Embed Size (px)
Citation preview

British Heart_Journal, I970, 32, 524-536.
'Primary' pulmonary hypertension,eosinophilia, and filariasis in Ceylon
Ivor Obeyesekere and Neil de SoysaFrom the Department of Cardiology, General Hospital, Colombo, Ceylon
'Primary' pulmonary hypertension, which is rare in western countries, wasfound to be relativelycommon in Ceylon.
The clinical and haemodynamic features were studied. There were two distinct types of thedisease, malignant and benign. Patients with the malignant form of the disease had a rapidlyprogressive illness of short duration and an invariably fatal outcome. Those with the benignformgave a-long history and, in spite of severe pulmonary hypertension, were only slightly disabled.They seemed to tolerate the disease better. An important factor which determined the clinicalcourse of the disease was the patency of theforamen ovale. This appeared to act as a safety valvepermitting a right-to-left shunt in times of stress. The foramen ovale was closed in all patientswith the malignant type. The therapeutic implications of this needfurther study.Many patients with 'primary' pulmonary hypertension had an unusually high eosinophil
count (normal range for Ceylon, o-5oo per cu.mm.). Patients in hospitals often have highercounts ranging from o-Iooo per cu.mm. due to intestinal parasitic infestation. Patients with'primary' pulmonary hypertension were found to have a significantly higher mean eosinophilcount than age-matched, sex-matched controls admitted to the Cardiology Unit with chronicrheumatic heart disease and congenital heart disease. The higher count was not due to intestinalparasitic infestation, and none of the other known causes of a raised eosinophil count werepresent.
Four patients had eosinophil counts over 3,ooo per cu.mm., the range commonly associated withtropicalpulmonary eosinophilia, a disease caused byfilariasis. These patients did not manifest anyof the symptoms of tropical pulmonary eosinophilia. Patients with 'primary' pulmonary hyper-tension were examinedfor evidence offilariasis (clinical, haematological, and serological). Volun-teers from among patients with tropical pulmonary eosinophilia and symptom-free patientspositive for Wuchereria bancrofti microfilaria were similarly tested and also catheterized forevidence of pulmonary hypertension. The results of these investigations and their significance arediscussed. The geographical incidence of 'primary' pulmonary hypertension and filariasis wassimilar.
Filarial worms are known to cause pulmonary hypertension in animals. There is sufficientevidence to suspect that the same may be true in humans. This may explain the high incidence ofthe disease in Ceylon and its unusually high prevalence among men.
'Primary' pulmonary hypertension has been not be homogeneous clinically or patho-defined as a disease of unknown aetiology, logically. We examined the possibility of thewhere the increased pulmonary artery pres- disease being different from that hitherto de-sure occurs in the absence of any recognizable scribed in temperate climates. We wish tolesion in the heart or pulmonary parenchyma. report the high incidence of the disease in
This paper describes the clinical features Ceylon with men and women almost equallyseen in 30 such patients investigated in the affected. An association with eosinophilia wasCardiology Unit, General Hospital, Colombo. examined. The relation of different aetio-In I957, Wade and Ball suggested that 'un- logical agents peculiar to the tropics wasexplained pulmonary hypertension' might studied and in particular filariasis as a causa-Received 2 February 1970. tive agent.
on May 18, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.32.4.524 on 1 July 1970. Dow
nloaded from

'Primary' pulmonary hypertension, eosinophilia, and filariasis in Ceylon 525
Subjects and methodsThe patients included in this study had severepulmonary hypertension as the only significantcardiovascular disorder. In particular, they didnot have congenital left-to-right shunts (intra-cardiac or extracardiac), organic valvular heartdisease, diseases of the left side of the heart whichmight cause pulmonary hypertension, or peri-cardial disease. They were free ofparenchymatouslung disease (such as emphysema, chronic bron-chitis, fibrosis), collagen disease, sarcoid, thoracicdeformities, and hypoventilatory disorders. Alsoexcluded were patients with any suspicion ofthromboembolic pulmonary hypertension causedby recurrent embolism.The main clinical features, serial electrocardio-
grams, phonocardiograms, and chest x-ray filmswere studied. Right heart catheterization was per-formed and selective angiocardiography donewhenever there was a doubt as to the correctdiagnosis.
Various blood tests were carried out: examina-tion for LE cells, and antinuclear factor, bloodpicture studies, anti-streptolysin titres, latexflocculation tests, erythrocyte sedimentation rate,and serum protein levels.The absolute eosinophil counts in patients with
'primary' pulmonary hypertension were com-pared with two unrelated groups of patients alsoadmitted to the Cardiology Unit. The controls,matched for age and sex, were from those sufferingfrom chronic rheumatic heart disease and congeni-tal heart disease. Since the commonest cause of araised eosinophil count in Ceylon is intestinalparasitic infestation, the stools of all three groupswere examined for helminth ova.A past history of filariasis was inquired for, and
clinical and haematological evidence of filarialinfection looked for. Two serological tests forfilarial antibodies, the filarial complement-fixationtest (Danaraj, I957; Danaraj, da Silva, andSchacher, 1957), and the fluorescent antibody testfor filarial antibodies (Jayewardena and Wijaya-ratnam, 1968) were also done on i5 patients. Thefindings were compared with similar tests per-formed on two groups of patients known to havea filarial aetiology: (i) symptom-free patients withmicrofilaria, and (2) patients with tropical pul-monary eosinophilia. The first group consisted ofvolunteers from areas where filariasis is endemic,where thick blood films were collected from thepopulation during house to house visits at night,and examined for W. bancrofti microfilaria andfound to be positive. The second group consisted
TABLE I Age-groups and sex of 30patients suffering from 'primary' pulmonaryhypertension
Sex of Age-group (yr.)patient 0-I0 II-20 21-30 31-40 4I-50 50
Female(i8) o 5 9 2 I IMale ( I2) I I 4 5 I 0Total I 6 13 7 2 I
of those suffering from tropical pulmonary eosini-philia attending the General Hospital, Colombo,complaining of cough and wheezing, especially atnight, with an absolute eosinophil count over3,000 per cu.mm. These two groups of controlpatients were catheterized, at which time bloodsamples were withdrawn from the pulmonaryartery and examined for microfilariae, and thepulmonary artery pressures were measured.
ResultsIncidence The incidence of 'primary' pul-monary hypertension in a consecutive seriesof iooo patients with cardiovascular diseasesof all types studied in the Cardiology Unit,General Hospital, Colombo, was 3.7 per cent(37 patients). The first 30 patients providethe material for this paper.
