Embed Size (px)
Citation preview
09/24/2012
1
Heart Failure: Optimizing Therapies to Advancing Care Options
Carolyn M Moffa MSN, FNP-C, CHFN
Deb Dougherty MSN, RN
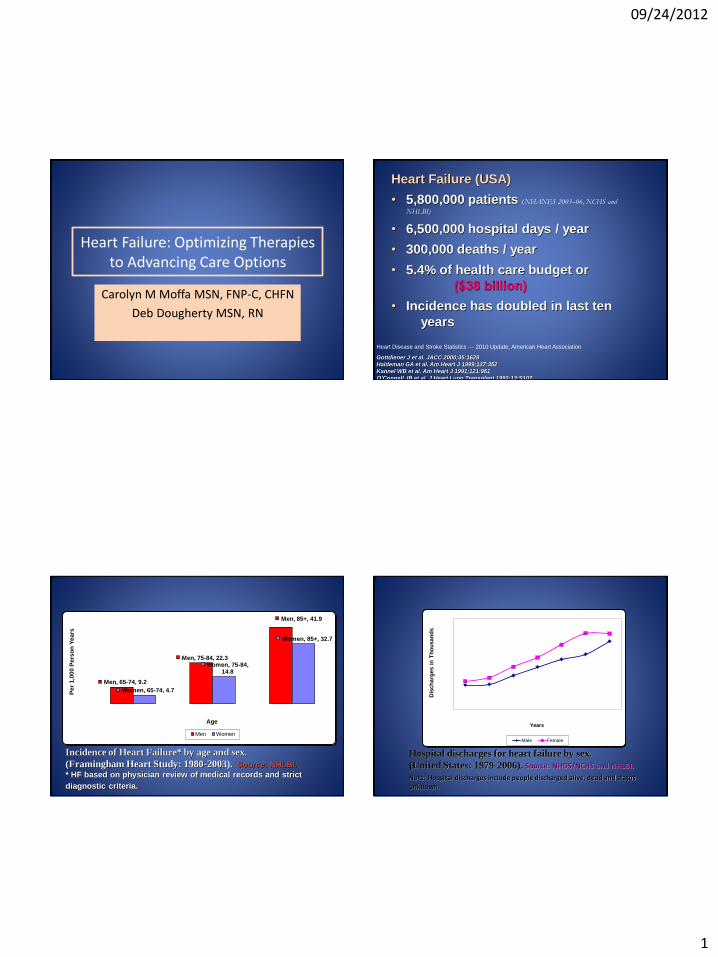
Heart Failure (USA)
• 5,800,000 patients (NHANES 2003–06, NCHS and
NHLBI)
• 6,500,000 hospital days / year
• 300,000 deaths / year
• 5.4% of health care budget or
($38 billion)
• Incidence has doubled in last ten
years
Heart Disease and Stroke Statistics — 2010 Update, American Heart Association
Gottdiener J et al. JACC 2000;35:1628
Haldeman GA et al. Am Heart J 1999;137:352
Kannel WB et al. Am Heart J 1991;121:951
O’Connell JB et al. J Heart Lung Transplant 1993;13:S107
Incidence of Heart Failure* by age and sex.
(Framingham Heart Study: 1980-2003). Source: NHLBI.
* HF based on physician review of medical records and strict
diagnostic criteria.
Men, 65-74, 9.2
Men, 75-84, 22.3
Men, 85+, 41.9
Women, 65-74, 4.7
Women, 75-84, 14.8
Women, 85+, 32.7
Per
1,0
00 P
ers
on
Years
Age
Men Women
Note: Hospital discharges include people discharged alive, dead and status unknown.
Hospital discharges for heart failure by sex.
(United States: 1979-2006). Source: NHDS/NCHS and NHLBI.
