AST = magnitude of ST segment depression; 12 = solid angle subtending the boundary of the ischemic territory; AV m = difference in transmembrane voltage between the ischemic and adjacent nonischemic regions; and K =- correc- tion term for the differences in intracellular and extracellular conductivity and changes in gap junctional conductance (63- 67). As a consequence, during the transient ischemia associ- ated with exercise, the magnitude of ST depression recorded by a surface electrode will be proportional to the area of ischemic territory subtended by the recording electrode (63- 69) and to the local transmembrane potential difference, which reflects the electrical consequences of the metabolic severity of
ischemia at the level of the myocardial cell (62-67). This relation remains proportional under conditions in which major changes in gap junctional conductance do not occur (63-68).
During exercise the severity of ischemia is directly propor- tional to changes in myocardial oxygen demand (70,71), which in turn can be linearly related to increasing heart rate (AHR) (72-75). As an arithmetic consequence, the ratio AVm/AHR should remain constant when the changing severity of ischemia is equilibrated with changing heart rate (51) and under condi- tions in which changes in conductance are proportional or small:
AST/AHR = (l)/4~r)(c), [21
where c = a new constant of proportionality (51). Thus, during exercise-induced transient subendocardial ischemia due to increased work load, the instantaneous ratio of changing ST segment depression to changing heart rate should be directly proportional to the area of ischemic boundary when the severity of ischemia is steadily related to progressive demand. Further, this ratio should remain independent of the metabolic effects of ischemic severity on transmembrane potential differ- ences across the ischemic boundary. The relations inherent in equation 2 provide a strong theoretic basis for the practical application of heart rate adjustment to analysis of the ST segment response to exercise, whereas equation 1 offers fur- ther insight into the poor performance of traditional exercise test criteria that are based solely on the magnitude and configuration of ST segment depression (1-9,76-78), particu- larly in the presence of limited effort tolerance or beta- adrenoceptor blockade (77-79). Of course, many factors relat- ing to changing coronary flow might alter these relations (80-88).
Clinical Applications of Heart Rate Adjustment
Like standard exercise tolerance test criteria, the ST seg- ment/heart rate slope and ST segment/heart rate index can each be applied to the identification of coronary obstruction and separately to the assessment of the anatomic and func- tional severity of disease (2,3,6,10-12,34,37). Test perfor- mance of each method and the performance of each method relative to standard test criteria will vary with these different major diagnostic purposes of exercise testing, so that the clinical application of the exercise tolerance test must be considered in intertest comparison of these methods (2,6,7).
Exercise testing for identification of coronary artery dis- ease. False positive and false negative responses of the heart rate-adjusted methods are well recognized in selected popu- lations, which require further clarification, but both the ST segment/heart rate slope and the simple ST segment/heart rate index can improve the identification of coronary disease in clinically relevant populations. In addition to early reports from Leeds (10-12), findings from Europe (15,16,26), Japan (21) and several centers in the United States (19,37,41,46,50)

JACC Vol. 25, No. 7 OKIN AND KLIGF1ELD 1729 June 1995:1726--35 HEART RATE ADJUSTMENT OF ST SEGMENT DEPRESSION
Table 1. Summary of Studies of ST Segment/Heart Rate Slope for Identification and Quantification of Coronary Artery Disease in Relation to Test Performance and Methodologic Variables
No. of ST Segment Measurement ST Segment Measurement Method of ST Segment Study* Patients Point (ms) Precision (~V) Measurement
Improved Performance: Identification of Disease
Kardash et al. (12) 60 J + 80 10 Magnifying graticnle Sievanan et al. (26) 156 J + 60 NR Computer average Ameisen et al. (29) 135 J + 70 25 Magnifying graticule Ameisen et al. (30) 113 J + 70 25 Magnifying graticute Okin et al. (42) 130 J + 60 10 Computer average Okin and Kligfield (46) 254 J + 60 10 Computer average
Improved Performance: Quantification of Disease
Okin et al. (27) 50 J + 70 25 Magnifying graticule Okin et al. (34) 128 J + 60 10 Computer average Kligfield et al. (48) 172 J + 60 10 Computer average
Improved Performance: Identification and Quantification of Disease
Elamin et al. (10) 64 J + 80 10 Magnifying graticule Elamin et al. (11) 206 J + 80 10 Magnifying graticule Finkelhor et al. (19) 64 J + 80 NR Computer average Sato et al. (21) 142 J + 60 10 Computer average Kligfield et al. (37) 300 J + 60 10 Computer average
No Significant Improvement in Performance
Quyyumi et aL (53)t 78 J + 80 10 Magnifying graticule Balcon et al. (54)? 49 J + 80 10 Magnifying graticule Thwaites et al. (55) 60 J + 80 10 Magnifying graticule
*Numbers in parentheses are reference numbers, tProbably no improvement; no direct comparison made with standard ST depression criteria. NR = not reported.
have demonstrated greater accuracy of the ST segment/heart rate slope than of standard ST segment depression criteria for the detection of significant coronary obstruction (Table 1). Improved sensitivity of the ST segment/heart rate slope rela- tive to standard ST segment depression criteria has been most evident among population groups in which false negative standard test responses are common, including patients with anatomically modest disease (37) and those with submaximal effort tolerance and parallel submaximal heart rate increases during exercise, a group in which exercise ECGs are frequently considered "nondiagnostic" because of limited effort toler- ance. Additional value of the ST segment/heart rate slope for identification of coronary disease is highlighted by 1) similar test outcomes in patients with and without beta-adrenergic blocking agents (12,48); 2) its ability to accurately detect coronary disease among subjects with upsloping ST depression >1 mm (100/xV) (37) (frequently considered an "equivocal" test response); and 3) the similar performance of this method in men and women (46). Improved accuracy for the detection of coronary disease has also been found for the simple ST segment/heart rate index in most (20,24,25,35,37,42,46) but not all studies (56,57,59,61) (Table 2).
