Embed Size (px)
Citation preview

British Heart_Journal, I971, 33, 95-I00.
Coronary atherosclerosis in Nigeria
A. Olufemi WilliamsFrom Department of Pathology, University of Ibadan,and University College Hospital, Ibadan, Nigeria
The relative rarity of ischaemic heart disease in the negro is well recognized, but there are veryfew morphological studies on the quantitative or qualitative aspects of the disease. Of 8,ooonecropsies carried out in the University College Hospital, Ibadan, over a io-year period, therewere IO Nigerians with proven myocardial infarcts. Of these, 4 were on the basis of coronaryembolism from endomyocardial fibrosis or bacterial endocarditis. Planimetric assessment ofSudan-stained coronary arteries obtainedfrom 279 heartsfrom consecutive unselected necropsiesof Nigerians over the age of IO years was carried out. Seventy-one per cent had no demonstrableatherosclerotic lesion, while in the remaining 29 per cent, the right coronary artery was slightlymore affected than the left descending or circumflex arteries. The average percentage of intimalsurface involvements of right and left coronary arteries was 23 and 2I, respectively. Fibrousplaques or complicated lesions were infrequent. Coronary thrombi were not seen, but there was a
patient who had left-sided endomyocardial fibrosis with myocardial infarction due to coronaryembolism. The severity of atherosclerosis increased with age. Though fatty streaking was notuncommon, particularly in early life, the factors that appear to protect the African, includingthe Nigerian, from advanced stages of coronary atherosclerosis and ischaemic heart disease arepoorly understood, but factors such as exercise, diet influenced by the socio-economic class, andfibrinolytic activity are probably significant.
The relative rarity of coronary artery diseasein the negro including the Nigerian is wellrecognized and the corresponding rarity ofischaemic heart disease has been very welldocumented (Becker, I946; Davies, I948;Edington, I954; Siew, I958). There are veryfew morphological studies on the quantitativeor qualitative aspects of this disease in theWest African (Goodale et al., I964; Lee et al.,i964), but information about atherosclerosisin the African is only forthcoming from studieson East and South African Bantus who differfrom the West African in their physical andcultural characteristics, dietary habits, andgenetic constitution (Walker and Grusin,I959; Walker, I963; Higginson and Pepler,1I954; Becker, 1946; Scott et al., 196I;Florentin et al., I963; Meyer et al., 1964).The present prospective study primarily
describes the extent, severity, and frequencyof coronary atherosclerosis in the Nigerian,and compares the findings with other popula-tion groups and secondarily describes thefrequency of ischaemic heart disease.The coronary arteries of 279 hearts (I59
Received 5 June 1970.
male, I20 female) were studied from con-secutive necropsies of patients over the age ofI0 years at the University College Hospital,Ibadan, a general teaching hospital of about500 beds. The population served by this hos-pital is partly urban and partly rural, a dis-tinction that is difficult to justify in severalparts of Africa. The majority of the patientswere from the lower socio-economic strata ofthe community and belonged to the Yorubatribe. The necropsy percentage in the hospitalduring the period of study was about 70.
Subjects and methodsAfter careful examination of the coronary ostia forocclusion or other lesions, the right and left coron-ary arteries were dissected off their beds and re-moved with their branches. For this study, theright coronary artery was from its origin (exclud-ing the ostium) to the margin of the posteriorinterventricular septum excluding any branches.The left descending coronary artery included theleft main coronary artery from its origin (exclud-ing the ostium) and the anterior descendingbranch and any of its subepicardial branches con-sidered to be large enough to be opened by bluntpointed iris scissors. The arteries were thenopened longitudinally to expose their intimal
on February 28, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.33.1.95 on 1 January 1971. Dow
nloaded from

96 A. Olufemi Williams