Dis
ch
arg
es i
n T
ho
usa
nd
s
Years
Male Female
09/24/2012
2
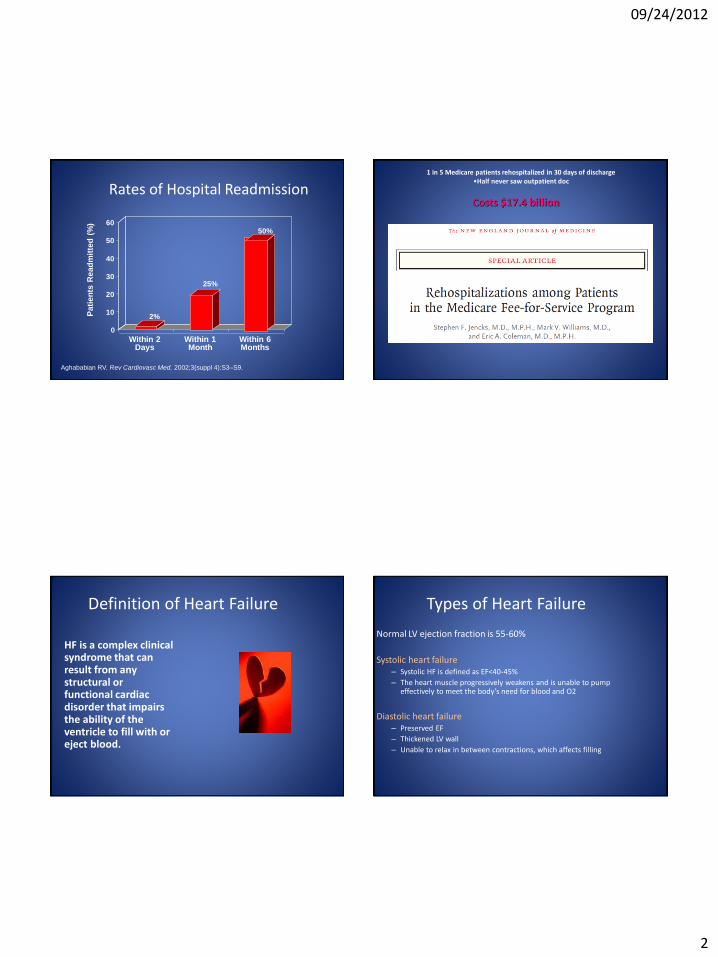
Rates of Hospital Readmission
0
10
20
30
40
50
60
Within 2 Days
Within 1 Month
Within 6 Months
Pati
en
ts R
ead
mit
ted
(%
)
2%
25%
50%
Aghababian RV. Rev Cardiovasc Med. 2002;3(suppl 4):S3–S9.
1 in 5 Medicare patients rehospitalized in 30 days of discharge •Half never saw outpatient doc
Costs $17.4 billion
Definition of Heart Failure
HF is a complex clinical syndrome that can result from any structural or functional cardiac disorder that impairs the ability of the ventricle to fill with or eject blood.
Types of Heart Failure
Normal LV ejection fraction is 55-60%
Systolic heart failure – Systolic HF is defined as EF<40-45%
– The heart muscle progressively weakens and is unable to pump effectively to meet the body’s need for blood and O2
Diastolic heart failure – Preserved EF
– Thickened LV wall
– Unable to relax in between contractions, which affects filling
09/24/2012
3
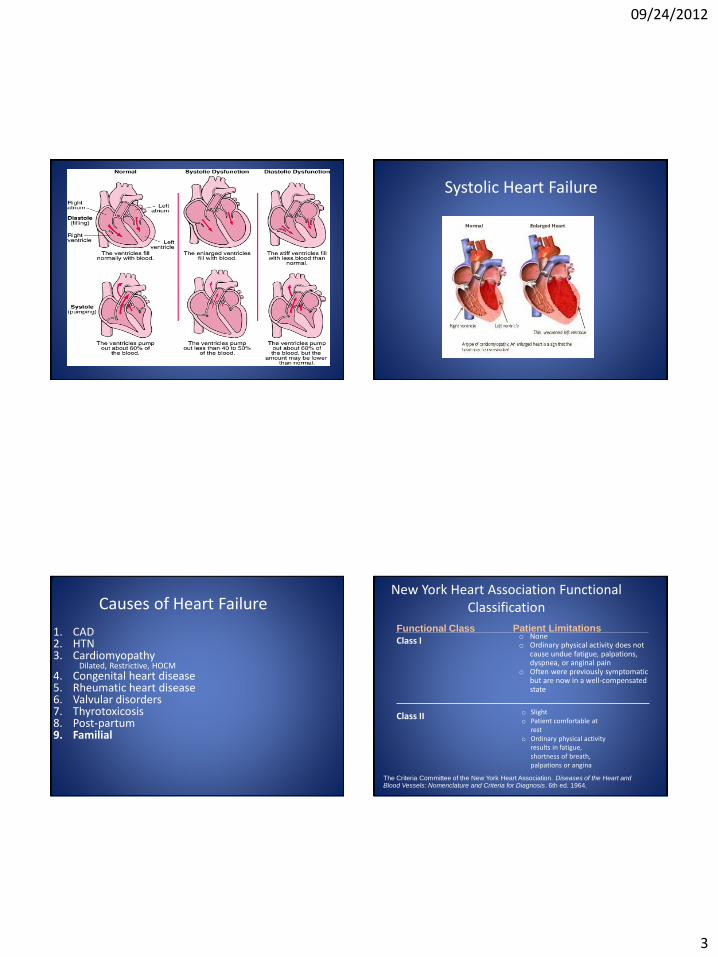
Systolic Heart Failure
Causes of Heart Failure
1. CAD 2. HTN 3. Cardiomyopathy
Dilated, Restrictive, HOCM