Exercise testing for assessment of disease severity. Unlike the heart rate-adjusted measures for simple identification of coronary disease, the ST segment/heart rate slope and ST segment/heart rate index do not perform comparably with respect to assessment of the anatomic severity of disease, even
when methodologic details are observed. Most studies of the regression-based ST segment/heart rate slope have demon- strated improved accuracy for the detection of three-vessel coronary artery disease (Table 1) (10-12,15,16,19,21,27,34,48). In addition, the ST segment/heart rate slope has been shown to be more accurate than standard criteria for assessment of the anatomic extent of coronary obstruction as alternately defined by high Duke jeopardy scores (34,48) or Gensini scores (19,34,48). Further, as a functional consequence of extensive coronary obstruction, high ST segment/heart rate slopes have been found to correlate with large decreases in left ventricular ejection fraction during exercise radionuclide cineangiography (28). However, the ST segment/heart rate slope has not been found to improve the exercise ECG assessment of disease severity in several studies (53-55) (Table 1), and the simple ST segment/heart rate index does not appear to consistently improve the exercise ECG identification of anatomically ex- tensive disease over standard criteria (Table 3).
Exercise testing for prediction of cardiovascular risk. In a totally nonreferred group of asymptomatic subjects within the Framingham offspring cohort (44), an abnormal ST segment/ heart rate index significantly concentrated the risk of future cardiovascular events. Improved risk stratification with heart rate adjustment was independent of age, gender and multiple additional cardiac risk factors (44), but coronary event risk was not significantly concentrated among subjects with a positive

1730 OKIN AND KLIGFIELD JACC Vol. 25, No. 7 HEART RATE ADJUSTMENT OF ST SEGMENT DEPRESSION June 1995:1726-35
Table 2. Summary of Studies of ST Segment/Heart Rate Index for Identification of Coronary Artery Disease in Relation to Test Performance and Methodologic Variables
No. of ST Segment Measurement ST Segment Measurement Method of ST Segment Study* Patients Point (ms) Precision (~V) Measurement
Improved Performance
Detrano et al. (20) 303 J + 80 10 Magnifying graticule Deckers et al. (22) 189 J + 80 NR Computer average Deckers et al. (23) 345 J + 80 NR Computer average Robert et at. (25) 135 J + 60 NR Computer average Kligfield et al. (37) 300 J + 60 10 Computer average Okin et ak (42) 130 J + 60 10 Computer average Okin and Kligfield (46) 254 J + 60 10 Computer average
No Significant Improvement in Performance
Lachterman et al. (56) 328 J point NR NR Herbert et al. (57) 200 J point NR NR Morise and Duval (59) 420 J + 80 NR Visual estimation
*Numbers in parentheses are reference numbers. NR = not reported.
test result according to standard ST segment depression crite- ria.
Relat ionship of Test Performance to Methodologic Variability
ST segment/heart rate slope and ST segment/heart rate index calculations are performed in our laboratory by a computerized ECG system that measures ST segment depres- sion below the isoelectric baseline to the nearest 10 txV at a point 60 ms after the J point from a 12-lead recording system modified by the addition of bipolar lead CM5 (excluding leads aVR, aVL and V1 from all analyses), with exercise according to the Cornell protocol. These methodologic details are required for test accuracy, but they have also been an important limitation to test application where traditional protocols and measurement procedures are standard practice. Seemingly small variations of these details can have large effects on test outcome. Therefore, the relative performance of standard and heart rate-adjusted criteria among different studies must be
examined in context of the separate effects of methodologic variables that are known to change the performance of exercise test criteria (Table 4).
Effect of ST segment measurement timing. The timing of ST segment depression measurement relative to the J point can have a profound effect on relative test performance of standard and heart rate-adjusted ST depression criteria. Traditionally, ST depression has been measured either at the J point or 60 to 80 ms after the J point (2,7,13,14,17,23, 42,49,56,61). Performance of standard ST depression criteria will vary with the timing of ST segment measurement relative to the J point, but measurements made at 60 ms after the J point have generally outperformed J-point measurements for the identification of coronary disease (13,14,17,23,42,49). Per- formance characteristics of both the ST segment/heart rate slope and ST segment/heart rate index are also optimized when ST segment depression is measured precisely at 60 ms after the J point (42). Use of J-point measurements reduces perfor- mance of heart rate-adjusted criteria to the level of standard test criteria (42). These findings provide a partial, reasonable
Table 3. Summary of Studies of ST Segment/Heart Rate Index for Identification of Anatomically Severe Coronary Artery Disease in Relation to Test Performance and Methodologic Variables
No. of ST Segment Measurement ST Segment Measurement Method of ST Segment Study* Patients Point (ms) Precision (~V) Measurement
Improved Performance
Detrano et al. (20) 303 J + 80 10 Magnifying graticule Watanabe et al. (24) 42 J + 80 10 Magnifying glass
No Significant Improvement in Performance
Okin et al. (34) 128 J + 60 10 Computer average Kligfietd et al. (48) 172 J + 60 10 Computer average Lachterman et al. (56) 328 J point NR NR Herbert et al. (57) 454 J point NR NR Bobbio et al. (60) 2,270 . J + 80 NR NR
*Numbers in parentheses are reference numbers. NR = not reported.