Age and sex distribution (Table I) Therewere i8 female and I2 male patients, giving asex ratio of 15: I. Their ages ranged from 9to 6I; 26 were between ii and 40 years.Three women were married, and 2 hadchildren.
Clinical features The clinical data aresummarized in Appendix II.There were two distinct types of the
disease, malignant and benign.
Malignant typeEight patients suffered from a malignant formof the disease, the illness being of short dura-tion, less than I year, rapidly progressive, re-sistant to treatment, and the outcome usuallyfatal. They were severely disabled; many de-veloped sinus tachycardia, intractable rightheart failure, and tricuspid incompetence.Seven patients died within 3 months of beingfirst examined.
Benign typeTwenty-two patients suffered from a morebenign, chronic form of the disease. Theygave a long history varying from ij to 35years. Right heart failure was either absent ormild, and response to treatment was usuallygood. Tricuspid incompetence was present ina few patients. In spite of a considerabledegree of pulmonary hypertension, they wereonly slightly disabled. The disease processappeared to be static or only slowly pro-gressive.
History The symptoms in the two groupswere similar, only more severe, more acute inonset, and more rapidly progressive in themalignant type.The presenting and universal complaint
on May 18, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.32.4.524 on 1 July 1970. Dow
nloaded from

526 Obeyesekere and de Soysa
was dyspnoea on effort. Effort tolerance waslimited to a varying degree by dyspnoeawhich occurred in all 30, palpitations in 26,undue fatigue in 2I, effort syncope in 20, andangina in I3. Seven patients complained of aconstant praecordial discomfort described as
a 'feeling of suffocation', a 'boring pain', anda 'bursting feeling' present both at rest andon effort, while seated and lying down. Four-teen complained of recurrent cough, and 7 ofpainless haemoptysis. Excessive sweating wasa troublesome symptom. All 8 patients withthe malignant type had severe dyspnoea, un-
due fatigue, effort syncope and angina, and inthe later stages were extremely distressed evenwhen lying still in bed.
There was no past history of leg vein-thrombosis, trauma to lower limbs, or pelvicoperations. Eight patients gave a past historyof undiagnosed febrile illnesses associatedwith severe joint and muscle pain. Two gavehistories of clinical filariasis: funiculitis inCase 17, lymphangitis in Case I5. Three gavehistories of tropical pulmonary eosinophilia.Case i underwent a thorocatomy in I960 forrepair of a suspected atrial septal defect. Atoperation she was found to be suffering from' primary' pulmonary hypertension confirmedby lung biopsy. Case i9 was examined by oneof us (I.O.) in I958 when pulmonary hyper-tension was diagnosed. Case 141 in I964 andCase 22 in I963 were independently investi-gated in different hospitals and diagnosed assuffering from 'primary' pulmonary hyper-tension.The patients ate a well-balanced diet, there
was no incriminating substance which could'have caused the disease, nor was there afamilial history of this disease.
Clinical examination The clinical picturewas dominated by signs of right ventricularhypertrophy and pulmonary hypertension,complicated in some instances by congestivecardiac failure and tricuspid incompetence.In the malignant type right heart failure, tri-cuspid incompetence, and sinus tachycardiawere usually present. Many of the patientswere underweight.
Cyanosis, clubbing of fingers, and mildpolycythaemia were unusual but occurred in afew patients with severe pulmonary hyper-tension as a late manifestation, probably dueto a right-to-left shunt across a patent fora-men ovale. This did not occur in patientswith the malignant type in all of whom the
1 Case 14 was investigated by Professor John Good-win at the Royal Postgraduate Medical School, London.
2 Case 2 was investigated at the ChristianHospital, Vellore, India.
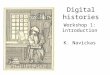
foramen ovale was closed. Cyanosis withoutclubbing occurred in the presence of severeright heart failure and was probably due to awide arteriovenous difference and arterial de-saturation, and disappeared when the failurewas corrected. All patients were in sinusrhythm, the pulse volume usually small. Jugu-lar venous pressure was often strikinglyraised. The systemic blood pressure andpulse pressure were often low. The cardiacimpulse was characterized by a powerful rightventricular heave, maximal between the leftsternal edge and mid-clavicular line. A palp-able lift was present in the right ventricularoutflow tract and closure of the pulmonaryvalve was palpable. The auscultatory signsconfirmed by phonocardiography are sum-marized in Fig. i. Over the pulmonary area: in3 patients there was narrow splitting of thesecond sound with accentuation of the secondcomponent; in I5 there was in addition a sys-tolic click, in 5 this was accompanied by ashort ejection systolic murmur; in 5 therewere both a loud ejection systolic murmur andan early diastolic murmur; finally, in 2 thesigns were overshadowed by a very loud pul-monary diastolic murmur, systole being ex-tremely short with the systolic click buried inthe first sound. Two patients had fixed split-ting of the second sound. Over the tricuspidarea: in I2 there was a prominent right atrialgallop and in 9 a pansystolic murmur of tri-cuspid incompetence.
Course and prognosis There was a re-markable difference in the course and prog-nosis in the two types.
In the benign type, patients gave a longhistory ranging from if to 35 years, and, inspite of severe pulmonary hypertension foundat the time of cardiac catheterization, theywere surprisingly only mildly restricted. Manycontinued to lead useful lives; some were em-ployed. For instance, Case 25 with a pulmon-ary artery pressure of 220/II2 mm.Hg, con-tinues his occupation as a school teacher.Case 24 with a pressure of I20/56 mm.Hgworked as a tractor driver till admission tohospital; Case 6 with a pressure of I20/60mm.Hg works as a stenographer. Thesepatients appear to have come to terms withtheir disease. The only death in this groupfollowed cardiac catheterization.
Eight patients, who belonged to the malig-nant type, gave a short history under oneyear, with rapid progressive deterioration.Seven died within a few months of being firstseen. Deaths were quite sudden, possibly as aresult of an arrhythmia, either atrial fibrilla-tion or an atrioventricular conduction defect.
on May 18, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.32.4.524 on 1 July 1970. Dow
nloaded from

'Primary' pulmonary hypertension, eosinophilia, and filariasis in Ceylon 527
TABLE 2 Electrocardiographic data in 30patients suffering from 'primary' pulmonaryhypertension
No. of Perpatients cent
Sinus rhythm 30 IOOElectrical axis
90- IO I 5 50Over I IO 15 50
Right atrial enlargement(p over 2-5 mm.) 17 56.6
Right ventricular hypertrophyGrade I I 3-3Grade II 5 I6-6Grade III I5 50Grade IV 7 23.3
Complete right bundle-branch block 2 6-6
The surviving patient continues to be very illwith sinus tachycardia, gross tricuspid in-competence, and right heart failure. Allpatients with 'primary' pulmonary hyper-tension reacted badly to chest infections, andbecame very breathless and cyanosed duringthese episodes. They are poor surgical risksand tolerate cardiac catheterization poorly.