4. Congenital heart disease 5. Rheumatic heart disease 6. Valvular disorders 7. Thyrotoxicosis 8. Post-partum 9. Familial
New York Heart Association Functional Classification
o None o Ordinary physical activity does not
cause undue fatigue, palpations, dyspnea, or anginal pain
o Often were previously symptomatic but are now in a well-compensated state
Functional Class Patient Limitations
The Criteria Committee of the New York Heart Association. Diseases of the Heart and Blood Vessels: Nomenclature and Criteria for Diagnosis. 6th ed. 1964.
Class I
Class II o Slight o Patient comfortable at
rest o Ordinary physical activity
results in fatigue, shortness of breath, palpations or angina
09/24/2012
4
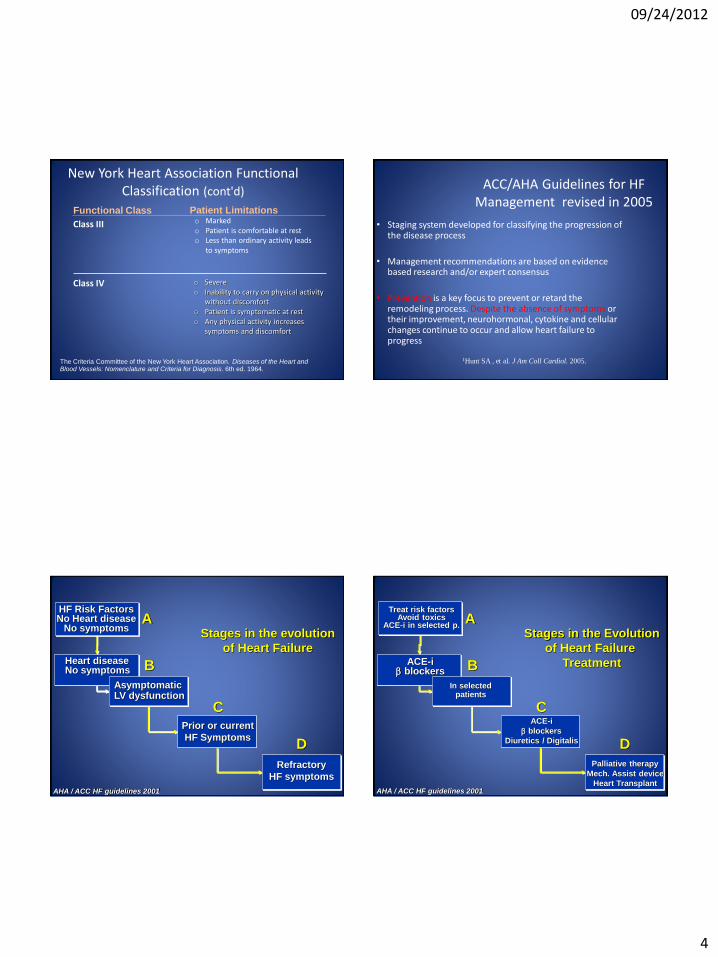
New York Heart Association Functional Classification (cont'd)
o Marked o Patient is comfortable at rest o Less than ordinary activity leads
to symptoms
o Severe o Inability to carry on physical activity
without discomfort o Patient is symptomatic at rest o Any physical activity increases
symptoms and discomfort
Functional Class Patient Limitations
The Criteria Committee of the New York Heart Association. Diseases of the Heart and Blood Vessels: Nomenclature and Criteria for Diagnosis. 6th ed. 1964.