JACC Vol. 25, No. 7 OKIN AND KLIGFIELD 1731 June 1995:1726-35 HEART RATE ADJUSTMENT OF ST SEGMENT DEPRESSION
Table 4. Methodologic Factors Affecting Performance of Heart Rate-Adjusted ST Segment Depression Criteria and Recommended Methodologic Criteria
Recommended Metbodotogic Methodologic Factors Criteria
1. Timing of ST segment depression 1. 60 ms after the J point measurement relative to the J point
2. Precision and accuracy of ST segment measurement
3. Definition of measurement baseline
4. Number and location of electrocardiographic leads
5. Exercise protocol
6. Method of heart rate correction (ST/HR slope vs. ST/HR index)
2. Accurate computer measurement to the nearest 10/xV
3. Measurement of ST segment deviation below the isoelectric baseline
4. Use of standard 12-leads and bipolar lead CMs, with exclusion of leads aVR, aVL and V 1 from all analyses
5. Cornell modification of the Bruce protocol
6. ST/HR slope
ST/HR = ST segment/heart rate.
explanation for reduced accuracy of the ST segment/heart rate index that has been reported when J-point measurements of ST segment depression are used (Table 2) (56,61).
Effects of ST segment measurement precision. In addition to the timing of ST segment measurement, precision of measurement can have a significant effect on the relative performance of standard and heart rate-adjusted ST segment criteria (43). Because heart rate-adjusted criteria are calcu- lated as continuous variables, even small differences in the measured magnitude of ST depression can change test out- come (31,37), particularly when the amount of ST depression is small. In contrast, standard exercise ECG criteria tradition- ally are interpreted as discrete variables, so that precise measurement of ST depression when it is <100/xV (1.0 ram) has no consequence for the routine definition of test outcome (31,37). Because much of the improvement in test sensitivity offered by heart rate-adjusted criteria is found in their ability to accurately identify coronary disease in patients with <100/xV of ST depression (37,42,44), less precise measure- ment or visual underestimation of the magnitude of ST de- pression in these patients would be expected to lower test accuracy. Indeed, it can be shown that use of ST segment measurements less precise than 10/xV can reduce sensitivity of the simple ST segment/heart rate index for detection of coronary artery disease by as much as 10% (43). These findings suggest possible additional methodologic explanation for the reduced relative performance of the ST segment/heart rate index in some studies (Tables 2 and 3).
Effect of lead selection and lead number. Differences in the number and position of ECG leads used can also affect the accuracy of both standard and heart rate-adjusted ST depres- sion criteria (1,38,77). In concordance with these observations, performance of both ST segment/heart rate slope and ST segment/heart rate index for detection of coronary disease has
been found to be reduced when fewer than the standard 12-leads plus lead CM 5 are used, whereas the relative differ- ence in performance between standard and heart rate- adjusted criteria appears to narrow with the use of fewer ECG leads (38). These considerations provide an additional expla- nation for the smaller difference in test accuracy found be- tween the ST segment/heart rate index and standard test criteria when alternative leads are used for heart rate-adjusted analyses (59). Further investigation is required to establish the contribution of specific leads to test performance and the value of lead-specific criteria during exercise testing.
Effect of exercise protocol. Differences in the type of exercise test protocol used can also have a profound effect on accuracy of the ST segment/heart rate slope (31,32,38). Calcu- lation of the ST segment/heart rate slope is highly dependent on small heart rate increments between exercise stages, which ensures detection of the maximal rate of ST segment depres- sion as a function of heart rate that occurs during peak exercise-related ischemia (10,11,31,38). Because the average change in heart rate between stages of the Cornell protocol is 10 beats/min (32), whereas heart rate increments between stages of the Bruce protocol are two to three times larger (38), test accuracy of the ST segment/heart rate slope decreases, and in many instances the ST segment/heart rate slope may not be calculable when patients exercise according to the Bruce protocol (33,38). These factors may in part explain the rela- tively lower test accuracy of the ST segment/heart rate slope in at least one early study (55). Other exercise protocols that produce a graded heart rate response to exercise (89-91) might also allow accurate calculation of the ST segment/heart rate slope, but this must be validated because exercise test performance can vary when different treadmill methods are used (31,32,38).
R e l a t i o n o f Tes t P e r f o r m a n c e to P o p u l a t i o n Se lec t ion
Beyond issues of methodologic variability, population se- lection can have separate and important effects on the relative sensitivity and specificity of exercise ECG criteria (50,92-95). As a consequence, exercise test performance must be related to and adjusted for the populations in which criteria are defined and in whom the test is to be used (50,92-94). It is unlikely that normalization of ST segment depression by heart rate alone should completely eliminate inaccurate exercise test findings in groups characterized by the occurrence of marked repolarization abnormalities that are known to be dispropor- tionate to the presence or extent of coronary obstruction. Thus, because factors other than discrete coronary obstruction, such as exercise-provoked epicardial vasoconstriction (87), as well as valvular and myopathic heart disease, can result in exercise-induced subendocardial ischemia and ST segment depression, false positive ST segment/heart rate slope and ST segment/heart rate index values in the absence of coronary disease are predictable in these patients (29,96).