Electrocardiograms The electrocardio-grams were abnormal in all patients, and aredescribed in Table 2.They were all in sinus rhythm, with an
electrical axis over go degrees; 56-6 per centhad right atrial enlargement. Varying degreesof right ventricular hypertrophy or completeright bundle-branch block were present inall. In Table 2 right ventricular hypertrophywas graded according to Hollister and Good-win (I963).
Radiology of the heart Radiological stud-ies were carried out in each patient and con-sisted of postero-anterior chest films withcardiac screening. The aorta was small, therewas considerable dilatation of the pulmonaryartery and main branches, with pruning ofthe peripheral vessels. There was variableenlargement of the right ventricle and rightatrium; the left ventricle and left atrium weresmall. The peripheral lung fields were un-remarkable. The average cardiothoracic ratiowas o059 (range 0o46-o93). At fluoroscopyhilar pulsation was conspicuously absent andconfirmed the absence of any left atrial en-largement. Cine-angiocardiograms were madein 9 patients. This procedure carried the riskof inducing collapse and ventricular stand-still. It was, therefore, performed only wherean atrial septal defect or other congenitalanomaly was suspected. Angiocardiographyconfirmed the absence of any shunts from theright chambers of the heart and excluded per-
PULMONARY AREASTAGE I
I7-
narrowly split second soundsecond component louderthan first
also, ejection click
also, short ejection murmur
I ~~~~2I1 C 2 .2 second sound split, longer
IV lii[ Iejection systolic murmur,U [jiil~II111.1 0 fiiiii ...l early diastolic murmur
I lwllilllllllllll1211 shortened- systoleIllliiiiiiiprolonged early diastoliclilI.. murmur
TRICUSPID AREASTAGE 1 2
U _ _ UI0normal1 ~~~~2,
sound
prominent fourth heart
IsIn7stolic murmur,
1 2
|[IV [ 1 ,also, short mid-diastolicut111 ii i I.IiiIIIiiIbli..murmur
0 heart sound 1111111 heart murmur click
FIG. I Summarizes the auscultatory signswhich were confirmed by phonocardiography.
sistent ductus arteriosus, atrial septal defect,or ventricular septal defect with reversed flow.The main and larger pulmonary arteries weregrossly dilated and clubbed with abruptnarrowing of the peripheral vessels.
Cardiac catheterization Patients withsevere pulmonary hypertension are bad risksfor cardiac catheterization. The signs of im-pending danger are sudden sinus bradycardia,AV dissociation or nodal rhythm, conspicuousdrop in venous saturation below (50%), andsudden hypotension. Immediate inhalation of
on May 18, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.32.4.524 on 1 July 1970. Dow
nloaded from

528 Obeyesekere and ds Soysa
ioo per cent oxygen and intracardiac atro-pine, or small doses of isoprenaline via a car-diac catheter, already in situ, averted certaindeath in 4 patients.The catheter data obtained from individual
patients are given in Appendix I. In summary,there were no shunts at any level and nosignificant gradients across the pulmonaryvalve. The pulmonary systolic blood pressureand the right ventricular pressures wereraised; over I00mm.Hg in 2I, and between 8oand I00 mm.Hg in 8. The pulmonary capillarywedge or left atrial pressures were normal.The right atrial pressures were raised. The leftatrium was entered through a patent foramenovale in I2 patients suffering from the benigntype ofthe disease. In no instance ofthe malig-nant type was the septum crossed. The arterialoxygen saturation was low: average 89 percent (range 79-97%). The venous oxygensaturation was often abnormally low, with anincreased AV oxygen difference which aver-aged 29 per cent (range II-44%).
Cardiac output averaged 3.7 l./min. (range2.I-5) in 25 patients. Pulmonary vascularresistance (normal I-2*5 units) was extremelyhigh, and averaged 20-4 units (range I3-44)in 23 patients.A conspicuous feature was the severity of
the pulmonary hypertension which was severein every patient (over 80 mm.Hg). Tenpatients had pulmonary artery pressures at orabove normal systemic artery levels (systolicpressure, 120 mm.Hg). One patient (Case 25)had the extremely high pressure of 220/112mm.Hg.
Blood studiesThe average haemoglobin level was I3'Ig./Ioo ml. (range 9-I-I7'5). Seven patientswere mildly polycythaemic, with haemo-globin levels over I4-6 g./ioo ml.The erythrocyte sedimentation rate, done in
all 30, was normal in 26. In 4 it was slightlyraised with readings in the first hour betweenI0 and 20. The plasma proteins were normalin all, total serum protein averaged 7-6g./Ioo ml. (range 6s5-9go); serum albumin,mean 4.39 g./I00 ml. (range 3-5-5-I); serumglobulin, mean 3.4 g./I00 ml. (range 2-I-4-I).
Blood for antinuclear factor was negative inthe I0 patients examined. Anti-streptolysintitre was within normal limits in I0 patientsexamined, and the latex flocculation testnegative in 8. The mean serum cholesterol inI0 patients was 20I mg./ioo ml. (range i66-250). There was no evidence of any blooddyscrasia in the blood-picture studies. Manypatients showed an increase in mature esoino-phils. Absolute eosinophil counts were, there-
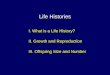
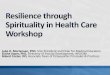
FIG. 2 Map of Ceylon, showing endemicareas for filariasis.
fore, done in all these patients, and comparedwith similar counts obtained from patients ofthe same age and sex suffering from chronicrheumatic heart disease and congenital heartdisease, the latter serving as controls.