Class III
Class IV
ACC/AHA Guidelines for HF Management revised in 2005
• Staging system developed for classifying the progression of the disease process
• Management recommendations are based on evidence based research and/or expert consensus
• Prevention is a key focus to prevent or retard the remodeling process. Despite the absence of symptoms or their improvement, neurohormonal, cytokine and cellular changes continue to occur and allow heart failure to progress
1Hunt SA , et al. J Am Coll Cardiol. 2005.
Heart disease No symptoms
HF Risk Factors No Heart disease
No symptoms
Asymptomatic LV dysfunction
Refractory
HF symptoms
Prior or current
HF Symptoms
Stages in the evolution
of Heart Failure
A
B
C
D
AHA / ACC HF guidelines 2001
ACE-i blockers
Treat risk factors Avoid toxics
ACE-i in selected p.
In selected patients
Palliative therapy
Mech. Assist device
Heart Transplant
ACE-i
blockers
Diuretics / Digitalis
Stages in the Evolution
of Heart Failure
Treatment
A
B
C
D
AHA / ACC HF guidelines 2001

09/24/2012
5
Case Study
August 2007
HPI
• TD: 26 year old female s/p delivery of healthy baby girl
• PMH/PSH
-Negative
• Medications
-Prenatal vitamins
• Allergies
-NKDA
• Social History
-+ tobacco 1PPD
-+ marijuana
- Negative ETOH
• Family History – Father: died secondary to HF,
SCD
– Mother: living, healthy
– Uncle: died SCD
Case Study
January 2008 (5 months PP) • Chief complaint:
– cough, SOB, fatigue, unable to do activities
• Physical exam: – BP 118/64 P88 T96.8 – General: healthy appearing female – HEENT: unremarkable – Neck: +JVD ~ 10cm – CV: RRR, +S1S2; neg S3, neg murmurs – Resp: Unlabored; +bibasilar crackles – Abd: soft with +NABS; nontender;
neg ascites – Exts: +2 edema BLEs – Neuro: CN II-XII intact; neg
motor/sensory deficits – Skin: no rashes, lesions
• Medications – None
• Labs: BMP normal; CBC normal; TSH normal; – BNP 6532
• CXR: Mild cardiomegaly and
interstitial edema
• Echo: LA dilated; LV dilated; severe global LV hypokinesis; EF 20%
Case Study
January 2008 (5 months PP) • A/P
– 1. Newly diagnosed cardiomyopathy with clinical evidence of HF
– Etiology? Postpartum vs familial vs viral
• Recommend – Lasix 40mg daily (IV to PO) – Lisinopril 20mg – Coreg 3.125mg BID – Education (Low Na diet, daily
weights, fluid restrictions, meds and side effects, dosing, etc)
– Plan for ICD in 3 months if no improvement in EF
March 2008
• ICD implant
Current Pharmacologic Approach to Heart Failure approved drugs, recommended for routine use
• Effect – Interferes with RAAS; enhances actions of kinins, prostaglandin
synthesis, delays remodeling
– Alleviate symptoms, reduce death, hospitalizations
• Clinical use: systolic and diastolic heart failure
– Given to all patients with systolic dysfunction
• Adverse effects
– Hypotension, azotemia, hyperkalemia, cough, angioedema