1732 OKIN AND KLIGFIELD JACC Vol. 25, No. 7 HEART RATE ADJUSTMENT OF ST SEGMENT DEPRESSION June 1995:1726-35
500-
200
ST DEPRESSION
(uv) 100.
Counterclockwise Clockwise Rate-Recovery Loop Rate-Recovery Loop
Coronary Artery Disease Clinical Normal
/ • • - - • Exercise
0I•/ O - - O R . . . . . . y i - • 0 0 \ /
O 1 O0
50 100 150 200 50 100 150 HEART RATE
(bpm)
200
Figure 2. ST segment deviation as a function of heart rate during exercise and recovery, with ST segment depression shown in the upward direction and ST segment elevation shown in the downward direction. Typical rate-recovery loops are shown for a clinically normal subject (right) and a patient with coronary artery disease (left). Despite a greater magnitude of ST segment depression at peak exercise in the clini- cally normal subject, there is a clockwise pattern of ST segment depression relative to heart rate during recov- ery; the patient with coronary disease has the opposite, counterclockwise pattern of recovery, bpm = beats/ min.
Similarly, false negative ST segment/heart rate slope values also are predictable where ST segment depression is minimal or entirely absent with exercise, such as often occurs after recent Q wave myocardial infarction (29,30,97-99). Additional factors that can affect the relative performance of heart rate-adjusted and standard methods are the extent of coronary disease in the study population (37) and the proportion of patients studied while receiving beta-blockers (48). The recog- nition of patients and populations in whom unreliably predic- tive ST segment/heart rate slope and ST segment/heart rate index responses may occur is of importance because incorpo- ration of such patients in evaluation of these methods may lead to biased interpretations of potential test accuracy and may explain some of the early discordant observations of ST segment/heart rate slope usefulness (Table 1).
Heart Rate Adjustment in the Postexercise Recovery Period
Additional applications of heart rate adjustment of ST segment depression can be found in the Hollenberg treadmill exercise score (5,100) and the rate-recovery loop (39,44). Both of these methods incorporate work load or heart rate into an evaluation of the ST segment response to exercise that extends into the postexercise recovery phase. The Hollenberg method has been shown (5) to improve sensitivity of the exercise ECG for detection and quantification of coronary disease and to improve specificity when screening healthy young men (100).
Analysis of the behavior of ST segment depression as a function of heart rate during both exercise and recovery using the rate-recovery loop (39,44) provides additional insight into the value of heart rate adjustment of ST depression. Physio- logic correlates of rate-rec6very loop patterns can be found in earlier observations that compared myocardial ischemia during exercise and recovery (76,101-103). Rate-recovery loops are constructed by plotting ST segment deviation with reference to changing heart rate throughout treadmill exercise and recovery (Fig. 2). Normal subjects typically exhibit a clockwise loop of ST depression as a function of heart rate during exercise and recovery, whereas patients with coronary artery disease most
commonly exhibit a counterclockwise loop of ST depression as a function of heart rate (39). The rate-recovery loop improves sensitivity of the exercise ECG for the detection of coronary artery disease with no loss in specificity compared with that for standard ST segment depression criteria (39). In contrast to standard ST depression criteria and heart rate-adjusted crite- ria that are derived from exercise phase data alone, sensitivity of the rate-recovery loop appears to be relatively independent of the extent of coronary artery disease (39). Alone and in combination with the ST segment/heart rate index, the rate- recovery loop can improve the prediction of future cardiovas- cular risk over that with standard ST depression criteria (44).
Clinical Implications and Future Directions The limitations of exercise electrocardiography require
reevaluation and reconsideration. We suggest that sensitivity and specificity of the exercise tolerance test can be increased in clinically important populations by the ST segment/heart rate slope and ST segment/heart rate index when careful attention is paid to the methodologic criteria that have been found to influence test performance. At the same time, simple demon- stration of imperfection of these methods does not obviate their value within clinically relevant, context-sensitive diagnos- tic strategies. The selected populations in which the heart rate-adjusted methods have been derived and tested to date represent only a segment of the possible clinical populations in which exercise testing can be applied, and it is clear that new test criteria must be developed and test performance examined in the precise population subgroups in which the test will be used (50,92-95). As a consequence, application of these crite- ria requires further evaluation in other important subsets of patients who frequently undergo exercise testing, such as those with atypical angina or nonanginal chest pain syndromes. Additional areas of test applicability that require further clarification include the modulating effects of drugs, circulating hormones and additional forms of noncoronary heart disease on the heart rate-adjusted methods and criteria.

JACC Vol. 25, No. 7 OKIN AND KLIGFIELD 1733 June 1995:1726-35 HEART RATE ADJUSTMENT OF ST SEGMENT DEPRESSION
C o n c l u s i o n s
At present, heart rate-adjusted methods can be useful in evaluating the ST segment response to exercise, and we believe that the ST segment/heart rate slope is a valuable marker for the presence and severity of coronary artery disease. Applied carefully, with use of context-sensitive criteria in clinically relevant populations and attention to important methodologic details, these methods can improve the clinical utility of the exercise ECG in the 6 to 8 million exercise ECGs that are performed annually in the United States.