Absolute eosinophil counts (Table 3).The normal range for Ceylonese patients is0-500 per cu.mm.; over 3,000 is considered toindicate tropical pulmonary eosinophilia. Thepatients with 'primary' pulmonary hyper-tension and the control groups were thereforegrouped under o-5oo, 50I-3,000, and over
3,000/cu. mm.The mean eosinophil count of the patients
was 1,689 per cu.mm. (range II8-9,898). Themean for controls with chronic rheumaticheart disease was 659/cu. mm. (range 0-2432),and for congenital heart disease 564/cu. mm.(range 62-I820). There was a significant
_o° =GENERAL HOSPITAL,COLOMBO(O=ENDEMIC AREAS FOR FILARIASIS* = RESIDENCE OF PATIENT
N
X W i E
on May 18, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.32.4.524 on 1 July 1970. Dow
nloaded from

'Primary' pulmonary hypertension, eosinophilia, and filariasis in Ceylon 529
difference between the means of 'primary'pulmonary hypertension compared withchronic rheumatic heart disease (p=0025-o-oi) and congenital heart disease (p=OOI-ooos). There was no significant differencebetween the means of chronic rheumaticheart disease and congenital heart disease.
Examination of stools Since the com-
monest cause of a high eosinophil count inCeylon is intestinal helminth infestation, thestools of patients and both control groupswere examined to determine the cause for theconspicuous difference in the eosinophilcounts. There was no significant difference.If anything the patients with 'primary' pul-monary hypertension had less severe infesta-tion than the controls.
Tests for filariasis The patients were
examined for evidence of filarial infection.Simultaneously the same tests were carriedout on two control groups of patients: (a)those with symptom-free microfilaria, and (b)those suffering from tropical pulmonaryeosinophilia. The haemoglobin percentages,erythrocyte sedimentation rates, and pul-monary artery pressures were also compared(Appendix III).A careful search was made for microfilaria
in the blood using thick films made fromfinger blood collected both during the day andnight, venous blood collected during the dayand night, and pulmonary artery blood col-lected during cardiac catheterization. Theywere negative in all patients with 'primary'pulmonary hypertension and tropical pulmon-ary eosinophilia, and positive in patients withsymptom-free microfilaria.The filaria complement-fixation test
(FCFT) was positive in 9 out of If patients(60%) with 'primary' pulmonary hyper-tension, 8 out of 8 (ioo%) with tropical pul-monary eosinophilia, and i out of 8 (I2'5%)with symptom-free microfilaria. The fluores-cent antibody test (FAT) was positive in 3 outof I5 patients (20%) with 'primary' pulmon-ary hypertension, 3 out of 6 (50%) withtropical pulmonary eosinophilia, and in none
of 8 (o%) with symptom-free microfilaria.Either FCFT or FAT was positive in i2
out of i5 (8o%) patients with 'primary' pul-monary hypertension; both tests were positivein one.The pulmonary artery pressures were nor-
mal in patients with tropical pulmonaryeosinophilia and symptom-free microfflaria.
Epidemiology Parasitological investiga-tions which have been carried out in Ceylonsince I947 have revealed that W. bancrofti
TABLE 3 Absolute eosinophil count andstool examination
Disease Absolute eosinophil count Stool examination<500 500-3000 > 3000 HW ova RW ova Whipworm
ova
'Primary' pulmonaryhypertension 7 I9 4 4 I 5
Chronic rheumaticheart disease i6 I4 0 4 6 4
Congenitalheart disease i8 I2 0 4 8 2
Two infestations were present in 3 patients with 'primary' pulmonary hypertension;3 patients with chronic rheumatic heart disease; and 4 patients with congenitalheart disease.
Mean Standard error No. of patients
'Primary' pulmonary hypertension I689 399 0 30Chronic rheumatic heart disease 659 99-0 30Congenital heart disease 564 86-4 30
Comparison of means of 'primary' pulmonary hypertension with chronic rheumaticheart disease shows a significant difference (p= 25-oI).Comparison of means of 'primary' pulmonary hypertension with congenital heartdisease shows a significant difference (p=O-OI0-005).There is no significant difference between the means of chronic rheumatic heartdisease and congestive heart disease.
infection is endemic along the South Westerncoastal border of the island, and pockets occurin some inland towns (Fig. 2). All 30 patientswith 'primary' pulmonary hypertension livedor had lived in these endemic areas.
Pathology Two necropsies were performed:on Case 2, a woman aged 30, who died duringcardiac catheterization, and on Case 23, a managed 2I, who died suddenly in hospital. Case23 had a strongly positive filaria complement-fixation test (titre i in i6o).
Case 2Heart weighed 450 g. and there was considerablehypertrophy of the right ventricle, with dilatationof the right atrium. The thickness of the walls ofthe four chambers of the heart was as follows:right atrium 4.5 mm., right ventricle 12 mm., leftatrium 2 mm., left ventricle IO mm. The papillarymuscles of the right ventricle were grossly hyper-trophied. There were no septal defects; the fora-men ovale was not patent, the pulmonary valveorifice (circumference 8-5 cm.), and the tricuspidvalve ring (circumference II 2 cm.) were dilated.Lung sections showed thickening of the arterieswith much intimal proliferation, narrowing, andocclusion of the lumen. Lung parenchyma showednormal histology. Pulmonary artery sectionshowed changes of atherosclerosis.