ACE inhibitors
09/24/2012
6
Current Pharmacologic Approach to Heart Failure approved drugs, recommended for routine use
• Effect – Inhibit the adverse effects of sympathetic system
– Delays and reverses remodeling
• Clinical use: systolic and diastolic heart failure
– Given to all patients with systolic HF in absence of fluid overload
• Adverse effects
– Hypotension, bradycardia, worsening HF
Beta blockers
Current Pharmacologic Approach to Heart Failure
• Effect – Antagonizes the distal convoluted tubule aldosterone
receptors
• Clinical Use – NYHA Class III-IV heart failure
• Adverse effects – Hyperkalemia (hold if K>5.0mEq/L or Cr>4 mg/dl)
– Renal failure
– Agranulocytosis
– Hepatotoxicity
Aldactone
Current Pharmacologic Approach to Heart Failure
• Effect – Directly dilates peripheral vessels
• Clinical use – Consider adding in patients already on ACE-I and B-Blocker who
are still symptomatic – Systolic and diastolic heart failure – Effective in African American patients with HF
• (A- HeFT Trial: J Card Fail 2002 Jun; 8 (3): 128-35)
• Adverse effects – Hypotension; Headache; Palpitations
Hydralazine/Imdur Diuretics in HF
• Mainstay in HF treatment • Directly reduces excess levels of extracellular
fluid • Symptom relief from congestion • Loop diuretics preferred due to increase in
sodium excretion up to 20-25%, enhances free water clearance, and is effective until renal function severely impaired

09/24/2012
7
SCD and Heart Failure
• Patients with HF are 6-9x more likely to develop lethal arrythmia and die from SCD
• Implantable cardiac defibrillator (ICD) as preventative therapy for SCD
• Patients with dyssynchrony (widened QRS) and EF<35%, may benefit from BiVentricular ICD to help restore synchrony and improve cardiac output
Mode of Death in HF Patients By Disease Severity
NYHA IV NYHA II NYHA III
Other 11% Other 24% Other 15%
CHF
56%
SD
33% CHF
12%
CHF
26%
SD
64% SD
59%
No. of deaths
n=27
No. of deaths
n=103
No. of deaths
n=232*
*One case unclassified
MERIT-HF Study Group. Lancet. 1999;353:2001–2007.
SD = Sudden death; CHF = mortality secondary to worsening heart failure
Other
11% Other
15% Other
24%
Case Study
June 2008 (3 months after ICD implant)
• Referral made by cardiologist to the Heart Failure Program for further management and consideration of advanced therapies – Maximal medical therapy,
education and counselling provided, prophylactic ICD in place….what’s the next step for a 27 year old patient with Class IV, Stage D HF???
Stage D
• Palliative Therapy
• Mechanical Assist Device
• Heart Transplant
Mechanical Assist Devices for Advanced Heart Failure

09/24/2012
8
Christiana Care LVADS
• 5 DT Implants since July 2011
• Managing 9 patients in the community
• Applying for JC certification this year
Indications for LVAD
• Bridge to Transplant – Non-reversible left heart failure