surfaces and the presence of thrombi or embolinoted. They were rinsed in normal saline for Iominutes and then fixed in 4 per cent formaldehydein saline. They were stained with 5 per centSudan IV solution, differentiated in at least 2changes of 8o per cent ethanol, and washed underrunning tap water. For tracing the outlines of thearteries and their lesions, polythene strips usedfor storing pathological specimens were used(Williams, I969). The strips were laid over thearteries, pinned to cork mats, and the tracingsobtained were used for planimetry. For quantita-tion of atherosclerotic lesions, planimetric assess-ment was employed (Cranston et al., I964). Theoutlines of different macroscopical types ofatherosclerotic lesions were traced systematically,each type of lesion being represented by a par-ticular symbol so that it could be distinguished.For this study, three types of macroscopicallesions were recognized, namely, fatty streaks,fibrous plaques, and complicated lesions. Thefatty streak was a flat or slightly raised intimallesion that stained distinctly with Sudan IV anddid not show any other type of change underlyingit. The fibrous plaque was a firm raised intimallesion which in the fresh stage was pale grey,glistening, and translucent. In cases where it waspartially or completely covered by sudanophilicdeposits, the area was graded as a fibrous plaquerather than a fatty streak. Complicated lesionsincluded calcification, haemorrhage, and ulcera-tion. Histological examination was carried out ondoubtful lesions, but these were infrequent. Fortopographic analyses, three major segments of thecoronary arterial system were considered, namelythe main trunk of the left coronary artery and itsanterior descending branch, which is referred toas the left descending coronary artery, the circum-flex branch of the left coronary artery, and theright coronary artery.With a rolling wheel planimeter (Allbrit), the
entire surface areas of the arteries were measured.The surface areas of the different macroscopicallesions were also measured systematically andrecorded as percentages of total intimal surface ofthe respective coronary segment. To reduceerror, all lesions were traversed twice with theplanimeter and the readings halved to give thetrue surface area in cm.2 The total surface areas
having been obtained, the percentage surface in-volvement by the different atherosclerotic lesionsin the segments of the coronary arteries was cal-culated. Several sections were taken from differentareas of the heart and examined histologically,using paraffin-embedded material and stainingroutinely with haematoxylin and eosin. VanGieson's stain was also used when indicated.
Results
The distribution of the 279 subjects, classifiedby age and sex, is shown in Table i. Of the279 patients, 82 (29%) had atheroscleroticlesions while the remaining 97 (7I%) hadno demonstrable lesion. The causes of deathin the 82 patients with coronary atherosclero-
sis are summarized in Table 2. Segmental andtopographic analyses in relation to age arepresented in Tables 3 and 4. The average per-centage of intimal surface involvement inboth sexes is summarized in Table 5. Theaverage percentage surface involvement byfatty streaks and fibrous plaques in relationto age is also presented in Table 6.
TABLE i Age and sex distribution of 279Nigerians with and without atherosclerosis
Age in With Without Totaldecades atherosclerosis atherosclerosis
Male Female Male Female
I1-20 I 4 II I0 262I-30 10 9 2I 2I 6i3I-40 8 9 24 33 744I-50 13 4 23 10 50
5I-60 7 4 I7 8 3661-70 8 2 7 2 I97I-80 I 0 I 0 28i-90 I 0 0 I 2Unknown - I 6 2 9
Total 49 33 ii0 87 279
TABLE 2 Causes of death in 82 Nigerianswith coronary atherosclerosis
Cause of death No. Percent
Heart disease (including hypertension) 22 26.4Malignant diseases I3 i6-iCirrhosis of liver 5 6-iInfection 20 24-5Diabetes 2 2-4Miscellaneous 20 24.5
82 I00
TABLE 3 Involvement of coronary arteriesin relation to age
Age in One segment Two segments All three Totaldecades involved involved segments
involved
LD LC R LD and LC LD LD, LCLC and R and R and R
II-20 I - 2 - I 42I-30 9 I - 3 5 i831-40 6 - 3 I 5 3 i841-50 2 I 3 3 8 175I-60 3 - - I I 7 I26i1-7o 2 I 3 4 97I-80 I - - - - I8-I90 - - - I - I
Total 22 - 7 7 I i6 29 82
LD, left anterior descending branch; LC, left circumflex branch; R, right coronaryartery.
on February 28, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.33.1.95 on 1 January 1971. Dow
nloaded from

Coronary atherosclerosis in Nigeria 97
TABLE 4 Average extent of coronary surfaceinvolvement of atherosclerosis
Age in Per cent Per cent Per centdecades LCA RCA average
I I-20 I7.9 29-6 23.421-30 13.9 I4.4 I4.231-40 I0-9 I3.9 15.54I-50 27I 24.4 25.75i-6o 27-8 39-7 33-76I-70 25.4 37.8 3.6
7I-80 50°5 0 25.38I-90 30-3 7 3 I8-8
LCA, left coronary artery (anterior decendingcircumflex); RCA, right coronary artery.