Case 23Heart weighed 390 g. and there was hypertrophyof the right ventricle. Thickness of the walls of
on May 18, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.32.4.524 on 1 July 1970. Dow
nloaded from

530 Obeyesekere and de Soysa
the four chambers was as follows: right atrium Woske, I960). Wood (I959) suggested that it3 mm., right ventricle I0 mm., left atrium 2 mm., was due to vascular spasm confined to theleft ventricle 8 mm. The right atrium was dilated, pulmonary vasculature, but did not specifyand the papillary muscles of the right ventricle the cause of the vasoconstriction.were prominent. There were no septal defects and While there is controversy as to thenatureno patent foramen ovale. The pulmonary valve Whilethere isecntovrs as to thatring was dilated, and the pulmonary artery and its and cause of the disease, it seems certain thatmain branches were prominent. There was an pulonary hypertension need not always beenlarged mediastinal lymph node, and the hilar the result of the same factors. There may belymph nodes were prominent. Normal architec- several varieties of the disease prevalent inture was maintained in the lymph nodes which different parts of the world. There are severalshowed some areas of diffuse infiltration with features that suggest that the disease seen ineosinophils, but no filarial worms were seen. Lung Ceylon may be a separate disease entity withhistology revealed pulmonary oedema with scat- a different aetiology and pathogenesis.tered eosinophils, patchy fibrosis, and thickening The recent progress in cardiac catheteriza-of septa, with mononuclears, plasma cells, and tion in Ceylon has shown that 'primary' pul-clumps of eosinophils in the septa in some areas. monam Ceyl on has ath higher inc-A glomus-like structure was seen in the septum of monary hypertension has a much higher inCi-the right lung. There was atherosclerosis of the dence here than in other parts of the world. Inpulmonary arteries, and some of the pulmonary the past 4 years, 37 patients were diagnosedveins showed thrombi. in the Cardiology Unit in a consecutive series
of I000 patients investigated with cardio-Treatment vascular disease of all types, an incidence ofThe patients were treated symptomatically. 37 per cent. Wood (I956) collected only 17Antibiotics, bronchodilators (aminophylline), instances in almost I0 years in a series of
and oxygen inhalation were used in the io,ooo cases, an incidence of only O-I7%. Ap encd of chest infection. Many the striking feature in the present series was thepresence wit lon. any patients large number of male patients affected.were treated with long-term anticoagulant Hitherto, the disease has been described pre-therapy in case there was an underlying dominantly in female patients, with a female-thromboembolic process which was not de-tomlraiOf4I(hpedta.I97tectable clinically. In view of eosinophilia and to-male ratio of 4:1 (Shepherd et al", 1957;a possible filarial aetiology, patients with high Short,, and Bedford, i957). In the presenteosinophil counts (over 2000) were given series the female-to-male ratio was I n5:I.courses of diethyl carbamazine orally. There The clinical picture was remarkable for thewas a rapid fall in the eosinophil count but no severity of the pulmonary hypertension. Ofsignificant clinical improvement. 2eetLfteploayhpreso.O
cliic29 patients- catheterized, 2I had pulmonary
systolic pressures of ioo mm.Hg and over, andDiscussion I2 had pressures of I20 and over. In Wood'sThe cause of 'primary' pulmonary hyper- series (1956) there was only one instance of atension is by definition unknown. Among the pressure over I00. Another striking featuremany theories suggested were 'congenital noticed in this series and not previously re-abnormal broncho-pulmonary anastomoses' ported was the presence of two clinical types,(Brinton, 1950), persistence of the foetal vas- benign and malignant. In the benign typecular pattern in the lung (Civin and Edwards, there was an insidious onset, a long history of1950), an overactive autonomic nervous sys- disability, with gradual progression of thetem (Dresdale, Schultz, and Michtom, I951), disease, and a low mortality. In the malignantand recurrent, minute, symptomless pulmon- type, the history was short, there was rapidary embolism (Wilcken, MacKenzie, and progressive deterioration, no response to con-Goodwin, I960; Goodwin, Harrison, and ventional therapy, and death occurred in aWilcken, I963). Recent histological studies of few months, often quite suddenly. The causethe pulmonary vessels support the view that of this striking difference may be due to thein the majority of cases, pulmonary hyper- patency of the foramen ovale in the benigntension is acquired (Heath and Edwards type, which permitted shunting of blood fromI960). A familial variety of the disease has the right to the left side of the heart when thebeen described (Dresdale, Michtom, and right side was overburdened. The foramenSchultz, I954), an association between pul- ovale was closed in all patients with the malig-monary hypertension, Raynaud's pheno- nant type, and in no instance was the septummenon, and rheumatoid arthritis, implying crossed during catheterization. By contrastthat the disease may be due to a generalized many patients suffering from the benign typecollagen disease rather than to a local vascular were found to have a patent foramen ovale.disease confined to the lungs (Rawson and The presence of a patent foramen ovale
on May 18, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.32.4.524 on 1 July 1970. Dow
nloaded from

'Primary' pulmonary hypertension, eosinophilia, andfilariasis in Ceylon 531
which permits filling of the left heart and actsas a safety valve for the right ventricle(though at the expense of central cyanosis)helps to prolong life. This obviously hastherapeutic implications and needs furtherinvestigation.An association between 'primary' pulmon-
ary hypertension and eosinophilia has beenshown. The normal eosinophil count inCeylon is regarded as o to 500 per cu. mm.However, in hospital practice counts of upto i,ooo are not uncommon and are oftencaused by intestinal parasites. It was for thisreason that the 2 control groups of patientsadmitted to the same unit and matched forage and sex were chosen (those with chronicrheumatic heart disease and congenital heartdisease). Patients with 'primary' pulmonaryhypertension had a significantly higher countwhich could not be accounted for by differ-ences in severity or prevalence of intestinalparasitic infestation. None ofthe known causesof a raised eosinophil count was present:allergic conditions, infections such as chorea,erythema multiforme, and leprosy, skin dis-eases, diseases of the haemopoietic system,such as leukaemia, pernicious anaemia, andpolycythaemia vera, fungal diseases, Hodg-kin's disease, sarcoidosis, carcinoma, ulcera-tive colitis, drug sensitivity, visceral larvamigrans, Loeffler's syndrome, polyarteritisnodosa, and tropical pulmonary eosinophilia.Even though 4 patients had eosinophil countsover 3,000 per cu.mm. and therefore fulfilledone of the criteria of tropical pulmonaryeosinophilia, they did not have any respira-tory symptoms such as a paroxysmal cough orbronchial asthma, a raised ESR, or radio-logical mottling in the lungs.
It has been established that tropical pul-monary eosinophilia is caused by filariasis. InI960, Webb, Job, and Gault showed micro-filariae in the lung, liver, and lymph nodes of apatient suffering from the disease. In I966,Danaraj et al. showed degenerating micro-filariae in eosinophilic granulomata in thelungs of these patients. He postulated thatadult worms were probably alive and pro-duced microfilariae which on reaching thelung were destroyed in an intense tissuereaction, producing the pulmonary symptomsand x-ray appearances characteristic of thedisease; the hypereosinophilia, high level ofcomplement-fixing antibodies to filaria pro-tein, and the raised ESR being part of animmune hypersensitivity reaction, due to anabnormal host parasite relationship. In symp-tom-free filariasis, when the parasites and hostare well adapted, there does not appear to bemuch tissue response as was shown by the low8
titres and poor antibody response, often withnegative complement-fixation tests, absenceof hypereosinophilia, and often normalerythrocyte sedimentation rates.