– Imminent risk of death
– Candidate for cardiac transplantation
• Destination Therapy – NYHA Class IIIB or IV heart failure
– Optimal medical therapy 45 of last 60 days
– Not candidate for cardiac transplantation
• For in-patient and out-patient use – May be transported via ground ambulance, fixed wing aircraft or
helicopter
Key Design Features
• Blood pump rotor is the only moving part
• Rotor spins on blood-lubricated bearings designed for long life
• Blood pump is driven by an integrated electric motor
• All motor drive and control electronics are outside of the implanted blood pump
• Speed range: 6,000 to 15,000 rpm
• Flow range: 3 – 10 L/min
HeartMate II Animation
09/24/2012
9
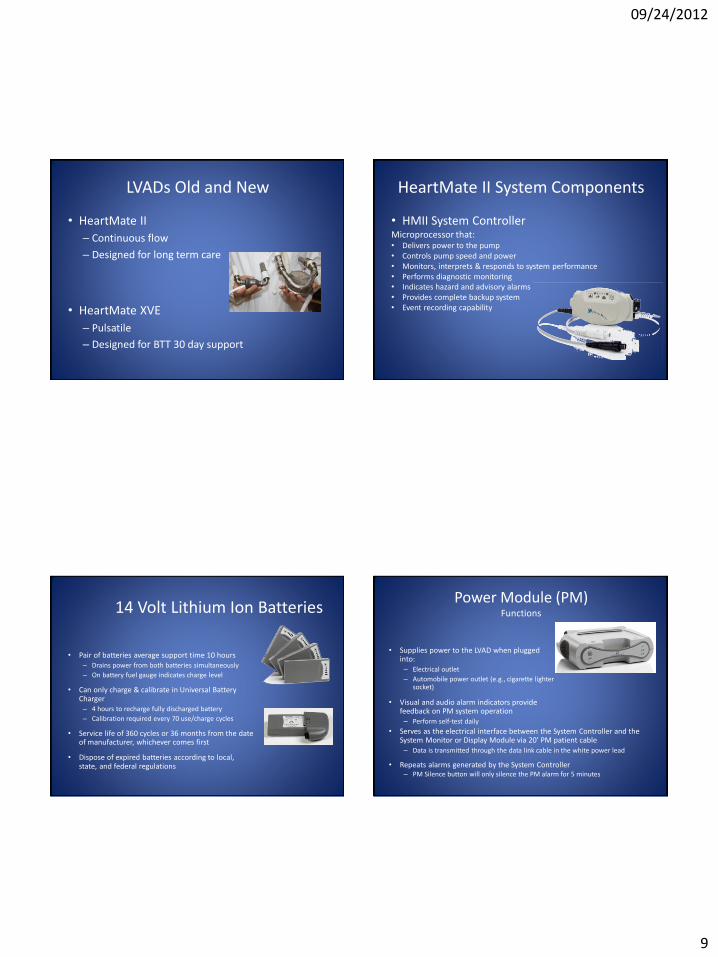
LVADs Old and New
• HeartMate II
– Continuous flow
– Designed for long term care
• HeartMate XVE
– Pulsatile
– Designed for BTT 30 day support
HeartMate II System Components
• HMII System Controller Microprocessor that: • Delivers power to the pump • Controls pump speed and power • Monitors, interprets & responds to system performance • Performs diagnostic monitoring • Indicates hazard and advisory alarms • Provides complete backup system • Event recording capability
14 Volt Lithium Ion Batteries
• Pair of batteries average support time 10 hours – Drains power from both batteries simultaneously
– On battery fuel gauge indicates charge level
• Can only charge & calibrate in Universal Battery Charger – 4 hours to recharge fully discharged battery
– Calibration required every 70 use/charge cycles
• Service life of 360 cycles or 36 months from the date of manufacturer, whichever comes first
• Dispose of expired batteries according to local, state, and federal regulations
Power Module (PM) Functions
• Serves as the electrical interface between the System Controller and the System Monitor or Display Module via 20’ PM patient cable – Data is transmitted through the data link cable in the white power lead
• Repeats alarms generated by the System Controller – PM Silence button will only silence the PM alarm for 5 minutes
• Supplies power to the LVAD when plugged into: – Electrical outlet
– Automobile power outlet (e.g., cigarette lighter socket)
• Visual and audio alarm indicators provide feedback on PM system operation – Perform self-test daily
09/24/2012
10
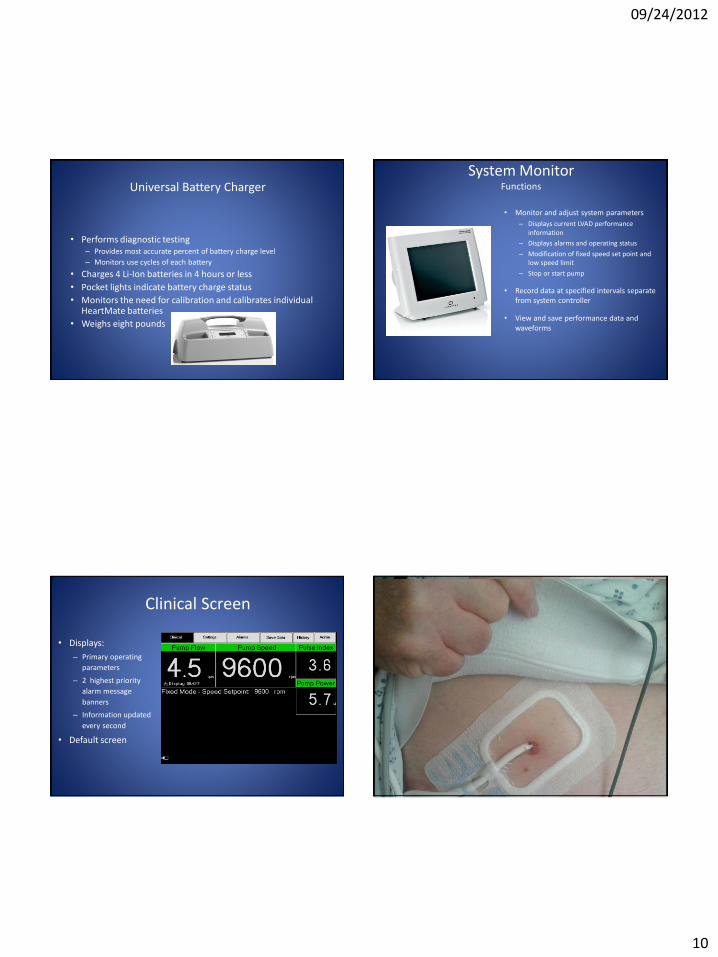
Universal Battery Charger
• Performs diagnostic testing – Provides most accurate percent of battery charge level
– Monitors use cycles of each battery
• Charges 4 Li-Ion batteries in 4 hours or less
• Pocket lights indicate battery charge status
• Monitors the need for calibration and calibrates individual HeartMate batteries
• Weighs eight pounds
System Monitor Functions
• Monitor and adjust system parameters
– Displays current LVAD performance information