R e f e r e n c e s
1. Chaitman BR, Bourassa MG, Wagniart P, Corbara F, Ferguson FJ. Improved efficiency of treadmill exercise testing using a multiple lead ECG system and basic hemodynamic exercise response. Circulation 1978;57: 71-9.
2. Goldschlager N, Seizer A, Cohn K. Treadmill stress tests as indicators of the presence and severity of coronary artery disease. Ann Intern Med 1976;85:277-286.
3. Weiner DA, Ryan TJ, McCabe CH, et al. Exercise stress testing correla- tions among history of angina, ST segment response and prevalence of coronary artery disease in the Coronary Artery Surgery Study (CASS). N Engl J Med 1979;301:230-5.
4. Kaplan MA, Harris CN, Aronow WS, Parker DP, Ellestad MH. Inability of the submaximal treadmill exercise test to predict the location of coronary disease. Circulation 1973;47:250-6.
5. Hollenberg M, Budge WR, Wisneski JA, Gertz WE. Treadmill score quantifies electrocardiographic response to exercise and improves test accuracy and reproducibility. Circulation 1980;61:276-85.
6. Sheffield LT. The exercise test in perspective. Circulation 1977;55:681-5. 7. Chaitman BR. The changing role of the exercise electrocardiogram as a
diagnostic and prognostic test for chronic ischemic heart disease. J Am Coil Cardiol 1986;8:1195-210.
8. Borer JS, Bresnike JF, Redwood DR. Limitations of the electrocardio- graphic response to exercise in predicting coronary artery disease. N Engl J Med 1975;293:367-71.
9. Epstein SE. Value and limitations of the electrocardiographic response to exercise in predicting coronary artery disease. Am J Cardiol 1978;42:667- 74.
10. Elamin MS, Mary DASG, Smith DR, Linden ILl. Prediction of severity of coronary artery disease using slope of submaximal ST segment/heart rate relationship. Cardiovasc Res 1980;14:681-91.
11. Elamin MS, Boyle R, Kardash MM, et al. Accurate detection of coronary artery disease by new exercise test. Br Heart J 1982;48:311-20.
12. Kardash M, Boyle R, Elamin MS, Stoker JB, Mary DASG, Linden RJ. Detection of the severity of coronary artery disease by the ST segment/heart rate relationship in patients on beta-blocker therapy. Cardiovasc Res 1982;16:508-15.
13. Simoons ML. Optimal measurements for detection of coronary artery disease by exercise electrocardiography. Comp Biomed Res 1977;10:483- 99.
14. Simoons ML, Hugenholtz PG. Estimation of the probability of exercise- induced ischemia by quantitative ECG analysis. Circulation 1977;56:552- 59.
15. Berenyi I, Hajduczki S, Baszormenyi E. Quantitative evaluation of exercise- induced ST segment depression for estimation of degree of coronary artery disease. Eur Heart J 1984;5:289-94.
16. Hajduczld I, Berenyi I, Enghoff E, Malmberg P, Erikson U. Qualitative and quantitative evaluation of the exercise electrocardiogram in assessing the degree of coronary heart disease. J Electrocardiol 1985;18:55-62.
17. Detry JMR, Robert A, Luwaert ILl, et al. Diagnostic values of computer- ized exercise testing in men without previous myocardial infarction: a multivariate, compartmental and probabilistic approach. Eur Heart J 1985;6:227-38.
18. Haraphongse M, Kappagoda T, Tymchak W, Rossall RE. The value of the sum of ST segment depression in 12 lead electrocardiogram in relation to
change in heart rate during exercise to predict the extent of coronary artery disease. Can J Cardiot 1986;2:64-7.
19. Finkelhor RS, Newhouse KE, Vrobel TR, Miron SD, Bahler RC. The ST segment/heart rate slope as a predictor of coronary artery disease: compar- ison with quantitative thallium imaging and conventional ST segment criteria. Am Heart J 1986;112:296-304.
20. Detrano R, Salcedo E, Passalaqua M, Friis R. Exercise electrocardio- graphic variables: a critical appraisal. J Am Coll Cardiol 1986;8:836-47.
21. Sato I, Keta K, Aihara N, Ohe T, Shimomura K, Hasegawa Y. Improved accuracy of the exercise electrocardiogram in detection of coronary disease and three-vessel coronary disease. Chest 1988;94:737-44.
22. Deckers JW, Rensing BJ, Simoons ML, Roelandt JRTC. Diagnostic merits of exercise testing in females. Eur Heart J 1989;10:543-50.
23. Deckers JW, Rensing B J, Tijssen JG, Vinke RVH, Azar A J, Simoons ML. A comparison of methods of analysing exercise tests for diagnosis of coronary artery disease. Br Heart J 1989;62:438-44.
24. Watanabe M, Yokata M, Miyahara T, et al. Clinical significance of simple heart rate-adjusted ST segment depression in supine leg exercise in the diagnosis of coronary artery disease. Am Heart J 1990;120:1102-10.
25. Robert AR, Melin JA, Detry JMR. Logistic discriminant analysis improves diagnostic accuracy of exercise testing for coronary artery disease in women. Circulation 1991;83:1202-9.
26. Sievanen H, Karhumaki L, Vuori I, Jaakko J. Improved diagnostic perfor- mance of the exercise ECG test by computerized multivariate ST-segment/ heart rate analysis. J Electrocardiol 1991;24:129-43.