In patients with 'primary' pulmonaryhypertension no microfilariae were found inthe blood nor were they seen in the lungs inthe two necropsies carried out. However,in one patient (Case 23) who had a stronglypositive filaria complement-fixation test (titrei/i6o), there were scattered areas of eosino-philic infiltration in the lungs and a diffuseeosinophilic infiltration in a mediastinallymph node. As these patients are poorsurgical risks, thoracotomy and lung biopsycould not justifiably be done. The frequentassociation with eosinophilia and hypereo-sinophilia in 4 patients who did not haveclinical tropical pulmonary eosinophilia, andthe frequent finding of a sensitivity to filarialprotein is highly suspicious, especially sincethe high eosinophilic counts responded totreatment with diethyl carbamazine. All 30patients lived in areas where filariasis wasendemic. Three patients gave a previoushistory of tropical pulmonary eosinophilia andtwo of clinical filariasis. In Ceylon filariasisaffects both sexes alike. If 'primary' pulmon-ary hypertension has a filarial aetiology, thiscould be an explanation for the high incidenceof the disease in male patients in this series. Itis known that during acute phases of filariasis,microfilariae continue to be liberated from theadult worms and find their way into the pul-monary circulation. It is therefore conceivablethat they embolize the pulmonary capillaries,setting into motion pulmonary hypertensionin the same manner that minute pulmonaryemboli consisting of blood clot or tumourparticles do. The low titres obtained in mostof these patients to the filaria complement-fixation test may be due to a long time lag be-tween the process of embolization and the de-velopment of pulmonary hypertension whichin most patients is a relatively slow process.
Filarial worms are known to cause pulmon-ary hypertension in animals. Dissanaike andParamananthan (I96I) described a new filarialworm Brugia (Brugiella) buckleyi found in theright ventricle and pulmonary arteries of theCeylon wild hare (Lepus nigricollis singhala).Electrocardiographic evidence of right ven-tricular hypertrophy was shown, and at nec-ropsy gross hypertrophy and dilatation of theright ventricle with pulmonary infarction inthe lungs (Jayasinghe, Fernando, and Dissa-naike, I964). Similar conditions occur in thedog where the filarial worm D. immitis is re-sponsible (Detweiler, Hubben, and Patterson,I960; Patterson and Luginbuhl, I963). While
on May 18, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.32.4.524 on 1 July 1970. Dow
nloaded from

532 Obeyesekere and de Soysa
Dissanaike and his co-workers make no men-tion of the histological changes that occur inthe pulmonary vessels of the hare, Smith andJones (I957) describe changes in the pulmon-ary vasculature of the dog very similar to thechanges that occur in pulmonary hypertensionin man. There is little doubt that filariasis is acause of pulmonary hypertension in some
animals. There is sufficient evidence to sus-pect that the same may be true in man. Sincefilariasis is endemic in certain areas and sowidespread, it might account for the highincidence of this mysterious disease, 'primary'pulmonary hypertension, in Ceylon, where itis almost as common in the male as in thefemale patient and in whom there is often an
associated eosinophilia.
We are grateful to Dr. Doris Peiris, Dr. C. H.Seneviratne, and Professor Gerald Cooray for theirreports on the post-mortem material, Dr. M.Weerasena for reporting on the cine-angiogramsand screening the patients, Dr. M. M. Ismail forcarrying out the filarial complement-fixation tests,Professor A. S. Dissanaike for examining theblood samples for microfilaria, and Dr. C. Muna-singhe for preparing Fig. 2.We also thank Professor John Goodwin and
Dr Richard Emanuel who very kindly correctedthe script.
ReferencesBrinton, W. D. (1950). Primary pulmonary hyper-
tension. British Heartiournal, 12, 305.Civin, W. H., and Edwards, J. E. (1950). Pathology of
pulmonary vascular tree: I. A comparison of theintrapulmonary arteries in the Eisenmenger com-
plex and in stenosis of ostium infundibuli associatedwith biventricular origin of the aorta. Circulation,2, 545.
Danaraj, T. J. (1957). Tropical pulmonary eosino-philia. British Medical3Journal, 2, i6i.
-, da Silva, L. S., and Schacher, J. F. (1957). Thefilarial complement fixation test in eosinophiliclung. Proceedings of the Alumni Association,Malaya, 30, I09.
-, Pacheco, G., Shanmugaratnam, K., and Beaver,P. C. (I966). The etiology and pathology of eosino-philic lung. American Journal of Tropical Medicineand Hygiene, I5, I83.
Detweiler, D. K., Hubben, K., and Patterson, D. F.(I960). Survey of cardiovascular disease in dogs:preliminary report on the first I,ooo dogs screened.American J'ournal of Veterinary Research, 21, 329.
Dissanaike, A. S., and Paramananthan, D. C. (I96I).On Brugia (Brugiella subgen. nov). buckleyi. n.sp.,
from the heart and blood vessels of the CeylonHare. Journal of Helminthology, 35, 209.
Dresdale, D. T., Michtom, R. J., and Schultz, M.(I954). Recent studies in primary pulmonaryhypertension, including pharmacodynamic obser-vations on pulmonary vascular resistance. Bulletinof the New York Academy of Medicine, 30, I95.
-, Schultz, M., and Michtom, R. J. (I95I). Primarypulmonary hypertension. I. Clinical and hemo-dynamic study. American Journal of Medicine, Ii,686.
Evans, W., Short, D. S., and Bedford, D. E. (I957).Solitary pulmonary hypertension. British Heart7ournal, 19, 93.
Goodwin, J. F., Harrison, C. V., and Wilcken, D. E. L.(I963). Obliterative pulmonary hypertension andthrombo-embolism. British Medical_Journal, I, 70I.
Heath, D., and Edwards, J. E. (I960). Configuration ofelastic tissue of pulmonary trunk in idiopathicpulmonary hypertension. Circulation, 21, 59.
-, Whitaker, W., and Brown, J. W. (1957). Idio-pathic pulmonary hypertension. British HeartJournal, I9, 83.
Hollister, R. M., and Goodwin, J. F. (I963). Theelectrocardiogram in cardiomyopathy. British HeartJournal, 25, 357.
Jayasinghe, J. B., Fernando, S. D. A., and Dissanaike,A. S. (I964). Electrocardiographic evidence ofcardiac hypertrophy in a hare infected with thefilarial worm Brugia (Brugiella) buckleyi. Annals ofTropical Medicine and Parasitology, 58, 328.
Jayewardena, L. G., and Wijayaratnam, Y. (I968).The fluorescent antibody test in the serologicaldiagnosis of the causative organisms of tropicaleosinophilia and filariasis. Journal of Helminthology,42, 57.
Patterson, D. F., and Luginbuhl, H. R. (I963).Clinico-pathologic Conference. Journal of theAmerican Veterinary Medical Association, 143, 6I9.
Rawson, A. J., and Woske, H. M. (I960). A study ofetiologic factors in so-called primary pulmonaryhypertension. Archives of Internal Medicine, 105,233.