DiscussionThe method of planimetric assessment ofatherosclerosis was preferred because it hadbeen found that reproducibility of results wasmuch better than visual estimates (Strong andEggen, i965; Williams, I969). Another ad-vantage of planimetry was that it providedrelatively accurate qualitative and quantitativerecords of disease severity, and furthermorethe tracings were permanent and could beused for comparative studies.
In a preliminary study of coronary arteriesin early life in Nigerians, no lesion was ob-served in patients under the age of Io years.This group of patients was therefore excludedfrom the present study. The relative paucityof subjects in the fifth decade upwards wasnot as a result of selection but a reflection ofthe African population structure or hospitaladmissions (Table i). It is noteworthy thatabout one-third and one-half of all thepatients in the fifth and sixth decades, respec-tively, had detectable coronary artery disease(Tables i and 2). This is in keeping with theobservation that atherosclerosis increases withage. The ratio of affected to healthy arteries(I:2-5) iS of interest, as it indicates, though
' crudely, the relative ratio frequency of coron-ary atherosclerosis in this series. This paperconsiders two major classes of mural athero-sclerosis: fatty streaks and raised lesions. The
TABLE 6 Average per cent of intimal surfaceinvolved with fatty streaks and raised lesionsin coronary arteries of 82 Nigerians atnecropsy
Age in Fatty Raiseddecades streaks (%) lesions (%)
I I-20 22-9 021-30 I5.I 0
3I-40 15.3 4.641-50 I7.3 3.55I6o 37-7 o0g6I-70 27.9 4.67I-80 25-2 08I-90 i8-8 0
latter includes fibrous plaques, calcifiedlesions, and lesions complicated by haemor-rhage, ulceration, or thrombosis. Raisedlesions evidently indicate a relatively ad-vanced stage of atherosclerosis. The presentstudy reveals that there is a steep rise in theamount of fatty streaking during the II-20year age-group. This is followed by a fall inthe second, third, and fourth decades, and a
rise in the fifth and sixth decades. There isconsiderable disparity between the amount of
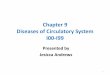
FIG. I Average percentage of intimal surfaceinvolvement of coronary arteries by fattystreaks and raised lesions. Note the disparityin the extent offatty streaks and fibrousplaques.
s40-
30
10u fatty streaks
20,
lu. lo0
10 ~~~~~raised lesions
0 -X-x-.A-x0 10 20 30 40 50 60 70Age in years
bTABLE 5 Average per cent intimal surface involvement in 82 Nigerians with atherosclerosis.of coronary arteries
,Left descending (%) Left circumflex (%) Right (%) Total area involved(%)
Fatty Fibrous Compli- Fatty Fibrous Compli- Fatty Fibrous Compli- Left ant. Rightstreaks plaques cated streaks plaques cated streaks plaques cated desc. and coron.
lesions lesions lesions circumfl. arteryartery
I9-I I.03 III I6-I 0-2 o-6 2I17 I-4 0-3 20-6 23-2
7
on February 28, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.33.1.95 on 1 January 1971. Dow
nloaded from

98 A. Olufemi Williams
60left coronary and
la circumflex arteriesv 50 X0001020u40S06-0 09
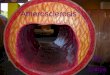
mnofriqht cornarytcroayateisbarteoclry.iinNgras oetesih
~ ~ ~ ~ ~~~
>
increase of involvement of the right coronaryin thefifth and sixth decades.
fatty streaking and raised lesions (Fig. I).Fibrous plaques are not observed in the firsttwo decades of life, and the severity is insig-nificant in later life as the average surfacearea involved is less than 5 per cent of thetotal corona rtery surface (Fig. I). Thisraises the question of the interrelation of fattystreaks and fibrous plaques. When fattystreaks and raised lesions are considered to-gether, the total areas involved in the leftcoronary artery with its circumflex brach
FIG. 3 Average percentage of intimal surfaceinvolvement of aorta and coronary arteries byfatty streaks and raised lesions in both sexes.Note the initial rise of atherosclerosis, mainlyfatty streaks, in early life (525 aortas, 279coronary arteries).