27. Okin PM, Kligfield P, Ameisen O, Gotdberg HL, Borer JS. Improved accuracy of the exercise electrocardiogram. Identification of three-vessel coronary disease in stable angina pectoris by analysis of peak heart rate-related changes in ST segments. Am J Cardiol 1985;55:271-6.
28. Kligfield P, Okin PM, Ameisen O, Wallis J, Borer JS. Correlation of the exercise ST/HR slope in stable angina pectoris with anatomic and radio- nuclide cineangiographic findings. Am J Cardiol 1985;56:418-421.
29. Ameisen O, Okin PM, Devereux RB, et al. Predictive value and limitations of the ST/HR slope. Br Heart J 1985;53:547-51.
30. Ameisen O, Kligfield P, Okin PM, Miller DH, Borer JS. Effects of recent and remote infarction on the predictive accuracy of the ST/HR slope. J Am Coil Cardiol 1986;8:267-73.
31. Kligfield P, Okin PM, Ameisen O, Borer JS. Evaluation of coronary artery disease by an improved method of exercise electrocardiography: the ST/HR slope. Am Heart J 1986;112:589-98.
32. Okin PM, Ameisen O, Kligfield P. A modified treadmill exercise protocol for computer-assisted analysis of the ST segment/heart rate slope: methods and reproducibility. J Electrocardiol 1986;19:311-8.
33. Kligfield P, Ameisen 0, Okin P. Relation of the exercise ST/HR slope to simple heart rate adjustment of ST segment depression. J Electrocardiol 1987;20 Suppl:135-40.
34. O/fin PM, Kligfield P, Ameisen O, Goldberg H, Borer JS. Identification of anatomically extensive coronary artery disease by the exercise electrocar- diographic ST segment/heart rate slope. Am Heart J 1988;115:1002-13.
35. Okin PM, Kligfield P, Milner MR, Goldstein SA, Lindsay J Jr. Heart rate adjustment of ST segment depression for reduction of false positive electrocardiographic responses to exercise in asymptomatic men screened for coronary artery disease. Am J Cardiol 1988;62:1043-7.
36. Kligfield P, Okin PM, Stumpf T, Zachman D. Computer-based ST/HR slope calculation on Marquette CASE 12: development and technical considerations. J Etectrocardiol 1988;21 Suppl:S134-8.
37. Kligfield P, Ameisen O, Okin PM. Heart rate adjustment of ST segment depression for improved detection of coronary artery disease. Circulation 1989;79:245-55.
38. Okin PM, Kligfietd P. Effect of exercise protocol and monitored leads on the accuracy of heart rate adjusted indices of ST segment depression for detection of three-vessel coronary artery disease. J Electrocardiol 1989;22: 187-94.
39. Okin PM, Ameisen O, Kligfield P. Recovery phase patterns of ST segment depression in the heart rate domain: identification of coronary artery disease by the rate recovery loop. Circulation 1989;80:533-41.
40. Okin PM, Kligfield P. Computer-based implementation of the ST segment/ heart rate slope. Am J Cardiol 1989;64:926-30.
41. Okin PM, Chen J, Kligfield P. Effect of baseline ST segment elevation on test performance of standard and heart-rate-adjusted ST segment depres- sion criteria. Am Heart J 1990;119:1280-6.

1734 OKIN AND KLIGFIELD JACC Vol. 25, No. 7 HEART RATE ADJUSTMENT OF ST SEGMENT DEPRESSION June 1995:1726 -35
42. Oldn PM, Bergman G, Kligfield P. Effect of ST segment measurement point on performance of standard and heart-rate-adjusted ST segment criteria for the identification of coronary artery disease. Circulation 1991;84:57-66.
43. Okin PM, Kligfield P. Effect of precision of ST segment measurement on identification and quantification of coronary artery disease by the ST/HR index. J Electrocardiol 1991;24 Suppl:62-7.
44. Okin PM, Anderson KM, Levy D, Kligfield P. Heart rate adjustment of exercise-induced ST segment depression: improved risk stratification in the Framingham Offspring Study. Circulation 1991;83:866-74.
45. Okin PM, Bergman G, Kligfield P. Heart rate adjustment of the time- voltage ST segment integral: identification of coronary disease and rela- tionship to standard and heart-rate-adjusted ST segment depression crite- ria. J Am Coil Cardiol 1991;18:1487-92.
46. Okin PM, Kligfield P. Identifying coronary artery disease in women by heart rate adjustment of ST segment depression: improved performance of linear regression over simple averaging method and comparison with standard criteria. Am J Cardiol 1992;69:297-302.
47. Okin PM, Kligfield P. Effect of measurement interval on performance of the ST integral for the identification of three-vessel coronary disease. J Electrocardiol 1992;25 Suppl:35-9.
48. Kligfield P, Okin PM, Goldberg HL. Value and limitations of heart rate adjusted ST segment depression criteria for the identification of anatomi- cally severe coronary obstruction: test performance in relation to method of rate correction, definition of extent of disease, and beta-blockade. Am Heart J 1993;125:1262-8.
49. Okin PM, Bergman G, Kligfield P. Measurement parameters for optimal performance of the ST integral. J Am Coll Cardiol 1993;22:168-74.
50. Okin PM, Kligfield P. Population selection and performance of the exercise electrocardiogram for the identification of coronary artery disease. Am Heart J 1994;127:296-304.