Shepherd, J. T., Edwards, J. E., Burchell, H. B.,Swan, H. J. C., and Wood, E. H. (1957). Clinical,physiological, and pathological considerations inpatients with idiopathic pulmonary hypertension.British Heart_Journal, 19, 70.
Smith, H. A., and Jones, T. C. (1957). VeterinaryPathology. Henry Kimpton, London.
Wade, G., and Ball, J. (1957). Unexplained pulmonaryhypertension. Quarterly J'ournal of Medicine, 50,(n.s. 26), 83.
Webb, J. K. B., Job, C. K., and Gault, E. W. (I96o).Tropical eosinophilia; demonstration of micro-filariae in lung, liver, and lymph-nodes. Lancet, I,835.
Wilcken, D. E. L., MacKenzie, K. M., and Goodwin,J. F. (I96o). Anticoagulant treatment of obliterativepulmonary hypertension. Lancet, 2, 78I.
Wood, P. (1956). Diseases of the Heart and Circulation,2nd ed. Eyre and Spottiswoode, London.
- (I959). Pulmonary hypertension. Modern Con-cepts of Cardiovascular Disease, 28, 513.
on May 18, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.32.4.524 on 1 July 1970. Dow
nloaded from

'Primary' pulmonary hypertension, eosinophilia, and filariasis in Ceylon 533
APPENDIX I Haemodynamic data in 29 patients suffering from 'primary' pulmonaryhypertension
Case RA RA Pressures (mm.Hg) Oxygen saturationNo. 'A wave' mean RV PA PA PCW or PV FA or FA PA Hb
mean LA systemic or (g./Ioo ml.)'A wave' BP RV
Cardiac output Pulmonary Foramen(1./min.) vasc. resist. ovale
(units)
I 7 3 I40,0,8 I40/72 82 62 5 2 I00/50 56 -
3 4 0 I52,4,8 I44/48 80 5
4 5 2 I00,0,4 I00/40 56 55 8 4 140,0,12 140/112 92 56 5 I I20,0,4 I20/60 72 2
7 5 2 II2,0,4 II2/60 64 48 10 5 120,0,8 I20/64 78 7
9 II 6 120,0,I6 120/64 74 -I0 I5 8 96,o,8 96/44 60 5II 6 3 II2,0,6 II2/64 68 -I2 12 7 96,O,4 96/44 58 4
I3 15 II 96,8,24 96/44 60 -
I4 I4 9 I00, 5, 8 Not entered 9I5 5 I 120,0,4 I20/60 72 5i6 8 4 85,0,4 88/48 56 -
I7 i6 I2 I12, 6, i6 I00/48 56 8i8 Expired before catheterizationI9 5 3 104,0,4 I04/64 64 -20 I2 8 96,o,8 96/52 60 -
2I 22 14 88, 4, i6 80/40 40 822 5 I 96,0,4 96/40 56 423 Io 5 i68, 8, i6 I68/60 io8 -
24 14 9 I20, 0, 12 I20/56 72 325 I5 9 200,8,i6 220/II2I60 826 I0 3 130,6,08 136/48 8o 027 20 i6 i44, 8, 24 Not entered -28 5 0 128,0 I20/72 88 629 4 0 104,0,8 104/48 72 3
30 4 2 88,0,4 88/40 52 2
6 100/70- 140/1006 i05/80
- I00/70- II0/80- 120/804 96/565 90/70- 104/72- I20/80- ii6/8o- I20/70- I00/80- I20/804 I20/80- II2/80- II0/80
- I20/80- II0/85- II0/805 II2/56
96/803 II2/80- I04/800 I00/70- II0/905 I10/85I IIo/8o2 110/80
82 56 I2-990 52 II 087 7I I2-2
90 62 13-8go 63 15.595 73 I2'482 65 i5.679 46 12.489 57 I5 695 6I I4.392 62 I2-289 52 9.I90 48 I3-086 55 I2-695 77 I2-290 77 14-885 57 I3-8
9I 78 I4.89I 5I I2-89I 48 II*088 44 I0797 67 I2-990 5' I5.I86 65 I7-695 73 10 992 67 13.395 76 I2-290 67 13 99I 78 II.7
4-6 20
3-6 i602 consumptionnot determined3.8 154-8 I95*0 I43-0 2I2-8 283.9 i64.6 I34-0 I72.4 242-I 29
4-002 consumptionnot determined4.3 I3
5*0 I32-8 2I2-I 193.2 I43-1 353-8 I93-6 444-6 174.54-4 202.7 23
02 consumptionnot determined
RA, right atrium; RV, right ventricle; PA, pulmonary artery; LA, left atrium; PCW, pulmonary capillary
wedge; FA, femoral artery; PV, pulmonary vein.
OpenClosedOpen
ClosedOpenClosedOpenOpenClosedClosed
OpenClosedOpenClosedClosedClosed
OpenClosedClosedClosedOpenClosedClosedOpenOpenOpen
on May 18, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.32.4.524 on 1 July 1970. Dow
nloaded from

534 Obeyesekere and de Soysa
APPENDIX I.1 Clinical data in patients with 'primary' pulmonary hypertension
ease No., age (yr.), Duration of Dyspnoea* Palpitation Undue Syncope Angina Haemoptysis Right heart Weight (kg.)and sex illness (yr.) fatigue failuret
I 26 F 8 + + + 0 + 0 0 0 38-I2 30 F 6 + + + + 0 + 0 0 55.83 23 F 5 + + + + + 0 0 0 30.84 23 F 6/I2 +++ + + + + 0 ++ 53.55 I7 F I5 + + 0 0 0 0 + 0 37.76 22 F 2 + + + + + 0 0 + 41.37 34 F 6 + + + + + 0 + 0 + 43'08 15 F 2 ++ + + 0 0 0 0 45.59 22 F 2/1I2 +++ 0 + + + 0 ++ 24.9I0 42 F 2/1I2 + + + + + + + 0 + + 49-9II I7 F 10 + + + 0 + 0 0 0 36.712 28 F 14 + + + 0 0 0 0 + 40.813 24 F 6/1I2 + + + + + + + 0 + + 46.714 6i F 35 + + + + + 0 + 0 35 415 28 F 6/I2 + + 0 0 + 0 + + 54.4i6 22 M 6/I2 + + + + + + + 0 + + 43.517 39 M if + + + 0 + 0 0 + 67.II8 21 M 4/12 + + + + + + + + + + + 47.2I9 I7 M 12 + + + + 0 0 0 0 42.220 33 M I ++ + + 0 0 0 0 38-521 9 M 7 ++ + + 0 0 0 + 24.922 50 M 3 + + + + + + 0 0 39-523 21 M 3/12 + + + + + + + + + 35-824 42 M 5 + + + + + 0 0 0 63.525 23 M II + + 0 0 + 0 0 0 39.926 40 M '4 + + + + + + 0 + 38.I27 38 M I +++ + + + + + ++ 59'028 I5 F I2 + + + 0 0 0 0 0 35.429 32 F 2 + + + + + 0 0 0 38.I30 i6 F 2 ++ + 0 0 + 0 0 36-7
* Dyspnoea on exertion: + mild; + + moderate; + + + severe; + + + + present at rest.t Right heart failure: + mild; + + severe.* Auscultation - pulmonary area: I narrowly split 2nd sound, 2nd component loud; II early ejection systolicclick; III short ejection systolic murmur; IV longer systolic murmur, early diastolic murmur; V prolonged earlydiastolic murmur.