– Displays alarms and operating status
– Modification of fixed speed set point and low speed limit
– Stop or start pump
• Record data at specified intervals separate from system controller
• View and save performance data and waveforms
Clinical Screen
• Displays:
– Primary operating
parameters
– 2 highest priority
alarm message
banners
– Information updated
every second
• Default screen
Driveline Site

09/24/2012
11
Clinical Factors to consider with LVAD
• Patients are on Coumadin and ASA
• May not have peripheral pulses
• BP by doppler method with a goal BP of 60 to 90
• No limitations with Cardioversion and Defibrillation
• CPR ?
• Driveline dressing change is sterile technique
Accessories
Shower Bag
Modular Belt Consolidated Bag
Holster Vest
Anatomical Placement Case Study
• Heart Failure Program
– Begin LVAD/cardiac transplant evaluation
• HIV, hepatitis profile, BMP, LFTs, nutrition eval; psychosocial eval; financial eval, etc
– Optimize medications
– Extensive counselling
– Absolute need for smoking cessation
– VO2 study for risk stratification

09/24/2012
12
Case Study
• Lost to follow-up!! And resurfaced three years later in March 2011!
– Hospitalized with diagnosis pneumonia
– Seen post discharge in NP HF clinic
• Was out of all HF medications
• Pt declined repeat echo (last echo was March 2008)
• Declined referral to EP for ICD interrogation
• Agreed to be rescheduled with HF Program to continue evaluation for LVAD/cardiac transplant
Case Study
• But…..was lost to follow-up!!!! And resurfaced one year later, 3/2012, when hospitalized for decompensated HF
• HPI – CC: extreme SOB, fatigue, orthopnea, PND, edema,
weight gain, early satiety, ascites – Echo: severe dilated cardiomyopathy with EF <10% – Consult to HF Program
• RHC: RA 15 (3-5); RV moderately to severely reduced; Severe MR; EF 10%; CO 1.6 (4-8)
• IV Milrinone initiated due to low output HF • Plan: LVAD as bridge to cardiac transplant
Case Study
• TD underwent successful implant of HM II LVAD on April 30, 2012!!
• Her clinical status has improved tremendously! • She maintains 100% compliance with her
medications, diet, exercise, follow-up medical appointments, and the care of her LVAD and driveline.
• She is listed for cardiac transplant!! • TD was invited to join us today at the conference,
but was unable to attend as she has enrolled in dental hygienist school!
Resources
• HF Clinic
– (302)733-1663
• Clinical Leader Heart Failure Program
– Carolyn M Moffa MSN, FNP-C, CHFN
– (302) 733-1663 or (302) 733-1293
• Director Heart Failure Program
– Dr Mitchell Saltzberg
– (302) 733-1507

09/24/2012
13
Deb Dougherty RN MSN VAD Coordinator 302-733-1834
To Reach the VAD Coordinator on Call Dial 1-855-VAD-CCHS 1-855-823-2247
Option 1
Thank you !!
• DVD from thoratec with pt testimonials





























