Embed Size (px)
Citation preview

Transthoracic echocardiography revealed alarge posteroinferior akinesis and an an-teroseptal hypokinesis without pericardialeffusion (PE). The next day the patient be-came abruptly hypotensive. Central venouspressure was 12 mmHg and jugular veinswere turgescent. Chest X-ray showed car-diomegaly with a double edge (Fig. 1).Blood pressure was restored after fluidchallenge. Because of suspected PE withcompromised cardiac filling, a transesoph-ageal echocardiography (TEE) was per-formed but failed to show any PE. The car-diac kinetics remained unchanged but theleft atria was compressed by a mediastinalmass. The mitral inflow Doppler signal
demonstrated large respiratory variations.The right ventricle was normokinetic al-though compressed, too.
A computerized tomodensitometry(CT) of the chest was performed and dem-onstrated a large anterior mediastinal he-matoma (MH) collected near the superiorvena cava ( Fig. 2) extending in front ofthe pericardium, above the diaphragm andcompressing the right ventricle. Acute re-nal failure appeared the next day with olig-uria and water overload. Continuous veno-venous hemofiltration was instituted. Atrialfibrillation refractory to electric or chemi-cal cardioversion caused hypotension resis-tant to increasing catecholamines. The pa-
Intensive Care Med (2003) 29:507–508DOI 10.1007/s00134-002-1632-8 C O R R E S P O N D E N C E
Vincent FraipontJean-Luc PetersThierry WeberChristophe LevauxClaude ChevoletLéon RadouxFrançois Damas
Heart enlargement after thrombolysis for unsuccessfulresuscitation
Received: 6 August 2002Accepted: 29 November 2002Published online: 24 January 2003© Springer-Verlag 2003
Abstract Thrombolysis has been recentlyreported for the treatment of unsuccessfulout-of-hospital cardiopulmonary resuscita-tion. This case report presents the first caseof mediastinal hematoma following throm-bolysis in this setting. Chest X-ray and he-modynamic pattern mimicked pericardialeffusion with cardiac-filling compromise.Diagnosis was established by transesopha-geal echocardiography and chest computer-ized tomodensitometry.Electronic supplementary material tothis paper can be obtained by using theSpringer Link server located athttp://dx.doi.org/10.007/s00134-002-1632-8.
Keywords Cardiopulmonary resuscitation ·Complications · Hemorrhage · Mediastinaldiseases · Sternum · Thrombolysis
Sir: Thrombolysis has been recently re-ported to stabilize patients with cardiac ar-rest and unsuccessful cardiopulmonary re-suscitation (CPR) [1]. We discuss the caseof a severe complication never reportedbefore.
A 72-year-old man was admitted to thehospital after resuscitation from suddendeath, with advanced life support providedby the mobile ICU. Repetitive ventricularfibrillation occurred despite a combinationof external counter shock and treatmentwith xylocaine and amiodarone. The elec-trocardiogram showed an acute inferiormyocardial infarction so thrombolysis wasinduced by the injection of reteplase 20 U,resulting in subsequent rhythm stabiliza-tion. On admission to ICU, the patient washemodynamically stable and ventilatedwith poor neurological status (e.g. withouta reaction to pain, miotic and fixed pupils).A sternal fracture was clinically visible.
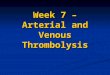
Fig. 1 Posteroanterior chest X-ray demonstrates cardiomegaly with double edge
Fig. 2 Computerized tomodensitometry shows large anterior mediastinal hematoma col-lecting near the superior vena cava and extending in front of pericardium

tient died on the 4th day due to extensiveischemic cardiac damage.
We therefore report the occurrence ofan unusual complication of thrombolysisafter unsuccessful CPR, which could haveexacerbated the primary heart injury. Inthis case, MH was not the direct cause ofdeath but it worsened hypotension throughheart compression at least at times duringthe evolution. The compromised cardiacfilling was reverted by fluid challenge aswould be expected in a tamponade. TEEsuggested MH with significant right heartcompression, which was confirmed by CT.TEE has been recently recommended forassessment of the extent of the hemomedi-astinum [2] and differential diagnosis withPE. TEE is conveniently performed at thebedside, safe and cost-effective. On theother side, CT allows good diagnostic ac-curacy and is available 24 h a day [3].
This is the first report of a MH with he-modynamic instability, secondary to a ster-nal fracture complicating CPR. The throm-bolysis certainly favored this bleeding. In-
deed, one case of spontaneous mediastinalhemorrhage following thrombolysis with-out CPR has been described already [4].On the other hand, a sternal fracture withMH is not uncommon in the context oftrauma but a mediastinal tamponade hasbeen reported only twice [3]. Althoughheart and chest injuries are also commonlyreported after CPR [5], no hemomediasti-num has been reported so far.
Were thrombolysis for unsuccessfulCPR to be generalized, all intensivistsshould be aware of this potential complica-tion.
References
1. Bottiger BW, Bode C, Kern S, Gries A,Gust R, Glatzer R, Bauer H, Motsch J,Martin E (2001) Efficacy and safety ofthrombolytic therapy after initially un-successful cardiopulmonary resuscita-tion: a prospective clinical trial. Lancet357:1583–1585
2. Vignon P, Rambaud G, Francois B, Preux PM, Lang RM, Gastinne H (1998)Quantification of traumatic hemomedi-astinum using transesophageal echocar-diography: impact on patient manage-ment. Chest 113:1475–1480
508
3. Crestanello JA, Samuels LE, KaufmanMS, Thomas MP, Talucci R (1999) Ster-nal fracture with mediastinal hematoma:delayed cardiopulmonary sequelae. J Trauma 47:161–164
4. Suddes KP, Thomas RD (1988) Medias-tinal hemorrhage: a complication ofthrombolytic treatment. BMJ 297:527–527
5. Baubin M, Rabl W, Pfeiffer KP, BenzerA, Gilly H (1999) Chest injuries afteractive compression-decompression car-diopulmonary resuscitation (ACD-CPR)in cadavers. Resuscitation 43:9–15
V. Fraipont (✉) · J.-L. Peters · T. WeberC. Levaux · C. Chevolet · L. RadouxF. DamasIntensive Care Unit, CHR Citadelle,Boulevard XIIème de Ligne 1, 4000 Liège,Belgiume-mail: [email protected].: +32-4-2257161Fax: +32-4-2256508