51. Okin PM, Kligfield P. Solid angle theory and heart rate adjustment of ST segment depression for the identification and quantification of coronary artery disease. Am Heart J 1994;127:658-67.
52. Kligfield P, Okin PM. Heart rate adjustment of ST segment depression: is the glass half empty or half full? J Am Coll Cardiol 1992;19:19-20.
53. Quyyumi AA, Raphael MJ, Wright C, Bealing L, Fox KM. Inability of the ST segment/heart rate slope to predict accurately the severity of coronary artery disease. Br Heart J 1984;51:395-8.
54. Balcon R, Brooks N, Layton C. Correlation of heart rate/ST slope and coronary angiographic findings. Br Heart J 1984;52:304-7.
55. Thwaites BC, Quyyumi AA, Raphael MJ, Canepa-Anson R, Fox KM. Comparison of the ST/heart rate slope with the modified Bruce exercise test in the detection of coronary artery disease. Am J Cardiol 1986;57:554-6.
56. Lachterman B, Lehmann KG, Detrano R, Neutel J, Froelicher VF. Comparison of ST segment/heart rate index to standard ST criteria for analysis of exercise electrocardiogram. Circulation 1990;82:44-50.
57. Herbert WG, Dubach P, Lehmann KG, Froelicher VF. Effect of/3-block- ade on the interpretation of the exercise ECG: ST level versus AST/HR index. Am Heart J 1991;122:993-1000.
58. Bobbio M, Detrano R. A lesson from the controversy about heart rate adjustment of ST segment depression. Circulation 1991;84:1410-3.
59. Morise AP, Duval RD. Accuracy of the ST/heart rate index in the diagnosis of coronary artery disease. Am J Cardiol 1992;69:603-6.
60. Bobbio M, Detrano R, Schmid JJ, et al. Exercise-induced ST depression and ST/heart rate index to predict triple-vessel or left main coronary disease: a mulfcenter analysis. J Am Coll Cardiol I992;19:11-8.
61. Rodriguez M, Froning J, Froelicher VF. ST0 or ST60. Am Heart J 1993;126:752-4.
62. Thiry PS, Rosenberg RM, Abbott JA. A mechanism for the electrocardio- gram response to left ventricular hypertrophy and acute ischemia. Circ Res 1975;36:92-104.
63. Holland RP, Brooks H. Precordial and epicardial surface potentials during myocardial ischemia in the pig: a theoretical and experimental analysis. Circ Res 1975;37:471-80.
64. Holland RP, Brooks H. TQ-ST segment mapping: critical review and analysis of current concepts. Am J Cardiol 1977;40:110-29.
65. Holland RP, Arnsdorf MF. Solid angle theory and the electrocardiogram: physiologic and quantitative interpretations. Prog Cardiovasc Dis 1977;19: 431-57.
66. Holland RP, Brooks H. Spatial and nonspatial influences on the TQ-ST
segment deflection of ischemia: theoretical and experimental analysis in the pig. J Clin Invest 1977;60:197-214.
67. Holland RP, Arnsdorf MF. Nonspatial determinants of electrograms in guinea pig ventricle. Am J Physiol 1981;240:C148-60.
68. Maehara K, Kyono H, Kitaoka S, et al. A comparison of ST segment deviation and calculated solid angle during acute regional ischemia in the isolated canine heart at precordial, epicardial and intramyocardial lead surfaces. J Electrocardiol 1986;19:235-46.
69. Mirvis DM, Keller FW, Ideker RE, Zettergren DG, Dowdie RF. Equiva- lent generator properties of acute ischemic lesions in the isolated rabbit heart. Circ Res 1978;42:676-85.
70. Mirvis DM, Ramanathan KB, Wilson JL. Regional blood flow correlates of ST segment depression in tachycardia-induced myocardial ischemia. Circu- lation 1986;73:365-73.
71. Mirvis DM, Ramanathan KB. Alterations in transmural blood flow and body surface ST segment abnormalities produced by ischemia in the circumflex and left anterior descending coronary arterial beds of the dog. Circulation 1987;76:697-704.
72. Holmberg S, Serzysko W, Varnauskas E. Coronary circulation during heavy exercise in control subjects and patients with coronary heart disease. Acta Med Scand 1971;190:465-80.
73. Kitamura K, Jorgensen CR, Gobel FL, Taylor HL, Wang Y. Hemodynamic correlates of myocardial oxygen consumption during upright exercise. J Appl Physiol 1972;32:516-22.
74. Jorgensen CR, Wang K, Wang Y, Gobel FL, Nelson RR, Taylor H. Effect of propanolol on myocardial oxygen consumption and its hemodynamic correlates during upright exercise. Circulation 1973;48:1173-82.
75. Gobel FL, Nordstrom LA, Nelson RR, Jorgensen CR, Wang Y. The rate-pressure product as an index of myocardial oxygen consumption during exercise in patients with angina pectorls. Circulation 1978;57:549-56.
76. Detry JMR, Piette F, Brasseur LA. Hemodynamic determinants of exercise ST segment depression in coronary patients. Circulation 1970;42:593-9.
77. Chaitman BR, Hanson JS. Comparative sensitivity and specificity of exercise electrocardiographic lead systems. Am J Cardiol 1981;47:1335-49.
78. Hlatky MA, Pryor DB, Harrell FE, Califf RM, Mark DB, Rosaf RA. Factors affecting sensitivity and specificity of exercise electrocardiography: multivariable analysis. Am J Med 1984;77:64-71.