< 4
30 50
0
e sares
and the right coronary artery are 2o06 percent and 23-2 per cent respectively (Table 5).The right coronary artery does not appear to bemore involved with atherosclerosis than the leftexcept in the fifth and sixth decades (Fig. 2),but this is not statistically significant. Therelative paucity of fibrous plaques and com-plicated lesions in all the arteries is highlysignificant as it explains the relatively lowincidence of the complications of coronaryatherosclerosis in the Nigerian (Fig. i).The steep rise of fatty streaks observed in
early life in the coronary arteries has also beenobserved in the aortas of Nigerians (Fig. 3)(Williams, I969), New Orleans Negroes andSouth African Bantus (McGill, I968). Thereis, however, some correlation between therate of fatty deposition in the coronaryarteries and aorta of Nigerians (Fig. 3).The most common single coronary segment
to be involved is the left anterior descendingcoronary artery. It is about three times asfrequently affected as the right coronaryartery. Except in one patient where the leftcircumflex artery is involved in conjunctionwith the right coronary artery (Table 3), it isinvariably involved with the left descendingcoronary artery. In fact, there is not a singleinstance in which the circumflex artery aloneis involved. It is, however, not uncommon forall three segments to be involved as seen inabout one-third of all our patients (Table 3).The causes of death in the 82 patients with
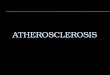
atherosclerotic lesions revealed that about one-quarter of all the patients had cardiac diseasesincluding hypertension. Apart from hyper-tensive cardiomegaly, other cardiac conditionsobserved were rheumatism, bacterial endo-carditis, and endomyocardial fibrosis. Therewas only one case of acute myocardial infarc-tion in the whole series. This was due tocoronary embolism from mural thrombosis ina heart with left ventricular endomyocardialfibrosis (Fig. 4). Of 8,ooo necropsies carriedout in the University College Hospital overa i0-year period, there were io Nigerians withproven myocardial infarcts. Some of thesewere on the bases of endomyocardial fibrosisor infective endocarditis. The present studyconfirms previous observations that coronaryatherosclerosis and coronary heart disease arerelatively rare in the negro or in peoples in-habiting developing countries (Richir andQuenum, I96I; Murthy, Dutta, and Rama-lingaswami, I963; Lee et al., I962; Thomaset al., I960).
In a previous study cerebral atherosclerosiswas found to be less severe in the Nigerianwhen compared with other population groups(Williams, Resch, and Loewenson, I969), and
on February 28, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.33.1.95 on 1 January 1971. Dow
nloaded from

Coronary atherosclerosis in Nigeria gg
) FIG . 4 Heart with left ventricular endomyocardial fibrosis. Note the thickened fibroustissue occupying the apex and outflow tract of the left ventricle. The interventricular septum,which is dark, is the seat of recent infarction. This is due to a coronary embolus. The leftatrial appendage is filled with an antemortem thrombus (arrow). There is also a smallaneurysm at the apex of the left ventricle.
raised lesions in the aorta were also relatively? low in the Nigerian (Williams, I969). It can
therefore be concluded that atherosclerosis ofthe aorta, coronary, and cerebral arteries is
s less severe in the Nigerian than in certainCaucasian groups living in highly developed
"..'and industrialized countries. The relativelyextensive coronary and aortic fatty streaking
win the Nigerian duplicates what has been ob-served in other Negro groups from NewOrleans, Jamaica, Puerto Rico, Sao Paulo,,and Durban (McGill, I968). Furthermore,the tendency to develop a minimal degree ofraised lesions is noteworthy, particularly whenit is compared with non-negro populations. Itappears that the negro, including the Nigerian,
is more susceptible to deposition of lipid inthe arterial intima in early life, but the lipiddoes not predispose to the advanced lesionsof atherosclerosis. The negro populations withextensive coronary lipid deposition are worthyof further studies, as they offer a uniqueopportunity to relate environment, lipidmetabolism, diet, fibrinolytic activity, andother characteristics to the formation of fattystreaks. Failure to convert fatty streaks tofibrous plaques, or the relative paucity offibrous plaques and complicated lesions in theNigerian explains the relative rarity of coron-ary heart disease. This finding also offers anopportunity to elucidate the problem ofcoronary atherosclerosis and ischaemic heart
on February 28, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.33.1.95 on 1 January 1971. Dow
nloaded from

IOO A. Olufemi Williams
disease in general before the community be-comes industrialized and subsequently afflu-ent. If this study is carried out again severalyears after industrialization and the standardof living has improved, it is likely that theseverity and extent of the disease will not beas low as it is now.
The author wishes to thank Messrs. Owolabi andOsotimehin for their technical assistance.
ReferencesBecker, B. J. P. (I946). Cardio-vascular disease in the
Bantu and Coloured races of South Africa. IV.Atheromatosis. South African Journal of MedicalSciences, II, 97.
Cranston, W. I., Mitchell, J. R. A., Russell, R. W. R.,and Schwartz, C. J. (I964). The assessment ofaortic disease. Journal of Atherosclerosis Research,4, 29.