on May 18, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.32.4.524 on 1 July 1970. Dow
nloaded from

'Primary' pulmonary hypertension, eosinophilia, andfilariasis in Ceylon 535
Cyanosis and jugular venous Auscultationt Systemic blood PA or RV Present status classification of pulmonaryclubbing offingers pressure (cm.) Pulm. Tricusp. pressure (mm.Hg) pressure (mm.Hg) hypertension
area area
IV II I20/80II III I30/90IV II 130/80III IV 100/40II II I20/80I I I20/8oIII II 120/90II II 90/70IV III 130/100II III 140/90III I I00/80IV II 130/70II III ioo/80V I I30/I00II I I30/80III IV II0/80III II Iio/8oII IV I00/80IV III I20/8oII II II0/80I II I20/70II II I30/80II II 90/70II I II0/90V I 100/80I II I00/70II IV I10/90II I II0/85II I Iio/8oII I Iio/8o
I40/72 Alive BenignI00150 Dead (died during catheterization) Benign144/48 Alive BenignIOO/40 Dead Malignant140/112 Alive BenignI20/60 Alive Benign112/60 Alive BenignI20/64 Alive BenignI20/64 Alive (severely disabled) Malignant96/44 Dead Malignant112/64 Alive Benign96/44 Alive Benign96/44 Dead MalignantI00, 5, 8 (RV) Alive BenignI20/60 Alive Benign88/4 Dead MaignantI00/48 Alive Benign
Dead MalignantI04/64 Alive Benign96/52 Alive Benign80/40 Alive Benign96/40 Alive BenignI68/60 Dead Maignant120/56 Alive Benign220/II2 Alive BenignI36/48 Alive Benign144,8, 24 Dead Malignant120/72 Alive BenignI05/68 Alive Benign88/40 Alive Benign
++00+0+000+000000000000
++
0
0
0
0
56
406I0686366545853I0668838
13040
on May 18, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.32.4.524 on 1 July 1970. Dow
nloaded from

536 Obeyesekere and de Soysa
APPENDIX III Comparison of absolute eosinophil counts, Hb tests forfilariasis, ESR, and pulmonary artery pressure in patients with (i) 'primary'pulmonary hypertension, (2) tropical pulmonary eosinophilia, and (3) symptom-free filariasis
Case age, and sex, Absolute Hb PA blood Thick film Venous FCFT FAT ESR PA pressureNo., eosinophil (g./Ioo ml.) for for blood for (titre) (ist hr.) (mm.Hg)
count microfilaria microfilaria microfilaria (mm.)
Tropicalpulmonaryeosinophilia
3I 2332 3033 2534 60
135 2936 4737 6
38 i5
F39 46
40 I741 24
Symptom-free 42 17filariasis 43 27
44 30
45 4046 I5
'Primary'pulmonaryhypertension
5 I77 348 I59 22I0 42ll I713 24I4 6i
I5 28'7 3922 5023 21
24 42
25 23
L26 40
F 9638M 20000M I2070M II950M 14280M I09I2F 8554F 57I9
F 1750F 6I2M 3650M 394M 784M I94M 836F 712
F 7I6F I672F 780F 7497F 560F 3483F 9898F 846F ii8M 896M 7I2M 336M Ioo8M ii6oM 688
9-69-6II.7I0-9I2-2II.3
9.510*1IO-I
I0-4II.3II.7I3.9I3.0I2-210-9
I5.5I5.6I2.4I5.6I4.312-2I3.0I2-6I2-2I3.2I0-7I2-9'5.'I7.6I0-9
-ve-ve-ve-ve-ve- ve- ve-ve
+ve- ve+ve+ve+ ve+ve-ve+ve
-ve-ve-ve-ve-ve-ve-ve-ve- ve-ve-ve-ve-ve-ve- ve
-ve-ve-ve-ve-ve-ve-ve-ve
+ve+ve+ve+ve+ve+ve+ve+ve
-ve-ve- ve- ve-ve-ve-ve-ve-ve-ve-ve-ve-ve-ve-ve
-ve-ve-ve-ve- ve-ve-ve-ve
+ ve+ve+ve+ve+ve+ve+ve+ve
-ve-ve- ve-ve-ve-ve-ve- ve-ve-ve-ve-ve-ve-ve-ve
+Iiln4O -ve 22+ I in 40 - ve 6+I in 8o - ve 20+ I in 40 + ve 24+i in i6o - ve 5I+ iin 40 + ve 28+i in 8o + ve 30+I in 40 - ve 64
-ve-ve-ve-ve-ve-ve-ve+ I in 20
- ve 42- ve I3- ve 5- ve 2I- ve 6- ve 3- ve 4- ve 20
+I in 5 - ve I0-ve -ve 5+I in I0 + ve 9+Iin5 -ve I0- ve - ve I9+iin8o -ve I0+i in 8o - ve 4-ve +ve 3-ve -ve -
-ve +ve -
+I in Io - ve 8+i in I60 - ve 4+I in 70 - ve 4+i in io - ve o- ve -ve I4
VA, pulmonary artery; FCFf, filaria complement-uxation test; FAT, fluorescent antibody test.
30/828/1I228/1224/1028/I024/I030/I026/8
20/620/622/826/o32/1022/824/I024/I0
140/II2112/64I20/64120/6496/441I2/6496/44I00/80I20/60I00/4896/40I68/80120/56220/112I36/48
on May 18, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.32.4.524 on 1 July 1970. Dow
nloaded from