79. Bailey IK, Anderson SD, Rozea P J, Bernstein L, Nyberg G, Korner PI. Effect of beta-adrenergic blockade with alprenelol on ST segment depres- sion and circulatory dynamics during exercise in patients with effort angina. Am Heart J 1976;92:416-26.
80. Fox KM. Exercise heart rate/ST segment relation: perfect predictor of coronary disease? Br Heart J 1982;48:309-10.
81. Bache RJ, Schwartz JS. Effect of perfusion pressure distal to a coronary stenosis on transmural myocardial blood flow. Circulation 1982;65:928-35.
82. Horwitz LD, Groves BM, Walsh RA, Sorensen SM, Latson TW. Functional significance of coronary collateral vessels in patients with coronary artery disease. Am Heart J 1982;104:221-5.
83. Kolibash AJ, Bush CA, Wepsic RA, Schroeder DP, Tetalman MR, Lewis RP. Coronary collateral vessels: spectrum of physiologic capabilities with respect to providing rest and stress myocardial perfusion, maintenance of left ventricular function and protection against infarction. Am J Cardiol 1982;50:230-8.
84. Hoffman JIE. Maximal coronary flow and the concept of coronary vascular reserve. Circulation 1984;70:153-9.
85. Schwarz F, Flameng W, Thiedemann KU, Schaper W, Schilpper M. Effect of coronary stenosis and myocardial function, ultrastructure and aortocoro- nary bypass graft hemodynamics. Am J Cardiol 1978;42:193-201.
86. Lipscomb K, Hooten S. Effect of stenotic dimensions and blood flow on the hemodynamic significance of model coronary arterial stenoses. Am J Cardiol 1978;42:781-92.
87. Gordon JB, Ganz P, Nabel EG, et al. Atherosclerosis influences the vasomotor response of epicardial coronary arteries to exercise. J Clin Invest 1989;83:1946-52.
88. Nabel EG, Selwyn AP, Ganz P. Paradoxical narrowing of atherosclerotic coronary arteries induced by increases in heart rate. Circulation 1990;81: 850-9.
89. Balke B, Ware RW. An experimental study of physical fitness of Air Force personnel. U.S. Armed Forces Med J 1959;10:675-88.
90. Nanghton J. Stress electrocardiography. Cardiovasc Clinics 1977;8:127-39.

JACC Vol. 25, No. 7 OKIN AND KLIGFIELD 1735 June 1995:1726-35 HEART RATE ADJUSTMENT OF ST SEGMENT DEPRESSION
91. Tamesis B, Stelken A, Byers S, et al. Comparison of the asymptomatic cardiac ischemic pilot and modified asymptomatic cardiac ischemic pilot versus Bruce and Cornell exercise protocols. Am J Cardio11993;72:715-20.
92. Ransohoff DF, Feinstein AR. Problems of spectrum and bias in evaluating the efficacy of diagnostic tests. N Engl J Med 1978;299:926-30.
93. Philbrick JT, Horowitz RI, Feinstein AR. Methodologic problems of exercise testing for coronary artery disease: groups, analysis and bias. Am J Cardiol 1980;46:807-12.
94. Philbrick JT, Horowitz RI, Feinstein All, Langou RA, Chandler JP. The limited spectrum of patients studied in exercise test research. JAMA 1982;2467-70.
95. Diamond GA. Reverend Bayes' silent majority: an alternative factor affecting sensitivity and specificity of exercise electrocardiography. Am J Cardiol 1986;57:1175-80.
96. Bishop N, Boyle RM, Watson DAW, Stoker JB, Mary DASG. Aortic valve disease and the ST segment/heart rate relationship: a longitudinal study before and after aortic valve replacement. J Electrocardiol 1988;21:31-8.
97. Bishop N, Hart G, Boyle RM, Stoker JB, Smith DR, Mary DASG. Use of the maximal ST/HR slope to estimate myocardial ischemia after recent myocardial infarction. Br Heart J 1987;57:512-20.
98. Castellanet MJ, Greenberg PS, Ellestad MH. Comparison of ST segment changes on exercise testing with angiographic findings in patients with prior myocardial infarction. Am J Cardiol 1978;42:716-23.
99. Adams K, Perry JR, Popio K, Gettes L, Sheps DS. Positive treadmill stress tests post-myocardial infarction in patients with single-vessel coronary disease. Am Heart J 1985;109:215-58.
100. Hollenberg M, Zottnick JM, Go M e t al. Comparison of a quantitative treadmill exercise score with standard electrocardiographic criteria in screening asymptomatic young men for coronary artery disease. N Eng J Med 1985;313:600-6.
101. Parker JO, Chiong MA, West RO, Case RB. Sequential alterations in myocardial lactate metabolism, ST segments and left ventricular function during angina induced by atrial pacing. Circulation 1969;40:113-31.
102. Tomoike H, Franklin D, McKown D, Kemper WS, Guberek M, Ross J Jr. Regional myocardial dysfunction and hemodynamic abnormalities during strenuous exercise in dogs with limited coronary flow. Circ Res 1978;42: 487-96.
103. Homans DC, Sublett E, Dai XZ, Bache RJ. Persistence of regional left ventricular dysfunction after exercise-induced myocardial ischemia. J Clin Invest 1986;77:66-73.