Davies, J. N. P. (I948). Pathology of Central Africannatives. Mulago Hospital post mortem studies. IX.Cardio-vascular diseases. East African MedicalJournal, 25, 454.
Edington, G. M. (I954). Cardiovascular disease ascause of death in the Gold Coast African. Transac-tions of the Royal Society of Tropical Medicine andHygiene, 48, 4I9.
Florentin, R. A., Lee, K. T., Daoud, A. S., Davies,J. N. P., Hall, E. W., and Goodale, F. (I963). Geo-graphic pathology of arteriosclerosis: a study of theage of onset of significant coronary arteriosclerosisin adult Africans and New Yorkers. Experimentaland Molecular Pathology, 2, 103.
Goodale, F., Lee, K. T., Scott, R. F., Edington, G. M.,and Davies, J. N. P. (I964). Geographic pathologyof arteriosclerosis. A study of disease patterns inautopsied individuals from Kampala, Uganda,Ibadan, Nigeria and Albany, New York. Experi-mental and Molecular Pathology, 3, 148.
Higginson, J., and Pepler, W. J. (i954). Fat intake,serum cholesterol concentration, and atherosclero-sis in the South African Bantu. II. Atherosclerosisand coronary artery disease. Journal of ClinicalInvestigation, 33, I366.
Lee, K. T., Daoud, A. S., Jarmolych, J., Jakovik, L.,and Florentin, R. (I964). Geographic pathologyof myocardial infarction. Part 4. Measurement ofamount of coronary arteriosclerosis in Africans,Koreans, Japanese and New Yorkers. AmericanJournal of Cardiology, 13, 30.
-, Shaper, A. G., Scott, R. F., Goodale, F., andThomas, W. A. (1962). Geographic studies per-taining to arteriosclerosis. Archives of Pathology,74, 48I.
McGill, H. C. (I968). Fatty streaks in the coronaryarteries and aorta. Laboratory Investigation, I8,560.
Meyer, B. J., Pepler, W. J., Meyer, A. C., and Theron,J. J. (I964). Atherosclerosis in Europeans andBantu. Circulation, 29, 4I5.
Murthy, M. S. N., Dutta, B. N., and Ramalingaswami,V. (I963). Coronary atherosclerosis in North India(Delhi area). Journal of Pathology and Bacteriology,85, 93.
Richir, C., and Quenum, C. (I96I). Etude morpho-logique des coronaires. Bulletin de la SocieteMedicale d'Afrique Noire de Langue Franfaise, 6,486.
Scott, R. F., Daoud, A. S., Florentin, R. A., Davies,J. N. P., and Coles, R. M. (I96I). Comparison ofthe amount of coronary arteriosclerosis in autopsiedEast Africans and New Yorkers. American Journalof Cardiology, 8, I65.
Siew, S. (I958). Comparative study of the autopsyincidence of cardiovascular disease in the Bantu onthe Witwatersrand. Leech (Johannesburg), 28, 2, 6i.
Strong, J. P., and Eggen, D. A. (I965). Atheroscleroticlesions. In Comparability in International Epi-demiology. Ed. by R. M. Acheson. MilbankMemorial Fund Quarterly, 43, No. 2, pt. 2, p. 57.
Thomas, W. A., Davies, J. N. P., O'Neal, R. M., andDimakulangan, A. A. (I960). Incidence of myo-cardial infarction correlated with venous and pul-monary thrombosis and embolism. A geographicstudy based on autopsies in Uganda, East Africaand St. Louis, U.S.A. American Journal of Cardi-ology, 5, 41.
Walker, A. R. P. (I963). Mortality from coronary heartdisease and from cerebral vascular disease in thedifferent racial populations in South Africa. SouthAfrican Medical Journal, 37, II55.
-, and Grusin, H. (I959). Coronary heart diseaseand cerebral vascular disease in the South AfricanBantu: examination and discussion of crude andage-specific death rates. AmericanJournal ofClinicalNutrition, 7, 264.
Williams, A. 0. (I969). Atherosclerosis in the Nigerian.Journal of Pathology, 99, 2I9.
-, Resch, J. A., and Loewenson, R. B. (I969).Cerebral atherosclerosis - a comparative autopsystudy between Nigerian Negroes and AmericanNegroes and Caucasians. Neurology (Minneapolis),19, 205.
on February 28, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.33.1.95 on 1 January 1971. Dow
nloaded from